Back to Journals » Cancer Management and Research » Volume 10
Relationship between IGF2BP2 and IGFBP3 polymorphisms and susceptibility to non-small-cell lung cancer: a case–control study in Eastern Chinese Han population
Authors Chen S, Qiu H, Liu C, Wang Y, Tang W, Kang M
Received 25 March 2018
Accepted for publication 26 May 2018
Published 28 August 2018 Volume 2018:10 Pages 2965—2975
DOI https://doi.org/10.2147/CMAR.S169222
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Shuchen Chen,1,* Hao Qiu,2,* Chao Liu,3 Yafeng Wang,4 Weifeng Tang,1 Mingqiang Kang1,5,6
1Department of Thoracic Surgery, Fujian Medical University Union Hospital, Fuzhou, Fujian Province, China; 2Department of Immunology, School of Medicine, Jiangsu University, Zhenjiang, Jiangsu Province, China; 3Department of Cardiothoracic Surgery, Affiliated People’s Hospital of Jiangsu University, Zhenjiang, Jiangsu Province, China; 4Department of Cardiology, The People’s Hospital of Xishuangbanna Dai Autonomous Prefecture, Jinghong, Yunnan Province, China; 5Key Laboratory of Ministry of Education for Gastrointestinal Cancer, Fujian Medical University, Fuzhou, Fujian Province, China; 6Fujian Key Laboratory of Tumor Microbiology, Fujian Medical University, Fuzhou, Fujian Province, China
*These authors contributed equally to this work
Background: IGF2BP2 and IGFBP3 polymorphisms may be associated with cancer risk.
Methods: With an aim to determine the association of variations in IGF2BP2 and IGFBP3 genes with risk of non-small-cell lung cancer (NSCLC), IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A polymorphisms were selected and genotyped in 521 NSCLC patients and 1,030 controls.
Results: We found that there was no difference in IGF2BP2 and IGFBP3 genotype distribution among the NSCLC patients and controls. The stratified analyses suggested that IGF2BP2 rs1470579 A>C polymorphism decreased the risk of NSCLC in some subgroups (female subgroup: CC vs AA: adjusted P=0.032 and CC vs AC/AA: adjusted P=0.028; <60 years subgroup: CC vs AA: adjusted P=0.012 and CC vs AC/AA: adjusted P=0.013; and never drinking subgroup: CC vs AA: adjusted P=0.046 and CC vs AC/AA: adjusted P=0.031). The stratified analyses also found that IGF2BP2 rs4402960 G>T polymorphism decreased the risk of NSCLC in some subgroups (female subgroup: TT vs GG: adjusted P=0.031 and TT vs GT/GG: adjusted P=0.026; <60 subgroup: TT vs GG: adjusted P=0.037 and TT vs GT/GG: adjusted P=0.038; and never drinking subgroup: TT vs GT/GG: adjusted P=0.046). Haplotype analysis indicated Ars1470579Crs2270628Grs3110697Grs4402960Ars6953668 haplotype decreased susceptibility of NSCLC (P=0.007).
Conclusion: Our study suggests that IGF2BP2 rs1470579 A>C, rs4402960 G>T single-nucleotide polymorphisms are candidates for decreased susceptibility to NSCLC among female, <60 years, and never drinking subgroups. In the future, more case–control studies with functional analysis are needed to confirm these preliminary findings.
Keywords: IGFBP3, IGF2BP2, polymorphism, haplotype, risk, NSCLC
Introduction
Lung cancer (LC) is the most common malignancy worldwide. It was reported that 1.8 million new LC patients were diagnosed in 2012, which accounted for about 13% of total cancer cases.1 Because of aging, air pollution, smoking, and exposure to occupational and/or environmental carcinogens, LC constitutes a burden all over the world. Some risk factors mentioned above might contribute to the development of LC; however, other susceptibility factors could also increase the incidence of LC. Nowadays, genetic variants were supported to influence the risk of LC, especially non-small-cell lung cancer (NSCLC), which was a common subtype of LC.
In humans, insulin-like growth factor 2 mRNA-binding protein 2 (IGF2BP2) is a protein which is encoded by IGF2BP2 gene.2,3 IGF2BP2 regulates insulin-like growth factor 2 (IGF2) translation by binding to the 5′ UTR of IGF2 mRNA.3 Gu et al reported that IGF2BP2 was overexpression in both ovarian cancer and ovarian low malignant potential tumor samples compared to either normal ovary or ovarian adenomas samples.4 A previous study also found that IGF2BP2/IGF-1/IGF-1 receptor signaling pathways might involve in cancer-mediated endothelial recruitment, which was an important feature of metastatic cancer in the tumor microenvironment.5 In addition, Liu et al found that an lncRNA (IGF2BP2-AS1) was associated with better overall survival in lung squamous cell carcinoma.6 In view of these previous studies, we thought that IGF2BP2 might influence the development of LC.
IGF family involves IGF ligands, IGF receptors, and IGF-binding proteins (IGFBPs). IGF-1 is a potent mitogen and regulates mitogenesis and antiapoptosis.7 IGFBP3, a major binding protein of IGF-1, interacts with IGF-1, regulates its biological activity, and may play important roles in antiproliferation and proapoptosis.8 Papadimitrakopoulou et al reported that IGFBP3 downregulation is an early event during head and neck carcinogenesis.9 Adenoviral IGFBP3 and farnesyltransferase inhibitor might decrease Akt expression and promote NSCLC cell apoptosis in vitro and in vivo.10 Results of a previous study highlighted that IGFBP3 could mediate LC progression. In addition, overexpression of IGFBP3 might induce apoptosis of NSCLC cells and promote cisplatin response in vitro.11
Several case–control studies focused on the association of IGF2BP2 and IGFBP3 polymorphisms with risk to cancer. Results of previous studies indicated that IGF2BP2 rs4402960 G>T single-nucleotide polymorphism (SNP) was associated with the development of breast cancer.12 Terry et al found that IGFBP3 rs2270628 variants increased IGF1 levels in plasma and was associated with the risk of ovarian cancer.13 In addition, IGFBP3 rs3110697 variants were significantly associated with IGFBP-3 levels in a multiethnic populations,14 and IGFBP3 rs3110697 AA genotypes increased the risk of death among Chinese postmenopausal women with breast cancer.15 However, the relationship between IGF2BP2 and IGFBP3 polymorphisms and NSCLC risk was unclear. With an aim to determine the potential association of genetic variations in IGF2BP2 and IGFBP3 genes with risk of NSCLC in Eastern Chinese Han populations, IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A SNPs were selected and genotyped in 521 NSCLC patients and 1,030 cancer-free controls.
Materials and methods
Ethics statement
This case–control study conformed to the Helsinki declaration and was approved by the Institutional Review Board of Fujian Medical University. A written consent was obtained from each participant.
Subjects
In our study, a total of 521 sporadic NSCLC cases and 1,030 age- and gender-matched controls were enrolled. All participants were recruited from the Department of Thoracic Surgery in Affiliated Union Hospital of Fujian Medical University and Affiliated People’s Hospital of Jiangsu University. All NSCLC patients (mean age at 59.76±10.71 years) were diagnosed by pathology. The corresponding information was retrieved from medical files (Table 1). The cancer-free controls were well-matched to NSCLC patients by age (mean age at 60.34±9.11 years) and sex (P=0.453). Individuals without any history of personal malignancy or autoimmune disorder were included as controls. Both NSCLC cases and controls were hereditarily unrelated and were from Eastern Chinese Han population. Each participant was informed about the study protocols and a written consent was obtained. A body mass index (BMI) ≥24 kg/m2 was considered as the criterion of Chinese individuals with obesity and overweight.16,17 The definitions of “ever smokers” and “ever drinkers” were described in our previous study.18
 | Table 1 Distribution of selected demographic variables and risk factors in NSCLC cases and controls Notes: Bold values are statistically significant (P<0.05). aTwo-sided chi-squared test and Student’s t-test. Abbreviations: BMI, body mass index; NSCLC, non-small-cell lung cancer; TNM, tumor-lymph node-metastasis. |
Selection of SNPs
To assess the relationship between IGF2BP2 and IGFBP3 SNPs and NSCLC risk, we selected polymorphisms in IGF2BP2 and IGFBP3 gene according to the publications, which were associated with the development of cancer.12,13,19–21
DNA extraction and genotyping
Using a universal Promega DNA kit (Promega Corporation, Fitchburg, WI, USA), genomic DNA was extracted from whole blood sample which was stored with EDTA-anticoagulation tube. IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T,22 rs3110697 G>A and rs6953668 G>A genotypes were determined by a custom-by-design 48-Plex PCR (SNPscanTM kit; Genesky Biotechnologies Inc., Shanghai, China).23 We used ABI 3730XL sequencer to obtain genotypes. The data were read out by GeneMapper 4.1 software (Thermo Fisher Scientific, Waltham, MA, USA). For quality control, 4% samples were randomly selected from 1,551 DNA samples and analyzed again. The genotypes of IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A and rs6953668 G>A polymorphisms were not changed.
