Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Research Trends in Chronic Obstructive Pulmonary Disease (2005-2024): From Drug Therapy to Comprehensive Rehabilitation Strategies
Authors Zhan M, Chen J, Zhang H
Received 18 June 2025
Accepted for publication 29 October 2025
Published 11 November 2025 Volume 2025:20 Pages 3659—3671
DOI https://doi.org/10.2147/COPD.S548108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jill Ohar
Miao Zhan,1,2 Jing Chen,2,3 Hongying Zhang1,2
1Department of Science and Education, The Affiliated Rehabilitation Hospital of Chongqing Medical University, Chongqing city, 400084, People’s Republic of China; 2School of Nursing, Chongqing Medical University, Chongqing city, 400016, People’s Republic of China; 3Department of Breast and Thyroid Surgery, The Second Affiliated Hospital of Chongqing Medical University, Chongqing city, 400010, People’s Republic of China
Correspondence: Hongying Zhang, Department of Science and Education, The Affiliated Rehabilitation Hospital of Chongqing Medical University, Chongqing city, 400084, People’s Republic of China, Email [email protected]
Objective: Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, which has driven efficient and economical management strategies to become a research focus. This study conducted a bibliometric analysis of drug treatment and comprehensive rehabilitation strategies for COPD, providing a scientific basis for future COPD management and offering valuable information and guidance to clinicians, researchers, and policymakers to optimize clinical treatment plans for COPD.
Materials and Methods: Using the statistical analysis software CiteSpace6.4. R1, 11,417 articles exported from the Web of Science Core Collection and Scopus from January 1, 2005, to December 31, 2024, were quantitatively analyzed in terms of annual publication volume, countries, institutions, and keywords, and presented in the form of graphs.
Results: After systematic screening, 3668 articles were included. The annual number of published papers in this field is increasing, but little cooperation has been observed between countries and institutions. In terms of contribution, the United States and the United Kingdom are in leading positions. At the institutional level, Sapienza University of Rome in Italy published the largest number of papers. The high-frequency keywords were pulmonary rehabilitation, quality of life, and bronchodilating agents. Keyword emergent analysis results showed that targeted drugs and intelligent healthcare are new research hotspots.
Conclusion: The management of COPD has achieved a fundamental transformation from being “drug-centered” to “patient-centered”. Research hotspots are mainly focused on bronchodilators and pulmonary rehabilitation, whereas targeted drugs and intelligent healthcare represent future directions of individualization and precision. In future, drugs, rehabilitation, and intelligent technologies should be integrated to build a full-process management model, and key empirical support should be provided through strengthened international collaboration.
Keywords: COPD, combination therapy, pulmonary rehabilitation, intelligent healthcare, bibliometrics
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic non-communicable disease among the elderly. Its main pathological feature is persistent airflow limitation caused by abnormal alveolar structures and bronchial lesions.1 According to the World Health Organization (WHO), approximately three million people die from COPD worldwide each year, and by 2030, it is expected to become the third leading cause of death globally.2,3 COPD accounts for 56% of the total cost of all respiratory diseases, imposing a severe economic and social burden on the global public health system.4 Against this backdrop of high burden and social pressure, exploring effective and cost-effective disease management strategies has become a current research hotspot.
Traditional drug treatment has played a significant role in alleviating symptoms and reducing the frequency of acute exacerbations, but its efficacy is limited in treating systemic damage caused by the disease (such as skeletal muscle atrophy, abnormal nutritional metabolism, anxiety, depression, and other extrapulmonary complications).5,6 The latest evidence-based approaches show that an individualized and interdisciplinary comprehensive rehabilitation strategy based on a thorough assessment and integrating exercise, nutritional support and psychological intervention, can not only significantly improve patients’ lung function, exercise endurance and quality of life, but also provide better economic benefits than simple drug treatment.7,8 Given the severe disease burden of COPD and the need for transformation in rehabilitation strategies, deepening research on COPD management system has significant public health value.
Bibliometric methods provide powerful tools for revealing the development trends of scientific research and help researchers quickly grasp hotspots and dynamics within the field.9 Although currently only a few studies exist in the international community that have conducted bibliometric analyses in the field of COPD, most have focused on drug treatment or specific rehabilitation methods, lacking a systematic review of the overall COPD management from “single drug treatment” to “comprehensive rehabilitation strategies”.10–12 To fill this gap, this study deliberately introduced the software CiteSpace as a literature visualization analysis tool. This software has unique advantages for identifying the emergence of research frontiers and visualizing the evolution of knowledge structures. Therefore, driven by the need to explore key future intervention directions for COPD, this article provides a phased summary of the research hotspots and development trends in the transition from pharmacological treatments to comprehensive rehabilitation strategies for COPD. This study aimed to offer a scientific basis for future COPD management and provide valuable information and guidance for clinicians, researchers, and policymakers to optimize clinical treatment plans for COPD.
Materials and Methods
Criteria for Inclusion and Exclusion of Literature
The inclusion criteria were as follows: (1) The research content was related to COPD drug treatment or comprehensive rehabilitation. (2) The Web of Science of Core Collection (WoSCC) and Scopus were limited to English articles. (3) Articles and reviews.
Exclusion criteria were: (1) Conferences, newspapers, books, patents, achievements, etc.; (2) Full texts that could not be obtained. (3) Repeatedly published literature.
Data Collection
On September 23, 2025, we searched WoSCC and Scopus for studies that met the inclusion and exclusion criteria from January 1, 2005, to December 31, 2024. The following keywords were used; (“Chronic Obstructive Airway Disease” OR “Chronic Obstructive Lung Disease” OR “COAD” OR “Chronic Obstructive Pulmonary Disease” OR “COPD” OR “Chronic Airflow Obstruction”) AND (“Drug Therapy” OR “Pharmacological Treatment” OR “Pulmonary Rehabilitation” OR “Respiratory Rehabilitation” OR “Multidisciplinary Intervention” OR “Non-pharmacological Intervention” OR “Comprehensive Rehabilitation” OR “Lung Rehabilitation”). A total of 3432 documents were retrieved in WoSCC and imported into the software Noteexpress in the “plain text” format. A total of 7985 documents were retrieved from Scopus. First, they were imported to CiteSpace6.4R1, then converted from the “CSV” to the “WOS” format, and finally imported into the software Endnote.
