Back to Journals » Orthopedic Research and Reviews » Volume 17
Research Review on the Mechanisms of Pathological New Bone Formation in Ankylosing Spondylitis
Authors Zhou X, Ma W, Zhang H, Zhao Z, Huang C ![]()
Received 26 May 2025
Accepted for publication 20 August 2025
Published 12 September 2025 Volume 2025:17 Pages 469—479
DOI https://doi.org/10.2147/ORR.S540714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Xingshun Zhou, Wenhui Ma, Hengsheng Zhang, Zilin Zhao, Cong Huang
Department of Radiology, No. 926 Hospital, Joint Logistics Support Force of PLA, Kaiyuan, Yunnan, 661699, People’s Republic of China
Correspondence: Zilin Zhao, Email [email protected] Cong Huang, Email [email protected]
Abstract: Ankylosing spondylitis (AS) is a long-lasting autoimmune disorder marked by inflammatory processes affecting the spinal column and sacroiliac joints, alongside abnormal bone growth. This review aims to summarize the mechanisms underlying pathological new bone formation in AS, focusing on key cell types, molecular pathways, and their roles in disease progression. We will discuss the interplay between osteoblasts and osteoclasts, the cytokines and signaling pathways that influence new bone formation, and how recent research findings contribute to our understanding of this complex process. Through a comprehensive analysis of relevant literature, this review seeks to provide a theoretical foundation and direction for future therapeutic strategies.
Keywords: Ankylosing spondylitis, new bone formation, osteoblasts, osteoclasts, cytokines
Introduction
Ankylosing spondylitis (AS) is a long-term inflammatory disorder that predominantly impacts the axial skeleton. The disease is marked by a progressive loss of spinal mobility and can lead to severe functional impairment, significantly impacting the quality of life for affected individuals.1 This condition is marked by notable pain, rigidity, and the progressive fusion of vertebrae. AS is classified within the spondyloarthritis category, which encompasses various associated disorders, including reactive arthritis and psoriatic arthritis. AS predominantly affects younger individuals, especially males, and its onset typically occurs between the ages of 20 and 40, and in rare cases after the age of 45. Even, late-onset AS (LoAS) is estimated to occur in around 3.5–13.8% of all cases of AS.2 One of the most distinctive features of AS is the pathological formation of new bone, known as syndesmophytes, which arises from the entheses—the sites where tendons and ligaments attach to bone. This pathological new bone formation not only contributes to the characteristic spinal fusion observed in AS but also exacerbates pain and limits mobility, leading to increased disability.3 The underlying mechanisms driving this aberrant bone formation are complex and multifactorial, involving genetic predispositions, immune dysregulation, environmental factors, and possibly microbiome interactions.
Genetic influences are fundamental in the pathogenesis of Ankylosing Spondylitis (AS), with the Human Leukocyte Antigen B27 (HLA-B27) recognized as the most prominent genetic indicator linked to this condition. Approximately 90% of patients with AS carry this allele, suggesting a strong genetic component to the disease’s pathogenesis.4 However, the presence of HLA-B27 alone cannot account for the full spectrum of AS cases, indicating that other genetic loci and environmental triggers are also involved. Recent genome-wide association studies (GWAS) have uncovered further genetic variants linked to ankylosing spondylitis (AS), enhancing our understanding of the various biological pathways involved in the condition.5
The significance of the immune system in AS is particularly remarkable. This condition is marked by an exaggerated immune reaction, which causes persistent inflammation at the entheses and triggers the formation of new bone. Key inflammatory cytokines, notably tumor necrosis factor-alpha (TNF-α) and interleukin-17 (IL-17), have been recognized as essential players in this mechanism. These cytokines facilitate the recruitment of immune cells to inflammatory sites, creating a cycle of inflammation and tissue repair that may become unregulated, ultimately resulting in abnormal bone formation.1 Moreover, recent research indicates that the gut microbiome could impact immune responses and play a role in the development of AS, emphasizing the interaction between genetic predispositions and environmental factors, including dietary habits and microbial exposure.6
Beyond genetic predispositions and immune system elements, external factors including physical stress, infections, and lifestyle choices such as tobacco use have been associated with the initiation and advancement of the disease. These elements may intensify inflammatory responses and facilitate the emergence of AS in individuals with a genetic vulnerability. For instance, contact with specific environmental toxins and infectious agents could instigate or amplify the inflammatory mechanisms that are hallmark features of AS.7
The primary aim of this review is to investigate the mechanisms underlying pathological new bone formation in ankylosing spondylitis (AS), with the goal of improving our comprehension of the disease’s pathophysiological aspects. By examining the interactions among genetic factors, immune system dysfunction, and environmental influences, we aspire to identify potential therapeutic targets and strategies that may enhance the management of AS. A thorough understanding of these mechanisms is essential for the development of innovative treatment approaches that not only alleviate the symptoms of AS but also address its root causes. This detailed examination will facilitate a more integrated strategy for the management of ankylosing spondylitis, ultimately leading to improved patient outcomes and enhanced quality of life.
The Basic Mechanisms of New Bone Formation
The process of new bone formation, referred to as osteogenesis, is a multifaceted biological phenomenon characterized by various cellular and molecular interactions. This segment explores the fundamental mechanisms underlying osteogenesis, emphasizing the activation and proliferation of osteoblasts, the function of osteoclasts, and the differentiation of bone marrow mesenchymal stem cells (BMSCs) (Table 1).
