Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Research Hotspots and Future Trends of Oxygen Therapy for COPD: A Bibliometric and Visualization Analysis from 1973 to 2024
Received 27 August 2025
Accepted for publication 25 January 2026
Published 16 February 2026 Volume 2026:21 563591
DOI https://doi.org/10.2147/COPD.S563591
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Jiaying Ni,* Ping Xu,* Wei Lu
Department of Emergency Medicine, Longhua Hospital Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Lu, Email [email protected]
Background: Oxygen therapy is fundamental in the management of chronic obstructive pulmonary disease (COPD), and its utilization has expanded significantly in recent years. This study aimed to explore global research trends, key contributors, and emerging topics in oxygen therapy for COPD.
Methods: Publications concerning oxygen therapy for COPD from 1973 to 2024 were retrieved from the Web of Science Core Collection. A bibliometric analysis was conducted employing VOSviewer, CiteSpace, and R 4.3.3. The contributions of countries, institutions, authors, and journals were systematically assessed.
Results: A total of 1,977 publications were analyzed, indicating an annual growth rate of 8.43%. The USA led with 359 publications (18.2%), followed by China with 167 (8.4%) and Italy with 115 (5.8%). The leading institution was Assistance Publique Hôpitaux de Paris, which produced 98 publications. Key journals in this field included CHEST, leading with 149 publications, followed by Respiratory Medicine (96) and Respiratory Care (87). Prominent authors included Maltais François, who contributed 25 publications and received 795 citations. Core keywords encompassed terms such as “mortality” (201 occurrences), “survival” (151 occurrences), and “therapy” (182 occurrences). Burst keyword analysis highlighted a recent emphasis on “interstitial lung disease” (2020– 2024) and “high-flow nasal cannula” (2022– 2024).
Conclusion: Oxygen therapy research for COPD has grown steadily since 1973. Keyword burst and temporal analyses indicate a recent shift of research focus from general oxygen supplementation toward modality-specific and context-specific strategies, including HFNC, exacerbation-related oxygen use, comorbidity-oriented management (eg, COPD–ILD overlap), and respiratory failure–related care, reflecting an increasing emphasis on precision and individualized oxygen therapy.
Keywords: oxygen therapy, chronic obstructive pulmonary disease, bibliometric analysis, VOSviewer, CiteSpace
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory airway disease.1 It is characterized by inflammation and remodeling of the lower airways and lung parenchyma, activation of inflammatory and immune processes, and persistent airflow limitation that is usually progressive, often associated with airway and alveolar abnormalities.2 COPD poses a major global health threat, affecting an estimated 300 million people in 2017, with the World Health Organization predicting it will become the third leading cause of death by 2030.3,4 In China, COPD affects a large population, with a diagnosis rate ranging from 23.61% to 30.00%, imposing a substantial burden on families and society.5 Management strategies for COPD include pharmacological treatments, lifestyle modifications, and physical therapy.6 Oxygen therapy is a key intervention, particularly for severe cases, to improve blood oxygen levels. Long-term oxygen therapy (LTOT) significantly reduces hospitalizations, extends survival, and enhances life quality in COPD patients.7
Oxygen therapy, which involves providing additional oxygen to improve blood oxygen saturation, is a well-established treatment for COPD patients.8 The primary types of oxygen therapy include LTOT and intermittent oxygen therapy. LTOT is primarily used for severe COPD patients, particularly those with resting blood oxygen saturation below 90%.9 Intermittent oxygen therapy is suitable for patients whose blood oxygen saturation decreases only during physical activity, providing temporary oxygen support to alleviate symptoms.7 In recent years, the application of oxygen therapy among COPD patients has become increasingly widespread, especially with the rise of home oxygen therapy.10 This widespread adoption has significantly shifted the focus of research, with growing emphasis on the accessibility, safety, and quality of home-based treatment.11,12 Research continues to explore the optimal oxygen concentration and flow settings, as well as the impact of various oxygen therapy methods on COPD prognosis.13 Still, the potential risks of oxygen therapy, such as oxygen toxicity and carbon dioxide retention, highlight the importance of adhering to established guidelines and maintaining careful monitoring during treatment.14
Bibliometrics is a quantitative method that employs mathematical and statistical tools to analyze academic literature. It examines patterns such as author contributions, institutional affiliations, citation metrics, and keyword trends to map the intellectual structure of a field.15–17 Currently, there are bibliometric analyses available on topics such as COPD and its relation to exercise and drug therapies.18,19 However, there is no comprehensive bibliometric analysis specifically focused on research hotspots and future trends in oxygen therapy for COPD. Therefore, this study presents the first comprehensive bibliometric analysis of oxygen therapy for COPD, aiming to map global research activity, identify key contributors and collaborations, and highlight both established and emerging research topics.
Materials and Methods
Data Source and Search Strategy
A comprehensive literature search covering the period from 1973 to 2024 was conducted using the Web of Science Core Collection (WoSCC) database on 29 September 2024. The search formula used was as follows: TS= (((oxygen) NEAR/1 (therapy OR treatment OR strategy)) OR Oxygenation*) AND TS = (chronic obstructive pulmonary disease* OR COPD* OR chronic airflow obstruction* OR chronic obstructive lung disease*).18,20 Only English-language research articles were included. This study exported the data using “Full record and cited references” and “plain text” formats. The extracted information included countries/regions, institutions, journals, publication counts, citation metrics, author data, and keywords.
Data Analysis and Visualization
Three primary tools were used for bibliometric analysis and visualization: VOSviewer (version 1.6.20), CiteSpace (version 6.3.R1), and R 4.3.3. VOSviewer was employed to construct bibliometric networks focusing on co-authorship, institutional collaboration, and co-citation patterns.21 In these visualizations, the node size reflected the number of publications or citations, color coding indicated cluster associations, and the links represented collaboration or co-occurrence relationships. Keyword co-occurrence analysis helped reveal prominent research trends and key collaborations across countries and institutions.21,22
CiteSpace was used to detect citation bursts and identify emerging research themes. The software was set to analyze publications from 1973 to 2024, with one-year time slices. The node type was set to keywords, and network pruning techniques were applied to streamline the visualizations.23 For analyzing research hotspots and trends, “Keywords Plus” from WoSCC instead of author keywords were utilized, as it offers more comprehensive coverage of research topics.
R 4.3.3 facilitated thematic evolution analysis and the visualization of global distribution networks, allowing for the identification of prominent research areas and international collaboration patterns.24 This study also incorporated bibliometric indices such as the H-index, which measures research productivity and citation impact, the G-index, which gives more weight to highly cited articles, and the M-index, reflecting the growth of the H-index over time.25,26 To evaluate the prominence of journals, Journal Citation Reports (JCR) rankings and impact factors (IF), collected from the most recent JCR, were included in the analysis.
Results
Overall Publication Trends
A total of 1,977 publications on oxygen therapy in COPD indexed between 1973 and 2024 were identified, as shown in Figure S1. These 1,977 documents reflect an annual growth rate of 8.43%. The analysis of authorship indicates that 10,417 authors contributed to these publications, with 72 documents being single-authored. International co-authorship is evident in 18.41% of the publications, highlighting the increasing cross-border collaborations in this research field. Moreover, the average number of citations per document is 32.24, indicating a growing impact of these studies within the scientific community. The trend in the number of publications, illustrated in Figure 1, demonstrates a marked growth trajectory, especially after 2010. Before 1980, the number of publications remained below five annually, but a significant increase commenced in the early 2010s, culminating in a peak of 123 publications in 2020. After 2020, the number of publications entered a plateau phase.
