Back to Journals » International Journal of Women's Health » Volume 18
Research Progress on the Classification of Cesarean Scar Pregnancy
Authors Wei J, Wu Y, Shen K, Hu C, Huang J ![]() , Pei C
, Pei C
Received 24 October 2025
Accepted for publication 18 January 2026
Published 6 February 2026 Volume 2026:18 574945
DOI https://doi.org/10.2147/IJWH.S574945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jianling Wei,1 Yating Wu,1 Kuifang Shen,1 Caihong Hu,1 Jingrui Huang,1,2 Chenlin Pei1
1Department of Obstetrics, Xiangya Hospital Central South University, Changsha, People’s Republic of China; 2Hunan Engineering Research Center of Early Life Development and Disease Prevention, Changsha, People’s Republic of China
Correspondence: Chenlin Pei, Department of Obstetrics, Xiangya Hospital Central South University, 87 Xiangya Road, Changsha, 410008, People’s Republic of China, Email [email protected] Jingrui Huang, Department of Obstetrics, Xiangya Hospital Central South University, 87 Xiangya Road, Changsha, 410008, People’s Republic of China, Email [email protected]
Abstract: Cesarean scar pregnancy (CSP) is a special type of ectopic pregnancy that occurs after a cesarean section. In recent years, with an increase in the cesarean section rate, the incidence of cesarean scar pregnancies has also increased. This article systematically reviews the development and latest progress of various CSP classification methods to compare the diagnosis and treatment strategies of different CSP classifications and better manage patients with CSP. We evaluated various classification methods using the Oxford Centre for Evidence-Based Medicine (OCEBM) 2011 level of evidence, providing a basis for objective and precise classification of CSP in the future and thus providing more accurate clinical guidance for individualized treatment.
Keywords: cesarean scar pregnancy, classification, treatment
Introduction
Cesarean scar pregnancy (CSP) is a special type of ectopic pregnancy in which the fertilized egg implants at the previous cesarean section scar, often caused by poor healing of the cesarean section incision or abnormal development of the fertilized egg.1–3 With the significant increase in the rate of cesarean sections, the incidence of CSP has also risen.4–7 The incidence of CSP ranges from 1/1800 to 1/2216.8–10 The clinical manifestations of CSP include vaginal bleeding and hypogastralgia,11–13 but these are atypical and can easily lead to missed or misdiagnosed cases. If not properly diagnosed and treated, it may result in complications such as uterine rupture and massive hemorrhage. Importantly, CSP is considered a precursor or early form of placenta accreta spectrum (PAS). And if the pregnancy continues, it has a high risk of progressing into morbidly adherent placenta in the second and third trimesters, which seriously endangers maternal life.14–18 An appropriate classification method for CSP can accurately assess its severity, provide a standard for evaluating treatment efficacy, and provide guidance for clinical decision-making. There are various classification methods for CSP, but they differ in terms of classification criteria and corresponding treatment measures. Currently, there are no comprehensive reviews on these classification methods. This article reviews the development and evolution of CSP classification methods, summarizes the latest progress, and systematically compares several major CSP classifications and their treatment strategies, to comprehensively understand the classification of CSP and thereby improve its diagnosis and treatment level.
Methods
The PubMed, Web of Science, China National Knowledge Infrastructure and Wanfang databases were searched for studies reporting on the progress on the classification of cesarean scar pregnancy during early pregnancy. All literature related to classification of cesarean scar pregnancy and corresponding treatments was considered adequately. The search keywords included: “cesarean scar pregnancy”, “CSP”, “classification”, “type”, “treatment”. The inclusion criteria were defined: (1) original research (including cohort studies, case series) or authoritative guidelines/consensus primarily focusing on the classification system of CSP; (2) clearly describing classification criteria; (3) providing full-text in Chinese or English. Exclusion criteria: (1) case reports; (2) studies that did not explicitly use or propose a specific classification method; (3) duplicate publications or incomplete data. Literature screening was independently conducted by two researchers, and any disagreements were resolved through discussion or consultation with a third researcher. For the included classification methods, we used the Oxford Centre for Evidence-based Medicine (OCEBM) levels of evidence grading criteria to assess their level of evidence. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram is detailed in Figure 1.
 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram of identification of studies. |
Classification
Vial’s classification
In 2000, based on the growth direction of the gestational sac, Vial et al19 first proposed a classification for CSP: endogenicand exogenic types. Sun et al found that remnant myometrial thickness, grading of Doppler signals at the mass site, and gestational sac diameter are the three main factors affecting surgical success.20 Vial’s classification pioneered the classification of CSP, but this classification method only considers the growth direction of the gestational sac and does not fully consider the influence of the above-mentioned factors. Therefore, its guiding value for choosing the surgical method is relatively weak compared to other classifications.