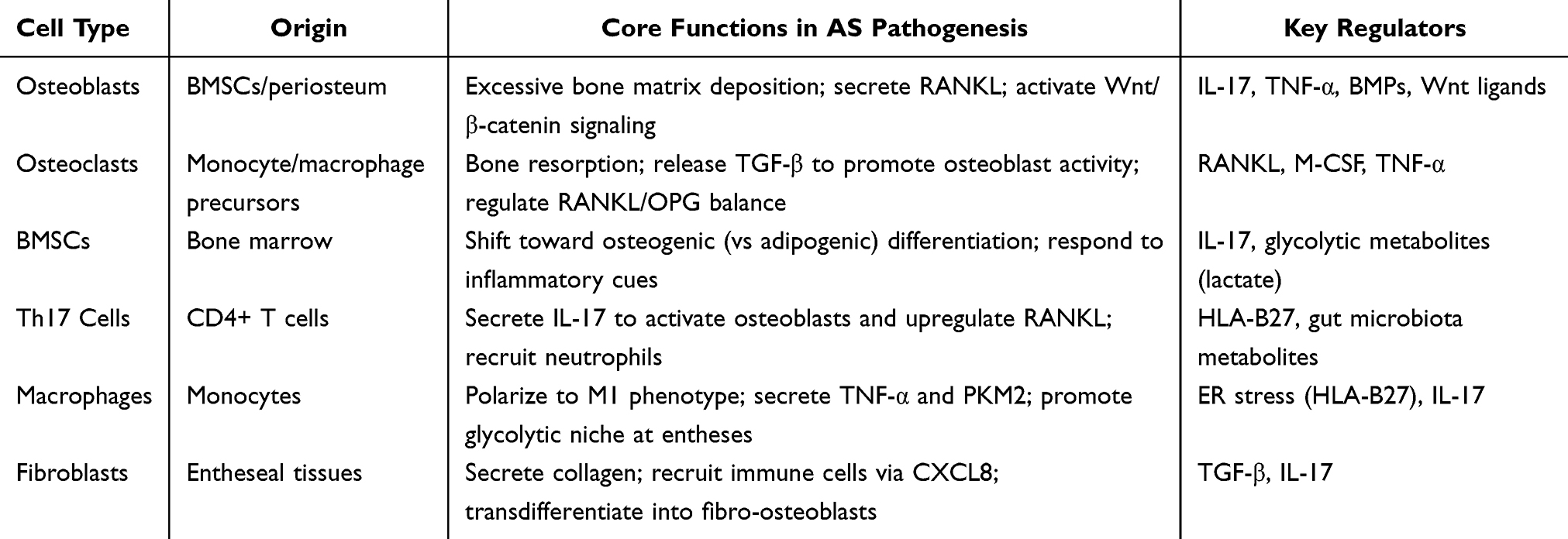 |
Table 1 Key Cell Types and Their Roles in AS Pathological New Bone Formation |
Activation and Proliferation of Osteoblasts
Osteoblasts are specialized cells responsible for bone formation. Their activation and proliferation are crucial for new bone formation and are influenced by various factors, including mechanical stress, hormonal signals, and local cytokine environments. The process begins with the recruitment of osteoprogenitor cells from the bone marrow or periosteum, which differentiate into mature osteoblasts. This differentiation is regulated by several signaling pathways, including the Wnt/β-catenin pathway, which is essential for osteoblast proliferation and function.
Mechanical loading serves as a crucial catalyst for the activation of osteoblasts. When bones experience mechanical stress, osteocytes, residing within the bone matrix, transmit signals to osteoblasts, thereby triggering the process of bone formation. This mechanotransduction mechanism encompasses a range of signaling molecules, including nitric oxide and prostaglandins, which stimulate osteoblast activity and facilitate the deposition of bone matrix. Additionally, the involvement of growth factors, such as bone morphogenetic proteins (BMPs) and transforming growth factor-beta (TGF-β), is fundamental to the differentiation and functional capacity of osteoblasts.
In pathological states such as osteoporosis, there is an imbalance between the activities of osteoblasts and osteoclasts, which results in diminished bone formation alongside heightened bone resorption. Consequently, it is crucial to comprehend the mechanisms governing the activation and proliferation of osteoblasts, as this knowledge is vital for formulating therapeutic approaches aimed at promoting bone formation in a range of clinical scenarios, including fractures and metabolic bone disorders.8
The Role of Osteoclasts in New Bone Formation
Osteoclasts are multinucleated cells that are integral to the process of bone resorption, which is vital for the proper remodeling of bone tissue. In contrast to osteoblasts, which are tasked with the formation of new bone, osteoclasts facilitate the removal of aged or compromised bone, thereby creating an opportunity for new bone to develop. The equilibrium between the activities of osteoblasts and osteoclasts is essential for the preservation of bone health.
The process by which osteoclasts develop from monocyte/macrophage precursors is governed by two primary factors: the receptor activator of nuclear factor-kappa B ligand (RANKL) and macrophage colony-stimulating factor (M-CSF). RANKL, secreted by osteoblasts and osteocytes, interacts with the RANK receptor located on osteoclast precursors, thereby facilitating their maturation into fully developed osteoclasts. Additionally, the functionality of osteoclasts is modulated by various local microenvironmental influences, such as cytokines and growth factors, which possess the capacity to either augment or suppress osteoclast activity.
Within the realm of new bone development, osteoclasts assume a role that transcends mere destruction; they are also instrumental in regulating this intricate process. Specifically, the act of bone resorption generates a microenvironment that is favorable for the recruitment and functionality of osteoblasts. This phenomenon is particularly pronounced during the early stages of bone healing, during which osteoclasts facilitate the resorption of compromised bone, thereby paving the way for the later deposition of new bone by osteoblasts.
Conversely, when osteoclast activity becomes excessive, it can precipitate pathological conditions such as osteoporosis, characterized by an increase in bone resorption that undermines the structural integrity of bone. Consequently, it is imperative to comprehend the dual functionality of osteoclasts in both the resorption and formation of bone to devise effective therapeutic strategies for addressing bone-related disorders.7
Differentiation of Bone Marrow Mesenchymal Stem Cells
Bone marrow mesenchymal stem cells (BMSCs) represent a class of multipotent stem cells with the potential to differentiate into multiple cell lineages, such as osteoblasts, chondrocytes, and adipocytes. Their capacity to transdifferentiate into osteoblasts plays an essential role in the processes of bone development and regeneration. The mechanism governing the differentiation of BMSCs into osteoblasts is influenced by a sophisticated interaction between intrinsic and extrinsic regulatory factors.
Intrinsic factors encompass the expression of particular transcription factors, including Runx2 and Osterix, which play a crucial role in the differentiation of osteoblasts. Extrinsic factors, including growth factors and cytokines present in the bone microenvironment, also play a significant role in this process. For example, BMPs are well-known inducers of osteogenic differentiation and are often used in clinical settings to enhance bone healing.