Statistical analysis
Age and BMI are expressed as mean ± SD. Student’s t-test was used to compare these continuous variables between NSCLC cases and cancer-free controls. The categorical variables (eg, IGF2BP2 and IGFBP3 genotypes, BMI, gender, age, tobacco use, and drinking status) were compared by using chi-squared test (χ2) or Fisher’s exact test. Whether the IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A and rs6953668 G>A genotypes in controls conformed to Hardy–Weinberg equilibrium (HWE) was determined by an Internet-based calculator (http://ihg.gsf.de/cgi-bin/hw/hwa1.pl).24–30 A P<0.05 (two-tailed) was accepted as the criterion of statistical significance. The relationship between IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A and rs6953668 G>A polymorphisms with NSCLC susceptibility was assessed by crude/adjusted ORs and 95% CIs. Adjusted for gender, age, tobacco use, drinking status, and BMI, multivariate linear regression was carried out to evaluate the relationship of these SNPs with susceptibility to NSCLC. We used an online SHEsis software (http://analysis.bio-x.cn/myAnalysis.php)31 to establish haplotypes of IGF2BP2 and IGFBP3 genes. We used SAS 9.4 software (windows version; SAS Institute Inc., Cary, NC, USA) to do all statistical analyses.
Results
Baseline characteristics
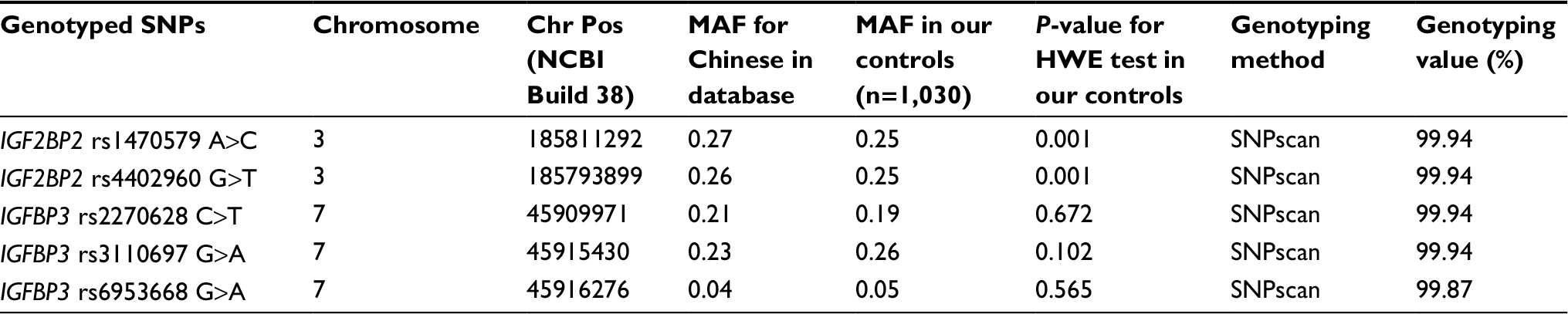
A total of 521 NSCLC cases were included in this study. The mean age of NSCLC cases was 59.76 years (SD: 10.71 years). Among them, 415 were adenocarcinoma (79.65%), 85 were squamous cell carcinoma (16.31%), and 21 were other subtype of NSCLC (4.03%). NSCLC patients included 315 cases with stage I/II and 206 with stage III/IV. Disease staging was determined according to American Joint Committee on Cancer criteria (version 7, 2010). We recruited 1,030 non-cancer controls, involving 588 males (57.09%) and 442 females (42.91%). Their mean ± SD age was 60.34±9.11 years. Characteristics of NSCLC cases and controls included in this study are listed in Table 1. The primary information for IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A SNPs was shown in Table 2. The successful ratio was >99.00% for each SNP. Minor allele frequency (MAF) of IGF2BP2 and IGFBP3 SNPs was similar to the data in Chinese database (Table 2). In controls, the genotype frequencies for IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A polymorphisms were in HWE (Table 2).
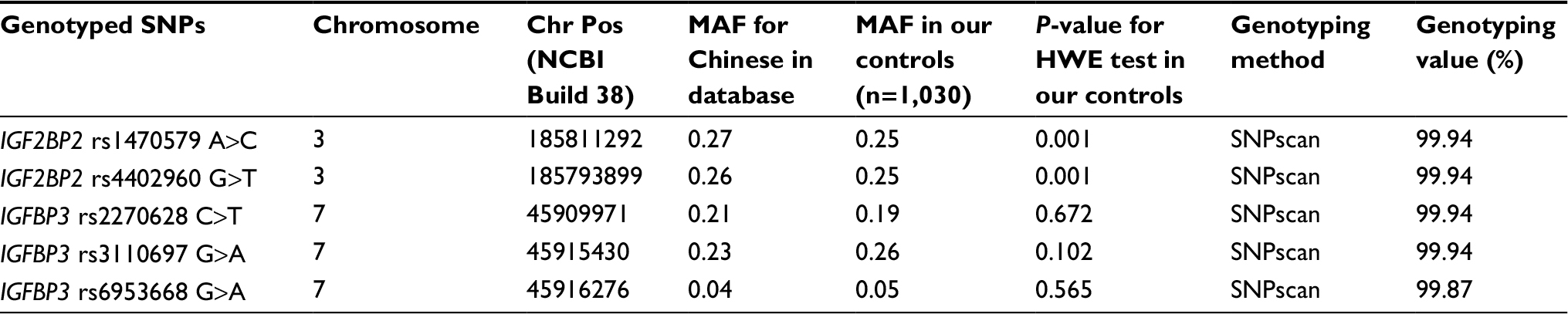 | Table 2 Primary information for IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A polymorphisms Abbreviations: MAF, minor allele frequency; HWE, Hardy–Weinberg equilibrium; SNP, single-nucleotide polymorphism. |
Association of IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A polymorphisms with NSCLC
Table 3 showed the frequencies of IGF2BP2 and IGFBP3 genotypes in different NSCLC subgroups and control group. Results of the single locus analyses were summarized in Table 4. We found that there was no difference in IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A genotype distribution among overall NSCLC patients and controls. In addition, similar findings were also identified among different NSCLC subtype and controls.
