Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Research Status and Hot Spot Visualization Analysis of Osteoporosis from 2014 to 2025
Authors Huang Y, Wang F, Lian K ![]() , Li L, Wang Z
, Li L, Wang Z
Received 20 May 2025
Accepted for publication 9 October 2025
Published 29 October 2025 Volume 2025:18 Pages 6985—7006
DOI https://doi.org/10.2147/JMDH.S541592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yongsong Huang,1 Fan Wang,1 Kun Lian,2 Lin Li,2 Zhenzhen Wang3
1Department of Orthopaedics, The Second Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, Hunan, 410005, People’s Republic of China; 2College of Traditional Chinese Medicine, Hunan University of Chinese Medicine, Changsha, Hunan, 410208, People’s Republic of China; 3Acupuncture Rehabilitation Department, Changsha Traditional Chinese Medicine Hospital, Changsha, Hunan, 410001, People’s Republic of China
Correspondence: Zhenzhen Wang, Acupuncture Rehabilitation Department, Changsha Traditional Chinese Medicine Hospital, Changsha, Hunan, 410001, People’s Republic of China, Tel +86-15243668363, Email [email protected]
Background: Osteoporosis is a progressive bone condition characterized by the erosion of bone mineral density and weakening of bones. A vast volume of clinical research experimental data on osteoporosis has been published in the last 12 years. These studies are mainly focused on clinical observations, animal experiments, and investigations into pathways and targets. However, this information remains disjointed with scarce systematic reviews and comprehensive analyses.
Material and Methods: The Web of Science Core Collection (WoSCC) and PubMed databases were utilized to retrieve relevant osteoporosis literature. Publication volume, journal, authors, keywords, countries, and institutions were bibliometrically and visually analyzed using Citespace 6.3.R3 software, Microsoft Excel 2019, and VOSviewer 1.6.18.0.
Results: There have been 10,343 published reviews and research articles on osteoporosis by 45,966 researchers from 9,462 institutions across 102 countries or regions. Annual publications have been on the rise, particularly in the last few years. The United States, Japan, and China are among the nations involved in this research area. Guangzhou University of Chinese Medicine, and Soochow University are prominent research institutions. Osteoporosis International journal had the most publications and the most cited. Cooper Cyrus was the leading author with a significant volume of publications, while Kanis Ja was noted for having a substantial number of co-citations. An analysis of keywords showed that bone-mineral density, postmenopausal women, and fracture had higher frequencies, leading to thirteen clusters.
Conclusion: Recent research hotspots in osteoporosis are centered on accurate diagnosis, understanding the disease’s pathogenesis, and developing effective, scientific prevention and treatment strategies.
Keywords: osteoporosis, risk factors, precision diagnosis and treatment, visual analysis, bibliometric analysis, pathogenesis
Introduction
Osteoporosis is a chronic bone condition characterized by reduced bone density and structural changes, increasing fracture risk. The bones weaken due to reduced bone mass and a modified microarchitecture, consequently elevating the risk of fragility and fracture.1,2 Globally, over 200 million individuals are affected by osteoporosis. Recent statistics indicate that 1 in 3 women and 1 in 5 men over 50 will experience osteoporotic fractures at some point in their lives.3–5 Osteoporosis imposes a significant disease burden; the economic burden in the US is projected to reach $25.3 billion annually by 2025, reflecting the significant costs associated with osteoporotic fractures and related healthcare needs.6 With increased life expectancy, osteoporosis poses significant health issues such as disability, pain, and even death, along with socio-economic challenges.7 Osteoporosis development is influenced by both natural aging processes and external factors, including glucocorticoid use, hormone deficiencies, decreased bone formation, and microarchitectural disorders.8
Introduced in 1969, bibliometrics, formerly called statistical bibliography, uses statistical methods to analyze literature, and tools like CiteSpace and VOSviewer, revealing research frontiers and trends in a field.9
This research aims to thoroughly assess the current research landscape in this field by analyzing literature on osteoporosis published between 2014 and 2025. It is also structured to analyze, interpret, and summarize relevant studies to delineate future research hotspots and paths, offering significant references and recommendations for scientists in their upcoming investigations and clinical practices.
Methods
Search Strategies
A search for osteoporosis-related literature was conducted on February 28, 2025, using PubMed and the Web of Science Core Collection. The search formula for the Web of Science Core Collection is: Osteoporosis (topic); The search formula in PubMed is: Osteoporosis [Title/Abstract]. The search time range is from 2014 to 2025. The article types are reviews and articles, and the publication language is English. Every article obtained through search was stored as “full records and cited literature” and saved to a text file titled download*txt.
Data Inclusion and Exclusion
Criteria for Inclusion
Research linked to osteoporosis, categorized as articles and reviews, was included.
Criteria for Exclusion
The same published articles, other forms of literature, literature lacking core data such as keywords or author information, and Literature with incorrect parameter formats or unrecognizable parameters.
Processing Procedure
The title, abstract, and full text of every article were reviewed by the first and second authors, who then eliminated any that were unrelated to the subject. They sought input from the third author if they disagreed.
Data Collection and Analysis
The text files previously mentioned were uploaded into the built-in data converter of CiteSpace 6.3.R3 software to produce data formats compatible with the application, which were then saved to corresponding folders. A project titled “osteoporosis” was established within CiteSpace, with the following parameters set as: Time slicing set from January 2014 to February 2025, years per slice = 2, Criteria for selection set to the Top 50, and Pruning options including Pathfinder and Pruning Tender Networks, while all other settings remained at their defaults. Depending on the research objectives, the node type areas were designated as either “keyword or reference.” The keyword Burst Analysis was then selected from the submenu.
Data from the annual publication report generated by CiteSpace was transferred and stored in Microsoft Office Excel 2019 to create a data analysis chart. The parameters for VOSviewer version 1.6.18.0 were as follows: The number of papers from countries should have exceed 3, the number of papers from institutions should surpass 20, the number of journal papers should be greater than 5, more than 400 journals should be cited overall, the number of papers authored by individuals should be more than 12, more than 100 authors should be cited overall, the frequency of keyword occurrences should be more than 70, and the total number of cited references should exceed 20. All other parameters should retain their default settings.
Results
General Information and Annual Publication Output
100,064 publications were obtained: 47,047 from Web of Science and 53,017 from PubMed. Following the removal of duplicate and irrelevant literature, 10,343 pieces of literature were ultimately included. The selection process for the literature is illustrated in Figure 1.
 |
Figure 1 Flowchart of literature selection. |
The advancement of knowledge in the subject is evidenced by the annual publication count, which also acts as a significant indicator of emerging trends.10 The annual publications in this area were summarized over the past 12 years, as depicted by Figure 2. The total volume of publications between 2014 and 2025 exhibited a consistent increasing trajectory. But since there were only two months of data available for 2025, a decrease was noted. Overall, this field has experienced significant growth and gained increasing attention, and is constantly developing and progressing.
 |
Figure 2 Annual number of publications on osteoporosis from 2014 to 2025. |
Distribution of Countries/Territories and Institutions
Collaboration charts provide a novel perspective for evaluating academic impact by illustrating research partnerships among countries and institutions. They uncover trends and highlight the strengths of international collaboration.11 This facilitates the discovery of significant research trends and the establishment of partnerships.11
Following the analysis with VOSviewer software, it was observed from Figure 3A that 102 countries or territories had papers published. Notably, 83 of these countries have published more than 3 papers. The leading countries or territories in terms of publication volume are China (n=4,157), USA (n=1,596), Japan (n=594), England (n=555), and South Korea (n=537). The publication statistics for the top 10 regions or countries are detailed in Table 1.
