")
Back to Journals » Journal of Pain Research » Volume 16
Residents of Mountainous Areas Have a Higher Low Back Pain Prevalence Than Flat Areas of Chongqing, China: A Cross-Sectional Study
Authors Ren X, Bai D, Zhang Y, Lin H, Zhang S, Li D, Wei H, Yue S
Received 17 December 2022
Accepted for publication 14 March 2023
Published 8 April 2023 Volume 2023:16 Pages 1169—1183
DOI https://doi.org/10.2147/JPR.S401894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Alaa Abd-Elsayed
Xiaomin Ren,1 Dingqun Bai,2 Yuan Zhang,3 Haidan Lin,2 Shu Zhang,2 Danyang Li,1 Hui Wei,1 Shouwei Yue1
1Rehabilitation Center, Qilu Hospital of Shandong University, Jinan, People’s Republic of China; 2Department of Physical Medicine & Rehabilitation, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Clinical Epidemiology Unit, Qilu Hospital of Shandong University, Jinan, People’s Republic of China
Correspondence: Shouwei Yue; Hui Wei, Rehabilitation Center, Qilu Hospital of Shandong University, Jinan, 250012, People’s Republic of China, Tel +18560086655 ; +18560083563, Fax +531 82166115, Email [email protected]; [email protected]
Background and Purpose: Epidemiological studies on low back pain in residents living in mountainous areas are scarce. The study was aimed at investigating the prevalence and associated factors of low back pain in Chongqing, relatively impoverished mountainous areas of China.
Materials and Methods: This was a cross-sectional study conducted at selected community or village health service centers in Chongqing over a 2-month period (May 2021 to June 2021), which included adults of Chongqing aged > 18 years with or without low back pain (N=1820) chosen by stratified, cluster-sampling. Associated factors of low back pain including sociodemographic characteristics, lifestyle, and occupational features were collected, along with medical history, Oswestry Disability Questionnaire (ODI), and Numerical Rating Scale (NRS) of patients with low back pain, and carried out for at least 20 minutes per respondent. Univariate and multivariate logistic regression models were utilized for statistical analysis.
Results: Overall, 30.5% of 1704 respondents presented with low back pain, with 26.3% living in flat areas and 35.6% in mountainous areas. The associated factors of low back pain were mountainous area residence (OR 1.4, 95% CI 1.1– 1.8), advanced age (OR 1.8, 95% CI 1.3– 2.5 for those aged 45– 59 years, OR 2.3, 95% CI 1.6– 3.4 for those aged 60– 74 years, and OR 2.1, 95% CI 1.2– 3.6 for those aged ≥ 75 years), married or remarried (OR 1.9, 95% CI 1.1– 3.2), divorced or widowed (OR 2.7, 95% CI 14– 5.4), moderate labor intensity (OR 1.4, 95% CI 1.1– 1.8), frequent stoop (OR 1.6, 95% CI 1.1– 2.4), and depressed mood (OR 1.6, 95% CI 1.2– 2.1). Residents in the mountainous areas had a higher score on Oswestry Disability Questionnaire (8.3 [SD 6.3] vs 6.2 [SD 4.3]) than those in flat areas.
Conclusion: Mountainous areas in Chongqing had higher prevalence of low back pain as 35.6%, compared with 26.3% in flat areas, with more severe dysfunction in low back pain patients. Multifactorial analysis found that the factors associated with low back pain in Chongqing residents included mountain residence, labor intensity, stoop, psychological factors and frequency of exercise.
Keywords: low back pain, prevalence, associated factors, China
Introduction
The leading cause of disability worldwide is low back pain (LBP).1 Pain can cause disability, which in turn can worsen pain, potentially leading to absence from work, depression, anxiety, and degressive quality of life.2,3 In recent decades, social support systems and healthcare providers have been negatively affected by the rapid increase in LBP disabilities, in low- and middle-income countries, including China.4 In 2017, musculoskeletal disorders were one of three main reasons for years lived with disability in China,5 and LBP is the second most burdensome musculoskeletal disorder after neck pain.6
Epidemiological studies on LBP are fewer in Asian countries than in Western countries.3 The maximum point-prevalence of LBP is 32.9% in high-income, 25.4% in middle-income, and 16.7% in low-income countries.3 China ranked second in the age-standardized one-year prevalence of LBP when compared with 19 member countries of Group 20, excluding the European Union, between 1990 and 2017.6 There are many factors related to LBP, including smoking, sex, age, marital status, occupation, and psychological factors.6,7
To our knowledge, there are few epidemiological investigations regarding LBP in people living in mountainous areas. Some studies pointed out that the potential risk of chronic LBP was increased among miners at high altitudes due to the decreased muscle endurance and fatigue caused by hypoxia.8 A study also showed that rural mountain residents walked up and down steep slopes on a daily basis, which increased the mechanical load on their bodies and may lead to musculoskeletal disorders such as knee and low back pain.9 Therefore, this study hypothesized that the prevalence of LBP and associated factors in mountainous areas would be different from those in flat areas due to their various topographical characteristics, labor characteristics, and residents’ lifestyles. In addition, the geographical constraints of mountainous areas lead to limited transportation, relative economic backwardness, and scarce medical resources. It has been reported that low- or middle-income areas are inclined to apply expensive, ineffective, and potentially harmful procedures and interventions to treat LBP, which invariably increased the cost of LBP treatment.10 LBP has driven people already living in low socioeconomic conditions into more severe poverty and more disability.11 A vicious cycle was created between mountains, low back pain, and poverty.
