Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Regular Inhaled Corticosteroids Use May Protect Against Severe COVID-19 Outcome in COPD
Authors Labor M ![]() , Kirui BK
, Kirui BK ![]() , Nyberg F
, Nyberg F ![]() , Vanfleteren LEGW
, Vanfleteren LEGW ![]()
Received 14 February 2023
Accepted for publication 14 June 2023
Published 7 August 2023 Volume 2023:18 Pages 1701—1712
DOI https://doi.org/10.2147/COPD.S404913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Marina Labor,1 Brian K Kirui,2 Fredrik Nyberg,2 Lowie EGW Vanfleteren3,4
1Cancer and Lung Health Care Unit, University Hospital in Linköping, Linköping, Sweden; 2School of Public Health and Community Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 3COPD Center, Department of Respiratory Medicine and Allergology, Sahlgrenska University Hospital, Gothenburg, Sweden; 4Department of Internal Medicine and Clinical Nutrition, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Correspondence: Marina Labor, Cancer and Lung Health Care Unit, University Hospital in Linköping, Linköping, Sweden, Tel +46739238935, Email [email protected]
Purpose: Population-based studies provide conflicting evidence about how inhaled corticosteroids (ICS) impact COVID-19 outcomes among COPD patients. We investigated whether regular ICS exposure affects risk, severity, or survival in SARS-CoV-2 infection, using a nationwide linked Swedish population register database.
Patients and Methods: During January–December 2020, we studied two defined Swedish adult populations – Whole population [≥ 40 years] (N = 5243479), and COPD subpopulation [≥ 40 years] (N = 133372), in three study cohorts, respectively: 1. Overall cohort (index date 1 Jan 2020), 2. COVID-19 diagnosed sub-cohort (index date = diagnosis date), and 3. COVID-19 hospitalized sub-cohort (index date = admission date). Regular exposure was defined as ≥ 3 ICS prescriptions in the year before index. Hazard ratios (HRs) for outcomes (COVID-19 onset, hospitalization, ICU admission, or death) related to ICS exposure were estimated using Cox regression. Confounding was controlled by propensity score methods applying Average Treatment effect in the Treated (ATT) weighting.
Results: Regular ICS use was associated with only very slightly increased onset of COVID-19, hospitalization, ICU admission, and death in the overall whole population cohort and in the overall COPD subpopulation cohort, except for ICU admission (marginally non-significant HRs, up to 1.13); and no clear increase in the diagnosed sub-cohorts. However, in the COVID-19 hospitalized COPD sub-cohort, ICS therapy showed reduced risks against progression to ICU admission and death, significant for death (HR 0.82 95% CI [0.67– 0.99]).
Conclusion: For COPD patients, ICS therapy offers some protection against progression to ICU admission and death among COVID-19 hospitalized patients. Our findings alleviate concerns about increased risks of COVID-19 by ICS treatment and provide evidence supporting the continuation of ICS therapy for COPD patients.
Keywords: COVID − 19, COPD, mortality
Introduction
Patients with chronic obstructive pulmonary disease (COPD) are of particular interest in relation to coronavirus disease 2019 (COVID-19) because COPD is a highly prevalent disease that is associated with impaired lung function. Overall, COPD patients seem not to have an increased risk of acquiring severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.1 In contrast, it has been shown that COPD patients with COVID-19 have more than fivefold increased risk of a severe disease course requiring intensive care unit (ICU) support, and higher mortality in comparison to other patient groups,2 which is at least partly explained by higher age and comorbidity prevalence.3–6
Inhaled corticosteroids (ICS) are commonly used in patients with COPD to prevent exacerbations and/or control symptoms. Early in the COVID-19 pandemic, concerns were raised related to potential impaired antiviral response associated with ICS use, due to suppression of interferon-mediated innate and adaptive immunity.7 Consequently, ICS users would have higher risk for severe illness if they acquired COVID-19. To date, published (mostly laboratory) studies and reviews rather suggest a potential preventive effect of pre-morbid and continued use of ICS against a hyperinflammatory response.8–10 A recent study, in contrast, reported that pre-morbid ICS use in COPD was not protective and even increased risk of developing COVID-19.11 A systematic review of more recent studies about pre-morbid and continued use of ICS found no evidence that ICS use was associated with worse outcomes, even though results and conclusions are likely confounded by different factors (ICS indication, sample size, lack of adjustment for comorbidities).6 Current recommendations are that standard maintenance and exacerbation ICS therapy should not be discontinued, because maintenance of optimal pharmacologic treatment generally is the best way to prevent exacerbations and/or reduce the severity of exacerbations, including those caused by viruses.12 In people who do not have COPD, ICS prescription initiated in mild COVID-19 appears to reduce the risk of admission to hospital or death and reduce the duration of symptoms.13 Besides, both ICS and oral corticosteroids (OCS) have been shown to be effective in the treatment of severe SARS-CoV-2 infection with respiratory failure in the advanced phase by reducing the hyperinflammatory response of the host and beneficially affecting the severity of acute lung injury.14,15 Due to the conflicting results summarized above, our primary objectives were to investigate, using a large Swedish population linked register database, whether ongoing regular ICS exposure may affect risk of onset, or severity (hospitalization, ICU admission or death) outcomes of SARS-CoV-2 infection in the whole population [≥40 years], as well as to investigate the effect of ICS use on these risks specifically in COPD patients, a vulnerable patient group with frequent use of ICS, within this same population database.