After the exclusion of 856 duplicate documents, 10,561 documents remained. After two researchers read the titles and abstracts in accordance with the inclusion and exclusion criteria, 6893 articles that were not relevant to this study were excluded. Eventually, 3668 articles were retained (Figure 1), named “download_929.txt”, and exported to CiteSpace 6.4R1 for visual analysis.
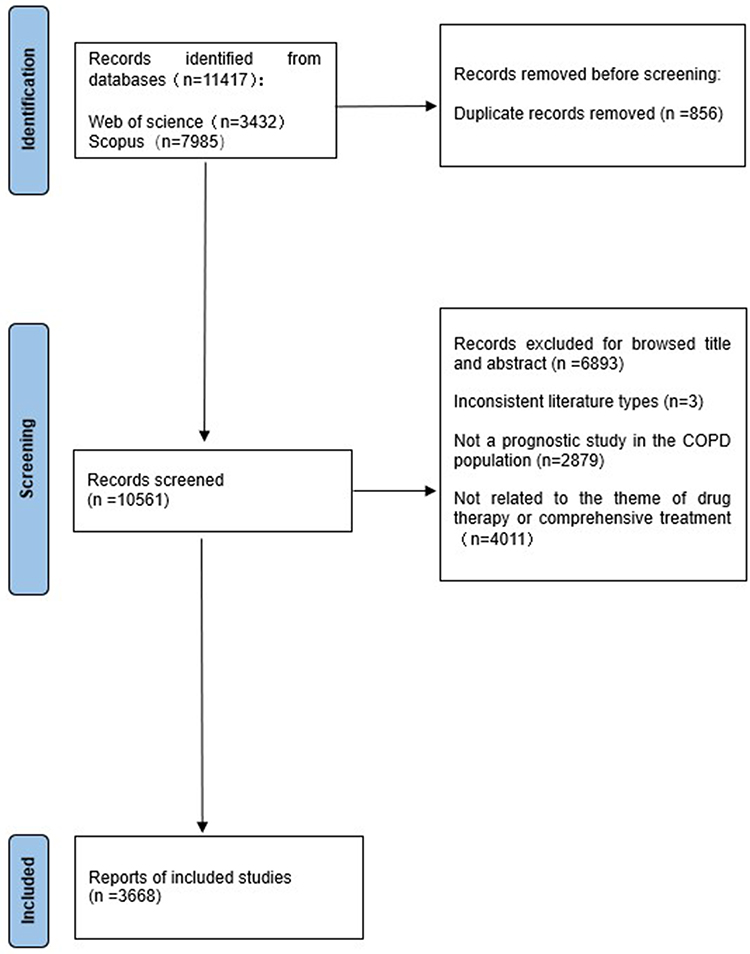 |
Figure 1 The flow chart of study screening process. |
Analytical Method
We set the time span from January 2005 to December 2024 for all analyses and selected “1” as the time node. (1) Number of published articles: Excel was used to plot the annual number of published articles. (2) Node types selected were country, institution, and keyword for the co-occurrence analysis. The k value of g-index was set to “25” and “pathfinder and pruning sliced networks” were used to trim the graph for clear observation of the graph. (3) Keyword cluster analysis: Cluster labels are represented by “#” The cluster module value Q (modularity) and average cluster silhouette value S (silhouette) obtained by the logarithmic likelihood test (LLR) algorithm were used. Among them, a Q value ˃0.3 indicates a significant cluster structure, while a S value ˃0.5 indicates a reasonable cluster and ˃0.7 means that the clustering is convincing.13 (4) Keyword emergent analysis: The γ value was set to 0.5, and the minimum duration was set to four years.
Results
The Number of Publication Outputs and Trends
Although the annual publication volume of literature on COPD, from drug treatment to comprehensive rehabilitation strategies, fluctuates, the overall situation shows an increasing trend (Figure 2), indicating that scientific research activities are becoming increasingly active globally, and the scale and speed of knowledge production are constantly improving. From 2005 to 2017, the number of published studies maintained a stable and relatively gentle growth, indicating that research in this field was in its initial accumulation stage, with increased attention and research investment of global scholars towards it. The irregular fluctuations in the number of published studies from 2018 to 2022 may be related to the global outbreak of the coronavirus 2019 (COVID-19) pandemic at the end of 2019, which limited research. In 2020, the number of published articles did not decrease but instead increased, reaching a peak of 306. This might be related to the attention paid by the global scientific research community to “the management of COPD in the context of COVID-19” Many studies have focused on the issues related to telemedicine, home-based rehabilitation, and digital health. This marks the beginning of a shift in research direction from “hospital-centered treatment” to “comprehensive rehabilitation in community and family settings”.
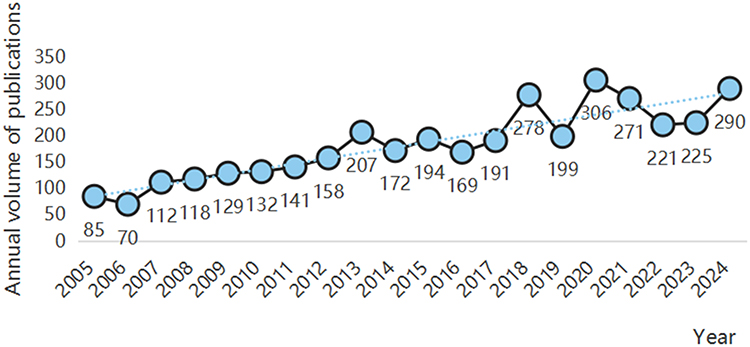 |
Figure 2 The number of publication outputs and growth trend from 2005 to 2024. |
Although the number of published papers in the following four years (2021–2024) slightly declined, it remained at a relatively high level, indicating that the field had entered a stage of adjustment and consolidation. The number of published papers from 2021–2022 slightly declined, possibly because of the postponement of some research projects or the reallocation of resources after the pandemic. The number of published papers in 2023–2024 gradually stabilized and showed a slight upward trend, indicating that the research group may gradually adapt to the new management direction and pay more attention to the long-term management of chronic diseases, rehabilitation interventions, and the optimization of health service models.
In conclusion, the overall trend of COPD expanding from drug treatment to comprehensive rehabilitation not only reflects the evolution of the focus of the global academic community in this field but also reveals the resilience demonstrated globally in response to public health emergencies. In the future, as interdisciplinary integration deepens, this field is expected to continuously expand its research depth and breadth in areas such as personalized medicine and digital health technology.