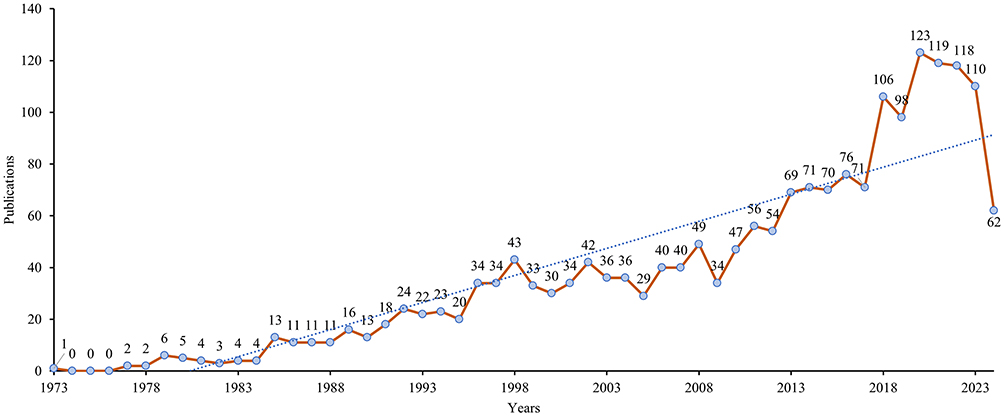 |
Figure 1 Annual number of publications. |
Countries/Regions Analysis
As shown in Table 1, the USA leads with 359 publications, representing 18.2% of the total, followed by China (167, 8.4%) and Italy (115, 5.8%). Both the USA and Canada exhibit notable levels of international collaboration, as evidenced by their multiple-country publication (MCP) ratios of 0.139 and 0.42, respectively. China, Italy, and Japan also contribute significantly, albeit with lower MCP ratios (Figure 2A). In terms of total citations, the USA ranks first with 14,374 citations, followed by Spain (8,234) and the UK (5,052), highlighting their influential roles in the research landscape (Table 1).
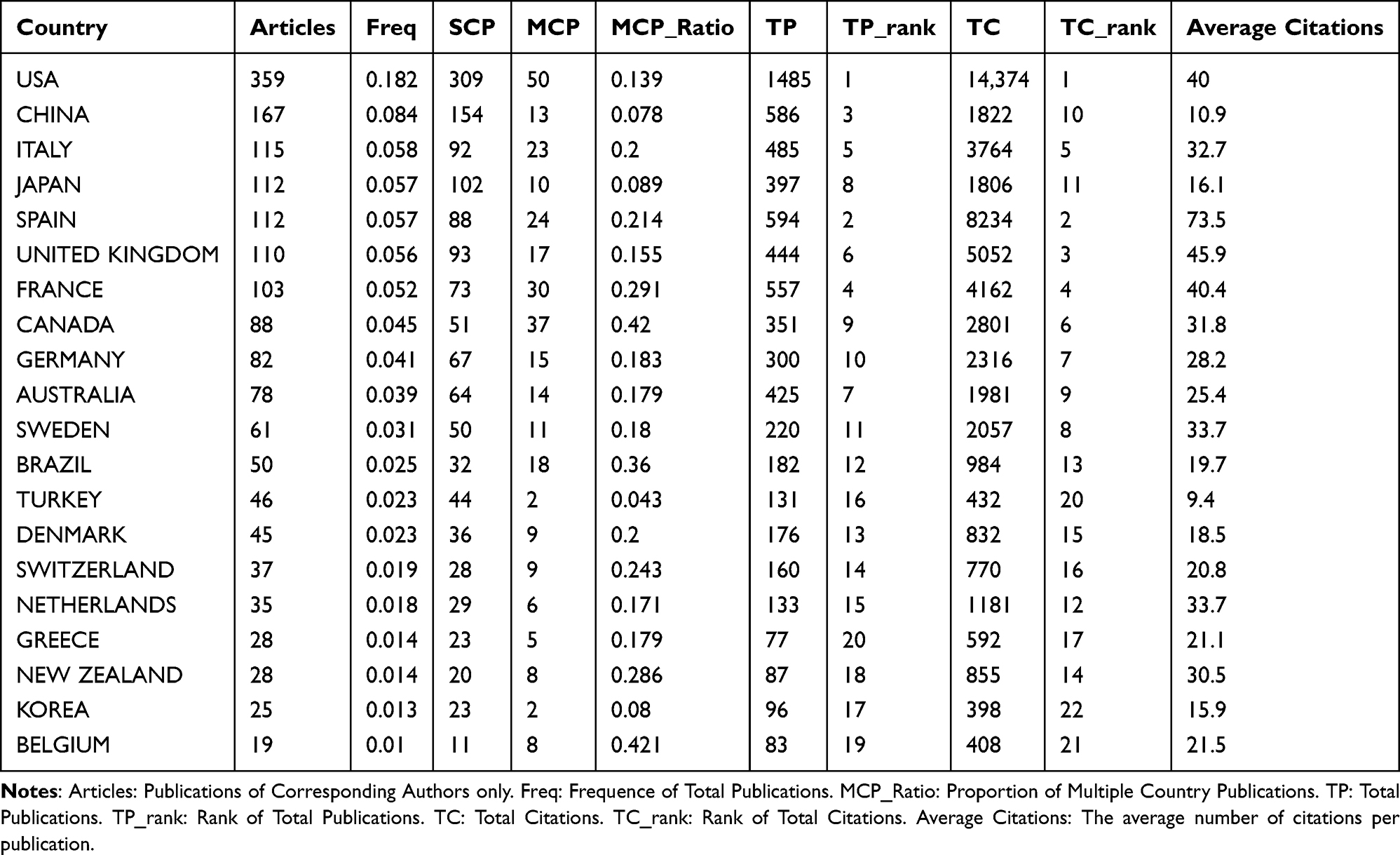 |
Table 1 Publication and Citation Profiles of Leading Countries |
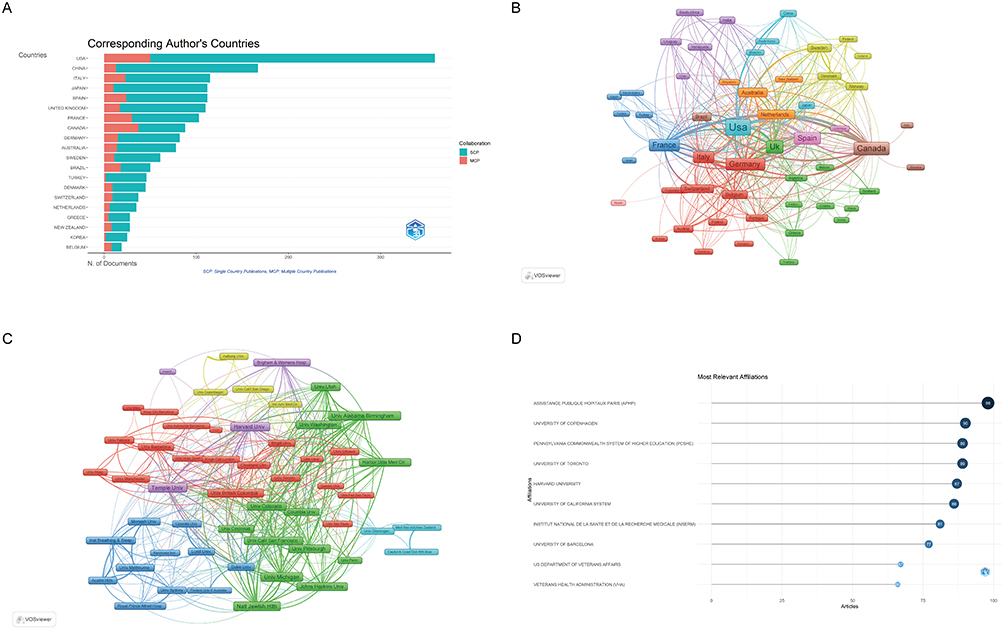 |
Figure 2 Analysis of countries and institutions. (A) Distribution of corresponding author’s publications by country. N, number. (B) Visualization map depicting the collaboration among different countries. (C) Visualization map depicting the collaboration among different institutions. (D) Top ten institutions by article count and rank. |
Figure 2B illustrates the international collaboration network, where the USA and Canada act as central nodes, maintaining extensive connections with other countries, thus playing pivotal roles in advancing research. Meanwhile, China, Italy, and Japan demonstrate more regionally concentrated collaborations, indicating a focus on national or localized networks.