Public health management faces great challenges in mountainous areas in China because of economic and regional constraints, aggravating poverty. The Chinese government has created the Healthy China 2030 plan, a health policy treating population health as the primary goal of economic development and political reform.5 A targeted poverty alleviation policy was implemented in China to eliminate all forms of poverty.12 We aimed to conduct this cross-sectional survey to respond to the national policy and enhance awareness of LBP in mountainous areas. Chongqing, China, was selected due to its undeveloped economic situation and the richness of special geomorphic features. It comprises three geomorphic features: the west and south have low and medium mountains, 30.24% in total area; the east and north have low hills, 38.81% in total area, and the central basin is a flat dam area, 30.94% in total area.
Therefore, we conducted this survey according to different terrain zones in Chongqing to assess the following questions for motivating clinicians to learn the epidemiological information of LBP in mountainous areas, assisting mountain residents to select healthier lifestyles, and prompting researchers to identify potential risk factors of LBP in mountainous areas, which will guide the direction of the next research:
- Is there a higher prevalence of LBP in mountainous areas than in flat areas of Chongqing?
- Are there specific associated factors for LBP in Chongqing?
- Do people with LBP living in mountainous areas have more severe pain and dysfunction than those living in flat areas in Chongqing?
Materials and Methods
Design
We conducted this stratified, cluster-sampling cross-sectional survey in Chongqing from May 2021 to June 2021. All investigators were medical workers trained for questioning technique and information filling of questionnaires homogeneously. Stratified sampling was divided into two layers considering terrain characteristics. The first layer was low and medium mountainous and low hilly areas (collectively referred to as mountainous areas), and the second layer was flat areas. Two communities were selected from the flat areas, with an average of 400–500 people in each. Five villages were selected from the mountainous areas, with an average of 100–300 people in each.
The investigators filled out paper questionnaires by asking participants questions. The questionnaire comprised four parts. The first part was the associated factors questionnaire (Appendix 1), including sociodemographic characteristics, lifestyle, and occupational features. Parts two to four were medical history (Appendix 2), Oswestry Disability Questionnaire (ODI) (Appendix 3), and Numerical Rating Scale (NRS) (Appendix 4) of patients with LBP, respectively. (Appendix 1–4 are presented in the Appendix). All participants needed to answer the questions of the first part, and only those with symptoms of LBP needed to complete the remaining parts of the questionnaire. According to the symptomatology definition, we diagnosed LBP as a type of pain localized between the lower edge of the costal bone and the subgluteal fold commonly accompanied by radiating pain in one or both limbs.
Participants
The respondents were aged 18 years or older, had no hearing or language impairment, no cognitive impairment, and lived in the surveyed area for ≥5 years. Pregnant or lactating women and participants with lumbar tumors and other severe underlying diseases were excluded. The respondents were enrolled by the local public health authorities in Chongqing during the regularly health surveillance.
Data Extraction
The survey data were inputed into EpiDate v.3.1 (The EpiData Association, Odense, Denmark) by two researchers. Disputed data and absent items were selected by comparing the results of the two-person input and checked through the original paper questionnaire. And the absent data were corrected through telephone inquiries. If participants could not be contacted or relevant data were not available, the questionnaire would be excluded from the study results.
Data Analysis
A randomized population study by Tsang et al13 found that the prevalence of LBP, among adults in Chongqing, was 17.6%. According to the formula for estimating the population rate  (deff, design effect; P, population rate; and δ, allowable error), the number of participants needed for the study was 1422 in the case where deff was 2.0 and the absolute error was 2.0%.
(deff, design effect; P, population rate; and δ, allowable error), the number of participants needed for the study was 1422 in the case where deff was 2.0 and the absolute error was 2.0%.
IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp was used for statistical analysis. First, the prevalence of LBP in Chongqing was calculated. Second, relationships between demographics and LBP status (LBP vs no LBP) were analyzed. Categorical variables, expressed as frequencies and percentages, were analyzed univariately using chi-square tests, Fisher’s exact test, and binomial logistic regression analysis. Variables with P values <0.1 were included in the multifactor binomial logistic regression analysis. The odds ratio (OR) with ±95% confidence interval (CI) was estimated, indicating associated variables with the probability of the LBP. Third, the Mann–Whitney U-test was used to evaluate the effect of terrain on LBP and degree of pain; the median (P25, P75) was used to represent measurement data that did not follow the normal distribution. In all the above statistical analyses, statistical significance was set as P values <0.05.
