Back to Journals » Patient Preference and Adherence » Volume 20
Regional Determinants of Non-Adherence: A Quantitative Survey of Healthcare Professionals’ Perceptions in Latin America, Asia Pacific, Middle East, Africa, Pakistan and China
Authors Tokgözoğlu L, Akbar M, Bryce A, Chen Z, Arnaout MS, Da Silva van der Laan A, Tan NC ![]()
Received 19 December 2025
Accepted for publication 23 April 2026
Published 15 July 2026 Volume 2026:20 590211
DOI https://doi.org/10.2147/PPA.S590211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Lale Tokgözoğlu,1 Mousa Akbar,2 Alfonso Bryce,3 Zhenyue Chen,4 Mohamad Samir Arnaout,5 Andressa Da Silva van der Laan,6 Ngiap Chuan Tan7,8
1Department of Cardiology, Hacettepe University, Ankara, Turkiye; 2Head of Cardiology Unit, Al SABAH Hospital, Shuwaikh Industrial, Kuwait City, Kuwait; 3Department of Research CARDIOGOLF, Clínica El Golf, Lima, Peru; 4Department of Cardiovascular Medicine, Shanghai Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China; 5Department of Internal Medicine, Division of Cardiology, American University of Beirut Medical Center, Beirut, Lebanon; 6Abbott Product Operations AG, Basel, Switzerland; 7Digital Healthcare, SingHealth Polyclinics, Bukit Merah, Singapore; 8Duke-NUS Medical School, SGH Campus, Outram, Singapore
Correspondence: Lale Tokgözoğlu, Department of Cardiology, Hacettepe University Cinnah caddesi 24/11 Çankaya, Ankara, Turkiye, Email [email protected]
Introduction: Non-adherence is a major burden in chronic diseases. In dyslipidemia, cholesterol levels are causing approximately 2.6 million deaths each year worldwide, while up to 90% of dyslipidemic patients exhibit poor medication adherence to combination therapies, making it the leading cause of insufficient therapeutic response in dyslipidemia management. The Regional Determinants of Non-Adherence project investigates healthcare professionals’ (HCPs) perceptions, comprehension, and attitudes towards patient adherence in managing dyslipidemia, emphasizing geographical differences and their influence on patient beliefs and behaviors.
Methods: This study was an online self-administered questionnaire targeting HCPs managing patients with dyslipidemia. Participants (cardiologists, endocrinologists, internal medicine specialists, family medicine practitioners, general practitioners, nurses) were selected based on their specialties and experience. The survey was conducted across four regions: Asia Pacific (APAC), Latin America (LATAM), Middle East Africa Pakistan (METAP), and China.
Results: Among 151 respondents, significant regional differences in perceptions of non-adherence to dyslipidemia treatment were observed. Globally, 42.6% of HCPs reported a 30% increase in mortality due to non-adherence. METAP respondents reported the highest awareness of adverse outcomes, while LATAM respondents highlighted socioeconomic barriers as primary challenges. METAP participants emphasized the importance of tailored patient education. Differences were also observed in the perceived efficacy of communication strategies, with respondents from METAP emphasizing the importance of tailored patient education. Additionally, disparities in local health authority support were found to influence HCPs’ ability to manage non-adherence effectively.
Discussion: Medication adherence is a global health concern with significant regional variations in HCPs’ perceptions of factors influencing adherence to treatments, highlighting the need to consider regional and cultural contexts in future adherence strategies.
Keywords: medication adherence, dyslipidemia, health care professionals, cardiovascular diseases, global health, patient education
Introduction
Non-adherence to prescribed medications remains a significant challenge in contemporary healthcare, with profound implications for patient health outcomes and healthcare systems globally. The consequences of poor adherence are far-reaching, encompassing adverse health outcomes such as cardiovascular events, target organ damage, and exacerbations of chronic diseases, which collectively contribute to increased healthcare costs and a notable reduction in patients’ quality of life.1 Despite the critical importance of adherence, measuring it accurately remains challenging due to the absence of universal parameters,2 with some studies indicating that the average adherence rate hovers around 50%.3–5
Particularly concerning is the relationship between non-adherence to statin therapy and increased mortality risk. Research has demonstrated that poor adherence to vascular medications is a significant contributor to cardiovascular diseases (CVD) events, with approximately 9% of all such events in Europe attributable to non-adherence alone.4 Furthermore, non-adherence is associated with poor clinical outcomes, higher mortality rates, and is responsible for over 30% of medicine-related hospitalizations.2 Dyslipidemia is a major risk factor for CVD, contributing substantially to global morbidity and mortality. Elevated cholesterol levels are estimated to cause approximately 2.6 million deaths each year worldwide. Multiple pharmacological options are available to control serum lipid levels, and most patients require combination therapy to achieve target lipid goals. Notably, up to 90% of individuals with dyslipidemia exhibit poor medication adherence, making poor adherence the leading cause of insufficient therapeutic response in dyslipidemia management.6
The reasons for non-adherence are multifaceted, encompassing patient-related factors (such as age, gender, beliefs, and symptoms), treatment-related factors (including complexity, tolerability, and frequency of treatment), disease-related factors (comorbidities, type, and severity of the condition), socio-economic factors (including access to care and drug reimbursement), and healthcare professional/system-related factors (like spent with patients and healthcare infrastructure). These factors, as identified by the World Health Organization (WHO), highlight the complexity of medication adherence and underscore the need for a nuanced understanding of this issue.1,2,7–10 Demographic characteristics also play a role in medication adherence. Age, for example, influences adherence rates, with different demographics exhibiting varying levels of adherence based on the average age of the population,10 or the fact that adherence rates are generally lower in developing countries compared to developed ones.9 Socio-economic factors also contribute to regional variations, as observed in studies conducted in South Korea11 where adherence to lipid-lowering therapy varies markedly by region and income, with higher adherence rate in the capital or big cities compared to cities from rural regions and lower income. The same is observed in Latin America, where adherence is often hindered by lack of time, dietary habits, and limited knowledge about dyslipidemia, all of which are influenced by local cultural and socioeconomic factors.12 In Middle East, Turkey, Africa, and Pakistan (METAP), conflict, displacement, and fragmented healthcare systems create substantial barriers to medication access and continuity, further reducing adherence.13 Finally in China, additional risk factors for poor adherence to lipid-lowering therapy include being employed rather than unemployed, having lower levels of medicine insurance coverage, receiving care in lower-level or rural health facilities, being managed outside cardiology departments, having a lower perceived cardiovascular risk, and not being treated with statins.8
Despite these insights, comprehensive understanding of the role of demographics in patient non-adherence remains elusive. Existing evidence on non-adherence to dyslipidemia treatment in these regions is limited by several key issues, including a scarcity of adherence-focused trials, predominant use of retrospective designs, heterogeneity in adherence and dyslipidemia definitions and measurements, underrepresentation of sociocultural and health system factors, and a lack of healthcare professionals’ viewpoint. The Regional Determinants of Non-Adherence project aims to fill this gap by exploring the perceptions, comprehension, and attitudes of healthcare professionals (HCPs) towards patient adherence in the management of dyslipidemia. This project seeks to provide a deeper understanding of whether geographical differences influence patient beliefs and adherence behaviors, and to investigate the dynamics of the patient-physician relationship in this context. Through these efforts, we aim to inform targeted strategies to improve adherence and optimize patient outcomes across diverse populations.