The microenvironment of the bone marrow, characterized by its unique cellular composition and extracellular matrix, also influences BMSC differentiation. Mechanical stimuli, such as those experienced during physical activity, can enhance the osteogenic potential of BMSCs by activating signaling pathways that promote bone formation.
Moreover, the interaction between BMSCs and other cell types, such as osteoblasts and osteoclasts, is critical for regulating bone homeostasis. For instance, osteoblasts can secrete factors that promote BMSC proliferation and differentiation, while osteoclasts can create a niche that supports BMSC survival and function.
In summary, the differentiation of BMSCs into osteoblasts is a vital component of new bone formation, influenced by a myriad of factors that ensure the proper balance between bone formation and resorption. Understanding these mechanisms is crucial for developing innovative therapies aimed at enhancing bone regeneration and treating bone-related diseases.8
The Impact of Cytokines
Cytokines act as critical messengers linking immune activation to pathological bone formation in AS, with TNF-α, IL-17, and FGFs emerging as central regulators. Their roles are multifaceted, spanning inflammation amplification, osteoclast-osteoblast crosstalk, and metabolic-osteogenic coupling. (Table 2).
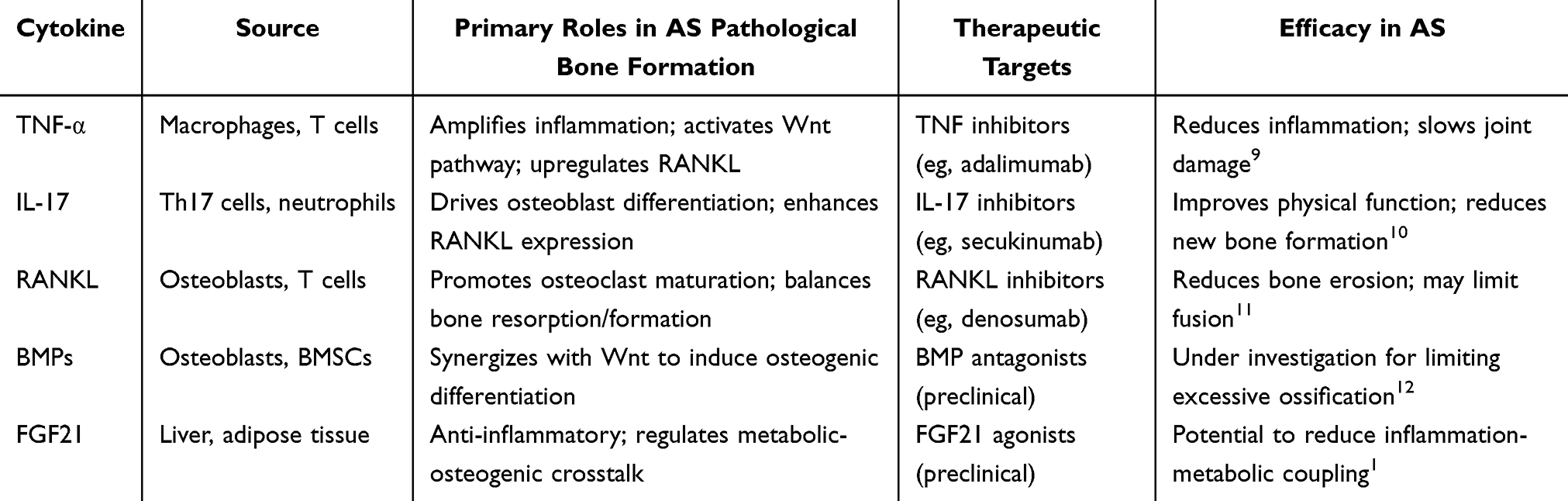 |
Table 2 Key Cytokines and Therapeutic Targets in AS |
Tumor Necrosis Factor-Alpha (TNF-α): A Pivotal Amplifier of Inflammation-Osteogenesis Crosstalk
TNF-α, primarily secreted by macrophages and activated T cells, drives a feedforward loop between inflammation and bone remodeling. It enhances IL-17 production by Th17 cells1 and directly activates the Wnt/β-catenin pathway in osteoblasts, promoting their differentiation.13 Concurrently, TNF-α upregulates RANKL expression in osteoblasts and fibroblasts, accelerating osteoclastogenesis.7 This dual role—amplifying inflammation while skewing bone turnover toward formation—makes TNF-α a cornerstone therapeutic target: anti-TNF agents (eg, adalimumab) reduce disease activity and slow structural progression, though they do not fully prevent fusion, likely due to residual IL-17-mediated pathways.9
Interleukin-17 (IL-17): Bridging Immune Responses to Pathological Ossification
IL-17, predominantly produced by Th17 cells (and neutrophils via NETs14), is a key driver of entheseal pathology. It directly stimulates osteoblasts to secrete BMPs and activate Runx2,15 while upregulating RANKL in both osteoblasts and fibroblasts to balance resorption and formation.7 In AS, elevated IL-17 correlates with syndesmophyte progression,10 and its inhibition (eg, secukinumab) reduces new bone formation more effectively than TNF blockers in preclinical models, highlighting its specificity for osteogenic pathways.10 Notably, IL-17 also recruits macrophages to entheses, reinforcing a pro-inflammatory niche via TNF-α and glycolytic metabolites (eg, lactate),13 creating a self-sustaining cycle.
Fibroblast Growth Factor (FGF): Metabolic Modulators of Bone Homeostasis
FGFs, particularly FGF21, link metabolic status to bone remodeling. FGF21, secreted by the liver and adipose tissue, exerts anti-inflammatory effects by suppressing Th17 polarization1 and modulates BMSC differentiation: it inhibits osteogenesis under basal conditions but may switch to a pro-osteogenic role in inflamed microenvironments (via crosstalk with TNF-α).16 This context-dependent function suggests FGF21 agonists could mitigate inflammation-driven bone loss in early AS while limiting excessive formation in advanced stages, though clinical translation remains preliminary.
Abnormalities in Signaling Pathways
The understanding of signaling pathways is crucial in comprehending the mechanisms underlying various diseases, including ankylosing spondylitis (AS). Abnormalities in key signaling pathways can lead to pathological changes and contribute to disease progression. This section will discuss three major signaling pathways implicated in AS: the Wnt/β-catenin pathway, the RANK/RANKL/OPG pathway, and the bone morphogenetic protein (BMP) pathway (Figure 1).
