Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Relationship Between α-Glucosidase Inhibitors Application and Bone Mineral Density in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Received 10 July 2025
Accepted for publication 5 November 2025
Published 16 November 2025 Volume 2025:18 Pages 4277—4286
DOI https://doi.org/10.2147/DMSO.S552309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Xiumei Luo,1,2 Shangjian Li,1,2 Ning Chen1,2
1Department of Endocrinology, Fudan University Zhongshan Hospital Xiamen Branch, Xiamen, Fujian, People’s Republic of China; 2Xiamen Osteoporosis Specialized Prevention and Treatment Center, Xiamen, Fujian, People’s Republic of China
Correspondence: Ning Chen, Department of Endocrinology, Zhongshan Hospital (Xiamen), Fudan University, No. 668 Jinhu Road, Xiamen, 361000, People’s Republic of China, Tel/Fax +86-0592-3569583, Email [email protected]
Purpose: To investigate the correlation between α-glycosidase inhibitors (AGIs) and bone mineral density (BMD) in patients with type 2 diabetes mellitus (T2DM).
Patients and Methods: A total of 251 patients with T2DM admitted to the Zhongshan Hospital, Fudan University (Xiamen Branch) from September 2018 to September 2020 were enrolled. Baseline information of patients was analyzed according to different BMD subgroups. Clinical characteristics and BMD were compared between AGIs Group (n = 58) and non-AGIs group (n = 193). Multiple linear regression model was used to examine the relationship between AGIs application and BMD.
Results: The lower BMD group showed the characteristics of older age, longer duration of diabetes, lower body mass index (BMI) and estradiol (E2). In the AGIs group, the proportion of females, duration of diabetes, incidence of diabetic peripheral vascular disease and the use of sulfonylureas were significantly higher than those in the non-AGIs group (p < 0.05), the results of HbA1c, TC, TG, LDL, FT3, FT4 were opposite (p < 0.05). Compared with the non-AGIs group, the BMD of femoral neck and lumbar spine in the AGIs group was significantly decreased, FRAX score and the prevalence of osteoporosis were remarkably increased, accompanied by a decrease in β-CTX and P1NP level. Multivariate linear regression analysis showed a significant negative correlation between AGIs and lumbar BMD after adjustment for potential confounding variables (β = − 0.053, 95% CI − 0.100~0.006, P = 0.029).
Conclusion: This study indicates that the use of AGIs in patients with T2DM is significantly associated with an increased risk of BMD decline, osteoporosis, and fracture.
Keywords: type 2 diabetes mellitus, α-glucosidase inhibitor, BMD, osteoporosis
Introduction
The prevalence of diabetes is increasing globally. According to IDF Diabetes Atlas (11th edition), the number of adults aged 20–79 with diabetes worldwide reached 589 million in 2024 and is expected to rise to 853 million by 2050, with 90% cases being type 2 diabetes mellitus (T2DM).1 Compared with healthy individuals, patients with T2DM have an increased risk of developing osteoporosis and related fractures (such as hip, spinal, or even any site),2,3 which may be related to insulin resistance and poor glycemic control,4 inflammation,5 hyperosmotic diuresis triggering the loss of calcium and phosphorus, and the impact of hypoglycemic drugs,6 and other factors that lead to the deterioration of the bone micro-environment. The influence of hypoglycemic drugs on bone mineral density (BMD) is intricately linked to the particular drug in question.6–11 Several hypoglycemic drugs, such as rosiglitazone12–15 and canagliflozin,16 have been shown to adversely affect bone health. Since T2DM patients require the use of hypoglycemic drugs for most of the disease process, the influences of different classes of hypoglycemic drugs on BMD and fracture risk need to be carefully evaluated.
China is the country with the most extensive use of α-glucosidase inhibitors (AGIs) worldwide.17 The results of previous researches on the of AGIs on bone mass are extremely inconsistent, and the approaches used to detect and evaluate bone metabolism are often one-sided, so the effects of AGIs on bone health need to be further investigated.
In this study, BMD was measured by dual-energy X-ray absorptiometry (DXA), and the levels of bone metabolism biomarker and FRAX scores for fracture risk were combined to comprehensively analyze the impacts of AGIs application on the BMD and fracture risk of T2DM patients.
Materials and Methods
Study Population
A total of 251 patients with T2DM admitted to the Zhongshan Hospital, Fudan University (Xiamen Branch) from September 2018 to September 2020 were enrolled. All patients met the 2018 American Diabetes Association’s (ADA’s) criteria for the diagnosis and classification of diabetes and were negative for serum glutamic acid decarboxylase antibodies, including 149 males and 102 females, and all patients underwent DXA scan. Medical records of the patients were reviewed to confirm their medication status. According to whether AGIs (including acarbose and voglibose) were used at admission, the patients were divided into the AGIs group and the Non-AGIs group. In addition, the AGIs group was required to have received the drug for at least 3 months prior to enrollment, while the non-AGIs group had no history of relevant drug use within 3 months prior to enrollment.
Exclusion criteria include: (1) previously and currently diagnosed with type 1 diabetes, secondary diabetes, and special type diabetes; (2) age ≤ 18 years; (3) estimated glomerular filtration rate (eGFR) < 60 mL/(min ·1.73m2); (4) use of estrogen, progestogen, glucocorticoids, bisphosphonates, desmuximab and other agents that may affect BMD within the past six months; (5) presence of any disease prone to secondary osteoporosis, such as hyperparathyroidism, multiple myeloma, autoimmune diseases; (6) long-term bed rest leading to bone loss; (7) metal implants affecting BMD detection; (8) presence of psychiatric disease, infection or stress state, severe organ dysfunction, and any other conditions considering unsuitable for inclusion.
