Back to Journals » Journal of Pain Research » Volume 18
Relationship Between Perceived Stress, Resilience, Mental Health, and Pain in Women with Migraines, a Case-Control Study
Authors Arlud S ![]() , Tong N, Xie N, Gao S, He N
, Tong N, Xie N, Gao S, He N
Received 12 December 2024
Accepted for publication 31 March 2025
Published 13 October 2025 Volume 2025:18 Pages 5399—5408
DOI https://doi.org/10.2147/JPR.S487780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rune Häckert Christensen
Sarnai Arlud,1,2 Narengerel Tong,3 Nabucha Xie,3 Sargai Gao,1 Nagongbilige He4
1Department of Psychosomatic Medicine, Inner Mongolia International Mongolian Hospital, Hohhot, People’s Republic of China; 2Department of Psychosomatic Medicine, Ordos Mongolian Medicine Hospital, Ordos, People’s Republic of China; 3School of Mongolian Medicine, Inner Mongolia Medical University, Hohhot, People’s Republic of China; 4Research Institution of Psychosomatic Medicine, Inner Mongolia Autonomous Region Traditional Chinese and Mongolian Medicine Research Institute, Hohhot, People’s Republic of China
Correspondence: Sarnai Arlud, Department of Psychosomatic Medicine, Inner Mongolia International Mongolian Hospital, 83# Da Xue Dong street, Saihan District, Hohhot, Inner Mongolia, 010065, People’s Republic of China, Tel +86 15661057622, Email [email protected]
Purpose: The protective role of resilience against migraine remains understudied, and the present study examined the role of resilience in the relationship between perceived stress, mental health, and pain in female migraineurs and healthy women.
Patients and methods: In this case-control study, 125 female migraineurs and 121 healthy female controls were included. The Perceived Stress Scale (PSS-13), Connor-Davidson Resilience Scale (CD-RISC-10), and SF12 health-related quality-of-life questionnaire were used for assessments mental (MCS) and physical (PCS) health condition. Correlation and mediation analyses were performed.
Results: Female migraineurs exhibited significantly higher perceived stress, lower resilience, and worse quality of life, including pain and MCS (all p < 0.05). Resilience partially mediated the relationship between perceived stress and MCS in healthy women, but not in migraineurs. Mental health fully mediated the relationship between perceived stress and pain in migraineurs, while in healthy women, both resilience and MCS sequentially mediated this relationship.
Conclusion: Resilience does not protect against the mental health impact of perceived stress in female migraineurs but has a partial protective effect in healthy women. Mental health mediates the impact of perceived stress on pain among migraineurs. These findings underscore the need for targeted stress management and resilience-building interventions in clinical practice for better outcomes in women with migraines.
Keywords: female migraines, perceived stress, psychiatric disorders, resilience
Introduction
Migraine is a common neurological disorder characterized by recurrent episodes of moderate to severe headaches, often accompanied by symptoms such as nausea, vomiting, and sensitivity to light and sound. It is a leading cause of disability worldwide, particularly among women, who are two to three times more prevalent in women than men, and women report a longer attack duration, increased risk of headache recurrence, greater disability, and a longer period of time required to recover.1–3 This gender disparity is attributed to hormonal fluctuations, particularly estrogen, which influence the onset and severity of migraine episodes.4
Women with migraines are at a higher risk of developing psychological disorders, including anxiety, depression, and post-traumatic stress disorder (PTSD).5 Studies have shown that the prevalence of depression in women with migraines is approximately twice that of women without migraines.6 Similarly, anxiety disorders are more common in women with migraines, with some studies suggesting that up to 50% of migraine sufferers experience anxiety.7 These psychiatric disorders not only amplify the risk of migraine chronification but also adversely affect disability and quality of life.8,9
Psychological stress is a well-established trigger for migraine attacks. Stress can exacerbate the frequency, severity, and duration of migraines, creating a vicious cycle where migraines themselves become a source of stress, further worsening the condition.10–12 Women, in particular, are more likely to report stress as a migraine trigger compared to men.13 Beyond triggering attacks, chronic stress can also contribute to the development of comorbid psychological disorders like anxiety and depression, which are already more prevalent in women with migraine.5
Resilience, defined as the ability to adapt and recover from adversity,14 may play a crucial role in helping individuals cope with chronic pain conditions such as migraines. It encompasses a dynamic process that allows individuals to bounce back from stressful experiences, maintain emotional balance, and derive meaning and growth from challenges. Research suggests that higher levels of resilience are linked to lower stress levels and improved mental health outcomes, including reduced rates of depression and anxiety.15–17 Furthermore, studies have indicate that resilience can reduce the likelihood of experiencing severe disability due to headaches.18 Additional findings indicated that individuals with migraines demonstrate lower levels of psychological resilience compared to the control group, and that resilience was positively associated with psychological well-being.19 Despite this, the precise role of psychological resilience in mediating the relationships between perceived stress, mental health, and pain in women with migraines remains understudied.
This study aims to fill that gap by hypothesizing a mediation model to explore these interactions. Specifically, we propose that (1) resilience will mediate the relationship between perceived stress and mental health, and (2) both resilience and mental health will subsequently mediate the relationship between perceived stress and pain. Furthermore, we intend to compare healthy women with those who experience migraines to gain deeper insights into these complex interactions.
