Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 18
Research Trends in HIV-Associated Nephropathy (HIVAN) from 2015 to 2025: A Bibliometric Analysis Using CiteSpace
Received 30 January 2026
Accepted for publication 22 April 2026
Published 5 May 2026 Volume 2026:18 600050
DOI https://doi.org/10.2147/HIV.S600050
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Shaowei Huang,1 Xiaofeng Wei2
1Department of Critical Care Medicine, Yunnan Provincial Hospital of Infectious Disease/Yunnan AIDS Care Center/Yunnan Mental Health Center, Kunming, Yunnan, 650301, People’s Republic of China; 2Central Sterile Supply Department, Kunming Maternal and Child Health Hospital, Kunming, Yunnan, 650031, People’s Republic of China
Correspondence: Shaowei Huang, Email [email protected]
Background: In recent years, HIV-associated nephropathy (HIVAN) has significantly impacted the compliance, quality of life, and treatment outcomes for patients with AIDS. This study employs CiteSpace bibliometric analysis to predict emerging topics and research trends, thereby offering clear scientific navigation and strategic recommendations for HIVAN research.
Methods: We retrieved publications related to HIVAN from the Web of Science Core Collection covering the period from 2015 to 2025. Utilizing CiteSpace, we analyzed the co-occurrence network, clustering,and timeline of research trends in this field to illustrate the knowledge evolution surrounding HIVAN.
Results: A total of 1,470 publications were included from 2015 to 2025. The United States maintained its dominant position in medical research, while countries such as the United Kingdom, South Africa, France, and China emerged as key contributors in the field. Prominent institutions, including the University of California system, Johns Hopkins University, and University of the London, were central to HIVAN research. Scholars such as Estrella, Michelle M. Shlipak, Michael G. and Kopp, Jeffrey B exhibited substantial academic output and garnered considerable citation attention. Leading journals, including “Clinical Infectious Diseases”, “PLOS ONE” and “AIDS” served as premier venues for review articles, providing essential platforms and establishing foundations for ongoing research. The research activity and academic impact of HIVAN within the sub-discipline of nephrology currently represent prominent areas of inquiry.
Conclusion: This study examined the knowledge network structure of HIVAN from 2015 to 2025 examined bibliometric analysis. Future research should focus on enhancing international collaboration, particularly in resource limited regions, to investigate various intervention strategies aimed at improving compliance, quality of life, and treatment outcomes for HIVAN patients.
Keywords: HIVAN, PLWH, CKD, ART, CiteSpace, Bibliometrics, Research trends
The human immunodeficiency virus (HIV) and chronic kidney disease (CKD) have emerged as significant public health concerns, complicating disease progression and treatment strategies. According to data from the United Nations AIDS Programme (UNAIDS),1 approximately 40.8 million individuals worldwide were living with HIV as of 2024, resulting in about 44.1 million deaths attributable to AIDS-related diseases. The prevalence of CKD among global HIV-infected individuals (People Living With HIV, PLWH) is 6.4%, with the highest rate in Africa at 7.9%.2 In Ethiopia,3 the prevalence of CKD among PLWH ranges from 7.6% to 20.7%. HIV directly damages the host or increases susceptibility to opportunistic infections, impacting all organ systems.4 The kidneys are one of the organs most frequently affected by HIV-infected individuals.5 PLWH patients often face age-related complications,and long-term antiretroviral therapy(ART) may contribute to the development of CKD, cardiovascular diseases and other adverse effects. Another study by Peck et al Research indicates that in Tanzania, adults infected with HIV who have undergone antiretroviral therapy (ART) for more than two years have a high risk of developing hypertension and kidney diseases.6 CKD is characterized by its progressive nature and can advance to end-stage renal disease (ESRD), which significantly diminishes patients’ quality of life and elevates mortality risk. The CKD of PLWH patients may be caused by various factors,7,8 including age,opportunistic infections, polypharmacy, drug interactions, as well as hypertension, diabetes, and other comorbidities. Additionally, HIV can directly induce CKD through infection of the kidneys, leading to the pathological process known as HIVAN. This process involves viral gene expression and the infection of glomerular and tubular epithelial cells. Furthermore, the kidneys can serve as a reservoir for HIV strains, triggering dysregulation of cellular pathways, inflammatory responses, cell death, and imbalance of cytoskeletal homeostasis.7 If adult PLWH patients develop renal dysfunction, it significantly increases the risk of drug side effects, acute kidney injury, hospitalization, and progression to end-stage renal disease.7,9 Concurrently, kidney diseases exacerbate the progression of conditions in PLWH adversely impacting treatment adherence, quality of life, and survival rates among individuals with HIV/AIDS. Consequently, HIVAN has emerged an a critical and urgent public health concern. Traditional analyses of the literature’s focal areas are often limited, lacking comprehensive assessments at microscopic, mesoscopic, and macroscopic levels. Currently, visualized bibliometric mapping analysis enables a thorough exploration of research trends across multidisciplinary studies.
Bibliometrics is an interdisciplinary field that systematically analyzes keyword clustering and the emergence of research trends using mathematical, bibliographic, and statistical methods. By employing bibliometric software such as CiteSpace, researchers can examine data related to publication trends, countries, institutions, authors, and journals. Furthermore, this software facilitates the construction of network maps to investigate the development of research trends. Accordingly, this study utilizes CiteSpace to analyze topics related to the research trends topics of HIVAN.
Methods and Materials
Search Strategy and Data Collection
On October 31, 2025, we performed an advanced search in the Web of Science Core Collection (WOSCC) utilizing the search formula “TS= (‘HIV’ OR ‘AIDS’ OR ‘Human Immunodeficiency Virus’)” and “TS= (‘nephropathy’ OR ‘kidney disease’ OR ‘renal disease’ OR ‘CKD’ OR ‘ESRD’ OR ‘HIVAN’)” (Figure 1). This approach identified the research trends within the domain of HIVAN. The date for the search extended was from January 1, 2015 to October 31, 2025, with the language filter set to “English” and the document type specified as “Article”. Initially, the two authors conducted independent searches in WOSCC and subsequently screened the titles, abstracts or full texts to assess their relevance to the research topic of this study. Following this, they independently reviewed, evaluated and discussed the findings to achieve a consensus. The data were then recorded in a plain text file and exported as “Full Record and Cited References”. This data is derived from an open network and does not necessitate additional ethical approval.
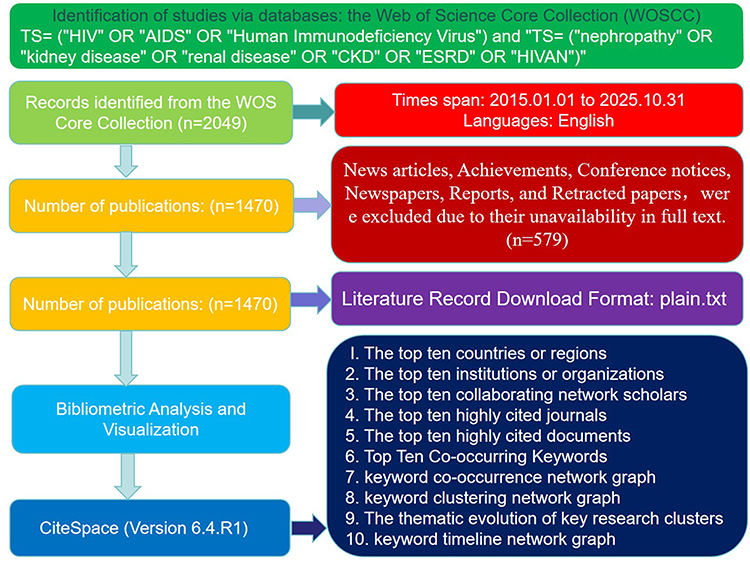 |
Figure 1 Flow chart of the data collection and analysis. |
Data Analysis Method
CiteSpace (Version 6.4.R1) was employed to import data from the download_X.txt file format (Figure 1). The parameter settings included a g-index (k=25) as the filtering criterion, a time slice unit of 1 and a time span from January 1, 2015 to October 31, 2025. To identify the most significant structural relationships within the network, the algorithms “pathfinder” and “pruning sliced networks” were selected for pruning, while the remaining parameters were maintained at their default values. Following execution, the parameters were optimized to yield the relevant data and network diagrams.
Research Results
General Information
After the search, a total of 2,049 original data points were obtained (Figure 1). A total of 579 irrelevant or duplicate documents, including news articles, achievements, conference notices, newspapers, reports, and retracted papers, were excluded due to their unavailability in full text. Ultimately, 1,470 target English documents that met the research criteria were included, comprising contributions from 11,320 authors, 8,101 institutions, 126 countries/regions, and 468 journals.
Publication Trends
The number of publications was 129 in 2015, rising to a peak of 142 in 2016. It reached 143 from 2017 to 2018, then dropped to 139 during 2019–2020. The figure remained elevated at 148 from 2021 to 2022, before significantly decreasing to 115 in 2023. Subsequently, it increased to 140 in 2024, only to decline again to 125 in 2025. Overall, the number of publications exhibited considerable fluctuations, with notable peaks in 2016 and during 2019–2020, while also reflecting a long-term downward trend. The linear regression equation derived from the publication trend graph is y= −2x+4173.6, with R2 =0.2909. The slope of −2 suggests an expected annual decline of approximately 2 publications, underscoring the long-term downward trajectory. The R2value of 0.2909 indicates that this linear model accounts for a moderate portion of the variability in publication numbers, implying that fluctuations are influenced not only by temporal factors but also influenced by other elements not captured in the model, such as shifts in research trends and policy changes.