Country Analysis
Each node represents a country. The larger the node, the more articles the country has published in this field. The lines connecting the nodes represent the connections between countries. The thicker the lines, the closer the connections between countries. After visual analysis (Figure 3), 114 nodes and 36 connections (with a density of 0.0056) were observed, indicating little cooperation among countries. The research was mainly concentrated in the United States (469 articles) and the United Kingdom (416 articles) (Table 1).
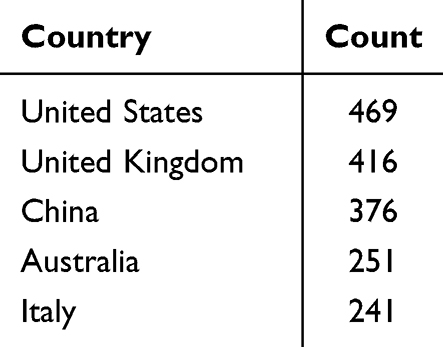 |
Table 1 The Top Five Countries in Terms of the Number of Published Articles |
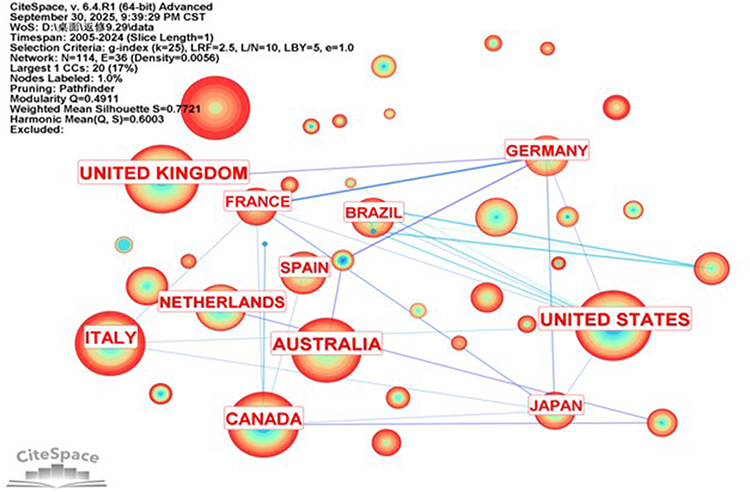 |
Figure 3 National visualization map. |
Institutional Analysis
According to institutional analysis, 510 institutions published relevant research (Figure 4) with seven inter-institutional connections (density 0.0001), indicating a lack of inter-institutional cooperation. The institutions that published more than 10 papers in this field are listed in Table 2. Sapienza University of Rome in Italy published the most papers (20), followed by the University Hospital of Leuven in Belgium (11), Glenfield Hospital in the UK (10), Maastricht University Medical Center in the Netherlands (10), and the National Heart and Lung Institute of Imperial College London in the UK (10).
 |
Table 2 Institutions with a Publication Volume of 10 or More Articles |
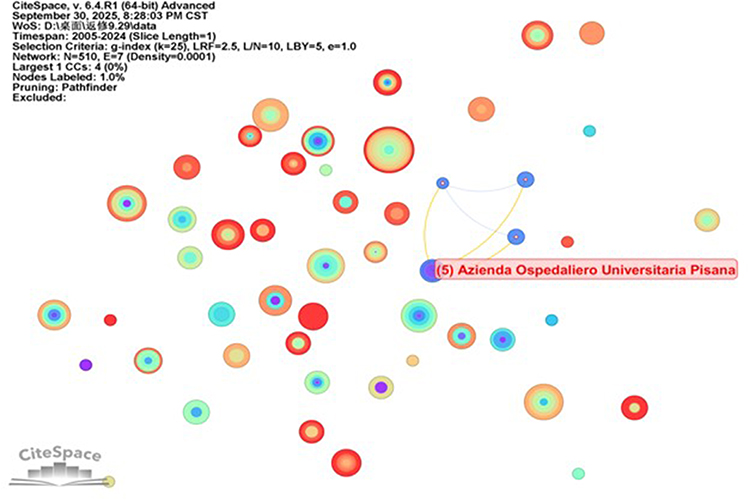 |
Figure 4 Institutional visualization map. |
Keyword Analysis
High-Frequency Keywords
Keywords are a vocabulary used to quickly summarize a research topic, core content, and research focus. Co-occurrence analysis is conducive for quickly identifying research hotspots and future research directions in this field. From 2005 to 2024, 863 high-frequency keywords were used in the field of COPD, from drug treatment to comprehensive rehabilitation strategies, with 3513 connections between each keyword and a density of 0.0094.
Research hotspots in this field are highly concentrated on the comprehensive management of COPD, especially in several core directions such as pulmonary rehabilitation, quality of life, drug treatment and functional assessment (Figure 5). First, the keywords “Pulmonary rehabilitation” and “Quality of life” not only rank high in frequency but also occupy a central position in the network structure, indicating that the improvement of patients quality of life by pulmonary rehabilitation has become an important issue in this field. Second, “Bronchodilating agents” and “Drug therapy” as frequently co-occurring keywords clearly indicate the core position of drug therapy—especially bronchodilators—in the basic treatment of COPD. “Forced expiratory volume” and “Six minute walk test”, as key indicators for evaluating pulmonary function and exercise tolerance in patients with COPD, frequently appear in the co-occurrence network, reflecting the emphasis of clinical research on objective functional assessment. Furthermore, the co-occurrence of “Middle aged” and “Disease exacerbation” suggests that researchers pay attention to the disease progression and acute attack management of the middle-aged population. The terms “Meta-analysis” and “Randomized controlled trial” as high-frequency methodological keywords indicate that this field attaches great importance to evidence-based medicine and the accumulation of high-quality clinical evidence (Table 3).