Information and Data Collection
Demographic and clinical information for all patients were obtained from the medical records and interviews, including age, gender, smoking history, drinking history, duration of T2DM, diabetic complications and hypoglycemic drug use. Height, weight, waist circumference, hip circumference, and blood pressure data were measured, and body mass index (BMI) and waist-to-hip ratio were calculated.
Laboratory indicators were based on early-morning venous blood after an overnight fast of 8 hours, and the detection items included: (1) Bone turnover markers: carboxy-terminal β-crosslinking telopeptide of type 1 collagen (β-CTX), type I procollagen amino-terminal peptide (P1NP), osteocalcin (OC) and 25-hydroxy vitamin D3 (25OHD). (2) Blood biochemical indicators: triacylglycerol (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), calcium (Ca), phosphorus (P), alanine aminotransferase (ALT), aspartate aminotransferase (AST), blood urea nitrogen (BUN), uric acid (UA), blood creatinine (CREA) and eGFR. (3) Glycometabolic indicators: glycated hemoglobin (HbA1c), fasting blood glucose (FBG), fasting insulin, and the HOMA-IR (Homeostatic Model Assessment for Insulin Resistance) was calculated according to the formula: fasting blood glucose (mmol·L−1) × fasting insulin (μU·mL−1)/22.5.18 (4) Hormone indicators: thyroid stimulating hormone (TSH), free triiodothyronine (FT3), free thyroxine (FT4), parathyroid hormone (PTH), estradiol (E2). Above indicators were determined by using the same methods as previously described.19
Definition of Osteoporosis and Assessment of Fracture Risk
Based on the Chinese guidelines for osteoporosis (2022 version),20 the definition of osteoporosis should include any one of the following three items: ① Minimum T-score of BMD ≤−2.5. ② Hip or vertebral fragility fractures, regardless of BMD measurement. ③ Fragility fractures of the proximal humerus, pelvis, or distal forearm with −2.5 < T-score < −1.0. BMD was measured by DXA (QDR4500A, Hologic Inc., Waltham MA, USA) at the femoral neck and lumbar spine (L1-L4), with a dedicated technician from the Department Medical Imaging responsible for the assessments. Fracture Risk Assessment Tool (FRAX) score21 was used to assess the 10-year probability of a major osteoporotic fracture and hip fracture.
Statistical Analysis
Data conforming to the normal distribution were expressed as mean ± standard deviation (SD), and T-test is used for statistical difference analysis. Non-normally distributed data were represented in terms of the median (P25, P75), and T-test was applied after the data was transformed into a normal distribution. Non-parametric test was conducted for data that could not be converted to normal. Group differences between the BMD tertiles were analyzed by ANOVA. Count data were expressed as n (%) and χ2 test was used. Multiple linear regression analysis was applied to explore the influence of AGIs on bone mass, with BMD as the dependent variable and related factors as covariates. Data were analyzed by SPSS 27.0 software, and statistical graphs were plotted by GraphPad Prism 9.0. P < 0.5 was considered statistically significant.
Results
Demographic and Clinical Characteristics of the Population Stratified by BMD
The patients were divided into groups by tertiles of femoral neck BMD and lumbar spine total BMD, respectively. The demographic and clinical characteristics of different BMD patients were compared in Table 1. In all groups, patients with lower BMI and E2 levels tended to have lower BMD. In the femoral neck BMD subgroups, the decrease of BMD was accompanied by the increase of patient’s age, the prolongation of diabetic course and the decline of LDL and FT4 levels (P < 0.05), and there were no significant differences in the use of hypoglycemic agents. However, in the lumbar spine BMD subgroups, the proportion of patients with AGIs application in the lowest BMD group was obviously higher and the uric acid level was notably lower than that in the other two groups (P < 0.05), while there were no marked deviations in age, diabetes course, LDL and FT4 levels among the groups. No striking differences between groups were found for any of the other analyzed indicators in both femoral neck BMD and lumbar spine BMD groups.