Kaelin’s Classification
Zosmer et al21 hold that CSP implanted in a cracked scar (niche) of the gestational sac exhibits different characteristics from CSP implanted on a well-healed scar. And in 2017, Kaelin Agten et al22 classified CSP as “on the scar” type and “in the niche” type and believed that patients with “on the scar” CSP had significantly better outcomes, compared to those with “in the niche” CSP. This classification method has good guiding value for the expectant treatment of CSP. However, the application of Kaelin’s classification method in clinical practice is limited and the guiding value of this classification method for other treatment options requires further research. More importantly, the Society for Maternal-Fetal Medicine considers Kaelin’s classification method equivalent to Vial’s classification method, and does not recommend expectant treatment for CSP.16
Zhang’s Classification
In 2016, based on years of clinical practice, Zhang et al23 proposed a new clinical classification system and recommended appropriate methods for CSP treatment. The system divides CSP into stable CSP and risky CSP based on whether there is a high risk of severe bleeding, and divides risky CSP into three types based on the thickness of the myometrium (between the gestational sac and bladder) and the position of the gestational sac. The specific classifications are as follows.
(1) Stable CSP: No significant vaginal bleeding or increase in serum β-hCG level
(2) Risky CSP: High risk of severe bleeding
①Risky type I (thin-walled type): the thickness of the myometrium was < 3 mm.
Type Ia: Cesarean scar in the lower uterine segment.
Type Ib: Cesarean scar in the upper uterine segment.
Type Ic: Large protruding mass in the lower or upper uterine segment.
②Risky type II (thick-walled type): the thickness of the myometrium is ≥ 3 mm.
Risky type III: Part of the gestational sac is located on the cesarean scar, with a risk of severe bleeding or a tendency towards dangerous placenta previa.
Zhang et al ‘s classification method provides more specific treatment suggestions; however, the classification criteria are highly subjective.
Chinese Medical Classification
In 2012, in order to better diagnose and treat CSP, the Family Planning Branch of the Chinese Medical Association formulated the “Expert opinion of diagnosis and treatment of cesarean scar pregnancy”,24 and based on this, updated the consensus to “Expert opinion of diagnosis and treatment of cesarean scar pregnancy” in 2016.25 CSP is classified by means of ultrasound examination based on the growth direction of the gestational sac and the thickness of the uterine myometrium (between the gestational sac on the anterior uterine wall and the bladder).
Type I: The gestational sac partially implants at the scar site of the uterus, with some or most of it located inside the uterine cavity. The uterine muscle layer between the gestational sac and bladder becomes thinner, with a thickness greater than 3 mm.
Type II: The gestational sac is partially implanted at the uterine scar site, with some or most of it located inside the uterine cavity. The uterine muscle layer between the gestational sac and bladder becomes thinner, with a thickness ≤ 3 mm.
Type III: The gestational sac is completely implanted in the muscular layer of the uterine scar and protrudes outward towards the bladder. The uterine muscular layer between the gestational sac and bladder becomes significantly thinner or even missing, with a thickness of ≤ 3 mm. Among these, type III has a special mass-type ultrasound manifestation.
This classification method provides an additional refinement and represents an extension of Vial’s classification, compensating for the deficiency of consideration for the thickness of the myometrium of the uterine scar in Vial’s classification, which can provide more individualized and specific treatment plans for CSP. However, the effect of gestational sac size on disease has not been fully considered.
Lin’s Classification
In 2018, Lin et al26 conducted a retrospective analysis of 109 patients with CSP and classified them into four grades based on their ultrasound manifestations.
Grade I: Less than 50% of the gestational sac implanted in the myometrium.
Grade II: more than 50% of the gestational sac is implanted in the myometrium.
Grade III: The gestational sac protrudes into the pelvic cavity;
Grade IV: The gestational sac becomes an “amorphous tumor” rich in blood vessels.
Lin’s classification is based on ultrasound manifestations, and is relatively intuitive. However, it is only classified based on ultrasound examination results and does not consider other factors.
Qilu Classification
In 2015, the obstetrics and gynecology team of Qilu Hospital of Shandong University first proposed the Qilu classification method.27 After years of clinical validation, the team further optimized the original classification through a retrospective case analysis in 2023, proposed a new Qilu classification, and recommended surgical treatment strategies for each classification based on expert opinion.28 This classification system is based on transvaginal ultrasound examination and is divided into the following five clinical types according to the thickness of the myometrium of the anterior uterine wall and diameter of the gestational sac.
Type I: Implantation of the gestational sac into the cesarean section scar, regardless of the size of the gestational sac, with a myometrial thickness greater than 3 mm in the anterior uterine wall.
Type II: The thickness of the myometrium of the anterior uterine wall is 1–3 mm.
IIa: The average diameter of the gestational sac or mass is ≤ 30 mm. (Figure 2).