 |
Table 3 Some High-Frequency Keywords |
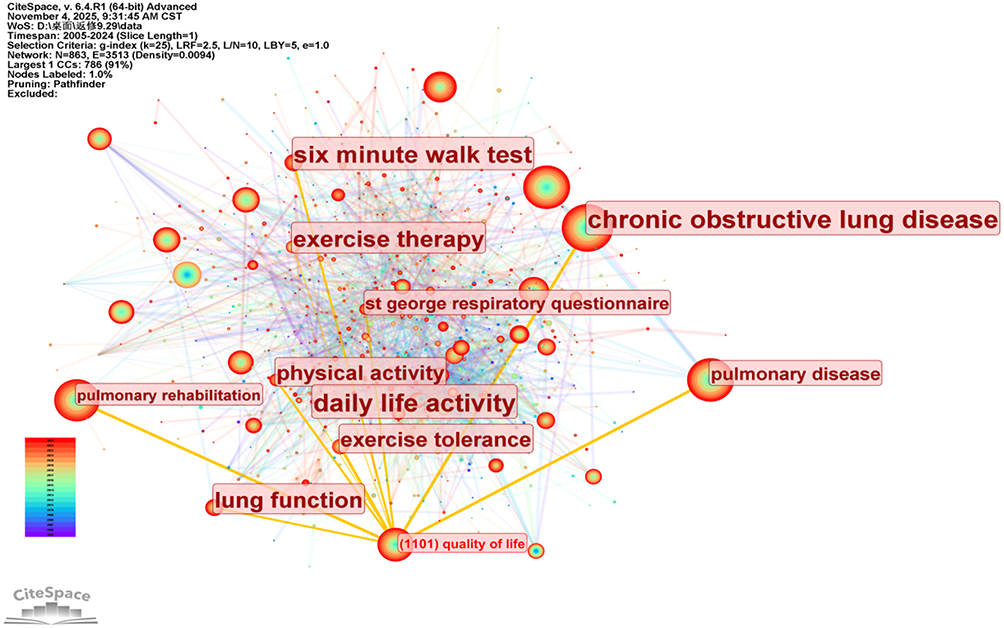 |
Figure 5 Keyword visualization map. |
Keyword Cluster Analysis
In the keyword clustering graph (Figure 6), 10 clustering labels were identified. With modularity Q=0.4911 (Q > 0.3), the clustering structure was significant, and the weighted mean silhouette value was S=0.7721 (S > 0.7), indicating that the clustering results of the graph were highly reliable. The close intersections among clusters indicate a relatively high co-occurrence frequency of keywords among different clusters.
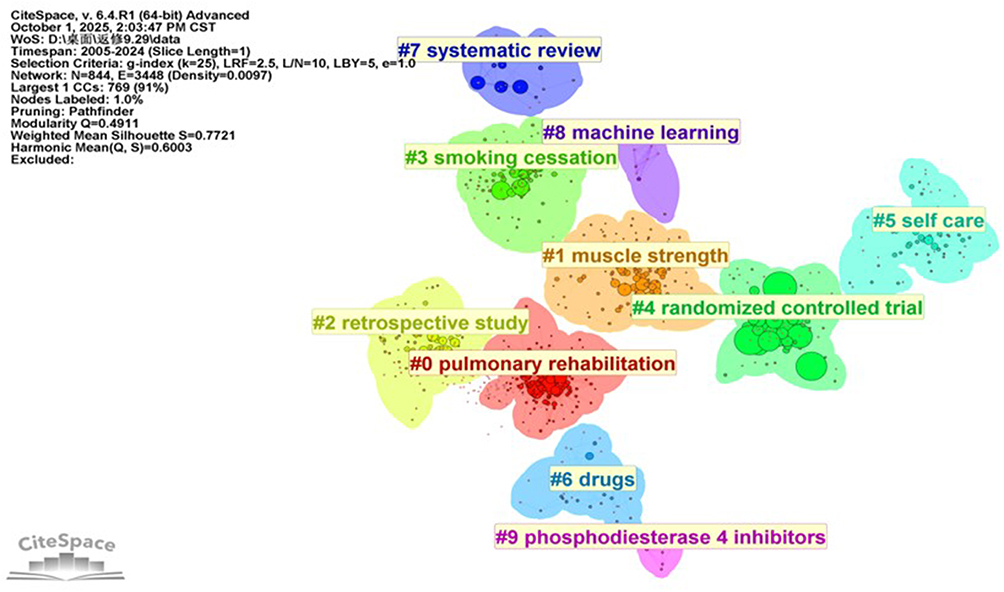 |
Figure 6 Keyword cluster analysis map. |
#0 Pulmonary rehabilitation, this cluster focuses on keywords such as “exercise tolerance” and “quality of life” reflecting the research’s attention to pulmonary rehabilitation training, improvement of exercise capacity and enhancement of patients’ quality of life. This is the core direction of non-pharmacological treatment for COPD. #1 Muscle strength includes “resistance training” “breathing muscle” etc, emphasizing the importance of respiratory muscle training and resistance training in the rehabilitation of COPD. #3 Smoking cessation, with keywords such as “influenza vaccine” indicates that research in this field focuses on behavioral intervention and preventive measures for COPD, especially in terms of smoking control and vaccination. #4 Randomized controlled trial and #7 Systematic review indicate that the research methods in this field are rigorous and attach great importance to high-level scientific evidence to guide clinical practice. #6 Drugs include “Chinese herbal” “C-reactive protein” etc, suggesting that the role of traditional Chinese medicine in anti-inflammatory treatment is gradually attracting attention. #8 Machine learning indicates that research is gradually developing towards intelligence; #9 Phosphodiesterase 4 inhibitors show that targeted drug therapy has been a research hotspot in recent years (Table 4).