Methods
Study Design
In this case-control study, 125 migraine woman and 121 health control completed a Chinese version of an electronic questionnaire via an online survey platform (Survey Star, Changsha Ranxing Science and Technology) between April 10 and April 16, 2023. The study was planned to detect mediating effect of resilience on the relationship between mental health and perceived stress, and mediating effect of resilience and mental health on the relationships between stress, and pain among female migraineurs and healthy women.
The study adhered to the code of ethics of the World Medical Association (Declaration of Helsinki) and was approved by the Ethical Committee Review Board of the International Mongolian Medicine Hospital of Inner Mongolia (ethics approval code B2022-006). Participants provided informed consent before completing the formal questionnaire.
Participants
We recruited participants through an advertisement posted on the Mongolian Mind-Body Interactive Psychotherapy Service WeChat app. The inclusion criteria were as follows: (1) a diagnosis of migraine based on the International Classification of Headache Disorders (ICHD-III), excluding other types of headaches; (2) age over 18 years; and (3) female. Perceived stress scale (PSS-13) questionnaire was designed for a community-based sample of individuals with a minimum education level of junior high school or higher. Exclusion criteria included: (1) an education level below junior high school, and (2) a diagnosis of other severe conditions, such as cancer. A total of 125 individuals met the criteria and completed a Chinese version of an electronic questionnaire administered through an online survey platform (Survey Star, Changsha Ranxing Science and Technology). In addition, 121 healthy female controls excluding migraine, any headache disorder, other types of chronic pain, hypertension, diabetes, cancer, insomnia, or endocrine diseases were recruited for comparison.
Measures
Perceived Stress Scale (PSS-13)
The Chinese version of 14 items PSS was used, where each item was rated on a 5-point Likert-type scale, ranging from 0 = “never” to 4 = “very often”. The scale can be clustered into two subscales, negative subscale (items 1,2,3,8,11,12 and 14) and positive subscale (items 4,5,6,7,9,10 and 13).12 Higher scores indicate more perceived stress. A previous study20 suggested excluding item 12, which we did. Cronbach’s α coefficient of the PSS-13 scale in this study was 0.887.
Connor-Davidson Resilience Scale (CD-RISC-10)
Resilience is a construct referring to the individual’s capacity to ‘bounce back’ from a challenging situation in an adaptive manner.21 This scale has shown good reliability and validity of this test in different populations.22 The Chinese version of the 10-item CD-RISC was used, where each item is rated on a 5-point Likert-type scale ranging from 0 = “Not true at all” to 4 = “True nearly all the time”.10-item scale sums a possible high score of 40. Higher scores indicate greater levels of resilience.23 Cronbach’s α coefficient of this scale in this study was 0.939.
SF-12
The SF-12 is a health-related quality-of-life questionnaire consisting of twelve questions that measure eight health domains to assess physical and mental health. Physical health-related domains include General Health (GH), Physical Functioning (PF), Role Physical (RP), and Body Pain (BP). Mental health-related scales include Vitality (VT), Social Functioning (SF), Role Emotional (RE), Mental Health (MH), the Mental Component Summary (MCS), and the Physical Component Summary (PCS). The MCS and PCS measure the latent mental and physical health concepts, respectively. Each of the components is scored on a scale from 0 to 100, and summary measures are standardized to produce a mean of 50 with a standard deviation of 10 for the United States (US) population (norm-based scoring); higher scores represent better health.24 Cronbach’s α coefficient of this scale in this study was 0.849.
Statistical Analysis
Statistical analysis was performed using SPSSAU. The internal consistency reliability of the 13 items PSS, 10 items CD-RISC and SF-12 health Survey were examined by Cronbach’s alpha and the reasonable acceptability criterion of ≥0.7. SF12 scoring was done with the SAS software. Qualitative variables are presented as counts (percentage) and were compared with the Chi2 test or Fisher exact test as appropriate. When considered normally distributed (z score of Skewness and Kurtosis≤ 3.29, see Supplementary table 1 Normality test), quantitative variables were either expressed as mean (± standard deviation) and compared using two independent samples t-tests, or when unequal variances were used, and effect sizes were calculated using Cohen’s d. For abnormally distributed data and ranked data summarized at median and quartiles [median (P25, P75)], the Mann–Whitney U-test was used. Comparisons were made and the effect size Cohen’s d was calculated using the online tool https://www.psychometrica.de/effect_size.html. P values were considered significant when they were less than 0.05, at which point larger effect sizes indicated a larger magnitude of difference, and the thresholds for distinguishing between small, medium, and large effect sizes in the usual case were respectively: 0.20, 0.50, and 0.80. The Spearman correlation coefficient was used to assess the correlation between scores. All statistical tests were two-tailed and employed a significance level of p < 0.05. The mediation model used stratified regression and used the bootstrap sampling method (Sampling 5000 times) for testing, which was considered significant if the bootstrap 95% CI did not contain zero.
Results
Baseline Characteristics
There were no differences in age, race, education, and marital status between the 121 healthy females and 125 female migraineurs, and their characteristics are shown in (Table 1).