Method
Study Design
This medical research was an online self-administered questionnaire focusing on the management of dyslipidemia in patients globally. The survey targeted healthcare professionals (HCPs) who manage patients with dyslipidemia and was conducted across 4 different regions: Asia Pacific (APAC), Latin America (LATAM), Middle East Africa Pakistan (METAP), and China. However, the goal was to contact at least 50 HCPs per region, to secure a minimum of 30 respondents per world region to ensure sufficient sample size for basic statistical analyses and meaningful regional comparisons. The cut-off of 30 participants per region was considered a pragmatic balance between the feasibility of recruitment and the statistical power and data interpretability. All responses were closed and declarative, reflecting the perceptions of the respondents. The questionnaire was distributed to HCPs involved in the care of patients with dyslipidemia, through emails and during professional meetings.
Objectives
This survey’s aim is to identify regional reasons and factors for adherence/non-adherence to treatment, from HCP point-of-view, in several countries, considering local cultures and beliefs. Results will be exploratory only.
The primary objectives of this survey were to: elucidate the determinants of medication adherence and non-adherence in patients with dyslipidemia from the perspectives of healthcare professionals (HCPs); assess their’ perceptions and knowledge regarding adherence and its clinical implications; evaluate geographical variations in the impact of patients’ beliefs on medication non-adherence; examine the dynamics of the patient-HCP relationship; and investigate influences from public health policies.
Questionnaire
The development and validation of the questionnaire used in this medical research involved collaboration between five cardiologists and two behavioral science expert. Leveraging a relevant literature review and their clinical expertise, these professionals ensured that the questionnaire effectively assessed local reasons and factors for adherence and non-adherence to treatment across several countries. A first meeting was scheduled to discuss the questionnaire structure with the 7 experts. Then, they made amendments and worked together through a collaborative document, until they reached agreement on final questions and formulations. A validation meeting was finally held to validate the final version of the questionnaire.
The questionnaire, composed of 19 questions, was divided into four sections, aimed to capture a comprehensive understanding of patient adherence. These sections included the perception of patient adherence, factors influencing adherence, healthcare professionals’ communication, and public policy support. The goal was to elucidate HCP ‘perceptions of adherence, explore geographical differences in the impact of patient beliefs on non-adherence, examine the relationship between patients and healthcare professionals, and identify potential public policy levers. The questionnaire is available in Supplementary 1.
To ensure clear comprehension of the questions, the questionnaire was made available in multiple languages: French, English, Spanish, Portuguese, and Chinese (Mandarin). Translations were reviewed and approved by native members of the project. Participating healthcare professionals were required to respond to the online survey after reading and accepting the privacy policy, which detailed the process related to the use and analysis of their personal information and responses. Each participant had to acknowledge the privacy policy disclosure and sign a consent form before accessing the questionnaire, which took approximately 20 minutes to complete. Privacy policies are available in Supplementary 2.
All responses from the participating healthcare professionals were collected, analyzed, and presented in aggregate form only, to maintain anonymity and encourage honest responses. The platform was aligned with the RGPD policies on the protection of data.
Participants
The medical specialties most likely to manage dyslipidemia patients were identified, and healthcare professionals (HCPs) from these fields were invited by a: care to participate in the survey. Selection criteria for the HCPs included their specialties, knowledge, and experience in managing dyslipidemia. The invited participants comprised cardiologists, endocrinologists, internal medicine specialists, family medicine practitioners, general practitioners, and nurses. This diverse group ensured a comprehensive understanding of dyslipidemia management across various medical disciplines. Exclusion criteria were the following: Non-HCPs, not managing patients with dyslipidemia, no sign consent.
Statistical Analysis
Standard descriptive statistics were used to express the results of the survey. For all items in the questionnaire, a descriptive statistical analysis was conducted using frequency and percentage analysis, with each item analyzed both globally and per region (APAC, China, LATAM, and METAP). Following the descriptive analysis, the four regions were compared using a Chi-squared test for each item. A significant Chi-squared test indicated a significant difference between the regional results. In such cases, pairwise comparisons between all regions were performed using a Chi-squared test with a Bonferroni-Holm adjustment to identify which specific regions were significantly different. For each statistical test, if the number of expected observations was less than five for any case, a Fisher exact test was also performed. All data analyses were conducted using SAS 9.4 software. A 5% threshold and 95% confidence interval was used for all statistical tests.
Results
The study includes 151 respondents spread out over 4 different regions, comprising 37 (24.5%), 30 (19.9%), 37 (24.5%), and 47 (31.1%) respondents from the APAC, China, LATAM and METAP regions respectively. Respondents were cardiologists, endocrinologists, internal medicine specialists, family medicine practitioners, general practitioners, and nurses. The results illustrates respondents’ perceptions, comprehension and attitude toward patient adherence in dyslipidemia management.
Global Results
42.0% of respondents believed that non-adherence to dyslipidemia treatment significantly contributes to increased mortality. Notably, regional differences in responses were minimal, though the METAP region exhibited the highest awareness at 53.3%, contrasting with APAC’s 29.7%. Regarding patient adherence, almost half of HCPs (48.3%) estimated that 50% of their patients adhered to dyslipidemia treatments, and a third (33.8%) estimated 75% adherence. Similar trends were observed for statin adherence, with 43,3% and 42% of respondents estimating 50% and 75% of adherence respectively. However, adherence estimations from their own active file were higher, with 48.3% and 53% of respondents respectively estimating 75% adherence for dyslipidemia treatments and for statins. Most HCPs (46.0%) identified that 25% of non-adherent patients were intentionally so. According to 73,3% of the respondents, 50 (39.3%) to 75% (34.0%) of non-intentionally non-adherent patients could benefit from apps/devices.
Factors Influencing Non-Adherence
Key factors influencing non-adherence included side effects (67.8%), health literacy (65.7%), perceived severity of cardiovascular disease (62.3%), susceptibility to cardiovascular events (57.5%), medication cost (54.4%), risk factors (52.2%) and treatment efficacy (50.4%). Conversely, lack of support, timing, mental health, and access to care were deemed less influential by a quarter of respondents. Cultural beliefs were deemed an influential factor by 50% of respondents however 26.7% of respondents considered this factor as having a lesser influence on non-adherence. Detailed results are presented in Table 1.