Results
Flow of Participants
The study recruited 1820 residents of Chongqing. Overall, 1738 residents completed the questionnaires, excluding 57 who refused to participate and 25 who did not meet the inclusion and exclusion criteria. After excluding 34 failed questionnaires, we included 1704 residents’ questionnaires in the statistical analysis. Among them, 935 were from flat areas and 769 from mountainous areas, 520 had LBP, and 1184 had no LBP (Figure 1).
 |
Figure 1 Process of epidemiological investigation of low back pain in Chongqing, China. Flat areas are abbreviated as “flat” and mountainous areas are abbreviated as “coteau.”. |
Demographic Characteristics
Most respondents were female (n=1084, 63.6%), aged 45–59 years (n=689, 40.4%), and of Han nationality (n=832, 48.8%). The respondents’ characteristics in flat and mountainous areas were similar to all study participants, except for exercising and entertainment. Most respondents in flat areas exercised occasionally (n=434, 46.4%), and most respondents in mountainous areas liked walking or fitness (n=299, 38.9%). Although most respondents in mountainous areas did not climb mountains often, significantly more respondents in mountainous areas (n=357, 46.4%) climbed mountains more often than those living in flat areas (n=123, 13.2%). Respondents living in mountainous areas also climbed more times and longer periods per week than those living in flat areas. For example, the number of respondents living in mountainous areas who climbed mountains more than 10 times (n=100, 13.0%) and climbed mountains more than 5 hours (n=184, 23.9%) per week were far more than those living in flat areas who climbed mountains more than 10 times (n=9, 1.0%) and climbed mountains more than 5 hours (n=32, 3.4%) per week (Table 1).
 |
Table 1 Demographic Characteristics of the Respondents in Chongqing, China |
Is There a Higher Prevalence of LBP in Mountainous Areas Than in Flat Areas of Chongqing?
Among the participants, 520 (30.5%) experienced LBP (Table 1). In total, 246 interviewees (26.3%) in flat areas and 274 (35.6%) in mountainous areas had LBP. The prevalence of LBP tended to increase with age (21.1% vs 31.5% vs 37.8% vs 36.1%), climbing times (28.0% vs 31.3% vs 37.8% vs 46.8%), climbing frequency (28.0% vs 32.4% vs 35.8% vs 41.2%), the labor intensity (26.2% vs 33.0% vs 37.7%), frequency of sadness (27.8% vs 36.6% vs 43.9%) and tended to decrease with exercise frequency (36.6% vs 29.2% vs 28.0%) (Table 2). In flat areas, prevalence of LBP was lower among people who reported increased exercise frequency (33.9% vs 28.3% vs 19.3%). It was higher among people who reported enhanced