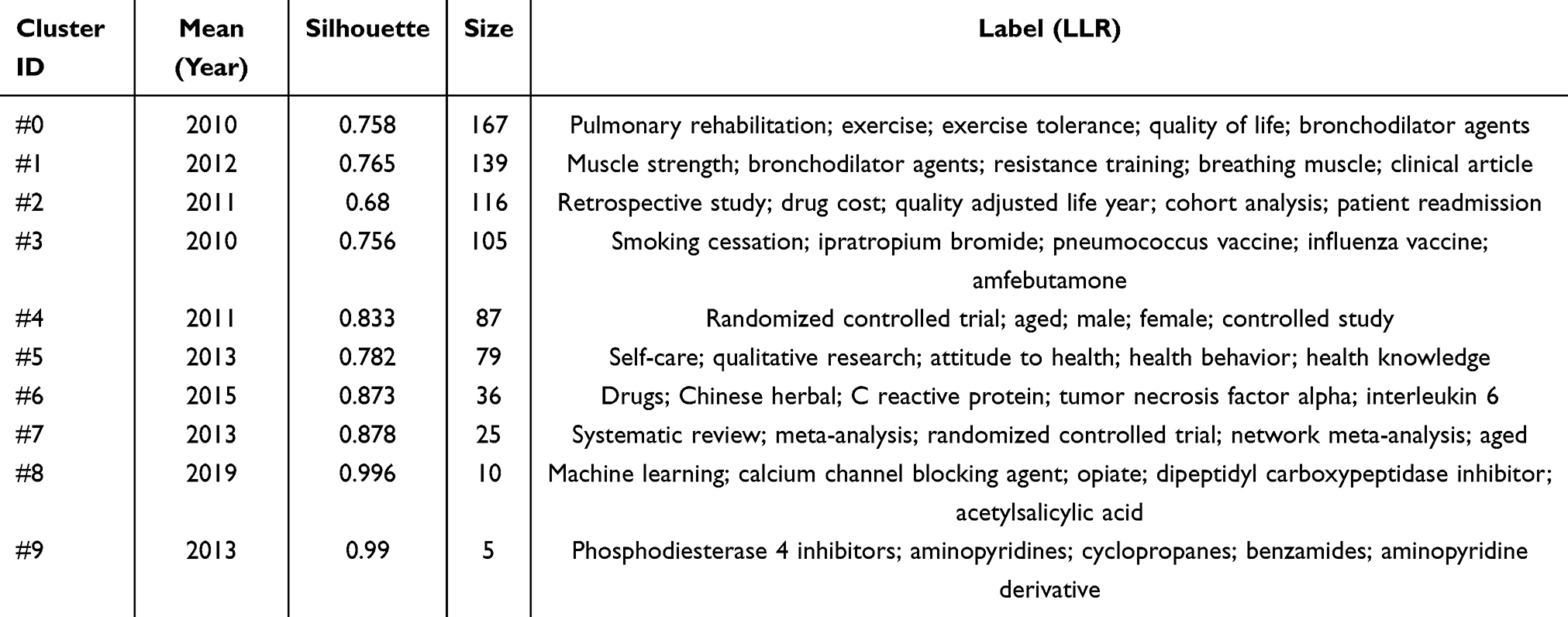 |
Table 4 Cluster Analysis |
Keyword Emergent Analysis
The sudden appearance of keywords refers to a significant and sudden increase in the frequency of keyword occurrence within a certain period, reflecting instantaneous changes in research hotspots. Among them, “Begin” is the earliest appearance time of the keyword, “End” is the end time of the keyword, and “Strength” is the strength of the keyword’s appearance within a specific time. The greater the strength, the greater the research popularity of the keywords within that period.
Based on the keyword emergence chart analyzed by CiteSpace (Figure 7), we obtained the top 20 most-cited keywords to identify emerging research hotspots or important turning points in this field, mainly involving three stages: the initial exploration period (2005–2010), the evolution and expansion period (2011–2015), and the patient-centered long-term management period (2016–2024).
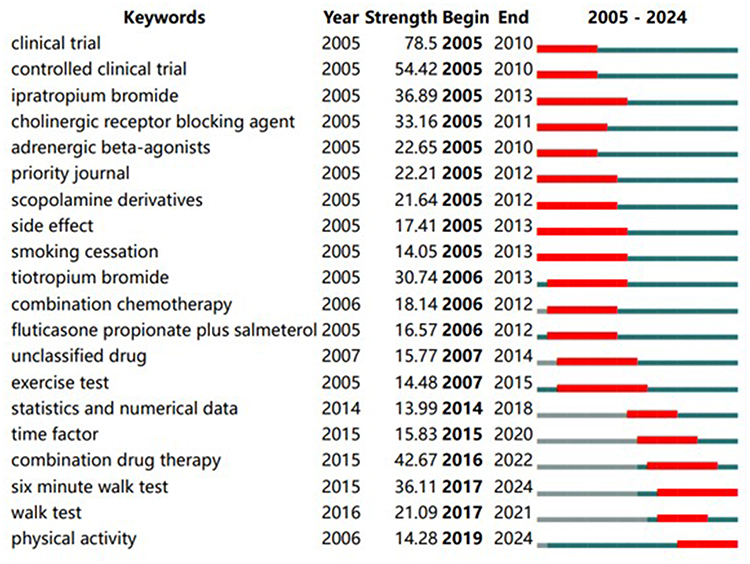 |
Figure 7 Top 20 keywords with the strongest citation bursts. |
Initial Exploration Period (2005–2010)
“Clinical trial (strength=78.5)” and “controlled clinical trial (strength=54.42)” were the research hotspots of this stage. This reveals that the current research is dedicated to exploring the efficacy and safety of the new COPD management model using a rigorous experimental design. These studies not only focus on the construction of evidence at the level of evidence-based medicine but also emphasize promoting the transformation of high-quality clinical data, laying a key scientific research foundation for the optimization of COPD management and the formation of individualized rehabilitation strategies. Moreover, “ipratropium bromide (strength=36.89)”, “tiotropium bromide (strength=30.74) and” adrenergic beta-agonists (strength=22.65)” were the most representative clinical drug research directions at the time. Their wide application and in-depth research not only confirmed their definite therapeutic effects in alleviating airway obstruction and improving lung function in patients with COPD, but also marked an important evolution in the drug treatment of COPD from a single symptomatic treatment to a combined, long-acting, and precise treatment strategy. Furthermore, “side effect (strength=17.41)” indicates that while scholars pursue the effectiveness of drug treatment, the safety of drugs has also become a core theme worthy of consideration. This lays a solid foundation for subsequent research on “combination drug therapy (strength=42.67)”.14,15 To ensure therapeutic effects while minimizing the side effects caused by excessive doses of a single drug, researchers have actively explored the combined use of drugs with different mechanisms of action to achieve synergistic effects and offset side effects. The conclusion of Mario et al also supports this view.16 Finally, the significance of “smoking cessation (strength=14.1)” as a basic treatment has also been confirmed.
Evolution and Expansion Period (2011–2015)
The sudden appearance of keywords “combination drug therapy (strength=42.67)” and “fluticasone propionate plus salmeterol (strength=16.57)” marks a core shift in drug treatment strategies—from monotherapy to combination therapy. Moreover, compound preparations such as fluticasone and salmeterol are the focus at this stage and play a significant role in improving the clinical outcomes of patients with COPD. For instance, Peter et al conducted a randomized controlled trial of inhaled corticosteroids combined with long-acting β2 receptor agonists, the results indicated that the combined treatment of fluticasone and salmeterol could effectively reduce the disease progression in patients with COPD and improve their quality of life and lung function.17 Clinical research on triple compound preparations has been widely carried out and recognized in recent years.18–20 “Exercise test (strength=14.5)” marks that the research focus has shifted from simple pulmonary function indicators to attention to patients’ exercise endurance, physical function and quality of life.