The Top Ten Countries or Regions
The United States leads with the highest number of citations at 676; the United Kingdom follows with 157 citations; South Africa 110 citations; France is fourth with 98 citations; China holds place with 95 citations; Italy is sixth with 86 citations; Canada ranks seventh with 77 citations; Australia is eighth with 68 citations; Spain is ninth with 67 citations; and Switzerland rounds out the top ten with 54 citations.
The Top Ten Institutions or Organizations
The University of California system ranks first in citation frequency, with a total of 121 citations. Johns Hopkins University follows in second place, amassing 109 citations. The University of London ranks third, with 96 citations. In fourth place is the United States Department of Veterans Affairs, which has received 89 citations. TheDepartment of Veterans Health Administration occupies the fifth position, with 86 citations. Harvard University is sixth, with 84 citations. The University of California, San Francisco, ranks seventh, with 82 citations. The French National Institute of Health and Medical Research is eighth, with 73 citations. University College London holds the ninth position, with 63 citations. Finally, the affiliated institution of Harvard Medical School ranks tenth, with 60 citations.
The Top Ten Collaborating Network Scholars
The author with the highest citation frequency is Estrella, Michelle M,10 with 29 citations. Following closely is Shlipak, Michael G,11 with 23 citations. Kopp, Jeffrey B12 ranks third with 21 citations, while Palella, Frank J13 19 and Post, Frank A14 are tied for fourth, each with 19 citations. Winkler, Cheryl A15 19 citations, placing her sixth. Scherzer, Rebecca16 ranks seventh with 17 citations, and Parikh, Chirag R17 follows in eighth with 14 citations. Jotwani, Vasantha18 holds the ninth position with 13 citations, and Mocroft, Amandarounds19 out the list in tenth place with 12 citations.
The Top Ten Highly Cited Journals
The “Clinical Infectious Diseases Journal”, ranks first in citation count, with 743 citations. The second is the “PLOS ONE”, which has 740 citations. The third is “AIDS”, with 717 citations. The journals ranked fourth through tenth include the “International Journal of Nephrology” with 692 citations, “The New England Journal of Medicine” with 648 citations, “American Journal of Nephrology” with 565 citations, “The Lancet” with 549 citations, “Journal of Acquired Immune Deficiency Syndromes” with 534 citations, “American Journal of Nephrology Society Journal” with 525 citations, and “Nephrology, Dialysis, and Transplantation” with 480 citations.
The Top Ten Highly Cited Documents
The most frequently cited work is “Lucas GM,20 2014, CLIN INFECT DIS, V59, PE96, doi:10.1093/cid/ciu617” which has received 63 citations. Following closely is “Mocroft A,19 2016, LANCET HIV, V3, PE23-32, doi:10.1016/S2352-3018(15)00211–8” with 54 citations. The third, most cited article is “Swanepoel CR,21 2018, KIDNEY INT, V93, P545, doi:10.1016/j.kint.2017.11.007” with 53 citations. The fourth position is held by “Ryom L,22 2013, J INFECT DIS, V207, P1359, doi:10.1093/infdis/jit043” with 53 citations. In fifth place is “Kasembeli AN,23 2015, J AM SOC NEPHROL, V26, P2882, doi: 10.1681/ASN.2014050469” with 43 citations. The sixth entry is “Abraham AG,24 2015, CLIN INFECT DIS, V60, P941, doi:10.1093/cid/ciu919” which has garnered 42 citations. The seventh one is “Scherzer R,25 2012, AIDS, V26, P867, doi:10.1097/QAD.0b013e328351f68f” with 41 citations. the Eighth is “Mocroft A,19 2015. PLOS Med. V12, PE1001809. doi:10.1371/journal.pmed.1001809” which has 39 citations. The ninth position is held by “Sax PE,26 2015, LANCET, V385, P2606, doi:10.1016/S0140-6736(15)60616-X” with 36 citations. Finally, the tenth most cited work is “Ekrikpo UE,2 2018, PLOS ONE,V13, PE0195443, doi:10.1371/journal.pone.0195443” which has received 32 citations.
Top Ten Co-Occurring Keywords
The keyword with the highest citation count is chronic kidney disease, cited 391 times. Following this, antiretroviral therapy ranks second with 253 citations, while risk occupies the third position with194 citations. Risk factor is fourth with 174 citations, and disease is fifth with 166 citations, Prevalence ranks sixth with 156 citations, and glomerular filtration rate is seventh with 143 citations. Infection follows in eighth place with 141 citations, while mortality ranks ninth with 139 citations. Lastly, human immunodeficiency virus is tenth with 136 citations.
Discussion
HIV-associated nephropathy (HIVAN) is a renal disorder marked by significant proteinuria. The disease progresses rapidly and ultimately culminates in chronic renal failure.Among people living with HIV (PLWH), other complications, such as diabetes, hypertension, and chronic hepatitis C, are also common. The presence of drug-related nephrotoxicity, which is either specific to or more prevalent in HIV, complicates the distinction between these conditions without biopsy confirmation or a robust case definition of HIVAN. Histological analysis of kidneys affected by HIVAN21,27,28 reveals collapsing glomerulopathy, dedifferentiated proliferation of podocytes and parietal epithelial cells within the glomerulus, formation of focal segmental glomerulosclerosis (FSGS), and microcystic dilation of the renal tubules, ultimately resulting in renal enlargement. Globally, the degree of renal insufficiency also varies by region, with 6.5% in North America, 6.2% in South America, and 2.7% in Europe.2 The prevalence of renal insufficiency among PLWH in Africa14 has been reported to be particularly high, ranging from 25% to 77%.29 A study conducted in Tanzania30,31 indicated a significant incidence of chronic kidney disease among HIV patients undergoing highly active antiretroviral therapy (HAART). Contributing factors include advanced age, male gender, hypertension, and elevated viral load, all of which are associated with chronic kidney disease (CKD). Our research data analyzes and predicts relevant cutting-edge topics and research trends in the field of HIVAN from multiple dimensions.
The trend in research publications (Figure 2) increased from 129 in 2015 to 142 in 2016 subsequently stabilizing within a range of 142 to148. This rise in popularity may be linked to the significant extension of AIDS patients’ survival due to the widespread implementation of antiretroviral therapy. As a major long-term complication of HIV, clinical focus on HIVAN, particularly focal segmental glomerulosclerosis, has sharply intensified. Basic research has investigated the direct damage inflicted by HIV on renal cells, examining the roles of HIV gene products and immune-inflammatory mechanisms. Concurrently, clinical research has concentrated on optimizing antiretroviral therapy (ART) regimens alongside renal protective treatments, leading to a surge in research output. Following a sudden decline to a low of 115 publications in 2021, although there was a rebound; however, the overall trend remained downward. The 114 publications recorded in 2025 were not fully accounted for. The global COVID-19 pandemic in 2021 resulted in the diversion of scientific research resources, hereby impacting the progress of research projects and data collection in the field of HIVAN. Basic research may have encountered a bottleneck in exploring mechanisms, prompting a shift in research focus to interdisciplinary areas, such as HIVAN complicated by diabetic nephropathy. The fluctuations in the volume of publications related to HIVAN research are influenced non-linearly by various factors, including the evolving research trends within the intersecting fields of nephrology, infectious diseases,and immunology. Although the long-term trend indicates a decline, this does not reflect a diminished significance of the field. This trend may be associated with the transformation of research methodologies and output formats, such as the transition from basic research to clinical guidelines and real-world studies, as well as the presentation of relevant findings in the form of reviews and clinical consensus, which were not captured in these statistics.
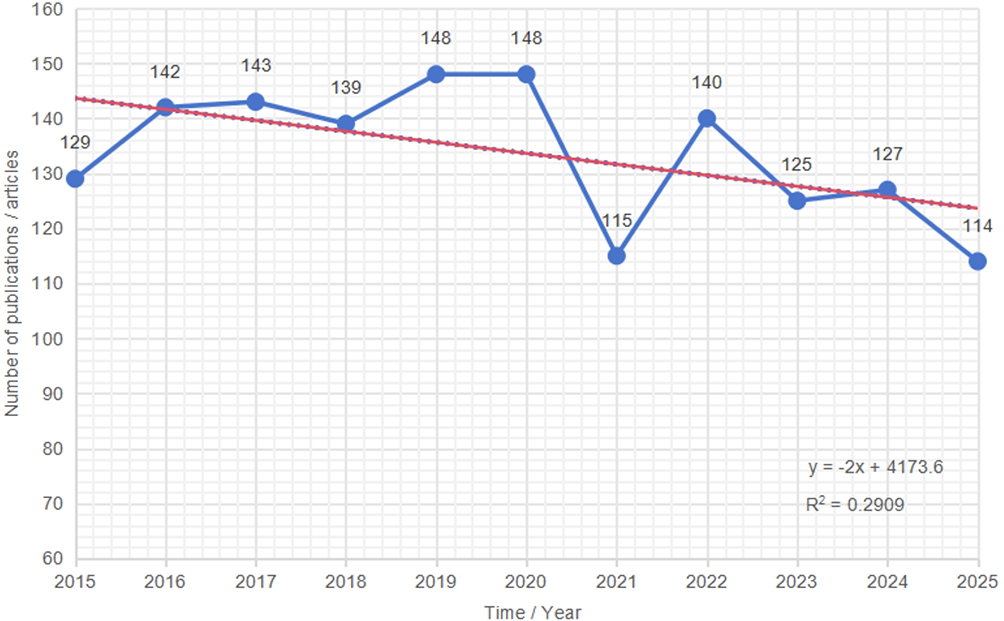 |
Figure 2 Trend chart of publication volume from 2015 to 2025. The horizontal axis denotes publication time, while the vertical axis indicates the number of publications per article. A red trend line is presented, with the linear regression equation given by y= −2x+4173.6, where R2 =0.2909. The slope of −2 suggests an expected annual decrease of approximately 2 articles, reflecting a long-term downward trend; The R2 value of 0.2909 indicates that this linear model possesses moderate explanatory power regarding changes in the number of publications. |
In the cooperation network map of countries and regions (Figure 3), circular nodes represent distinct countries or regions. The size and color intensity of the nodes indicate the scale and activity of scientific research output. For instance, the node representing the United States is the largest and exhibits the most intense color, signifying its dominant position in medical scientific research. The nodes for the United Kingdom, South Africa, France, and China are the second largest, representing key contributors in this field. The lines connecting the nodes illustrate cross-national scientific research collaborations, with the density of these lines indicating the strength of cooperation. Major countries including the United States, the United Kingdom, South Africa, France, and China, establish a core-sub-core distribution of scientific research capabilities, highlighting the concentration of resources in medical scientific research. Their output of results is globally leading. The dense cross-national connections reveal illustrate the trend of global collaboration in medical scientific research, particularly in the domains of infectious diseases, public health, and the mechanisms underlying difficult-to-treat conditions. Such research necessitates the integration of data, technology, and resources from various nations. For instance, partnerships between African nations and those in Europe and America may prioritize tropical diseases and primary healthcare. Prominent cooperation hubs, including leading medical institutions in the United States and research team clusters in China, serve as reference points for cross-national multicenter studies, technology transfer, and resource sharing. Additionally, these collaborations highlight the scientific research division of labor influenced by regional variations in disease spectra. For example, African countries concentrate on field research related to tropical diseases, whereas European and American nations emphasize mechanistic studies and the development of new pharmaceuticals.