Institutional Analysis
An analysis of institutional affiliations, as shown in Figure 2C, reveals that among the 177 institutions involved in international collaborations with a minimum of 6 articles, Temple University has the highest number of collaborations with other countries (153), followed by the University of Michigan (148) and National Jewish Health (140). These institutions form strong domestic and international collaborative networks, as demonstrated by their total link strengths (Table 2). Figure 2D reveals that Assistance Publique Hôpitaux de Paris (APHP) leads with 98 publications. This is followed by the University of Copenhagen (90), the Pennsylvania Commonwealth System of Higher Education (89), and the University of Toronto (89). Figure 2D also highlights the most relevant affiliations in the field, where APHP, the University of Copenhagen, and Harvard University are among the top contributors. Their positions in the collaboration network underscore their central roles in driving research developments.
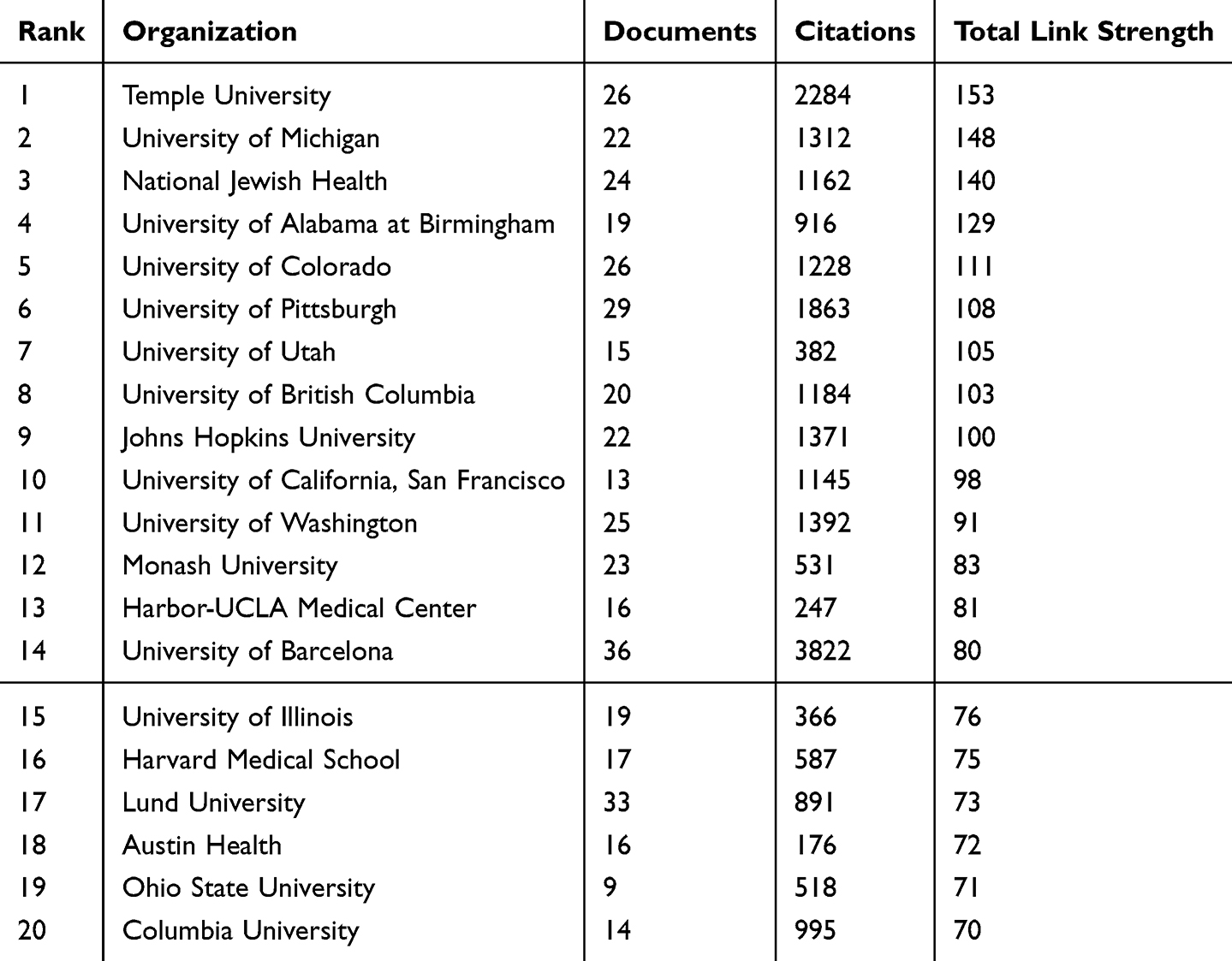 |
Table 2 Top 20 Institutions Ranked by Total Link Strength |
Authors Analysis
A total of 10,417 authors have contributed to this research field from 1973 to 2024. Table S1 delineates the high-impact authors, with Maltais François leading the list with 25 publications and 795 citations, indicating a substantial influence within the field. Criner Gerard J. and Martinez Fernando J. also rank prominently, with 22 and 16 publications, respectively. The co-authorship network, depicted in Figure S2, illustrates the collaboration patterns among leading authors. Several clusters are evident, each representing distinct research foci. The red cluster is dominated by Martinez Fernando J. and Criner Gerard J., displaying strong connections to other influential authors such as Han Meilan K. and Bourbeau Jean. The yellow cluster is led by O’Donnell Denis E., while the purple cluster is centered on Wedzicha Jadwiga A. These distinct clusters underscore the specialization and collaboration among authors within various subfields.
Journal Analysis
The collected papers are published across 490 journals, with CHEST leading with 149 publications, followed by Respiratory Medicine (96) and Respiratory Care (87) (Table S2). These journals cover diverse fields such as pulmonology, intensive care, and respiratory therapy. Figure S3a visualizes the co-authorship network of journals, where the most influential journals, including CHEST, European Respiratory Journal, and American Journal of Respiratory and Critical Care Medicine, occupy central positions with extensive links to other journals.