Patient-Centered Long-Term Management Period (2016–2024)
The “six minute walk test (strength=36.11)”, as a low-complexity and safe test that measures the 6-minute walking distance of patients to assess their exercise endurance and predict morbidity and mortality, has the highest burst intensity at this stage.21,22 The term “physical activity (strength=14.28)” has persisted as an explosive word to this day, which indicates that research in this field has always focused on patient-centered outcome indicators, especially in recent years. This reflects that the goal of COPD management is not only to improve lung function and alleviate symptoms but also to encourage and assist patients to return to life and increase daily activity levels to improve long-term prognosis and quality of life.
In summary, over the past 20 years, treatment strategies and outcome indicators have been optimized. Treatment strategies for COPD have evolved from single-drug regimens to combined regimens. Although widely used bronchodilators and other drugs in the early stages laid the foundation for treatment, managing the high heterogeneity of the disease is difficult. Combination therapy has thus become a cutting-edge trend, overcoming limitations through synergistic effects,23 which is consistent with the research conclusion of Gao et al.10 Besides, pulmonary function can accurately reflect the ventilation and diffusion function status of patients’ lungs. It is not only the gold standard for the early diagnosis of COPD but also a key biological indicator for dynamic assessment of disease prognosis.24 The wide application of the six-minute walk test indicates that the assessment focus has extended from lung function to exercise tolerance and quality of life, embodying a patient-centered modern management concept.
Discussion
This study systematically reviewed the research trends and the evolution of hotspots in the transition from drug treatment to comprehensive rehabilitation strategies for COPD from 2005 to 2024. The results showed that research hotspots in this field have gradually expanded from the early exploration of drug efficacy to a comprehensive system covering pulmonary rehabilitation, functional assessment, quality of life improvement and personalized remote health management.
The Development Context and Prospects of Drug Therapy
The American Thoracic Society has emphasized the core position of drug therapy in the management of COPD, explicitly stating that individualized and stepwise drug treatment strategies should be adopted based on the severity of the patient’s symptoms and the risk of acute exacerbation.25 This study reviews the development of drug treatment for COPD over the past 20 years. Its evolution profoundly reflects the continuous advancement of clinical practice towards precision and individualization. In the early stage, the research focus was mainly on monotherapy, and clinical randomized controlled trials became the main method to verify the efficacy of drugs. With the accumulation of evidence-based studies, combination therapy strategies have gradually become mainstream. Multiple systematic reviews have shown that compound preparations significantly improve the quality of life and reduce the frequency of acute exacerbations in patients with COPD compared with single drugs.26–28 However, although triple therapy is reliable in terms of overall efficacy and safety, the incidence of pneumonia is significantly higher than that of monotherapy or dual-drug therapy.29,30 This contradiction has directly driven the current drug treatment model towards precision and individualization. In recent years, the exploration of targeted drugs such as phosphodiesterase-4 inhibitors and traditional Chinese medicine for anti-inflammatory treatment has not only enriched the drug treatment options for COPD but has also expanded the depth and breadth of its treatment, injecting new vitality into this field.
Breakthroughs and Composition of Comprehensive Rehabilitation Strategies
Although drug therapy plays a core role in the management of COPD, it is difficult to comprehensively address systemic problems, such as the progressive decline of respiratory function and the increased psychological and social burden of patients solely relying on drugs. In the comprehensive rehabilitation system for COPD, non-pharmaceutical interventions have shifted from an auxiliary role to a core pillar in patients with drug treatment. The keyword analysis of this study clearly reveals this trend: Behaviors and rehabilitation interventions such as “pulmonary rehabilitation” “resistance training” “smoking cessation” and “influenza vaccine” constitute current research hotspots.
Among these, pulmonary rehabilitation, as the cornerstone of non-pharmaceutical interventions, holds a particularly prominent core position in the co-occurrence network. This non-pharmaceutical treatment approach organically integrates methods such as exercise training, nutritional support, psychological intervention, and self-management, and with the aid of telemedicine technology, has formed a multi-disciplinary intervention system that enhances synergy.31,32 This not only breaks the vicious cycle of “breathing difficulties - reduced activity - functional decline” at the physiological level, but also enhances patients’ confidence in disease management at the psychological level. Currently, this is the most effective means of reducing costs and increasing efficiency. Many high-quality randomized controlled trials and systematic reviews have consistently confirmed that a systematic pulmonary rehabilitation program can significantly improve exercise endurance, strengthen respiratory muscle function, alleviate breathing difficulties, and enhance overall quality of life.33–36
Of note, this study indicates that this field is deeply integrating with intelligent technologies in the future. The emergence of “machine learning” in clustering indicates that this field is moving towards a new stage of digitalization and intelligence. However, through the analysis of multidimensional health data (such as lung function and activity ability), the algorithm can more accurately predict the risk of acute exacerbation and identify a population that does not comply with treatment to customize a dynamically optimized rehabilitation plan for each patient.37,38 Furthermore, the popularization of remote monitoring devices and mobile medical applications has broken through the limitations of geography and time, extending rehabilitation intervention from hospital wards to patients’ homes, achieving real-time guidance and feedback, and greatly enhancing the accessibility and sustainability of rehabilitation.39–42 These technological means offer a new path for achieving efficient, precise, and more accessible individual health management, indicating that non-pharmaceutical interventions are making a leap towards a smarter and more forward-looking era.
Patient-Centered Management
“Putting people first” is the product of the combination of traditional Chinese culture and modern social concepts, patient-centered services are an important principle in the field of medical services.43 The fundamental purpose of medical intelligence should be to build a patient-centered and data-driven collaborative care system, rather than weakening the dominant position of patients. The results of this study reveal that early research was highly dependent on objective pulmonary function indicators such as “forced expiratory volume” while in the recent patient-centered management stage (2016–2024), “six minute walk test” and “physical activity” monitoring have become key bases for evaluating exercise endurance and quality of life. This transformation reflects that current clinical practice places greater emphasis on patients’ actual functional status and their ability to participate in daily life, stressing that the treatment goal is not only to alleviate symptoms, but also to enhance overall health and daily activity functions.