Materials and Methods
Study Design, Data Sources and Study Population
We conducted a cohort study in a Swedish nationwide population of individuals aged 40 years and above and free of COVID-19 on 1 Jan 2020 (N = 5243 479). Data come from the SCIFI-PEARL (Swedish COVID-19 Investigation for Future Insights – a Population Epidemiology Approach using Register Linkage) project, described in detail elsewhere.16 This project database, now extended to the entire Swedish population, includes all individuals who developed COVID-19 in the Swedish population, identified using a range of register data.
For the current study, we defined two study populations of Swedish adults ≥40 years: 1) whole population, and 2) COPD subpopulation, and within these populations studied three different study cohorts (with corresponding index dates): an overall cohort (index date 1 Jan 2020), a COVID-19 diagnosed sub-cohort (individuals with COVID-19 infection onset with infection date as their index date), and hospitalized sub-cohort (COVID-19 patients with admission date as their index date). The overall cohort and sub-cohorts of COPD patients included individuals with COPD on 1 Jan 2020, identified based on International Classification of Diseases, revision 10 (ICD-10) diagnostic codes J41–J44 related to specialist care visits or hospital admissions in the National Patient Register (NPR) or being registered as COPD patients in the Swedish National Airway Register (SNAR), from 1 Jan 2015 until 31 Dec 2019.
Beyond the two data sources already mentioned, used for defining the study population, baseline comorbidities and some COVID-19 outcomes, other data sources within SCIFI-PEARL used in this study were: 1. SmiNet (the national database of notifiable diseases) for diagnosis based on reporting positive PCR result by doctors and/or laboratories; 2. The Swedish Intensive Care Register (SIR) for admissions to ICU; 3. The Cause-of-Death Register (CDR) for COVID-19 death; 4. The National Prescribed Drug Register (NPDR) for treatments with prescription medications; and 5. National sociodemographic registers, ie, the Register of Total Population (RTB), and Longitudinal Integrated Database for Health Insurance and Labor Market Studies (LISA) from Statistics Sweden with data on immigration, emigration, deaths and sociodemographic characteristics. The linked data thus comprehensively contained detailed information for each subject regarding COVID-19, demographics, comorbidities, prescribed medications, and clinical data for COPD patients. The study has ethical approval from the Swedish Ethical Review Authority and complies with the Declaration of Helsinki. Informed consent was not required, since the study is based on secondary healthcare data.
Exposure, Outcomes, and Follow-Up
The main study exposure was regular ongoing ICS exposure, defined as the presence of at least three filled ICS prescriptions (with Anatomical Therapeutic Chemical (ATC) codes R03BA, R03AK, R03AL08, and R03AL09) within the year before index date in the NPDR. Non-exposed individuals received less than 3 prescriptions of ICS in the same period. This definition was chosen to capture a patient’s consistent and continuous use of the medication over this time and likely continued use after the index date into the study follow-up period. Swedish prescriptions normally cover approximately 3 months of use, so mostly this would mean continuous use; our data also confirmed that with this definition >85% of individuals in the whole population and COPD population in our study who were exposed to ICS had their last prescriptions filled within 100 days and are likely to be regular users.
We defined COVID-19 outcomes as: COVID-19 onset (individuals with positive test result for SARS-CoV-2 in SmiNet, or an out- or inpatient primary or secondary diagnosis with ICD-10 U07.1 or U07.2 in the NPR; event date was the earliest of these), hospitalization (primary or secondary diagnosis U07.1 or U07.2 from inpatient care in the NPR; event date was the date of admission), intensive care unit (ICU) admission (U07.1 or U07.2 from SIR; event date being date of admission) and death (underlying or contributing cause of death U07.1 or U07.2 in the CDR).
In all analyses, follow-up started on the respective cohort index date, and extended to the earliest of outcome, emigration, death, or end of follow-up on 31 Dec 2020.
Covariates
We included the following covariates: sociodemographic factors from national sociodemographic registers were age (≥40 years), gender, employment status (unemployed 40–64 years, employed 40–64, employed 65+ and retired), education (primary, secondary, or higher). Comorbidities were defined based on ICD-10 codes registered during 2015–2019 in the NPR, including hypertension, cardiovascular disease, heart failure, stroke, ischemic heart disease (IHD), diabetes, respiratory disease, COPD, asthma, respiratory failure, lung cancer, rheumatologic and immunologic disease, chronic kidney disease and kidney failure. Drug exposures were based on ATC codes in NPDR in 2019, and included oral corticosteroids, biologics, short- and long-acting bronchodilator agonists, short- and long-acting muscarinic antagonists, leukotriene receptor antagonists, immunosuppressants, and statins. Patient factors that were obtained from SNAR registrations during 2015–2019 included body mass index, smoking, and post-bronchodilator Forced Expiratory Volume in one second, percent of predicted (FEV1% predicted) based on the Swedish Hedenström reference values.17 Missing data were common for patient factors as they were not recorded on every visit and were addressed by 1) using the last observations carried forward 2) missing post-bronchodilator FEV1 values replaced with pre-bronchodilator FEV1 values 3) supplementing smoking and BMI data from similar information in other registers as described in Table S1. In addition, our analytic strategy included gradient boosting modeling which handles missing as a separate category in the propensity score estimation, thereby balancing the proportions of missing between the exposure groups.18
Statistical Analysis
The study populations were characterized using absolute and relative frequencies for categorical variables, and averages and standard deviations for continuous variables. The number and incidence rates of events were computed.