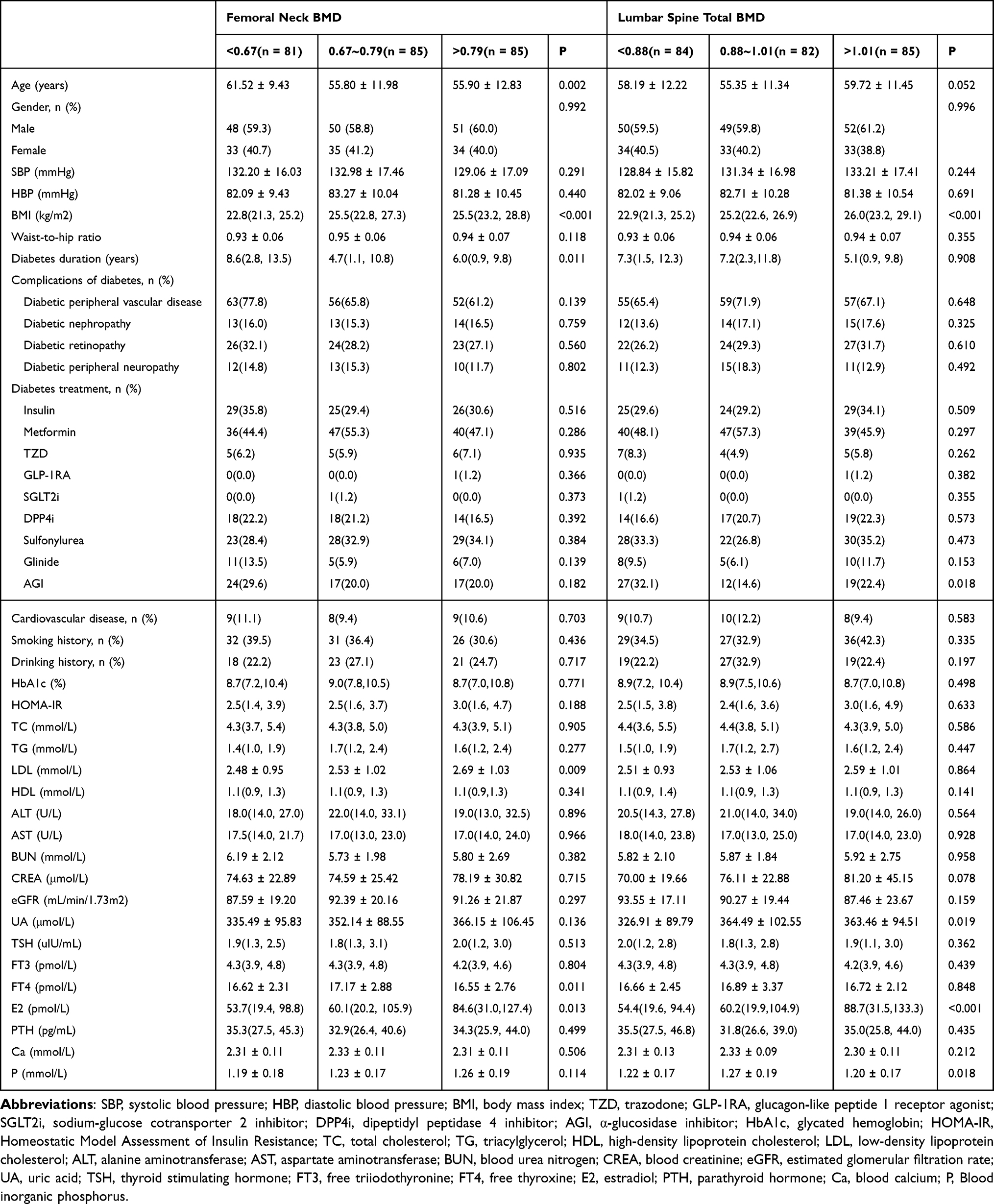 |
Table 1 Demographic and Clinical Characteristics of the Population Stratified by BMD |
Comparison of Basic Data Between T2DM Patients with and without AGIs Application
Of the 251 T2DM patients included, 58 received AGIs therapy and 193 did not. The AGIs group consisted of 26 males and 32 females, and the non-AGIs group consisted of 123 males and 70 females. Table 2 showed that compared with the Non-AGIs group, the AGIs group had obvious higher proportion of female, longer diabetes course, more patients with concomitant diabetic peripheral vascular lesions, and sulfonylurea application, and had significant lower values of HbA1c, TC, TG, LDL, FT3, and FT4 (all P < 0.05). The remaining parameters between the two groups were not statistically significant.
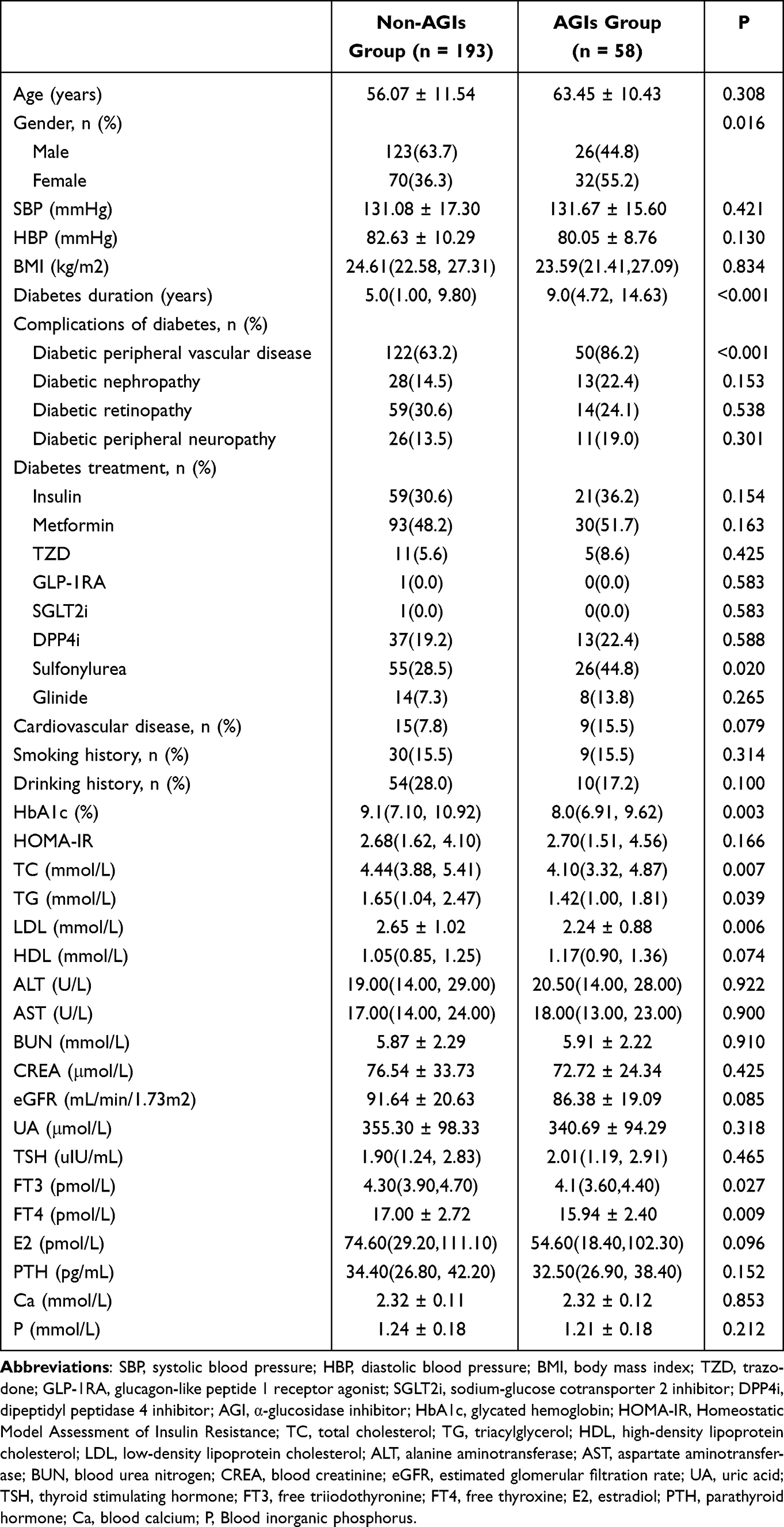 |
Table 2 Comparison of Basic Data Between Non-AGIs and AGIs Groups |
Comparison of the Risk of Osteoporosis and Fracture Between the AGIs Group and the Non-AGIs Group
The comparison of BMD, FRAX score and prevalence of osteoporosis between AGIs group and Non-AGIs group were presented in Table 3. The results showed that the BMD of both femoral neck and lumbar spine were significantly lower and the FRAX score was notably higher in the AGIs group than those in the Non-AGIs group (P < 0.05), indicating a higher risk of severe osteoporotic fracture and hip fracture within 10 years. Meanwhile, the proportion of patients with osteoporosis