Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Residual Inflammatory Risk Is Associated with Cognitive Impairment After Acute Ischemic Stroke
Authors Gang Y, Gong X ![]() , Zhu B
, Zhu B ![]() , Yu C, Xue M, Wang T, Chen C
, Yu C, Xue M, Wang T, Chen C
Received 1 August 2025
Accepted for publication 29 November 2025
Published 19 December 2025 Volume 2025:21 Pages 2871—2880
DOI https://doi.org/10.2147/NDT.S557670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Yuwen Gang,1,2 Xiuqun Gong,1 Beibei Zhu,1 Chuanqing Yu,1 Min Xue,1 Tao Wang,1 Congxia Chen1
1Department of Neurology, the First Hospital of Anhui University of Science and Technology, Huainan, Anhui Province, People’s Republic of China; 2School of Medicine, Anhui University of Science and Technology, Huainan, Anhui Province, People’s Republic of China
Correspondence: Xiuqun Gong, Department of Neurology, the First Hospital of Anhui University of Science and Technology, 203 Huaibin Road, Huainan, Anhui Province, 232007, People’s Republic of China, Tel +86-15395474600, Email [email protected]
Objective: Acute ischemic stroke (AIS) may lead to varying degrees of cognitive impairment, while the inflammatory response plays a significant role in this process. This study aims to examine the relationship between residual inflammation risk (RIR) and the development of post-stroke cognitive impairment (PSCI) in patients with acute ischemic stroke.
Methods: This prospective cohort study enrolled a total of 172 patients diagnosed with AIS over the study period from January 2024 to December 2024. They were divided into four groups: RIR only [low-density lipoprotein cholesterol (LDL-C) < 2.6 mmol/L and high-sensitivity CRP (hsCRP) ≥ 2 mg/L], residual cholesterol risk (RCR) only (LDL-C ≥ 2.6 mmol/L and hsCRP < 2 mg/L), both risk or residual cholesterol and inflammatory risk (RCIR) (LDL-C ≥ 2.6 mmol/L and hsCRP ≥ 2 mg/L), and neither risk (LDL-C < 2.6mmol/L and hsCRP < 2 mg/L). PSCI is defined as a Montreal Cognitive Assessment (MoCA) score below 22 at 6 months after stroke. The final analysis included 172 patients who completed the follow-up. The association between RIR and PSCI was analyzed by multivariable logistic regression analyses.
Results: Among the 172 enrolled patients, 58 (33.7%) developed PSCI. The proportion of patients with neither risk, RIR, RCR, and RCIR was 23.8% (n=41),18.6% (n=32), 32.0% (n=55) and 25.6% (n=44), respectively. Compared to those without PSCI, patients with PSCI had a higher prevalence of hyperlipidemia (P = 0.026), a greater proportion of RIR (P = 0.015), and higher white blood cell count (P = 0.042) and neutrophil count (P = 0.016). Logistic regression analysis, adjusting for major confounding factors, identified RIR as an independent factor associated with PSCI occurrence (OR 4.496, 95% CI 1.571– 17.477, P = 0.030; RCIR: OR 7.357, 95% CI 2.081– 26.006, P = 0.002).
Conclusion: This study presents what is, to our knowledge, the first evidence that RIR is associated with PSCI among acute ischemic stroke patients.
Keywords: residual inflammatory risk, post-stroke cognitive impairment, acute ischemic stroke
Introduction
Stroke remains a leading global cause of death and disability. Acute ischemic stroke (AIS) constitutes its most common and predominant subtype.1 While advancements in acute medical care have increased the number of stroke survivors, a notable proportion, approximately 30% to 40% experience progressive cognitive decline during recovery, ultimately developing post-stroke cognitive impairment (PSCI). PSCI significantly reduces quality of life and increases the societal care burden, presenting a major challenge in cerebrovascular disease prevention and management.2,3 Studies indicate that 26.1% of patients with first-ever ischemic stroke exhibit cognitive impairment at 90 days post-event, with this prevalence further increasing by 6 months.4,5
Increasing evidence shows that inflammation plays a key role in the pathophysiological process of stroke and may be an important driver of the occurrence and development of PSCI. An acute ischemic stroke event triggers an intense local and systemic inflammatory response. Ischemia-hypoxia in brain tissue leads to the release of damage-associated molecular patterns (DAMPs), which activate microglia and astrocytes, and promote the infiltration of peripheral immune cells into the brain parenchyma. These cells release large amounts of pro-inflammatory cytokines (such as IL-1β, IL-6, TNF-α) and chemokines.6–9 This persistent inflammatory state not only exacerbates secondary brain injury and compromises blood-brain barrier (BBB) integrity but also directly impairs neuronal and synaptic function and adversely affects neuroplasticity.10–12 Multiple clinical studies have observed that elevated levels of circulating inflammatory biomarkers during the acute or recovery phase are significantly associated with subsequent cognitive decline and an increased risk of PSCI in stroke patients.13,14 This suggests that chronic, low-grade inflammatory responses, whether systemic or within the central nervous system, may serve as a potential biological pathway connecting acute cerebrovascular events to long-term cognitive deterioration.