Hazard ratios (HRs) and 95% confidence intervals (CI) for studied outcomes related to ICS exposure were estimated using Cox regression models. Propensity score analysis using Average Treatment effect in the Treated (ATT) weighting was applied in the Cox regression models to control the effect of confounding when comparing exposed and corresponding non-exposed groups. Propensity scores were estimated using a gradient boosted logistic regression model (twang package in R), including all potential confounders in the model, and optimizing the number of trees to give the best possible balance as measured by the lowest average standardized mean differences (SMD) across the potential confounders.18 The balance between the exposed and non-exposed groups was evaluated prior to and after propensity score weighting using the SMD and considered satisfactory when the SMD was <0.25, or preferably <0.1.19 If satisfactory balance overall could not be achieved, a “doubly robust” model was estimated, including imbalanced covariates (SMD >0.1) also in the outcome model.20 R (version 4.0.2) for statistical computing was used for all analyses.
Results
In the overall (population-based, pre-COVID-19) cohorts, 3% (186,577/5,243,479) of the whole population and 35.7% (47,559/133,372) of COPD patients were regularly exposed to ICS (Table 1). The mean age of the ICS-exposed tended to be higher than for the non-exposed in the overall cohorts and COVID-19 diagnosed sub-cohorts, especially for the whole population (Table 1, Table S2, respectively), but this difference was less obvious in the COVID-19 hospitalized sub-cohorts (Table S3). ICS-exposed in all cohorts were more often women. The ICS-exposed tended to have more comorbidities and higher medication use than the non-exposed in the whole population cohorts and sub-cohorts, but this was not consistently seen in the COPD cohorts (Table 1, Tables S2 and S3). The low SMDs after propensity score weighting for most covariates indicated that a very good balance was achieved between the exposed and non-exposed after weighting for most cohorts, but less satisfactory for the whole population overall cohort (Table 1, Tables S2 and S3). For this cohort, the doubly robust analysis was thus implemented.
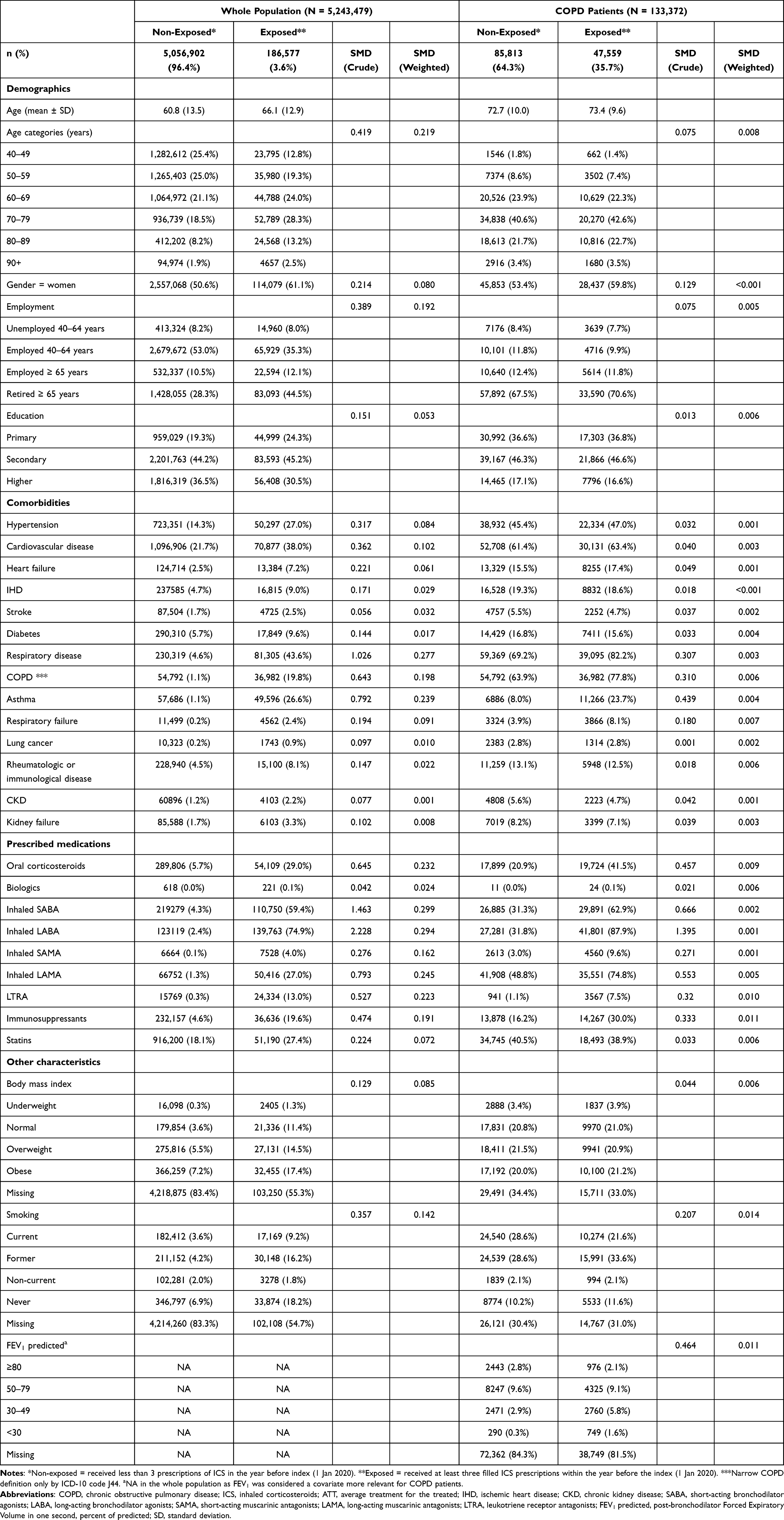 |
Table 1 Demographic Characteristics, Comorbidities, and Prescribed Medications of the Overall Cohorts of the Whole Population and COPD Patients on 1 Jan 2020, for Individuals ≥40 Years of Age Exposed and Non-Exposed to Prior Regular Treatment with Inhaled Corticosteroids (ICS), with Standardized Mean Differences (SMD) to Assess Differences for All Characteristics Between the Cohorts Before (Crude) and After ATT Weighting by Propensity Scores (Weighted) |
ICS-Exposure Related Risk for COVID-19 Outcomes in the Overall Cohort
The incidence rates of COVID-19 events were generally higher in the ICS-exposed compared to the non-exposed groups (Table S4). The ATT-weighting adjusted models showed weak and non-significant associations between previous ICS exposure and increased risk of COVID-19 onset, hospitalization, ICU admission and mortality in the whole population, and in COPD patients substantial associations similarly were not indicated for the studied outcomes, with a weak significant estimate only for hospitalization (Table 2).