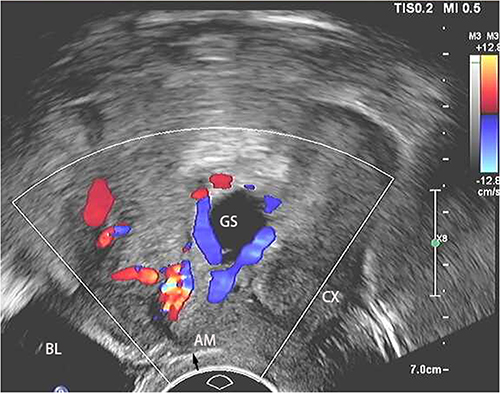 |
Figure 2 Cesarean scar pregnancy Type IIa. The thickness of the myometrium of the anterior uterine wall is 1.34mm, and the diameter of the gestational sac is 22mm. The arrow indicates thearea where the myometrial thickness was measured. Abbreviations: AM, anterior myometrium; BL, bladder; CX, cervix; GS, gestational sac. |
IIb: The average diameter of the gestational sac or mass is greater than 30 mm.
Type III: Uterine anterior wall muscle layer thickness ≤ 1mm.
IIIa: The average diameter of the gestational sac or mass is ≤ 50 mm. (Figure 3).
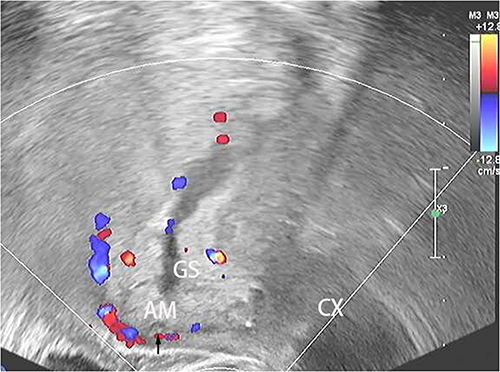 |
Figure 3 Cesarean scar pregnancy Type IIIa. The thickness of the myometrium of the anterior uterine wall is 0.8mm, and the diameter of the gestational sac is 28mm. The arrow indicates thearea where the myometrial thickness was measured. Abbreviations: AM, anterior myometrium; CX, cervix; GS, gestational sac. |
IIIb: The average diameter of the gestational sac or mass was > 50 mm or accompanied by a uterine arteriovenous fistula.
According to the new classification system for ectopic pregnancies caused by cesarean section scars, the recommended first-line surgical treatment had an overall success rate of 97.5%. This classification system has been evaluated and found to have a high success rate for the treatment of ectopic pregnancies caused by cesarean scars.
In 2017, Cali et al29 proposed an interesting ultrasound sign, the crossover sign (COS). They classified it as COS1 or COS2 based on the relationship between the endometrial line and the diameter of the gestational sac S-I (superior-inferior). This new classification system, which is mainly used to assess the relationship between the gestational sac and endometrial line, may help determine whether CSP will progress to placenta accreta. COS, myometrial thickness, and CSP typehave been proposed as potential predictors of CSP outcomes as ultrasound markers.30 However, the identification of COS is highly dependent on the experience and technical proficiency of the ultrasound physician, and there is a possibility of false positives for cervical pregnancy or false negatives for excessive forward or backward flexion of the uterus. Therefore, there are limitations to its clinical application.
Comparison
Common Grounds
Classification Purpose
All classification methods aim to assist clinical doctors in accurately diagnosing and assessing the severity of CSP through systematic classification criteria.
Classification Criteria
Although the CSP classification criteria mentioned above may not be the same, there are similarities in the classification criteria among certain classification methods. For example, the Chinese Medical Classification, Qilu Classification, and Zhang’s classification are all based on the thickness of the myometrium of the anterior uterine wall, with Type I and Type II being divided by 3 mm, while In the Zhang’s classification, the high-risk types I and II are distinguished by 3 mm, which is similar to the Chinese Medical Classification and Qilu Classification, Vial’s classification, and Kaelin’s classification, according to the direction of blastocyst growth at the scar site.
Treatment Methods
Among the classification methods reviewed, the main treatment methods included drug therapy (preferably methotrexate [MTX]), curettage (supplemented with hysteroscopy and laparoscopy if necessary), laparoscopic resection surgery, and open surgery. For CSP with different classification methods, the treatment for type I in both the Chinese Medical Classification and Qilu Classification is ultrasound-guided curettage. Both Lin’s classification and the Chinese medical classification method believe that MTX treatment for CSP has a certain effect, but the total treatment time is long and there is a possibility of treatment failure, with a success rate of 71–83%. Therefore, drug therapy alone is not recommended as the preferred treatment for CSP.25,26 A recent study based on standardized management algorithms also supports this viewpoint. Its results show that active intervention (such as curettage) for early CSP is highly safe, while expectant management is associated with a significantly increased risk of complications.31
Differences
Classification Criteria
Type II and III of the Qilu classification are still classified by the thickness of the myometrium of the anterior uterine wall and are classified into subtypes based on the diameter of the gestational sac or mass. Types II and III of the Chinese medical classification system are classified based on the location of the gestational sac and scar.