labor intensity (23.8% vs 27.1% vs 44.1%), and increased frequency of depressed mood (23.5% vs 31.1% vs 61.1%) (Table 3). People with a higher prevalence of LBP in mountainous areas were mainly concentrated in those aged ≥60 years (45.4%, 40.0%), divorced or widowed (45.5%), farmers (38.5%), with moderate labor intensity (41.4%), frequent bending (54.9%) and so on. It is noteworthy that the prevalence of LBP is higher in those who frequently climbed (40.9%), and it increased with increasing frequency of climbing (31.1% vs 35.8% vs 40.7% vs 47.0%) and duration of climbing (31.1% vs 38.8% vs 40.8% vs 41.8%) in mountainous areas. (Table 4).
 |
Table 2 Univariate Analysis of the Associations Between Demographics and Low Back Pain Status in Chongqing |
 |
Table 3 Univariate Analysis of the Associations Between Demographics and Low Back Pain Status in Flat Areas of Chongqing |
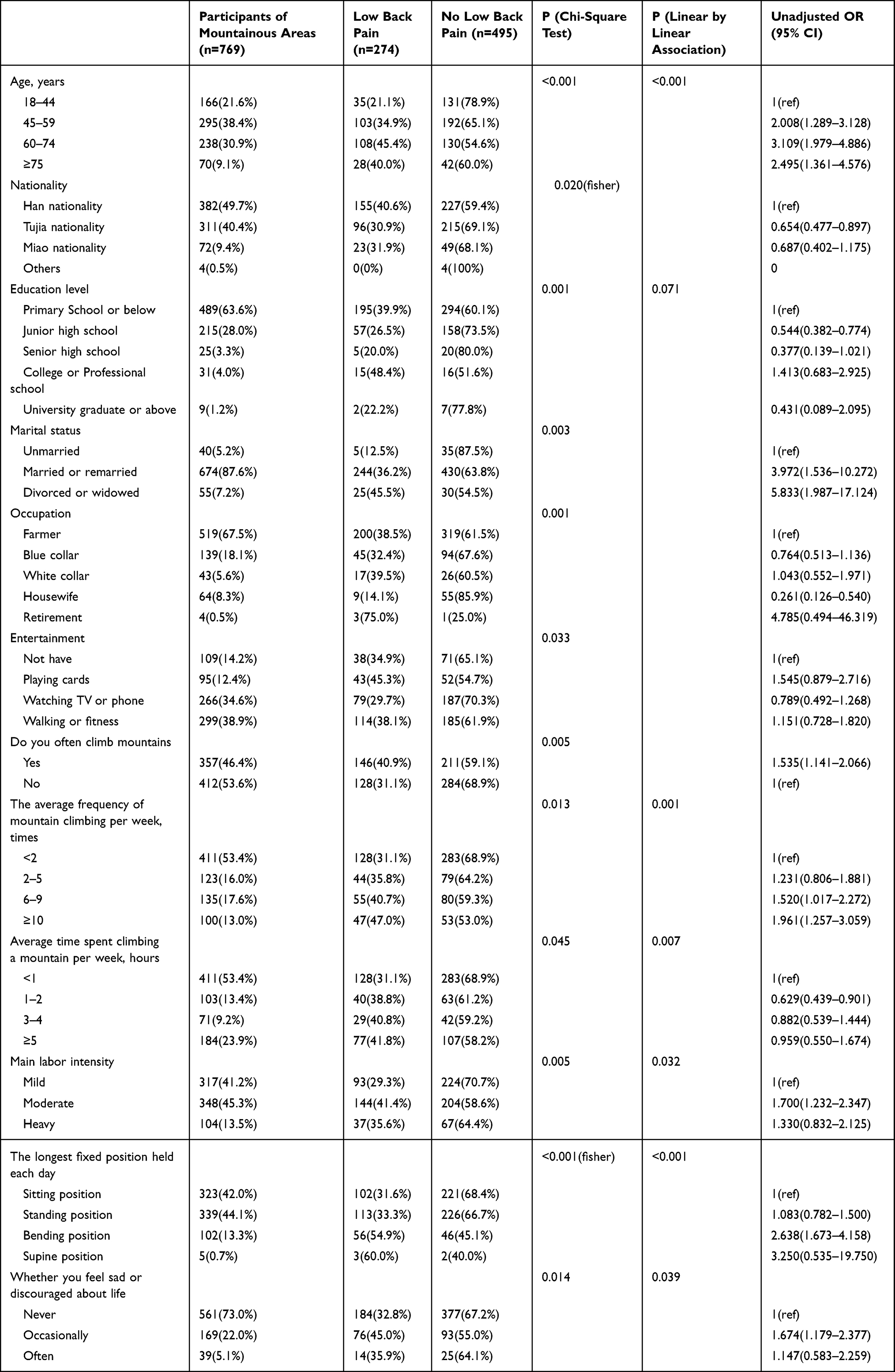 |
Table 4 Univariate Analysis of the Associations Between Demographics and Low Back Pain Status in Mountainous Areas of Chongqing |
Are There Specific Associated Factors for LBP in Chongqing?
We obtained modifiable associated factors by multifactorial logistic regression analysis, which were mountainous area residence (OR 1.4, 95% CI 1.1–1.8), advanced age (OR 1.8, 95% CI 1.3–2.5; OR 2.3, 95% CI 1.6–3.4; OR 2.1, 95% CI 1.2–3.6), married or remarried (OR 1.9, 95% CI 1.1–3.2), divorced or widowed (OR 2.7, 95% CI 1.4–5.4), less exercise ([OR 0.7, 95% CI 0.5–0.9] for often exercise), moderate labor intensity (OR 1.4, 95% CI 1.1–1.8), frequent stoop (OR 1.6, 95% CI 1.1–2.4), depressed mood (OR 1.6, 95% CI 1.2–2.1), and high school education as a potential protective factor for LBP (OR 0.563, 95% CI 0.319–0.996) (Figure 2). For flatland residents, age 45–74 years (OR 2.0, 95% CI 1.3–3.1; OR 2.5, 95% CI 1.5–4.3), university or higher education (OR 2.6, 95% CI 1.2–5.3), and occasional or frequent sadness (OR 1.5, 95% CI 1.1–2.1; OR 5.8, 95% CI 2.1–16.0) were associated factors for LBP, while regular exercise (OR 0.4, 95% CI 0.3–0.7) was an associated factor in the reverse for LBP (Figure 3). For mountainous areas, residents aged 60–74 (OR 2.3, 95% CI 1.3–4.2), 75 years and older (OR 2.3, 95% CI 1.1–4.7), married or remarried (OR 3.4, 95% CI 1.3–9.1), divorced or widowed (OR 4.1, 95% CI 1.3–12.6), fond of playing cards (OR 2.7, 95% CI 1.4–5.3), frequent bending (OR 2.0, 95% CI 1.1–3.6), and occasionally feeling sad (OR 1.7, 95% CI 1.1–2.4) were associated factors for LBP, while Tujia nationality (OR 0.6, 95% CI 0.5–0.9) and being a housewife (OR 0.4, 95% CI 0.2–0.97) were associated factors in the reverse for LBP (Figure 4).