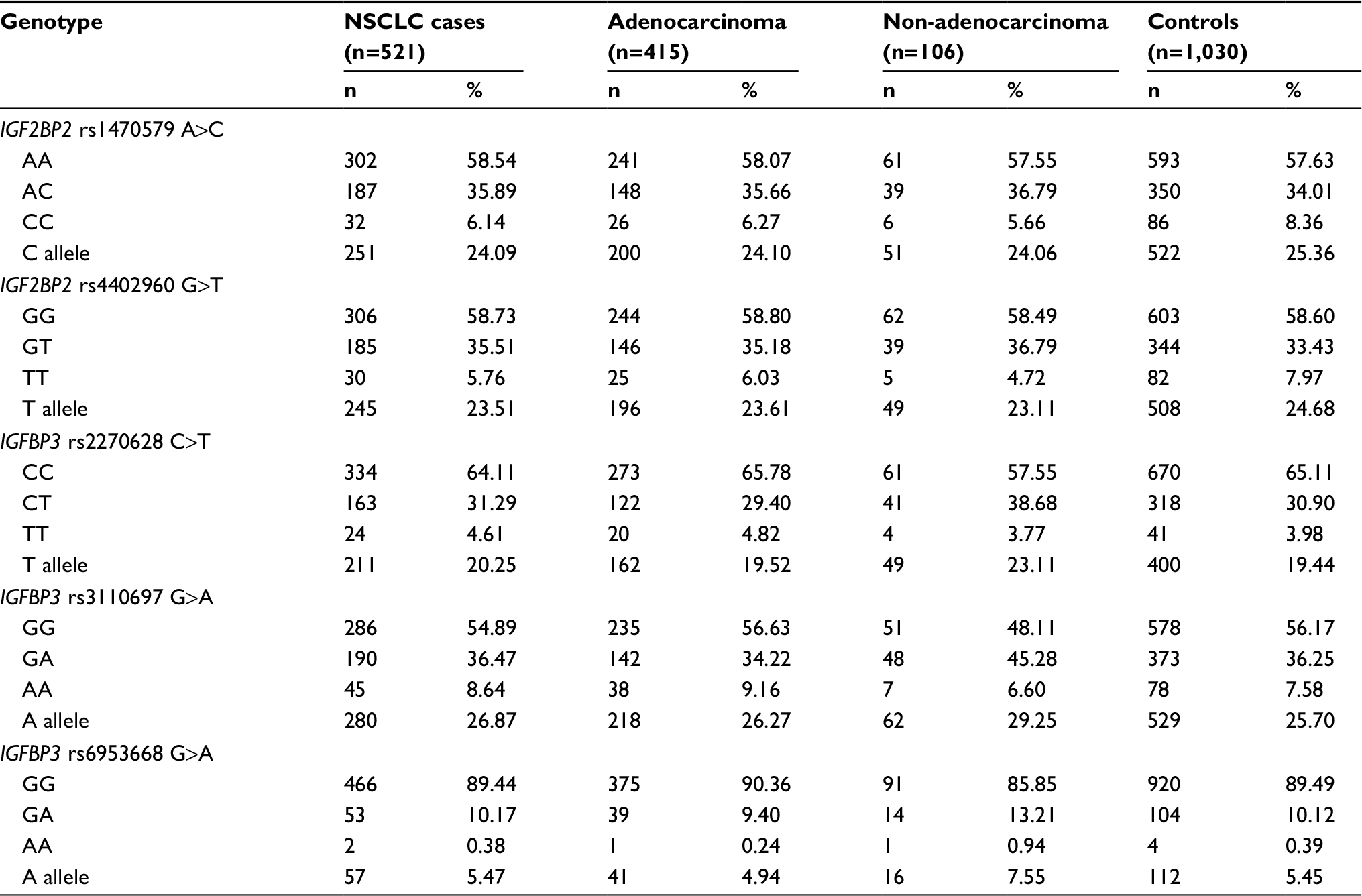 | Table 3 The frequencies of IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A and rs6953668 G>A polymorphisms in different NSCLC subgroups Abbreviation: NSCLC, non-small-cell lung cancer. |
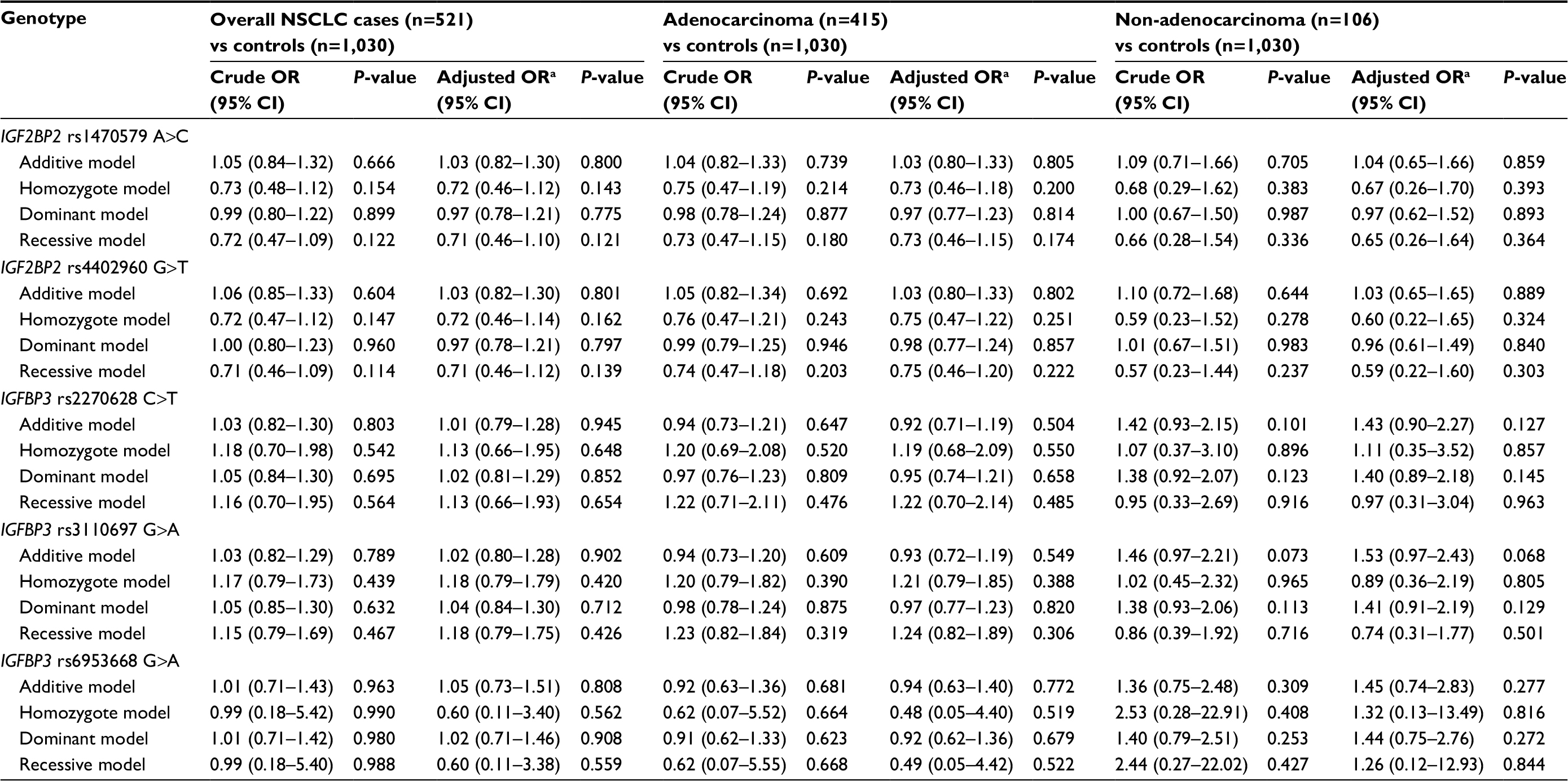 | Table 4 Logistic regression analyses of association of IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A polymorphisms with risk of NSCLC Note: aAdjusted for age, sex, smoking status, alcohol use, and BMI status. Abbreviations: NSCLC, non-small-cell lung cancer; BMI, body mass index. |
Association of IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A polymorphisms with NSCLC in a stratification analysis
As shown in Table 5, the stratified analyses suggested that IGF2BP2 rs1470579 A>C polymorphism decreased the risk of NSCLC in some subgroups (female subgroup: CC vs AA: adjusted OR =0.46, 95% CI =0.23–0.94, P=0.032 and CC vs AC/AA: adjusted OR =0.46, 95% CI =0.23–0.92, P=0.028; <60 years subgroup: CC vs AA: adjusted OR =0.36, 95% CI =0.16–0.80, P=0.012 and CC vs AC/AA: adjusted OR =0.37, 95% CI =0.17–0.81, P=0.013; and never drinking subgroup: CC vs AA: adjusted OR =0.61, 95% CI =0.37–0.99, P=0.046 and CC vs AC/AA: adjusted OR =0.59, 95% CI =0.36–0.95, P=0.031).