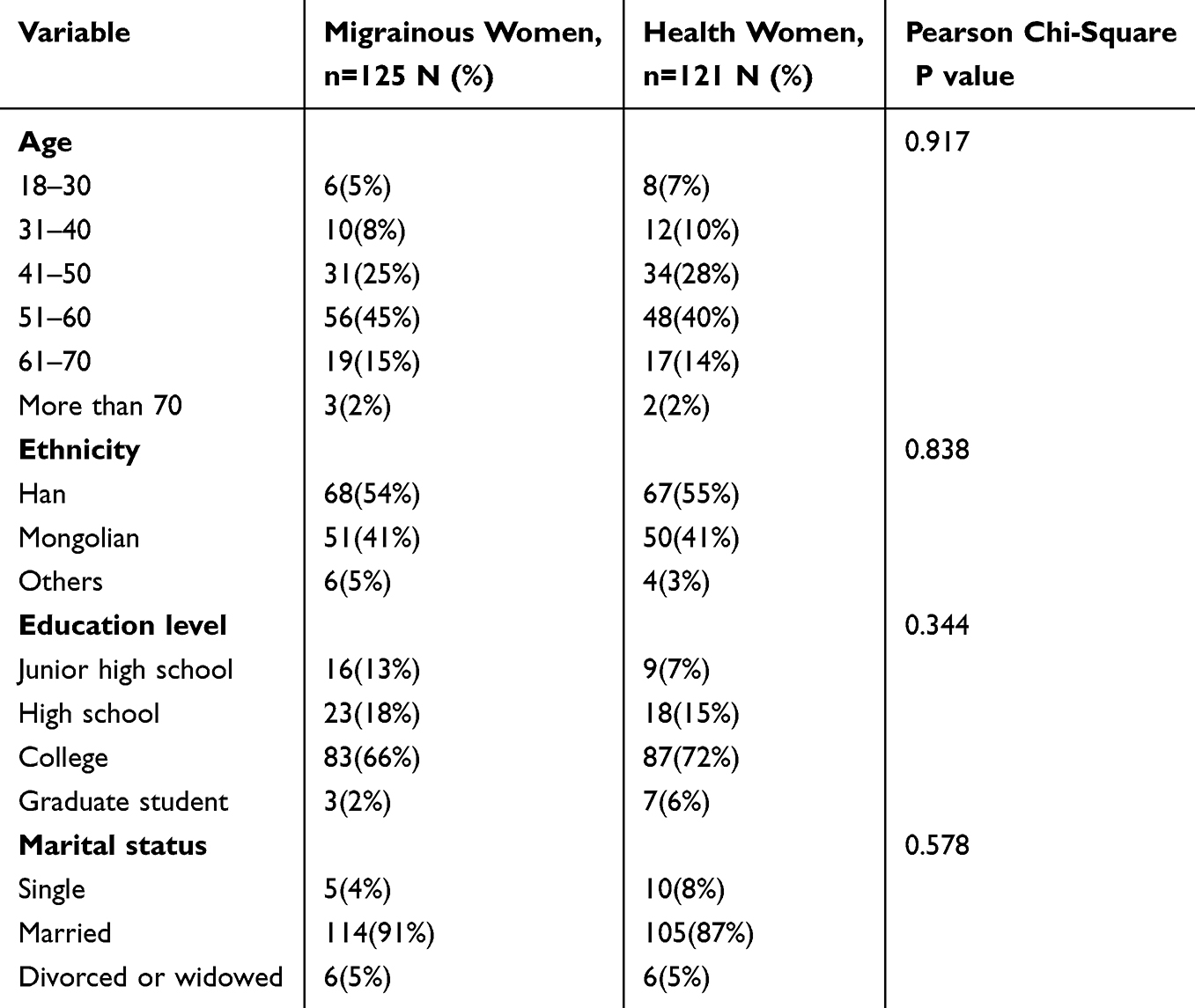 |
Table 1 Characteristics of the Study |
The Differences in Perceived Stress, Resilience and Quality of Life Between Women With Migraine and Healthy Women
Perceived stress (PSS-13) was significantly higher in women with migraines compared to healthy women (p = 0.007). Conversely, resilience (CD-RISC-10) was significantly lower in migraine woman than in healthy controls (p = 0.032). Additionally, quality of life, encompassing eight health domains as well as the Physical Component Summary (PCS) and Mental Component Summary (MCS), was significantly lower in women with migraines compared to healthy controls (p < 0.05) (Table 2). Among these measures, body pain demonstrated the largest effect size (Cohen’s d= 0.80).