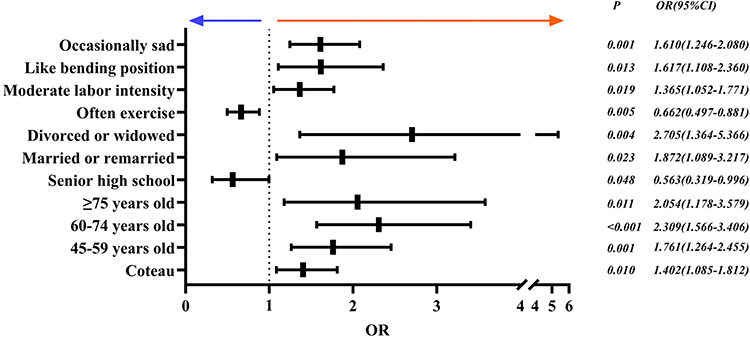 |
Figure 2 Multivariate analysis of the associations between demographics and low back pain status in Chongqing, China. P values <0.05 were statistically significant. Bounded by OR=1 (indicated as a vertical dashed line in the figure), the potential protective factors for LBP are on the left and the potential risk factors for LBP are on the right. Flat areas are abbreviated as “flat” and mountainous areas are abbreviated as “coteau.” Confounders included occupation, smoking or not, drinking or not, climb mountains or not, the frequency of mountain climbing, and the time to be spent climbing mountains. |
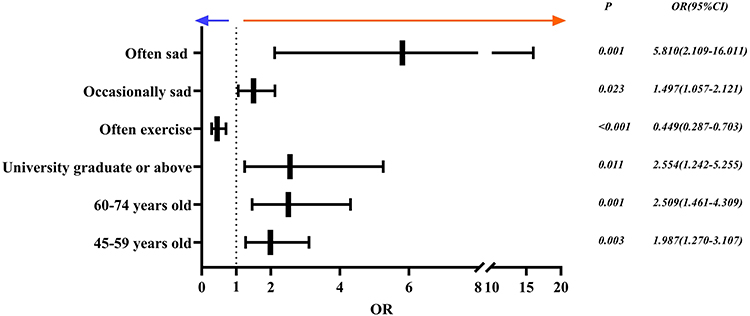 |
Figure 3 Multivariate analysis of the associations between demographics and low back pain status in flat areas of Chongqing, China. Confounders included marital status, and main labor intensity. |
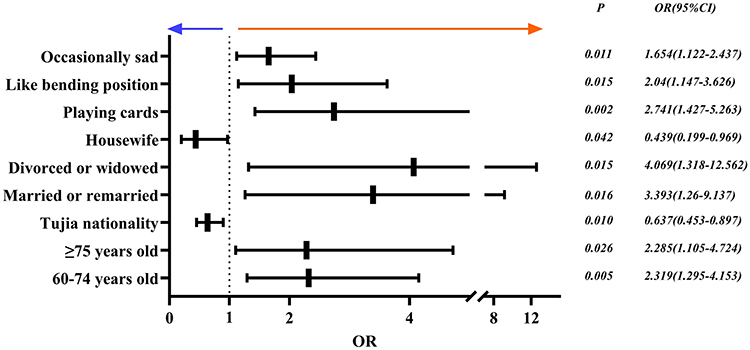 |
Figure 4 Multivariate analysis of the associations between demographics and low back pain status in mountainous areas of Chongqing, China. Confounders included education level, climb mountains or not, the frequency of mountain climbing, the time to be spent climbing mountains, and main labor intensity. |
Do Patients with LBP Residing in Mountainous Areas Manifest More Severe Pain and Dysfunction Than Those in Flat Areas in Chongqing?
Finally, among interviewees with LBP, the ODI score of mountain areas was higher than that of flat areas (3.0–8.0 vs 3.8–11.0). Residents of mountainous areas showed greater dysfunction and degree of pain compared with residents in flat areas (P=0.012; P<0.001) (Table 5).
 |
Table 5 Effect of Terrain on Low Back Pain Dysfunction and Degree of Pain |
Discussion
This stratified, cluster-sampling survey of over 1700 residents in Chongqing showed that the LBP prevalence is higher in Chongqing than in middle-income countries and low-income countries,3 especially in the mountainous areas where LBP prevalence was 35.6%. Residing in mountainous areas, older age, being married and remarried, divorced and widowed, less exercise, moderate labor intensity, frequent stoop, and depressed mood were associated factors for LBP. In addition, the associations between different residential areas and LBP may be caused by the different characteristics of the populations. The population of flat areas highly associated with LBP was primarily middle-aged and elderly, and highly educated people, while LBP in mountainous areas was concentrated in older people, and frequently bending due to occupational characteristics (for example, farmers). Finally, we also found that although there is no difference in the degree of pain between LBP patients in mountainous and those in flat areas, LBP patients in mountainous areas suffer more serious dysfunction.
To our knowledge, this is the first epidemiological survey conducted in China on a large population comparing LBP in flat areas and mountainous areas. Liu C et al14 found that the prevalence of LBP in mountainous areas in Taiwan was 56.4%, but it was specific to the elderly. Wu et al15 reported the age-adjusted point prevalence of LBP in China while lacking provincially specific studies. Thus, Chongqing was selected to conduct this survey with unique topographical characteristics while controlling for other confounding factors (eg, climate). In the next sections, we will discuss in detail the factors associated with LBP as well as the pain level and dysfunction of LBP patients in Chongqing.