The Kaelin’s classification method is based on whether the implanted scar site has healed well.
The Lin’s classification method divides CSP into four levels based on the positional relationship between the gestational sac and the uterus.
Treatments
The specific treatment plans for each classification method are shown in Table 1.
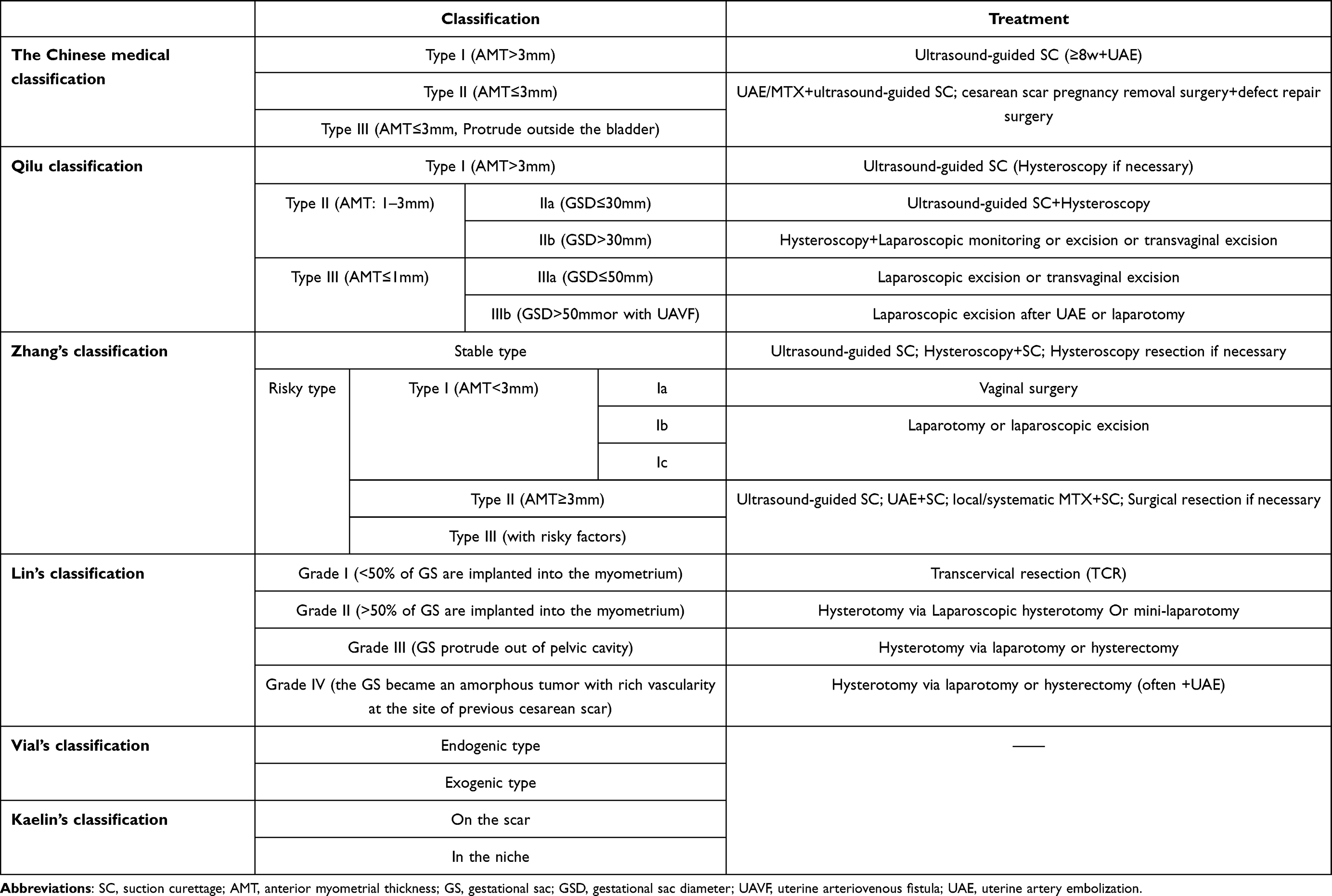 |
Table 1 Comparison of the Classifications |
Guidelines
At present, there is no unified standard for the diagnosis and treatment of CSP around the world, but the guidelines that are widely used include the “Expert opinion of diagnosis and treatment of cesarean scar pregnancy”by the Chinese Medical Association (CMA)25 and the “Cesarean scar ectopic pregnancy” by the Society for Maternal-Fetal Medicine (SMFM) in the United States.16 Both of thememphasize individualized treatment based on risk assessment, but there are significant differences in their classification criteria, treatment concepts, and recommendation intensities.