Therefore, the future management of COPD urgently needs to build an “integrated and personalized” comprehensive care model that integrates precise drug treatment, structured rehabilitation interventions, and intelligent remote technology. This model should consider the core life needs and functional outcomes of patients as their ultimate goal and ultimately achieve a transformation from passive medical care centered on diseases to an active health model that is people-oriented and centered on function and quality of life.
Research Advantages and Limitations
This study utilized the data analysis software CiteSpace to conduct a visual analysis of the literature from the WoSCC and the Scopus databases. Through the annual number of published papers, countries, institutions, and keywords, it deeply explored the phased research hotspots and future directions for COPD, from drug treatment to comprehensive rehabilitation, were identified. This study aimed to lay the foundation for subsequent research to address the global health challenges of COPD.
However, this study had some limitations. (1) This study only included relevant literature from the WoSCC and Scopus databases, which may lead to certain biases in the results of the data analysis. (2) This study included only English literature and excluded non-English literature. This situation may have affected the interpretation of the results.
Conclusion
COPD has undergone a fundamental transformation from drug treatment to comprehensive rehabilitation strategies, shifting from “drug-centered” to “patient-centered”, and from “symptom control” to “comprehensive rehabilitation”. Bronchodilators and pulmonary rehabilitation are research hotspots in this field. Targeted drugs and intelligent medical care have shown great potential for clinical application, indicating that the management of COPD will increasingly focus on intelligence and precision. Future research should focus on integrating drug therapy, rehabilitation training, and intelligent technology to build a systematic and personalized full-process management model to effectively improve the long-term prognosis and quality of life of patients. However, this study also shows that cross-border and cross-institutional cooperation networks are relatively scattered. Therefore, deepening international academic collaborations and conducting high-quality multicenter clinical studies are key to promoting the continuous development of comprehensive management strategies for COPD.
Acknowledgments
Thanks to all study participants. We also would like to express their appreciation to Professor CM Chen, who invented CiteSpace, which is free to use.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Halpin DMG, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
2. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385(9963):117–171. doi:10.1016/S0140-6736(14)61682-2.
3. Kahnert K, Jörres RA, Behr J, Welte T. The diagnosis and treatment of COPD and its comorbidities. Dtsch Arztebl Int. 2023;120(25):434–444. doi:10.3238/arztebl.m2023.027
4. Forum of International Respiratory Societies. The Global Impact of Respiratory Disease.
5. Yamada H, Matsumoto I, Makita N, et al. Effect of timing of bronchodilator therapy initiation on exacerbations in patients with chronic obstructive pulmonary disease: a retrospective cohort study. Respir Res. 2022;23(1):255. doi:10.1186/s12931-022-02184-6
6. Shioya T, Sato S, Iwakura M, et al. Improvement of physical activity in chronic obstructive pulmonary disease by pulmonary rehabilitation and pharmacological treatment. Respir Investig. 2018;56(4):292–306. doi:10.1016/j.resinv.2018.05.002
7. Mulhall P, Criner G. Non-pharmacological treatments for COPD. Respirology. 2016;21(5):791–809. doi:10.1111/resp.12782
8. Zeng Y, Wu Q, Chen Y, Cai S. Early comprehensive pulmonary rehabilitation for hospitalized patients with acute ex-acerbation of chronic obstructive pulmonary disease: a randomized controlled trial. Rehabil Med. 2024;56:jrm39953. doi:10.2340/jrm.v56.39953
9. Thompson DF, Walker CK. A descriptive and historical review of bibliometrics with applications to medical sciences. Pharmacotherapy. 2015;35(6):551–559. doi:10.1002/phar.1586
10. Zhen G, Yingying L, Jingcheng D. Drug therapies for COPD: a bibliometric review from 1980 to 2021. Front Pharmacol. 2022;13:820086. doi:10.3389/fphar.2022.820086
11. Zhou Y, Liu X, Wu W. Mapping the global research landscape and hotspot of exercise therapy and chronic obstructive pulmonary disease: a bibliometric study based on the web of science database from 2011 to 2020. Front Physiol. 2022;13:947637. doi:10.3389/fphys.2022.947637
12. Chen M, Zhang Y, Mao Y, et al. Bibliometric analysis of exercise and chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2023;18:1115–1133. doi:10.2147/COPD.S406955
13. Han X, Wei D. Advances in research on abused women in china: bibliometric analysis by CiteSpace. Trauma Violence Abuse. 2023;24(2):966–980. doi:10.1177/15248380211050562
14. Melani AS, Croce S, Fabbri G, Messina M, Bargagli E. Inhaled corticosteroids in subjects with chronic obstructive pulmonary disease: an old, unfinished history. Biomolecules. 2024;14(2):195. doi:10.3390/biom14020195
15. Parri G, Nieri D, Roggi MA, Vagaggini B, Celi A, Paggiaro P. Fluticasone furoate, umeclidinium bromide, and vilanterol as a combination therapy for chronic obstructive pulmonary disease. Expert Rev Respir Med. 2018;12(12):997–1005. doi:10.1080/17476348.2018.1548936
16. Cazzola M, Rogliani P, Calzetta L, Matera MG. Triple therapy versus single and dual long-acting bronchodilator therapy in COPD: a systematic review and meta-analysis. Eur Respir J. 2018;52(6):1801586. doi:10.1183/13993003.01586-2018
17. Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. doi:10.1056/NEJMoa063070
18. Singh D. Pharmacological treatment of stable chronic obstructive pulmonary disease. Respirology. 2021;26(7):643–651. doi:10.1111/resp.14046
19. Calzetta L, Matera MG, Rogliani P, Cazzola M. The role of triple therapy in the management of COPD. Expert Rev Clin Pharmacol. 2020;13(8):865–874. doi:10.1080/17512433.2020.1787830
20. Zhang S, Wang J, Li X, Zhang H. Comparative effectiveness and safety of triple therapy and non-triple therapy interventions for COPD: an overview of systematic reviews. Ther Adv Respir Dis. 2024;18:17534666241259634. doi:10.1177/17534666241259634