The well-established relationship between cardio-cerebral vascular diseases and low-density lipoprotein cholesterol (LDL-C) is widely recognized. However, the PROVE IT-TIMI trial demonstrated that despite achieving significant reductions in LDL-C levels, patients receiving intensive statin therapy still exhibited residual cardiovascular risk. This residual risk may be linked to underlying inflammation.15 Consequently, residual inflammatory risk (RIR) is commonly defined based on elevated high-sensitivity C-reactive protein (hsCRP) levels, typically using a threshold of ≥2 mg/L.16 Current research continues to explore novel risk markers for ischemic stroke.17 However, in contrast to indicators such as the triglyceride-glucose index, the association between residual inflammatory risk (RIR)—a well-established predictor of cardiovascular events—and post-stroke cognitive impairment (PSCI) has not been sufficiently investigated. Clarifying this association could hold certain implications for personalized medicine, potentially identifying patients who would benefit most from targeted anti-inflammatory strategies to mitigate cognitive decline. This study, therefore, aims to investigate the association between elevated RIR and PSCI in patients with acute ischemic stroke.
Materials and Methods
Study Population
This prospective study enrolled patients with AIS admitted to the Department of Neurology at the First Hospital of Anhui University of Science and Technology between January 2024 and December 2024. The study protocol received approval from the hospital’s Ethics Committee, and written informed consent was obtained from all participants.
Inclusion criteria comprised: (1) hospital admission within 7 days of symptom onset; and (2) age ≥ 18 years. Exclusion criteria were: (1) use of cognition-affecting medications within the preceding 2 weeks or pre-existing cognitive impairment; (2) Montreal Cognitive Assessment (MoCA) score < 22; and (3) severe acute/chronic infection, autoimmune disease, or malignancy.
Baseline Data Collection
Baseline clinical data, including age, sex, height, weight, educational attainment, current smoking status, current alcohol intake status, and medical history (hypertension, diabetes, hyperlipidemia, and ischemic stroke), were extracted from medical records. Educational attainment was categorized as either ≤9 years or >9 years. Clinical conditions were operationally defined as follows: Hypertension was diagnosed as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on three separate resting measurements, or current antihypertensive medication use; diabetes required fasting blood glucose ≥7.0 mmol/L and/or 2-hour postprandial blood glucose ≥11.1 mmol/L, or current treatment with insulin or oral hypoglycemic agents; ischemic stroke history was documented as present or absent based on medical records; smoking status defined current smokers as those actively smoking or having quit within one month prior to admission; alcohol intake was defined as consumption at least twice monthly.
Blood Sample Collection and Measurements
Fasting venous blood should be collected within 24 hours after admission. The median time from symptom onset to blood collection was 31.6 hours. Laboratory analyses included: lipid profile [total cholesterol, triglycerides, LDL-C, high-density lipoprotein cholesterol (HDL-C)] measured using a Siemens ADVIA 1800 fully automated biochemical analyzer; hsCRP quantified using a Mindray BC 7500 fully automated hematology analyzer; and complete blood count parameters (white blood cells, neutrophils, lymphocytes, monocytes) analyzed using a Sysmex BC 7500 fully automated hematology analyzer.
Post-Stroke Cognitive Impairment Assessment
Enrolled patients underwent baseline cognitive assessment using both the Montreal Cognitive Assessment (MoCA) at admission, with identical reassessments conducted at the 6-month follow-up. The cognitive assessments were conducted by clinicians who had received standardized training and were blinded to the patients’ laboratory results, including RIR group status. The MoCA, chosen for its established superior sensitivity in detecting PSCI, served as the primary outcome. PSCI was defined as a MoCA score of <22 at the 6-month follow-up, capturing short-term cognitive outcomes.18
Statistical Analysis
Statistical analysis was carried out using software SPSS (version 26.0), and R (version 4.4.3). Continuous variables were assessed for normality via the Kolmogorov–Smirnov test. Normally distributed data are presented as mean ± standard deviation (SD) and compared using independent samples t-test, non-normally distributed data are expressed as median (interquartile range) with Mann–Whitney U-tests for group comparisons. Categorical and ordinal variables are reported as frequencies (percentages), analyzed using chi-square tests or rank-sum tests, respectively.
Based on current guidelines defining LDL-C <2.6 mmol/L as the treatment target for high-risk populations and hsCRP ≥2 mg/L indicating high inflammatory status,19,20 patients were stratified using these thresholds into four mutually exclusive groups: RIR only (LDL-C <2.6 mmol/L and hsCRP ≥2 mg/L), residual cholesterol risk (RCR) only (LDL-C ≥2.6mmol/L and hsCRP <2 mg/L), both risk or residual cholesterol and inflammatory risk (RCIR) (LDL-C ≥2.6 mmol/L and hsCRP ≥2 mg/L), and neither risk (LDL-C <2.6 mmol/L and hsCRP<2 mg/L). The relationship between RIR and PSCI was evaluated using multivariable logistic regression. Three progressively adjusted models were constructed: Model 1 accounted for age and sex; Model 2 additionally adjusted for education level, smoking history, alcohol intake, hypertension, diabetes, hyperlipidemia, prior stroke, and baseline NIHSS scores; Model 3 further incorporated white blood cell and neutrophil counts. Statistical significance was defined as p < 0.05.