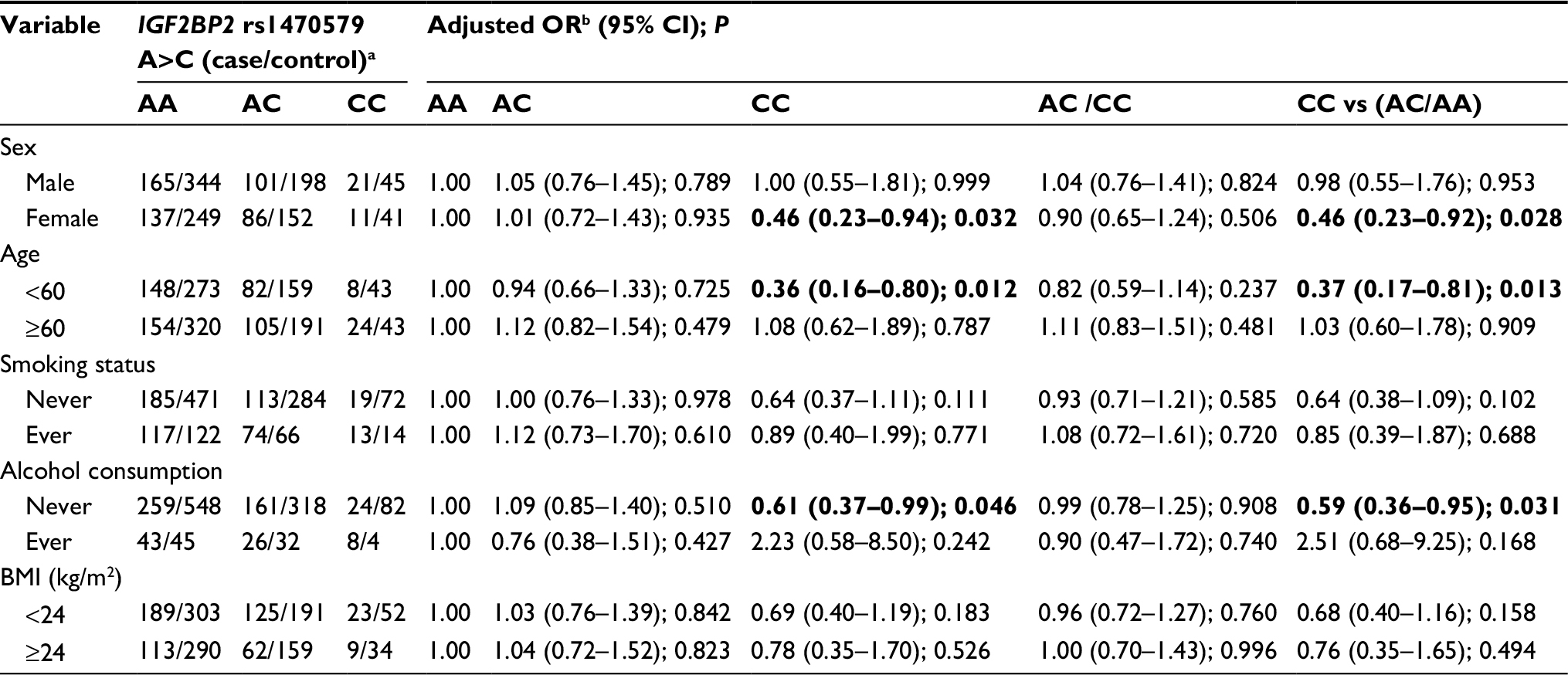 | Table 5 Stratified analyses between IGF2BP2 rs1470579 A>C polymorphism and NSCLC risk by sex, age, BMI, smoking status, and alcohol consumption Notes: aFor IGF2BP2 rs1470579 A>C, the genotyping was successful in 521 (100.00%) NSCLC cases and 1,029 (99.90%) controls. bAdjusted for multiple comparisons (age, sex, BMI, smoking status, and alcohol consumption [besides stratified factors accordingly]) in a logistic regression model. Bold values are statistically significant (P<0.05). Abbreviations: NSCLC, non-small-cell lung cancer; BMI, body mass index. |
As shown in Table 6, we also found that IGF2BP2 rs4402960 G>T polymorphism decreased the risk of NSCLC in some subgroups (female subgroup: TT vs GG: adjusted OR =0.46, 95% CI =0.21–0.93, P=0.031 and TT vs GT/GG: adjusted OR =0.44, 95% CI =0.21–0.91, P=0.026; <60 subgroup: TT vs GG: adjusted OR =0.44, 95% CI =0.20–0.95, P=0.037 and TT vs GT/GG: adjusted OR =0.45, 95% CI =0.21–0.96, P=0.038; and never drinking subgroup: TT vs GT/GG: adjusted OR =0.61, 95% CI =0.37–0.99, P=0.046).
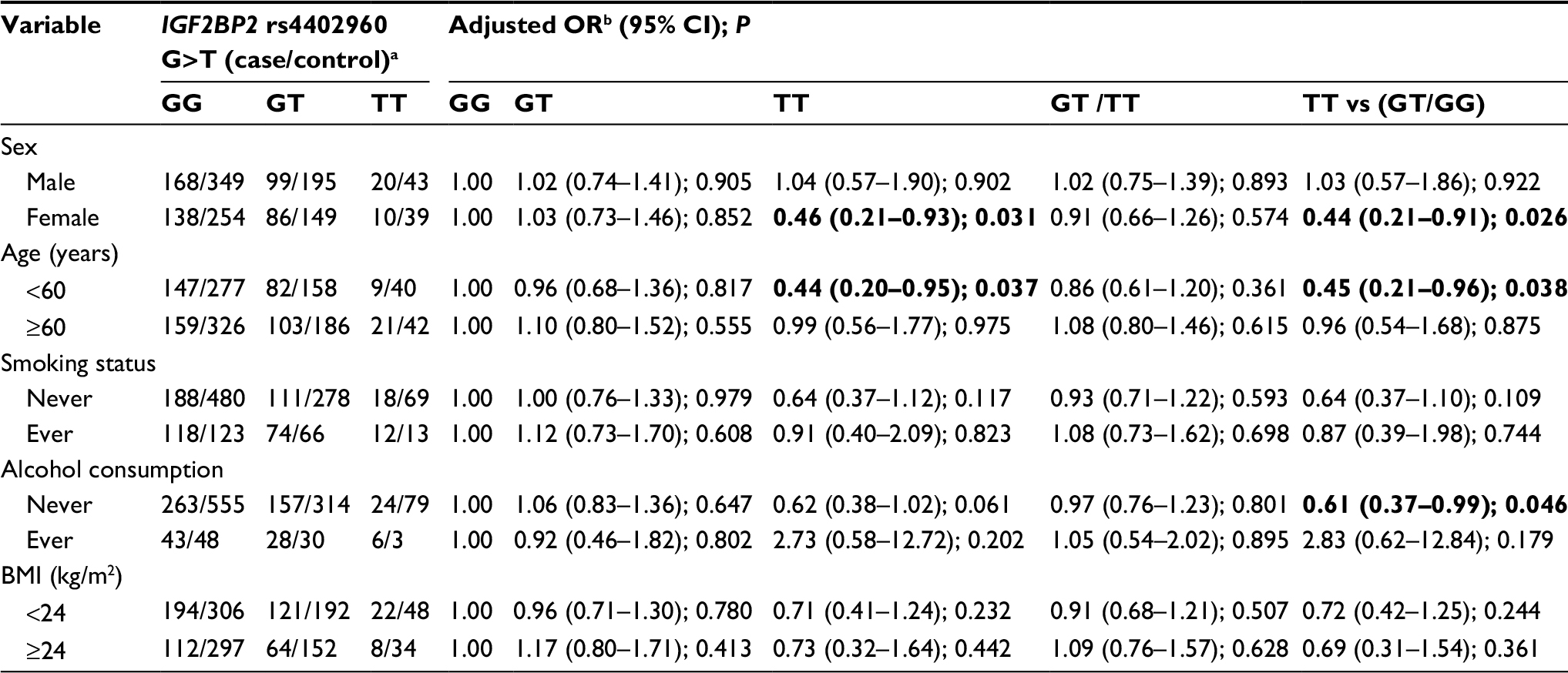 | Table 6 Stratified analyses between IGF2BP2 rs4402960 G>T polymorphism and NSCLC risk by sex, age, BMI, smoking status, and alcohol consumption Notes: aFor IGF2BP2 rs4402960 G>T, the genotyping was successful in 521 (100.00%) NSCLC cases and 1,029 (99.90%) controls. bAdjusted for multiple comparisons (age, sex, BMI, smoking status and alcohol consumption [besides stratified factors accordingly]) in a logistic regression model. Bold values are statistically significant (P<0.05). Abbreviations: NSCLC, non-small-cell lung cancer; BMI, body mass index. |
However, we found no significant difference in IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A genotype distribution among NSCLC cases and controls (Tables 7–9, respectively).