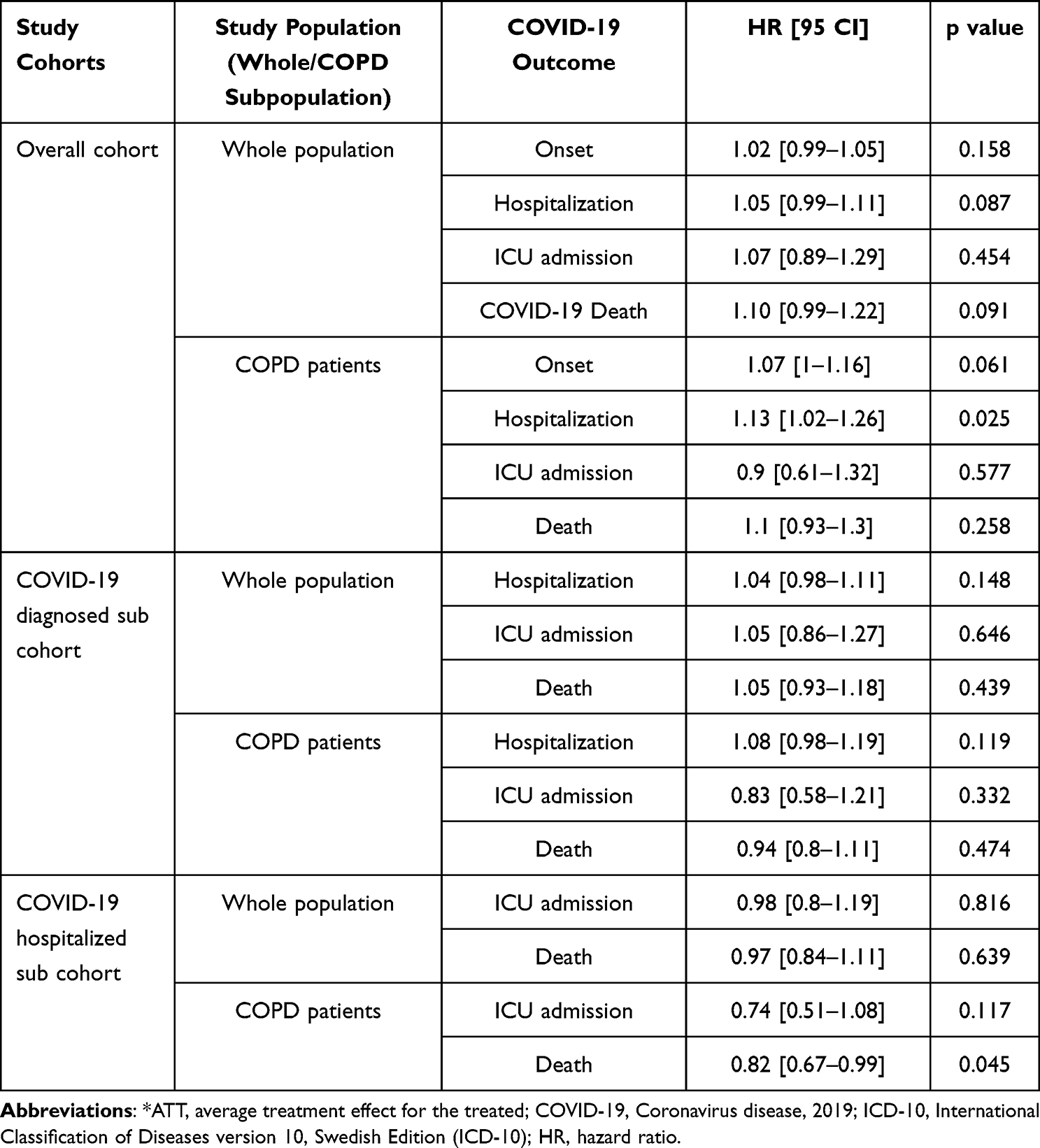 |
Table 2 Hazard Ratios with 95 Confidence Intervals Comparing the Risk of Various COVID-19 Outcomes Between Individuals ≥40 Years of Age with Prior Regular Exposure to ICS to Non-Exposed Individuals, Adjusted for Multiple Confounders by Propensity Score Weighting ATT* Weighting |
ICS-Exposure Related Risk for COVID-19 Hospitalization or Death in Those with Diagnosed COVID-19 (COVID-19 Diagnosed Sub-Cohorts)
No significant associations between previous ICS exposure and hospitalization, admission or mortality were observed in the ATT-weighting adjusted models in COVID-19 patients from the whole population or from the COPD population in the COVID-19 diagnosed sub-cohort (Table 2).