Results
Baseline Characteristics
A total of 204 patients with AIS were initially enrolled in this study. Of these, 13 patients developed pulmonary infections, 9 lacked part of the laboratory data, and 10 were lost to follow-up. Consequently, 172 patients completed the 6-month post-discharge follow-up (Figure 1).
Among them, there were 101 men and 71 women. The median age was 70 (60.25–77.75) years and the median duration of education was 6 (3–10) years. Comorbidities among these AIS patients included hypertension (65.7%), diabetes mellitus (34.9%), hyperlipidemia (22.1%), and a history of stroke (27.9%).
Based on the 6 months follow-up assessments, PSCI was diagnosed in 58 patients (33.7%), with the proportions of PSCI varying across different residual risk groups as shown in Figure S1 (Supplementary Figure S1). Comparative data between the PSCI and post-stroke non-cognitive impairment (PSNCI) groups are presented in Table 1. Compared to the PSNCI group, patients in the PSCI group were significantly older (P < 0.001), had fewer years of education (P = 0.004), and exhibited higher white blood cell counts (P = 0.042), neutrophil counts (P = 0.016), and RIR ratio (P < 0.001).
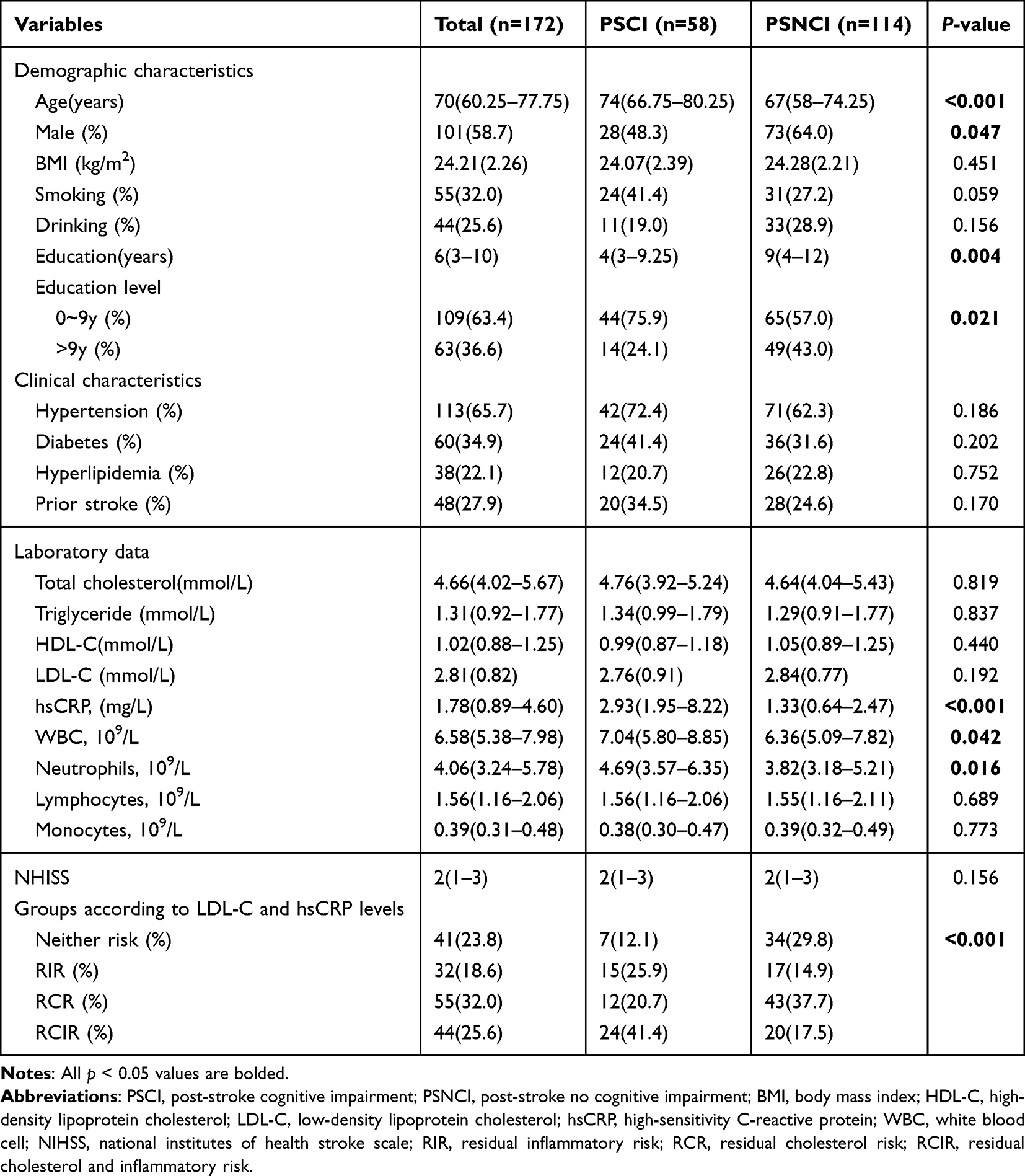 |
Table 1 Baseline Characteristics of the Follow-up Patients by Cognitive Status |
Baseline characteristics stratified by LDL-C and hsCRP levels are shown in Table 2. The proportions of patients categorized as having no residual risk, RIR, RCR, and RCIR were 23.8%, 18.6%, 32.0%, and 25.6%, respectively. Significant differences were observed among the four groups for years of education (P = 0.035), smoking status (P = 0.038), total cholesterol (P < 0.001), HDL-C (P = 0.002), white blood cell count (P < 0.001), neutrophil count (P < 0.001), lymphocyte count (P = 0.015), and monocyte count (P = 0.003).