was obviously higher in the AGIs group than in the Non-AGIs group (P < 0.05). Additionally, statistical analysis of bone turnover markers revealed that the β-CTX and P1NP levels in the AGIs group were significantly lower than those in the Non-AGIs group (P < 0.01), while no significant difference was observed in 25OHD and OC levels between the two groups (Figure 1), suggesting that the bone transformation rate in AGIs group was lower.
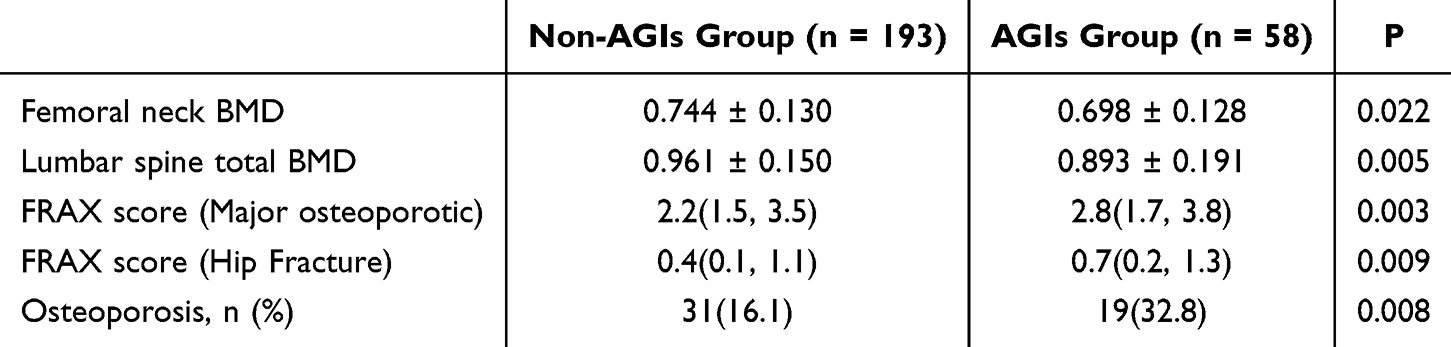 |
Table 3 The Comparison of BMD, FRAX Score and Prevalence of Osteoporosis Between AGIs Group and Non-AGIs Group |
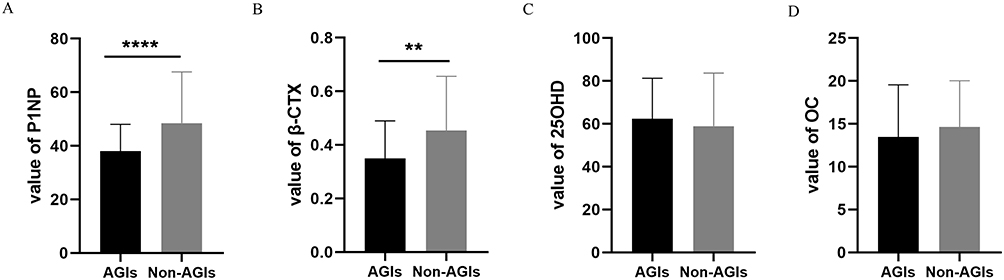 |
Figure 1 Bone turnover markers between AGIs group and Non-AGIs group. Notes: (A) type I procollagen amino-terminal peptide (P1NP); (B) carboxy-terminal β-crosslinking telopeptide of type 1 collagen (β-CTX); (C) osteocalcin (OC); (D) 25-hydroxy vitamin D3 (25OHD). **P < 0.01, ****P < 0.0001. |
Correlation Between AGIs Application and BMD Level in T2DM Patients
In order to further explore the correlation between AGIs application and BMD in T2DM patients, a multiple linear regression analysis was conducted with BMD value as the dependent variable. Table 4 indicated a distinguish negative correlation between AGIs application and lumbar spine total BMD after adjusting for potential confounding variables (β = −0.053, 95% CI −0.100~-0.006, P = 0.029). However, there was no significant correlation between AGIs application and femoral neck BMD.