ICS- Exposure Related Risk for COVID-19 ICU Admission or Death in Hospitalized COVID-19 Patients (COVID-19 Hospitalized Sub-Cohorts)
In the whole population hospitalized sub-cohort, no significant association was observed in the ATT adjusted models between ICS therapy and ICU mortality or death (Table 2). The point estimates were both close to 1 and non-significant. In contrast, the COVID-19 hospitalized sub-cohort among COPD patients showed reduced risk for ICU admission and mortality in patients receiving previous ICS therapy with significant protection for mortality (HR 0.82 95% CI [0.67–0.99]) (Table 2). A trend of shifting risk towards protection with more severe COVID-19 in COPD patients can thus be observed (Figure 1).
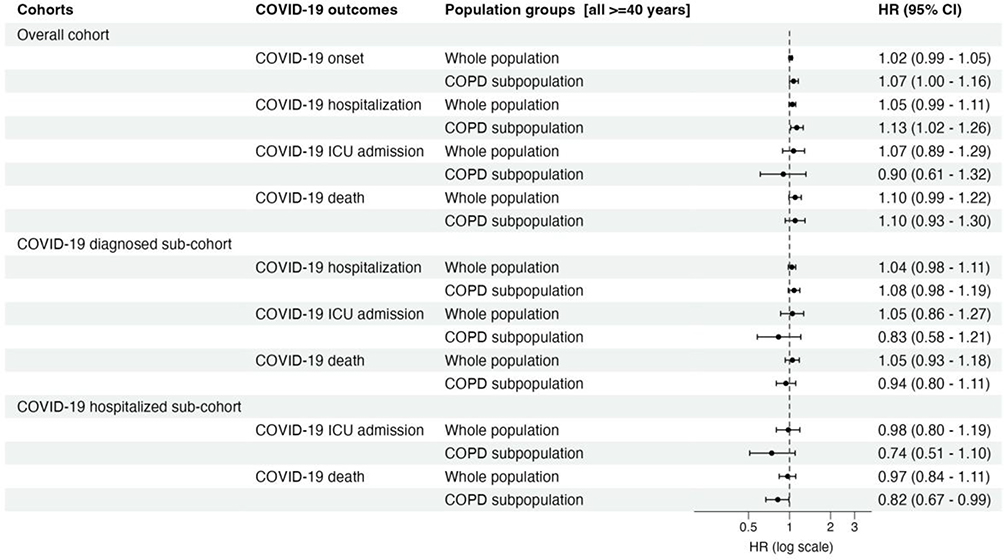 |
Figure 1 Forest plot comparing the risk of various definitions of COVID-19 between persons with pre-index exposure to ICS to non-exposed persons. The figure summarizes Average treatment for the treated (ATT) adjusted hazard ratios with 95% CI. Abbreviations: HR, hazard ratio; CI, confidence interval; ICU, intensive care unit; COPD, chronic obstructive pulmonary disease; COVID-19, Coronavirus disease. |
Discussion
This study shows only weak non-significant associations between regular ICS exposure and COVID-19 onset, hospitalization, ICU admission and mortality in the overall cohort from the whole population and similarly in the overall COPD patient cohort, but not in the COPD patient population overall cohort or sub-cohorts in which regular ICS use appears even to be protective against severe COVID-19 disease, in particular against mortality in COPD patients hospitalized for COVID-19.
Ongoing ICS treatment may confer some risk of developing both mild and severe COVID-19, especially in a mixed whole population. In vitro studies have suggested that corticosteroids may impair antiviral innate immune response21,22 and that ICS use leads to delayed virus clearance.23 This could be a possible explanation to a slightly more frequent mild (onset) and more severe outcomes in the overall cohorts that we observed also in this study, although these effects were weak and non-significant. The observed associations could also partly be explained by underlying health differences between the exposed, who tended to have more comorbidities and higher medication use, and the non-exposed, despite extensive covariate balancing of the two groups by use of propensity score methods. Overall, however, we observed little evidence of COVID-19 risk from ICS use for COPD patients, especially in the diagnosed and hospitalized COPD sub-cohorts who might have a higher need of such treatment, and thus a better risk-benefit profile in terms of preventing or alleviating COVID-19-related exacerbations by consistent ICS use.