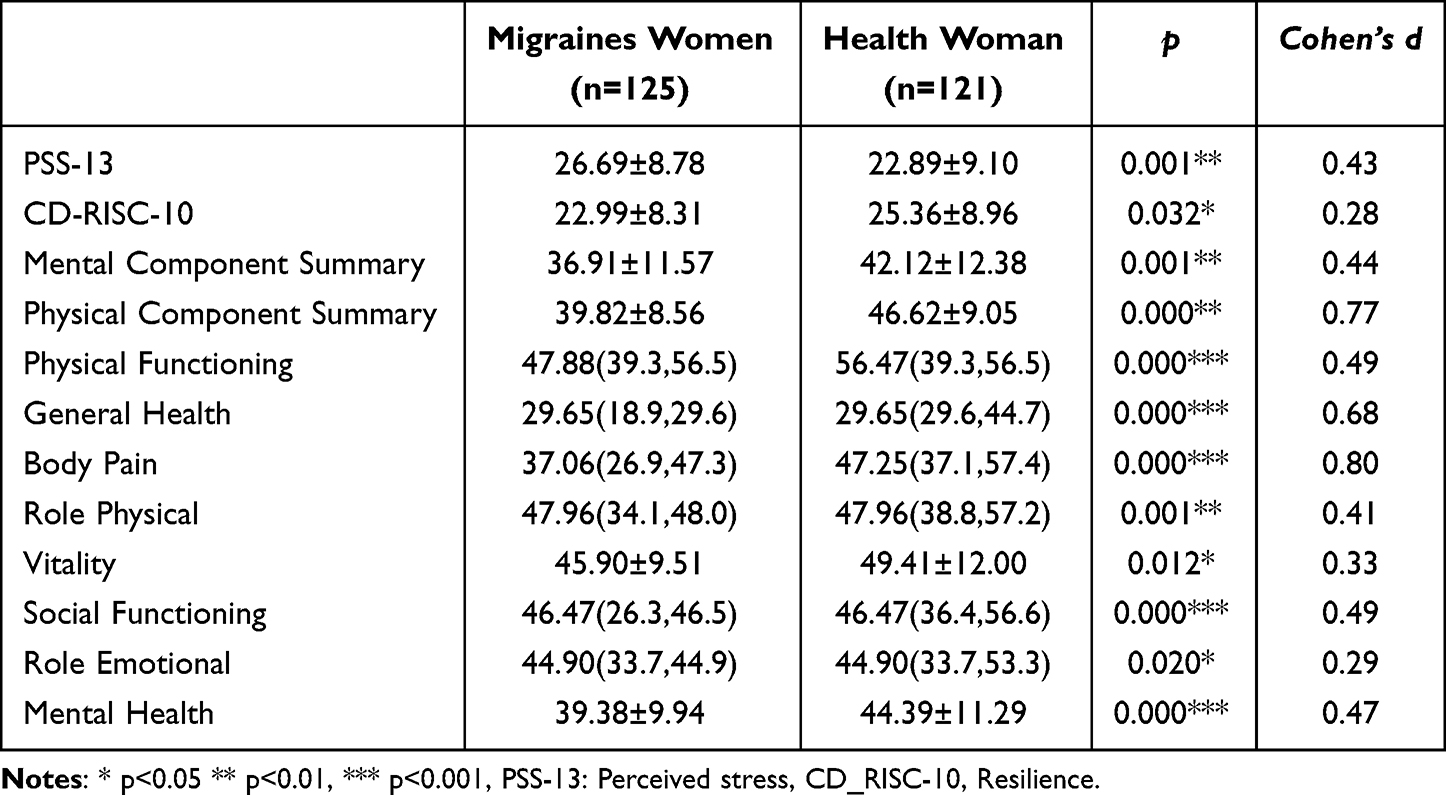 |
Table 2 Differences in Perceived Stress, Resilience and Quality of Life in Healthy Women and Female Migraineurs |
Correlations
The Spearman correlations between perceived stress (PSS), resilience (CD_RISC), and eight dimension of quality of life, PCS and MCS in migraineurs and healthy women are shown in Tables 3 and 4. The results revealed significant correlations between except physical functioning all dimensions of quality of life and perceived stress (all p < 0.01) in healthy women; however, perceived stress was not correlated with PCS, physical functioning and body pain in women suffering migraines. Resilience was significantly correlated with perceived stress in women suffering from migraine and healthy women. However, resilience was not correlated with PCS, physical function and body pain in any of the groups of women.
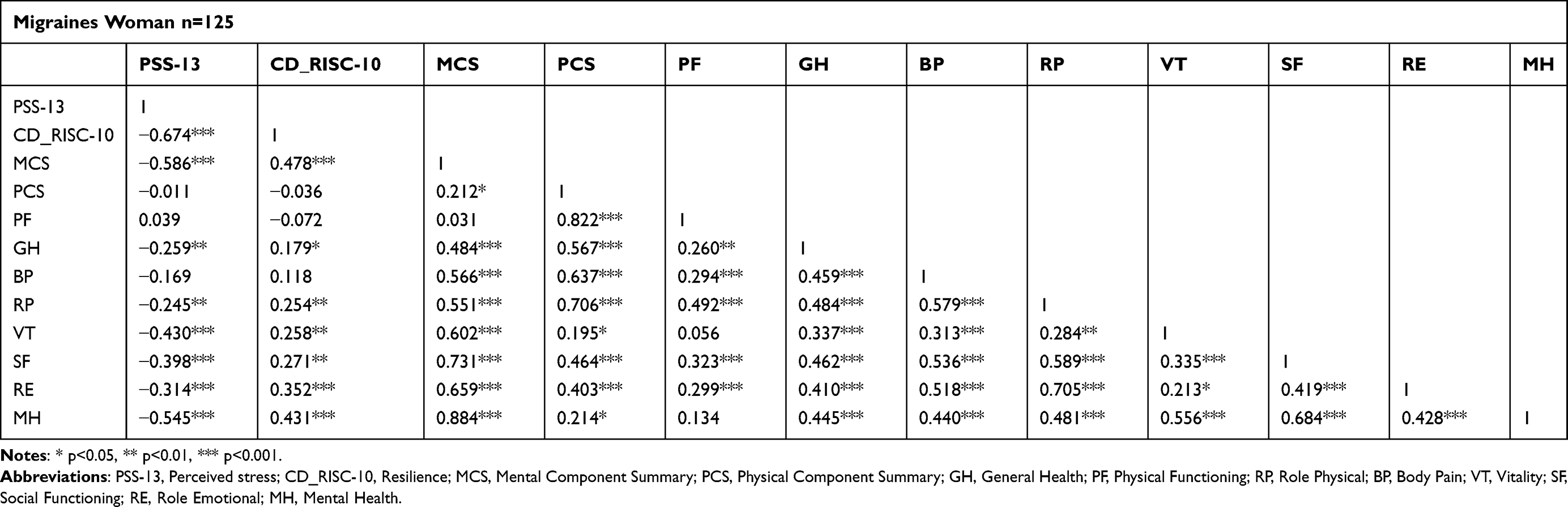 |
Table 3 Correlation in Women Suffering Migraines |
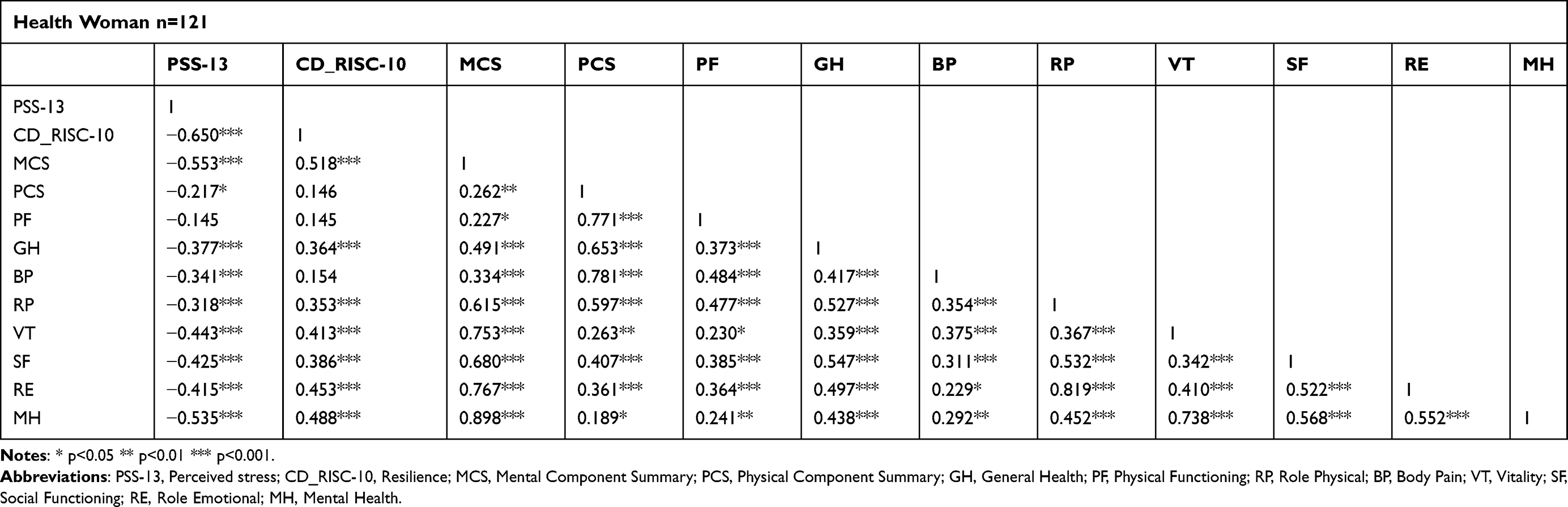 |
Table 4 Correlation in Healthy Women |
Mediated Effect Analysis
A bootstrapped mediation model was carried out to further verify: (1) the mediating effect of resilience in the perceived stress and mental health; (2) mediating effect of resilience and mental health on the relationship between perceived stress and pain.