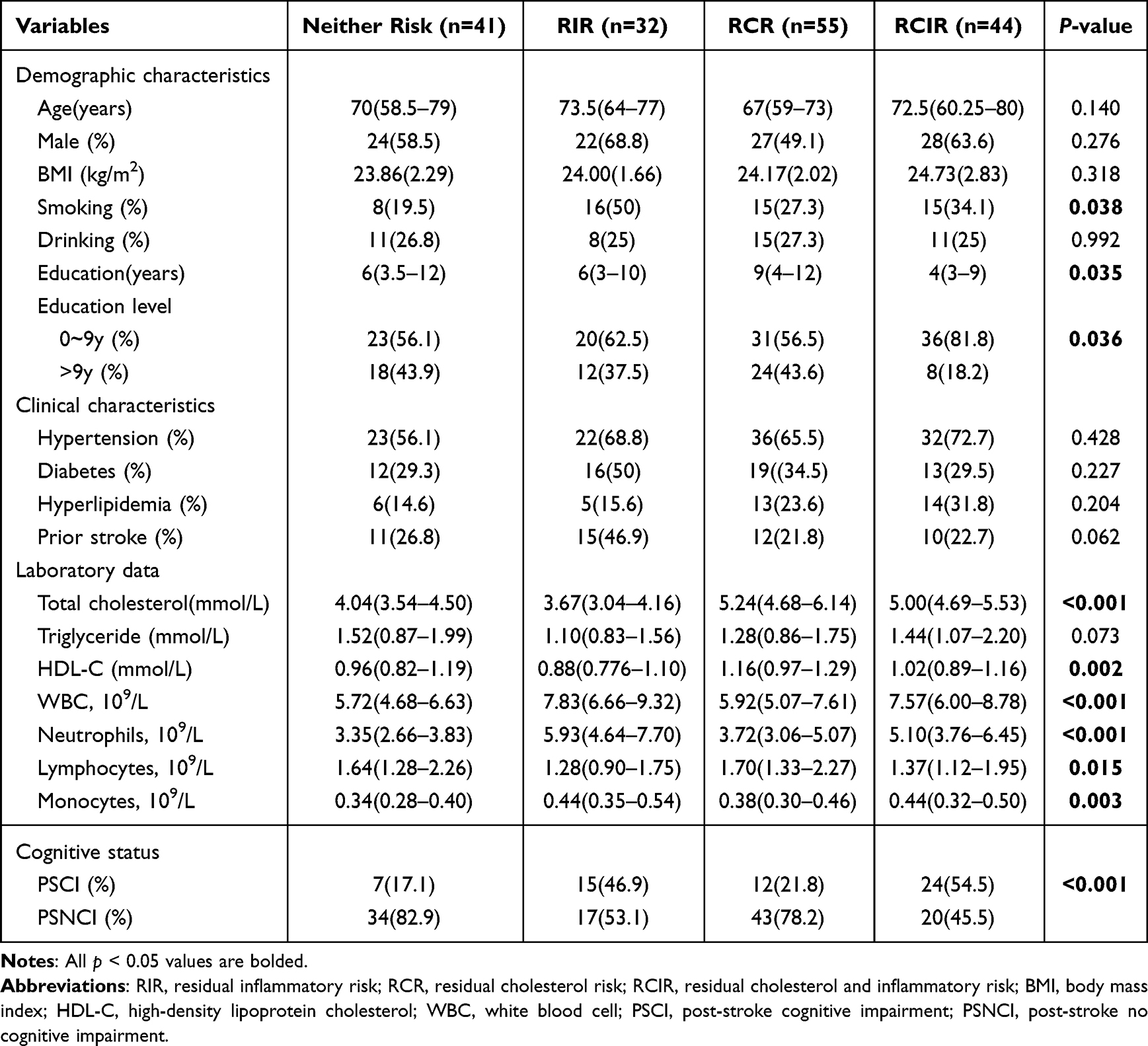 |
Table 2 Baseline Characteristics According to LDL-C and hsCRP Levels |
Associations of RCR, RIR, and RCIR with PSCI
Logistic regression analysis revealed that patients with RIR (OR 4.286, 95% CI 1.471–12.488, P = 0.008) and RCIR (OR 5.829, 95% CI 4.129–15.954, P = 0.001) had a significantly higher risk of developing PSCI compared with patients without residual risk. This association remained significant even after adjusting for gender, age, years of education, smoking status, alcohol consumption, hypertension, diabetes, hyperlipidemia, prior stroke history, white blood cell count, and neutrophil count (RIR: OR 4.496, 95% CI 1.157–17.477, P = 0.030; RCIR: OR 7.357, 95% CI 2.081–26.006, P = 0.002) (Figure 2).