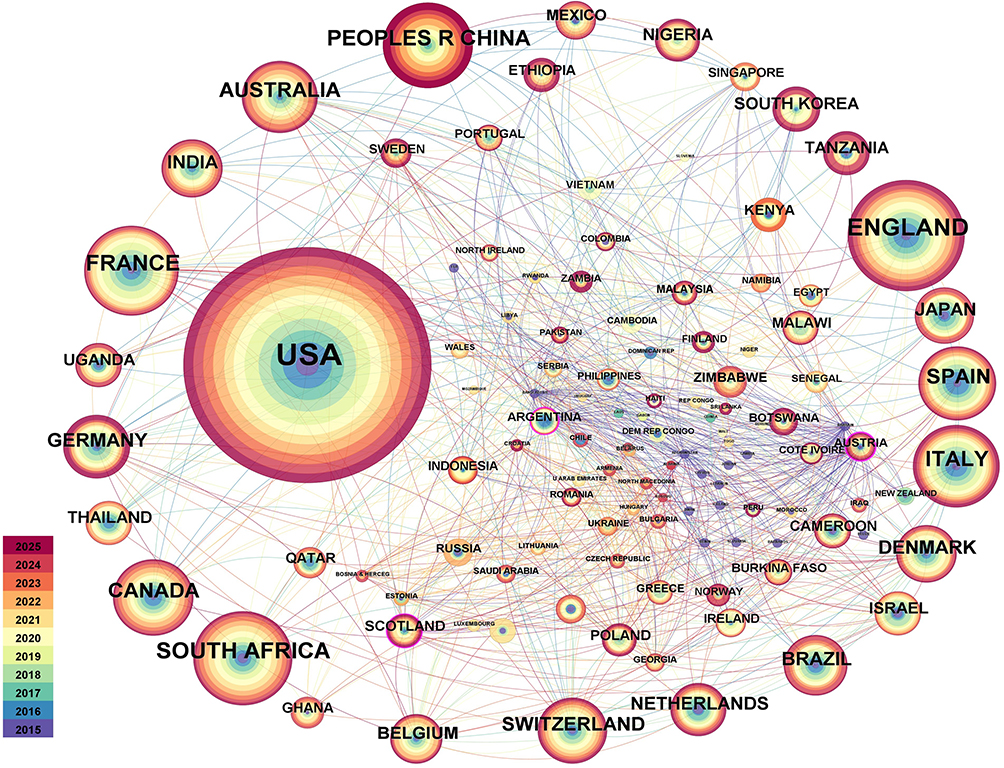 |
Figure 3 Network map of countries and regions, encompassing N=126, E=867, and Density=0.1101, e=1.0. Nodes represent research institutions, with node size corresponding to research output and influence, Node color indicates to the year (Orange for new, blue for old), while the lines illustrate cooperative relationships. |
The institutional cooperation network map of the HIVAN field (Figure 4) illustrates the prominent roles of leading European and American institutions University College London (UCL) and the University of London in the United Kingdom constitute a core cluster, serving as a significant research hub in HIVAN. In United States, Harvard University, the University of California system, Johns Hopkins University, and the Veterans Health Administration (VHA) form another substantial cluster. The VHA frequently conducts cohort studies involving PLWH, including those with kidney disease. The French National Institute of Health and Medical Research (Inserm) is a key participant in continental Europe. Between 2015 and 2020, the collaboration among institutions represented by blue nodes was relatively dispersed, indicating a foundational accumulation stage in HIVAN research. Following 2020, the nodes of core institutions represented by orange nodes expanded, and collaboration intensified, reflecting an increased research focus on HIVAN in the post-combined ART of HIVAN era. ART has significantly decreased HIV-related mortality, yet kidney disease has merged as a critical complication.Despite the extensive implementation of ART, which has markedly lowered the incidence of opportunistic infections among individuals infected with HIV and has improved their health status and life expectancy to near-normal levels, serious kidney disease remains prevalent in this population. In resource-limited settings, routine laboratory monitoring often fails to provide a sufficient foundation for making informed decisions regarding antiretroviral therapy. The absence of regular testing creases the risk of undetected HIV-related renal dysfunction. In developing countries particularly in Africa, where resources for kidney transplantation and dialysis are scarce, the early detection of kidney diseases in (people living with HIV, PLWH) is of considerable clinical and economic significance. This map illustrates the centralized and clustered nature of the HIVAN study across Europe and America, where leading institutions have collaborated to enhance the understanding and treatment of HIVAN. However, participation from institutions in developing countries has been limited. Furthermore the incidence of HIVAN is disproportionately higher among African populations. Moving the forward, it is essential to strengthen global cooperation in this area.
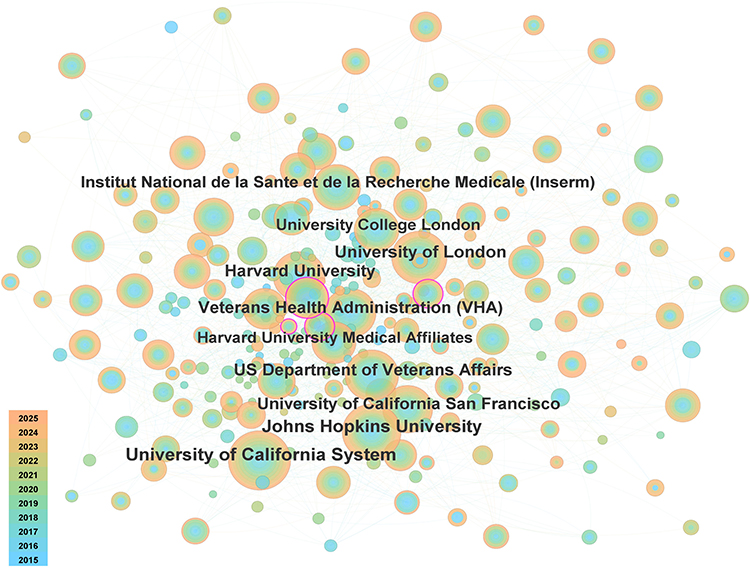 |
Figure 4 Presents a network map of institutional cooperation characterized by N=349, E=1042, Density=0.0172, and e=1.0. |
In the Top 10 list of scholars exhibiting a sudden increase in cooperation (Figure 5), “Strength” (sudden increase intensity) signifies the immediate academic impact of the authors’ research findings. Scholars such as Estrella10 and Palella,13 who experienced a pronounced increase in intensity from 2015 to 2019, concentrated on research areas including the diagnosis and treatment of infectious diseases and the mechanisms underlying chronic diseases, which represented core hotspots during the early and middle stages of the field. Conversely, authors like Campbell32 and Hamzah,33 whose sudden increase commenced after 2021, are engaged in cutting-edge medical domains, such as novel biomarkers and precision diagnosis and treatment technologies. The research of authors such as Fox34 and Marconi,35 who witnessed a sudden increase in 2022, may be aligned with emerging clinical needs. For instance, public health strategies in the post-pandemic era and targeted therapies for rare diseases are anticipated to be focal points in the next 3–5 years. The sudden increase periods of most authors extend until 2025, suggesting that the prominence of COVID-19 and related research, including long-COVID, vaccine boosters, and new antiviral drugs, will remain significant in the coming years. During the pandemic,chronic kidney disease was a risk factor for severe COVID-19 and mortality.36–38 Patients undergoing dialysis exhibited a higher incidence of COVID-19 compared to those with chronic kidney disease who did not require renal replacement therapy.