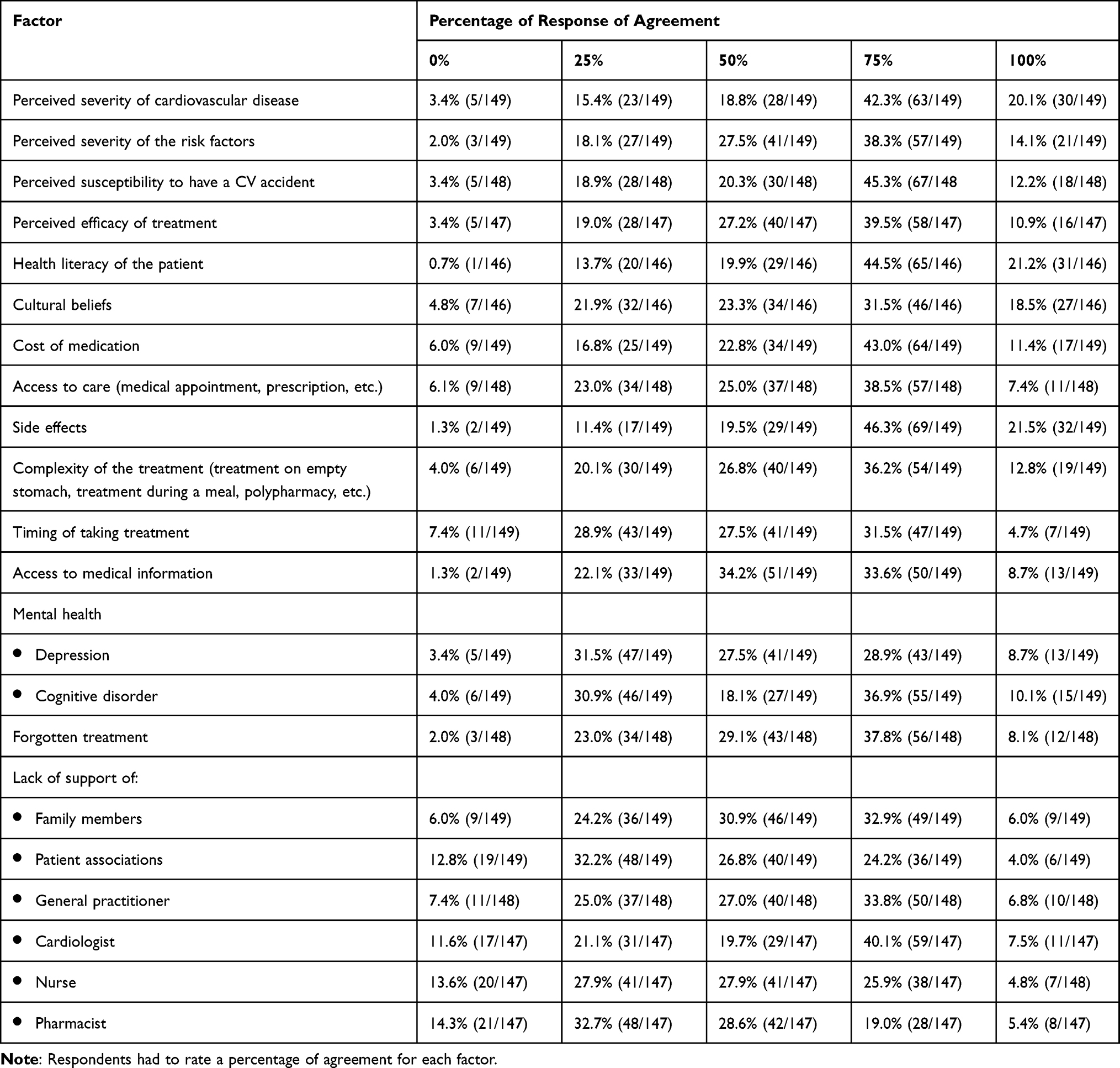 |
Table 1 Factors Influencing the Non-Adherence of the Patients |
Communication
In terms of healthcare provider communication, HCPs rated their personal practices higher than general practices, especially regarding patient personalized communication (82.6% vs 65.7%) and open-ended questions (72.2% vs 58.4%). Nevertheless, when asked about the assumption of adherence, 65.8% of respondents indicated that HCPs generally believe their patients are adherent to treatment, and 64.9% of respondents believe their own patients are adherent. For both general and personal practice, patient expertise on their disease was recognized by 37.6% of respondents, while over a third (34.8% and 38.3%) viewed patients as non-experts. Results are presented in Table 2.