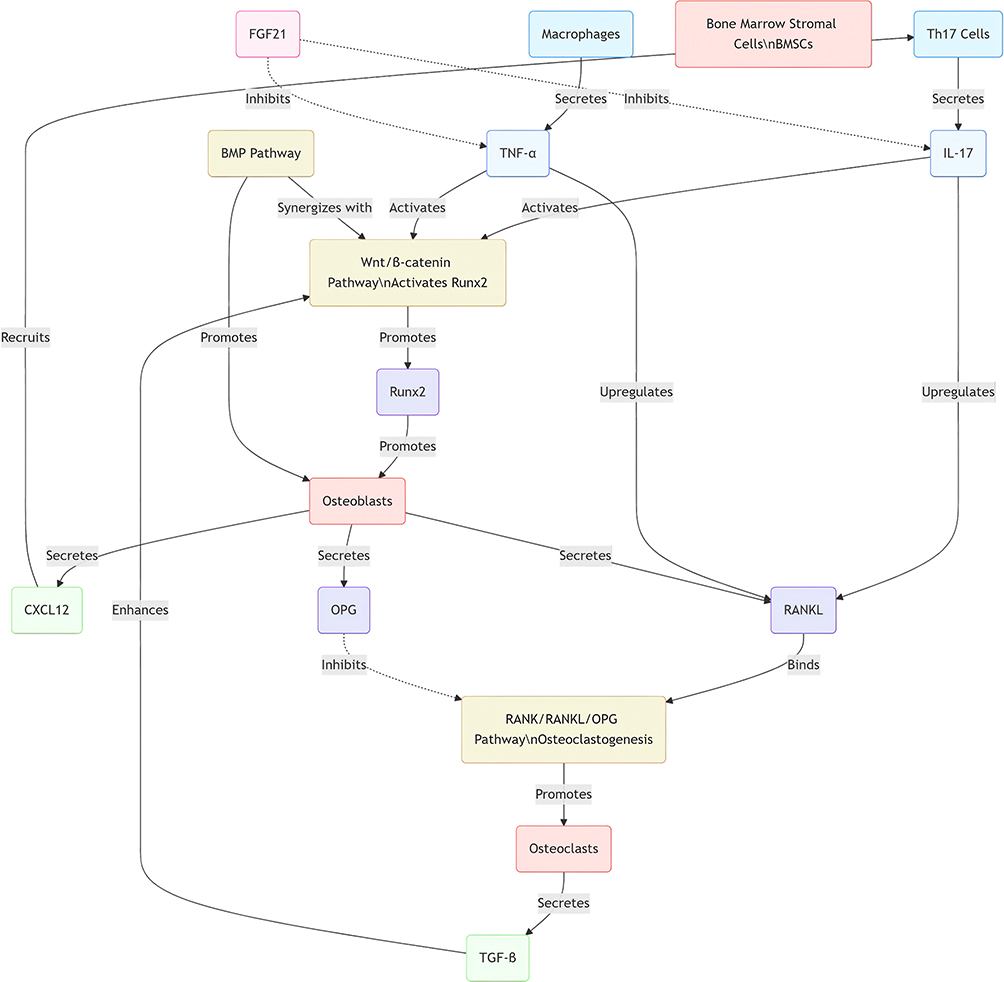 |
Figure 1 Schematic of integrated signaling networks in AS pathological new bone formation. Key pathways (Wnt/β-catenin, RANK/RANKL/OPG, BMP) are interconnected via pro-inflammatory cytokines (TNF-α, IL-17) and cellular crosstalk between immune cells (Th17, macrophages) and bone cells (osteoblasts, osteoclasts, BMSCs). |
Wnt/β-Catenin Pathway
The Wnt/β-catenin signaling cascade serves as a fundamental modulator of various cellular activities, such as proliferation, differentiation, and migration. Within the framework of ankylosing spondylitis, this pathway has been identified as a pivotal factor in the abnormal bone formation that typifies the condition. Dysregulated activation of the Wnt/β-catenin pathway has been associated with the pronounced new bone development seen in individuals afflicted with ankylosing spondylitis, resulting in spinal fusion and rigidity.17 The pathway’s dysregulation is often associated with inflammatory processes, which further exacerbate the condition.
Research has demonstrated that the Wnt/β-catenin signaling pathway is activated in response to inflammatory cytokines, such as TNF-α and IL-17, which are commonly elevated in AS.13 This activation leads to the upregulation of osteogenic markers and promotes the differentiation of mesenchymal stem cells into osteoblasts, contributing to ectopic bone formation. Additionally, the interplay between Wnt signaling and other pathways, such as the RANK/RANKL/OPG pathway, highlights the complexity of the regulatory networks involved in AS pathology.18 Periostin has been shown to play a role in bone anabolism through the regulation of Wnt-β-catenin signaling.19,20 One study concluded that serum periostin levels were lower in patients with AS than in healthy controls and also negatively correlated with disease activity, periostin has been shown to play a role in bone anabolism through the regulation of Wnt-β-catenin signaling. One study concluded that serum periostin levels were lower in patients with AS than in healthy controls and also negatively correlated with disease activity.20
Furthermore, studies have indicated that inhibiting the Wnt/β-catenin pathway could provide therapeutic benefits by reducing pathological bone formation in AS.7 This suggests that targeting this pathway may offer a novel approach to managing the disease, particularly in patients with severe manifestations of spinal fusion.
RANK/RANKL/OPG Signaling Pathway
The RANK/RANKL/OPG signaling pathway plays a crucial role in the regulation of bone metabolism, especially regarding the process of osteoclastogenesis. RANKL, which is secreted by osteoblasts and various other cell types, interacts with RANK receptors located on osteoclast precursors, thereby facilitating their maturation into fully developed osteoclasts that undertake the task of bone resorption.21 In the context of ankylosing spondylitis, the aberrant regulation of this signaling pathway has been associated with heightened osteoclast activity, leading to bone erosion and exacerbating the distinctive bone remodeling irregularities characteristic of the disease.