With reference to the first hypothesis, the results showed that resilience had a partial mediating effect on the perceived stress and MCS in healthy women (Bootstrap 95% CI: −0.246 ~ −0.027, Ratio = 23.3%); however, there was no mediating effect in women suffering migraine; the 95% range included the number 0 (Bootstrap 95% CI: −0.226 ~ 0.034) (Table 5 and Figure 1).
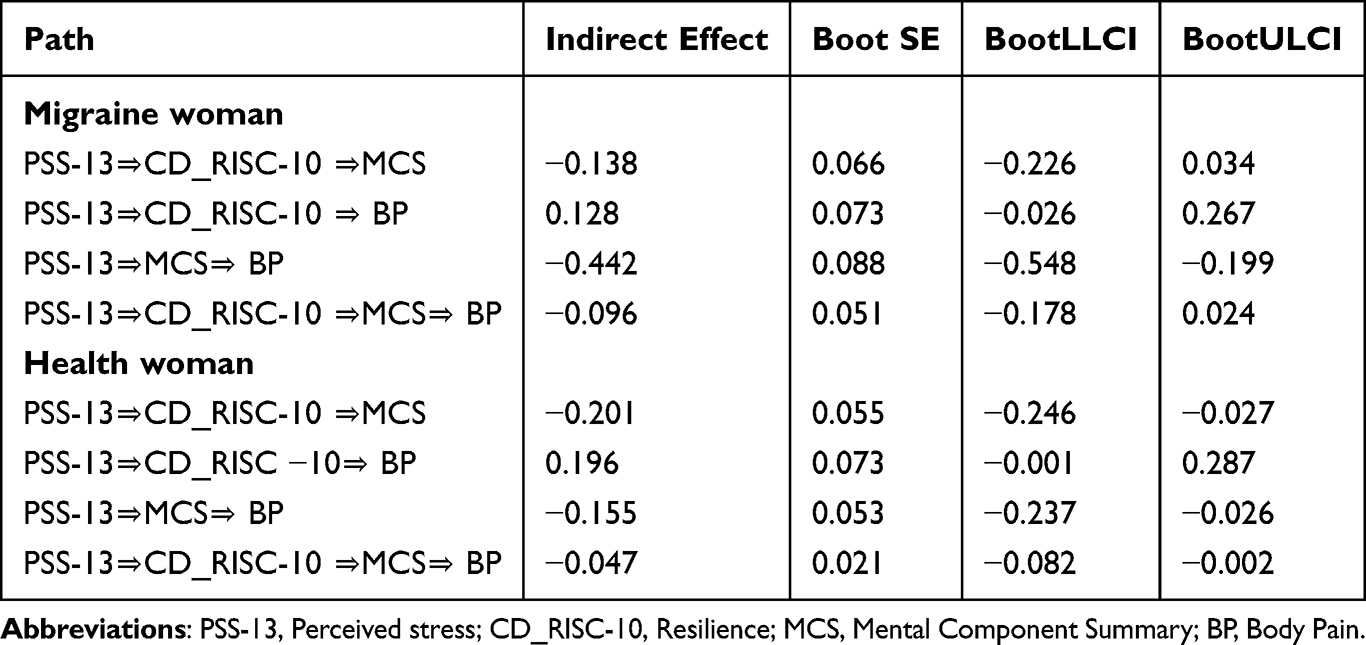 |
Table 5 Results of the Deviation-Corrected Percentile Bootstrap Method Analysis |
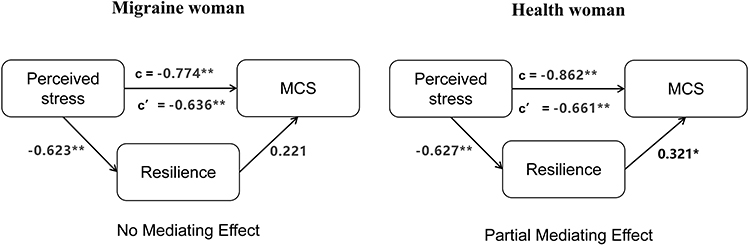 |
Figure 1 The mediating effect of resilience in the perceived stress and Mental component summary in healthy women and those with migraine. Notes: * p<0.05, ** p<0.01. |
With reference to the second hypothesis, we found the mediating effects of MCS and the sequential chain mediating effect of resilience and MCS on the association between perceived stress and pain (bootstrap 95% CI: −0.237~-0.026 and bootstrap 95% CI: −0.082~-0.002, respectively) in healthy women. However, these mediation effects were not observed in women suffering migraines; the 95% range included the number 0; however, MCS played full mediation in perceived stress and pain in female migraineurs (Bootstrap 95% CI: −0.548 ~-0.199, Ratio = 100%) (Table 5 and Figure 2).
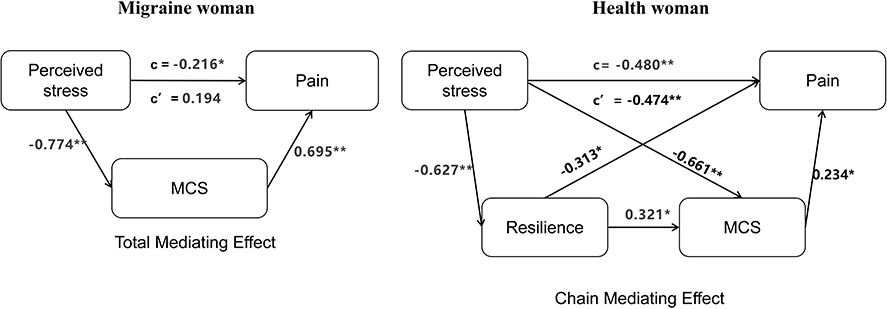 |
Figure 2 Mediating effect of resilience and Mental component summary in the relationship between perceived stress and pain in healthy women and those with migraine. Notes: * p<0.05, ** p<0.01. |
Discussion
This case-control study revealed significantly higher levels of perceived stress, lower psychological resilience, and poorer quality of life, including greater pain severity and worse mental health outcomes, in women with migraine compared to healthy controls. Notably, this study is the first to examine the role of resilience in the relationships between perceived stress and mental health in both women with migraine and healthy women. The findings highlight distinct patterns in these relationships between the two groups. In healthy women, resilience partially mediated the relationship between perceived stress and mental health, suggesting that higher resilience can buffer the negative impact of stress on mental well-being. Additionally, resilience and mental health demonstrated a chain mediation effect in healthy women, where resilience influenced mental health, which in turn mitigated pain perception. This underscores the protective role of resilience in mitigating the effects of stress on both mental health and pain in healthy individuals. In contrast, among women with migraine, resilience did not mediate the relationship between perceived stress and mental health, furthermore, mental health fully mediated the relationship between perceived stress and pain, highlighting the protective role of resilience may be compromised in this population.