 |
Figure 5 Illustrates the cooperation among the top ten authors, with red bars denote periods of citation burst. Key contributing authors in this field include Estrella, Michelle M,10 Scherzer, Rebecca,16 Palella, Frank J,13 Campbell, Lucy,32 Hamzah, Lisa,33 Binns-roemer, Elizabeth,32 Fox, Julie,34 Marconi, Vincent C,35 Shamu, Tinei,39 and Chimbetete, Cleophas10 whose work has driven significant advances in HIVAN research. |
The sudden surge in citations of highly cited authors (Figure 6) corroborates and enhances our findings, unveiling the primary contributors of knowledge in the field. The map vividly illustrates the progression of authoritative authors in the field, with their citation spikes aligning closely with significant health events like the COVID-19 pandemic and shifts in research methodologies. Author POZNAK A’s40 citation burst spanned from 2017 to 2019, predating the COVID-19 outbreak. The waning of his impact does not signify obsolescence but rather the integration of his findings as widely accepted knowledge in the field. The exceptionally high intensity (12.64) of SWANEPOEL CR21 from 2020 to 2021 signifies that this work has become a central focus in recent years. The citation burst of authors MARCUS JL41 and GALLANT J42 from 2021 to 2025 started at the beginning of the pandemic, defining as they defined the clinical characteristics and risks of associated with PLWH infected with COVID-19, Their contributions have significantly advanced clinical research on COVID-19-related renal injury, and issuing far-reaching clinical management guidelines. Currently, authors EKRIKPO UE2 (intensity 12.3), HERON JE43 (intensity 9.88), KUDOSE S44 (intensity 6.74), ALFANO G45 (intensity 8.09), and WYATT CHRISTINAM46 (intensity 8.37) from 2022 to 2023 represent the most active research forces, transitioning from initial phenomenon descriptions to exploring underlying mechanisms and developing refined treatment strategies. For instance, KUDOSE S may concentrate on investigating the pathological mechanisms of COVID-19-related renal injury, while ALFANO G may focus on the infection management for specific populations such as kidney transplant recipients. EKRIKPO UE further underscores the globalization of research efforts, particularly highlighting that high-quality studies from regions with significant disease burdens, such as Africa, are garnering global attention. Timely diagnosis and management of chronic kidney disease (CKD)within he PLWH population are essential for preserving renal function and preventing the progression to end-stage renal disease (ESRD).
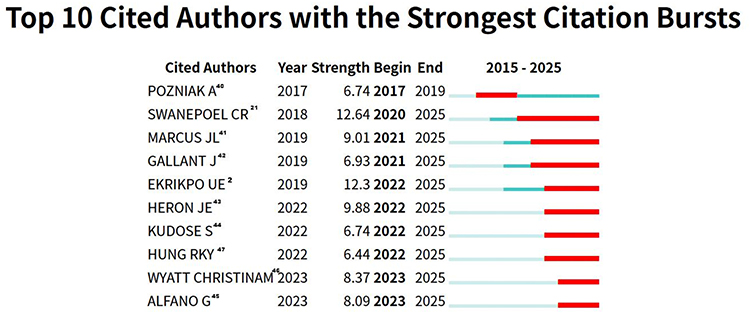 |
Figure 6 Displays an emergence chart of the ten most highly cited authors, where red bars indicate periods of citation burst. The most influential cited authors in this field include POZNIAK A,40 SWANEPOEL CR,21 MARCUS JL,41 GALLANT J,42 EKRIKPO UE,2 HERON JE,43 KUDOSE S,44 HUNG RKY,47 WYATT CHRISTINAM,46 and ALFANO G45 whose work has shaped the landscape of HIVAN research. |
The sudden emergence map of highly cited journals (Figure 7) illustrates the processes through which cutting-edge knowledge is generated, disseminated, and acknowledged by the academic community. These journals serve as central hubs for the distribution of domain-specific knowledge and collectively establish the primary channels for the dissemination of research findings across this interdisciplinary field. “KIDNEY INT REP”,48 “OPEN FORUM INFECT DI”,49 and “VIRUSES-BASEL”50 constitute the professional foundation of this research area. “KIDNEY INT REP” is a top-tier journal in nephrology, “OPEN FORUM INFECT DI” serves as ta significant platform in infectious diseases, and “VIRUSES-BASEL” specializes in virology. The citation bursts observed from 2021 to 2022 indicate that fundamental biological and clinical issues related to viral infections, particularly COVID-19 and renal injury, represent the cornerstone of this research hotspot. “ECLINICALMEDICINE”,34 “JAMA NETW OPEN”,51 “J CLIN MED”, and “FRONT MED-LAUSANNE”52 are esteemed open-access journals that cover a broad spectrum of medical open-access topics. Beginning in 2022 to 2023, a larger community of clinicians and researchers must engage with and implement these findings, making these high-impact, rapidly disseminating journals the preferred choice. The hotspot issue of HIV/kidney/COVID requires the joint attention of experts from multiple fields such as general practice, internal medicine, and public health. Journals such as “SCI REP-UK”53 and “JAMA NETW OPEN” exhibit the highest sudden increases in citation intensity (18.25,16.99), indicating that the research they publish is large in quantity, wide in scope, and can be quickly cited by all sectors. Journals like “INT J ENV RES PUB HE”54 and “JAMA NETW OPEN”, whose sudden increase started from 2021to 2022, correspond to the explosive research in emerging fields such as public health and precision medicine. Additionally, such as “SCI REP-UK” and “FRONT MED-LAUSANNE”, which began to see significant increases from 2017 to 2019 and are projected to continue through 2025, reflect the sustained interest in popularity of interdisciplinary medical research, including medical engineering and translational medicine.
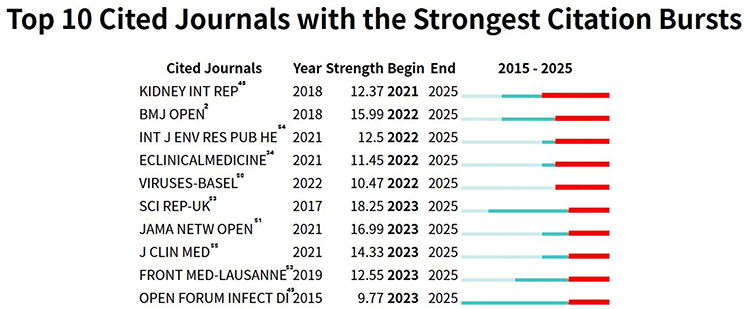 |
Figure 7 Provides an emergence chart of the top ten highly cited journals, with red bars denote periods of citation burst. Key high-impact publication venues in this field include “KIDNEY INT REP”,48 “BMJ Open”,2 “Int J Environ Res Public He”,54 “ECLINICALMEDICINE”,34 “VIRUSES-BASEL”,50 “Sci Rep-UK”,53 “JAMA Netw Open”,51 “J CLIN MED”,55 “FRONT MED-LAUSANNE”,52 and “OPEN FORUM INFECT DI”49 with landmark studies published in these journals. Abbreviations: KIDNEY INT REP, International Journal of Nephrology; BMJ OPEN, British Medical Journal Open; INT J ENV RES PUB HE, International Journal of Environmental Research and Public Health; ECLINICAL MEDICINE, Clinical Medicine; VIRUSES-BASE, Viruses; SCI REP-UK, Science Report; JAMA NETW OPEN, Journal of the American Medical Association: Open Network; J CLIN MED, Clinical Medicine Journal; FRONT MED-LAUSANNE, Medical Frontiers; OPEN FORUM INFECT DI, Open Forum in Infectious Diseases. |
The initial years marking the sudden increase in citations of highly cited references (Figure 8) are all concentrated from 2020 to 2022 and continue to the present, strongly indicating that around 2020, there was a drastic and consensual shift in the knowledge paradigm in this research field, and these few papers are the foundational works supporting this shift. For instance, papers such as Kapp JB12 (2011) and Solomon R25 (2012) published from 2011 to 2016, the citation volume may have been relatively stable in the years after publication. However, their citation counts experienced a dramatic surge after being rediscovered or their value was re-evaluated around 2020. Additionally, works like Marcus JL (2020) and Heron JE (2020) published around 2020 represent pivotal contributions to the field. Once authoritative diagnosis and treatment guidelines or consensus are issued, they quickly become the behavioral guidelines for global clinicians and researchers. The citation burst periods of most papers last until 2025, meaning that the research they have laid the foundation for will still dominate in the next few years. Monitoring the citing works of these core papers is the most effective method for identifying the latest advancements and points of innovation in the field.