In AS, elevated levels of RANKL and decreased levels of OPG have been observed, leading to an increased RANKL/OPG ratio that favors osteoclastogenesis.11 This imbalance is further exacerbated by inflammatory cytokines, which can stimulate RANKL production and enhance osteoclast activity, thereby promoting bone loss.7 Targeting this pathway has shown promise in preclinical studies, with RANKL inhibitors, such as denosumab, demonstrating efficacy in reducing bone resorption and potentially preventing the progression of AS.22
Moreover, the RANK/RANKL/OPG pathway’s role extends beyond bone metabolism; it is also involved in immune regulation and the pathogenesis of various cancers, indicating its multifaceted nature.23 Understanding the intricate interactions within this pathway may provide insights into novel therapeutic strategies for managing AS and its associated complications.
Bone Morphogenetic Protein (BMP) Pathway
The bone morphogenetic protein (BMP) pathway is another critical signaling cascade involved in bone formation and remodeling. BMPs are a group of growth factors that play essential roles in osteoblast differentiation and bone regeneration. In ankylosing spondylitis, the BMP pathway has been implicated in the aberrant bone formation that characterizes the disease.24
Research indicates that BMP signaling can be dysregulated in AS, leading to enhanced osteoblast activity and excessive bone formation.15 This dysregulation is often associated with inflammatory processes, as BMPs can be upregulated in response to inflammatory cytokines present in the AS microenvironment. Furthermore, the interaction between BMP signaling and other pathways, such as Wnt and RANK/RANKL/OPG, underscores the complexity of the regulatory mechanisms governing bone metabolism in AS.12
Therapeutically, targeting the BMP pathway presents a potential strategy for managing AS. Studies have shown that modulating BMP signaling can influence osteoblast differentiation and activity, thereby impacting bone formation.25 Additionally, understanding the role of BMPs in the context of inflammation and bone remodeling may lead to the development of novel therapeutic approaches aimed at mitigating the pathological bone changes associated with AS.
In summary, the irregularities observed in the Wnt/β-catenin, RANK/RANKL/OPG, and BMP signaling pathways are crucial contributors to the development of ankylosing spondylitis. Focusing on these pathways could open up novel strategies for therapeutic intervention, thereby enhancing patient outcomes and overall quality of life. Additional research is essential to clarify the specific mechanisms that govern these signaling pathways and their interrelations within the framework of ankylosing spondylitis.
The Relationship Between the Immune System and New Bone Formation
The immune system does not merely initiate inflammation in AS; it actively reprograms bone cell behavior via cellular crosstalk and microenvironmental cues, driving pathological ossification.
Autoimmune Triggers: HLA-B27 and the Immune-Osteogenic Switch
HLA-B27 misfolding in APCs induces ER stress, activating both adaptive (Th17 polarization) and innate (macrophage glycolysis13) responses. This triggers IL-17 and TNF-α secretion, which converge on entheseal fibroblasts and BMSCs: fibroblasts upregulate CXCL8 to recruit more immune cells,26 while BMSCs shift toward osteogenesis via CaSR-PLCγ signaling.27 Notably, HLA-B27-associated autoantibodies may directly activate osteoblasts, independent of inflammation,28 creating a “double hit” model where immune dysregulation and bone cell auto-reactivity synergize.
Inflammatory Microenvironments: Skewing Bone Turnover
Chronic inflammation disrupts the osteoclast-osteoblast balance via cytokine-mediated pathways. Pro-inflammatory cytokines (TNF-α, IL-17, IL-6) upregulate RANKL while downregulating OPG,29 tipping the RANKL/OPG ratio toward osteoclast activation and bone resorption—though in AS, this resorption is paradoxically followed by excessive formation, as osteoclast-derived TGF-β and collagen fragments recruit osteoblasts.23 Macrophage polarization exacerbates this: M1 macrophages secrete TNF-α to amplify inflammation, while their glycolytic byproducts (lactate) stabilize HIF-1α in BMSCs, enhancing Runx2 expression.13 MDSCs, conversely, may temper this process via anti-inflammatory IL-10, explaining variability in fusion rates.30
In summary, the interplay between the immune system and the processes of new bone formation is intricate and possesses multiple dimensions. Autoimmune reactions may induce persistent inflammation, subsequently influencing bone metabolism by enhancing the formation of osteoclasts while suppressing the activity of osteoblasts. A comprehensive understanding of these interactions is crucial for the advancement of targeted therapeutic strategies that seek to restore equilibrium in bone metabolism and alleviate the detrimental impacts of inflammatory disorders on skeletal health. Additional investigations are required to clarify the specific mechanisms at play and to pinpoint prospective therapeutic targets for disorders marked by abnormal bone formation.
Exploration of New Treatment Strategies
The exploration of new treatment strategies in the field of medicine is crucial for addressing complex diseases. This section discusses three innovative approaches: the application of biological agents, the development of targeted drugs, and the prospects of gene therapy (Table 3).