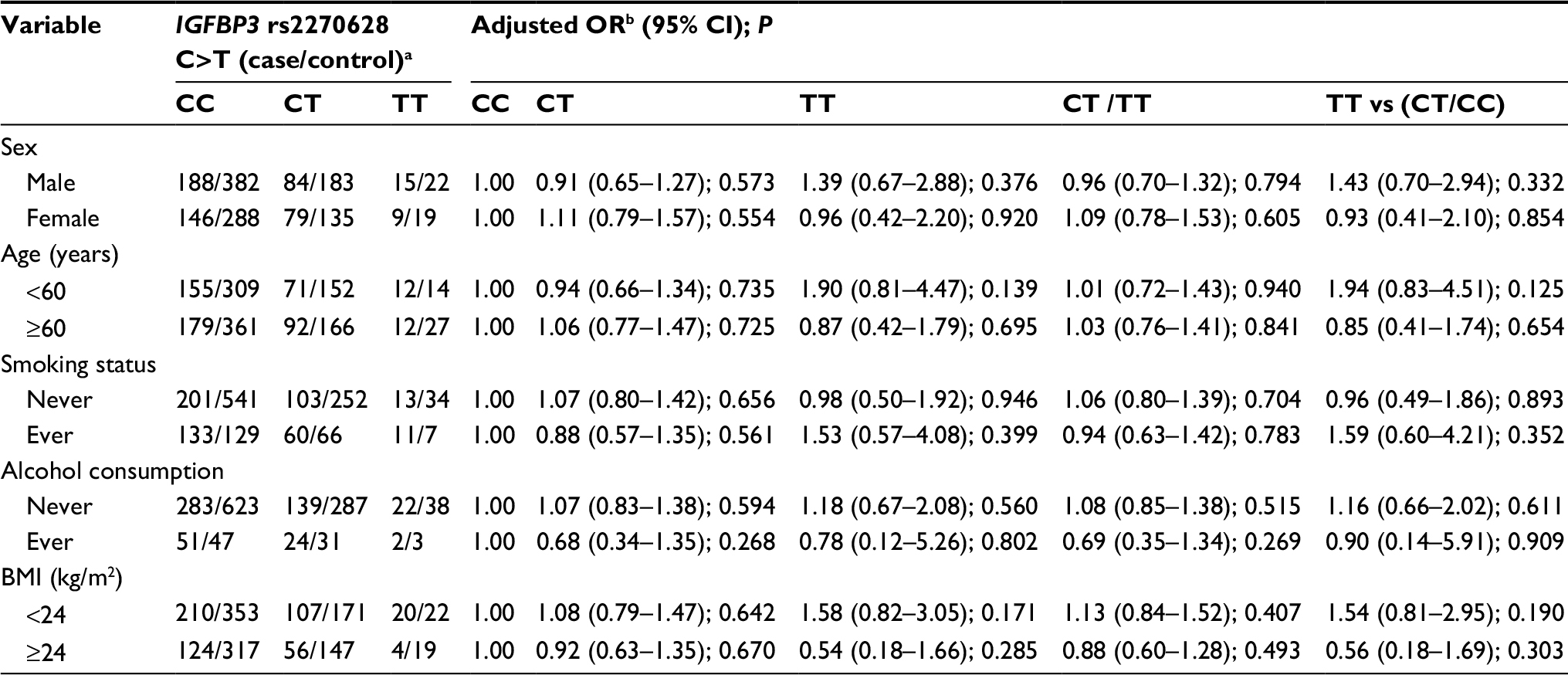 | Table 7 Stratified analyses between IGFBP3 rs2270628 C>T polymorphism and NSCLC risk by sex, age, BMI, smoking status, and alcohol consumption Notes: aFor IGFBP3 rs2270628 C>T, the genotyping was successful in 521 (100%) NSCLC cases and 1,029 (99.90%) controls. bAdjusted for multiple comparisons (age, sex, BMI, smoking status, and alcohol consumption [besides stratified factors accordingly]) in a logistic regression model. Abbreviations: NSCLC, non-small-cell lung cancer; BMI, body mass index. |
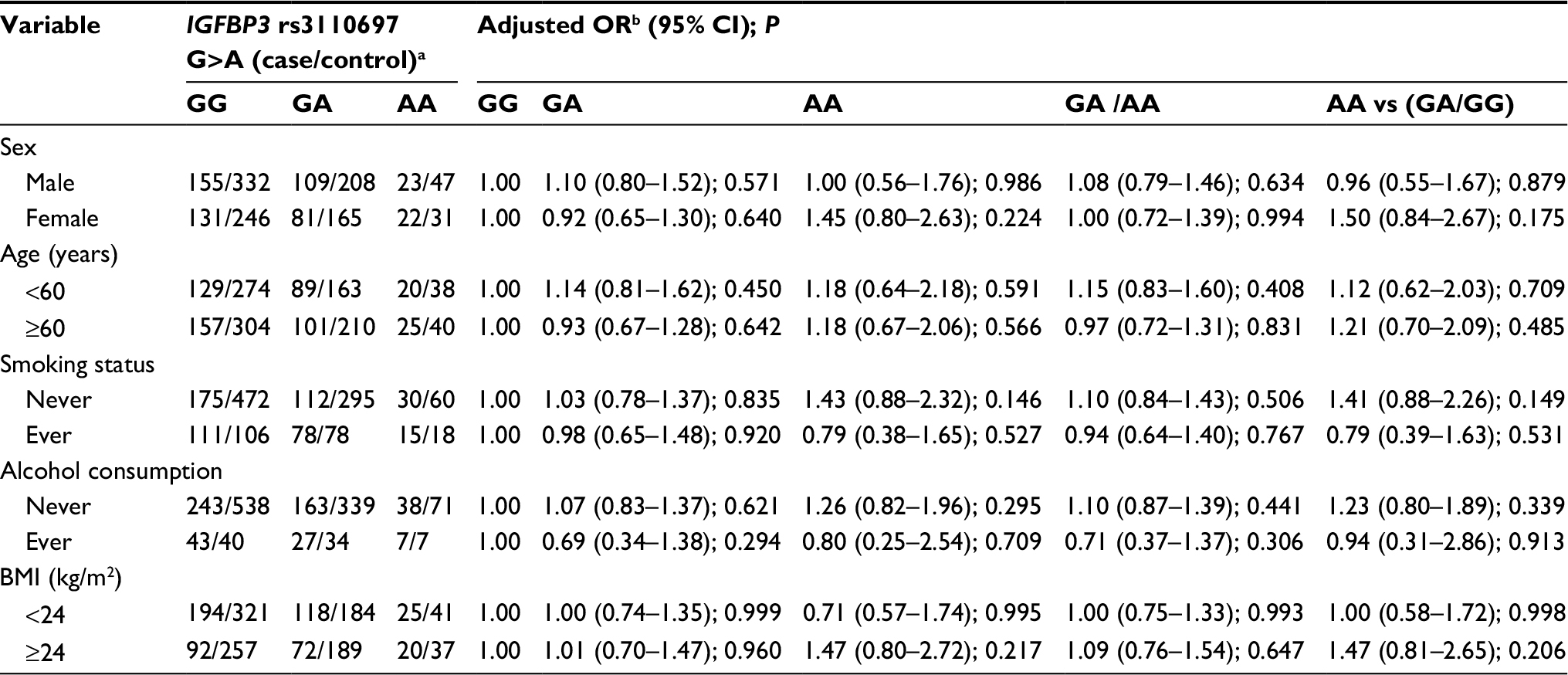 | Table 8 Stratified analyses between IGFBP3 rs3110697 G>A polymorphism and NSCLC risk by sex, age, BMI, smoking status, and alcohol consumption Notes: aFor IGFBP3 rs3110697 G>A, the genotyping was successful in 521 (100%) NSCLC cases and 1,029 (99.90%) controls. bAdjusted for multiple comparisons (age, sex, BMI, smoking status, and alcohol consumption [besides stratified factors accordingly]) in a logistic regression model. Abbreviations: NSCLC, non-small-cell lung cancer; BMI, body mass index. |
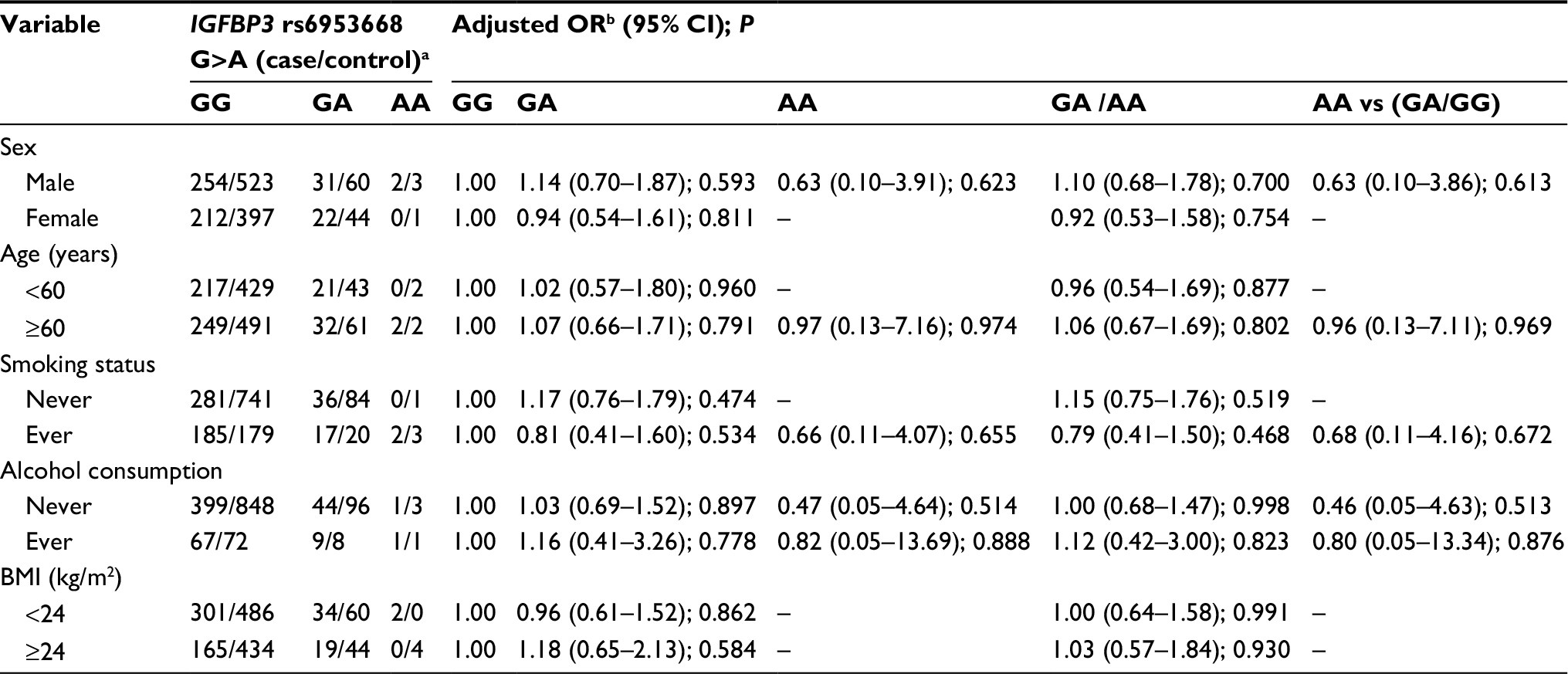 | Table 9 Stratified analyses between IGFBP3 rs6953668 G>A polymorphism and NSCLC risk by sex, age, BMI, smoking status, and alcohol consumption Notes: aFor IGFBP3 rs6953668 G>A, the genotyping was successful in 521 (100%) NSCLC cases and 1,028 (99.81%) controls. bAdjusted for multiple comparisons (age, sex, BMI, smoking status, and alcohol consumption [besides stratified factors accordingly]) in a logistic regression model. Abbreviations: NSCLC, non-small-cell lung cancer; BMI, body mass index. |