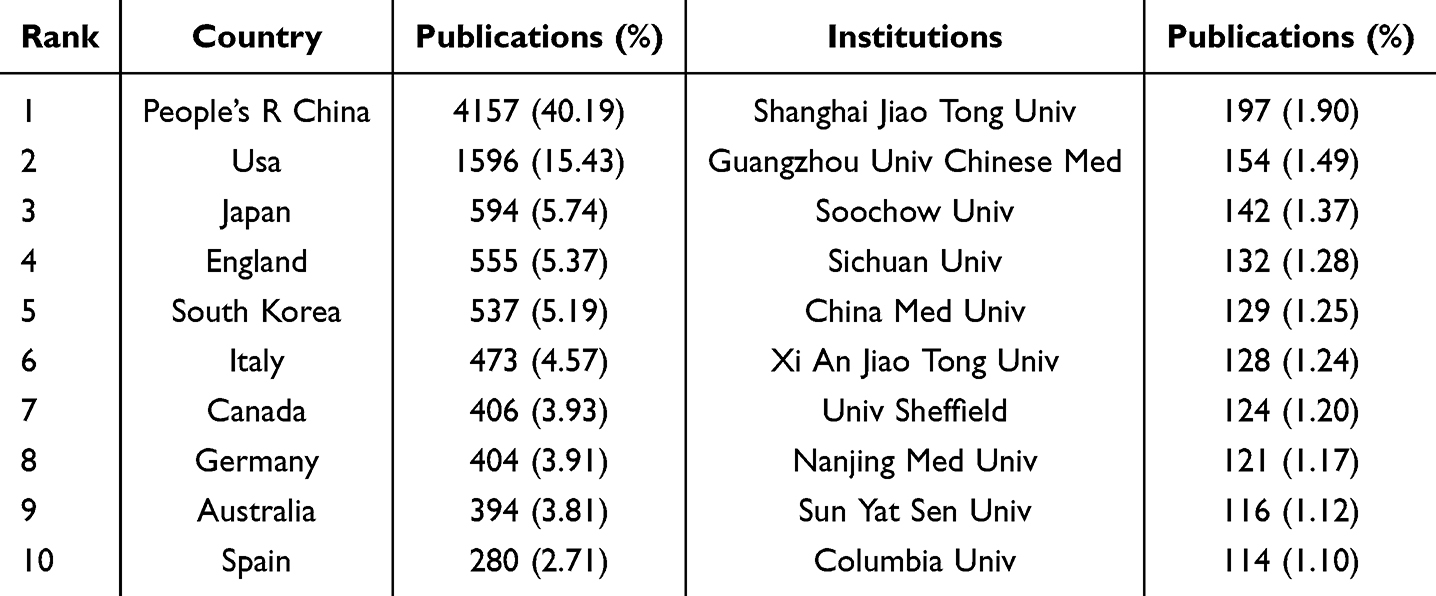 |
Table 1 Top 10 Productive Countries/Territories Listed by Level of Research Productivity |
 |
Figure 3 Co-occurrence maps (A) Countries/Territories; (B) Institutions. |
An examination of the institutions that have published research revealed that 9,462 were involved in research in this area, with 253 of them having published over 20 papers. Shanghai Jiao Tong University produced the most articles (n=197), then by Guangzhou University of Chinese Medicine (n=154), Soochow University (n=142), Sichuan University (n=132), and China Medical University (n=129). In addition, 80% of the leading 10 institutions based on the volume of published research papers are located in China. This statistic demonstrates the strong and dynamic collaboration among institutions within the country, which effectively leverages regional strengths and bolsters the academic influence of China in the field. The collaborative efforts among these institutions are illustrated in Figure 3B, while Table 1 lists the top ten institutions ranked by their publication output.
Productive Journals and Co-Cited Journals
An examination of journals and their co-citations was carried out to determine the journals that were most frequently published and co-cited in the area of osteoporosis. The software analysis revealed that 10,343 articles were published across 1,784 different academic journals. Table 2 lists the top 10 journals and co-cited journals associated with osteoporosis. The journal with the most publications was Osteoporosis International (n=611), followed by Archives of Osteoporosis (n=347), Frontiers in Endocrinology (n=218), Bone (n=195), and Journal of Bone and Mineral Metabolism (n=159). Among all the journals included, journals with more than five publications were selected for density mapping (Figure 4A) to show more clearly the high-yielding journals.
 |
Table 2 The Top 10 Osteoporosis-Associated Journals and the Co-Cited Journals |
 |
Figure 4 The density maps (A) Journals; (B) Co-cited journals. |
A total of 26,331 journals were cited, with 190 of them receiving over 400 citations each. The density map illustrated in Figure 4B highlights journals that have been co-cited more than 100 times. As indicated in Table 2, the journal cited the most was Osteoporosis Int (n=32,382), followed by the J Bone Miner Res (n=28,285), Bone (n=16,063), J Clin Endocr Metab (n=10,392), and New Engl J Med (n=7,838).
The organization of topics within academic journals is effectively depicted by the dual-map overlay of journals, which has cited journals on the right and citing journals on the left. The connections between citing and cited journals are depicted by colored pathways. As illustrated in Figure 5, the 5 key reference paths indicated that published studies in Molecular/Biology/Genetics, Health/Nursing/Medicine, and Sports/Rehabilitation/Sport journals were predominantly cited by Molecular/Biology/Immunology and Medicine/Medical/Clinical journals.
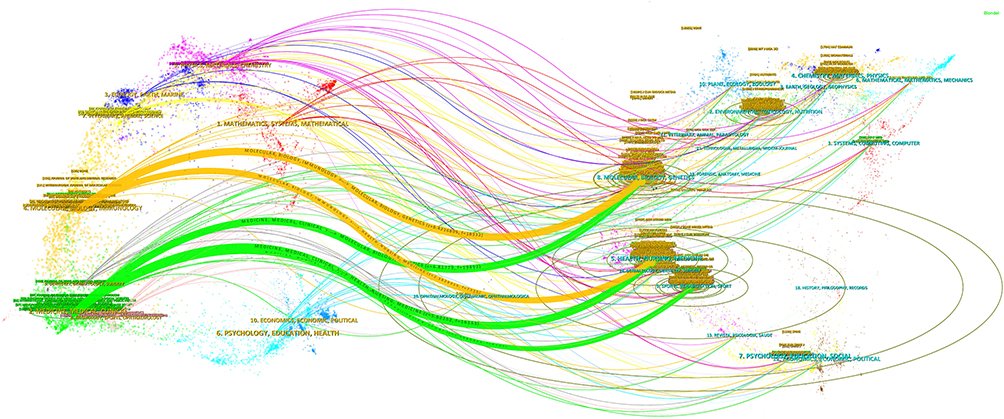 |
Figure 5 The dual-map overlay of journals related to osteoporosis. Notes: Left: the citing journals, Right: the cited journals. |
Authors and Cited Authors Analysis
According to the findings from the VOSviewer software, 45,966 authors published relevant literature on osteoporosis. Table 3 illustrates that Cooper Cyrus had the most publications (n=49), then Lewiecki E. Michael (n=44), Leslie William D (n=43), Reginster Jeanyves (n=38), and Zhang Lei (n=35). Additionally, applying a minimum threshold of 12 publications per author, a final count of 234 authors was chosen to create the network map. The findings illustrated in Figure 6A, which employed various colors to denote different clusters, indicated a strong link among these clusters. Additionally, strong collaborations in the same cluster were readily identifiable among authors, including pairs like Zhang Lei and Li Jie, Nakamura Toshitaka and Soen Satoshi, Lewiecki E Michael and Nieves Jeri W, as well as Cooper Cyrus and Reginster Jeanyves.
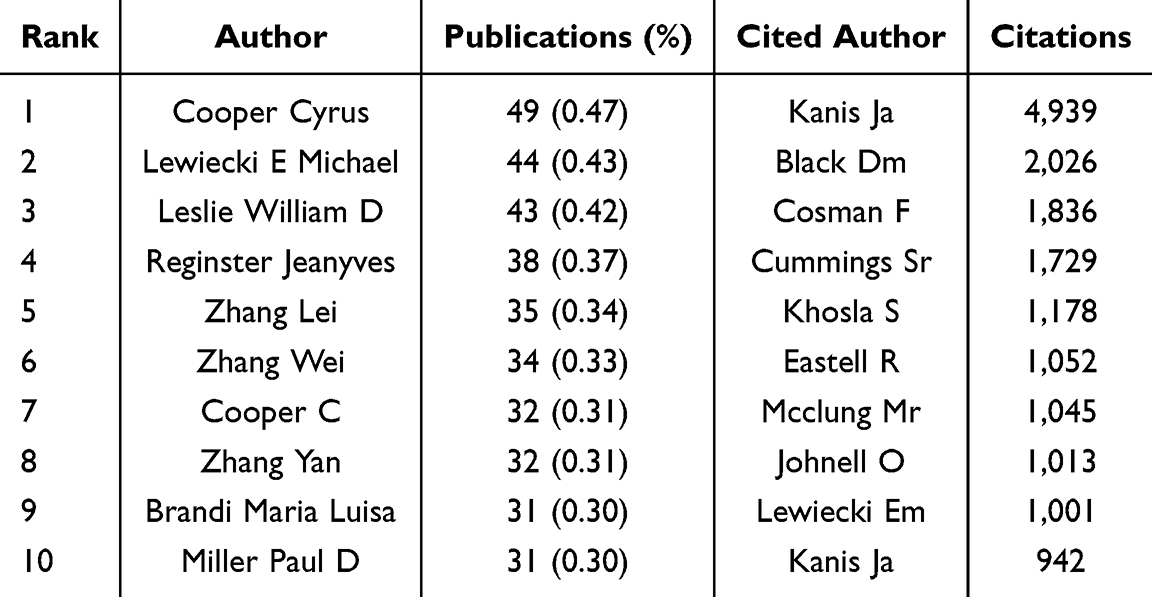 |
Table 3 Top 10 Authors by Count of Citations or Publications |
 |
Figure 6 The osteoporosis co-occurrence maps (A) Authors; (B) Co-authors. |
Two or more authors who have been referenced together in multiple studies are co-cited authors. We identified 124,905 co-authors in all, as shown in Figure 6B. According to the information presented in Table 3, each of the top ten authors received over 900 co-citations, with Kanis Ja being the most frequently cited (n=4,939), followed by Black Dm (n=2,026), Cosman F (n=1,836), Cummings Sr (n=1,729), and Khosla S (n=1,178). Furthermore, the density map includes 415 authors who have received more than 100 co-citations, effectively illustrating authors that are co-cited most frequently by using a spectrum of color.