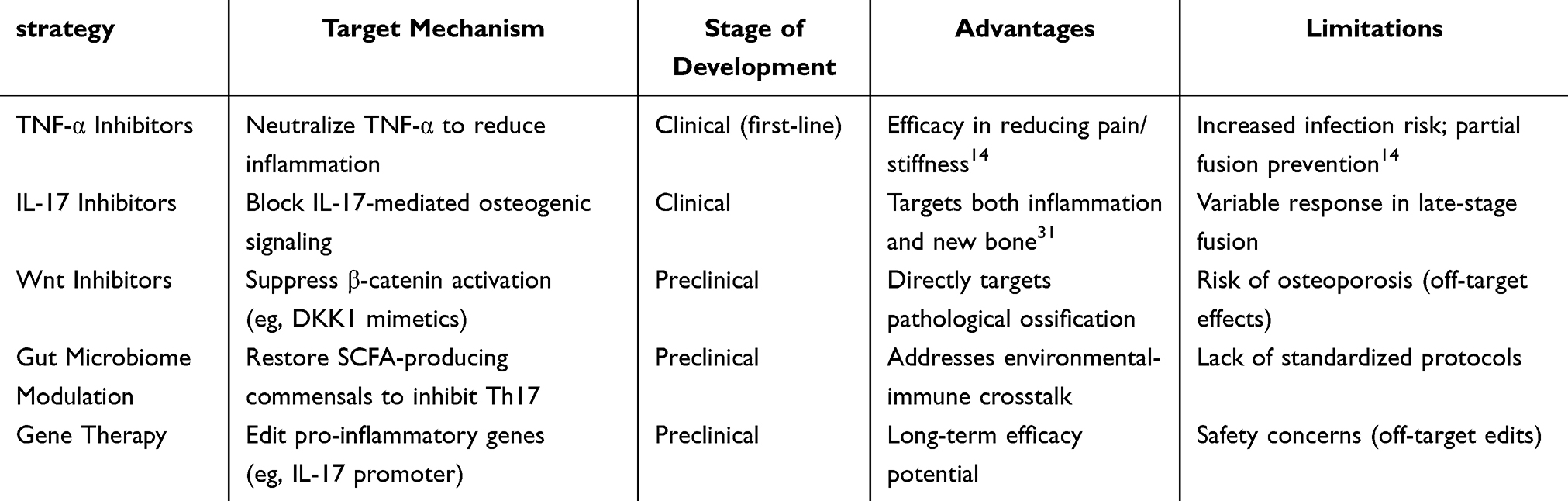 |
Table 3 Emerging Treatment Strategies and Mechanisms |
Application of Biological Agents
Biological agents, including monoclonal antibodies and recombinant proteins, have revolutionized the treatment landscape for various diseases, particularly autoimmune disorders and cancers. These agents are formulated to precisely target particular elements of the immune system or cancer cells, providing a more customized treatment strategy in contrast to conventional small molecule pharmaceuticals. For example, biological agents like tumor necrosis factor (TNF) inhibitors have demonstrated considerable effectiveness in managing disorders such as rheumatoid arthritis and AS by selectively neutralizing pro-inflammatory cytokines. This targeted action leads to a reduction in inflammation and helps in averting joint damage.27
The use of biological agents is not without challenges. The production of these agents can be complex and costly, and their administration often requires careful monitoring for adverse effects. Moreover, the development of resistance to biological therapies is a growing concern. For example, in AS, while TNF inhibitors have improved patient outcomes, some individuals may not respond adequately or may experience a loss of response over time.15
Recent progress in the field of biotechnology has resulted in the creation of bispecific antibodies, which possess the ability to target two distinct antigens concurrently. This innovation not only improves therapeutic effectiveness but also holds the promise of minimizing the likelihood of resistance development. Furthermore, there is an increasing interest in integrating biologics with conventional pharmacological treatments in combination therapies to improve overall treatment outcomes. Such a diverse strategy seeks to harness the advantages of both biological and traditional medical therapies, thereby offering a more thorough treatment framework for patients suffering from multifaceted diseases.28
Development of Targeted Drugs
The development of targeted therapies signifies a transformative approach in the management of various diseases, especially in the fields of oncology and chronic inflammatory disorders. Unlike conventional therapies that often affect both healthy and diseased cells, targeted drugs are designed to interact with specific molecular targets associated with disease pathology. This specificity not only enhances therapeutic efficacy but also minimizes side effects, improving the overall quality of life for patients.
In the context of ankylosing spondylitis, for instance, researchers are investigating the role of specific signaling pathways involved in the disease’s pathogenesis. Recent studies have highlighted the importance of the interleukin-17 (IL-17) pathway in promoting inflammation and pathological bone formation in AS. The utilization of monoclonal antibodies aimed at interleukin-17 (IL-17) has exhibited encouraging results in clinical studies, revealing substantial decreases in disease severity and enhancements in physical capabilities.10
Moreover, the development of small molecule inhibitors that target specific kinases involved in inflammatory signaling pathways is gaining traction. These inhibitors can modulate the activity of key enzymes, thereby altering the disease course at a molecular level. For example, inhibitors targeting Janus kinase (JAK) pathways have been shown to be effective in various inflammatory disorders, including AS, by interrupting the signaling cascade that leads to inflammation and bone formation.32
The progress in precision medicine, which customizes therapeutic approaches according to the unique genetic characteristics of individuals, significantly amplifies the possibilities for the development of targeted pharmaceuticals. By identifying specific genetic mutations or biomarkers associated with disease, clinicians can select the most appropriate targeted therapy for each patient, thereby optimizing treatment outcomes and minimizing unnecessary side effects.33
Prospects of Gene Therapy
Gene therapy holds immense potential as a transformative approach for treating genetic disorders and complex diseases. By directly modifying the genetic material within a patient’s cells, gene therapy aims to correct the underlying causes of diseases rather than merely alleviating symptoms. This innovative strategy has gained significant attention in recent years, particularly with the advancements in gene-editing technologies such as CRISPR-Cas9, which allow for precise modifications of the genome.34
In the context of ankylosing spondylitis and other inflammatory diseases, gene therapy could offer a novel avenue for treatment by targeting specific genes involved in inflammatory pathways. For instance, researchers are exploring the use of gene editing to downregulate pro-inflammatory cytokines or to enhance the expression of anti-inflammatory factors, potentially leading to long-lasting therapeutic effects.31
However, the clinical application of gene therapy is not without challenges. Issues related to delivery mechanisms, off-target effects, and long-term safety remain significant hurdles that need to be addressed. The development of effective viral vectors for gene delivery, as well as the exploration of non-viral delivery systems, is critical for the successful implementation of gene therapy in clinical settings.35
The future of gene therapy also hinges on robust clinical trials to establish safety and efficacy. As more gene therapies enter clinical trials, the accumulation of data will provide valuable insights into the long-term effects and potential complications associated with these treatments. This knowledge will be essential for refining gene therapy approaches and ensuring that they can be safely integrated into routine clinical practice.34
In conclusion, the exploration of new treatment strategies, including the application of biological agents, the development of targeted drugs, and the prospects of gene therapy, represents a promising frontier in the fight against complex diseases. Continued research and innovation in these areas will be crucial for improving patient outcomes and advancing the field of medicine.