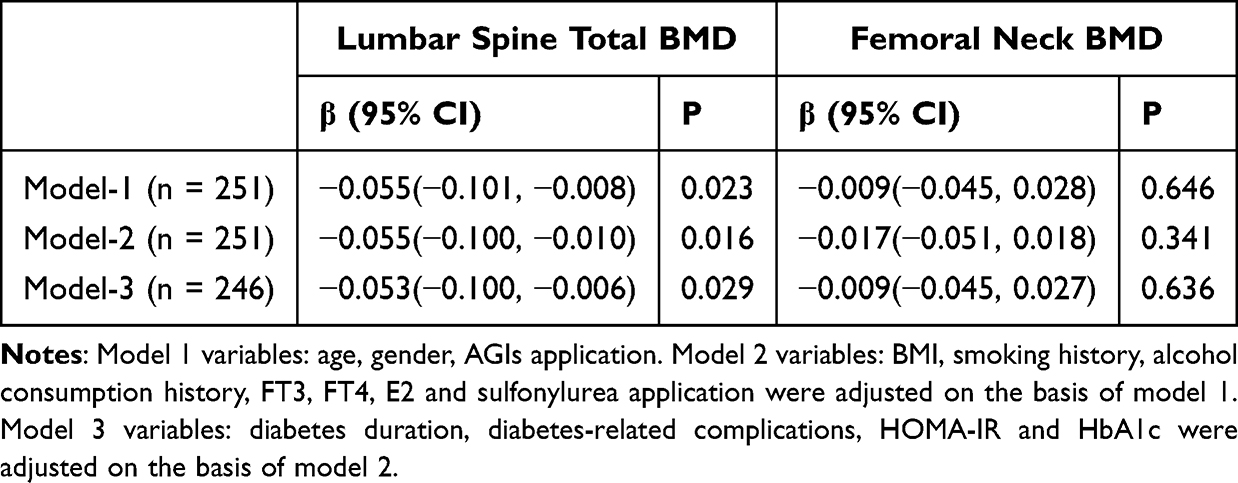 |
Table 4 Multiple Linear Regression Analysis Evaluated the Association Between AGIs Application and BMD in T2DM Patients |
Discussion
With the increasingly serious aging of China’s population, the prevalence of osteoporosis, as an age-related disease, is also ascending. It is worth noting that T2DM patients are more prone to fractures than non-T2DM patients, even at the same BMD levels.2,3,22,23 Therefore, in the whole process of diabetes management, it is necessary to carefully evaluate the potential factors that promote the decline of bone mass in T2DM patients, especially those that can be avoided or changed, such as medication choice. This study used DXA to measure BMD levels in patients and the FRAX score to assess bone strength and the risk of fractures within 10 years. The findings revealed that BMD levels in T2DM patients were negatively correlated with the application of AGIs. Compared with the patients without AGIs use, patients with AGIs use had lower BMD values, higher incidence of osteoporosis, and higher FRAX scores, accompanied by the reduction of both bone turnover markers P1NP and β-CTX levels. Furthermore, AGIs application was identified as an independent risk factor for a decrease in lumbar BMD.
AGIs delay the digestion of starch and sucrose in the intestines by reversibly and competitively inhibiting pancreatic α-amylase and membrane-bound intestinal α-glucosidase, flattening the postprandial blood glucose excursions,24 with high safety and no drug interaction. Current research on oral AGIs and bone health is limited. In 2021, a meta-analysis compared the fracture risks associated with various hypoglycemic drugs and found that voglibose reduced the risk of fractures in diabetic patients and was significantly beneficial than insulin, sodium-glucose cotransporter 2 inhibitors (SGLT2i), dipeptidyl peptidase 4 inhibitors (DPP4i), and some glucagon-like peptide 1 receptor agonists (GLP-1RAs) in terms of fracture.25 In the same year, a double-blind, randomized clinical trial indicated that attenuating postprandial glycemic indices, with an AGI, markedly decreased postprandial bone resorption and could be explained by the rise in serum GLP-1,26 suggesting that AGI may have bone-protective effects. However, a nationwide observational study in Japanese elderly with diabetes found AGI was related to increased hip fracture risk compared with metformin.27 Additionally, a small sample clinical control study in 2023 demonstrated that treatment with acarbose reduced postprandial suppression of bone resorption in patients with T2DM.28 Overall, the current evidence is inconclusive and conflicting regarding the effects of AGIs on bone metabolism and risk of fractures.