21. Agarwala P, Salzman SH. Six-minute walk test: clinical role, technique, coding, and reimbursement. Chest. 2020;157(3):603–611. doi:10.1016/j.chest.2019.10.014
22. Du H, Wonggom P, Tongpeth J, Clark RA. Six-minute walk test for assessing physical functional capacity in chronic heart failure. Curr Heart Fail Rep. 2017;14(3):158–166. doi:10.1007/s11897-017-0330-3
23. Rodrigues G, Antão J, Deng Q, et al. Trends in initial pharmacological COPD treatment in primary care (2010-2021): a population-based study using the PHARMO data network. Respir Res. 2024;25(1):447. doi:10.1186/s12931-024-03073-w
24. Neder JA, De-torres JP, Milne KM, O’Donnell DE. Lung function testing in chronic obstructive pulmonary disease. Clin Chest Med. 2020;41(3):347–366. doi:10.1016/j.ccm.2020.06.004
25. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. an official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
26. Oba Y, Keeney E, Ghatehorde N, Dias S. Dual combination therapy versus long-acting bronchodilators alone for chronic obstructive pulmonary disease (COPD): a systematic review and network meta-analysis. Cochrane Database Syst Rev. 2018;12(12):CD012620. doi:10.1002/14651858.CD012620.pub2
27. Tanimura K, Sato S, Fujita Y, et al. The efficacy and safety of additional treatment with short-acting muscarinic antagonist combined with long-acting beta-2 agonist in stable patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Chron Respir Dis. 2023;20:14799731231166008. doi:10.1177/14799731231166008
28. Mammen MJ, Pai V, Aaron SD, Nici L, Alhazzani W, Alexander PE. Dual LABA/LAMA therapy versus LABA or LAMA monotherapy for chronic obstructive pulmonary disease. A systematic review and meta-analysis in support of the American Thoracic Society clinical practice guideline. Ann Am Thorac Soc. 2020;17(9):1133–1143. doi:10.1513/AnnalsATS.201912-915OC
29. Zheng Y, Zhu J, Liu Y, et al. Triple therapy in the management of chronic obstructive pulmonary disease: systematic review and meta-analysis. BMJ. 2018;363:k4388. doi:10.1136/bmj.k4388
30. Lee HW, Kim HJ, Jang EJ, Lee CH. Comparisons of efficacy and safety between triple (inhaled corticosteroid/long-acting muscarinic antagonist/long-acting beta-agonist) therapies in chronic obstructive pulmonary disease: systematic review and bayesian network meta-analysis. Respiration. 2021;100(7):631–643. doi:10.1159/000515133
31. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
32. Ji W, Kwon H, Lee S, et al. Mobile health management platform-based pulmonary rehabilitation for patients with non-small cell lung cancer: prospective clinical trial. JMIR mHealth uHealth. 2019;7(6):e12645. doi:10.2196/12645
33. Spruit MA, Pitta F, McAuley E, ZuWallack RL, Nici L. Pulmonary rehabilitation and physical activity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(8):924–933. doi:10.1164/rccm.201505-0929CI
34. Lamberton CE, Mosher CL. Review of the evidence for pulmonary rehabilitation in COPD: clinical benefits and cost-effectiveness. Respir Care. 2024;69(6):686–696. doi:10.4187/respcare.11541
35. Rutkowski S, Rutkowska A, Kiper P, et al. Virtual reality rehabilitation in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2020;15:117–124. doi:10.2147/COPD.S223592
36. Bernocchi P, Vitacca M, La Rovere MT, et al. Home-based telerehabilitation in older patients with chronic obstructive pulmonary disease and heart failure: a randomised controlled trial. Age Ageing. 2018;47(1):82–88. DOI:10.1093/ageing/afx146
37. Smith LA, Oakden-Rayner L, Bird A, et al. Machine learning and deep learning predictive models for long-term prognosis in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet. 2023;5(12):e872–e881. doi:10.1016/S2589-7500(23)00177-2
38. Zhao X, Wang Y, Li J, et al. A machine-learning-derived online prediction model for depression risk in COPD patients: a retrospective cohort study from CHARLS. J Affect Disord. 2025;377:284–293. doi:10.1016/j.jad.2025.02.063
39. Koh JH, Chong LCY, Koh GCH, Tyagi S. Telemedical interventions for chronic obstructive pulmonary disease management: umbrella review. J Med Internet Res. 2023;25:e33185. doi:10.2196/33185
40. Te Braake E, Vaseur R, Grünloh C, Tabak M. The state of the art of eHealth self-management interventions for people with chronic obstructive pulmonary disease: scoping review. J Med Internet Res. 2025;27:e57649. doi:10.2196/57649
41. Chen Y, Zhang Y, Long X, Tu H, Chen J. Effectiveness of virtual reality-complemented pulmonary rehabilitation on lung function, exercise capacity, dyspnea, and health status in chronic obstructive pulmonary disease: systematic review and meta-analysis. J Med Internet Res. 2025;27:e64742. doi:10.2196/64742
42. Schiebler ML, Seo JB. Artificial intelligence analysis of bronchiectasis is predictive of outcomes in chronic obstructive pulmonary disease. Radiology. 2023;307(1):e222675. doi:10.1148/radiol.222675
43. Raina SK, Kumar R, Gupta RK. A primary care-based patient centric palliative care model. J Family Med Prim Care. 2019;8(5):1519–1522. doi:10.4103/jfmpc.jfmpc_391_19
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Re-Defining High Risk COPD with Parameter Response Mapping Based on Machine Learning Models
Pu Y, Zhou X, Zhang D, Guan Y, Xia Y, Tu W, Lu Y, Zhang W, Fu CC, Fang Q, de Bock GH, Liu S, Fan L
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2471-2483
Published Date: 4 October 2022
Development and Validation of a Multivariable Exercise Adherence Prediction Model for Patients with COPD: A Prospective Cohort Study

Ricke E, Bakker EW
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:385-398
Published Date: 22 March 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Development of a Pulmonary Rehabilitation Patient Decision Aid for Patients with Chronic Obstructive Pulmonary Disease: Mixed Methods Study
Jiang Y, Guo J, Chen M, Zou X, Sun P, Gao J, Nuerdawulieti B, Wang S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1377-1389
Published Date: 12 July 2023
Exercise Prescription Training in Chronic Obstructive Pulmonary Disease: Benefits and Mechanisms
Liu S, Yang A, Yu Y, Xu B, Yu G, Wang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1071-1082
Published Date: 15 April 2025