SMFM 2022 Guideline
The SMFM guidelines primarily adopt and integrate the concepts of the Vial’s classification and the Kaelin’s classification, treating them as equivalent, and simplifying CSP into two types: Type I (endogenous/on the scar type) and Type II (exogenous/in the niche type). This classification focuses on the growth direction of the gestational sac and its anatomical relationship with the scar, aiming to identify high-risk cases (especially Type II) that are highly prone to developing into placentaaccreta spectrum (PAS) and leading to catastrophic bleeding.
CMA 2016 Guideline
To standardize the diagnosis and treatment of CSP, the Chinese Medical Association released the “Consensus on Diagnosis and Treatment of Cesarean Scar Pregnancy”in 2012,24 which was updated into “Expert opinion of diagnosis and treatment of cesarean scar pregnancy” in 2016.25 The guideline adopts an ultrasound-based classification system (Types I, II, and III). The core quantitative indicator is the anterior myometrial thickness (AMT), with 3mm as the critical threshold. This classification is highly consistent with the principles of the Qilu classification, both emphasizing the predictive role of AMT in bleeding risk and prognosis.
Treatment Strategies of the Two Guidelines
In summary, the fundamental difference between the SMFM Guidelines (2022) and the CMA (2016) lies in their core logic: SMFM adopts a “risk warning”method aimed at identifying high-risk CSP and promoting active intervention. Its recommendation of intragestational MTX has been supported by recent clinical efficacy data;32 whereas CMA adopts a “risk stratification” quantitative classification approach, establishing a tiered surgical pathway with prevention of intraoperative bleeding as animportantfact and UAE as a key safeguard. Understanding this difference is crucial for reasonably drawing on different guidelines in clinical practice (Table 2).
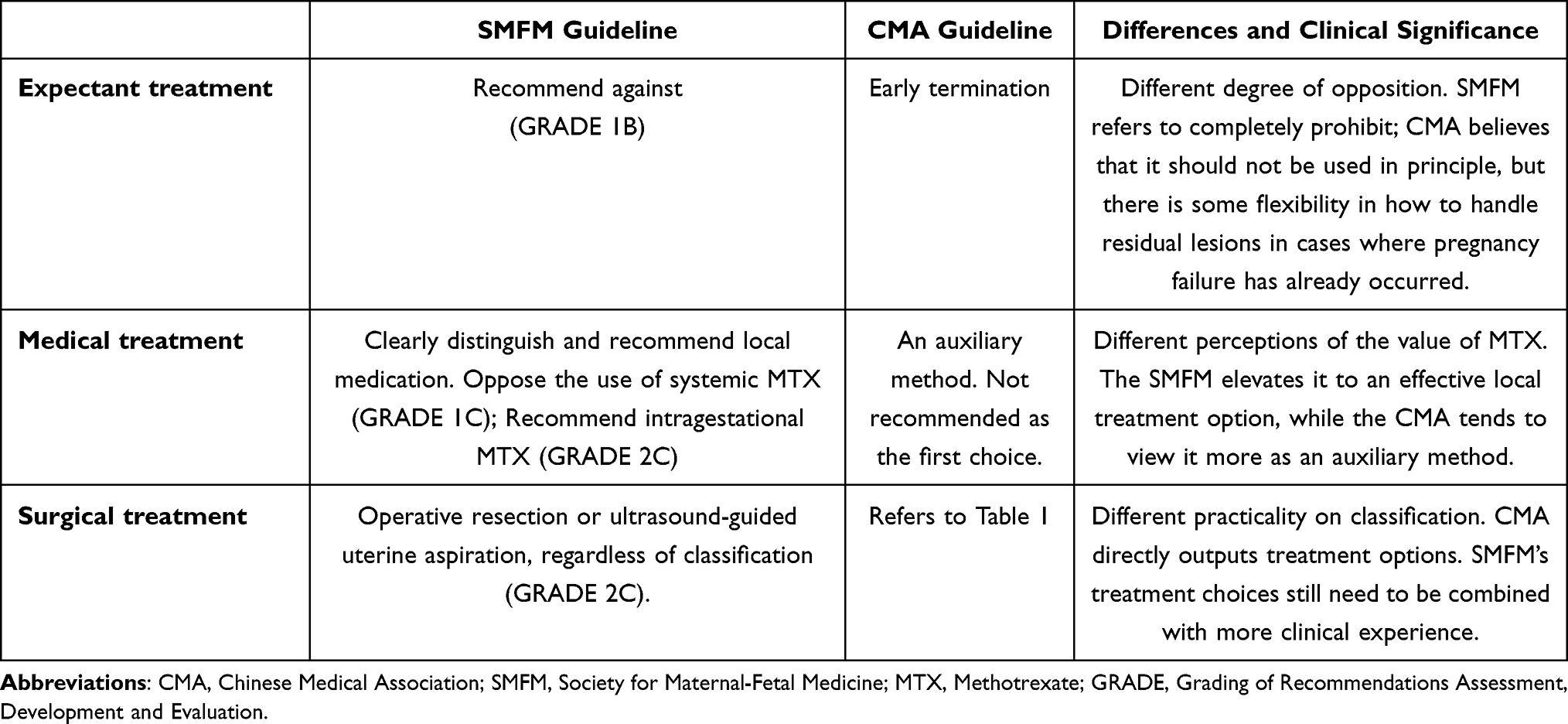 |
Table 2 Comparison of Treatment Recommendations in SMFM Guideline and CMA Guideline |
Evidence Level of Different CSP Classification Methods
Table 3 shows the six classification methods mentioned in this article using the Oxford Centre for Evidence-Based Medicine (OCEBM) 2011 level. Current evidence shows that Kaelin’s, Zhang’s, Lin’s, and Qilu’s classifications have the highest evidence level, all at level2b. However, the sample capacity of the first three classification methods was relatively small, and the Qilu classification had more detailed criteria. The Vial classification and the Chinese medical classification system had the lowest clinical evidence level (level 4).