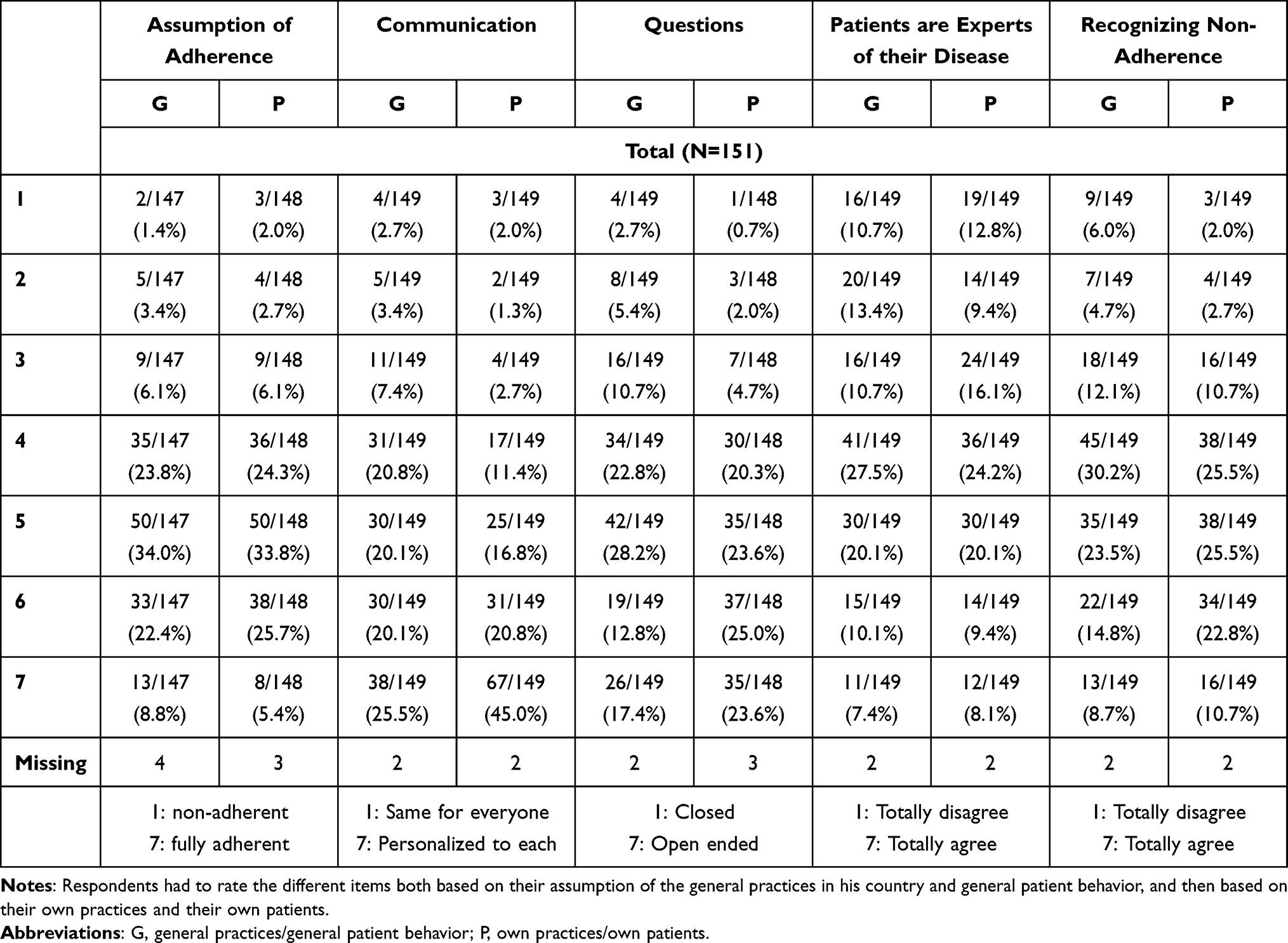 |
Table 2 Physicians’ Assumption Regarding Their Patients and Practices |
The healthcare professionals-patient relationship was considered crucial by 67.3% of respondents for impacting adherence. Communication issues tied to non-adherence were attributed to age, time constraints, socio-cultural levels, and patient transparency, each cited by over 50% of respondents.
Public Policies
To improve patient adherence, respondents indicated that public policies should focus on all the proposed support measures, with more than 70% giving high scores (5–7) for each proposition: access to disease information (77.6%), access to HCP appointments (77.3%), access to treatment information (77.0%), access to care (74.8%), and cost of medication (72.3%).
According to 42.6% of the respondents, non-adherence can lead to a 30% increase in mortality and a total of 71% considered the increase to be at least 20%. This opinion is shared by respondents from all regions with no significant difference between the different regions.
Finally, the responses highlighted similarities in the perception of statin adherence, intentionally and unintentionally non-adherent patients benefiting from technological aids, and the influence of disease severity, risk factors, treatment efficacy, health literacy, cultural beliefs, and side effects on adherence. Additionally, consistent assumptions and practices were observed in HCPs’ evaluation of patient adherence and communication.
Regional Determinants of Non-Adherence
The results presented below are focusing only on the questions presenting statistical differences between the regions. Two questions resulted in a significant difference in the global effect, but no significant difference was identified following the pairwise comparison. The first one is “What percentage of dyslipidemia patients do you estimate to be adherent to dyslipidemia treatment in general?” And the second one is the lack of support of pharmacist as a factor having influence on patient’s non-adherence.
Perception of Patient Adherence
The following factors: complexity of treatment, timing of treatment, depression, cognitive disorder, forgotten treatment, lack of support from family members, and general practitioners showed significant differences across two or more regions. They are presented in Table 3.
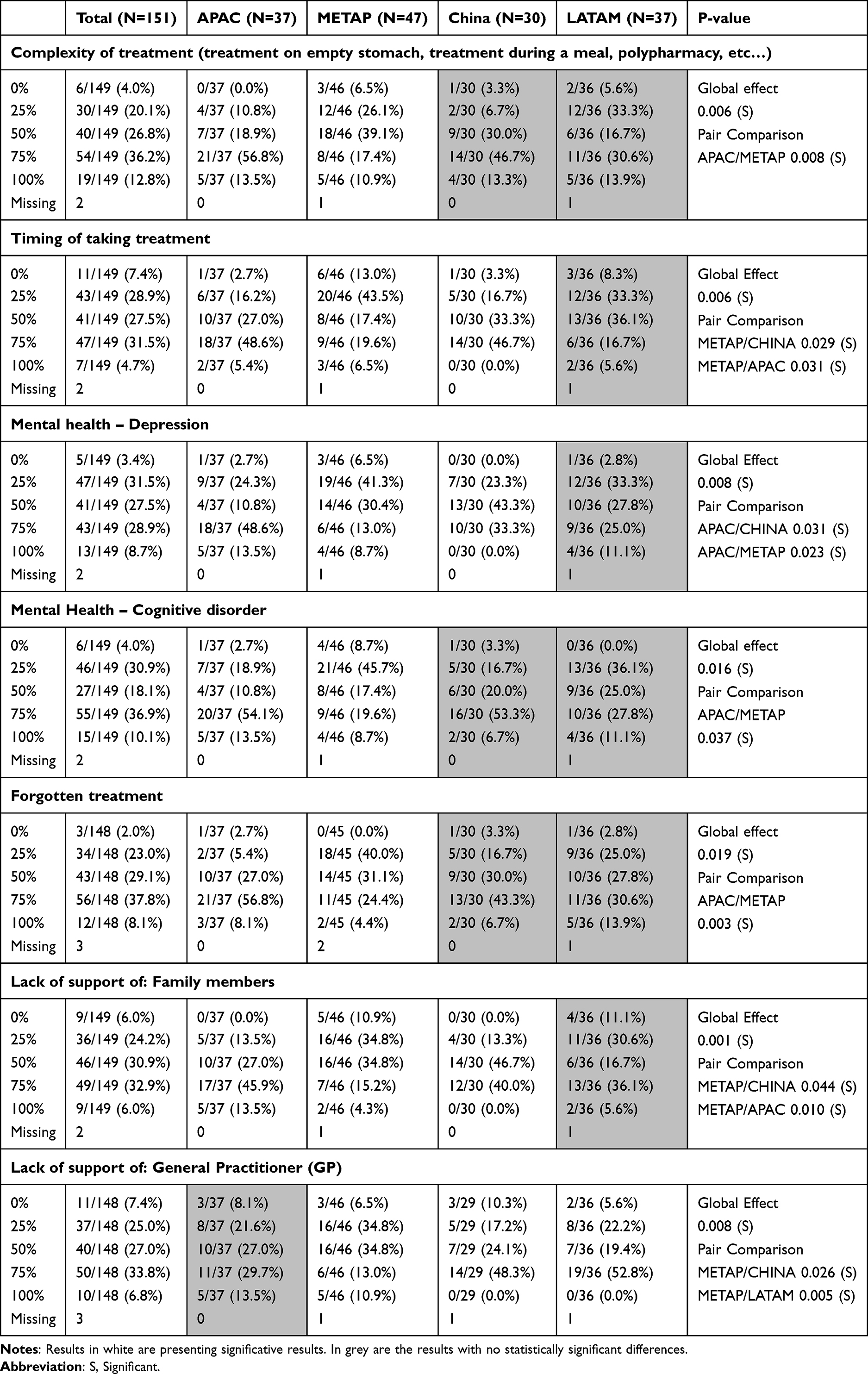 |
Table 3 Regional Differences in Factors Influencing Non-Adherence |
Regarding the complexity of treatment, there is a notable difference (p-value: 0.008) between APAC and METAP regions. 70.3% of APAC’s respondents estimate that the complexity of treatment has a high influence on non-adherence in comparison only 28.3% of METAP’s respondents answered 75% or above when ask about the importance of the factor. When it comes to the timing of taking treatment, METAP shows a significant difference compared to both APAC (p= 0.031) and China (p= 0.029). METAP respondents indicated that the timing of taking treatment is less influential on adherence than the perceptions held by APAC and China with respectively 26.1%, 54.0% and 46.7% respondents selecting 75% or 100% when voting.