Based on the statistical results of 251 T2DM patients included in this study, we found that the use of AGIs was negatively correlated with the level of lumbar spine BMD and may increase the risk of osteoporosis and fracture. This result may be partially due to the longer duration of diabetes and more diabetic peripheral vascular lesions in the patients in AGIs-group, since previous studies had shown that T2DM complications were associated with a higher risk of fracture.29 In a Danish case-control study, diabetic retinopathy (OR 2.1), kidney disease (OR 2.0), neuropathy (OR 1.9), and macrovascular complications (OR 1.9) were all associated with an increased risk of fracture30. Fracture events were also more common when T2DM persisted over 10 years.30 In addition, the levels of HbA1c, FT3 and FT4 in AGIs group were significantly lower than those in Non-AGIs group, hinting that the reduction of BMD was not caused by worse blood glucose control,31 hyperthyroidism,32 and other adverse factors for bone. Although the proportion of female in AGIs group was higher than that in the Non-AGIs group, there was no significant difference between the two groups in age and E2 level. It should be noted that in terms of the types of hypoglycemic drugs, only one of the 251 patients used GLP-1RA because it was not widespread at that time. The use of sulfonylureas was higher in the AGIs group than in the Non-AGIs group, but the impact of sulfonylureas on bone mass remains unclarified. Previous studies showed a reduced incidence of fractures in patients treated with sulfonylureas,33,34 while paradoxically, other studies suggested that sulfonylureas may increase the risk of falls and fractures by increasing hypoglycemia.8,35
To further clarify the bone conversion after AGIs use, we analyzed the levels of bone turnover markers and found that the levels of P1NP and β-CTX were significantly declined in the AGIs group, suggesting a lower bone transformation rate.
Existing researches have shown that in T2DM patients, AGIs regulate postprandial glucose and bone resorption by stimulating GLP-1 secretion and inhibiting DPP-4 to improve circulating GLP-1 levels,36–38 and acarbose was found to have a positive effect on the intestinal microbiota.39 Therefore, it is speculated that the alteration of intestinal microbiota and intestinal insulin may be related to the mechanism by which AGIs affect bone metabolism, but the above conclusions have not been fully verified and recognized.
More interestingly, we found that AGIs application was an independent risk factor for lumbar spine BMD reduction in T2DM patients, but there was no significant correlation with femoral neck BMD. It was speculated that this may be related to the different metabolic and bone composition characteristics of different skeletal sites. The lumbar spine is cancellous bone, which may be more prone to bone loss.
So far, there is insufficient research on the impacts of commonly used hypoglycemic drugs AGIs on bone metabolism. Our study provides more evidence for the effects of AGIs on bone mass in T2DM. We found that in clinically severe diabetic patients, the use of AGIs was associated with a decrease in BMD and potentially an increased the risk of osteoporosis and fractures, which may suggest caution in the use of AGIs among patients with T2DM patients and poor BMD. However, as a cross-sectional study, this study has several limitations: 1. The sample size is small; 2. As a single-center study, there is a selection bias; 3. There is a lack of data on the duration and dosage of AGIs used by patients, which limits further analysis, thus reducing its value. The effects and mechanisms of AGIs on bone metabolism require further large-sample and scientifically designed studies for validation.
Conclusion
This study indicates that the use of AGIs in patients with T2DM is significantly associated with an increased risk of reduced BMD, osteoporosis, and fracture.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author or the first author upon reasonable request.
Ethical Approval
This research was approved by the Ethics Committee of Xiamen Hospital, Zhongshan Hospital Affiliated to Fudan University on February 29, 2024 (No. B2024-014). All patients in this study provided informed written consent for inclusion. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Helsinki Declaration and its later amendments or comparable ethical standards.
Acknowledgments
We are grateful to all the patients for their participation.