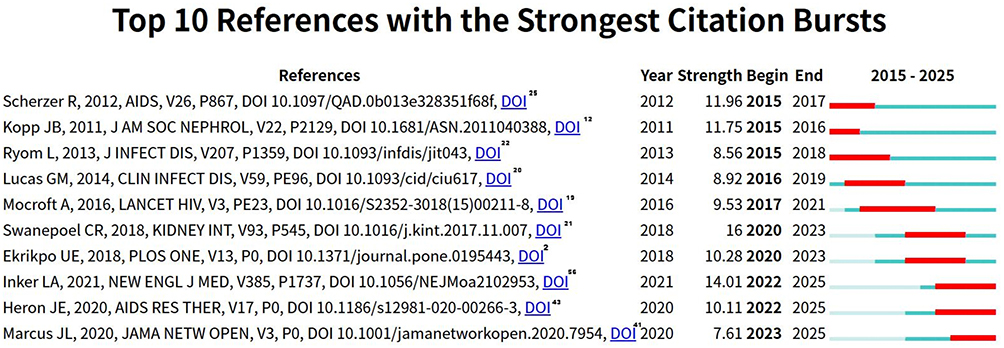 |
Figure 8 Depicts a graph of the top ten most cited papers, with red bars indicate periods of citation burst. Key landmark studies in this analysis include Scherzer R (2012),25 Kopp JB (2011),12 Ryom L (2013),22 Lucas GM (2014),20 Mocroft A (2016),19 Swanepoel CR (2018),21 Ekrikpo UE (2018),2 Inker LA (2021),56 Heron JE (2020)43 and Marcus JL (2020)41 which represent pivotal advances in HIVAN research. |
The co-occurrence keyword network map in the HIVAN field (Figure 9) visually represents research trends and academic associations. Circular nodes in the map represent academic papers. The size and color depth of the nodes usually correspond to the citation volume. The larger the node and the warmer the color, the stronger the academic influence. The lines connecting the nodes illustrate the co-citation relationships among papers; denser lines, signify a higher the association between academic themes.For instance, the highlighted large nodes at the edge and center correspond to core results with high influence in the field, reflecting the fields of medicine. The clustering of nodes connecting the lines elucidates the inheritance and intersection of academic ideas Areas characterized by dense lines represent emerging research clusters, highlighting trends in cross-disciplinary integration within medical scientific research and offering data support for topic selection and strategic planning. In the keyword co-occurrence clustering map (Figure 10), #0 focal segmental glomerulosclerosis, as the red core cluster, is the characteristic pathological manifestation of HIVAN, reflecting the continuous focus of research on the characteristic renal injury of HIVAN, such as podocyte lesions and glomerular collapse, and is the key entry point for distinguishing HIVAN from other kidney diseases. #5 people living with hiv,as the cyan-green cluster, reflects the extension of the research perspective from disease pathology to the full-cycle management of the patient population. This cluster emphasizes the importance of maintaining kidney health in individuals infected with HIV, the compounded effects of comorbidities, such as diabetes and hypertension on renal kidneys function, and the long-term renal damage attributable to the immune dysfunction induced by HIV infection. Cluster #3, identified as kidney transplantation and represented in green, reflects ongoing investigations into treatment alternatives for patients with end-stage HIVAN. The research focuses on the feasibility of kidney transplantation in PLWH, the equilibrium between postoperative immunosuppression and HIV viral control, and the long-term outcomes for transplanted kidneys. #2 renal therapy, the yellow cluster, covers ART, renal replacement therapy, etc. It not only focuses on the reversal effect of ART on HIVAN but also explores strategies to reduce drug-related nephrotoxicity and alternative treatment options for end-stage renal disease. #1 hepatitis c virus, the orange cluster, reflects the research dimension of HIV and hepatitis C virus (HCV) co-infection. HCV can cause nephropathies such as membranoproliferative glomerulonephritis. Clinically, the linked damage to liver and kidney function in HIV/HCV co-infected individuals needs to be considered simultaneously. The research directions include the diagnosis, treatment, and impact on kidney prognosis of co-infection. #4 chronic kidney disease, the green cluster, extends the long-term management needs of HIVAN as CKD, covering disease progression monitoring, complication prevention, lifestyle intervention, etc., which is highly consistent with the clinical situation of the increasing burden of CKD after the long-term survival of PLWH. #6 Acute kidney injury and #7 Cystatin C are involved in the blue and purple clusters, which pertain to the early identification of acute kidney injury and the application of sensitive renal function markers such as cystatin C, facilitating the early screening, disease monitoring, and risk stratification of HIV-associated nephropathy (HIVAN). In people living with HIV (PLWH), chronic kidney disease (CKD) and HIVAN are non-communicable complications that may progress to end-stage renal disease(ESRD).24,57 Although European guidelines32,47 recommend avoiding the use of drugs with potential nephrotoxicity, such as atazanavir, lopinavir, and tenofovir disoproxil fumarate (TDF), in patients with impaired renal function, they do not provide specific recommendations for antiretroviral therapy (ART). Renal impairment is the most common complication of HIV infection, existing both before and after the implementation of ART. Long-term immune and virological management after kidney transplantation in HIVAN patients, assessment of the renal safety of new ART drugs, and in-depth application of multi-omics in the pathogenesis of HIVAN may become hotspots for future research. Through clustering and co-occurrence relationships, the research landscape in the field of HIVAN is systematically presented, from pathology to clinical practice and from single-disease research to interdisciplinary research, providing a clear visual reference for understanding the research logic and future directions in this field. Tracing the hotspots, constructing the context, and planning the frontiers in the field of HIVAN assist researchers in precisely grasping the scientific research logic from basic mechanisms to clinical translation. This understanding facilitates academic advancements in critical in areas, including CKD management, ESRD treatment, and interdisciplinary complications research.
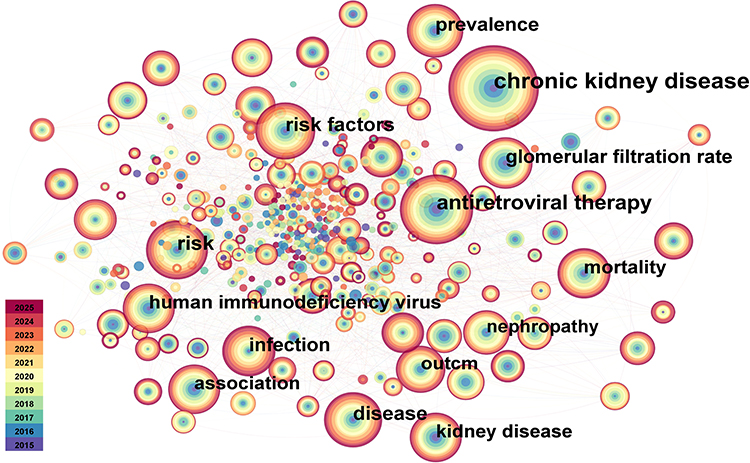 |
Figure 9 Keyword co-occurrence network graph, characterized by N=418, E=1770, Density=0.0203, and e=1.0. |
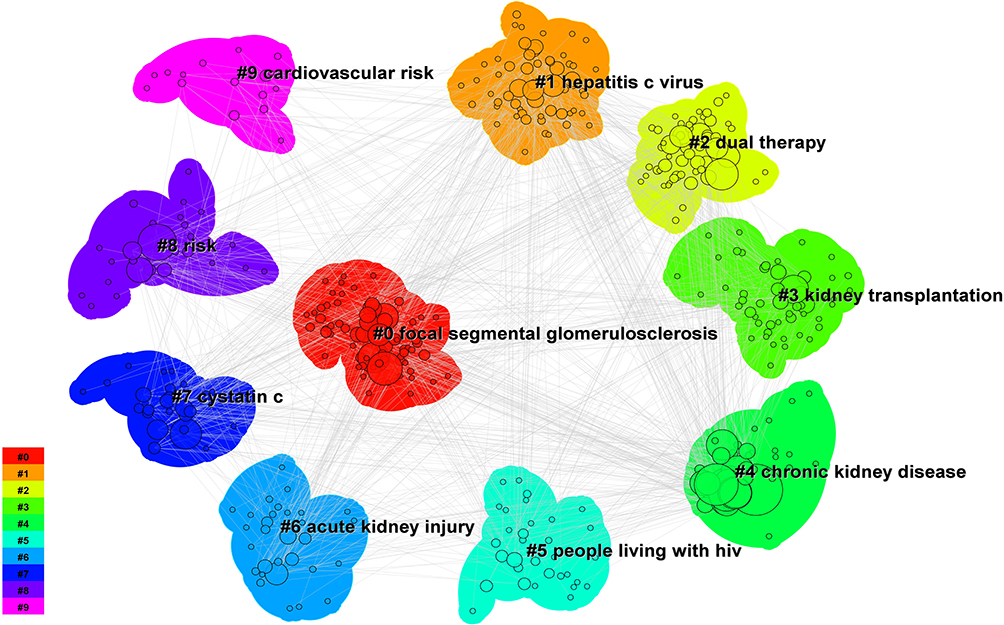 |
Figure 10 Illustrates a keyword clustering network graph, exhibiting a Modularity Q=0.4315 (Q> 0.30), which indicates a significant, structural organization. The and Weighted Mean Silhouette S=0.7198 (S> 0.5), indicating good internal consistency. The themes are categorized into 10 clusters, each represented by distinct color, with the corresponding core themes labeled on the right. Clustering ranking: The numerical order reflects the size and academic influence of the clusters. The #0 section represents the largest and central cluster, while larger numbers #9 such as cardiovascular risk indicate smaller, developing themes. |
The keyword chronological distribution map in the field of HIVAN (Figure 11) illustrates several trends. #0 Focal segmental glomerulosclerosis, a hallmark pathological manifestation of HIVAN, garnered significant attention prior to 2015. This thetrend reflects early research’s focus on the characteristic renal pathology of HIVAN, which serves as a critical marker distinguishing it from other nephropathies. #5 Attention to people living with HIV (PLWH) increased around 2020, indicating a shift in research perspective from disease pathology to patient group management. This shift emphasizes the long-term renal health of PLWH and the compounded damage to the kidneys resulting from comorbidities such as diabetes and hypertension. #9 Cardiovascular risk has seen a rising trend in attention in recent years, revealing that HIVAN patients not only face the risk of renal failure but also have a significantly increased risk of cardiovascular events due to chronic inflammation and metabolic disorders, including dyslipidemia induced by ART drugs. Research has increasingly focused on the comprehensive management of “renal-cardiac comorbidities”. #1 Hepatitis C virus reflects the intersection of liver and kidney diseases. The co-infection rate of HIV and hepatitis C virus (HCV) is high, and HCV can cause nephropathies such as membranoproliferative glomerulonephritis. The continuous popularity of this topic in the figure reflects the research need for liver-kidney linked damage in the context of co-infection. Clinically, it is essential to monitor the liver and renal functions of patients co-infected with HIV and HCV simultaneously. #2 Renal therapy and #3 Kidney transplantation represent the themes of “renal treatment” and “kidney transplantation”, highlighting the clinical exploration of HIVAN treatment. This exploration ranges from ART to delay the progression of nephropathy to the feasibility of kidney transplantation for ESRD, necessitating a careful balance between the risks of HIV-related immunosuppression and transplant rejection. #7 Cystatin C suggests that “cystatin C”, as a sensitive renal function marker, is used for the early screening of HIVAN; #8 Risk encompasses genetic risks, such as mutations in the APOL1 gene, and treatment risks, including the nephrotoxicity associated with ART drugs, facilitating clinical risk stratification and personalized management. From the early research focus on the characteristic pathology of HIVAN to the recent shift towards full-cycle patient management, including comorbidities and cardiovascular risks, the application of biomarkers, and the implementation of comprehensive intervention strategies. The long-term prognosis of HIVAN patients after kidney transplantation, the renal safety of new ART drugs, and the application of multi-omics in the mechanism of HIVAN This progression, from understanding pathological mechanisms to enhancing patient management and addressing comorbidity risks, offers a clear framework for comprehending the developmental trajectory and future directions in this field.