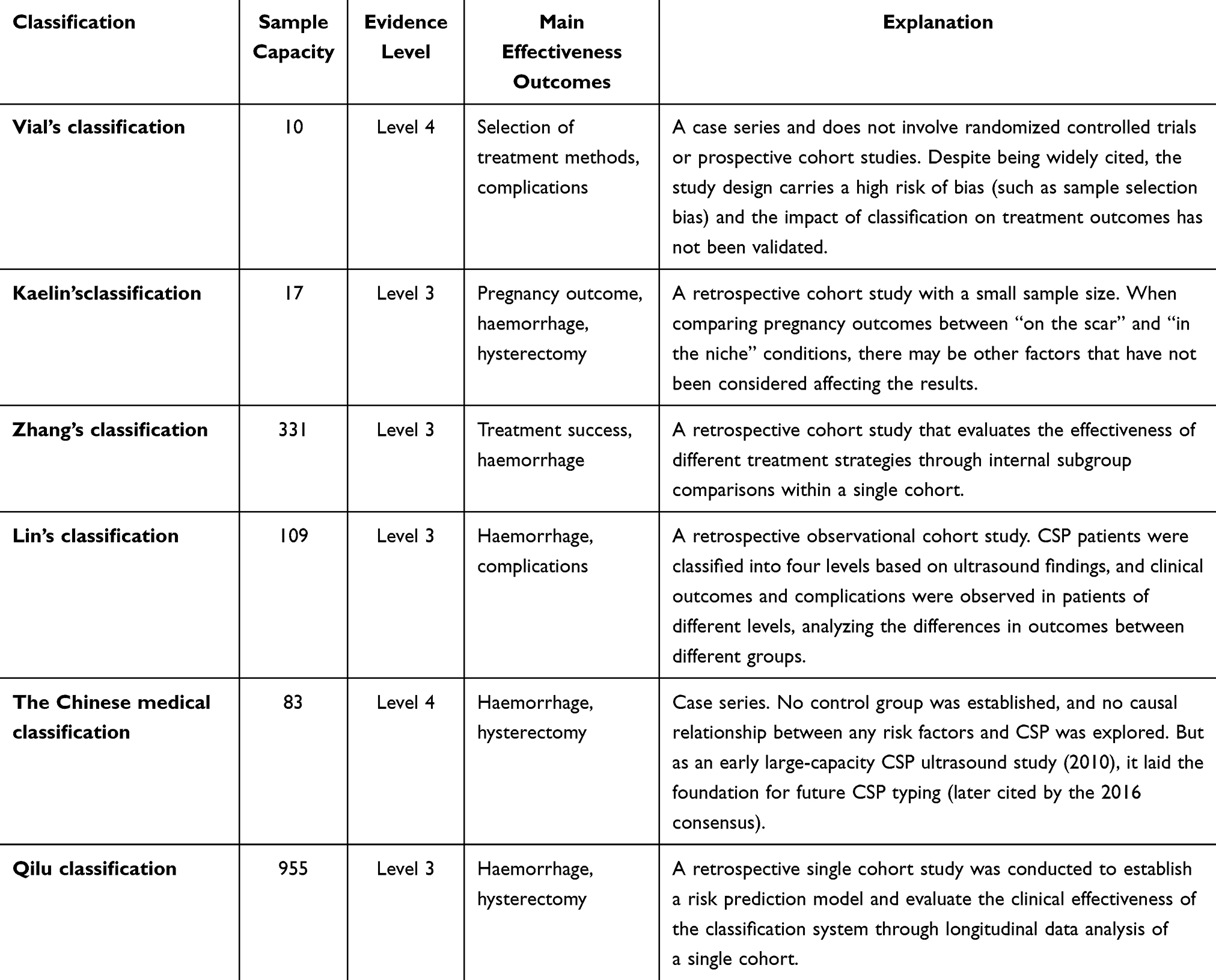 |
Table 3 Oxford Centre for Evidence-Based Medicine (OCEBM) Level of Different Types |
Conclusion
The classification method of CSP has gradually developed from traditional anatomical position (Vial’s classification) to a multi-parameter comprehensive evaluation system. Currently, two predominant management philosophies are reflected in major guidelines: the “risk alert”method (exemplified by the SMFM guidelines, which simplify CSP into 2 types) and the “risk stratification” approach (embodied by the CMA guidelines and Qilu classification, which use quantified anterior myometrial thickness and gestational sac diameter to guide tiered surgical pathways). CSP classifications such as those proposed by Zhang, Lin, and Qilu, (OCEBM Level 2b), offer detailed treatments. And Qilu classificationhas the larger sample capacity, refines the subtypes of anterior myometrial thickness and diameter of gestational sac. Therefore, Qilu classification has a better evidence level and stronger clinical applicability. However, no single classification system fits all situations; clinicians should consider the specific situation—including available ultrasound accuracy, institutional technical capacity, patient fertility desires, and complication—and refer to local guidelines to select the classifications and treatment.