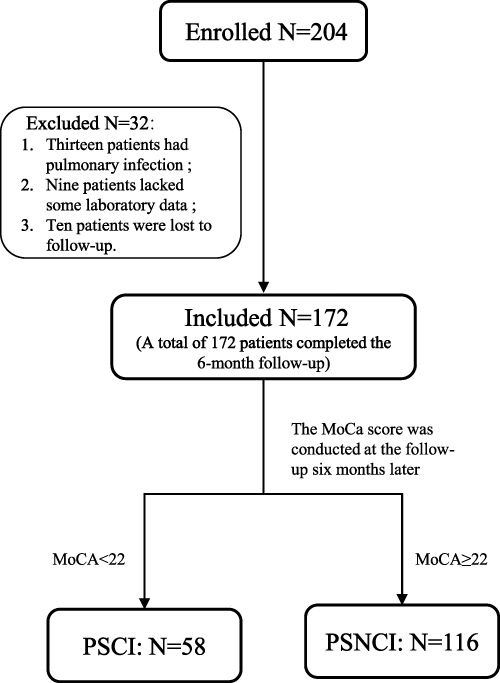 |
Figure 1 Study enrollment flow chart. |
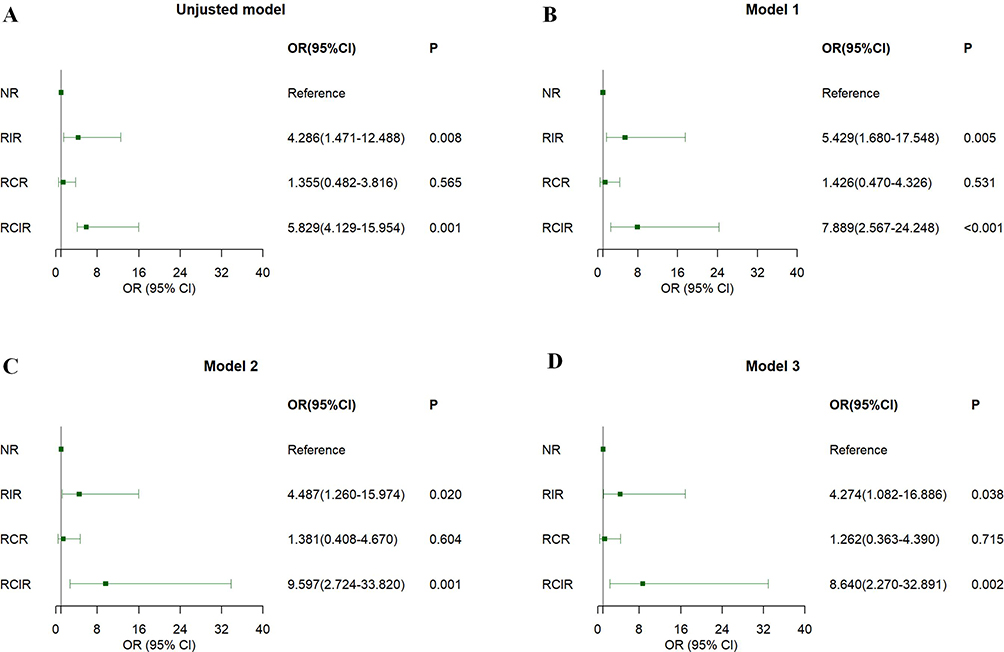 |
Figure 2 Logistic regression analysis for exploring the association between RIR, RCR and RCIR with PSCI (A) Unjusted model (B) Model 1 accounted for age and sex; (C) Model 2 additionally adjusted for education level, smoking history, alcohol intake, hypertension, diabetes, hyperlipidemia, and prior stroke; (D) Model 3 further incorporated white blood cell and neutrophil counts. Abbreviations: PSCI, post-stroke cognitive impairment; OR, odds ratios; CI, confidence interval; NR, neither risk; RIR, residual inflammatory risk; RCR, residual cholesterol risk; RCIR, residual cholesterol and inflammatory risk. |
Discussion
According to the findings of our investigation into the association between RIR and PSCI, RIR and cognitive decline in patients suffering from acute ischemic stroke were substantially positively connected. Furthermore, the robust positive connection between RIR and PSCI persisted even after controlling for potential confounding variables.
