Back to Journals » Patient Preference and Adherence » Volume 20
Patient Knowledge and Adherence to Oral Anticoagulation Therapy: Findings from an Observational Study in Italian Tertiary Care Hospitals
Authors Stella M, Boccardi D, Baiardi G ![]() , Lantieri F, Astuni P, Sacco F, Pasquariello S, Cameran Caviglia M, Zanini M, Natali E, Robbiano L, Caneva G, Duce R, Antonucci G, Innocenti L, Nanni L, Mattioli F
, Lantieri F, Astuni P, Sacco F, Pasquariello S, Cameran Caviglia M, Zanini M, Natali E, Robbiano L, Caneva G, Duce R, Antonucci G, Innocenti L, Nanni L, Mattioli F ![]()
Received 21 March 2026
Accepted for publication 17 June 2026
Published 10 July 2026 Volume 2026:20 610940
DOI https://doi.org/10.2147/PPA.S610940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Manuela Stella,1,2,* Davide Boccardi,1,* Giammarco Baiardi,3,* Francesca Lantieri,4 Pietro Astuni,1 Fabio Sacco,5 Stefano Pasquariello,6 Michela Cameran Caviglia,1 Milko Zanini,4 Eleonora Natali,7 Luigi Robbiano,4 Giacomo Caneva,3 Rita Duce,8 Giancarlo Antonucci,8 Leonello Innocenti,8 Luca Nanni,3 Francesca Mattioli1,8
1Department of Internal Medicine, University of Genoa, Genoa, Italy; 2IRCCS Istituto Giannina Gaslini, Genoa, Italy; 3Department of Laboratory Diagnostics, IRCCS Azienda Ospedaliera Metropolitana, Plesso Ospedale Policlinico San Martino, Genoa, Italy; 4Department of Health Science, University of Genoa, Genoa, Italy; 5Integrated Department of Mental Health and Addiction Pathologies, ASL Alessandria, Alessandria, Italy; 6Department of Mental Health and Addictions, ASST Santi Paolo E Carlo, Milan, Italy; 7Immunohematology and Transfusion Medicine Unit, ASL 5, La Spezia, Italy; 8Ente Ospedaliero Ospedali Galliera, Genoa, Italy
*These authors contributed equally to this work
Correspondence: Francesca Mattioli, Department of Internal Medicine, University of Genoa, Genoa, Italy, Email [email protected]
Purpose: To assess treatment adherence, knowledge of oral anticoagulant (OA) therapy, and quality of life in adult patients on chronic anticoagulation, and to evaluate whether a brief educational intervention improves understanding and self-management.
Patients and Methods: An observational study was conducted in patients receiving OAs at three thrombosis centers in Genoa, Italy. Adherence, knowledge, and quality of life were assessed using validated questionnaires: Tool for Adherence Behaviour Screening (TABS), Anticoagulation Knowledge Tool (AKT), and EuroQol-5D-5L. A clinical pharmacologist delivered a brief educational session on treatment risks, drug–food interactions, and management. Questionnaires were re-administered at follow-up. Data were analyzed using descriptive statistics and nonparametric tests (Mann–Whitney, Kruskal–Wallis).
Results: A total of 124 patients were enrolled (58.9% women; mean age 69.6 years); 61% were on Vitamin K Antagonists, while the remaining patients were treated with Direct Oral Anticoagulants. Mean adherence and knowledge scores were 37.1/40 and 18.1/23, respectively. Knowledge was weakly but significantly correlated with adherence (rs=0.190, p=0.035). Women showed higher knowledge scores than men (p=0.0117). Adherence and knowledge differed across centers (p=0.0037 and p< 0.0001), with better outcomes in more individualized settings. Patients were more familiar with lifestyle aspects than with scientific therapy details. Quality of life varied by gender (p=0.0351), education (p=0.0021), occupation (p=0.0156), age (p=0.012) and living alone (p=0.041). At follow-up, knowledge scores increased after the educational intervention (18.1 vs 21.7); however, only 25 patients completed the questionnaires again, limiting the reliability of these findings, which should therefore be considered exploratory.
Conclusion: A weak but significant association between knowledge and treatment adherence was observed in patients receiving oral anticoagulants. Patient education may be a useful tool to improve patients’ understanding of the risk-benefit profile of anticoagulation treatment and thus treatment adherence. However, further studies are issued to confirm this study hypothesis-generating exploratory findings with a larger patient population and more objective measures of patient adherence.