Indeed, ICS treatment might have benefit on cardiovascular related mortality in COPD as recently shown in large trials comparing triple inhaled combination therapy (including bronchodilators and ICS) with dual inhaled therapy (including bronchodilators only).24,25 This is relevant in the context of COPD, ICS and COVID-19, as cardiovascular disease is the most common comorbidity in patients with COPD and a risk factor for worse COVID-19 outcome. Other evidence has also suggested that ICS treatment in active COVID-19 disease or in susceptible populations may hinder progression to severe disease in the whole population. For example, Song et al reported that 14-day ciclesonide inhalation initiated after COVID-19 onset shortened SARS-CoV-2 viral shedding duration, and possibly inhibited the progression to acute respiratory failure in patients with mild-to-moderate COVID-19.26 Similarly, the STOIC trial found that administering inhaled budesonide to adult COVID-19 outpatients reduced the need for emergency visits and speeded up recovery, being an effective treatment of early COVID-19 and even affecting the rate of the persistent long-term symptoms in COVID-19.27 A study by Baker et al based on STOIC showed that enhanced immune response is activated already in early COVID-19 in the upper airway, and can be measured up to 35 days after the initial infection. According to the authors, it is possible to predict which patients will clinically deteriorate, by noting a blunted interferon and an exaggerated CCL24 airway inflammatory response. However, the inflammatory pathways and patterns of inflammation in the upper respiratory tract and circulation following COVID-19 infection were modulated by inhaled budesonide.28 Clemency et al showed that participants who were treated with ciclesonide had fewer subsequent emergency department visits or hospital admissions for reasons related to COVID-19 (odds ratio, 0.18; 95% CI, 0.04–0.85).29 One of the explanations might be that ICS modulate the inflammatory response. Taking ICS may be beneficial in dealing with virus infections, specifically coronavirus. As mentioned, ciclesonide blocks SARS-CoV-2 RNA replication in vitro9 and inhibits SARS-CoV-2 cytopathic activity,30 reducing thus the risk of developing severe COVID-19. Previously, both the PRINCIPAL and COVERAGE trials suggested that it was difficult to show that early administration of inhaled corticosteroid reduce the risk of clinical worsening in high-risk COVID-19 positive populations which includes COPD patients.31,32 In fact, our results show that among COPD patients hospitalized for COVID-19 there was even a clear protective effect. This may be related to the consistent ICS intake during the COVID-19 pandemic, since the prior treatment is most often continued and likely provide protection during this time frame. Part of this protective effect may also be explained by the fact that ICS therapy downregulates the SARS-CoV-2 receptors ACE2 and ADAM17,33 for which inhibition seems to be related to COVID-19 susceptibility and severity.34 Therefore, the ICS-mediated downregulation of ACE2 is thought to be protective, and COPD patients should definitely continue ICS both in general (prior to COVID-19) and after having developed COVID-19.
Regarding severe clinical outcomes or mortality, inconsistent results have been reported. Sen et al showed that prior ICS therapy did not increase COVID-19 related healthcare utilization or mortality outcome in patients with COPD.35 Bloom et al similarly showed neither benefit nor harm from ICS in patients with both COPD and asthma who were hospitalized with COVID-19 when it comes to inpatient clinical outcomes.36 Schultze et al, on the other hand, reported increased risk of mortality among patients with COPD on ICS although sensitivity analyses suggested this was from unmeasured confounding due to reduced baseline health status in patients on ICS.11 Aveyard et al studied COPD patients hospitalized with COVID-19 where prior ICS therapy was associated with a modest risk of severe COVID-19. The estimated risk was reduced but not normalized when adjusted for comorbidities and demographic factors.37 Important factors related to ICS use in relation to COVID-19 are the timing of ICS use, as well as the underlying indication for usage, which may explain the heterogenous results. Regular prior use (for an underlying condition) has been shown to have a different effect than administration at or after time of infection.38 Our results are consistent with this view, and suggest that conditional on contracting COVID-19, a prior treatment with ICS is protective – possibly related to continued administration during the COVID-19 infection.
This study has several strengths, including a large sample size, high data completeness for most covariates except for some patient factors with some missing data, and the capability of assessing whether prior use of ICS was associated with outcomes in a nationwide cohort reflecting both the whole population and COPD patients with COVID-19. Another important strength of our study is the use of nationwide register data, which minimized the possibility of selection bias. However, this study also has limitations. Inherent to its retrospective observational design, causal interpretation of the findings is still subject to residual bias from potential residual or unmeasured confounding. For example, patients with lung diseases or ICS treatment may have other comorbidities or characteristics that are not captured in the data that may bias the risk estimates. Nevertheless, by our propensity score analysis, we adjusted for a wide range of comorbidities and markers of disease severity and treatment and achieved quite good balance between compared groups in all analyses, so that major residual confounding is unlikely. We also lacked some important data on COPD severity for all COPD individuals that would have been desirable for our analyses, eg, Global Initiative for Chronic Obstructive Lung Disease (GOLD) grouping, but available FEV1 data were a good surrogate despite some missingness. Another limitation is the considerable amount of missing data on key variables like smoking, BMI and FEV1. Although we used analytical methods to deal with missing values, it might impact on the validity of the results. Similarly, although register data captures data on prescription drugs very well, some ICS are also available over the counter and may not have been captured in our data.
Conclusion
In summary, this large population study suggests that the benefits of ongoing ICS therapy in COPD patients outweighs the potential associated risks. There is no evidence to support discontinuation of ICS among patients with COPD for COVID-19-related reasons. On the contrary, our results provide support for the continuation of ICS treatment for COPD patients, considering the protective effect in reducing severe disease, including mortality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The SCIFI-PEARL study has basic funding based on grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (grants ALFGBG-938453, ALFGBG-971130, ALFGBG-978954,) and previously from FORMAS (Research Council for Environment, Agricultural Sciences and Spatial Planning), a Swedish Research Council for Sustainable Development (grant 2020-02828). This research was also based on support from the Swedish Heart-Lung Foundation (20210030, 20210581).
Disclosure
ML has received personal fees from AstraZeneca, Chiesi, GSK, Novartis, Boehringer-Ingelheim and Sanofi. LV has received grants and personal fees from AstraZeneca and personal fees from GSK, Novartis, Boehringer-Ingelheim, Menarini, Resmed, Chiesi, AGA Linde, Zambon and Pulmonx. FN was an employee of AstraZeneca until 2019 and holds some AstraZeneca shares. The authors report no other conflicts of interest in this work.