SNP haplotypes
We harnessed an online SHEsis software31 to establish haplotypes of IGF2BP2 and IGFBP3 gene (Table 10). Finally, 19 haplotypes of IGF2BP2 and IGFBP3 genes were constructed. When Ars1470579Crs2270628Grs3110697Grs4402960Grs6953668 haplotype was used as reference, Ars1470579Crs2270628Grs3110697Grs4402960Ars6953668 haplotype decreased susceptibility to NSCLC (P=0.007, Table 10).
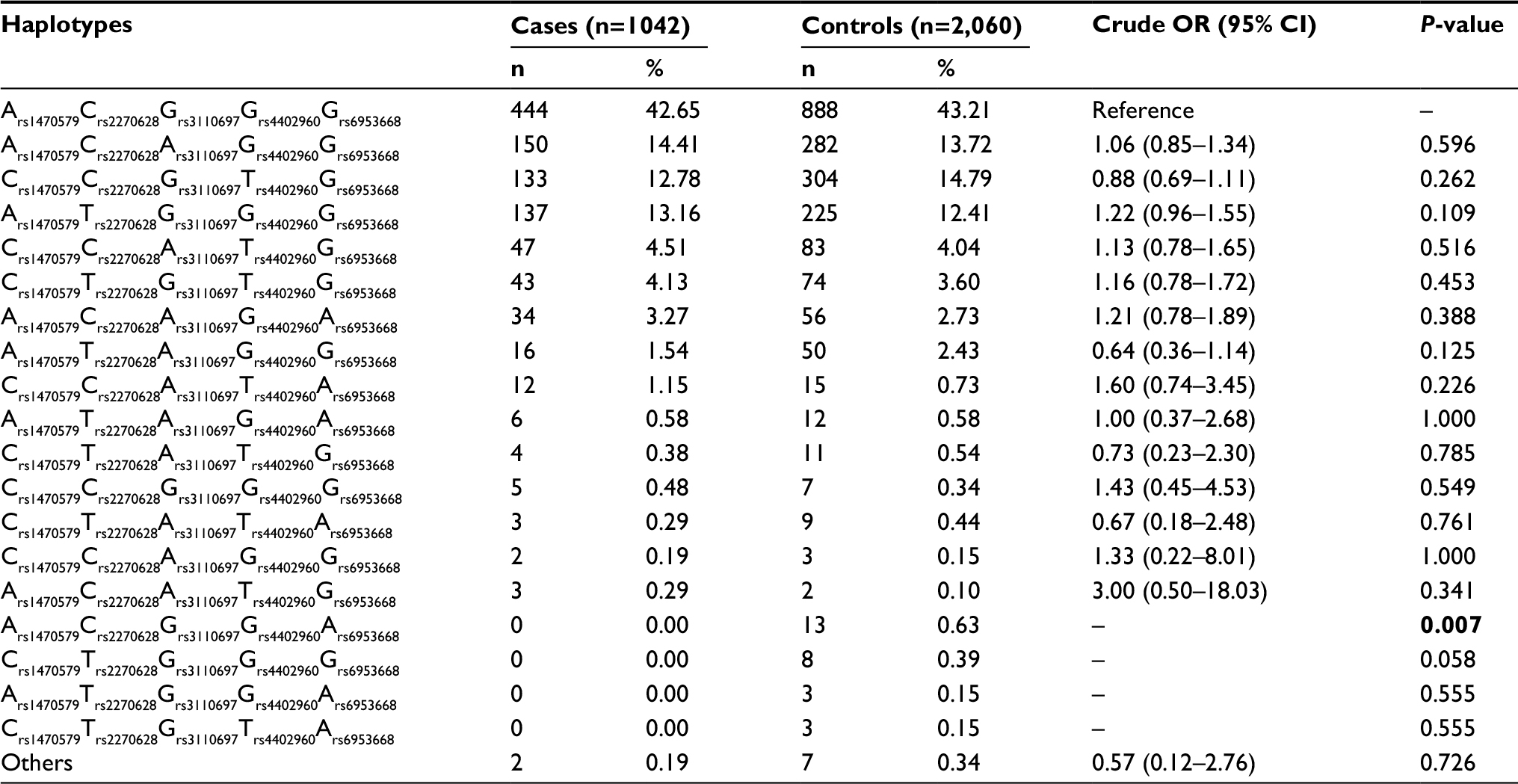 | Table 10 IGF2BP2 and IGFBP3 haplotype frequencies (%) in patients and controls and risk of NSCLC Note: Bold values are statistically significant (P<0.05). Abbreviation: NSCLC, non-small-cell lung cancer. |
Discussion
In this study, we explored the potential relationship of IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A SNPs with susceptibility to NSCLC. We found that IGF2BP2 rs1470579 A>C, rs4402960 G>T and IGFBP3 rs2270628 C>T, rs3110697 G>A, and rs6953668 G>A polymorphisms might not confer risk to overall NSCLC. However, in stratified analyses, we found significant associations between IGF2BP2 rs1470579 A>C, rs4402960 G>T polymorphisms and decreased risk of NSCLC in female, <60 years, and never drinking subgroups. We also found that Ars1470579Crs2270628 Grs3110697Grs4402960Ars6953668 haplotype decreased susceptibility to NSCLC. To our knowledge, the present study was the first investigation to identify the correlation between IGF2BP2 rs1470579 A>C, rs4402960 G>T polymorphisms and the decreased risk of NSCLC in Asians.