Keyword Co-Occurrence, Clusters, and Evolution
Co-Occurrence of Keywords Analysis
In academic research, keywords are important words or concepts that represent the core focus and theoretical underpinnings of a study, aiding in discoverability and indexing.12 Consequently, by examining the keywords of a paper, we can gain insights into its themes and main arguments, as well as identify the current state of research and emerging trends.13 Utilizing VOSviewer software, a total of 21,309 keywords were identified. Among these, 216 keywords were found to appear more than 70 times, as shown in Figure 7A. The co-occurrence timeline diagram of keywords is shown in Figure 7B. The keyword “osteoporosis” ranked first (n=6,615), followed by “bone-mineral density” (n=2,668), “postmenopausal women” (n=1,710), “women” (n=1,560), “risk” (n=1,427), “fracture” (n=1,103), “bone” (n=982), “prevention” (n=855) and “postmenopausal osteoporosis” (n=814) using a frequency-based ranking. Illustration of the top 20 keywords in Table 4 according to frequency.
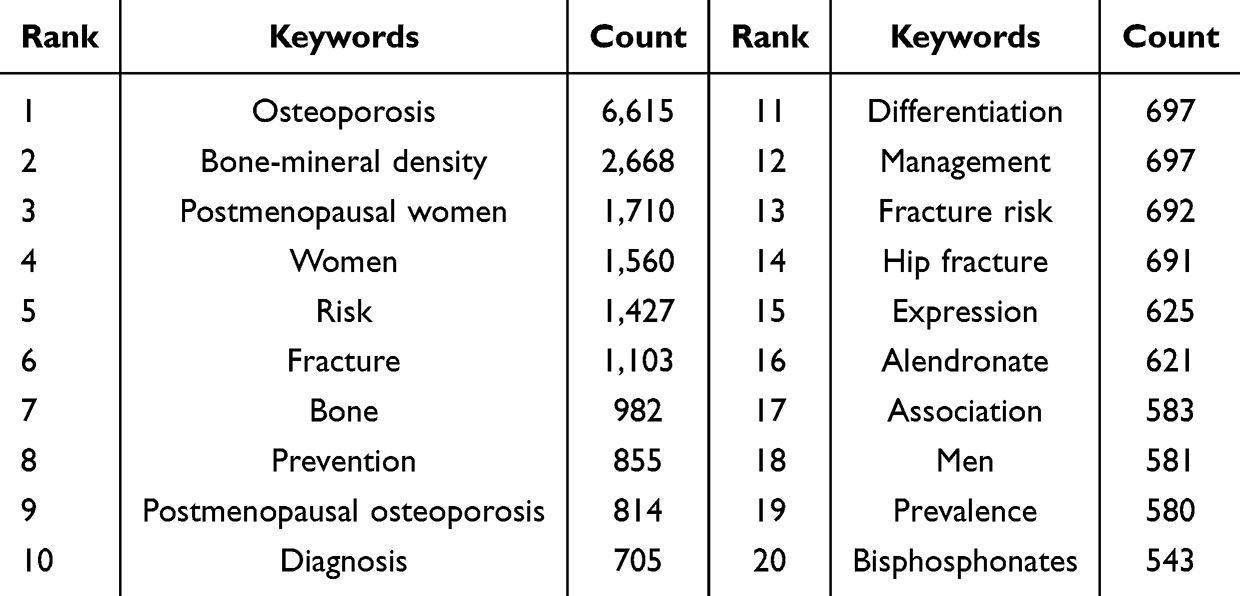 |
Table 4 The Top 20 Osteoporosis-Related Keywords |
 |
Figure 7 (A) Keyword co-occurrence network diagram of osteoporosis-related research; (B) Keyword co-occurrence timeline diagram. |
Keyword Cluster Analysis
The keyword clustering feature of CiteSpace assists readers in identifying the key research pathways in this field. Additionally, the cluster timeline map incorporates, providing a clearer visualization of the emergence and duration of each cluster, thereby effectively illustrating the evolution of each research direction. Figure 8A illustrates the application of the LLR method for categorizing keywords into thirteen distinct groups. Figure 8B provides a visual representation of the research focus and the evolutionary trajectory at each stage. Furthermore, Table 5 lists the representative keywords for each cluster. Our analysis revealed that the thirteen clusters encompassed four primary research directions. The first aspect was on the diagnosis and examination of osteoporosis, which included cluster #8 bone mineral density. The second aspect addressed the primary morbidity and complications associated with osteoporosis, which included cluster #5 obesity, #7 type 2 diabetes mellitus, and #11 glucocorticoid induced osteoporosis. The third aspect pertained to preventing and managing osteoporosis, which included Cluster #2 teriparatide,#4 fracture liaison service, and #9 vitamin d. Lastly, the fourth aspect examined the pathogenesis of osteoporosis, which included cluster #0 osteoclast, #1 osteogenic differentiation, #3 trabecular bone, #6 mendelian randomization, #10 cohort study, and #12 deep learning.
 |
Table 5 Keyword Clustering Data Sheet |
 |
Figure 8 The keywords of osteoporosis-related research cluster map (A) and cluster landscape map (B). |
Burst Keywords Analysis
The burst detection algorithm identifies changes in variables within a set time interval. By examining the burst detection of keywords, it is possible to understand the prevailing research trends at a given time and anticipate future research directions based on the persistence of these hotspots.14,15 The metric used to assess the intensity of citation surges is referred to as the intensity value; a higher value indicates a more significant surge. Figure 9 illustrates the top 30 keywords with the most pronounced citation burst. The intensity values for these keywords varied between 5.4 and 20.28, with burst durations spanning from 3 to 5 years. Notably, strontium ranelate recorded the highest intensity at 20.28. Keywords such as artificial intelligence, osteogenesis, network pharmacology, traditional Chinese medicine, molecular docking, cellular senescence, and bone targeting remain relevant today, indicating their significance in research now and in the future.
 |
Figure 9 Top 30 keywords with the highest frequency of citation bursts. |
Analysis of References
Figure 10A presents a map illustrating co-cited references. The paper by Cosman F, published in Osteoporosis Int in 2014, is the most frequently cited work. The ten most cited articles are organized as detailed in Table 6.3,16–24 Citation burst describes references that experience a high frequency of citations over an extended period. Figure 10B displays the top 30 references with the most significant burst values. Among the burst intensity results, Cosman F recorded the highest intensity at 120.7. Furthermore, Camacho PM, Compston JE, and Johnston CB have garnered significant attention.