Keywords: medication adherence, patient experience data, clinical pharmacology, quality of life, patient education, patient-reported outcome measures
Introduction
Oral anticoagulant (OA) drugs - vitamin K antagonist (VKAs) and direct-acting oral anticoagulants (DOACs) - are the primary care treatment for the long-term prevention of thromboembolic events (TEs). VKAs act through an indirect mechanism of action by inhibiting the vitamin K epoxide reductase complex (VKORC1), enzyme essential in the vitamin K cycle.1 Currently available VKAs in Italy are warfarin and acenocoumarol, both are indicated for the treatment and prevention of pulmonary embolism (PE), deep vein thrombosis (DVT), arterial thromboembolism associated with chronic atrial fibrillation, mechanical or biological heart valve prostheses, intracardiac mural thrombosis, and acute myocardial infarction.2,3 Despite their widespread use, have a major limitation related to their interaction profile with numerous drugs and dietary components, which may contribute to adherence issues and increase the risk of bleeding or recurrence of TEs.4,5 Consequently, monitoring of VKAs anticoagulant activity is mandatory and standardized throughout hospitals by the measurement of the International Normalized Ratio (INR), which provides a reliable indicator of the functionality of the extrinsic coagulation pathway affected by the pharmacodynamic mechanism of VKAs.6 Thus, numerous follow-up visits are required to monitor patients on VKAs which may have a significant impact on their quality of life (QoL) and represent a substantial cost for the National Health Service (NHS). INR monitoring is indeed costly, both in terms of healthcare personnel time (physicians and nurses) and laboratory resources of the NHS.7,8
DOACs act as selective, competitive and reversible inhibitors of either the activated coagulation factor X (apixaban, edoxaban, rivaroxaban)9–11 or thrombin (dabigatran).12 DOACs represent an excellent alternative to VKAs for similar indications due to their favorable pharmacokinetic profile and the reduced need for frequent follow-up visits (approximately every six months), although they still require careful evaluation of drug–drug interactions (DDIs) during prescription. DOACs may also be used in patients previously treated with VKAs, who demonstrate poor control of INR (time in therapeutic range, TTR <50%), or poor treatment adherence.13–15 Monitoring of DOACs plasma levels is nowadays spread to many hospitals by means of both indirect and direct methods of quantification, since recent International Council for Standardization in Haematology guidelines suggest therapeutic drug monitoring of DOACs in patients with multiple factors that can interfere with their pharmacokinetics.16 Exposure to anticoagulant drugs in Italy increases with patient age in both sexes, reaching a national prevalence of use of 5.8% with adherence generally worsening with increasing age, due to deteriorating cognitive function, likely worsening health status, and changing socioeconomic conditions.17
Adherence to therapy is an act that requires active involvement of the patient; adherence refers to the degree to which the patient follows medical instructions regarding the use of a particular treatment. Adherence is divided into primary adherence, which refers to the extent to which a patient initiates a new prescription, and secondary adherence, which refers to persistence with a specific drug treatment over time. Generally, secondary adherence is more widely studied, as we have done in our study. Adherence is considered good when it exceeds 80%, and data from the literature on patients using OA in AF show adherence of 63% at 6 months of therapy and 70% at 12 months.18 Several aspects can influence adherence to treatment in chronic conditions including social and economic factors (poverty, cost of medication), therapy (long duration of therapy, polypharmacy, side effects) and the quality of the relationship with healthcare professionals. Another very important factor that often leads to non-adherence is when therapy is administered in an asymptomatic condition, as is often the case with anticoagulant therapy.18 Knowledge of the disease and the related treatment is one of the patient-related factors that seems to correlate best with treatment outcomes. Among patient-related factors associated with therapeutic outcomes, knowledge of the disease and its treatment plays a key role.7,19 Some studies point out the existence of a direct correlation between treatment knowledge of the risks and benefits of the medication and adherence to the treatment plan.20–23
Poor adherence to treatment is one of the possible factors behind therapeutic ineffectiveness, leading to damage to patients’ health and a waste of health care system resources; however, non-adherence to therapy is often not adequately considered in clinical care pathways, resulting in increased morbidity and mortality.8,14 Data from the literature show that the use of Patient Experience Data (PED) is increasingly being encouraged,24 including for registration purposes and in the early stages of drug development. This is because PED, in particular the patient-reported outcome measures (PROMs), provides unique information as it reports the patient’s direct experience.25 Specifically, direct and indirect methods can be used to measure adherence. Direct methods include direct observation of prescribed drug use, pill counting, therapeutic drug monitoring (TDM), and biomarker measurement; indirect methods, on the other hand, include methods included in the PEDs, such as interviews with patients, questionnaires, and evaluation of clinical response.19,20 In clinical practice, greater confidence in patient reported outcomes may facilitate the effective use of PEDs, improving treatment adherence and supporting the identification of factors contributing to non-adherence.25
Another important tool that has proven useful in improving patients’ understanding of their conditions and treatments is “the therapeutic education”. Therapeutic education is intended as a complementary and facilitative approach to medical and surgical treatments. The primary goal of therapeutic education is to improve patients’ understanding of their illnesses and treatments, thereby enabling them to better manage their condition by taking an active role in managing their own treatment. Specifically, several studies have shown that structured therapeutic education programs can have beneficial implications for patients; moreover, the World Health Organization promotes therapeutic education as a model of care for chronic diseases.26–28
The primary objective of the present study was to assess by indirect methods the degree of adherence to and knowledge of oral anticoagulation therapy using questionnaires, in a population of adult patients chronically treated for the prevention of thromboembolic events.