Co-citation analysis, as presented in Figure S3b, provides further insights into the relationships between journals and their influence on the field. CHEST and the European Respiratory Journal appear as central nodes, representing journals with strong associations with others in the network. Alongside them, the American Journal of Respiratory and Critical Care Medicine and Thorax also demonstrate significant impact, reflected by frequent co-citations, indicating their importance in ongoing research. Among all the journals, the American Journal of Respiratory and Critical Care Medicine boasts the highest IF (19.3), emphasizing its leading role, while the European Respiratory Journal and CHEST also maintain high impact factors of 16.6 and 9.5 (Table S2).
Keywords Analysis
The top 20 keywords with the highest occurrences are listed in Table 3. Besides the topic keywords of this study, such as “obstructive pulmonary disease”, “COPD”, and “oxygen therapy”, notable keywords include “mortality” (201 occurrences, 807 total link strength), “survival” (151 occurrences, 673 total link strength), and “quality-of-life” (120 occurrences, 543 total link strength). The keyword evolution network reveals a distinct temporal shift in research focus within oxygen therapy for COPD. In the early period (before ~2000), research centered on fundamental pathophysiology, with keywords such as hypoxemia, gas exchange, hemodynamics, and cor pulmonale occupying central network positions. During the intermediate period (approximately 2000–2015), the focus moved toward therapeutic effectiveness and patient-centered outcomes, reflected by increased centrality of oxygen therapy, exercise, dyspnea, noninvasive ventilation, mechanical ventilation, and survival. In the recent period (after ~2015), emerging keywords including exacerbations, management, adults, guidelines, interstitial lung disease, and high-flow nasal cannula have gained prominence and act as bridges across clusters, indicating a transition toward context-specific, modality-oriented, and population-tailored oxygen strategies in COPD research (Figure 3A).
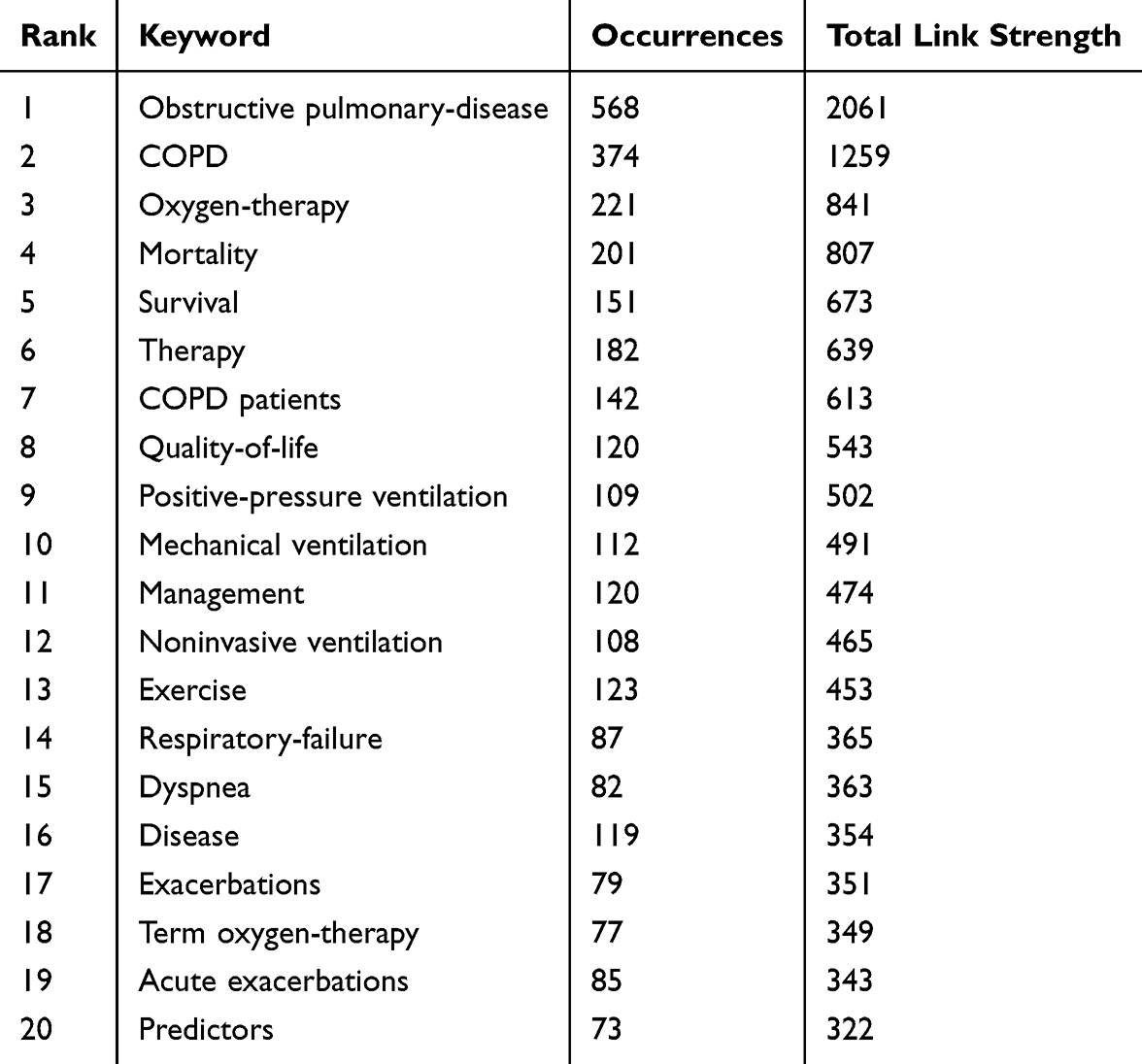 |
Table 3 Top Keywords by Occurrence and Collaboration Strength in COPD Research |
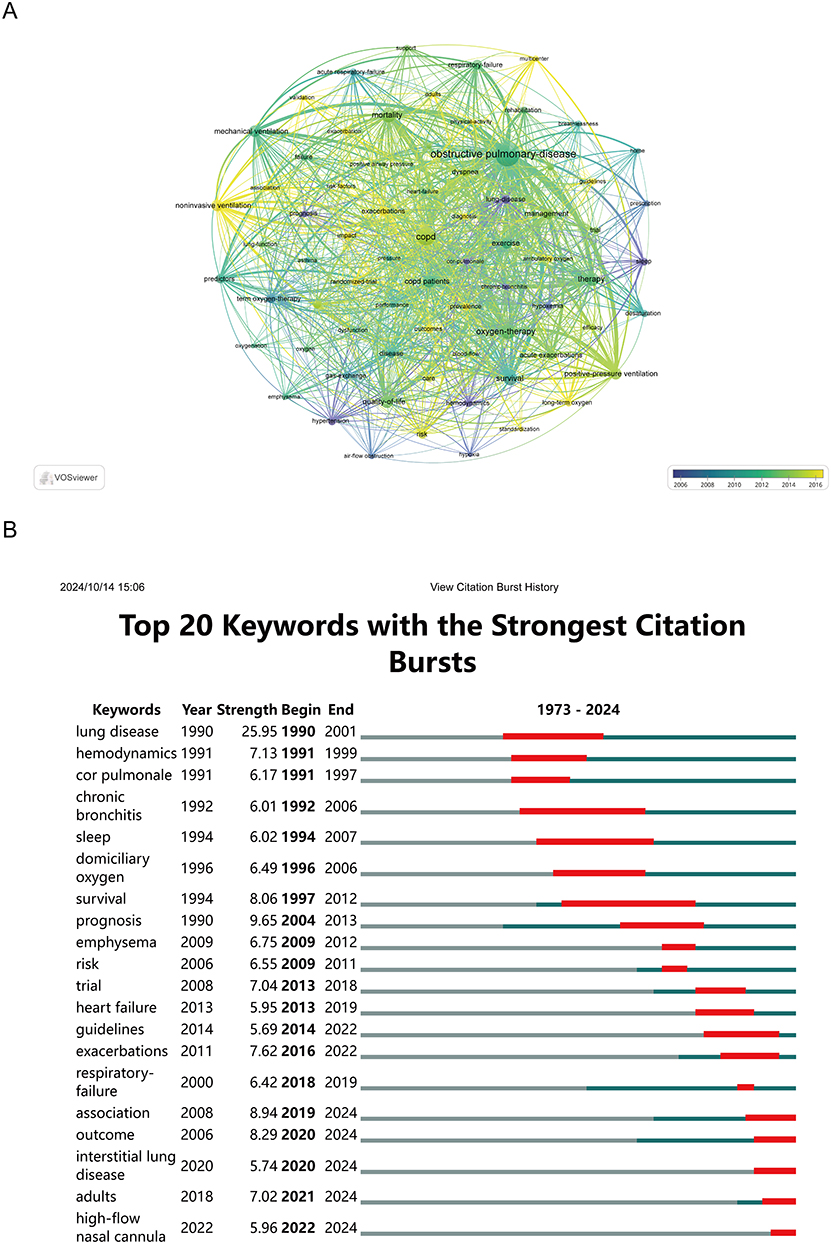 |
Figure 3 Analysis of keywords. (A) Visual analysis of keyword co-occurrence network analysis. (B) Top 20 Keywords with the Strongest Citation Bursts. |
The analysis of citation bursts, depicted in Figure 3B, identifies the top 20 keywords with the strongest citation bursts. For example, keywords such as “lung disease”, “hemodynamics”, and “cor pulmonale” experienced strong bursts in the 1990s. More recent bursts, including “exacerbations” and “guidelines”, have gained prominence from 2014 onwards, indicating a shift towards more specific clinical management aspects of pulmonary diseases. The figure highlights emerging keywords like “interstitial lung disease” (2020–2024), “adults” (2021–2024), and “high-flow nasal cannula” (2022–2024), which have recently gained attention, marking a shift towards a growing focus on advanced therapeutic strategies tailored to distinct respiratory conditions.
Discussion
The publication trend shows a gradual increase in the number of studies from 1973 in the field of oxygen therapy for COPD. Future research will focus on age-specific oxygen strategies, the use of high-flow nasal cannula (HFNC), preventing exacerbations, managing comorbidities like COPD-ILD overlap, and optimizing respiratory failure treatments, all aimed at improving personalized care and patient outcomes.
Our bibliometric analysis of COPD oxygen therapy research reveals a clear expansion in scholarly output over the past five decades. Using annual publication counts, the compound annual growth rate (CAGR) from 1977 (2 articles) to 2000 (30 articles) was approximately 12.5%, indicating rapid early growth as foundational research on pathophysiology and basic oxygen therapy mechanisms accumulated. In contrast, the CAGR from 2000 to 2023 (30 to 110 articles) stabilized at approximately 5.8%, reflecting sustained research activity with a maturation of clinical and applied topics. These growth rates for COPD oxygen therapy are consistently above global averages for scientific publication growth. According to Bornmann et al (2021), the overall growth rate of scientific publications across disciplines in major bibliographic databases is about 4.1% per year across extended timeframes, representing the typical “doubling” pace of modern science output.27