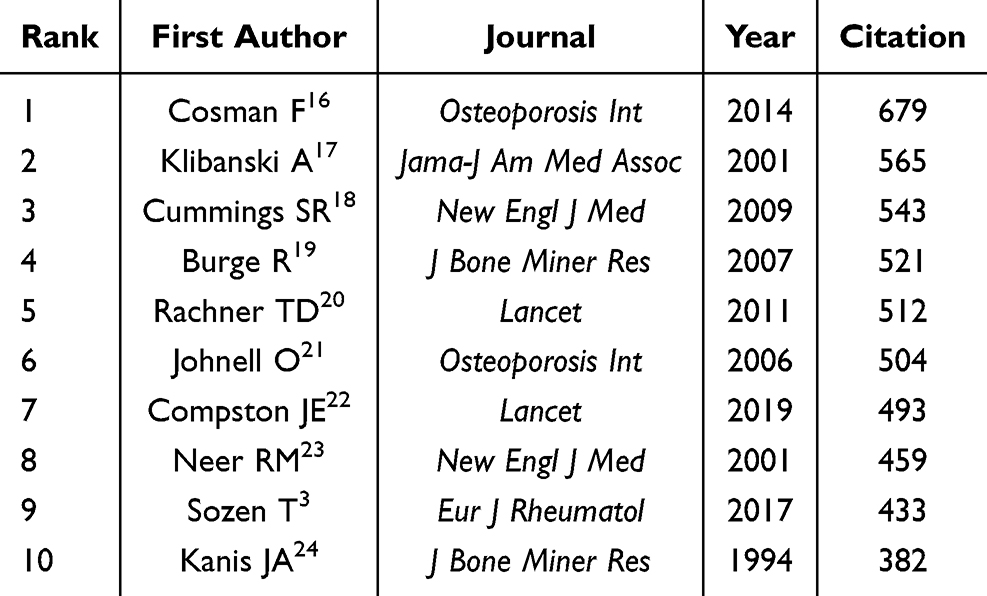 |
Table 6 Top 10 Most Cited Publications |
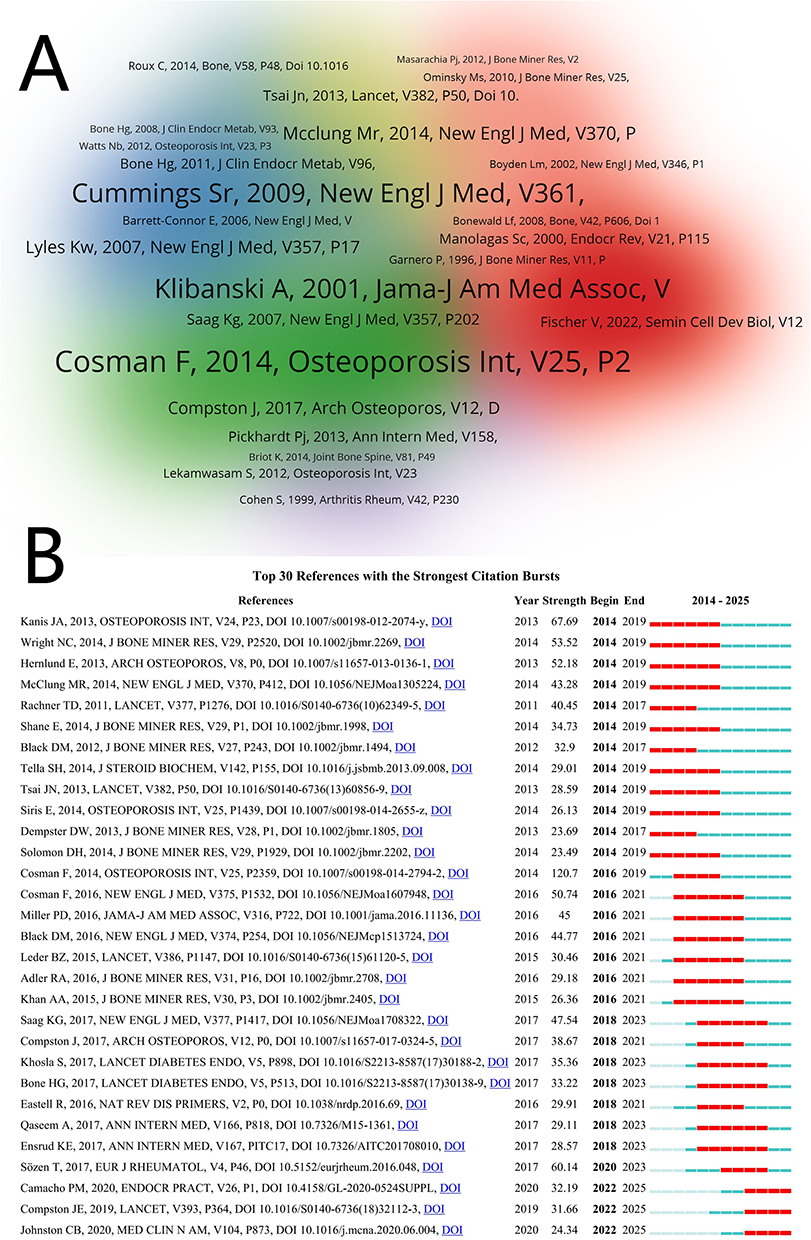 |
Figure 10 (A) Map of co-cited references. (B) Top 30 co-cited references with the most significant citation bursts.25–53 |
Discussion
General Information
Based on our screening criteria, 10,343 articles were identified. This collection includes contributions from 45,966 authors affiliated with 9,462 institutions in 102 countries and regions, ultimately resulting in the inclusion of 1,784 journals from the WoSCC and PubMed databases.
Through the application of bibliometrics and visual analysis techniques to examine relevant literature, we observed a consistent rise in publication numbers in osteoporosis from 2014 to 2025, particularly in the most recent years. This trend suggests that researchers have been interested in this area before 2014, and it continues to be a significant contemporary research topic. As more comprehensive studies are published, the volume of literature will continue to rise; however, numerous critical scientific challenges remain to be addressed. Consequently, this area remains a promising research hotspot that warrants further investment in manpower, material, and financial resources.
Examining the distribution and collaboration among nations, regions, and institutions can enhance global cooperation. In this study, China was determined to have the largest volume of publications, then the USA, Japan, England, and South Korea. Shanghai Jiao Tong University was ranked as the institution with the most publications, then Guangzhou University of Chinese Medicine, Soochow University, Sichuan University, and China Medical University. The primary research contributors in this field are scholars from China and the United States, who are recognized for having the most significant and impactful studies on osteoporosis. This prominence may be attributed to factors such as economic advancement, a higher level of scientific inquiry, financial backing, and the availability of skilled personnel in these countries. Additionally, from the map, we can observe that China established significant and extensive collaborations with other countries. Key institutions such as Shanghai Jiao Tong University, the University of Sheffield, Seoul National University, and the University of Toronto form the foundation of these cooperative efforts. However, the level of overall collaboration remains insufficient. Consequently, it is crucial to remove academic obstacles and cultivate more profound and extensive collaborations and exchanges between nations and institutions to advance this field and enhance clinical care for a larger patient population.
Analyzing journals and major publications can aid researchers in identifying the most appropriate journal for submission. Osteoporosis International journal emerged as the leading journal with the largest publications (n=611) as well as the most co-citations (n=32,382). Furthermore, the findings from the journal double atlas superposition revealed that articles in Molecular/Biology/Genetics, Health/Nursing/Medicine, and Sports/Rehabilitation/Sport were predominantly referenced by journals centered on Molecular/Biology/Immunology and Medicine/Medical/Clinical disciplines. This suggests that the investigations in this area are chiefly oriented towards basic studies and translational medicine. Moreover, highlighting authors who have a significant number of co-published or co-cited works within a specific field can help in identifying the intellectual structure of the research field. By conducting an analysis, additional insights regarding potential collaborators and influential research teams can be made available. From our investigation, Cooper Cyrus was the most published author (n=49) and Kanis Ja was the most co-cited author (n=4,939), as Table 3 demonstrates, suggesting that they have the potential to make significant contributions to the field.
The Hotspots and Frontiers
Analyzing the co-occurrence of keywords in bibliometric data can reveal hotspots and potential directions within a specific research field by identifying frequently used and related terms. According to the information presented in Table 4. The top 20 high-frequency keywords associated with osteoporosis included bone mineral density, postmenopausal women, risk, fracture, bone, and prevention. These key words reflect the research trends and key contents in this field. Therefore, we further summarize, sort out and analyze these key words. This paper elaborates on the hot directions and trends in this research field from multiple aspects and provides examples, hoping to offer reference and inspiration for future researchers.
Study on Risk Factors and Clinical Diagnosis
Osteoporosis is a prevalent public health issue in China, specifically affecting women and the elderly.54 The investigation of risk factors and clinical diagnosis related to osteoporosis is currently a significant area of research and a prominent topic of interest. Keywords associated with this field include bone mineral density, diagnosis, computed tomography, biochemical markers, quantitative ultrasound, x-ray absorptiometry, postmenopausal women, risk factors, and ovariectomy.
Osteoporosis, characterized by weakened bones and increased fracture risk, can stem from various factors, including hormonal changes, bad habits, genetic predispositions, and certain medical conditions or medications.55,56 These factors directly and indirectly disrupt bone remodeling by affecting osteoclasts (bone-resorbing cells) and osteoblasts (bone-forming cells), ultimately reducing bone quality.55 Risk factors for osteoporosis are categorized into modifiable and non-modifiable groups. Lifestyle habits and long-term use of glucocorticoids fall under the modifiable group, whereas genetic traits and race fall under the non-modifiable group.55 Osteoporosis was further positively correlated with several factors, including marital status, current smoking habits, being underweight, having a history of hypertension, a history of fractures, an extended duration of menopause, and the occurrence of menopause itself.54
Vitamin deficiencies are linked to an elevated likelihood of developing osteoporosis by epidemiological research investigations, indicating that vitamins are beneficial for bone health when taken within biological constraints.57 Glucocorticoid therapy is a significant contributor to skeletal and endocrine complications.58 Evidence suggests that kynurenines may serve as potential biomarkers for osteoporosis, sarcopenia, osteosarcopenia, and frailty in the elderly.59 In numerous clinical and preclinical studies related to osteoporosis, the ketogenic diet has shown harmful effects by hindering bone formation and compromising bone microarchitecture.60
New methods of diagnosing and evaluating osteoporosis have been made possible by recent advancements in medical imaging, particularly CT scans.61 Patients who are suspected of having osteoporosis, whether due to fragility fractures or low bone mineral density (BMD) as assessed by Dual-energy X-ray absorptiometry (DXA), should undergo an assessment to exclude secondary causes.62,63 Current evidence indicates that incorporating Trabecular Bone Score (TBS) alongside BMD and clinical risk factors improves fracture risk probability in both primary and secondary osteoporosis, aiding the initiation and therapy selection for osteoporosis.64 It is important to note that a DXA machine cannot differentiate between low BMD resulting from osteoporosis and that caused by osteomalacia; therefore, clinicians must conduct a thorough evaluation along with relevant laboratory tests.65 The trabecular bone score is a predictor of hip fractures and significant osteoporotic fractures, functioning at least in part independently of BMD and clinical risk factors.64
Study on Pathogenesis and Targets
The pathogenesis of osteoporosis is extremely complex, involving oxidative stress and inflammation, and disruptions in apoptosis and hormone metabolism, resulting in bone loss and elevated fracture risk. A thorough investigation into the pathogenesis and mechanisms of the disease is crucial for preventing and treating the disease. The research focus of keywords such as bone loss, oxidative stress, inflammation, apoptosis, calcium, osteoblast, osteoclast, metabolism, mechanisms, and trabecular bone can help establish the trajectory of research, find research gaps, and aid in the development of its therapy.