References
1. De Vito A, Fiore V, Princic E, et al. Predictors of infection, symptoms development, and mortality in people with SARS-CoV-2 living in retirement nursing homes. PLoS One. 2021;16(3):e0248009. doi:10.1371/journal.pone.0248009
2. Lippi G, Henry BM. Chronic obstructive pulmonary disease is associated with severe coronavirus disease 2019 (COVID-19). Respir Med. 2020;167:105941. doi:10.1016/j.rmed.2020.105941
3. Guan WJ, Liang WH, Zhao Y, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J. 2020;55(5):2000547. doi:10.1183/13993003.00547-2020
4. Zhao Q, Meng M, Kumar R, et al. The impact of COPD and smoking history on the severity of COVID-19: a systemic review and meta-analysis. J Med Virol. 2020;92:1915–1921. doi:10.1002/jmv.25889
5. Calmes D, Graff S, Maes N, et al. Asthma and COPD are not risk factors for ICU stay and death in case of SARS-CoV2 Infection. J Allergy Clin Immunol Pract. 2021;9:160–169 doi:10.1016/j.jaip.2020.09.044
6. Halpin DMG, Rabe A, Loke WJ, et al. Epidemiology, healthcare resource utilization, and mortality of Asthma and COPD in COVID-19: a systematic literature review and meta-analyses. J Asth Aller. 2022;15:811–825. doi:10.2147/JAA.S360985
7. Finney LJ, Glanville N, Farne H, et al. Inhaled corticosteroids downregulate the SARS-CoV-2 receptor ACE2 in COPD through suppression of type I interferon. J All Clin Immun. 2021;147(2):510–519 doi:10.1016/j.jaci.2020.09.034
8. Halpin DMG, Singh D, Hadfield RM. Inhaled corticosteroids and COVID-19: a systematic review and clinical perspective. Eur Respir J. 2020;55(5):2001009. doi:10.1183/13993003.01009-2020
9. Furci F, Caminati M, Senna G, et al. The potential protective role of corticosteroid therapy in patients with asthma and COPD against COVID-19. Clin Mol Allergy. 2021;19:19. doi:10.1186/s12948-021-00159-4
10. Matsuyama S, Kawase M, Nao N, et al. The inhaled corticosteroid ciclesonide blocks coronavirus RNA replication by targeting viral NSP15. J Virol. 2021;95(1):e01648–20 doi:10.1128/JVI.01648-20
11. Schultze A, Walker AJ, MacKenna B, et al. Risk of COVID-19-related death among patients with chronic obstructive pulmonary disease or asthma prescribed inhaled corticosteroids: an observational cohort study using the OpenSAFELY platform. Lancet Respir Med. 2020;8(11):1106–1120. doi:10.1016/S2213-2600(20)30415-X
12. Global initiative for chronic obstructive lung disease global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease global initiative for chronic obstructive lung disease (2023 report); 2022. Available from: http://www.goldcopd.org/.
13. Griesel M, Wagner C, Mikolajewska A, et al. Inhaled corticosteroids for the treatment of COVID-19. The Cochrane database of systematic reviews; 2022:CD015125.
14. Romagnoli S, Peris A, De Gaudio AR, et al. SARS-CoV-2 and COVID-19: from the Bench to the Bedside. Physiol Rev. 2020;100(4):1455–1466. doi:10.1152/physrev.00020.2020
15. Janssen MT, Ramiro S, Mostard RL, et al. Three-month and six-month outcomes of patients with COVID-19 associated hyperinflammation treated with short-term immunosuppressive therapy: follow-up of the CHIC study. RMD Open. 2021;7(3):e001906. doi:10.1136/rmdopen-2021-001906
16. Nyberg F, Franzén S, Lindh M, et al. Swedish Covid-19 investigation for future insights – a population epidemiology approach using register linkage (SCIFI-PEARL). CLEP. 2021;13:649–659. doi:10.2147/CLEP.S312742
17. Zhu Y, Coffman DL, Ghosh D. A boosting algorithm for estimating generalized propensity scores with continuous treatments. J Cau Inf. 2015;3(1):25–40. doi:10.1515/jci-2014-0022
18. Ridgeway G, McCaffrey D, Morral A, et al. Toolkit for weighting and analysis of nonequivalent groups: a guide to the twang package. Vignette. 2021;2021:26.