Additionally, the UNESCO Science Report 2021 documents that worldwide scientific output was 21% higher in 2019 than in 2015, corresponding to an approximate global publication growth rate of 4–5% per year over that period.28 The comparatively higher growth rate in COPD oxygen therapy suggests that this field is expanding faster than the average rate of science production, likely driven by rising clinical burden, technological innovation, and interdisciplinary interest in tailored oxygen strategies for chronic respiratory disease.
General Information on Authors, Countries, Institutions, and Journals
Key authors like Maltais François, Criner Gerard J., and Martinez Fernando J. are based in institutions within high-output countries like Canada and the USA. These authors have high citation counts and total link strengths, reflecting their substantial influence and frequent collaborations with other prominent researchers. They participated in the analysis of existing literature and, through expert consensus discussions, proposed important directions for future COPD research.29–31
The USA leads in publications The prominence of institutions like the University of California System, Harvard University, and the Pennsylvania Commonwealth System of Higher Education demonstrates the extensive infrastructure and collaborative networks within the USA. The high citation count for USA-based research further emphasizes the country’s influential role in advancing this field. The USA’s extensive and well-established research infrastructure, backed by substantial funding from government agencies, private institutions, and research-focused universities, facilitates comprehensive studies and large-scale clinical trials.32,33
The top journals for publishing COPD-related oxygen therapy research include CHEST, European Respiratory Journal, and the American Journal of Respiratory and Critical Care Medicine. These journals have high impact factors (eg, American Journal of Respiratory and Critical Care Medicine with an IF of 19.3), which attract high-quality studies and ensure widespread dissemination of findings.34 These journals cover topics such as pulmonology, respiratory care, and critical care, reflecting the interdisciplinary nature of COPD research.35–37
Research Topic Evolution: Findings from Keyword Analysis
The keyword evolution network reveals a clear temporal shift in research focus within oxygen therapy for COPD. In the early period (before ~2000), research primarily focused on the pathophysiology of COPD and its complications, including hypoxemia, impaired gas exchange, hemodynamic alterations, and cor pulmonale. This aligns with the traditional focus of oxygen therapy research on the physiological effects of correcting hypoxemia and its impact on organ systems.38 Long-term oxygen therapy has been demonstrated to improve survival in patients with severe hypoxemic COPD. During the intermediate period (approximately 2000–2015), research gradually shifted toward therapeutic efficacy and patient-centered outcomes. Numerous studies evaluated the effects of oxygen therapy on exercise capacity, dyspnea relief, the need for mechanical ventilation, and survival. Noninvasive ventilation (NIV) emerged as a key component in the management of acute respiratory failure during COPD exacerbations, significantly reducing intubation rates and treatment failure.39 In this phase, research increasingly emphasized individualized oxygen therapy, perioperative optimization, and integration with respiratory training and rehabilitation. In the recent period (after ~2015), keywords such as “exacerbations”, “management”, “guidelines”, “adults”, “interstitial lung disease”, and “high-flow nasal cannula” have gained prominence, reflecting a transition toward context-specific, modality-oriented, and population-tailored oxygen strategies. This trend is further supported by the keyword burst analysis, which indicates that HFNC, adults, and interstitial lung disease have recently attracted increased attention. Furthermore, recent clinical guidelines emphasize that oxygen therapy in COPD should be individualized, based on criteria such as resting hypoxemia, exercise-induced desaturation, and severity of acute exacerbations. Oxygen delivery should be adjusted according to arterial blood gas analysis and clinical symptoms.40 This evolution, from mechanistic studies to efficacy evaluation and then to context-specific, guideline-based strategies, reflects the overall trend of oxygen therapy research progressing toward precision clinical application.