Oxidative stress is identified as a major contributor to the onset of osteoporosis. Along with mitochondrial dysfunction, they can negatively influence cellular behavior and outcomes, thereby participating in osteoporosis development.66 Moreover, oxidative stress triggers apoptosis of osteocytes and alters the levels of specific factors, including receptor activator κB ligand (RANKL), sclerostin, and, as recent studies suggest, fibroblast growth factor. This disruption leads to impaired bone remodeling and elevated bone resorption.67 Additionally, Studies indicate that ferroptosis, a type of cell death, substantially participates in the development of diabetes osteoporosis, postmenopausal osteoporosis, and glucocorticoid-induced osteoporosis.68
In his review, Fang69 explored the existing insights into how extracellular vesicles (EVs) influence bone homeostasis, detailing their classification, biogenesis, and the complex regulatory functions in osteoporosis. The study determined that EVs originating from different sources have varying impacts on osteoporosis. Particularly, EVs produced by osteoblasts, endothelial cells, myocytes, and mesenchymal stem cells facilitate bone formation through their specific cargo of proteins, miRNAs, and cytokines. In contrast, EVs released by osteoclasts and immune cells enhance bone resorption and suppress bone development.69 According to earlier research,70 normal bone remodeling is reliant on proteostasis. However, the deterioration of proteostasis associated with aging results in a dysfunctional proteostasis network (PN), which is unable to sustain bone homeostasis.70 According to Amroodi, bone remodeling involves the Wnt, Notch, JAK/STAT, NF-κB, and TGF-β signaling pathways, and disruption of these pathways contributes to osteoporosis.71 Notably, the Wnt/β-catenin signaling pathway is recognized as a primary mechanism in osteoblast differentiation and a vital therapeutic avenue for osteoporosis.72
The imbalance between osteoblasts and osteoclasts is a crucial contributor to the onset of osteoporosis.73 B-lymphocytes, traditionally recognized for participating in adaptive humoral immunity, are identified as significant regulators of bone remodeling. They use a variety of cytokines, such as RANK, OPG, and IL-7, to interact with osteoclasts and osteoblasts.74 During inflammation, B-lymphocytes facilitate the activation and differentiation of osteoclasts.74 Conversely, they also exhibit immunomodulatory functions, with regulatory B-lymphocytes (Bregs) producing TGF-β1 to inhibit harmful osteoclastogenesis.74 Additionally, neutrophils, the most abundant type of leukocyte in the body, participate in the proinflammatory environment that contributes to osteoporotic changes in bone structure.74
The feedback loop in the endocrine system works to control the release of hormones and maintain the homeostasis of metabolism, thereby regulating the function of target organs.75 The breakdown of this feedback loop results in various endocrine and metabolic disorders, such as osteoporosis, type II diabetes, and hyperlipidemia.75 Numerous studies have confirmed that m(6)A is essential for bone marrow mesenchymal stem cells (BMSCs), osteoblasts, and osteoclasts to proliferate, differentiate, migrate, invade, and repair. These processes all affect the entire pathophysiology of osteoporosis.76
Study on Primary Morbidity and Complications
There are two main classifications of osteoporosis: primary and secondary. Primary osteoporosis is largely connected to the aging process.77 Osteoporosis that arises from underlying medical conditions or the use of medications is categorized as secondary osteoporosis.77,78 This disease is associated with numerous primary morbidities and complications. A thorough diagnosis and treatment addressing both the symptoms and underlying causes present significant challenges that merit extensive investigation and analysis. Keywords relevant to this area of research include obesity, sarcopenia, chronic obstructive pulmonary disease, breast cancer, estrogen deficiency, type 2 diabetes mellitus, rheumatoid arthritis, hip fractures, vertebral fractures, osteoarthritis, and osteonecrosis.
The primary outcome of osteoporosis is an elevated likelihood of bone fractures, which can result in disability, persistent pain, and potentially early mortality, especially among older adults.79,80 Osteoporotic fractures adversely influence quality of life and are linked to severe complications such as pneumonia, skin infections, and sepsis.81 Jiao82 conducted a comprehensive study that revealed an important link between indicators of obesity and BMD, providing important perspectives into the intricate link between obesity and bone health. Despite this, the relationship between obesity and osteoporosis is multifaceted, indicating that further research into the molecular mechanisms involved is essential.83
Numerous conditions associated with lipid metabolism disorders, like nonalcoholic fatty liver disease, atherosclerosis, obesity, and menopause, are associated with osteoporotic phenotypes.84 Liver injury induced by different liver diseases can cause an imbalance in bone metabolism, indicating a novel regulatory paradigm between the liver and bone.85 Nevertheless, little is known about how the liver-bone axis contributes to primary and secondary osteoporosis.85 The rates of osteopenia and osteoporosis are notably high in individuals with chronic pancreatitis, which may elevate the likelihood of fracture occurrence.86
Earlier research has indicated that osteoporosis may result as a side effect of breast cancer treatment, although the precise mechanisms involved are largely unknown.87 It can also be a chronic complication of diabetes mellitus.88 Moreover, individuals with Gaucher disease often experience various bone manifestations, including osteopenia/osteoporosis, and osteonecrosis.89 Additionally, in individuals with beta-thalassaemia, osteoporosis substantially contributes to morbidity and arises from various factors.90 First, a decrease in trabecular bone tissue with cortical thinning results from bone marrow expansion brought on by ineffective erythropoiesis. Second, excessive iron loading raises bone turnover by causing endocrine dysfunction. Finally, a decrease in optimal bone mineralization may follow physical inactivity brought on by disease complications.90
Study on Early Prevention and Clinical Treatment
The treatment of osteoporosis is a comprehensive process that mainly includes lifestyle adjustments, basic supplements, and medications. It is crucial for patients to adhere to a nutritious diet that includes foods high in calcium and sufficient protein, engage in moderate physical activity, and refrain from smoking while limiting alcohol consumption. Furthermore, calcium and vitamin D are frequently recommended as dietary supplements. Pharmacotherapy plays a vital role in treatment, with options including bisphosphonates, denosumab, teriparatide, baricitinib, and romosozumab. In addition, traditional Chinese medicine such as Jintiange capsule, Qianggu capsule can also be effective. For patients on long-term treatment, a sequential treatment pattern, such as teriparatide sequential bisphosphonate, or disumab, is important to effectively improve bone mineral density and reduce fracture risk. The representative keywords of this research direction include teriparatide, denosumab, bisphosphonates, hormone replacement therapy, zoledronic acid, alendronate, and traditional Chinese medicine.