Author Contributions
Xiumei Luo: data curation, formal analysis, funding acquisition, investigation, resources, writing – original draft, writing – review and editing. Shangjian Li: data curation, formal analysis, investigation, validation, methodology, writing – original draft. Ning Chen: conceptualization, methodology, project administration, supervision, validation, writing – review and editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the natural science foundation of Xiamen, China (No.3502Z202374021).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ceriello A, Colagiuri S. IDF global clinical practice recommendations for managing type 2 diabetes - 2025. Diabet Res Clin Pract. 2025;222 Suppl 1:112152. doi:10.1016/j.diabres.2025.112152
2. Wang J, You W, Jing Z, Wang R, Fu Z, Wang Y. Increased risk of vertebral fracture in patients with diabetes: a meta-analysis of cohort studies. Int Orthopaedics. 2016;40(6):1299–1307. doi:10.1007/s00264-016-3146-y
3. Moayeri A, Mohamadpour M, Mousavi S, Shirzadpour E, Mohamadpour S, Amraei M. Fracture risk in patients with type 2 diabetes mellitus and possible risk factors: a systematic review and meta-analysis. Ther Clin Risk Manage. 2017;13:455–468. doi:10.2147/TCRM.S131945
4. Ballato E, Deepika F, Prado M, et al. Circulating osteogenic progenitors and osteoclast precursors are associated with long-term glycemic control, sex steroids, and visceral adipose tissue in men with type 2 diabetes mellitus. Front Endocrinol. 2022;13:936159. doi:10.3389/fendo.2022.936159
5. Hofbauer L, Busse B, Eastell R, et al. Bone fragility in diabetes: novel concepts and clinical implications. Lancet Diabetes Endocrinol. 2022;10(3):207–220. doi:10.1016/S2213-8587(21)00347-8
6. Cortet B, Lucas S, Legroux-Gerot I, Penel G, Chauveau C, Paccou J. Bone disorders associated with diabetes mellitus and its treatments. Joint Bone Spine. 2019;86(3):315–320. doi:10.1016/j.jbspin.2018.08.002
7. Zhao J, Li Y, Zhang H, et al. Preventative effects of metformin on glucocorticoid-induced osteoporosis in rats. J Bone Min Metabo. 2019;37(5):805–814. doi:10.1007/s00774-019-00989-y
8. Raj J, Venkatachalam S, Shekoba M, Norris J, Amaravati R. Conventional antidiabetic agents and bone health: a pilot case-control study. Perspectives Clin Res. 2019;10(4):177–182. doi:10.4103/picr.PICR_125_18
9. Josse R, Majumdar S, Zheng Y, et al. Sitagliptin and risk of fractures in type 2 diabetes: results from the TECOS trial. Diabetes Obesity Metab. 2017;19(1):78–86. doi:10.1111/dom.12786
10. Cai T, Li H, Jiang L, et al. Effects of GLP-1 receptor agonists on bone mineral density in patients with type 2 diabetes mellitus: a 52-week clinical study. Biomed Res Int. 2021;2021(1):3361309. doi:10.1155/2021/3361309
11. Akyay O, Canturk Z, Selek A, et al. The effects of exenatide and insulin glargine treatments on bone turnover markers and bone mineral density in postmenopausal patients with type 2 diabetes mellitus. Medicine. 2023;102(39):e35394. doi:10.1097/MD.0000000000035394
12. Grey A, Bolland M, Gamble G, et al. The peroxisome proliferator-activated receptor-gamma agonist rosiglitazone decreases bone formation and bone mineral density in healthy postmenopausal women: a randomized, controlled trial. J Clin Endocrinol Metab. 2007;92(4):1305–1310. doi:10.1210/jc.2006-2646
13. Zinman B, Haffner SM, Herman WH, et al. Effect of rosiglitazone, metformin, and glyburide on bone biomarkers in patients with type 2 diabetes. J Clin Endocrinol Metab. 2010;95(1):134–142. doi:10.1210/jc.2009-0572
14. Billington EO, Grey A, Bolland MJ. The effect of thiazolidinediones on bone mineral density and bone turnover: systematic review and meta-analysis. Diabetologia. 2015;58(10):2238–2246. doi:10.1007/s00125-015-3660-2
15. Kahn SE, Zinman B, Lachin JM, et al. Rosiglitazone-associated fractures in type 2 diabetes: an analysis from A diabetes outcome progression trial (ADOPT). Diabetes Care. 2008;31(5):845–851. doi:10.2337/dc07-2270
16. Thrailkill KM, Clay Bunn R, Nyman JS, et al. SGLT2 inhibitor therapy improves blood glucose but does not prevent diabetic bone disease in diabetic DBA/2J male mice. Bone. 2016;82:101–107. doi:10.1016/j.bone.2015.07.025
17. Yang W, Liu J, Shan Z, et al. Acarbose compared with metformin as initial therapy in patients with newly diagnosed type 2 diabetes: an open-label, non-inferiority randomised trial. Lancet Diabetes Endocrinol. 2014;2(1):46–55. doi:10.1016/S2213-8587(13)70021-4
18. Zhou JQWK, Zheng SL. Correlation between serum ferritin levels and pancreatic β-cell function in patients with type 2 diabetes. Diab New World. 2021;24(17):1–4.
19. Li S, Luo X, Lu Z, Chen N. Association of midnight cortisol level with bone mineral density in chinese patients with type 2 diabetes mellitus: a cross-sectional study. Diabetes Metab Syndr Obes. 2024;17:2943–2953. doi:10.2147/DMSO.S470391
20. Chinese Society of Osteoporosis and Bone Mineral Research. Guidelines for the diagnosis and treatment of primary osteoporosis (2022). Chin Gen Pract. 2023;26(14):1671–1691.
21. Jiang X, Gruner M, Trémollieres F, et al. Diagnostic accuracy of FRAX in predicting the 10-year risk of osteoporotic fractures using the USA treatment thresholds: a systematic review and meta-analysis. Bone. 2017;99:20–25. doi:10.1016/j.bone.2017.02.008
22. Costantini S, Conte C. Bone health in diabetes and prediabetes. World J Diab. 2019;10(8):421–445. doi:10.4239/wjd.v10.i8.421
23. Liu X, Chen F, Liu L, Zhang Q. Prevalence of osteoporosis in patients with diabetes mellitus: a systematic review and meta-analysis of observational studies. BMC Endocr Disord. 2023;23(1):1. doi:10.1186/s12902-022-01260-8