Prior studies on PSCI have employed heterogeneous definitions, assessment methods, and study populations, leading to considerable variation in reported epidemiology and associated risk factors. In our cohort of AIS patients, the incidence of PSCI at 6 months was 33.7%. This finding aligns with several previous reports,21,22 but is slightly lower than that reported by Zhao et al.23 This discrepancy may stem from our inclusion criteria, which encompassed only AIS patients and excluded those with transient ischemic attack (TIA). Consistent with earlier research, our study confirms that advanced age and lower educational attainment are significant risk factors for PSCI.24 Mechanistically, aging contributes to cumulative neurobiological damage,25 while lower education levels are associated with reduced cognitive reserve—the brain’s capacity to compensate for damage through alternative neural pathways and adaptive mechanisms.26,27
Multiple clinical studies indicate that RIR is relatively prevalent in clinical practice, with reported incidence rates ranging from 29% to 37%.28–30 In our study, the RIR incidence rate was 18.6%. This comparatively lower rate may be attributable to the limited sample size of this study and differences in the included population. Previous research on RIR has primarily focused on its association with cardiovascular disease, stroke, and their prognoses. For instance, Liao et al demonstrated that RIR is associated with poor postoperative outcomes in patients with acute coronary syndrome,31 while Yu et al found that RIR predicts poor outcomes in patients with symptomatic intracranial atherosclerotic stenosis.32 Furthermore, residual inflammation increases the risk of stroke recurrence, and each recurrent stroke event may cause additional cognitive impairment.33 In this study, we observed that six months after stroke onset, patients with RIR had a significantly higher incidence of PSCI compared to those without RIR. This association persisted even after adjusting for a series of confounding factors. This finding suggests that RIR may serve as a potential predictive biomarker for PSCI, thereby offering a rationale for its use in risk stratification and for enriching patient selection in trials of targeted anti-inflammatory interventions.
Persistent neuroinflammation may underlie the potential mechanism through which RIR contributes to PSCI. First, persistent inflammatory mediators in the circulation can directly cross the compromised blood-brain barrier or activate microglia and astrocytes within the central nervous system (CNS) through signaling pathways. This leads to chronic neuroinflammation, and this sustained inflammatory state causes multiple forms of neural damage.34–36 Second, this sustained neuroinflammation can directly damage neurons and impair synaptic function. Inflammatory cytokines, such as TNF-α and IL-1β, interfere with the expression of synaptic plasticity-associated molecules, including brain-derived neurotrophic factor (BDNF), and compromise neurotransmission as well as learning and memory processes in cognition-critical regions such as the hippocampus.37–39 Third, the inflammatory response further compromises the blood-brain barrier, creating a vicious cycle that allows increased infiltration of peripheral inflammatory mediators and immune cells into the brain parenchyma. These infiltrating components directly impair the neurovascular unit (NVU).34,40–42 Fourth, the chronic inflammatory environment also impairs oligodendrocyte function and impedes remyelination, leading to a decline in white matter integrity and damaged brain network connectivity efficiency.43–45 Finally, the persistent inflammatory state suppresses the survival, proliferation, and differentiation of neural stem cells (NSCs), severely compromising the brain’s intrinsic capacity for self-repair and compensation after stroke.46 Therefore, the sustained, low-level inflammatory state represented by RIR significantly increases the risk of PSCI through synergistic effects on neurons, synapses, blood-brain barrier, white matter and nerve regeneration.
This study has several limitations. First, the single-center design with a specific regional cohort and the modest sample size may introduce selection bias and limit the generalizability of our findings Second, the relatively short follow-up period precludes assessment of the long-term trajectory of RIR and cognitive impairment development; consequently, the current results may underestimate the true magnitude of long-term effects. Third, the number of outcome events was limited relative to the number of covariates in the model (ie, low event-variable ratios), which reflected mainly the wide confidence intervals in the multivariate models, implying uncertainty in the estimation of the precise value of the effect size. Fourth, as an observational cohort study, it demonstrates a significant association between RIR and PSCI but cannot establish causality. Crucially, we lacked data from prospective interventional studies, such as randomized controlled trials of anti-inflammatory therapies, to determine whether reducing RIR effectively prevents PSCI. Finally, although we adjusted for major known confounders, potential unmeasured factors influencing inflammation and cognition (eg, novel biomarkers, detailed lifestyle factors, or subclinical comorbidities) were not evaluated and should be addressed in future investigations.
Conclusion
This study suggests that RIR may serve as a predictor of PSCI in patients with AIS, laying the groundwork for future hypothesis-driven research. Our findings highlight the potential for clinical translation, such as screening for RIR in stroke survivors to identify those at high risk for cognitive decline. The essential next step is the large-scale, multi-center validation of RIR to robustly confirm its value for clinical stratification and intervention.
Ethics Statement
The study was approved by the ethics committee of the First Hospital of Anhui University of Science and Technology (2023-KY-B113-001).
Consent
Informed consent was obtained from all patients.
Funding
This work was supported by Medical Special Cultivation Project of Anhui University of Science and Technology (YZ2023H1C003) and Research Project of Anhui Health Commission (Youth Project supported by Provincial Finance) (AHWJ2023A30221).
Disclosure
The authors report no conflicts of interest in this work.