A study assessed the effectiveness and safety of a denosumab biosimilar, QL1206 (60 mg), in comparison to a placebo among postmenopausal Chinese women suffering from osteoporosis and an elevated likelihood of fractures.91 The findings indicated that QL1206 significantly enhanced the bone mineral density (BMD) in the lumbar spine, total hip, femoral neck, and trochanter relative to the placebo, while also facilitating the rapid decline in the indicators of bone turnover.91 Continued investigation into the creation of targeted ligands and nanocarriers may increase the potential for osteoporosis-targeted treatments to be used in clinical settings.92
In women with osteoporosis with an elevated likelihood of fracture, weekly injections of teriparatide, followed by alendronate, led to substantially lower incidence of morphometric vertebral fractures than alendronate monotherapy.93 A regimen of monthly subcutaneous romosozumab at 210 mg for 12 months, then by 24 months of open-label weekly oral alendronate at 70 mg (romosozumab-to-alendronate), substantially lowered the fracture risk relative to 36 months of alendronate treatment alone in postmenopausal women with osteoporosis and before fracture.94
Treatments aimed at altering gut microbiota, like the use of probiotics or antibiotics, are shown to influence bone remodeling.95,96 Lyu95 investigated the effectiveness of probiotics as a treatment strategy for osteoporosis. The findings may aid in the creation of novel therapies aimed at the gut microbiota for managing osteoporosis. Natural products made from a wide range of food ingredients and medicinal plants have been shown in previous studies to modulate programmed cell death through various mechanisms. These products have great potential for osteoporosis prevention and treatment, demonstrating the rise of more widely accepted complementary and alternative medicines that are less expensive, have fewer adverse effects, and work for longer.97 In the academic field, mesenchymal stem cell-derived EVs are emerging as promising therapeutic approaches for osteoporosis, and engineered strategies can enhance their therapeutic effects.98 Several clinical trials and epidemiological research indicate that supplementing with zinc (Zn), magnesium (Mg), fluoride (F), and strontium (Sr)may enhance bone quality and possibly lower the risk of developing osteoporosis.99
According to a number of studies, antioxidants may be incorporated into innovative treatment methods to improve avenues for managing and preventing osteoporosis and bone diseases associated with oxidative stress.67 Specifically, compounds like anthocyanins, resveratrol, lycopene, oleuropein, some vitamins, and thiol antioxidants may be efficacious against osteoporosis.67 By increasing PDLF and the activity of osteoblasts, inhibiting osteoclast participation, increasing chondrocyte production in the cartilage matrix, and reducing the degradation of connective tissue, ginsenosides may provide positive effects.100 Preclinical research employing animal models has shown their effectiveness in boosting bone density, reducing the symptoms of osteoarthritis, and improving periodontitis.100
Strengths and Limitations
Accurate diagnosis and treatment of osteoporosis are crucial for global research and clinical practice. Employing CiteSpace analysis offers a more effective means of identifying research priorities and trends than conventional review methods.
However, it also presents specific limitations. CiteSpace cannot fully substitute for system retrieval. Firstly, the literature data gathered is incongruent, undermining the reliability of the atlas visualization. Secondly, differences in the volume of articles included and the retrieval outcomes could result from different data updates. Nonetheless, literature analysis through visualization offers significant benefits by enhancing comprehension of the most authoritative works within the research field, and it can also lay the groundwork for future studies.
Conclusion
This study used CiteSpace and VOSviewer software to visualize and bibliometrically analyze 10,343 publications on osteoporosis. The increasing number of publications each year suggests growing interest and significant research potential in this field. China and the United States have been the primary contributors in this field of research; however, it is essential to strengthen collaborations among various countries, regions, and institutions to collectively advance development and progress in this area. The central focus of the study has been to address the prevention of osteoporosis, as well as accurate diagnosis and treatment.
Data Sharing Statement
The article contains the original contributions of this study. For any further inquiries, please get in touch with the corresponding authors.
Acknowledgments
The authors express their gratitude to the Second Affiliated Hospital of Hunan University of Chinese Medicine for its assistance with this research, as well as to the editors and reviewers for their insightful feedback and approval to enhance the manuscript.
Funding
This work was supported by the Key Plans of Hunan Administration of Traditional Chinese Medicine Research Program Project, China (Grant No. A2024032), Hunan Clinical Research Center of Bone Injury of Traditional Chinese Medicine, China (Grant No. 2020SK4013).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yang J, Jiang T, Xu G, et al. Bibliometrics analysis and visualization of sarcopenia associated with osteoporosis from 2000 to 2022. J Pain Res. 2023;16:821–837. doi:10.2147/JPR.S403648
2. Zhivodernikov IV, Kirichenko TV, Markina YV, et al. Molecular and cellular mechanisms of osteoporosis. Int J Mol Sci. 2023;24(21):15772. doi:10.3390/ijms242115772
3. Sozen T, Ozisik L, Basaran NC. An overview and management of osteoporosis. Euro J Rheumatol. 2017;4(1):46–56. doi:10.5152/eurjrheum.2016.048
4. Shen Y, Huang X, Wu J, et al. The global burden of osteoporosis, low bone mass, and its related fracture in 204 countries and territories, 1990-2019. Front Endocrinol. 2022;13:882241. doi:10.3389/fendo.2022.882241
5. Adejuyigbe B, Kallini J, Chiou D, et al. Osteoporosis: molecular pathology, diagnostics, and therapeutics. Int J Mol Sci. 2023;24(19):14583. doi:10.3390/ijms241914583
6. Rashki Kemmak A, Rezapour A, Jahangiri R, et al. Economic burden of osteoporosis in the world: a systematic review. Med J Islam Repub Iran. 2020;34:154. doi:10.34171/mjiri.34.154
7. Wang H, Luo Y, Wang H, et al. Mechanistic advances in osteoporosis and anti-osteoporosis therapies. MedComm. 2023;4(3):e244. doi:10.1002/mco2.244
8. Liu J, Xu D, Liu L, et al. Regular sling core stabilization training improves bone density based on calcium and vitamin D supplementation. BMC Musculoskelet Disord. 2023;24(1):815. doi:10.1186/s12891-023-06896-8
9. Lian K, Li X, Wang XY, et al. A bibliometric and visual analysis of research trends and hotspots of myocardial apoptosis: a review. Medicine. 2023;102(38):e35236. doi:10.1097/MD.0000000000035236
10. Tao Z, Wang F, Jiang Z, et al. A bibliometric analysis of hepatolenticular degeneration research in traditional Chinese medicine using CiteSpace and VOSviewer: a study protocol for systematic review. Medicine. 2024;103(49):e40781. doi:10.1097/MD.0000000000040781
11. Li Z, Xiong Q, Li S, et al. Quantitative analysis and visualization of literature on acupuncture and related TCM therapies for the treatment of colorectal cancer based on CiteSpace. Front Oncol. 2023;13:1290588. doi:10.3389/fonc.2023.1290588
12. Ma K, Luo C, Du M, et al. Advances in stem cells treatment of diabetic wounds: a bibliometric analysis via CiteSpace. Skin Res Technol. 2024;30(4):e13665. doi:10.1111/srt.13665
13. Xu CJ, Li X. Research trends in the early diagnosis of ovarian cancer during 2001-2020: a bibliometric analysis. Eu J Gynaecol Oncol. 2022;43(2):321–334.
14. Ai YZ, Xing YX, Yan LM, et al. Atrial fibrillation and depression: a bibliometric analysis from 2001 to 2021. Front Cardiovas Med. 2022;9. doi:10.3389/fcvm.2022.775329
15. Hand DJ, Keim DA, Ng R. Special issue: selected papers from the eighth ACM SIGKDD international conference on knowledge discovery and data mining - part. Data Mining Know Discover. 2003;7(3):239–240. doi:10.1023/A:1024041103148
16. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporosis Int. 2014;25(10):2359–2381. doi:10.1007/s00198-014-2794-2
17. Klibanski A, Adams-Campbell L. Osteoporosis prevention, diagnosis, and therapy. JAMA J Am Med Assoc. 2001;285(6):785–795. doi:10.1001/jama.285.6.785
18. Cummings SR, San Martin J, McClung MR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361(8):756–765. doi:10.1056/NEJMoa0809493
19. Burge R, Dawson-Hughes B, Solomon DH, et al. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Mineral Res. 2007;22(3):465–475. doi:10.1359/jbmr.061113
20. Rachner TD, Khosla S, Hofbauer LC. Osteoporosis: now and the future. Lancet. 2011;377(9773):1276–1287. doi:10.1016/S0140-6736(10)62349-5
21. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Inter. 2006;17(12):1726–1733.
22. Compston JE, McClung MR, Leslie WD. Osteoporosis. LANCET. 2019;393(10169):364–376. doi:10.1016/S0140-6736(18)32112-3
23. Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):1434–1441. doi:10.1056/NEJM200105103441904
24. Kanis JA, Melton LJ, Christiansen C, et al. The diagnosis of osteoporosis. J Bone Mineral Res. 1994;9(8):1137–1141. doi:10.1002/jbmr.5650090802
25. Kanis JA, McCloskey EV, Johansson H, Cooper C, Rizzoli R, Reginster JY. Scientific advisory board of the European society for clinical and economic aspects of osteoporosis and osteoarthritis (esceo) and the committee of Scientific advisors of the International osteoporosis foundation (iof). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2013;24(1):23–57. doi:10.1007/s00198-012-2074-y
26. Wright NC, Looker AC, Saag KG, et al. The recent prevalence of osteoporosis and low bone mass in the United States based on bone mineral density at the femoral neck or lumbar spine. J Bone Min Res. 2014;29(11):2520–2526. doi:10.1002/jbmr.2269
27. Hernlund E, Svedbom A, Ivergård M, et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International osteoporosis foundation (iof) and the European federation of pharmaceutical industry associations (EFPIA). Arch Osteoporos. 2013;8(1):136. doi:10.1007/s11657-013-0136-1
28. McClung MR, Grauer A, Boonen S, et al. Romosozumab in postmenopausal women with low bone mineral density. N Engl J Med. 2014;370(5):412–420. doi:10.1056/NEJMoa1305224
29. Rachner TD, Khosla S, Hofbauer LC Osteoporosis: now and the future. Lancet. 2011;377. doi:10.1016/S0140-6736(10)62349-5...