Dai et al reported that IGF2BP2 is a tumor promoter which promotes malignancy proliferation through its client mRNAs IGF2 and high mobility group A1.32 In many human malignancies, the gene encoding IGF2BP2 was found to be amplified and overexpressed. Recently, Barghash et al found that elevated expression of IGF2BP2 was associated with a shorter survival and metastasis in esophageal adenocarcinoma.33 Several case–control studies reported that IGF2BP2 rs4402960 G>T polymorphism was associated with the risk of T2DM and might affect the therapeutic efficacy of antidiabetic in Chinese population.34,35 We found that the IGF2BP2 rs4402960 TT genotype was associated with the decreased susceptibility of NSCLC among female, <60 years, and never drinking patients. Previous report showed that IGF2BP2 rs4402960 G>T polymorphism was associated with the increased risk of breast cancer in a Chinese population.12 The other case–control study did not find any association between IGF2BP2 rs4402960 G>T polymorphism and colorectal cancer.36 We identified that IGF2BP2 rs4402960 T allele might probably be a protective factor for NSCLC, which was not consistent with the findings of previous studies. It is believed that there are some LC-related driver genes possessing low frequency variant, which modify the states of chromatin or DNA.37 In addition, intronic region could bind to some proteins and even directly alter special gene transcription.37–39 rs4402960 G>T polymorphism is located in the intron region of IGF2BP2 gene, which may influence the post-transcription process. IGF2BP2 rs4402960 G>T polymorphism may accordingly alter the risk of NSCLC through post-transcription process mechanisms, and our study suggested that IGF2BP2 rs4402960 TT genotype and T allele play an important role in lung carcinogenesis. In the future, the function of the IGF2BP2 rs4402960 G>T polymorphism needs to be explored in NSCLC patients. A replicated study should also be carried out.
We found that there was a significant difference in genotype distribution of IGF2BP2 rs1470579 A>C polymorphism between NSCLC patients and controls in female, <60 years, and never drinking subgroups. The IGF2BP2 rs1470579 CC genotype was less frequent in NSCLC cases compared with controls in some subgroups, suggesting that IGF2BP2 rs1470579 CC genotype decreased the risk of NSCLC. Recent reports showed that IGF2BP2 rs1470579 A>C SNP might play important roles in different diseases. Some previous studies suggested that IGF2BP2 rs1470579 A>C was associated with the risk of type 2 diabetes mellitus (T2DM). For example, Horikawa et al found that this SNP was a susceptibility marker for T2DM in a Japanese population,40 and Huang et al found that this SNP was a risk factor for T2DM in a Chinese population.35 In addition, a quantitative assessment demonstrated that this common polymorphism was associated with the development of T2DM. Therefore, whether the A-to-C variant in the intron region of IGF2BP2 gene does influence the expression of IGF2BP2 gene needs to be further studied.
Using SHEsis software,31 we constructed 19 haplotypes to assess the potential inherited patterns of IGF2BP2 and IGFBP3 genes. Compared with Ars1470579Crs2270628Grs3110697Grs4402960Grs6953668 haplotype, we found that Ars1470579Crs2270628Grs3110697Grs4402960Ars6953668 haplotype significantly decreased the risk of NSCLC (P=0.007, Table 10). To the best of our knowledge, we first identified the relationship of this haplotypes with susceptibility to NSCLC. However, this rare haplotype only influenced a very minor fraction (<1%) of the studied populations. In the future, more studies with a larger sample size and an adequate methodological quality should be performed to confirm or refute these primary findings.
Some limitations in the current study should be acknowledged. First, we selected only some functional polymorphisms in IGF2BP2 and IGFBP3 genes. In the future, a fine-mapping study should be conducted to further study the potential relationship of GF2BP2 and IGFBP3 polymorphisms with risk of NSCLC. Second, in this case–control study, the sample size of NSCLC patients was relatively limited, which might lead to lack of sufficient power to identify true correlation, especially in the subgroup analysis. In the future, more NSCLC cases and controls should be enrolled, and a replicated study should be carried out. Third, this case–control study was hospital-based. The cancer-free controls recruited from local hospitals might not completely represent a general Eastern Chinese Han population. Fourth, the genotype frequencies of IGF2BP2 rs1470579 A>C and rs4402960 G>T polymorphisms were not in HWE, which might lead to bias. Fifth, a functional experimentation was not performed. Finally, because of the lack of the information on survival of NSCLC, we did not further analyze the role of GF2BP2 and IGFBP3 variants on NSCLC prognosis.
Conclusion
Our study suggests that IGF2BP2 rs1470579 A>C, rs4402960 G>T polymorphisms are candidates for decreased susceptibility to NSCLC in Eastern Chinese Han population among female, <60 years, and never drinking subgroups. Compared with Ars1470579 Crs2270628Grs3110697Grs4402960Grs6953668 haplotype, Ars1470579Crs2270628Grs3110697Grs4402960Ars6953668 haplotype significantly decreased risk of NSCLC. In the future, more case–control studies with comprehensive resequencing or SNP functional analysis are needed to confirm these preliminary findings.
Acknowledgments
We appreciate all subjects who participated in this study. We wish to thank Dr Yan Liu (Genesky Biotechnologies Inc., Shanghai, China) for technical support. This study was supported in part by the Natural Science Foundation of Fujian Province (Grant No. 2017J01291).