References
1. JD Steinmetz, KM Seeher, N Schiess, et al. Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024;23(4):344–381. doi:10.1016/s1474-4422(24)00038-3
2. Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350(15):1495–1504. doi:10.1056/NEJMoa040583
3. Chi X, Fan X, Fu G, Liu Y, Zhang Y, Shen W. Research trends and hotspots of post-stroke cognitive impairment: a bibliometric analysis. Front Pharmacol. 2023;14:1184830. doi:10.3389/fphar.2023.1184830
4. Dec-ćwiek M, Wrona P, Homa T, Słowik J, Bodzioch A, Słowik A. Incidence and Factors Associated With Cognitive Impairment 90 Days After First Ever Ischemic Stroke. Int J Geriatr Psychiatry. 2025;40(5):e70087. doi:10.1002/gps.70087
5. Mijajlović MD, Pavlović A, Brainin M, et al. Post-stroke dementia - a comprehensive review. BMC Med. 2017;15(1):11. doi:10.1186/s12916-017-0779-7
6. Shichita T, Ito M, Yoshimura A. Post-ischemic inflammation regulates neural damage and protection. Front Cell Neurosci. 2014;8:319. doi:10.3389/fncel.2014.00319
7. Doll DN, Barr TL, Simpkins JW. Cytokines: their role in stroke and potential use as biomarkers and therapeutic targets. Aging Dis. 2014;5(5):294–306. doi:10.14336/ad.2014.0500294
8. Gao X, Su G, Chai M, et al. Research progress on mechanisms of ischemic stroke: regulatory pathways involving Microglia. Neurochem Int. 2024;172:105656. doi:10.1016/j.neuint.2023.105656
9. Zhou X, Zhu Y, Gao D, et al. Matrilin-3 supports neuroprotection in ischemic stroke by suppressing astrocyte-mediated neuroinflammation. Cell Rep. 2024;43(4):113980. doi:10.1016/j.celrep.2024.113980
10. Huang X, Hussain B, Chang J. Peripheral inflammation and blood-brain barrier disruption: effects and mechanisms. CNS Neurosci Ther. 2021;27(1):36–47. doi:10.1111/cns.13569
11. Yamaguchi A, Jitsuishi T, Hozumi T, et al. Temporal expression profiling of DAMPs-related genes revealed the biphasic post-ischemic inflammation in the experimental stroke model. Mol Brain. 2020;13(1):57. doi:10.1186/s13041-020-00598-1
12. Irisa K, Shichita T. Neural repair mechanisms after ischemic stroke. Inflamm Regen. 2025;45(1):7. doi:10.1186/s41232-025-00372-7
13. Assayag EB, Molad J, Seyman E, et al. Preventing post-stroke dementia. The MARCH Trial. Protocol and statistical analysis plan of a randomized clinical trial testing the safety and efficacy of Maraviroc in post-stroke cognitive impairment. Eur Stroke J. 2022;7(3):314–322. doi:10.1177/23969873221098857
14. Gallucci L, Sperber C, Guggisberg AG, et al. Post-stroke cognitive impairment remains highly prevalent and disabling despite state-of-the-art stroke treatment. Int J Stroke. 2024;19(8):888–897. doi:10.1177/17474930241238637
15. Ray KK, Cannon CP, Cairns R, et al. Relationship between uncontrolled risk factors and C-reactive protein levels in patients receiving standard or intensive statin therapy for acute coronary syndromes in the PROVE IT-TIMI 22 trial. J Am Coll Cardiol. 2005;46(8):1417–1424. doi:10.1016/j.jacc.2005.08.024
16. Ridker PM. How Common Is Residual Inflammatory Risk? Circ Res. 2017;120(4):617–619. doi:10.1161/circresaha.116.310527
17. Bukke SPN, Pathange BBR, Nelluri KDD, et al. Association of triglyceride glucose index with clinical outcomes in ischemic stroke: a retrospective study. BMC Neurol. 2024;24(1):371. doi:10.1186/s12883-024-03873-z
18. Salvadori E, Pasi M, Poggesi A, Chiti G, Inzitari D, Pantoni L. Predictive value of MoCA in the acute phase of stroke on the diagnosis of mid-term cognitive impairment. J Neurol. 2013;260(9):2220–2227. doi:10.1007/s00415-013-6962-7
19. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
20. JI Cleeman. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
21. Lo JW, Crawford JD, Desmond DW, et al. Profile of and risk factors for poststroke cognitive impairment in diverse ethnoregional groups. Neurology. 2019;93(24):e2257–e2271. doi:10.1212/wnl.0000000000008612
22. Douiri A, Rudd AG, Wolfe CD. Prevalence of poststroke cognitive impairment: south London Stroke Register 1995-2010. Stroke. 2013;44(1):138–145. doi:10.1161/strokeaha.112.670844
23. Zhao P, Zhang G, Wang Y, et al. Peripheral immunity is associated with cognitive impairment after acute minor ischemic stroke and transient ischemic attack. Sci Rep. 2024;14(1):16201. doi:10.1038/s41598-024-67172-w
24. Ji Y, Wang X, Wu H, et al. Incidence and risk factors of post-stroke cognitive impairment in convalescent elderly patients with first-episode acute ischemic stroke. Asian J Psychiatr. 2023;84:103583. doi:10.1016/j.ajp.2023.103583
25. Gonzales MM, Garbarino VR, Pollet E, et al. Biological aging processes underlying cognitive decline and neurodegenerative disease. J Clin Invest. 2022;132(10). doi:10.1172/jci158453