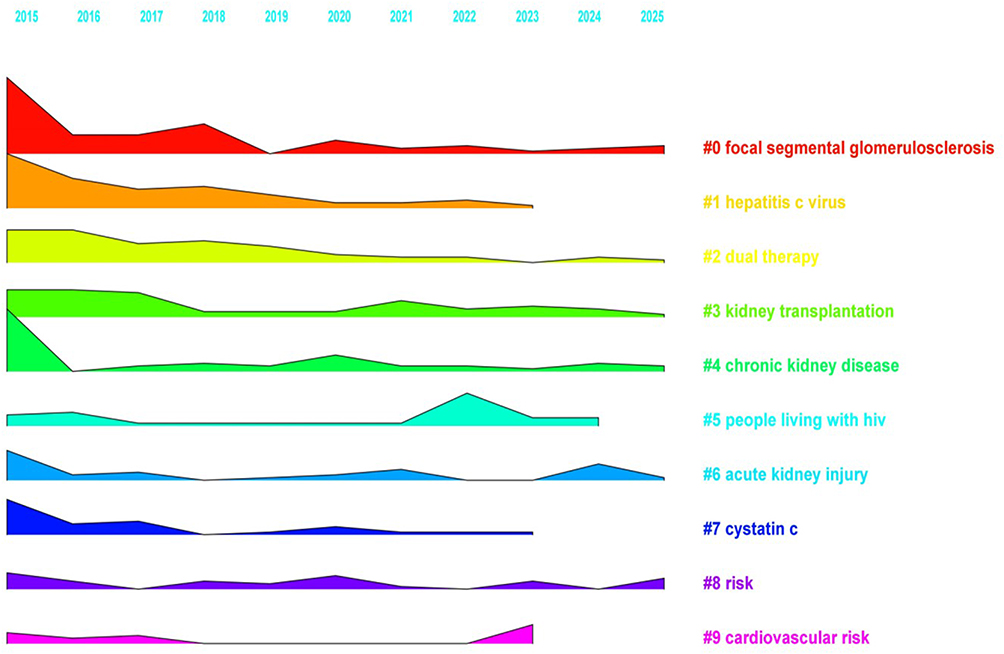 |
Figure 11 Temporal line plot visualizing the thematic evolution of key research clusters (#0-#9) from 2015 to 2025. The horizontal axis denotes the publication year, while each colored horizontal line represents a distinct keyword cluster identified via log-likelihood ratio (LLR) clustering. The vertical position and intensity of each cluster reflect its relative research activity and prominence over time, with warmer colors indicating higher recent engagement. The #0-#9 labels in the figure are the cluster identifiers for the keyword co-occurrence analysis. The smaller the label number, the larger the research cluster and the stronger its influence. #0, focal segmental glomerulosclerosis, represents the largest cluster, while the larger number #9, cardiovascular risk, corresponds to smaller and emerging themes. |
In the timeline-associated network map (Figure 12), a multi-dimensional analysis of HIVAN and the associations indicated by various colors and lines systematically presents the core dimensions of the disease, including pathological mechanisms, clinical phenotypes, treatment interventions, and molecular pathways. The colored nodes on the left side of the figure represent disease subtypes, pathological mechanisms, or molecular markers, while the annotations on the right side correspond to clinical phenotypes, treatment strategies, or research directions. The red node (Kidney disease) highlights the typical pathology of HIVAN, which is closely linked to the direct infection of renal epithelial cells by HIV and the dysregulation of host genes, such as APOL1 mutations. In the population, the genetic susceptibility to kidney disease and AIDS is regulated by variations in the APOL1 gene.58 The green node (Antiretroviral therapy chronic kidney disease) illustrates the dual effects of antiretroviral therapy (ART). It can reduce the occurrence of HIVAN by inhibiting viral replication but may also cause chronic renal injury due to drug toxicity, such as that of tenofovir. Antiretroviral therapy has improved the survival rate of HIV patients, but long-term exposure can lead to age-related diseases and side effects, such as cardiovascular and kidney diseases, affecting the quality of life and increasing the risk of death.44 The blue/purple nodes are associated with complications such as immune complex-mediated nephropathies, including HIV immune complex nephropathy, HIVICK, and thrombotic microangiopathy, which reflect the complex phenotypes of immune dysregulation following HIV infection. The direct infection of renal cells by HIV initiates a cascade of inflammatory factors, resulting in podocyte damage, glomerular collapse, and ultimately leading to proteinuria and renal failure. Early ART can reverse HIVAN, prolonged use of these medications may induce metabolic nephropathies including diabetic nephropathy and renal arteriosclerosis. The risk of developing HIVAN is significantly elevated in individuals of African descent due to mutations in the APOL1 gene. ART combined with renal protection strategies, such as ACEI/ARB drugs, while being vigilant about drug nephrotoxicity; for refractory diseases such as thrombotic microangiopathy, complement inhibitors can be tried. There are unconnected nodes in the figure, such as the cross-mechanism between APOL1 mutations and immune pathways and the assessment of the renal safety of new ART drugs. Through the visual network structure, the complex etiology, phenotypes, and intervention measures of HIVAN are integrated into a systematic framework, providing an intuitive reference tool for clinical decision-making and scientific research exploration. Relevant studies59 have shown that CKD in PLWH is affected by various factors, including direct viral insult, age, hepatitis co-infection, long-term ART exposure, low CD4 count, high viral load, co-infection, opportunistic infection, multi-drug combination, and genetics. HIVAN has become a major health hazard among all HIV-infected populations. Relevant guidelines or research have recommended routine renal function testing. Discontinuation of antiretroviral therapy is associated with increased HIV-related mortality; therefore, it is advisable to enhance the monitoring of nephrotoxicity. Suppression outcomes varied substantially by geographical distance to facility, Intensive adherence counselling (IAC) session attendance, provider cadre, disclosure status, and reported experiences of fear and stigma.59 This includes the active surveillance of risk factors through regular screening and the implementation of preventive strategies to mitigate renal injury and long-term complications arising from antiretroviral therapy. Additionally, non-communicable diseases such as hypertension and diabetes elevate the risk of CKD, necessitating routine screening for the early diagnosis and management of these risk factors.
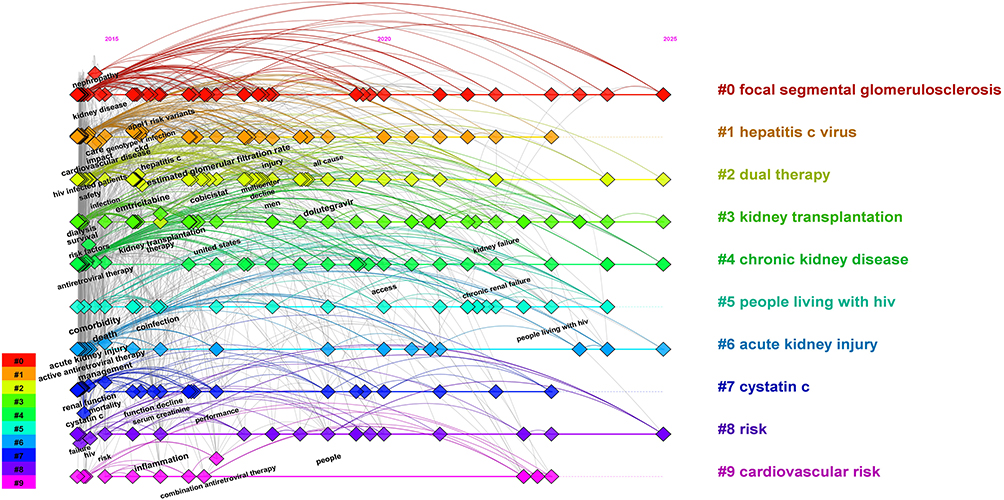 |
Figure 12 Displays a keyword timeline network graph, show casing the popularity of research topics/keywords (indicated by node size), their appearance time (horizontal axis: 2015–2025), theme clustering (represented by color), and the strength of inter-theme associations (depicted by line thickness). |
We conducted comprehensive integrated analyses from various perspectives, including countries or regions, institutions or organizations, journals, authors, references, and keywords. The turning points of this research all converged perfectly between 2020 and 2021. This is an interdisciplinary field focusing on the intersection of HIV infection and kidney diseases, which has evolved into a cutting-edge clinical research hotspot on HIV-kidne-COVID under the impact of the COVID-19 pandemic. The core knowledge production and update are carried out through high-burst journals, and this research is interpreted from multiple dimensions surrounding the co-occurring keywords related to HIVAN, such as glomerular filtration rate, kidney transplantation, immune response, and HCV. However, this research has its limitations. First, the literature included in this study is sourced from the Web of Science Core Collection (WOSCC), which represents only a subset of relevant research on this topic. Affected by factors including the data formats of bibliometric tools, computer software and data updates, domestic and international databases such as PubMed, Scopus, Google Scholar, CNKI, Wanfang, and VIP were excluded, leading to a reduced dataset. Additionally, the data on the quality of articles, authors, or institutions are limited, and some widely used data indicators such as the H-index and Impact Factor are also lacking. Furthermore, this study only included English articles. English is the most commonly used language for publishing academic literature worldwide, and future research should integrate data in multiple non-English languages including Chinese and German for a more comprehensive analysis. Future research that closely links these bibliometric models with the global burden and clinical studies of AIDS-related diseases will enable a more in-depth elaboration of the academic value of the HIVAN domain, and also provides operational insights for future research cooperation and resource allocation in the AIDS-related domain.