Recent Bursts
The keyword analysis provided insights into research hotspots, revealing a shift towards more specialized terms in recent years. Specifically, the recent keyword bursts in the past five years highlight emerging focus areas:
The keyword “High-flow Nasal Cannula (2022–2024)” reflects an increased focus on noninvasive ventilation techniques that have shown promise in enhancing patient outcomes. HFNC therapy has gained popularity due to its ability to provide stable oxygen delivery and improve patient comfort, aligning with recent advancements in COPD management strategies.41,42 A recent systematic review and meta-analysis compared HFNC with conventional oxygen therapy (COT) in hypercapnic COPD patients. In cases of acute hypercapnia, HFNC significantly reduced arterial partial pressure of carbon dioxide (PaCO2) and treatment failure rates, though it did not show significant improvements in arterial partial pressure of oxygen (PaO2) or respiratory rate (RR). In chronic hypercapnic COPD, HFNC was linked to lower exacerbation rates, despite not achieving significant improvements in PaCO2 or PaO2.43,44 However, despite the increasing prominence of high-flow nasal cannula (HFNC) in COPD research, several limitations constrain its current clinical utility. Meta‑analyses suggest that while HFNC likely reduces acute exacerbation rates and may lower hospital admissions in patients with chronic hypercapnic COPD, its effect on mortality remains uncertain and evidence quality is generally low to moderate, indicating a need for more robust trials with longer follow‑up (systematic review and meta‑analysis).45 In acute hypercapnic COPD, HFNC has demonstrated short‑term reductions in PaCO2 and treatment failure relative to conventional oxygen therapy, but improvements in PaO2 and respiratory rate are not consistently observed across studies.42 Practical challenges also persist. Optimal patient selection criteria, including defining disease severity thresholds and identifying phenotypes most likely to benefit, are not yet standardized. Variability in HFNC settings (eg, flow rate, duration of use) across trials contributes to heterogeneity in outcomes and limits generalizability. Tolerance and adherence issues have been reported in home settings, further complicating implementation in routine care.46 Taken together, HFNC is a promising noninvasive respiratory support for COPD, but substantial evidence gaps remain, necessitating large, well-designed trials and real-world studies to define its comparative efficacy, optimal patient selection, and guideline-based role.
The keyword “Adults (2021–2024)” reflects a growing emphasis on developing advanced therapeutic strategies tailored to adult populations, especially in the context of COPD management. This focus is likely driven by demographic shifts and the rising prevalence of COPD among aging adults, necessitating age-specific management protocols in oxygen therapy.47,48 Older adults, in particular, have a higher prevalence of COPD, mainly due to prolonged exposure to risk factors and the natural aging process. This population often experiences “inflamm-aging”, a persistent, low-grade systemic inflammation that not only reduces lung function and overall health status but also limits daily activities and contributes to common comorbidities. Age-related physiological changes further complicate COPD management in older adults. Factors such as altered pharmacokinetics and pharmacodynamics, polypharmacy, and potential drug interactions pose significant challenges, affecting both treatment efficacy and safety. As current therapies mainly aim to alleviate symptoms, there is a pressing need for alternative approaches that target disease progression.49–51
The keyword “Interstitial Lung Disease (2020–2024)” signals an expanding research focus to encompass COPD-related comorbidities, emphasizing the overlap between COPD and interstitial lung disease (ILD). This overlap has significant implications for comprehensive patient management, as these coexisting conditions often lead to worse clinical outcomes.52,53 This overlap presents diagnostic challenges, as symptoms such as dyspnea and hypoxemia are nonspecific, and definitive PH diagnosis often requires invasive testing, while reliable biomarkers and imaging criteria remain limited.54 One critical complication is pulmonary hypertension, which is frequently observed in patients with both COPD and ILD. This form of pulmonary hypertension is distinct, characterized by the loss of small pulmonary vessels, potentially exacerbated by long-term tobacco exposure, and leads to reduced oxygen uptake, clinical deterioration, and increased mortality risk.55 The unique pathomechanisms of pulmonary hypertension in chronic lung diseases pose challenges for treatment, as most therapies approved for pulmonary arterial hypertension have proven ineffective or even harmful, highlighting the distinct pathophysiology and treatment challenges. However, inhaled Treprostinil has shown promise in enhancing exercise capacity among patients with ILD and pulmonary hypertension,56 yet long-term survival benefits, efficacy in COPD-predominant PH, and integration into standardized, phenotype-specific management remain unresolved. These findings underscore the urgent need for safe, effective treatments and non-invasive diagnostic tools to better identify and manage pulmonary hypertension in patients with COPD and ILD.57,58
The keyword “Respiratory Failure (2019–2024)” signifies an important area of focus in COPD management, reflecting the severe complications that often arise in the advanced stages of the disease.59,60 Managing respiratory failure in COPD has become increasingly critical, with a strong emphasis on acute care and noninvasive ventilation techniques. Noninvasive ventilation has been the preferred first-line treatment for over 40 years in conditions such as COPD and cardiogenic pulmonary edema. However, its use in treating acute hypoxemic respiratory failure has yielded mixed results, presenting higher risks of therapy failure (intubation) and increased mortality.61–63
Significance and Limitations
This study offers several practical implications for researchers and clinicians. It provides a comprehensive overview of current research hotspots, identifies leading authors, institutions, and journals, and highlights emerging trends in oxygen therapy for COPD. By tracking active keywords and recent citation bursts, it clarifies how research priorities have shifted over time, revealing areas such as high-flow nasal cannula use, COPD-ILD overlap, and pulmonary hypertension that warrant further investigation. These insights can inform evidence-based clinical strategies, patient management protocols, and health policy decisions, guiding resource allocation, guideline development, and the design of future studies to address unmet needs in COPD care.
However, the study has certain limitations. It relied on a single database, which may not fully capture the breadth of literature in this field, potentially excluding relevant books and editorials. Moreover, the analysis was restricted to English-language publications, potentially omitting valuable research published in other languages. Additionally, the focus on specific keywords might have overlooked broader concepts related to COPD management and oxygen therapy. This study is based on bibliometric analysis of published literature and, as such, provides a descriptive, pattern-based overview rather than hypothesis-driven or experimental evidence. Consequently, the identification of clusters, keyword bursts, or emerging topics reflects trends in the literature but does not constitute definitive evidence of research priorities or clinical importance. Interpretations drawn from these patterns should therefore be considered exploratory and indicative rather than conclusive. Future studies should consider incorporating multiple bibliographic databases and broader, more inclusive search terms to capture a wider range of publications, including gray literature and studies in related respiratory conditions, such as ILD.
Conclusion
The publication trend in oxygen therapy research for COPD shows a gradual increase in studies from 1973, with a notable surge beginning in the early 2010s. Future research in oxygen therapy for COPD is shifting towards personalized approaches, focusing on age-specific strategies, high-flow nasal cannula use, exacerbation management, COPD-ILD comorbidity, and improved treatments for respiratory failure to enhance patient outcomes.