Data Sharing Statement
Data sharing is not applicable to this article, as no new data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the National Key Research and Development Program of China (2022YFC2703300), Scientific Research Project of Hunan Provincial Health Commission (202105022347), Scientific Research Project of Hunan Provincial Development and Reform Commission (2021212), Natural Science Foundation of Hunan Province (2022JJ40789), and the National Natural Science Foundation of China (82301927, 82371700).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Timor-Tritsch IE, McDermott WM, Monteagudo A, et al. Extreme enhanced myometrial vascularity following cesarean scar pregnancy: a new diagnostic entity. J Matern Fetal Neonatal Med. 2022;35(25):5846–10. doi:10.1080/14767058.2021.1897564
2. Noël L, Thilaganathan B. Caesarean scar pregnancy: diagnosis, natural history and treatment. Curr Opin Obstet Gynecol. 2022;34(5):279–286. doi:10.1097/GCO.0000000000000808
3. Kirk E, Ankum P, Jakab A, et al. Terminology for describing normally sited and ectopic pregnancies on ultrasound: ESHRE recommendations for good practice. Hum Reprod Open. 2020;2020(4):hoaa055. doi:10.1093/hropen/hoaa055
4. Leone T, Padmadas SS, Matthews Z. Community factors affecting rising caesarean section rates in developing countries: an analysis of six countries. Soc Sci Med. 2008;67(8):1236–1246. doi:10.1016/j.socscimed.2008.06.032
5. Feng XL, Xu L, Guo Y, et al. Factors influencing rising caesarean section rates in China between 1988 and 2008. Bull World Health Organ. 2012;90(1):30–9,39A. doi:10.2471/BLT.11.090399
6. Jauniaux E, Zosmer N, De Braud LV, et al. Development of the utero-placental circulation in cesarean scar pregnancies: a case-control study. Am J Obstet Gynecol. 2022;226(3):399.e1–399.e10. doi:10.1016/j.ajog.2021.08.056
7. Kutlesic R, Kutlesic M, Vukomanovic P, et al. Cesarean scar pregnancy successfully managed to term: when the patient is determined to keep the pregnancy. Medicina. 2020;56(10):496. doi:10.3390/medicina56100496
8. Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies: etiology, diagnosis, and management. Obstetr Gynecol. 2006;107(6):1373–1381. doi:10.1097/01.AOG.0000218690.24494.ce
9. Jurkovic D, Hillaby K, Woelfer B, et al. First‐trimester diagnosis and management of pregnancies implanted into the lower uterine segment cesarean section scar. Ultrasound Obstet Gynecol. 2003;21(3):220–227. doi:10.1002/uog.56
10. Sekiguchi A, Okuda N, Kawabata I, et al. Ultrasound detection of lacunae-like image of a cesarean scar pregnancy in the first trimester. J Nippon Med Sch. 2013;80(1):70–73. doi:10.1272/jnms.80.70
11. Jin L, Fan G, Lang J. Early diagnosis and treatment of cesarean scar pregnancy. Chin J Reprod Contracept. 2005;25(10):630–634.