The large confidence intervals found for some variables indicated that those associations may not be so accurate. In the present study, the variables age and marital status had larger confidence intervals in the results of the multifactorial analysis, thus the relationship between these two variables and LBP needs to be further clarified. It has been reported that the prevalence of LBP was higher during work years, and then decreased after retirement.16 A study of middle-aged and elderly Japanese women noted a significant increase in the prevalence of LBP after the age of 70, which may be related to the lifelong agricultural work characteristics of the female population in the region.17 The average retirement age of the Chinese is 60 years.18 The present study found a definite correlation between residents aged 40–59 years and LBP, and the association between residents 60 or older and LBP was relevant, but the accuracy of the correlation was diminished. This may be explained by the fact that a large proportion of the population in Chongqing were farmers (Table 1) who would have been devoted to agricultural work throughout their lives, leading to a relatively increased prevalence of LBP in people over 60 years old and then strengthening the correlation between people over 60 years old and LBP. Moreover, this present study showed an association between marital status and LBP with wide ranges of confidence intervals. Contrary to the studies of Lee et al19 and Takahashi et al17 they did not reveal an association between LBP and marital status. The association between LBP and marital status needs to be specified more clearly.
The four variables “moderate labor intensity, frequent stoop, depressed mood, and frequent exercise” in the multivariate analysis of the present study had relatively narrow confidence intervals for their correlation with LBP, which indicated that the relationship between them and LBP was more accurate.
First of all, moderate labor intensity was an associated factor for LBP in Chongqing residents. Yolande et al20 reported that current exposure to a weight-bearing environment would increase the risk of chronic LBP after 5 years. Takahashi et al17 found that the prevalence of LBP was significantly greater in the manual labor group than in the unmanual labor group. A meta-analysis concluded that lifting heavy weights may have profound effects on the musculoskeletal health of workers, with the intensity and frequency of lifting significantly predicting the onset of LBP.21 In the present study, the prevalence of LBP was higher among residents engaged in moderate-intensity labor such as the intermittent lifting of moderately heavy loads, weeding and hoeing of fields (Table 2), which was consistent with the above studies.
As a second point, the present study found that frequent stoop was significantly associated with an increased prevalence of LBP. Similarly, a Korean study of factors associated with LBP in farmers revealed that occupation-related biomechanical factors were strongly associated with LBP, and repetitive forward bending, twisting, and backwards tilting of the low back were potential risk factors for LBP among the population.19 And Żywień et al22 found that LBP in adults was associated with spinal curvatures. Some studies also indicated that anterior lumbar flexion and twisting were correlated with increased pressure on the intervertebral discs, and repetitive motions caused degeneration and herniation of the discs.23,24 Thus, frequent bending was a potential risk factor that cannot be ignored by Chongqing residents.
Depressed mood was another significant independent predictor of LBP in the present study. Chronic pain and mental disorders are independent of each other and often coexist in individuals as comorbidities.25 A study has demonstrated that depression is a strong, independent risk factor for LBP.26 Furthermore, depressed Chinese people tend toward somatization.27 Significant effects of LBP on sleep, depression/psychological problems and social life have also been observed.28 Patients with chronic LBP had a relatively high prevalence of anxiety symptoms.29 Consequently, the causal relationship between LBP and psychological factors needs to be confirmed by additional research.
Finally, the prevalence of LBP among residents who exercise regularly was found to be significantly below the reference for the present study (adjusted OR of 0.662), which was in accordance with the findings of Masiero S, Yiengprugsawan V, and Hashimoto et al30–32 However, the effectiveness of physical activity on LBP was controversial. Some studies have highlighted that the relationship between physical activity and LBP was a U-shaped curve,33,34 which indicated that inadequate or excessive exercise can predispose to the development of LBP. Sundell CG et al35 reported that increased physical activity was associated with the risk of developing LBP, the duration of LBP, and disability due to LBP.
There was no difference in the degree of pain between patients with LBP in mountainous areas and flat areas in Chongqing, but the degree of dysfunction was significantly worse in patients with LBP in mountainous areas than in flat areas. The present study revealed a statistically significant difference in the pain level of patients with LBP in the two regions (mean difference, 0.3; P = 0.012). However, according to the minimum clinically important difference (MCID) of the NRS recommended by the international consensus that MCID of NRS was 2,36 there was no clinically meaningful difference in pain levels between patients with LBP in the two regions. Hartvigsen et al4 demonstrated that absence of management of pain can exacerbate functional impairment in patients with LBP. The degree of dysfunction of LBP patients in mountainous areas was more severe with no difference in pain level, which may be caused by the inadequate medical resources and popularization of LBP rehabilitation treatment in mountainous areas due to geographical limitations, resulting in the insufficient treatment of LBP, and the inferior degree of completion of ODI-related functions such as self-care ability, lifting, walking and sitting of LBP patients. These indicate that we may reduce the impact of LBP on the function in mountainous areas by enhancing “pain management” guidance for LBP patients.