In terms of mental health, both depression and cognitive disorders have a significant global effect on treatment adherence. The significant differences in depression are observed between APAC and the other two regions, METAP (p= 0.023) and China (p= 0.031). However, cognitive disorder differences are significant only between APAC and METAP (p= 0.037). APAC (62.1%) perceives that depression has a higher influence on adherence than what is perceived in China (33.3%) or METAP (21.7%). Similarly, for cognitive disorders, APAC (67.6%) estimates a higher influence on adherence to medication compared to METAP (28.3%).
For forgotten treatments, again a significant difference (p= 0.003) appears between METAP and APAC, reflecting the same pattern as before (28.8% vs 64.9%).
Regarding the lack of support from family members, METAP shows a significant difference when compared to both APAC (p= 0.010) and China (p= 0.044). While 45.7% of METAP’s respondents considers this factor to have less influence (25% or below), only 13.3% of China respondents and 13.5% of APAC respondents voted the same way.
Lastly, the lack of support from general practitioners (GPs) shows a significant difference with METAP compared to both LATAM (p= 0.005) and China (p= 0.026), following the same observation pattern.
For all the factors that revealed a significant global effect, METAP had a significant difference with at least one region and perceived the factor as less influencing compared to the perception of the other region. Results are presented in Table 3.
HCPs’ Communication
The question regarding HCPs’ communication with their patients shows significant global effect (p=0.022). APAC and METAP had a significant difference (p=0.004) with 59.4% of APAC’s respondents rating communication as highly personalized (scores 6 or 7), whereas in METAP, only 28.8% rated it similarly, with an average score between 3 and 5. When asked about their own communication practices, more than half of the participants from China and LATAM rated their communication as totally personalized (score 7), with 53.3% and 58.3% respectively, while only 35.1% of APAC respondents gave a highly positive rating. Those results led to statistically significant differences between APAC and both LATAM (p=0.044) and CHINA (p=0.045). Furthermore, METAP showed a statistically significant difference with LATAM (p=0.045) with 58.3% of LATAM rating their communication as personalized to each patient compared to the 37% of METAP.
Regarding the perception of patients as experts of their disease, LATAM and APAC showed a significant difference (p= 0.001) as 30.6% of LATAM respondents totally disagreed (score 1) with the notion, and no APAC respondents gave a score of 1 only 26.8% scored higher than 5. Conversely, only 26.8% of LATAM scored higher than 5 versus 51.3% of APAC. Similarly, when asked about their perception of their own patients’ expertise, LATAM had a significant difference with every region (APAC p<0.001 – CHINA p= 0.003 – METAP p<0.001). Indeed 31.6% of LATAM respondents totally disagreed, with 0% agreeing, whereas other regions showed a more optimistic outlook.
The question regarding the relationship between patients and HCPs impacting non-adherence resulted in a significant global effect (p<0.001) and significant differences in between all regions except the pair LATAM-APAC. LATAM showed the highest agreement with 94.5% of scores 5 and above, followed by APAC at 91,8%, then METAP with 72.7% and finally China showed the least overwhelming agreement with 56.8%.
Communication issues associated with non-adherence also varied: for APAC, the main issue was patients not admitting non-adherence (78.4%); for China, it was the socio-cultural level (73.3%); and for LATAM and METAP, it was a lack of time (80.6% and 71.1%, respectively). Additionally, significant differences were noted for three answers: the lack of time (p=0.029), the use of overly technical terms (p= 0.006) and the absence of communication issues (p= 0.007), with distinct regional variations in perceptions and challenges. For the first one, China and LATAM were statistically different (p=0.024) as China considered lack of time to be less relevant compared to LATAM. The use of overly technical terms was considered by China to be more relevant than by both LATAM (p= 0.019) and METAP (p=0.009). Finally, none of LATAM’s respondents chose the answer “there is no communication issue” whereas more than a quarter of respondents from China and APAC ticked that answer resulting in a significant difference between LATAM and both regions (China p= 0.006 and APAC p= 0.006). Results are presented in Table 4.