In conclusion, this study addresses the critical issue of “HIV-Associated Nephropathy (HIVAN)” Utilizing the bibliometric analysis tool CiteSpace, it systematically reviews and investigates the distribution, research trends, and evolutionary trajectory of related knowledge from 2015 to 2025. The findings reveal both the global distribution and regional focus of research within the domain of AIDS-related kidney diseases. This study constructs a knowledge system for AIDS research by identifying key institutions, academic contributors, and authoritative scholars. It clarifies the thematic focus and knowledge evolution in AIDS-related kidney disease research, indicating that academic activities and influence in this area represent a significant aspect of global public health medical research. By offering a comprehensive, data-driven visualization of the knowledge network surrounding AIDS-related kidney diseases, this study addresses the limitations of traditional literature reviews and provides objective insights into the field’s development over the past decade. It systematically outlines research trends, clarifies the current research landscape, identifies key contributors, and highlights principal research themes, with particular emphasis on the distinctive role of HIVAN within the broader context of kidney disease research. Furthermore, it underscores the necessity of enhancing international collaboration, especially in resource-limited regions. These findings offer scientific guidance for future research aimed at improving treatment adherence, quality of life, and clinical outcomes for patients with AIDS-related kidney diseases.
Abbreviations
USA, United States; ENGLAND, United Kingdom; SOUTH AFRICA, South Africa; FRANCE, France; PEOPLES R CHINA, China; ITALY, Italy; CANADA, Canada; AUSTRALIA, Australia; SPAIN, Spain; SWITZERLAND, Switzerland. University of London, University of London; US Department of Veterans Affairs, US Department of Veterans Affairs; Veterans Health Administration (VHA), Veterans Health Administration; Harvard University, Harvard University; University of California San Francisco, University of California San Francisco; Institut National de la Sante et de la Recherche Medicale (Inserm), French National Institute of Health and Medical Research; University College London, University College London; Harvard University Medical Affiliates, Harvard University Medical Affiliates. CLIN INFECT DIS, Clinical Infectious Diseases; PLOS ONE, Public Library of Science One; aids, AIDS; KIDNEY INT, International Journal of Nephrology; NEW ENGL J MED, New England Journal of Medicine; AM J KIDNEY DIS, American Journal of Kidney Diseases; LANCET, Lancet; JAIDS-J ACQ IMM DEF, Journal of Acquired Immune Deficiency Syndromes; J AM SOC NEPHROL, Journal of the American Society of Nephrology; NEPHROL DIAL TRANSPL, Nephrology Dialysis Transplantation.
Ethical Statement
This data is derived from an open network and does not necessitate additional ethical approval.
Acknowledgments
We would like to express our gratitude to all the authors and colleagues from the department who provided guidance and strong support during this collaborative research and paper-writing process. The greatest thanks are extended to Xiaofeng Wei, Ruijia Huang (Rica) and Ruiqi Huang for their encouragement and support during the writing process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial,or not-for-profit sectors.
Disclosure
All authors declare that they have no conflicts of interest for this work.
References
1. Global HIV & AIDS Statistics—2025 Fact Sheet. Joint United Nations Programme on HIV/AIDS; 2025. Available from: https://www.unaids.org/en/resources/fact-sheet.
2. Ekrikpo UE, Kengne AP, Akpan EE, Effa EE, Bello AK, Okpechi IG. Prevalence and correlates of traditional risk factors for cardiovascular disease in a Nigerian ART-naive HIV population: a cross-sectional study. BMJ Open. 2018;8(7):e019664. doi:10.1136/bmjopen-2017-019664
3. Kefeni BT, Hajito KW, Getnet M. Renal function impairment and associated factors among adult HIV-positive patients attending antiretroviral therapy clinic in Mettu Karl Referral Hospital: cross-sectional study. HIV AIDS. 2021;13:631–18. doi:10.2147/HIV.S301748
4. Mekuria Y, Yilma D, Mekonnen Z, Kassa T, Gedefaw L. Renal function impairment and associated factors among HAART Naïve and experienced adult HIV positive individuals in Southwest Ethiopia: a comparative cross sectional study. PLoS One. 2016;11(8):e0161180. doi:10.1371/journal.pone.0161180
5. Torre D, Speranza F, Martegani R. Impact of highly active antiretroviral therapy on organ-specific manifestations of HIV-1 infection. HIV Med. 2005;6(2):66–78. doi:10.1111/j.1468-1293.2005.00268.x
6. Peck RN, Shedafa R, Kalluvya S, et al. Hypertension, kidney disease, HIV and antiretroviral therapy among Tanzanian adults:a cross-sectional study. BMC Med. 2014;12:125. doi:10.1186/s12916-014-0125-2
7. Wearne N, Davidson B, Blockman M, Swart A, Jones ES. HIV, drugs and the kidney. Drugs Context. 2020;9:2019–11. doi:10.7573/dic.2019-11-1
8. Hughes K, Chang J, Stadtler H, Wyatt C, Klotman M, Blasi M. HIV-1 infection of the kidney: mechanisms and implications. AIDS. 2021;35(3):359–367. doi:10.1097/QAD.0000000000002753
9. Ibrahim F, Naftalin C, Cheserem E, et al. Immunodeficiency and renal impairment are risk factors for HIV-associated acute renal failure. AIDS. 2010;24:2239–2244. doi:10.1097/QAD.0b013e32833c85d6
10. Estrella MM, Li M, Tin A, et al. The association between APOL1 risk alleles and longitudinal kidney function differs by HIV viral suppression status. Clinl Infect Dis. 2015;61(5):627–634. doi:10.1093/cid/civ025
11. Shlipak MG, Sarnak MJ, Katz R, et al. Cystatin C and the risk of death and cardiovascular events among elderly persons. N Engl J Med. 2005;352(20):2040–2050. doi:10.1056/NEJMoa043363
12. Kopp JB, Nelson GW, Sampath K, et al. APOL1 variants and the risk of FSGS and hypertension attributed to kidney disease in African Americans. J Am Soc Nephrol. 2011;22(11):2129–2137. doi:10.1681/ASN.2011040388
13. Palella FJ, Estrella MM, Mei L, et al. Long-term kidney function, proteinuria, and associated risks among HIV-infected and uninfected men. J Acquired Immu Defic Syndr. 2019;81(2):202–210. doi:10.1097/QAI.0000000000002147
14. Post FA, Wainberg MA, Mocroft A, et al. The D:A:D study: design and methods of a prospective cohort study of the long-term effects of antiretroviral therapy. J Acquired Immu Defic Syndr. 2006;43(suppl. 1):S1–S10. doi:10.1097/01.qai.0000237344.71288.8e
15. Winkler CA, Ahuja SK, Kopp JB, et al. Genetic variation in the APOL1 gene and HIV-associated nephropathy. J Am Soc Nephrol. 2012;23(1):134–141. doi:10.1681/ASN.2011070725
16. Scherzer R, Lin H, Abraham AG, et al. Use of urine biomarker-derived clusters to predict the risk of chronic kidney disease and all-cause mortality in HIV-infected women. Nephrol Dial Transplant. 2016;31(9):1478–1485. doi:10.1093/ndt/gfv426
17. Parikh CR, Yasuda T, Karumanchi SA, et al. Urinary biomarkers for the detection of chronic kidney disease. Kidney Int. 2010;77(11):987–994. doi:10.1038/ki.2010.100
18. Jotwani V, Abraham AG, Estrella MM, et al. Association of urinary biomarkers with incident chronic kidney disease in HIV-infected adults. Clin J Am Soc Nephrol. 2016;11(10):1764–1772. doi:10.2215/CJN.01230216
19. Mocroft A, Ryom L, Hill A, et al. Kidney function decline in HIV-infected individuals on modern antiretroviral therapy. Lancet HIV. 2016;3(5):e23–e31. doi:10.1016/S2352-3018(15)00211-8
20. Lucas GM, Anastos K, Cohen M, et al. Kidney disease outcomes in HIV-infected individuals with and without hepatitis C coinfection. Clin Infect Dis. 2014;59(10):e96–e103. doi:10.1093/cid/ciu617
21. Swanepoel CR, Atta MG, D’Agati VD, et al. Kidney disease in the setting of HIV infection: conclusions from a KDIGO controversies conference. Kidney Int. 2018;93(3):545–559. doi:10.1016/j.kint.2017.11.007
22. Ryom L, Hill A, Mocroft A, et al. Risk of end-stage renal disease in HIV-infected individuals initiating antiretroviral therapy. J Infect Dis. 2013;207(9):1359–1367. doi:10.1093/infdis/jit043
23. Kasembeli AN, Duarte R, Ramsay M, et al. APOL1 risk variants are strongly associated with HIV-associated nephropathy in Black South Africans. J Am Soc Nephrol. 2015;26(11):2882–2890. doi:10.1681/ASN.2014050469