Study Limitations
Owing to the increase in migrant workers, the female population included in this study was greater than the male population, which weakened the representativeness of the sample to some extent. Besides, there was a lack of scale assessment of the mood factor variable, which may have increased the influence of participants’ subjective factors on this variable. In future studies, scales assessing mood factors should be included. And in addition to assessing the effect of physical factors such as weight and height on LBP, other physical factors such as spinal curvatures and the pressure pain threshold on LBP can still be assessed.22 Also, Constraints imposed by the time point of the survey have possibly classified a proportion of patients in remission from chronic LBP as LBP-free populations, resulting in a relatively lower prevalence of LBP. Lastly, the present study design failed to clarify the causal relationship between LBP and demographic characteristics of Chongqing residents, and additional cohort studies would be needed to identify risk factors for LBP.
Conclusion
The prevalence of LBP in Chongqing residents has reached 30.5%, in which, the prevalence of LBP in mountainous areas was much higher than that in flat areas. The associations between LBP and labor intensity, frequent stoop, depressed mood, and frequent exercise were well defined in Chongqing residents, however, the associations between LBP and age and marital status remain to be determined more clearly. Lastly, an individual analysis of LBP patients revealed that although there was no difference in pain levels between the mountainous and flat LBP patients, the degree of dysfunction was more severe in the mountainous LBP patients.
Abbreviations
LBP, Low back pain; ODI, Oswestry Disability Questionnaire; NRS, Numerical Rating Scale; MCID, Minimum Clinically Important Difference.
Ethics Approval
The Qilu Hospital of Shandong University Scientific Research Ethics Committee (KYLL-202111-060) approved this study. And the study complied with the Declaration of Helsinki. All participants gave written informed consent before data collection began.
Acknowledgments
We thank all respondents of the survey for their active cooperation. We are grateful for the support and assistance of Xiushan County Traditional Chinese Medicine Hospital, township government agencies, and township health centers of Xiushan County in this survey process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors meet the authorship criteria and have read and agreed to the manuscript.
Funding
This work was supported by the Department of Science & Technology of Shandong Province [grant numbers 2020LYXZ024]; the Shandong University [grant numbers 2020SDUCRCB004]; and the National Natural Science Foundation of China [grant numbers 81972155].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maher C, Ferreira G. Time to reconsider what global burden of disease studies really tell us about low back pain. Ann Rheum Dis. 2022;81(3):306–308. doi:10.1136/annrheumdis-2021-221173
2. Dawson AP, Schluter PJ, Hodges PW, Stewart S, Turner C. Fear of movement, passive coping, manual handling, and severe or radiating pain increase the likelihood of sick leave due to low back pain. Pain. 2011;152(7):1517–1524. doi:10.1016/j.pain.2011.02.041
3. Vlaeyen JWS, Maher CG, Wiech K, et al. Low back pain. Nat Rev Dis Primers. 2018;4(1):52. doi:10.1038/s41572-018-0052-1
4. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
5. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
6. Wu D, Wong P, Guo C, Tam LS, Gu J. Pattern and trend of five major musculoskeletal disorders in China from 1990 to 2017: findings from the Global Burden of Disease Study 2017. BMC Med. 2021;19(1):34. doi:10.1186/s12916-021-01905-w
7. Ye S, Jing Q, Wei C, Lu J. Risk factors of non-specific neck pain and low back pain in computer-using office workers in China: a cross-sectional study. BMJ Open. 2017;7(4):e014914. doi:10.1136/bmjopen-2016-014914
8. Vearrier D, Greenberg MI. Occupational health of miners at altitude: adverse health effects, toxic exposures, pre-placement screening, acclimatization, and worker surveillance. Clin Toxicol. 2011;49(7):629–640. doi:10.3109/15563650.2011.607169
9. Abe T, Okuyama K, Hamano T, et al. Assessing the Impact of a Hilly Environment on Depressive Symptoms among Community-Dwelling Older Adults in Japan: a Cross-Sectional Study. Int J Environ Res Public Health. 2021;18(9):4520. doi:10.3390/ijerph18094520
10. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383. doi:10.1016/S0140-6736(18)30489-6
11. Sharma S, McAuley JH. Low Back Pain in Low- and Middle-Income Countries, Part 1: the Problem. J Orthop Sports Phys Ther. 2022;52(5):233–235. doi:10.2519/jospt.2022.11145
12. Zhu M, Shuai C. Probe into the targeted poverty mitigation policy in China based on causal inference: evidence from Chongqing in the Three Gorges Reservoir region. PLoS One. 2021;16(1):e0244928. doi:10.1371/journal.pone.0244928