Abbreviations
COPD, chronic obstructive pulmonary disease; LTOT, Long-term oxygen therapy; HFNC, high-flow nasal cannula; COT, conventional oxygen therapy.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Vogelmeier CF, Román-Rodríguez M, Singh D, Han MK, Rodríguez-Roisin R, Ferguson GT. Goals of COPD treatment: focus on symptoms and exacerbations. Respir Med. 2020;166:105938. doi:10.1016/j.rmed.2020.105938
2. Uwagboe I, Adcock IM, Lo Bello F, Caramori G, Mumby S. New drugs under development for COPD. Minerva Med. 2022;113(3):471–13. doi:10.23736/S0026-4806.22.08024-7
3. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
4. Kahnert K, Jörres RA, Behr J, Welte T. The diagnosis and treatment of COPD and its comorbidities. Dtsch Arztebl Int. 2023;120(25):434–444. doi:10.3238/arztebl.m2023.027
5. Zhu B, Wang Y, Ming J, Chen W, Zhang L. Disease burden of COPD in China: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:1353–1364. doi:10.2147/COPD.S161555
6. Labaki WW, Rosenberg SR. Chronic obstructive pulmonary disease. Ann Intern Med. 2020;173(3):Itc17–itc32. doi:10.7326/AITC202008040
7. Branson RD. Oxygen Therapy in COPD. Respir Care. 2018;63(6):734–748. doi:10.4187/respcare.06312
8. Halpin DMG, Criner GJ, Papi A, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. the 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2021;203(1):24–36. doi:10.1164/rccm.202009-3533SO
9. Edwards L, Perrin K, Williams M, Weatherall M, Beasley R. Randomised controlled crossover trial of the effect on Ptco2 of oxygen-driven versus air-driven nebulisers in severe chronic obstructive pulmonary disease. Emerg Med J. 2012;29(11):894–898. doi:10.1136/emermed-2011-200443
10. Wiles KS. 2023 year in review: home oxygen therapy. Respir Care. 2024;69(9):1182–1188. doi:10.4187/respcare.12070
11. Khor YH, Ekstrom M. The benefits and drawbacks of home oxygen therapy for COPD: what’s next? Expert Rev Respir Med. 2024;18(7):469–483. doi:10.1080/17476348.2024.2379459
12. Jacome C, Jacome M, Correia S, et al. Effectiveness, adherence and safety of home high flow nasal cannula in chronic respiratory disease and respiratory insufficiency: a systematic review. Arch Bronconeumol. 2024;60(8):490–502. doi:10.1016/j.arbres.2024.05.001
13. Fu Y, Chapman EJ, Boland AC, Bennett MI. Evidence-based management approaches for patients with severe chronic obstructive pulmonary disease (COPD): a practice review. Palliat Med. 2022;36(5):770–782. doi:10.1177/02692163221079697
14. Piraino T, Madden M, Roberts KJ, Lamberti J, Ginier E, Strickland SL. AARC clinical practice guideline: management of adult patients with oxygen in the acute care setting. Respir Care. 2022;67(1):115–128. doi:10.4187/respcare.09294
15. Jiang S, Liu Y, Zheng H, et al. Evolutionary patterns and research frontiers in neoadjuvant immunotherapy: a bibliometric analysis. Int J Surg. 2023;109(9):2774–2783. doi:10.1097/JS9.0000000000000492
16. Pei Z, Chen S, Ding L, et al. Current perspectives and trend of nanomedicine in cancer: a review and bibliometric analysis. J Control Release. 2022;352:211–241. doi:10.1016/j.jconrel.2022.10.023
17. Reddy VP, Singh R, McLelland MD, et al. Bibliometric analysis of the extracranial-intracranial bypass literature. World Neurosurg. 2022;161:198–205.e195. doi:10.1016/j.wneu.2022.01.095
18. Zhen G, Yingying L, Jingcheng D. Drug therapies for COPD: a bibliometric review from 1980 to 2021. Front Pharmacol. 2022;13:820086. doi:10.3389/fphar.2022.820086
19. Chen M, Zhang Y, Mao Y, et al. Bibliometric analysis of exercise and chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2023;18:1115–1133. doi:10.2147/COPD.S406955
20. Zhou Y, Liu X, Wu W. Mapping the global research landscape and hotspot of exercise therapy and chronic obstructive pulmonary disease: a bibliometric study based on the web of science database from 2011 to 2020. Front Physiol. 2022;13:947637. doi:10.3389/fphys.2022.947637
21. van Eck NJ, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538. doi:10.1007/s11192-009-0146-3
22. Yeung AWK, Mozos I. The innovative and sustainable use of dental panoramic radiographs for the detection of osteoporosis. Int J Environ Res Public Health. 2020;17(7):2449. doi:10.3390/ijerph17072449
23. Synnestvedt MB, Chen C, Holmes JH. CiteSpace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. 2005;2005:724–728.
24. Aria M, Cuccurullo C. bibliometrix: an R-tool for comprehensive science mapping analysis. J Informetrics. 2017;11(4):959–975. doi:10.1016/j.joi.2017.08.007
25. Bertoli-Barsotti L, Lando T. A theoretical model of the relationship between the h-index and other simple citation indicators. Scientometrics. 2017;111(3):1415–1448. doi:10.1007/s11192-017-2351-9
26. Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci U S A. 2005;102(46):16569–16572. doi:10.1073/pnas.0507655102
27. Bornmann L, Haunschild R, Mutz R. Growth rates of modern science: a latent piecewise growth curve approach to model publication numbers from established and new literature databases. Humanities Soc Sci Commun. 2021;8(1):224. doi:10.1057/s41599-021-00903-w
28. UNESCO. UNESCO Science Report: The Race Against Time for Smarter Development. Paris: UNESCO Publishing; 2021.
29. Celli BR, Decramer M, Wedzicha JA, et al. An official American thoracic society/european respiratory society statement: research questions in COPD. Eur Respir J. 2015;45(4):879–905. doi:10.1183/09031936.00009015
30. Celli BR, Decramer M, Wedzicha JA, et al. An official American thoracic society/European respiratory society statement: research questions in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;191(7):e4–e27. doi:10.1164/rccm.201501-0044ST
31. Celli BR, Decramer M, Wedzicha JA, et al. An official American thoracic society/european respiratory society statement: research questions in COPD. Eur Respir Rev. 2015;24(136):159–172. doi:10.1183/16000617.00000315
32. Moses H 3rd, Matheson DHM, Cairns-Smith S, George BP, Palisch C, Dorsey ER. The anatomy of medical research: US and international comparisons. JAMA. 2015;313(2):174–189. doi:10.1001/jama.2014.15939
33. Gresham GK, Ehrhardt S, Meinert JL, Appel LJ, Meinert CL. Characteristics and trends of clinical trials funded by the national institutes of health between 2005 and 2015. Clin Trials. 2018;15(1):65–74. doi:10.1177/1740774517727742
34. Regard L, Burgel PR. CFTR modulators for the treatment of COPD: the jury is still out! Am J Respir Crit Care Med. 2024;211(5):687–9.
35. Wan E, Yen AA, Elalami R, et al. Airway mucus plugs on chest computed tomography are associated with exacerbations in COPD. Am J Respir Crit Care Med. 2024;211(5):814–22.
36. Vaes AW, Sievi NA, Clarenbach CF, et al. Determinants of mortality in patients with COPD: physical capacity or physical activity? Chest. 2024;167(4):1064–1067. doi:10.1016/j.chest.2024.10.032
37. Amegadzie JE, Mehareen J, Khakban A, Joshi P, Carlsten C, Sadatsafavi M. Twenty-year trends in excess costs of chronic obstructive pulmonary disease. Eur Respir J. 2024;25(1):1514.