The Role of Psychological Resilience in Mental Health Comorbidity
Psychological resilience is strongly associated with mental health outcomes.25 Lower resilience in migraine patients may be linked to childhood adversity, as studies have shown that migraine progression is associated with adverse childhood experiences (ACEs).18,26,27 Cumulative exposure to ACEs is correlated with lower adult resilience, particularly among women, independent of adult socioeconomic factors and social support.28 This suggests that resilience may be significantly influenced by early life experiences. Individuals with lower resilience often struggle to cope with stress or trauma, increasing their vulnerability to comorbid psychiatric conditions such as depression, anxiety, and post-traumatic stress disorder (PTSD).25,29 Higher resilience, on the other hand, is associated with fewer symptoms of these disorders. For example, in individuals with traumatic spinal cord injury (SCI), resilience acts as a protective factor against suicidal ideation, underscoring its critical role in mental health following traumatic events.30
The Impact of Psychiatric Comorbidities on Treatment Challenges in Migraine
These psychiatric comorbidities in migraine are associated with higher medical costs, greater functional impairment, increased headache frequency over time, and greater difficulty in managing the condition. A study by Bottiroli et al (2021) found that individuals who do not respond to migraine medications have a higher prevalence of personality disorders and anxiety disorders, and are more likely to report experiencing severe stressors.31 Another study by Torres-Ferrus et al (2024) showed that an anti-CGRP monoclonal antibody against CGRP was effective in reducing depressive symptoms in migraine patients. However, the patients who did not respond to the medication also showed less reduction in depression symptoms.32 Additionally, mood and anxiety disorders are risk factors for the development of medication-overuse headache (MOH). Compared to individuals with migraine alone, those with MOH have four times greater odds of having mood disorders and 3.5 times greater odds of having anxiety disorders.33 These findings highlight the complex interplay between psychiatric comorbidities and migraine severity, emphasizing the need for integrated treatment approaches that address both the neurological and psychological aspects of migraine.
Clinical Implications and Interventions
A comprehensive treatment approach is essential for migraine patients, encompassing both pharmacological and non-pharmacological interventions, as well as the management of behavioral and psychological factors.34 Lifestyle modifications, such as regular exercise, a balanced diet, and adequate sleep, can enhance psychological resilience and reduce migraine frequency. However, there is limited clinical evidence on the efficacy of integrating pharmacological and non-pharmacological treatments for migraine, highlighting the need for further longitudinal studies to evaluate their potential benefits.
Study Limitations
First, because this was a case-control study, determining causality between key variables was challenging. Future longitudinal studies are needed to understand causality. Second, information gathered through participant self-reports may have affected the reliability of our results, and more objective markers of stress may be included in the future. Third, body pain and MCS from the SF12 scale used in this study should be changed in the future with specific migraine-related questionnaires and psychiatric condition diagnosis and related questionnaires. Fourth, other confounding variables such as lifestyle factors (eg, sleep, diet, and exercise) were not included in this study. Therefore, future studies need to adopt a longitudinal study design, use more specific scales, and control for a wider range of confounders to determine causal relationships between psychological resilience, perceived stress, pain, and mental health.
Conclusion
We found significantly higher levels of perceived stress, lower resilience, and worse quality of life in women with migraine than in healthy controls. Mediation analysis showed that resilience has no protective effect on mental health from perceived stress in women affected by migraine but partially affects healthy women. Furthermore, mental health had a crucial role in the relationship between perceived stress and pain in women with migraine. There were also the mediating effects of mental health and the sequential chain mediating effect of resilience and mental health on the association between perceived stress and pain in health woman. These findings highlight the importance of targeted stress management and resilience-building interventions in clinical practice to improve outcomes for women with migraines.
Acknowledgments
This study was supported by the Mongolian Medicine Standardization Project of the Inner Mongolia Autonomous Region (2019-MB003), the Transformation Project of Scientific and Technological Achievements of the Inner Mongolia Autonomous Region (CGZH2018175), and Inner Mongolia Major Project 2017 (NMGZDZX2017). We would also like to thank Ruiming Gao for advising us on our paper.
Disclosure
The Authors declare that there is no conflict of interest.
References
1. Eisenstein M. Closing the gender gap in migraine research. Nature. 2020;586(7829):S16. doi:10.1038/d41586-020-02867-4
2. Broner SW, Bobker S, Klebanoff L. Migraine in women. Seminars Neurol. 2017;37(6):601. doi:10.1055/s-0037-1607393
3. Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017;16(1):76–87. doi:10.1016/S1474-4422(16)30293-9
4. Ahmad SR, Rosendale N. Sex and gender considerations in episodic migraine. Current Pain Headache Rep. 2022;26(7):505–516. doi:10.1007/s11916-022-01052-8
5. Minen MT, Begasse De Dhaem O, Kroon Van Diest A, et al. Migraine and its psychiatric comorbidities. J Neurol Neurosurg. 2016;87(7):741–749.