13. Jackson T, Chen H, Iezzi T, Yee M, Chen F. Prevalence and correlates of chronic pain in a random population study of adults in Chongqing, China. Clin J Pain. 2014;30(4):346–352. doi:10.1097/AJP.0b013e31829ea1e3
14. Liu CT, Wu BY, Chen YH, Tsai MY. Pain Experiences and Coping Strategies in Rural Older Adults With Chronic Musculoskeletal Pain in Mountainous Areas of Taiwan. Pain Manag Nurs. 2022;23(4):524–531. doi:10.1016/j.pmn.2021.08.010
15. Wu A, Dong W, Liu S, et al. The prevalence and years lived with disability caused by low back pain in China, 1990 to 2016: findings from the global burden of disease study 2016. Pain. 2019;160(1):237–245. doi:10.1097/j.pain.0000000000001396
16. Dionne CE, Dunn KM, Croft PR. Does back pain prevalence really decrease with increasing age? A systematic review. Age Ageing. 2006;35(3):229–234. doi:10.1093/ageing/afj055
17. Takahashi A, Kitamura K, Watanabe Y, et al. Epidemiological profiles of chronic low back and knee pain in middle-aged and elderly Japanese from the Murakami cohort. J Pain Res. 2018;11:3161–3169. doi:10.2147/JPR.S184746
18. Chen X, Giles J, Yao Y, et al. The path to healthy ageing in China: a Peking University-Lancet Commission. Lancet. 2022;400(10367):1967–2006. doi:10.1016/S0140-6736(22)01546-X
19. Lee HJ, Oh JH, Yoo JR, et al. Prevalence of Low Back Pain and Associated Risk Factors among Farmers in Jeju. Saf Health Work. 2021;12(4):432–438. doi:10.1016/j.shaw.2021.06.003
20. Esquirol Y, Niezborala M, Visentin M, Leguevel A, Gonzalez I, Marquié JC. Contribution of occupational factors to the incidence and persistence of chronic low back pain among workers: results from the longitudinal VISAT study. Occup Environ Med. 2017;74(4):243–251. doi:10.1136/oemed-2015-103443
21. Coenen P, Gouttebarge V, van der Burght AS, et al. The effect of lifting during work on low back pain: a health impact assessment based on a meta-analysis. Occup Environ Med. 2014;71(12):871–877. doi:10.1136/oemed-2014-102346
22. Żywień U, Barczyk-Pawelec K, Sipko T. Associated Risk Factors with Low Back Pain in White-Collar Workers-A Cross-Sectional Study. J Clin Med. 2022;11(5):1275. doi:10.3390/jcm11051275
23. Nachemson AL. Disc pressure measurements. Spine. 1981;6(1):93–97. doi:10.1097/00007632-198101000-00020
24. Sato K, Kikuchi S, Yonezawa T. In vivo intradiscal pressure measurement in healthy individuals and in patients with ongoing back problems. Spine. 1999;24(23):2468–2474. doi:10.1097/00007632-199912010-00008
25. Tsang A, Von Korff M, Lee S, et al. Common chronic pain conditions in developed and developing countries: gender and age differences and comorbidity with depression-anxiety disorders. J Pain. 2008;9(10):883–891. doi:10.1016/j.jpain.2008.05.005
26. Carroll LJ, Cassidy JD, Côté P. Depression as a risk factor for onset of an episode of troublesome neck and low back pain. Pain. 2004;107(1–2):134–139. doi:10.1016/j.pain.2003.10.009
27. Lee S, Tsang A. A population-based study of depression and three kinds of frequent pain conditions and depression in Hong Kong. Pain Med. 2009;10(1):155–163. doi:10.1111/j.1526-4637.2008.00541.x
28. Bansal D, Asrar MM, Ghai B, Pushpendra D. Prevalence and Impact of Low Back Pain in a Community-Based Population in Northern India. Pain Physician. 2020;23(4):E389–e398. doi:10.36076/ppj.2020/23/E389
29. Hu Y, Yang Z, Li Y, Xu Y, Zhou X, Guo N. Anxiety Symptoms and Associated Factors Among Chronic Low Back Pain Patients in China: a Cross-Sectional Study. Front Public Health. 2022;10:878865. doi:10.3389/fpubh.2022.878865
30. Masiero S, Sarto F, Cattelan M, et al. Lifetime Prevalence of Nonspecific Low Back Pain in Adolescents: a Cross-sectional Epidemiologic Survey. Am J Phys Med Rehabil. 2021;100(12):1170–1175. doi:10.1097/PHM.0000000000001720
31. Yiengprugsawan V, Hoy D, Buchbinder R, Bain C, Seubsman SA, Sleigh AC. Low back pain and limitations of daily living in Asia: longitudinal findings in the Thai cohort study. BMC Musculoskelet Disord. 2017;18(1):19. doi:10.1186/s12891-016-1380-5
32. Hashimoto Y, Matsudaira K, Sawada SS, et al. Objectively Measured Physical Activity and Low Back Pain in Japanese Men. J Phys Act Health. 2018;15(6):417–422. doi:10.1123/jpah.2017-0085
33. Heneweer H, Vanhees L, Picavet HS. Physical activity and low back pain: a U-shaped relation? Pain. 2009;143(1–2):21–25. doi:10.1016/j.pain.2008.12.033
34. Bendix T. Physical exercises and low back pain. Scand J Med Sci Sports. 2006;16(4):217–218. doi:10.1111/j.1600-0838.2006.00576.x
35. Sundell CG, Bergström E, Larsén K. Low back pain and associated disability in Swedish adolescents. Scand J Med Sci Sports. 2019;29(3):393–399. doi:10.1111/sms.13335
36. Ostelo RW, Deyo RA, Stratford P, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–94. doi:10.1097/BRS.0b013e31815e3a10
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.