30. Shane E, Burr D, Abrahamsen B, et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone Min Res. 2014;29(1):1–23. doi:10.1002/jbmr.1998
31. Black DM, Reid IR, Boonen S, et al. The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal fracture trial (PFT). J Bone Min Res. 2012;27(2):243–254. doi:10.1002/jbmr.1494
32. Tella SH, Gallagher JC Prevention and treatment of postmenopausal osteoporosis. J Steroid Biochem Mol Biol. 2014;142:155–170. doi:10.1016/j.jsbmb.2013.09.008
33. Tsai JN, Uihlein AV, Lee H, et al. Teriparatide and denosumab, alone or combined, in women with postmenopausal osteoporosis: the data study randomised trial. Lancet. 2013;382(9886):50–56. doi:10.1016/S0140-6736(13)60856-9
34. Dempster DW, Compston JE, Drezner MK, et al. Standardized nomenclature, symbols, and units for bone histomorphometry: a 2012 update of the report of the ASBMR histomorphometry nomenclature committee. J Bone Min Res. 2013;28(1):2–17. doi:10.1002/jbmr.1805
35. Solomon DH, Johnston SS, Boytsov NN, McMorrow D, Lane JM, Krohn KD Osteoporosis medication use after hip fracture in U.S. patients between 2002 and 2011. J Bone Min Res. 2014;29(9):1929–1937. doi:10.1002/jbmr.2202
36. Cosman F, de Beur SJ, LeBoff MS, et al. National osteoporosis foundation. Clinician’s Guide to prevention and treatment of osteoporosis. Osteoporos Int. 2014;25(10):2359–2381. doi:10.1007/s00198-014-2794-2
37. Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med. 2016;375(16):1532–1543. doi:10.1056/NEJMoa1607948
38. Miller PD, Hattersley G, Riis BJ, et al. Active study investigators. Effect of Abaloparatide vs placebo on new vertebral fractures in postmenopausal women with osteoporosis: a randomized clinical trial. JAMA. 2016;316(7):722–733. doi:10.1001/jama.2016.11136
39. Black DM, Rosen CJ Clinical Practice. Postmenopausal Osteoporosis. N Engl J Med. 2016;374(3):254–262. doi:10.1056/NEJMcp1513724
40. Leder BZ, Tsai JN, Uihlein AV, et al. Denosumab and teriparatide transitions in postmenopausal osteoporosis (the DATA-Switch study): extension of a randomised controlled trial. Lancet. 2015;386. doi:10.1016/S0140-6736(15)61120-5
41. Adler RA, El-Hajj Fuleihan G, Bauer DC, et al. Managing osteoporosis in patients on long-term bisphosphonate treatment: report of a task force of the American society for Bone and mineral research. J Bone Min Res. 2016;31(1):16–35. doi:10.1002/jbmr.2708
42. Khan AA, Hanley DA, Felsenberg D, et al. International task force on osteonecrosis of the jaw. Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Min Res. 2015;30(1):3–23. doi:10.1002/jbmr.2405
43. Saag KG, Petersen J, Brandi ML, et al. Romosozumab or alendronate for fracture prevention in women with osteoporosis. n Engl J Med. 2017;377(15):1417–1427. doi:10.1056/NEJMoa1708322
44. Compston J, Cooper A, Copper C, et al. National Osteoporosis Guideline Group (NOGG). Uk clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos. 2017;12(1):43. doi:10.1007/s11657-017-0324-5
45. Khosla S, Hofbauer LC Osteoporosis treatment: recent developments and ongoing challenges. Lancet Diabetes Endocrinol. 2017;5(11):898–907. doi:10.1016/S2213-8587(17)30188-2
46. Bone HG, Wagman RB, Brandi ML, et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomised freedom trial and open-label extension. Lancet Diabetes Endocrinol. 2017;5(7):513–523. doi:10.1016/S2213-8587(17)30138-9
47. Eastell R, O’Neill TW, Hofbauer LC, et al. Postmenopausal osteoporosis. nat Rev Dis Primers. 2016;2:16069. doi:10.1038/nrdp.2016.69
48. Qaseem A, Forciea MA, McLean RM, et al. Treatment of low bone density or osteoporosis to prevent fractures in men and women: a clinical practice guideline update from the American college of physicians. Ann Intern Med. 2017;166(11):818–839. doi:10.7326/M15-1361
49. Ensrud KE, Crandall CJ Osteoporosis. Ann Intern Med. 2017;167(3). doi:10.7326/AITC201708010
50. Sözen T, Özışık L, Başaran NÇ An overview and management of osteoporosis. Eur J Rheumatol. 2017;4(1):46–56. doi:10.5152/eurjrheum.2016.048
51. Camacho PM, Petak SM, Binkley N, et al. American association of clinical ENDOCRINOLOGISTS/AMERICAN college of endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal OSTEOPOROSIS-2020 update. Endocr Pract. 2020;26(Suppl 1). doi:10.4158/GL-2020-0524SUPPL..
52. Compston JE, McClung MR, Leslie WD Osteoporosis. Lancet. 2019;393(10169):364–376. doi: 10.1016/S0140-6736(18)32112-3.
53. Johnston CB, Dagar M Osteoporosis in Older Adults. Med Clin N Am. 2020;104(5):873–884. doi:10.1016/j.mcna.2020.06.004
54. Liu Y, Huang X, Tang K, et al. Prevalence of osteoporosis and associated factors among Chinese adults: a systematic review and modelling study. J Glob Health. 2025;15:04009. doi:10.7189/jogh.15.04009
55. Stromsnes K, Fajardo CM, Soto-Rodriguez S, et al. Osteoporosis: causes, mechanisms, treatment and prevention: role of dietary compounds. Pharmaceuticals. 2024;17(12):1697. doi:10.3390/ph17121697
56. Cao G, Hu S, Ning Y, et al. Traditional Chinese medicine in osteoporosis: from pathogenesis to potential activity. Front Pharmacol. 2024;15:1370900. doi:10.3389/fphar.2024.1370900
57. Skalny AV, Aschner M, Tsatsakis A, et al. Role of vitamins beyond vitamin D(3) in bone health and osteoporosis. Int J Mol Med. 2024;53(1):9. doi:10.3892/ijmm.2023.5333
58. Ward LM, Bakhamis SA, Koujok K. Approach to the pediatric patient with glucocorticoid-induced osteoporosis. J Clin Endocrinol Metab. 2025;110(2):572–591. doi:10.1210/clinem/dgae507
59. Ballesteros J, Rivas D, Duque G. The role of the kynurenine pathway in the pathophysiology of frailty, sarcopenia, and osteoporosis. Nutrients. 2023;15(14):3132. doi:10.3390/nu15143132
60. Luo C, Dai Z, He W, et al. Ketogenic diet and β-hydroxybutyrate in osteoporosis: current progress and controversy. Front Nutr. 2025;12:1508695. doi:10.3389/fnut.2025.1508695
61. Ong W, Liu RW, Makmur A, et al. Artificial intelligence applications for osteoporosis classification using computed tomography. Bioengineering. 2023;10(12):1364. doi:10.3390/bioengineering10121364
62. Mirza F, Canalis E. Management of endocrine disease: secondary osteoporosis: pathophysiology and management. Eur J Endocrinol. 2015;173(3):R131–51. doi:10.1530/EJE-15-0118
63. Camacho PM, Petak SM, Binkley N, et al. American association of clinical endocrinologists and American college of endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis - 2016 - executive summary. Endocr Pract. 2016;22(9):1111–1118. doi:10.4158/EP161435.ESGL
64. Shevroja E, Reginster JY, Lamy O, et al. Update on the clinical use of trabecular bone score (TBS) in the management of osteoporosis: results of an expert group meeting organized by the European society for clinical and economic aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO), and the international osteoporosis foundation (IOF) under the auspices of WHO collaborating center for epidemiology of musculoskeletal health and aging. Osteoporos Int. 2023;34(9):1501–1529. doi:10.1007/s00198-023-06817-4
65. Sabri SA, Chavarria JC, Ackert-Bicknell C, et al. Osteoporosis: an update on screening, diagnosis, evaluation, and treatment. Orthopedics. 2023;46(1):e20–e26. doi:10.3928/01477447-20220719-03
66. Riegger J, Schoppa A, Ruths L, et al. Oxidative stress as a key modulator of cell fate decision in osteoarthritis and osteoporosis: a narrative review. Cell Mol Biol Lett. 2023;28(1):76. doi:10.1186/s11658-023-00489-y
67. Marcucci G, Domazetovic V, Nediani C, et al. Oxidative stress and natural antioxidants in osteoporosis: novel preventive and therapeutic approaches. Antioxidants. 2023;12(2):373. doi:10.3390/antiox12020373