Disclosure
The authors report no conflicts of interest in this work.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
Zhang JY, Chan EK, Peng XX, Tan EM. A novel cytoplasmic protein with RNA-binding motifs is an autoantigen in human hepatocellular carcinoma. J Exp Med. 1999;189(7):1101–1110. | ||
Nielsen J, Christiansen J, Lykke-Andersen J, Johnsen AH, Wewer UM, Nielsen FC. A family of insulin-like growth factor II mRNA-binding proteins represses translation in late development. Mol Cell Biol. 1999;19(2):1262–1270. | ||
Gu L, Shigemasa K, Ohama K. Increased expression of IGF II mRNA-binding protein 1 mRNA is associated with an advanced clinical stage and poor prognosis in patients with ovarian cancer. Int J Oncol. 2004;24(3):671–678. | ||
Png KJ, Halberg N, Yoshida M, Tavazoie SF. A microRNA regulon that mediates endothelial recruitment and metastasis by cancer cells. Nature. 2011;481(7380):190–194. | ||
Liu B, Chen Y, Yang J. LncRNAs are altered in lung squamous cell carcinoma and lung adenocarcinoma. Oncotarget. 2017;8(15):24275–24291. | ||
Khandwala HM, McCutcheon IE, Flyvbjerg A, Friend KE. The effects of insulin-like growth factors on tumorigenesis and neoplastic growth. Endocr Rev. 2000;21(3):215–244. | ||
Pollak M. Insulin-like growth factor physiology and neoplasia. Growth Horm IGF Res. 2000;10(Suppl A):S6–S7. | ||
Papadimitrakopoulou VA, Brown EN, Liu DD, et al. The prognostic role of loss of insulin-like growth factor-binding protein-3 expression in head and neck carcinogenesis. Cancer Lett. 2006;239(1):136–143. | ||
Lee HY, Moon H, Chun KH, et al. Effects of insulin-like growth factor binding protein-3 and farnesyltransferase inhibitor SCH66336 on Akt expression and apoptosis in non-small-cell lung cancer cells. J Natl Cancer Inst. 2004;96(20):1536–1548. | ||
Wang YA, Sun Y, Palmer J, et al. IGFBP3 Modulates lung tumorigenesis and cell growth through IGF1 signaling. Mol Cancer Res. 2017;15(7):896–904. | ||
Liu G, Zhu T, Cui Y, et al. Correlation between IGF2BP2 gene polymorphism and the risk of breast cancer in Chinese Han women. Biomed Pharmacother. 2015;69:297–300. | ||
Terry KL, Tworoger SS, Gates MA, Cramer DW, Hankinson SE. Common genetic variation in IGF1, IGFBP1 and IGFBP3 and ovarian cancer risk. Carcinogenesis. 2009;30(12):2042–2046. | ||
Cheng I, Delellis Henderson K, Haiman CA, et al. Genetic determinants of circulating insulin-like growth factor (IGF)-I, IGF binding protein (BP)-1, and IGFBP-3 levels in a multiethnic population. J Clin Endocrinol Metab. 2007;92(9):3660–3666. | ||
Deming SL, Ren Z, Wen W, et al. Genetic variation in IGF1, IGF-1R, IGFALS, and IGFBP3 in breast cancer survival among Chinese women: a report from the Shanghai Breast Cancer Study. Breast Cancer Res Treat. 2007;104(3):309–319. | ||
Zhai Y, Zhao WH, Chen CM. Verification on the cut-offs of waist circumference for defining central obesity in Chinese elderly and tall adults. Zhonghua Liu Xing Bing Xue Za Zhi. 2010;31(6):621–625. | ||
Zhang X, Zhang S, Li Y, et al. Association of obesity and atrial fibrillation among middle-aged and elderly Chinese. Int J Obes. 2009;33(11):1318–1325. | ||
Tang W, Zhang S, Qiu H, et al. Genetic variations in MTHFR and esophageal squamous cell carcinoma susceptibility in Chinese Han population. Med Oncol. 2014;31(5):915. | ||
Qiu H, Wang Y, Kang M, et al. The relationship between IGF2BP2 and PPARG polymorphisms and susceptibility to esophageal squamous-cell carcinomas in the eastern Chinese Han population. Onco Targets Ther. 2017;10:5525–5532. | ||
Liu X, Chen Z, Zhao X, et al. Effects of IGF2BP2, KCNQ1 and GCKR polymorphisms on clinical outcome in metastatic gastric cancer treated with EOF regimen. Pharmacogenomics. 2015;16(9):959–970. | ||
Yang HP, Liu JF, Rao J, et al. Insulin-like growth factor binding protein-3 (IGFBP-3) genetic variant and the risk of esophageal squamous cell carcinoma in a Chinese population. Genet Mol Res. 2014;13(2):4146–4153. | ||
Liu C, Tang W, Chen S, et al. IGFBP3 polymorphisms and risk of esophageal cancer in a Chinese population. Int J Clin Exp Med. 2015;8(9):17006–17014. | ||
Yin J, Wang X, Wei J, et al. Interleukin 12B rs3212227 T > G polymorphism was associated with an increased risk of gastric cardiac adenocarcinoma in a Chinese population. Dis Esophagus. 2015;28(3):291–298. | ||
Zhang S, Wang Y, Jiang H, et al. Association between the CD28 IVS3 +17T>C (rs3116496) polymorphism and cancer susceptibility: a meta-analysis involving 8,843 subjects. Int J Clin Exp Med. 2015;8(10):17353–17361. | ||
Zhang S, Wang Y, Jiang H, et al. Peroxisome proliferator-activated receptor gamma rs1801282 C>G polymorphism is associated with polycystic ovary syndrome susceptibility: a meta-analysis involving 7,069 subjects. Int J Clin Exp Med. 2015;8(10):17418–17429. | ||
Tang W, Wang Y, Jiang H, et al. Programmed death-1 (PD-1) rs2227981 C > T polymorphism is associated with cancer susceptibility: a meta-analysis. Int J Clin Exp Med. 2015;8(12):22278–22285. | ||
Qiu H, Cheng C, Wang Y, et al. Investigation of cyclin D1 rs9344 G>A polymorphism in colorectal cancer: a meta-analysis involving 13,642 subjects. Onco Targets Ther. 2016;9:6641–6650. | ||
Tang W, Qiu H, Ding H, et al. Association between the STK15 F31I polymorphism and cancer susceptibility: a meta-analysis involving 43,626 subjects. PLoS One. 2013;8(12):e82790. | ||
Tang W, Qiu H, Jiang H, et al. Lack of association between cytotoxic T-lymphocyte antigen 4 (CTLA-4) -1722T/C (rs733618) polymorphism and cancer risk: from a case-control study to a meta-analysis. PLoS One. 2014;9(4):e94039. | ||
Tang W, Wang Y, Chen S, et al. Investigation of cytotoxic T-lymphocyte antigen 4 polymorphisms in gastric cardia adenocarcinoma. Scand J Immunol. 2016;83(3):212–218. | ||
Shi YY, He L. SHEsis, a powerful software platform for analyses of linkage disequilibrium, haplotype construction, and genetic association at polymorphism loci. Cell Res. 2005;15(2):97–98. | ||
Dai N, Ji F, Wright J, Minichiello L, Sadreyev R, Avruch J. IGF2 mRNA binding protein-2 is a tumor promoter that drives cancer proliferation through its client mRNAs IGF2 and HMGA1. Elife. 2017;6:e27155. | ||
Barghash A, Golob-Schwarzl N, Helms V, Haybaeck J, Kessler SM. Elevated expression of the IGF2 mRNA binding protein 2 (IGF2BP2/IMP2) is linked to short survival and metastasis in esophageal adenocarcinoma. Oncotarget. 2016;7(31):49743–49750. | ||
Zhang LF, Pei Q, Yang GP, et al. The effect of IGF2BP2 gene polymorphisms on pioglitazone response in Chinese type 2 diabetes patients. Pharmacology. 2014;94(3–4):115–122. | ||
Huang Q, Yin JY, Dai XP, et al. IGF2BP2 variations influence repaglinide response and risk of type 2 diabetes in Chinese population. Acta Pharmacol Sin. 2010;31(6):709–717. | ||
Sainz J, Rudolph A, Hoffmeister M, et al. Effect of type 2 diabetes predisposing genetic variants on colorectal cancer risk. J Clin Endocrinol Metab. 2012;97(5):E845–E851. | ||
Zhu QG, Zhang SM, Ding XX, He B, Zhang HQ. Driver genes in non-small cell lung cancer: Characteristics, detection methods, and targeted therapies. Oncotarget. 2017;8(34):57680–57692. | ||
Yan B, Guan D, Wang C, et al. An integrative method to decode regulatory logics in gene transcription. Nat Commun. 2017;8(1):1044. | ||
He B, Lu C, Zheng G, et al. Combination therapeutics in complex diseases. J Cell Mol Med. 2016;20(12):2231–2240. | ||
Horikawa Y, Miyake K, Yasuda K, et al. Replication of genome-wide association studies of type 2 diabetes susceptibility in Japan. J Clin Endocrinol Metab. 2008;93(8):3136–3141. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.