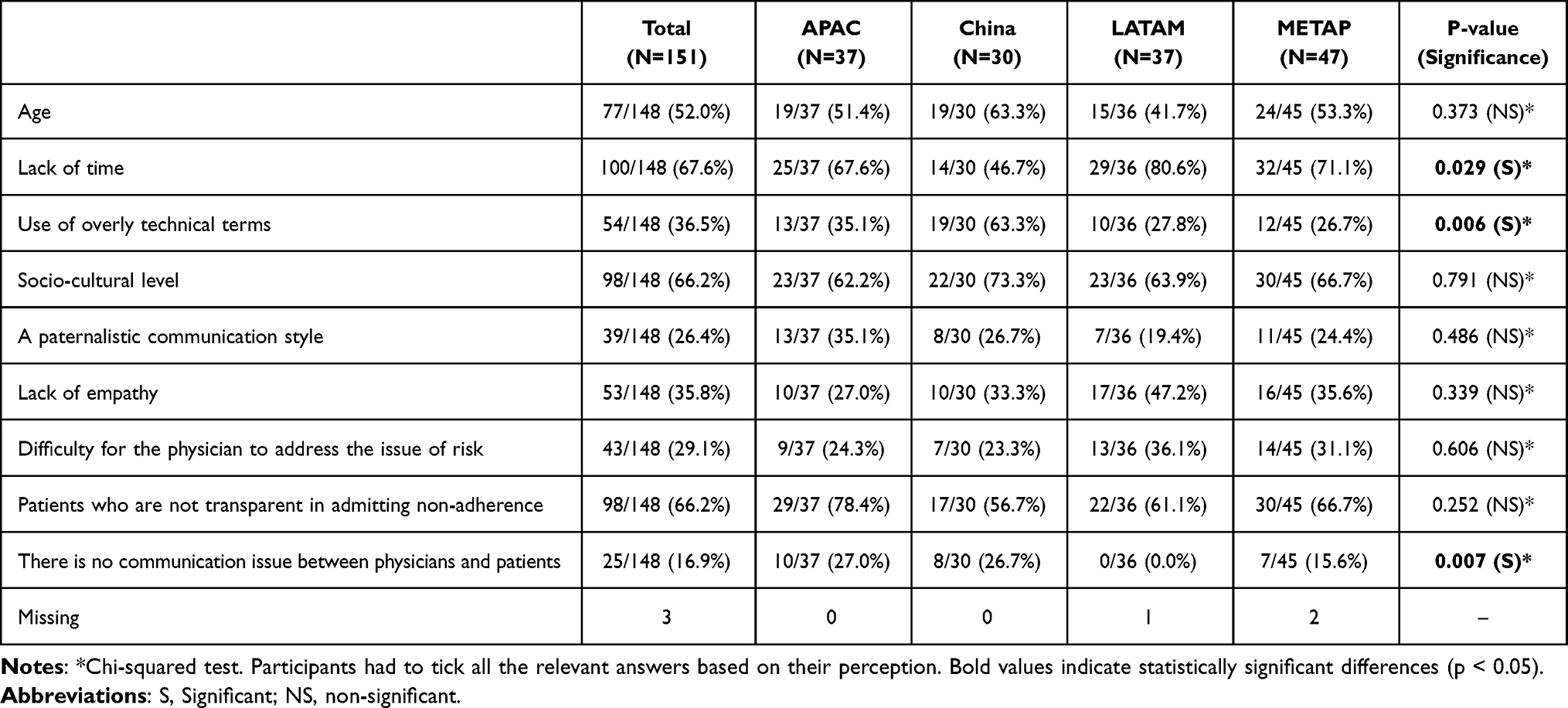 |
Table 4 Communication Issues Between Physicians and Patients Associated with Non-Adherence |
Health Authorities Support
Health authorities support the following public policies based on respondents’ feedback from Question 18 going from 1 totally disagree to 7 totally agree. There were no statistical differences regarding the cost of medication, with a global high agreement (median score of 6). However, significant regional differences were observed in other areas. Access to disease information showed a significant global effect (p= 0.040), after pairwise comparisons, significant difference was observed between LATAM and China (p= 0.037). LATAM rated access to disease information as more necessary than China, with 88.9% of LATAM respondents giving high scores (5–7) compared to 61.4% in China. Similar trends were observed with significant global effects for access to treatment information (p= 0.042) and access to HCPs appointments (p= 0.006). For both criteria respectively, 91,6% and 91,4% of LATAM’s respondents answered 5 or above compared to 66.6% and 60.7% of China’s respondents, (p=0.0010 and p=0.0028, respectively). Additionally, access to care (global effect p <0.001) was significantly more important in LATAM, with 91.7% giving high scores compared to 48.2% in China (p= 0.002) and 70.2% in APAC (p= 0.048).
Discussion
This exploratory study provides crucial insights into the global challenge of non-adherence to dyslipidemia treatments, highlighting both the universal and region-specific factors perceived by healthcare professionals as influencing patient adherence. A key finding is the urgent need for increased awareness and communication about the consequences of non-adherence, as evidenced by the fact that less than half of the respondents (42.6%) correctly estimated the number of premature deaths associated with it. This lack of awareness underscores the necessity for targeted educational initiatives. The consistency in responses across regions for most questions suggests that non-adherence is a widespread issue with common underlying factors, making it a global health concern. However, significant regional differences in healthcare professionals’ perceptions, particularly between APAC and METAP, and LATAM and CHINA, reveal the need for tailored interventions.
Key factors such as side effects (67.8%), patient health literacy (65.7%), and perceived severity of cardiovascular disease (62.3%) were identified as major influences on non-adherence with no significant difference across the regions. These three determinants of non-adherence are consistently observed because they reflect universal mechanisms of patient behavior: side effects directly undermine tolerance of long-term therapy, while limited health literacy and a low perceived cardiovascular risk weaken understanding and motivation to continue treatment. As a result, concerns about adverse effects, difficulties in understanding medical information, and underestimation of cardiovascular risk repeatedly emerge in international studies as core drivers of poor adherence to dyslipidemia and other cardiovascular medication.8,14
However, other influential factors revealed significant differences across at least two of the regions. Notably, healthcare professionals in the METAP region identified several factors complexity of treatment, timing of taking treatment, mental health issues, forgotten treatments, and lack of support from family and general practitioners (GPs) as having less influence on non-adherence compared to their counterparts in other regions, especially APAC. This difference was most pronounced with the APAC region, indicating a significant disparity in perceptions. Two main mechanisms can help explain this difference in perceptions. First, studies show that clinicians often underestimate patient-level barriers such as regimen complexity, mental health issues, forgetfulness, and lack of social or family support compared with what patients report, a gap that appears particularly marked in Middle Eastern contexts where communication about such difficulties may be more constrained.15 Second, in many METAP countries, structural barriers like access, cost, and fragmented health systems dominate clinicians’ concerns, so these “system-level” problems tend to overshadow timing, family support, or GP involvement, whereas in several Asia-Pacific settings the literature more frequently highlights patient and family-related determinants of adherence, leading APAC HCPs to rate these factors as more influential.
The perception of the complexity of treatment as a determinant of non-adherence is debated within the METAP region. Alefishat et al found it to be a significant factor,16 whereas Arafat et al reported that an increased number of medications could lead to better adherence.17 This contradiction may explain the regional differences in HCPs opinions, reflecting varying clinical experiences and general opinions.
The impact of the timing of treatment on adherence remains unclear. A randomized controlled trial (RCT) in Malaysia suggested better adherence with evening doses, though the results were not statistically significant. Conversely, a cross-sectional study indicated that night-time or random administration could lead to poorer adherence.18 These mixed findings contribute to differing regional perspectives.