26. Springer MV, Whitney RT, Ye W, et al. Education Levels and Poststroke Cognitive Trajectories. JAMA Network Open. 2025;8(3):e252002. doi:10.1001/jamanetworkopen.2025.2002
27. Rieckmann A, Bäckman L. Implicit learning in aging: extant patterns and new directions. Neuropsychol Rev. 2009;19(4):490–503. doi:10.1007/s11065-009-9117-y
28. Patterson SL. Immune dysregulation and cognitive vulnerability in the aging brain: interactions of microglia, IL-1β, BDNF and synaptic plasticity. Neuropharmacology. 2015;96(Pt A):11–18. doi:10.1016/j.neuropharm.2014.12.020
29. Blazing MA, Giugliano RP, de Lemos JA, et al. On-treatment analysis of the Improved Reduction of Outcomes: vytorin Efficacy International Trial (IMPROVE-IT). Am Heart J. 2016;182:89–96. doi:10.1016/j.ahj.2016.09.004
30. Robinson JG, Farnier M, Krempf M, et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372(16):1489–1499. doi:10.1056/NEJMoa1501031
31. Liao J, Qiu M, Su X, et al. The residual risk of inflammation and remnant cholesterol in acute coronary syndrome patients on statin treatment undergoing percutaneous coronary intervention. Lipids Health Dis. 2024;23(1):172. doi:10.1186/s12944-024-02156-3
32. Yu Y, Lou Y, Pan Y, et al. Residual inflammatory risk predicts long-term outcomes following stenting for symptomatic intracranial atherosclerotic stenosis. Stroke Vasc Neurol. 2024;9(4):407–417. doi:10.1136/svn-2023-002421
33. Baba SS, Yarube IU. Raised high-sensitivity C-reactive protein and cognitive impairment among African stroke survivors within the first three months following stroke. J Clin Neurosci. 2021;88:191–196. doi:10.1016/j.jocn.2021.03.018
34. Candelario-Jalil E, Dijkhuizen RM, Magnus T. Neuroinflammation, Stroke, Blood-Brain Barrier Dysfunction, and Imaging Modalities. Stroke. 2022;53(5):1473–1486. doi:10.1161/strokeaha.122.036946
35. Yang J, Ran M, Li H, et al. New insight into neurological degeneration: inflammatory cytokines and blood-brain barrier. Front Mol Neurosci. 2022;15:1013933. doi:10.3389/fnmol.2022.1013933
36. Fan KQ, Huang T, Yu JS, Li YY, Jin J. The clinical features and potential mechanisms of cognitive disorders in peripheral autoimmune and inflammatory diseases. Fundam Res. 2024;4(2):226–236. doi:10.1016/j.fmre.2022.12.005
37. Belarbi K, Jopson T, Tweedie D, et al. TNF-α protein synthesis inhibitor restores neuronal function and reverses cognitive deficits induced by chronic neuroinflammation. J Neuroinflammation. 2012;9(1):23. doi:10.1186/1742-2094-9-23
38. Han R, Liu Z, Sun N, et al. BDNF Alleviates Neuroinflammation in the Hippocampus of Type 1 Diabetic Mice via Blocking the Aberrant HMGB1/RAGE/NF-κB Pathway. Aging Dis. 2019;10(3):611–625. doi:10.14336/ad.2018.0707
39. Puzzo D, Bizzoca A, Loreto C, et al. Role of F3/contactin expression profile in synaptic plasticity and memory in aged mice. Neurobiol Aging. 2015;36(4):1702–1715. doi:10.1016/j.neurobiolaging.2015.01.004
40. Fleming A, Bourdenx M, Fujimaki M, et al. The different autophagy degradation pathways and neurodegeneration. Neuron. 2022;110(6):935–966. doi:10.1016/j.neuron.2022.01.017
41. Cai Y, Zhang Y, Leng S, et al. The relationship between inflammation, impaired glymphatic system, and neurodegenerative disorders: a vicious cycle. Neurobiol Dis. 2024;192:106426. doi:10.1016/j.nbd.2024.106426
42. Kempuraj D, Dourvetakis KD, Cohen J, et al. Neurovascular unit, neuroinflammation and neurodegeneration markers in brain disorders. Front Cell Neurosci. 2024;18:1491952. doi:10.3389/fncel.2024.1491952
43. Wang M, Thomson AW, Yu F, Hazra R, Junagade A, Hu X. Regulatory T lymphocytes as a therapy for ischemic stroke. Semin Immunopathol. 2023;45(3):329–346. doi:10.1007/s00281-022-00975-z
44. Bonfanti E, Gelosa P, Fumagalli M, et al. The role of oligodendrocyte precursor cells expressing the GPR17 receptor in brain remodeling after stroke. Cell Death Dis. 2017;8(6):e2871. doi:10.1038/cddis.2017.256
45. Yuan Y, Liu H, Dai Z, He C, Qin S, Su Z. From Physiology to Pathology of Astrocytes: highlighting Their Potential as Therapeutic Targets for CNS Injury. Neurosci Bull. 2025;41(1):131–154. doi:10.1007/s12264-024-01258-3
46. Jiao Y, Liu YW, Chen WG, Liu J. Neuroregeneration and functional recovery after stroke: advancing neural stem cell therapy toward clinical application. Neural Regen Res. 2021;16(1):80–92. doi:10.4103/1673-5374.286955
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Serum Albumin and the ApoB/ApoA1 Ratio with Acute Post-Stroke Cognitive Impairment: A Propensity Score–Matched Case–Control Study
Liu D, Zhang J, Wei X, Zhang S, Yan F
International Journal of General Medicine 2026, 19:575959
Published Date: 28 April 2026