24. Bischoff H. Pharmacology of alpha-glucosidase inhibition. Eur J Clin Invest. 1994;24:3–10.
25. Zhang Y, Yuan Y, Zheng Y, Chen S, Xie B. Effects of anti-diabetic drugs on fracture risk: a systematic review and network meta-analysis. Front Endocrinol. 2021;12:735824. doi:10.3389/fendo.2021.735824
26. Kreitman A, Schneider S, Hao L, Schlussel Y, Bello N, Shapses S. Reduced postprandial bone resorption and greater rise in GLP-1 in overweight and obese individuals after an α-glucosidase inhibitor: a double-blinded randomized crossover trial. Osteoporosis Int. 2021;32(7):1379–1386. doi:10.1007/s00198-020-05791-5
27. Tamaki J, Ogawa S, Fujimori K, et al. Hip and vertebral fracture risk after initiating antidiabetic drugs in Japanese elderly: a nationwide study. J Bone Min Metabo. 2023;41(1):29–40. doi:10.1007/s00774-022-01372-0
28. Dalsgaard N, Gasbjerg L, Helsted M, et al. Acarbose diminishes postprandial suppression of bone resorption in patients with type 2 diabetes. Bone. 2023;170:116687. doi:10.1016/j.bone.2023.116687
29. Eller-Vainicher C, Cairoli E, Grassi G, et al. Pathophysiology and management of type 2 diabetes mellitus bone fragility. J Diab Res;2020. 7608964. doi:10.1155/2020/7608964
30. Vestergaard P, Rejnmark L, Mosekilde L. Diabetes and its complications and their relationship with risk of fractures in type 1 and 2 diabetes. Calcified Tissue Int. 2009;84(1):45–55. doi:10.1007/s00223-008-9195-5
31. Compston J. Type 2 diabetes mellitus and bone. J Internal Med. 2018;283(2):140–153. doi:10.1111/joim.12725
32. Delitala A, Scuteri A, Doria C. Thyroid hormone diseases and osteoporosis. J Clin Med. 2020;9(4):1034. doi:10.3390/jcm9041034
33. Melton L, Leibson C, Achenbach S, Therneau T, Khosla S. Fracture risk in type 2 diabetes: update of a population-based study. J Bone Min Res. 2008;23(8):1334–1342. doi:10.1359/jbmr.080323
34. Kanazawa I, Yamaguchi T, Yamamoto M, Sugimoto T. Relationship between treatments with insulin and oral hypoglycemic agents versus the presence of vertebral fractures in type 2 diabetes mellitus. J Bone Min Metabo. 2010;28(5):554–560. doi:10.1007/s00774-010-0160-9
35. Zhang Z, Cao Y, Tao Y, et al. Sulfonylurea and fracture risk in patients with type 2 diabetes mellitus: a meta-analysis. Diab Res Clin Pract. 2020;159:107990. doi:10.1016/j.diabres.2019.107990
36. Moritoh Y, Takeuchi K, Hazama M. Chronic administration of voglibose, an alpha-glucosidase inhibitor, increases active glucagon-like peptide-1 levels by increasing its secretion and decreasing dipeptidyl peptidase-4 activity in ob/ob mice. J Pharmacol Exp Therapeut. 2009;329(2):669–676. doi:10.1124/jpet.108.148056
37. Ueno H, Tsuchimochi W, Wang H, et al. Effects of miglitol, acarbose, and sitagliptin on plasma insulin and gut peptides in type 2 diabetes mellitus: a crossover study. Diabetes Ther. 2015;6(2):187–196. doi:10.1007/s13300-015-0113-3
38. Lee A, Patrick P, Wishart J, Horowitz M, Morley J. The effects of miglitol on glucagon-like peptide-1 secretion and appetite sensations in obese type 2 diabetics. Diabetes Obesity Metab. 2002;4(5):329–335. doi:10.1046/j.1463-1326.2002.00219.x
39. Wang Z, Hu J, Wang J, Chen Y, Dong B, Wang Y. A comparative study of acarbose, vildagliptin and saxagliptin intended for better efficacy and safety on type 2 diabetes mellitus treatment. Life Sci. 2021;274:119069. doi:10.1016/j.lfs.2021.119069
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Hemoglobin Levels and Osteoporosis in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Ye T, Lu L, Guo L, Liang M
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2803-2811
Published Date: 14 September 2022
Prevalence and Risk Factors of Osteoporosis in Patients with Type 2 Diabetes Mellitus in Nanchang (China): A Retrospective Cohort Study
Li T, Hu L, Yin XL, Zou Y, Fu HY, Li HL
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3039-3048
Published Date: 28 September 2022
Liraglutide in Combination with Insulin Has a Superior Therapeutic Effect to Either Alone on Fracture Healing in Diabetic Rats
Liu H, Tian F, Hu Y, Ping S, Zhang L
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1235-1245
Published Date: 29 April 2023
Development of Machine Learning Models for Predicting Osteoporosis in Patients with Type 2 Diabetes Mellitus—A Preliminary Study
Wu X, Zhai F, Chang A, Wei J, Guo Y, Zhang J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1987-2003
Published Date: 30 June 2023
Triglyceride Glucose Index is Strongly Associated with a Fragility Fracture in Postmenopausal Elderly Females with Type 2 Diabetes Mellitus Combined with Osteoporosis: A 6-Year Follow-Up Study
Pan J, Huang X, Wang Q, Sun J, Zhai Z, Mo J, Huang J, Lu W
Clinical Interventions in Aging 2023, 18:1841-1849
Published Date: 9 November 2023