Mental health, particularly depression, was a significant point of difference between APAC and China, with APAC reporting a higher influence of depression on non-adherence. This could be related to the higher incidence of depression in APAC, influenced by factors such as race, treatment availability, and societal factors. However, both regions face a significant mental health problem and developed programs to promote it. China invested in suicide prevention interventions whereas Thailand focused more on mental health promotion interventions.19 Furthermore, the METAP respondents considered depression and cognitive disorder as having significantly less influence on medication adherence compared to APAC respondents despite also being burden by mental health disorders.20
Forgetfulness, a form of unintentional non-adherence, are most common at the beginning of treatment when patients have not yet developed routine habits.2,3 This factor was perceived differently across regions, with APAC HCPs attributing more influence on it compared to METAP HCPs. Nonetheless, a systematic review on medication adherence factors in the Middle East and North Africa identified forgetfulness as a major barrier to adherence, in which many interventions can overcome this hindrance.20
The lack of support from either family or GPs was deemed significantly less influential by METAP than by the other regions. As pointed out by Jaam et al, the lack of social support is under investigated in the METAP regions and further research is needed.21 The paucity of research could explain the difference in the HCPs’ perceptions across the different regions. Cultural differences in family dynamics, the role of family in patients and the varying involvement of primary care providers in different healthcare systems.
In our study, we observed notable regional differences in HCPs’ perceptions and attitudes, both in general and within their personal practice. Specifically, the question of HCPs’ communication revealed a significant global effect, although the specific regions showing differences varied between the general and personal contexts. Initially, METAP and APAC displayed significant differences on the general question, but this was not replicated in the personal context, where a broader array of regions showed differences without including the METAP-APAC pair. Similarly, regarding HCPs viewing patients as experts in their diseases, a significant global effect was again observed. Initially, only LATAM and APAC exhibited significant differences; however, when HCPs considered their personal practice, LATAM significantly differed from all other regions. LATAM HCPs generally disagreed with the notion, contrasting with the more neutral or agreeable stances from other regions.
Additionally, in the context of public policies’ focus, significant differences consistently involved China and LATAM, with one notable difference between APAC and LATAM concerning access to care. These findings underscore the complex and variable nature of regional perspectives in the medical community, highlighting the necessity for tailored communication and policy approaches sensitive to regional disparities.
The challenge of poor adherence to dyslipidemia treatment persists globally, with approximately a quarter to a third of the study population across various regions exhibiting poor adherence rates. This issue is not unique to any specific region, indicating a widespread problem that necessitates global attention and solutions. Existing literature, including a systematic review from Colombia, highlights an adherence rate of 70% for patients on lipid-lowering drugs.22 Despite ongoing efforts, the prevalence of poor adherence remains troublingly high.
Several factors contribute to the sustained prevalence of poor adherence. Firstly, interventions may lack effectiveness or efficiency due to diverse healthcare systems, varying levels of patient education, and socioeconomic disparities across regions. Furthermore, many interventions are not sustainable in the long term, often due to insufficient resources, inconsistent follow-up, and the complexity of managing chronic conditions like dyslipidemia.
The root causes of poor adherence may not have been fully addressed. Barriers such as medication costs, side effects, patient beliefs about medication necessity and efficacy, and the complexity of treatment regimens play significant roles. Additionally, there may be gaps in healthcare provider-patient communication and trust, leading to misunderstandings and non-compliance. Addressing these multifaceted issues requires a comprehensive approach, integrating patient education, system-level changes, and personalized care strategies to enhance adherence and ultimately improve outcomes in dyslipidemia management.
Despite its comprehensive approach, the study has limitations. First, data were collected through a self-administered online questionnaire, which may introduce potential biases in self-reported data response, as participants may have provided answers perceived as professionally appropriate rather than strictly reflecting their actual practices. Variability in healthcare systems and practices across regions may also have influence responses. Moreover, ordinal response categories were analyzed as nominal. Although it is appropriate for our descriptive analysis, it may have led to some loss of information. Second, given that this was not a clinical study, there were no predefined hypotheses and no formal sample size calculation except minimal requested for statistical analysis, but we expected to receive more responses to the questionnaire. The small and imbalanced sample size across regions impacts the quality of the statistical analysis, and limits the generalization of the findings. Nevertheless, the study’s strength lies in its broad geographical scope and the identification of both universal and region-specific barriers to adherence. Future research should aim to address these limitations of this exploratory study and further explore the root causes of non-adherence, particularly the psychosocial and systemic factors, to develop more effective, sustainable interventions tailored to regional needs.
Conclusion
In conclusion, this survey revealed medication adherence as a global health concerned with some significant regional differences in healthcare professionals’ perceptions of factors influencing patient adherence to cardiovascular treatments. These differences underscore the importance of considering regional and cultural contexts when developing strategies to improve adherence. Understanding these nuances can help tailor interventions to address specific barriers and improve patient outcomes globally.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study, under the General Data Protection Regulations (GDPR) may be available for research collaboration purposes upon reasonable request to the corresponding author and will require the completion of a data processing agreement.
Ethical Approval and Consent to Participate
Ethics Committee approval was not required for this type of survey, in accordance with the national regulations of the countries where the study was conducted. The questionnaire did not collect any patient-related information, and the results were analyzed anonymously and in aggregate form only. Participating Healthcare professionalswere required to read the data privacy policy section before completing the questionnaire and had to agree to the terms and consent to participate to gain access. No human or animal experimentation was conducted in this study.
Acknowledgment
The authors thank Prof. Robert Horne and Prof. Eric Bruckert for their support in drafting the questionnaire. They also thank the KPL Paris agency, with Alice Moreau-Gely providing medical writing and editorial support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that this study received funding from Abbott, Switzerland. The funder was not involved in the study design, collection, analysis, interpretation of data, or the writing of this article.
Disclosure
Alfonso Bryce has received honoraria for lectures from Abbott, AstraZeneca, Bayer, Biotoscana, Boehringer, Bristol Myers Squibb, Emcure, Farmakonsuma, Farmindustria, Glaxo, Grupo Farma, Megalabs, Menarini, Merck Serono, MSD, Novartis, OM, Pfizer, Roemmers, Sanofi Aventi, Servier, Schering-Ploug, Tecnofarma and Teva. In addition, he has received research grants from Abbott, Glaxo, MSD, Novartis and Takeda, personal fees for advisory board participation from Abbott, AstraZeneca, Boehringer, Glaxo, MSD, Novartis, Pfizer, and honoraria as consultant from Servier. Lale Tokgözoğlu declare having receiving fees for several project not related to this article from Abbott, Amarin, Amgen, AstraZeneca, Bayer, Daiichi Sankyo, Lilly, Menarini, MSD, Novartis, Novo Nordisk, Sanofi, Pfizer, Ultragenyx, Viatris, Zentiva. Mohamad Samir Arnaout has received honoraria from different pharmaceutical companies for lectures, consultation and advisory boards, such as Abbott, Boehringer, Merck Serono, Servier, Novartis and AstraZeneca. Andressa Da Silva van der Laan declare being Abbott employee. Ngiap Chuan Tan, Zhenyue Chen and Mousa Akbar have no conflicts of interest to declare for this work.