12. Panaitescu AM, Ciobanu AM, Gică N, et al. Diagnosis and management of cesarean scar pregnancy and placenta accreta spectrum: case series and review of the literature. J Ultrasound Med. 2021;40(9):1975–1986. doi:10.1002/jum.15574
13. Maheux-Lacroix S, Li F, Bujold E, et al. Cesarean scar pregnancies: a systematic review of treatment options. J Minim Invasive Gynecol. 2017;24(6):915–925. doi:10.1016/j.jmig.2017.05.019
14. Osborn DA, Williams TR, Craig BM. Cesarean scar pregnancy: sonographic and magnetic resonance imaging findings, complications, and treatment. J Ultrasound Med. 2012;31(9):1449–1456. doi:10.7863/jum.2012.31.9.1449
15. Timor-Tritsch IE, Monteagudo A, Santos R, et al. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am J Obstet Gynecol. 2012;207(1):44.e1–13. doi:10.1016/j.ajog.2012.04.018
16. Miller R, Gyamfi-Bannerman C. Society for maternal-fetal medicine consult series #63: cesarean scar ectopic pregnancy. Am J Obstet Gynecol. 2022;227(3):B9–B20. doi:10.1016/j.ajog.2022.06.024
17. D’Antonio F, Timor‐Tritsch IE, Khalil A, et al. New classification of placenta accreta spectrum disorders should include presence of cesarean scar pregnancy. Ultrasound Obstet Gynecol. 2022;59(4):563. doi:10.1002/uog.24880
18. Obore N, Jin W, Huiqin Q, et al. Pregnant women with severe factor VII deficiency undergoing cesarean section managed with a short-term regimen of recombinant factor VIIa. Maternal-Fetal Med. 2023;5(3):195–198. doi:10.1097/FM9.0000000000000194
19. Vial Y, Petignat P, Hohlfeld P. Pregnancy in a cesarean scar. Ultrasound Obstet Gynecol. 2000;16(6):592–593. doi:10.1046/j.1469-0705.2000.00300-2.x
20. Sun QL, Luo L, Gao C-Y, et al. Scoring system for the prediction of the successful treatment modality in women with cesarean scar pregnancy. Int J Gynaecol Obstet. 2019;146(3):289–295. doi:10.1002/ijgo.12881
21. Zosmer N, Fuller J, Shaikh H, et al. Natural history of early first-trimester pregnancies implanted in Cesarean scars. Ultrasound Obstet Gynecol. 2015;46(3):367–375. doi:10.1002/uog.14775
22. Kaelin Agten A, Cali G, Monteagudo A, et al. The clinical outcome of cesarean scar pregnancies implanted “on the scar” versus “in the niche”. Am J Obstet Gynecol. 2017;216(5):510.e1–510.e6. doi:10.1016/j.ajog.2017.01.019
23. Zhang H, Huang J, Wu X, et al. Clinical classification and treatment of cesarean scar pregnancy. J Obstetr Gynaecol Res. 2017;43(4):653–661. doi:10.1111/jog.13267
24. Chinese Society Of Family Planning, C.M.A. Consensus on diagnosis and treatment of cesarean scar pregnancy. Natl Med J China. 2012;92(25):1731–1733.
25. Family planning subgroup CSOO. Expert opinion of diagnosis and treatment of cesarean scar pregnancy. Chin J Obstet Gynecol. 2016;51(8):568–572.
26. Lin S, Hsieh C-J, Tu Y-A, et al. New ultrasound grading system for cesarean scar pregnancy and its implications for management strategies: an observational cohort study. PLoS One. 2018;13(8):e0202020. doi:10.1371/journal.pone.0202020
27. Yanjun K, Yanli B, Teng Z. Practical clinical classification and its application in treatment of cesarean scar pregnancy. Progress Obstetr Gynecol. 2019;28(10):731–735.
28. Ban Y, Shen J, Wang X, et al. Cesarean scar ectopic pregnancy clinical classification system with recommended surgical strategy. Obstet Gynecol. 2023;141(5):927–936. doi:10.1097/AOG.0000000000005113
29. Cali G, Forlani F, Timor‐Tritsch IE, et al. Natural history of cesarean scar pregnancy on prenatal ultrasound: the crossover sign. Ultrasound Obstet Gynecol. 2017;50(1):100–104. doi:10.1002/uog.16216
30. Jayaram P, Okunoye G, Al Ibrahim AA, et al. Expectant management of caesarean scar ectopic pregnancy: a systematic review. J Perinat Med. 2018;46(4):365–372. doi:10.1515/jpm-2017-0189
31. Bucak M, Chawla K, Mark KS, et al. Standardized algorithm for cesarean scar pregnancy management: single-center outcomes. J Matern Fetal Neonatal Med. 2025;38(1):2501693. doi:10.1080/14767058.2025.2501693
32. Swiercz G, Kabza J, Zacharska K, et al. Caesarean scar pregnancy. Analysis of medical intragestational therapy in a cohort of 35 patients. Med Stud. 2023;39(4):359–363. doi:10.5114/ms.2023.134087
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recurrent Hepatocellular Carcinoma: Patterns, Detection, Staging and Treatment
Papaconstantinou D, Tsilimigras DI, Pawlik TM
Journal of Hepatocellular Carcinoma 2022, 9:947-957
Published Date: 3 September 2022
Clinical Application of a New Cesarean Scar Pregnancy Classification and Evaluation System and a Risk Scoring System
Fu P, Zhang L, Zhou T, Wang S, Liu R
International Journal of General Medicine 2024, 17:115-126
Published Date: 16 January 2024