6. Breslau N, Schultz LR, Stewart WF, Lipton RB, Lucia VC, Welch KM. Headache and major depression: is the association specific to migraine? Neurology. 2000;54(2):308–313. doi:10.1212/WNL.54.2.308
7. Smitherman TA, Maizels M, Penzien DB. Headache chronification: screening and behavioral management of comorbid depressive and anxiety disorders. Headache. 2008;48(1):45–50. doi:10.1111/j.1526-4610.2007.00974.x
8. Lantéri-Minet M, Radat F, Chautard M-H, Lucas C. Anxiety and depression associated with migraine: influence on migraine subjects’ disability and quality of life, and acute migraine management. Pain. 2005;118(3):319–326. doi:10.1016/j.pain.2005.09.010
9. Seng EK, Buse DC, Klepper JE, et al. Psychological factors associated with chronic migraine and severe migraine-related disability: an observational study in a tertiary headache center. Headache. 2017;57(4):593–604. doi:10.1111/head.13021
10. Kelman L. The triggers or precipitants of the acute migraine attack. Cephalalgia. 2007;27(5):394–402. doi:10.1111/j.1468-2982.2007.01303.x
11. Eskin M, Akyol A, Çelik EY, Gültekin BK. Social problem-solving, perceived stress, depression and life-satisfaction in patients suffering from tension type and migraine headaches. Scand J Psychol. 2013;54(4):337–343. doi:10.1111/sjop.12056
12. An Y-C, Liang C-S, Lee J-T, et al. Effect of sex and adaptation on migraine frequency and perceived stress: a cross-sectional case-control study. Front Neurol. 2019;10:598. doi:10.3389/fneur.2019.00598
13. Wacogne C, Lacoste JP, Guillibert E, Hugues FC, Le Jeunne C. Stress, anxiety, depression and migraine. Cephalalgia. 2003;23(6):451–455. doi:10.1046/j.1468-2982.2003.00550.x
14. Kalisch R, Baker DG, Basten U, et al. The resilience framework as a strategy to combat stress-related disorders. Nat Human Behav. 2017;1(11):784–790. doi:10.1038/s41562-017-0200-8
15. Sarrionandia A, Ramos-Díaz E, Fernández-Lasarte O. Resilience as a mediator of emotional intelligence and perceived stress: a cross-country study. Front Psychol. 2018;9. doi:10.3389/fpsyg.2018.02653
16. Catabay CJ, Stockman JK, Campbell JC, Tsuyuki K. Perceived stress and mental health: the mediating roles of social support and resilience among black women exposed to sexual violence. Int Soc Affective Disorders. 2019;259:143–149.
17. Lara-Cabrera ML, Betancort M, Muñoz-Rubilar CA, Rodríguez Novo N, De Las Cuevas C. The mediating role of resilience in the relationship between perceived stress and mental health. Int J Environ Res Public Health. 2021;18(18):9762. doi:10.3390/ijerph18189762
18. Casucci G, Villani V, d’Onofrio F, Russo A. Migraine and lifestyle in childhood. Neurol Sci. 2015;36 Suppl 1:97–100. doi:10.1007/s10072-015-2168-3
19. Kurtses Gürsoy B, Köseoğlu Toksoy C. Psychological resilience and stress coping styles in migraine patients. Neuropsychiatr Dis Treat. 2023;19:63–72. doi:10.2147/NDT.S398838
20. Huang F, Wang H, Wang Z, et al. Psychometric properties of the perceived stress scale in a community sample of Chinese. BMC Psychiatry. 2020;20(1):130. doi:10.1186/s12888-020-02520-4
21. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depression Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
22. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028.
23. Ye ZJ, Qiu HZ, Li PF, et al. Validation and application of the Chinese version of the 10-item Connor-Davidson Resilience Scale (CD-RISC-10) among parents of children with cancer diagnosis. Eur J Oncol Nurs. 2017;27:36–44.
24. Ge YJ, Xin SM, Luan DC et al. Association of physical activity, sedentary time, and sleep duration on the health-related quality of life of college students in Northeast China. Health Qual Life Outcomes. 2019;17(1):124. doi:10.1186/s12955-019-1194-x
25. Mesman E, Vreeker A, Hillegers M. Resilience and mental health in children and adolescents: an update of the recent literature and future directions. Curr Opin Psychiatry. 2021;34(6):586–592. doi:10.1097/YCO.0000000000000741
26. Tietjen GE, Brandes JL, Peterlin BL, et al. Childhood maltreatment and migraine (part II). Emotional abuse as a risk factor for headache chronification. Headache. 2010;50(1):32–41.
27. Mays I, Flynn J, McGuire B, Egan J. The role of attachment style, adverse childhood experiences and dissociation in migraine. J Trauma Dissoc. 2022;23(3):245–278.
28. Daníelsdóttir HB, Aspelund T, Thordardottir EB, et al. Adverse childhood experiences and resilience among adult women: a population-based study. Elife. 2022;11:e71770.
29. Dhungana S, Koirala R, Ojha SP, Thapa SB. Resilience and its association with post-traumatic stress disorder, anxiety, and depression symptomatology in the aftermath of trauma: a cross-sectional study from Nepal. Eur Psychiatry. 2022;65:S673–S674. doi:10.1192/j.eurpsy.2022.1732
30. Usta Sağlam NG, Aksoy Poyraz C, Doğan D, Erhan B. Suicidal ideation, post-traumatic stress disorder, and depression in traumatic spinal cord injury: what resilience tells us. J Spinal Cord Med. 2022;46:309–316.
31. Bottiroli S, De Icco R, Vaghi G, et al. Psychological predictors of negative treatment outcome with Erenumab in chronic migraine: data from an open label long-term prospective study. J Headache Pain. 2021;22(1):114.
32. Torres-Ferrús M, Gallardo VJ, Alpuente A, Caronna E, Giné-Ciprés E, Pozo-Rosich P. Improvement of migraine depressive symptoms is not related to headache frequency: exploring the impact of anti-CGRP therapies. Cephalalgia. 2024;44(2):3331024231222923.
33. Radat F, Creac’h C, Swendsen JD, et al. Psychiatric comorbidity in the evolution from migraine to medication overuse headache. Cephalalgia. 2005;25(7):519–522. doi:10.1111/j.1468-2982.2005.00910.x
34. Sepe FN, Lanni C, Michelis DD, Lancia G. The impact of psychological treatment on catastrophization and pharmacological response in chronic migraine: a single-center experience. Paper presented at: medRxiv2024.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.