68. Wu X, Fang X, Lu F, et al. An update on the role of ferroptosis in the pathogenesis of osteoporosis. EFORT Open Rev. 2024;9(8):712–722. doi:10.1530/EOR-23-0148
69. Fang F, Yang J, Wang J, et al. The role and applications of extracellular vesicles in osteoporosis. Bone Res. 2024;12(1):4. doi:10.1038/s41413-023-00313-5
70. Ma C, Yu R, Li J, et al. Targeting proteostasis network in osteoporosis: pathological mechanisms and therapeutic implications. Ageing Res Rev. 2023;90:102024. doi:10.1016/j.arr.2023.102024
71. Amroodi MN, Maghsoudloo M, Amiri S, et al. Unraveling the molecular and immunological landscape: exploring signaling pathways in osteoporosis. Biomed Pharmacother. 2024;177:116954. doi:10.1016/j.biopha.2024.116954
72. Wang X, Qu Z, Zhao S, et al. Wnt/β-catenin signaling pathway: proteins’ roles in osteoporosis and cancer diseases and the regulatory effects of natural compounds on osteoporosis. Mol Med. 2024;30(1):193. doi:10.1186/s10020-024-00957-x
73. Wang K, Hu S. The synergistic effects of polyphenols and intestinal microbiota on osteoporosis. Front Immunol. 2023;14:1285621. doi:10.3389/fimmu.2023.1285621
74. Frase D, Lee C, Nachiappan C, et al. The inflammatory contribution of B-lymphocytes and neutrophils in progression to osteoporosis. Cells. 2023;12(13):1744. doi:10.3390/cells12131744
75. Yuan W, Xu J, Yang N, et al. Engineered dynamic hydrogel niches for the regulation of redox homeostasis in osteoporosis and degenerative endocrine diseases. Gels. 2023;10(1):31. doi:10.3390/gels10010031
76. Tian S, Song Y, Guo L, et al. Epigenetic mechanisms in osteoporosis: exploring the power of m(6)A RNA modification. J Cell Mol Med. 2025;29(1):e70344. doi:10.1111/jcmm.70344
77. Glaser DL, Kaplan FS. Osteoporosis. Definition and clinical presentation. Spine. 1997;22(24 Suppl):12S–16S. doi:10.1097/00007632-199712151-00003
78. Emkey GR, Epstein S. Secondary osteoporosis: pathophysiology & diagnosis. Best Pract Res Clin Endocrinol Metab. 2014;28(6):911–935. doi:10.1016/j.beem.2014.07.002
79. Al Anouti F, Taha Z, Shamim S, et al. An insight into the paradigms of osteoporosis: from genetics to biomechanics. Bone Rep. 2019;11:100216. doi:10.1016/j.bonr.2019.100216
80. Prentice A. Diet, nutrition and the prevention of osteoporosis. Public Health Nutr. 2004;7(1A):227–243. doi:10.1079/PHN2003590
81. Zhang X, Man KW, Li GH, et al. Osteoporosis is a novel risk factor of infections and sepsis: a cohort study. EClinicalMedicine. 2022;49:101488. doi:10.1016/j.eclinm.2022.101488
82. Jiao Y, Sun J, Li Y, et al. Association between adiposity and bone mineral density in adults: insights from a national survey analysis. Nutrients. 2023;15(15):3492. doi:10.3390/nu15153492
83. Du Y, Huo Y, Yang Y, et al. Role of sirtuins in obesity and osteoporosis: molecular mechanisms and therapeutic targets[. Cell Commun Signal. 2025;23(1):20. doi:10.1186/s12964-024-02025-7
84. Zhang J, Hu W, Zou Z, et al. The role of lipid metabolism in osteoporosis: clinical implication and cellular mechanism. Genes Dis. 2024;11(4):101122. doi:10.1016/j.gendis.2023.101122
85. Gao H, Peng X, Li N, et al. Emerging role of liver-bone axis in osteoporosis. J Orthop Translat. 2024;48:217–231. doi:10.1016/j.jot.2024.07.008
86. Koh A, Oyende O, Humes DJ, et al. Risk of osteopaenia, osteoporosis and osteoporotic fractures in patients with chronic pancreatitis: a systematic review and meta-analysis. Clin Nutr. 2023;42(7):1086–1094. doi:10.1016/j.clnu.2023.05.019
87. Xu J, Cao B, Li C, et al. The recent progress of endocrine therapy-induced osteoporosis in estrogen-positive breast cancer therapy. Front Oncol. 2023;13:1218206. doi:10.3389/fonc.2023.1218206
88. Bao K, Jiao Y, Xing L, et al. The role of wnt signaling in diabetes-induced osteoporosis. Diabetol Metab Syndr. 2023;15(1):84. doi:10.1186/s13098-023-01067-0
89. Marcucci G, Brandi ML. The diagnosis and therapy of osteoporosis in gaucher disease. Calcif Tissue Int. 2025;116(1):31. doi:10.1007/s00223-024-01340-y
90. Bhardwaj A, Swe K, Sinha NK. Treatment for osteoporosis in people with beta-thalassaemia. Cochrane Database Syst Rev. 2023;5(5):CD010429. doi:10.1002/14651858.CD010429.pub3
91. Zhang H, Gu J-M, Chao A-J, et al. A Phase III randomized, double-blind, placebo-controlled trial of the denosumab biosimilar QL1206 in postmenopausal Chinese women with osteoporosis and high fracture risk. Acta Pharmacol Sin. 2023;44(2):446–453. doi:10.1038/s41401-022-00954-y
92. Wen C, Xu X, Zhang Y, et al. Bone targeting nanoparticles for the treatment of osteoporosis. Int J Nanomed. 2024;19:1363–1383. doi:10.2147/IJN.S444347
93. Mori S, Hagino H, Sugimoto T, et al. Sequential therapy with once-weekly teriparatide injection followed by alendronate versus monotherapy with alendronate alone in patients at high risk of osteoporotic fracture: final results of the Japanese osteoporosis intervention trial-0]. Osteoporos Int. 2023;34(1):189–199. doi:10.1007/s00198-022-06570-0
94. McClung MR, Betah D, Leder BZ, et al. Romosozumab improves microarchitecture as assessed by tissue thickness-adjusted trabecular bone score in postmenopausal women with osteoporosis. J Bone Miner Res. 2025;40(2):193–200. doi:10.1093/jbmr/zjae194
95. Lyu Z, Hu Y, Guo Y, et al. Modulation of bone remodeling by the gut microbiota: a new therapy for osteoporosis. Bone Res. 2023;11(1):31. doi:10.1038/s41413-023-00264-x
96. Zheng XQ, Wang DB, Jiang YR, et al. Gut microbiota and microbial metabolites for osteoporosis. Gut Microbes. 2025;17(1):2437247. doi:10.1080/19490976.2024.2437247
97. Li Z, Li D, Chen R, et al. Cell death regulation: a new way for natural products to treat osteoporosis. Pharmacol Res. 2023;187:106635. doi:10.1016/j.phrs.2022.106635
98. Chen Y, Huang Y, Li J, et al. Enhancing osteoporosis treatment with engineered mesenchymal stem cell-derived extracellular vesicles: mechanisms and advances. Cell Death Dis. 2024;15(2):119. doi:10.1038/s41419-024-06508-w
99. Skalny AV, Aschner M, Silina EV, et al. The role of trace elements and minerals in osteoporosis: a review of epidemiological and laboratory findings. Biomolecules. 2023;13(6):1006. doi:10.3390/biom13061006
100. Ko SY. Therapeutic potential of ginsenosides on bone metabolism: a review of osteoporosis, periodontal disease and osteoarthritis. Int J Mol Sci. 2024;25(11):5828. doi:10.3390/ijms25115828
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bibliometrics Analysis and Visualization of Sarcopenia Associated with Osteoporosis from 2000 to 2022
Yang J, Jiang T, Xu G, Liu W
Journal of Pain Research 2023, 16:821-837
Published Date: 13 March 2023
Trends in Acupuncture Therapy for Microcirculation and Hemorheology from 1998 to 2023: A Bibliometric and Visualized Study
Wang Q, Zhang Q, Lu F, Hu H, Zhu M
Journal of Pain Research 2024, 17:177-196
Published Date: 8 January 2024
Risk Factors for Psoriasis Flares: A Narrative Review
Potestio L, Lauletta G, Tommasino N, Portarapillo A, Salsano A, Battista T, Martora F, Megna M
Psoriasis: Targets and Therapy 2024, 14:39-50
Published Date: 30 May 2024
The Global Research Trends on Intrinsic Capacity of Older Adults: A Bibliometric and Visual Analysis of Papers Published During 2015–2023
Cao X, Tian Y, Chen H, Li S, Zhou J
Journal of Multidisciplinary Healthcare 2024, 17:3323-3339
Published Date: 11 July 2024
Self-Management of Kidney Transplant Recipients Research: A Comprehensive Bibliometric Analysis
Lou J, Hu Z, Yuan M, Luo R, Zhang T, Ye Q, Zhou X, Feng B
Journal of Multidisciplinary Healthcare 2024, 17:6071-6090
Published Date: 24 December 2024