Conclusion
AS is a long-term inflammatory condition defined by the abnormal development of new bone, a phenomenon that is intrinsically intricate and involves multiple dimensions. The intricate interplay among various cell types, molecular mechanisms, and immune responses involved in this process highlights the necessity of a comprehensive understanding of AS pathophysiology. This article has elucidated the significance of these interactions, which not only advances our knowledge of AS but also lays the groundwork for the development of innovative therapeutic strategies aimed at improving patient outcomes and quality of life.
From an expert perspective, it is crucial to acknowledge the diversity of research findings surrounding the pathogenesis of new bone formation in AS. Different studies have employed a variety of methodologies, ranging from genetic and molecular analyses to imaging and clinical evaluations, each contributing unique insights into the disease process. This diversity, while enriching, can also lead to challenges in interpreting the findings and reaching consensus on the most effective treatment modalities. As researchers and clinicians, we must strive to balance these varying perspectives, integrating results from preclinical studies, clinical trials, and patient-reported outcomes to form a holistic understanding of AS.
Furthermore, the exploration of novel targeted therapies represents a promising avenue for future research. The identification of specific molecular targets that mediate the pathological processes of new bone formation could revolutionize the therapeutic landscape for AS. However, the transition from bench to bedside requires a careful evaluation of the safety and efficacy of these new treatments. It is essential to conduct rigorous clinical trials that not only assess the biological effects of these therapies but also consider their impact on functional outcomes and overall quality of life for patients.
The future of AS research must also consider the growing body of evidence supporting the role of the immune system in the disease’s pathogenesis. Understanding the contributions of various immune cells and their signaling pathways can provide critical insights into the mechanisms driving inflammation and bone formation. This knowledge can potentially lead to the identification of biomarkers that predict disease progression and treatment response, enabling a more personalized approach to therapy.
As we move forward, collaboration among researchers, clinicians, and patients will be vital in addressing the complexities of AS. Multidisciplinary teams can facilitate the sharing of knowledge across different fields, fostering innovation and enhancing the translation of research findings into clinical practice. Moreover, engaging patients in the research process can ensure that their experiences and preferences are reflected in the development of new treatment modalities.
In summary, the abnormal formation of new bone associated with ankylosing spondylitis highlights the necessity for a comprehensive understanding of the disease’s underlying mechanisms. By integrating various research viewpoints and emphasizing the investigation of targeted therapies, substantial progress can be achieved in enhancing the prognosis and overall quality of life for those impacted by this debilitating disorder. The journey towards effective treatment demands a dedication to continuous research, collaborative efforts, and a focus on patient-centered care, which will ultimately result in advancements capable of revolutionizing the management of ankylosing spondylitis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Hwang MC, Ridley L, Reveille JD. Ankylosing spondylitis risk factors: a systematic literature review. Clin Rheumatol. 2021;40(8):3079–3093. doi:10.1007/s10067-021-05679-7
2. Uslu S, Semih Gulle S, Sen G, et al. Assessing safety and efficacy of TNFi treatment in late onset ankylosing spondylitis: a TURKBIO registry study. Sci Rep. 2024;14(1):14194. doi:10.1038/s41598-024-65180-4
3. Ma Y, Lai J, Wan Q, et al. Exploring the common mechanisms and biomarker ST8SIA4 of atherosclerosis and ankylosing spondylitis through bioinformatics analysis and machine learning. Front Cardiovasc Med. 2024;11:1421071. doi:10.3389/fcvm.2024.1421071
4. Nagit RE, Rezus E, Cianga P. Exploring the pathogenesis of spondylarthritis beyond HLA-B27: a descriptive review. Int J Mol Sci. 2024;25(11):6081. doi:10.3390/ijms25116081
5. Liao HT, Tsai CY, Lai CC, et al. The potential role of genetics, environmental factors, and gut dysbiosis in the aberrant non-coding RNA expression to mediate inflammation and osteoclastogenic/osteogenic differentiation in ankylosing spondylitis. Front Cell Dev Biol. 2021;9:748063. doi:10.3389/fcell.2021.748063
6. Rizzo C, Camarda F, Donzella D, et al. Metabolomics: an Emerging Approach to Understand Pathogenesis and to Assess Diagnosis and Response to Treatment in Spondyloarthritis. Cells. 2022;11(3):549. doi:10.3390/cells11030549
7. Bilski R, Kamiński P, Kupczyk D, et al. Environmental and Genetic Determinants of Ankylosing Spondylitis. Int J Mol Sci. 2024;25(14):7814. doi:10.3390/ijms25147814
8. Anesi A, Generali L, Sandoni L, et al. From Osteoclast Differentiation to Osteonecrosis of the Jaw: molecular and Clinical Insights. Int J Mol Sci. 2019;20(19):4925. doi:10.3390/ijms20194925
9. Fahim T, Laouedj S, Abderrahmane A, et al. Corrigendum: numerical study of perforated obstacles effects on the performance of solar parabolic trough collector. Front Chem. 2023;11:1160174. doi:10.3389/fchem.2023.1160174
10. Lee JH, Lee SH, Jeon C, et al. The complement factor H-related protein-5 (CFHR5) exacerbates pathological bone formation in ankylosing spondylitis. J Mol Med. 2024;102(4):571–583. doi:10.1007/s00109-024-02428-6
11. Takegahara N, Kim H, Choi Y. RANKL biology. Bone. 2022;159:116353. doi:10.1016/j.bone.2022.116353