19. Stuart EA, Lee BK, Leacy FP. Prognostic score-based balance measures can be a useful diagnostic for propensity score methods in comparative effectiveness research. J Clin Epidemiol. 2013;66(8 Suppl):S84–S90.e1. doi:10.1016/j.jclinepi.2013.01.013
20. Funk ML, Westreich D, Wiesen C, et al. Doubly robust estimation of causal effects. Am J Epidemiol. 2011;173(7):761–767. doi:10.1093/aje/kwq439
21. Davies JM, Carroll ML, Li H, et al. Budesonide and formoterol reduce early innate anti-viral immune responses in vitro. PLoS One. 2011;6:e27898. doi:10.1371/journal.pone.0027898
22. Simpson JL, Carroll M, Yang IA, et al. Reduced antiviral interferon production in poorly controlled asthma is associated with neutrophilic inflammation and high-dose inhaled corticosteroids. Chest. 2016;149:704–713. doi:10.1016/j.chest.2015.12.018
23. Singanayagam A, Glanville N, Girkin JL, et al. Corticosteroid suppression of antiviral immunity increases bacterial loads and mucus production in COPD exacerbations. Nat Commun. 2018;9:2229. doi:10.1038/s41467-018-04574-1
24. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS Trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease. A randomized, double-blind, multicenter, parallel-group study. Am J Respir Crit Care Med. 2021;203(5):553–564. doi:10.1164/rccm.202006-2618OC
25. Stone IS, Barnes NC, James WY, et al. Lung deflation and cardiovascular structure and function in chronic obstructive pulmonary disease: a randomized controlled trial. Am. J Respir Crit Care Med. 2016;193:717–726. doi:10.1164/rccm.201508-1647OC
26. Song J-Y, Yoon J-G, Seo Y-B, et al. Ciclesonide inhaler treatment for mild-to-moderate COVID-19: a randomized, open-label, phase 2 trial. J Clin Med. 2021;10(16):3545. doi:10.3390/jcm10163545
27. Ramakrishnan S, Nicolau DV, Langford B, et al. Inhaled budesonide in the treatment of early COVID-19 illness: a randomised controlled trial. Lancet Respir Med. 2021;9(7):763–772. doi:10.1016/S2213-2600(21)00160-0
28. Baker JR, Mahdi M, Nicolau DV, et al. Early Th2 inflammation in the upper respiratory mucosa as a predictor of severe COVID-19 and modulation by early treatment with inhaled corticosteroids: a mechanistic analysis. Lancet Respir Med. 2022;10(6):545–556. doi:10.1016/S2213-2600(22)00002-9
29. Clemency BM, Varughese R, Gonzalez-Rojas Y, et al. Efficacy of inhaled ciclesonide for outpatient treatment of adolescents and adults with symptomatic COVID-19: a randomized clinical trial. JAMA Intern Med. 2022;182(1):42–49. doi:10.1001/jamainternmed.2021.6759
30. Halpin DMG, Faner R, Sibila O et al. Do chronic respiratory diseases or their treatment affect the risk of SARS-CoV-2 infection? Lancet Respir Med. 2020;8:436–443. doi:10.1016/S2213-2600(20)30167-3
31. Yu LM, Bafadhel M, Dorward J, et al.; PRINCIPLE Trial Collaborative Group. Inhaled budesonide for COVID-19 in people at high risk of complications in the community in the UK (PRINCIPLE): a randomised, controlled, open-label, adaptive platform trial. Lancet. 398;2021:843–855. doi:10.1016/S0140-6736(21)01744-X
32. Duvignaud A, Lhomme E, Onaisi R, et al.; Coverage Study Group. Inhaled ciclesonide for outpatient treatment of COVID-19 in adults at risk of adverse outcomes: a randomised controlled trial (COVERAGE). Clin Microbiol Infect. 2022;28(7):1010–1016. doi:10.1016/j.cmi.2022.02.031
33. Milne S, Li X, Yang CX, et al. Inhaled corticosteroids downregulate SARS-CoV-2- related genes in COPD: results from a randomised controlled trial. Eur Respir J. 2021;58:2100130. doi:10.1183/13993003.00130-2021
34. Tay MZ, Poh CM, Rénia L, et al. The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol. 2020;20:363–374. doi:10.1038/s41577-020-0311-8
35. Sen P, Majumdar U, Zein J, et al. Inhaled corticosteroids do not adversely impact outcomes in COVID-19 positive patients with COPD: an analysis of Cleveland Clinic’s COVID-19 registry. PLoS One. 2021;16(6):e0252576. doi:10.1371/journal.pone.0252576
36. Bloom CI, Drake TM, Docherty AB, et al. ISARIC investigators. Risk of adverse outcomes in patients with underlying respiratory conditions admitted to hospital with COVID-19: a national, multicentre prospective cohort study using the ISARIC WHO Clinical Characterisation Protocol UK. Lancet Respir Med. 2021;9(7):699–711. doi:10.1016/S2213-2600(21)00013-8
37. Aveyard P, Gao M, Lindson N, et al. Association between pre-existing respiratory disease and its treatment, and severe COVID-19: a population cohort study. Lancet Respir Med. 2021;9:909–923 doi:10.1016/S2213-2600(21)00095-3
38. Singh D, Halpin DMG. Inhaled corticosteroids and COVID-19-related mortality: confounding or clarifying? Lancet Respir Med. 2020;8:1065–1066. doi:10.1016/S2213-2600(20)30447-1
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
Recommended articles
Six-Minute Walking Test and 30 Seconds Chair-Stand-Test as Predictors of Mortality in COPD – A Cohort Study
Höglund J, Boström C, Sundh J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2461-2469
Published Date: 4 October 2022
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
Prognostic Properties of the GOLD 2023 Classification System
Brat K, Svoboda M, Zatloukal J, Plutinsky M, Volakova E, Popelkova P, Novotna B, Dvorak T, Koblizek V
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:661-667
Published Date: 20 April 2023
RETRO-POPE: A Retrospective, Multicenter, Real-World Study of All-Cause Mortality in COPD
Koblizek V, Milenkovic B, Svoboda M, Kocianova J, Holub S, Zindr V, Ilic M, Jankovic J, Cupurdija V, Jarkovsky J, Popov B, Valipour A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2661-2672
Published Date: 17 November 2023
Respiratory Infection Triggering Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Abi Abdallah G, Diop S, Jamme M, Legriel S, Ferré A
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:555-565
Published Date: 27 February 2024