38. Hess MW. Oxygen therapy in COPD. Respir Care. 2023;68(7):998–1012. doi:10.4187/respcare.10876
39. Ferrer M, Torres A. Noninvasive ventilation and high-flow nasal therapy administration in chronic obstructive pulmonary disease exacerbations. Semin Respir Crit Care Med. 2020;41(6):786–797. doi:10.1055/s-0040-1712101
40. Venkatesan P. GOLD COPD report: 2024 update. Lancet Respir Med. 2024;12(1):15–16. doi:10.1016/S2213-2600(23)00461-7
41. Nagata K, Horie T, Chohnabayashi N, et al. Home high-flow nasal cannula oxygen therapy for stable hypercapnic COPD: a randomized clinical trial. Am J Respir Crit Care Med. 2022;206(11):1326–1335. doi:10.1164/rccm.202201-0199OC
42. Zhang L, Wang Y, Ye Y, Gao J, Zhu F, Min L. Comparison of high-flow nasal cannula with conventional oxygen therapy in patients with hypercapnic chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2023;18:895–906. doi:10.2147/COPD.S402506
43. Li X-Y, Tang X, Wang R, et al. High-flow nasal cannula for chronic obstructive pulmonary disease with acute compensated hypercapnic respiratory failure: a randomized, controlled trial. Int J Chron Obstruct Pulmon Dis. 2020;15:3051–3061. doi:10.2147/COPD.S283020
44. Rochwerg B, Granton D, Wang DX, et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: a systematic review and meta-analysis. Intensive Care Medicine. 2019;45(5):563–572. doi:10.1007/s00134-019-05590-5
45. Pitre T, Abbasi S, Su J, Mah J, Zeraatkar D. Home high flow nasal cannula for chronic hypercapnic respiratory failure in COPD: a systematic review and meta-analysis. Respir Med. 2023;219:107420. doi:10.1016/j.rmed.2023.107420
46. Theunisse C, de Graaf NTC, Braam AWE, et al. The effects of home high-flow nasal cannula oxygen therapy on clinical outcomes in patients with severe COPD and frequent exacerbations. J Clin Med. 2025;14(3):868. doi:10.3390/jcm14030868
47. Bowdish DME. The aging lung: is lung health good health for older adults? Chest. 2019;155(2):391–400. doi:10.1016/j.chest.2018.09.003
48. Matera MG, Hanania NA, Maniscalco M, Cazzola M. Pharmacotherapies in older adults with COPD: challenges and opportunities. Drugs Aging. 2023;40(7):605–619. doi:10.1007/s40266-023-01038-0
49. Andina N, de Meuron L, Schnegg-Kaufmann AS, et al. Increased inflammasome activation is associated with aging and chronic myelomonocytic leukemia disease severity. J Immunol. 2023;210(5):580–589. doi:10.4049/jimmunol.2200412
50. Barnes PJ, Baker J, Donnelly LE. Cellular senescence as a mechanism and target in chronic lung diseases. Am J Respir Crit Care Med. 2019;200(5):556–564. doi:10.1164/rccm.201810-1975TR
51. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679.
52. Dawod YT, Cook NE, Graham WB, Madhani-Lovely F, Thao C. Smoking-associated interstitial lung disease: update and review. Expert Rev Respir Med. 2020;14(8):825–834. doi:10.1080/17476348.2020.1766971
53. Olsson KM, Corte TJ, Kamp JC, et al. Pulmonary hypertension associated with lung disease: new insights into pathomechanisms, diagnosis, and management. Lancet Respir Med. 2023;11(9):820–835. doi:10.1016/S2213-2600(23)00259-X
54. Genecand L, Wacker J, Guerreiro I, et al. Pulmonary hypertension associated with interstitial lung disease: a review on diagnosis and treatment with a focus on emerging therapies. Respiration. 2025;104(8):575–585. doi:10.1159/000544800
55. Wright JL. Pulmonary hypertension in chronic obstructive pulmonary disease: current theories of pathogenesis and their implications for treatment. Thorax. 2005;60(7):605–609. doi:10.1136/thx.2005.042994
56. Cassady SJ, Almario JAN, Ramani GV. Therapeutic potential of treprostinil inhalation powder for patients with pulmonary arterial hypertension: evidence to date. Drug Healthc Patient Saf. 2024;16:51–59. doi:10.2147/DHPS.S372239
57. Cho SJ, Stout-Delgado HW. Aging and lung disease. Annu Rev Physiol. 2020;82(1):433–459. doi:10.1146/annurev-physiol-021119-034610
58. Nathan SD, Barbera JA, Gaine SP, et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur Respir J. 2019;53(1):1801914. doi:10.1183/13993003.01914-2018
59. Fabbri LM, Celli BR, Agustí A, et al. COPD and multimorbidity: recognising and addressing a syndemic occurrence. Lancet Respir Med. 2023;11(11):1020–1034. doi:10.1016/S2213-2600(23)00261-8
60. Piraino T. Noninvasive respiratory support in acute hypoxemic respiratory failure. Respir Care. 2019;64(6):638–646. doi:10.4187/respcare.06735
61. André S, Conde B, Fragoso E, Boléo-Tomé JP, Areias V, Cardoso J. COPD and cardiovascular disease. Pulmonology. 2019;25(3):168–176. doi:10.1016/j.pulmoe.2018.09.006
62. McNicholas WT, Hansson D, Schiza S, Grote L. Sleep in chronic respiratory disease: COPD and hypoventilation disorders. Eur Respir Rev. 2019;28(153):190064. doi:10.1183/16000617.0064-2019
63. Spruit MA, Rochester CL, Pitta F, et al. Pulmonary rehabilitation, physical activity, respiratory failure and palliative respiratory care. Thorax. 2019;74(7):693–699. doi:10.1136/thoraxjnl-2018-212044
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge Mapping of Acupuncture for Fibromyalgia from 1990 to 2022: A Bibliometric Analysis
Li P, Zheng H, Chen Y, Liu Z, He J
Journal of Pain Research 2022, 15:2405-2426
Published Date: 18 August 2022
Research Hotspots and Trends on Acupuncture for Neuropathic Pain: A Bibliometric Analysis from 2002 to 2021
Liu D, Chen B, Li T, Zheng L, Li J, Du W, Wang M, Huang Y
Journal of Pain Research 2022, 15:3381-3397
Published Date: 25 October 2022
Knowledge Mapping of International Research on Acupuncture for Chronic Pain: A Bibliometric Analysis

Jiao H, Ding R, Jin P, Wang J, Xu J, Tian W
Journal of Pain Research 2022, 15:3711-3728
Published Date: 2 December 2022
Bibliometrics Analysis and Visualization of Sarcopenia Associated with Osteoporosis from 2000 to 2022
Yang J, Jiang T, Xu G, Liu W
Journal of Pain Research 2023, 16:821-837
Published Date: 13 March 2023
Global Trends and Performances of Acupuncture Therapy on Bell’s Palsy from 2000 to 2023: A Bibliometric Analysis
Yu G, Luo S, Zhu C, Chen L, Huang H, Nie B, Gu J, Liu J
Journal of Pain Research 2023, 16:2155-2169
Published Date: 26 June 2023