12. Mota RF, Cavalcanti de Araújo PH, Cezine MER, et al. RANKL impairs the TLR4 pathway by increasing TRAF6 and RANK interaction in macrophages. Biomed Res Int. 2022;2022:7740079. doi:10.1155/2022/7740079
13. Weng W, Zhang Y, Gui L, et al. PKM2 promotes proinflammatory macrophage activation in ankylosing spondylitis. J Leukoc Biol. 2023;114(6):595–603. doi:10.1093/jleuko/qiad054
14. Papagoras C, Chrysanthopoulou A, Mitsios A, et al. Neutrophil extracellular traps and interleukin 17 in ankylosing spondylitis. Mediterr J Rheumatol. 2021;32(2):182–185. doi:10.31138/mjr.32.2.182
15. Wang K, Lu J, Song C, et al. Extracellular vesicles derived from ligament tissue transport interleukin-17A to mediate ligament-to-bone crosstalk in ankylosing spondylitis. Adv Sci. 2024;11(46):e2406876. doi:10.1002/advs.202406876
16. He P, Lu X, Zhong M, et al. Plasma alpha-trypsin inhibitor heavy chain 4 as an age-specific biomarker in the diagnosis and treatment of major depressive disorder. Front Psychiatry. 2024;15:1449202. doi:10.3389/fpsyt.2024.1449202
17. De Leon-Oliva D, Barrena-Blázquez S, Jiménez-álvarez L, et al. The RANK-RANKL-OPG system: a multifaceted regulator of homeostasis, immunity, and cancer. Medicina. 2023;59(10):1752. doi:10.3390/medicina59101752
18. Raffaele B, Nicola M, Cinzia R, et al. Mechanisms of ossification of the entheses in spondyloarthritis physiopathogenic aspects and possible therapeutic implication. Tissue Cell. 2025;94:102803. doi:10.1016/j.tice.2025.102803
19. Sakellariou GT, Anastasilakis AD, Bisbinas I, et al. Circulating periostin levels in patients with AS: association with clinical and radiographic variables, inflammatory markers and molecules involved in bone formation. Rheumatology. 2015;54(5):908–914. doi:10.1093/rheumatology/keu425
20. Solmaz D, Uslu S, Kozacı D, et al. Evaluation of periostin and factors associated with new bone formation in ankylosing spondylitis: periostin may be associated with the Wnt pathway. Int J Rheum Dis. 2018;21(2):502–509. doi:10.1111/1756-185X.13186
21. Kumar P, Faruqui T, Yadav AK, et al. Targeting caspase pathway by novel N-Me aziridine derivatives for hepatocellular carcinoma drug discovery. J Biomol Struct Dyn. 2024;42(23):12981–12992. doi:10.1080/07391102.2023.2274520
22. Sariyildiz A, Benlidayi IC, Turk I, et al. Evaluation of the relationship between blood cell markers and inflammation, disease activity, and general health status in ankylosing spondylitis. Rev Assoc Med Bras. 2023;69(10):e20230722. doi:10.1590/1806-9282.20230722
23. Zhao Y, Wang HL, Li TT, et al. Baicalin ameliorates dexamethasone-induced osteoporosis by regulation of the RANK/RANKL/OPG signaling pathway. Drug Des Devel Ther. 2020;14:195–206. doi:10.2147/DDDT.S225516h
24. Huang X, Li Y, Liao H, et al. Research advances on stem cell-derived extracellular vesicles promoting the reconstruction of alveolar bone through RANKL/RANK/OPG pathway. J Funct Biomater. 2023;14(4):193. doi:10.3390/jfb14040193
25. Liu HW, Wei DX, He DW, et al. The rs6427384 and rs6692977 single nucleotide polymorphisms of the Fc Receptor-Like 5 (FCRL5) gene and the risk of ankylosing spondylitis: a case control study in a single center in China. Med Sci Monit. 2020;26:e920956. doi:10.12659/MSM.920956
26. Liu Z, Cai M, Ke H, et al. Fibroblast insights into the pathogenesis of ankylosing spondylitis. J Inflamm Res. 2023;16:6301–6317. doi:10.2147/JIR.S439604
27. Li X, Chen S, Hu Z, et al. Aberrant upregulation of CaSR promotes pathological new bone formation in ankylosing spondylitis. EMBO Mol Med. 2020;12(12):e12109. doi:10.15252/emmm.202012109
28. Tsai WH, Lin YC, Lan SH, et al. Generation of induced pluripotent stem cells from an HLA-B27 positive ankylosing spondylitis patient with syndesmophyte formation. Stem Cell Res. 2024;80:103508. doi:10.1016/j.scr.2024.103508
29. Jing W, Liu C, Su C, et al. Role of reactive oxygen species and mitochondrial damage in rheumatoid arthritis and targeted drugs. Front Immunol. 2023;14:1107670. doi:10.3389/fimmu.2023.1107670
30. Ren Y, Bäcker H, Müller M, et al. The role of myeloid derived suppressor cells in musculoskeletal disorders. Front Immunol. 2023;14:1139683. doi:10.3389/fimmu.2023.1139683
31. Gao J, Pi C, Pan J, Zhou W. Research progress on Hippo signaling pathway effector molecules in rheumatic immune system diseases. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2024;53(3):376–381. doi:10.3724/zdxbyxb-2023-0567
32. Zhang S, Hao W, Chen D, et al. Intermittent administration of PTH for the treatment of inflammatory bone loss does not enhance entheseal pathological new bone formation. Biochem Biophys Res Commun. 2024;711:149888. doi:10.1016/j.bbrc.2024.149888
33. Attarian S. New treatment strategies in Myasthenia gravis. Rev Neurol. 2024;180(9):971–981. doi:10.1016/j.neurol.2024.09.006
34. Chakraborty A, Yu ASL. Prospects for gene therapy in polycystic kidney disease. Curr Opin Nephrol Hypertens. 2025;34(1):121–127. doi:10.1097/MNH.0000000000001030
35. Shao M, Zhang W, Li Y, et al. Patch-seq: advances and biological applications. Cell Mol Neurobiol. 2023;44(1):8. doi:10.1007/s10571-023-01436-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Curculigoside is a Promising Osteoprotective Agent for Osteoporosis: Review
Du J, Qin W, Wen F, Liu Y, Zhang Q, Liu W, Huang C, Feng Z, Pan Z, Gu E
Drug Design, Development and Therapy 2025, 19:3323-3336
Published Date: 28 April 2025
The Role of Sirtuins in Bone Repair From the Perspective of Glucose Metabolism
Ding Y, Gao Y, Sun J, Cai Z
International Journal of General Medicine 2025, 18:5013-5031
Published Date: 1 September 2025
Research Advances on the Mechanism and Diagnosis of Bone Bridging in Ankylosing Spondylitis
Wang M, Liang Z
Orthopedic Research and Reviews 2026, 18:592297
Published Date: 16 March 2026
Role of Cytokines in Bone Diseases and Their Therapeutic Application
Guha A, Wahi P, Lal G
ImmunoTargets and Therapy 2026, 15:604392
Published Date: 7 May 2026