24. Abraham AG, Althoff KN, Jing Y, et al. End-stage renal disease among HIV-infected adults in North America. Clin Infect Dis. 2015;60(6):941–949. doi:10.1093/cid/ciu919
25. Scherzer R, Abraham AG, Estrella MM, et al. Urinary biomarkers of kidney disease in HIV-infected individuals. AIDS. 2012;26(7):867–874. doi:10.1097/QAD.0b013e328351f68f
26. Sax PE, Wohl D, Yin MT, et al. Tenofovir alafenamide versus tenofovir disoproxil fumarate, coformulated with elvitegravir, cobicistat, and emtricitabine, for initial treatment of HIV-1 infection: two randomised, double-blind, Phase 3, non-inferiority trials. Lancet. 2015;385(9987):2606–2615. doi:10.1016/S0140-6736(15)60616-X
27. Zhu JY, Fu Y, van de Leemput J, et al. HIV-1 Nef acts in synergy with APOL1-G1 to induce nephrocyte cell death in a new Drosophila model of HIV-related kidney diseases. bioRxiv [Preprint]. 2024;
28. Rosenberg AZ, Naicker S, Winkler CA, Kopp JB. HIV-associated nephropathies:epidemiology, pathology, mechanisms and treatment. Nat Rev Nephrol. 2015;11(3):150–160. doi:10.1038/nrneph.2015.9
29. Msango L, Downs JA, Kalluvya SE, et al. Renal dysfunction among HIV-infected patients starting antiretroviral therapy. AIDS. 2011;25(11):1421–1425. doi:10.1097/qad.0b013e328348a4b1
30. Mapesi H, Kalinjuma AV, Ngerecha A, et al; KIULARCO Study Group. Prevalence and evolution of renal Impairment in people living with HIV in rural Tanzania. Open Forum Infect Dis. 2018;5(4):ofy072. doi:10.1093/ofid/ofy072
31. Mwemezi O, Ruggajo P, Mngumi J, Furia FF. Renal dysfunction among HIV-infected patients on antiretroviral therapy in Dar es Salaam, Tanzania: a cross-sectional study. Int J Nephrol. 2020;2020:8378947. doi:10.1155/2020/8378947
32. Campbell L, Hung RKY, Binns-Roemer E, et al. Genetic variants of APOL1 are major determinants of kidney failure in people of African Ancestry with HIV. Kidney Int Rep. 2022;7(4):786–796. doi:10.1016/j.ekir.2022.01.1054
33. Hamzah L, Gathogo EN, Hilton R, et al. Kidney transplantation in HIV-positive adults: the UK experience. Int J STD AIDS. 2013;24(9):596–601. doi:10.1177/0956462413493266
34. Fox J, Hung RKY, Johnson MA, et al. The epidemiology of kidney disease in people of African Ancestry with HIV in the UK. EClinicalMedicine. 2021;38:101024. doi:10.1016/j.eclinm.2021.101006
35. Marconi VC, Manyazewal T, Worku A, et al. The potential use of Digital Health Technologies in the African context: a systematic review of evidence from Ethiopia. Npj Digital Med. 2021;4(1):158. doi:10.1038/s41746-021-00483-8
36. Cheng Y, Luo R, Wang K, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020;97(5):829–838. doi:10.1016/j.kint.2020.03.005
37. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. doi:10.1136/bmj.m1966
38. Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–436. doi:10.1038/s41586-020-2521-4
39. Tinei S, Chimbetete C, Shawarira-Bote S, Mudzviti T, Luthy R. Outcomes of an HIV cohort after a decade of comprehensive care at Newlands Clinic in Harare, Zimbabwe: TENART cohort. PLoS One. 2017;12(10):e0186726. doi:10.1371/journal.pone.0186726
40. Pozniak A, Arribas JR, Gathe J, et al. Antiretrovirals and the kidney in current clinical practice: renal pharmacokinetics, alterations of renal function and renal toxicity. AIDS. 2014;28(5):637–648. doi:10.1097/QAD.0000000000000232
41. Marcus JL, Glidden DV, Mayer KH, et al. HIV infection and the risk of end-stage renal disease in a large urban cohort. J Acquir Immune Defic Syndr. 2021;87(4):495–502. doi:10.1097/QAI.0000000000002684
42. Gallant JE, Arribas JR, Gupta RK, et al. Long-term renal safety of tenofovir alafenamide versus tenofovir disoproxil fumarate in HIV-1-infected treatment-naive adults. AIDS. 2021;35(3):359–367. doi:10.1097/QAD.0000000000002753
43. Heron JE, Isnard Bagnis C, Gracey DM. Contemporary issues and new challenges in chronic kidney disease amongst people living with HIV. BMC Infect Dis. 2020;20(1):266. doi:10.1186/s12981-020-00266-3
44. Kudose S, Hsu CY, Estrella MM. Trends in chronic kidney disease among people living with HIV in the United States, 2000-2020. Clin J Am Soc Nephrol. 2023;18(3):345–354. doi:10.2215/CJN.05620522
45. Alfano G, Cappelli G, Fontana F, et al. Kidney disease in HIV infection. J Clin Med. 2019;8(8):1254. doi:10.3390/jcm8081254
46. Wyatt CM, Fisher MC, Estrella MM. HIV-associated kidney diseases: progress, gaps, and future directions. Clin Microbiol Rev. 2025;38(4):e00207–25. doi:10.1128/cmr.00207-25
47. Ambrosioni J, Levi L, Alagaratnam J, et al; EACS Governing Board. Major revision version 12.0 of the European AIDS Clinical Society guidelines 2023. HIV Med. 2023;24(11):1126–1136. doi:10.1111/hiv.13542
48. Rossetti S, Spinelli L, Giugliano G, et al. Diagnosis and management of HIV-associated nephropathy: a clinical practice update. Kidney Int Rep. 2021;6(10):2678–2687. doi:10.1016/j.ekir.2021.06.025
49. Post FA, Jose S, Hamzah L, et al. Guidelines for the management of chronic kidney disease in HIV-infected patients. Open Forum Infect Dis. 2023;10(5):ofad234. doi:10.1093/ofid/ofad234
50. Marasco D, Blasi M, Hughes K, et al. HIV-1 infection and renal epithelial cell injury: molecular mechanisms and therapeutic targets. Viruses. 2022;14(11):2556. doi:10.3390/v14112556
51. Han TM, Lucas GM, Wyatt CM, et al. Trends in HIVAN diagnosis and management in the United States (2015–2023). JAMA Netw Open. 2023;6(7):e2327567. doi:10.1001/jamanetworkopen.2023.27567
52. Hughes K, Klotman PE, Blasi M, et al. Molecular mechanisms of injury in HIV-associated nephropathy. Front Med Lausanne. 2023;10:323356. doi:10.3389/fmed.2023.323356
53. Wyatt CM, Qian W, Cen J, et al. APOL1 genetic variants and risk of HIVAN in African populations: a population-based study. Sci Rep. 2023;13(1):4567. doi:10.1038/s41598-023-30876-9
54. Oguoma UM, Van Wyk R, Pienaar J, et al. Environmental risk factors for chronic kidney disease in people living with HIV in sub-Saharan Africa. Int J Environ Res Public Health. 2022;19(15):9245. doi:10.3390/ijerph19159245
55. Li Y, Zhang L, Wang H, et al. Estimation of renal function by three CKD-EPI equations in Chinese HIV/AIDS patients. J Clin Med. 2021;10(12):2600. doi:10.3390/jcm10122600
56. Gudaz H, Ogu HA, Schwartz EJ. Long-term dynamics of the kidney disease epidemic among HIV-infected individuals. Spora. 2020;6:52–60. doi:10.61403/2473-5493.1050
57. Waters L, Winston A, Reeves I, et al. BHIVA guidelines on antiretroviral treatment for adults living with HIV-1 2022. HIV Med. 2022;23(Suppl 5):3–115. doi:10.1111/hiv.13446
58. Ali A, Mulatu K, Feleke SF, Wassie GT. Prevalence of chronic kidney disease and associated factors among patients with underlying chronic disease at Dessie Referral Hospital, East Amhara Region, Ethiopia. Front Epidemiol. 2023;3:1154522. doi:10.3389/fepid.2023.1154522
59. Ejalu DL, Okello PS, Puleh SS, et al. Viral load suppression after intensive adherence counselling among previously non-suppressed adolescents and young people with HIV in East-Central Uganda. HIV AIDS. 2026;18:588885. doi:10.2147/HIV.S588885
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge Atlas of the Co-Occurrence of Epilepsy and Autism: A Bibliometric Analysis and Visualization Using VOSviewer and CiteSpace
Wang Y, Huo X, Li W, Xiao L, Li M, Wang C, Sun Y, Sun T
Neuropsychiatric Disease and Treatment 2022, 18:2107-2119
Published Date: 19 September 2022
Enhancing Literature Review and Understanding Under Global Pandemic
Qiao G, Song H, Hou S, Xu J
Risk Management and Healthcare Policy 2023, 16:143-158
Published Date: 3 February 2023
Bibliometric Analysis of Research Themes and Trends of the Co-Occurrence of Autism and ADHD
Liu A, Lu Y, Gong C, Sun J, Wang B, Jiang Z
Neuropsychiatric Disease and Treatment 2023, 19:985-1002
Published Date: 24 April 2023
Hotspots and Trends in Research on Treating Pain with Electroacupuncture: A Bibliometric and Visualization Analysis from 1994 to 2022
Hu L, Yang J, Liu T, Zhang J, Huang X, Yu H
Journal of Pain Research 2023, 16:3673-3691
Published Date: 3 November 2023
Global Research Status of Maca (Lepidium Meyenii Walp.): A Bibliometric Analysis of Hotspots, Bursts, and Trends
Li K, Zhao C, Dang M, Ren R, Fu M, Bai Y, Wang J, Zhang Q, Luan F
Drug Design, Development and Therapy 2025, 19:2329-2349
Published Date: 27 March 2025