References
1. Burnier M. The role of adherence in patients with chronic diseases. Eur J Internal Med. 2024;119:1–13. doi:10.1016/j.ejim.2023.07.008
2. Lam WY, Fresco P. Medication adherence measures: an overview. BioMed Res Int. 2015;2015:1–12. doi:10.1155/2015/217047
3. Chia L (Rebecca), Schlenk EA, Dunbar-Jacob J. Effect of personal and cultural beliefs on medication adherence in the elderly. Drugs Aging. 2006;23(3):191–202. doi:10.2165/00002512-200623030-00002
4. Chowdhury R, Khan H, Heydon E, et al. Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences. Eur Heart J. 2013;34(38):2940–2948. doi:10.1093/eurheartj/eht295
5. Cea-Calvo L, Marín-Jiménez I, De Toro J, et al. Association between non-adherence behaviors, patients’ experience with healthcare and beliefs in medications: a survey of patients with different chronic conditions. Current Med Res Opin. 2020;36(2):293–300. doi:10.1080/03007995.2019.1676539
6. Kengne AP, Brière JB, Zhu L, et al. Impact of poor medication adherence on clinical outcomes and health resource utilization in patients with hypertension and/or dyslipidemia: systematic review. Expert Rev Pharmacoeconom Outcomes Res. 2024;24(1):143–154. doi:10.1080/14737167.2023.2266135
7. Lee SQ, Raamkumar AS, Li J, et al. Reasons for primary medication nonadherence: a systematic review and metric analysis. JMCP. 2018;24(8):778–794. doi:10.18553/jmcp.2018.24.8.778
8. Lopes J, Santos P. Determinants of non-adherence to the medications for dyslipidemia: a systematic review. PPA. 2021;15:1853–1871. doi:10.2147/PPA.S319604
9. Ortega Cerda JJ, Sanchez Herrera D, Miranda ÓA R, Ortega Legaspi JM. Adherencia terapéutica: un problema de atención médica. Acta Medica Gruop Angeles. 2018;16(3):226–232.
10. Perez JH. Adherencia al tratamiento farmacológico. Med Resp. 2015;8:47–52.
11. Han KT, Choi DW, Kim S. Regional and income disparities in treatment and drug adherence of patients with dyslipidemia: a retrospective cohort study in South Korea, 2003–2015. BMC Geriatr. 2021;21(1):585. doi:10.1186/s12877-021-02510-5
12. Del Razo F, Martin-Vences AJ, Brito-Córdova GX, et al. Primary barriers of adherence to a structured nutritional intervention in patients with dyslipidemia. Nutrients. 2021;13(6):1744. doi:10.3390/nu13061744
13. Almahmeed W, Alabadla Z, Al awadi F, et al. Improving therapeutic adherence and reducing therapeutic inertia in the management of people with cardiometabolic diseases: a call-to-action from the Middle East. Adv Ther. 2025;42(3):1340–1359. doi:10.1007/s12325-024-03103-5
14. Rezaei S, Vaezi F, Afzal G, Naderi N, Mehralian G. Medication adherence and health literacy in patients with heart failure: a cross-sectional survey in Iran. Health Lit Res Pract. 2022;6(3):e191–e199. doi:10.3928/24748307-20220718-02
15. Waheedi M, Jeragh-Alhaddad F, Awad A, Enlund H. “Patients’ understanding is the problem”: physicians’ views of nonadherence among Arabs with type 2 diabetes. PPA. 2017;11:1413–1421. doi:10.2147/PPA.S138468
16. Alefishat E, Jarab AS, Al-Qerem W, Abu-Zaytoun L. Factors associated with medication non-adherence in patients with dyslipidemia. Healthcare. 2021;9(7):813. doi:10.3390/healthcare9070813
17. Arafat Y, Mohamed Ibrahim MI, Awaisu A, et al. Using the transtheoretical model’s stages of change to predict medication adherence in patients with type 2 diabetes mellitus in a primary health care setting. DARU J Pharm Sci. 2019;27(1):91–99. doi:10.1007/s40199-019-00246-7
18. Said AH, Abd Rahim IS, Mohamad Zaini NNB, Saiful Nizam NIB. Factors affecting adherence to lipid-lowering drugs: a scoping review. Oman Med J. 2023;38(4):e523. doi:10.5001/omj.2023.67
19. Moeller‐Saxone K, Davis E, Herrman H. Promoting mental health in Asia‐Pacific: systematic review focusing on
20. Travers KU, Pokora TD, Cadarette SM, Mould JF. Major depressive disorder in Africa and the Middle East: a systematic literature review. Expert Rev Pharmacoeconom Outcomes Res. 2013;13(5):613–630. doi:10.1586/14737167.2013.838026
21. Jaam M, Ibrahim MIM, Kheir N, Awaisu A. Factors associated with medication adherence among patients with diabetes in the Middle East and North Africa region: a systematic mixed studies review. Diab Res Clin Pract. 2017;129:1–15. doi:10.1016/j.diabres.2017.04.015
22. Cáceres C, Lora ÁJ, Villabona SJ, Rocha MC, Camacho PA. Cumplimiento del tratamiento farmacológico en enfermedades crónicas no transmisibles en la población colombiana: revisión sistemática y metaanálisis. Biomedica. 2023;43(Sp. 3):51–65. doi:10.7705/biomedica.7077
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Its Associated Determinants in Older Adults with Type 2 Diabetes and Cardiovascular Comorbidities
Al-Azayzih A, Kanaan RJ, Altawalbeh SM, Al-Qerem W, Smadi S
Patient Preference and Adherence 2023, 17:3107-3118
Published Date: 29 November 2023
Improving Medication Adherence and Lifestyle Changes: An Image-Based Educational Tool for Patients with Heart Failure
Gao L, Xie Q, Liu T, Liu H, Yan S, Han Y, Zhang M, Zhu D, Guo N, Nicholas S, Maitland E, Wang D
Patient Preference and Adherence 2025, 19:2251-2262
Published Date: 30 July 2025
Patient Knowledge and Adherence to Oral Anticoagulation Therapy: Findings from an Observational Study in Italian Tertiary Care Hospitals
Stella M, Boccardi D, Baiardi G, Lantieri F, Astuni P, Sacco F, Pasquariello S, Cameran Caviglia M, Zanini M, Natali E, Robbiano L, Caneva G, Duce R, Antonucci G, Innocenti L, Nanni L, Mattioli F
Patient Preference and Adherence 2026, 20:610940
Published Date: 10 July 2026