Patients and Methods
Study Design
This is a non-profit, prospective observational multicentre study. The primary objective of the present study was to assess the degree of adherence and knowledge of oral anticoagulation therapy in a population of adult patients chronically treated for the prevention of thromboembolic event. For this purpose, two questionnaires were administered, namely the Tool Adherence Behavior Screening (TABS) and the Anticoagulation Knowledge Tool (AKT).29–31 The study also aims to address the following secondary objectives: i) to assess possible differences in adherence and knowledge levels between patients on VKAs and patients on DOACs and to evaluate whether the level of knowledge affects adherence to therapy; ii) to reassess, at the next follow-up visit, the level of adherence and knowledge of OA therapy through re-administration of the TABS and AKT questionnaires in the enrolled population; iii) to assess the occurrence of any treatment-related adverse events (AEs); iv) to evaluate patients’ reported QoL, assessed by self-administration of the Health-related Quality Of Life measure (EuroQol-5D-5L) questionnaire.32,33
The study was approved by the Territorial Ethics Committee-Liguria Region (authorization nr. 387/2023). Written informed consent was obtained from all patients.
Setting
This multicenter study was conducted at the Thrombosis Center and Anticoagulation Clinic of E.O. Ospedali Galliera (Genoa, Italy), and at the Anticoagulation Clinic of IRCCS Ospedale Policlinico San Martino (Genoa, Italy), which represent the two main hospitals in the city and cover a large proportion of the local population.
Clinical and laboratory data were collected from the patients’ medical record in the context of clinical routine analysis between September 2023 and June 2024. All information and metadata were anonymized before statistical analysis.
At baseline, all enrolled patients completed the questionnaires and participated in a therapeutic education session with the Clinical Pharmacologist. Follow-up questionnaires were scheduled at the subsequent visit.
Participants
All outpatients (aged ≥18 years) on chronic OAs treatment with for at least one month, referring to the aforementioned outpatient clinics and who provided written informed consent, were enrolled. Exclusion criteria were any condition that affected the ability to complete the assessment, including severe impairment of cognitive function, delirium, Alzheimer’s disease or any other severe neurological disease, refusal to provide informed consent or the presence of language barriers.
During a routine visit (first study visit), the general clinical condition of the participants was assessed and any changes in OA therapy were made only according to routine. Immediately prior to the visit, TABS and AKT questionnaires were administered to the patients by the investigating physician, together with the self-administered EuroQol-5D-5L questionnaire. After the completion of the questionnaires, a therapeutic education phase was conducted during the same first visit by a Clinical Pharmacologist, during which the completed questionnaires were reviewed together with the patient, with the goal of correcting any errors in adherence and knowledge and improving the patient’s knowledge of their anticoagulant therapy. The session lasted an average of 10–15 minutes, depending on the participants’ prior knowledge and their speed in understanding new information. During the educational session, no written informational material was provided to the patients, but the physician highlighted the essential aspects of the patient’s therapy, placing particular emphasis on potential drug-drug, drug-herbal, and drug-food interactions.
During this session, the investigator was available to answer all the patient’s questions and doubts regarding OA therapy. All data in the medical record regarding anthropometric measurements (age, sex, origin, schooling, occupation, height, weight, etc..), laboratory tests pertaining to the patient’s coagulation status and overall health status, performed according to normal clinical practice, were collected in the case report form (CRF) by the investigator.
At the time of the next scheduled visit (second study visit - planned after an average of 3 weeks for patients treated with VKAs and after about six months for patients treated with DOACs), TABS, AKT, and EuroQol-5D-5L questionnaires were once again administered by the investigator to the patients in the same manner as above and the data were collected on CRFs. The primary endpoint was the assessment of adherence and knowledge among patients receiving oral anticoagulant therapy, measured through the administration of the TABS and AKT questionnaires, respectively.
Secondary endpoint were assessed by: analysing any differences in TABS and AKT scores between patients on VKA therapy and patients on DOAC therapy; measuring the correlation between patient adherence and knowledge, stratifying by various covariates (eg. age, gender, origin, education, profession, etc.); differences in scores between the first and second administration of the TABS and AKT questionnaires; recording the number of adverse events; evaluating changes in quality of life between the first visit and the second evaluation.
It was also planned to collect any adverse events (AEs) related to the treatment and reported in the patient’s medical record.
Questionnaires
TABS is a validated component of the Beliefs and Behaviour Questionnaire (BBQ);30 the latter is a 30-item questionnaire comprising multiple scales. Although the TABS sub-scale has not been validated for the assessment of adherence (AD) in patients on anticoagulation treatment, it has been validated for use in patients with chronic diseases. The TABS subscale is structured in two sections, Adherence and Non-adherence, each comprising four questions, for a total of eight item. Answers on patient behaviors and beliefs can be scored from 1 to 5, ranging from “always” to “never”. For the Adherence section, the maximum score of 5 was given if the patient answered “always”. The questions in this section are designed to assess positive behaviors that are considered favorable for the patient to adopt. For the section on Non-adherence, the items were scored in the opposite way, with the maximum score of 5 given to “never”. Since the questionnaire was administered by the physician as a structured interview rather than being self-administered, the Italian translation did not require an additional validation study. However, all eight items and possible answers were translated and verified by two different translators. To ensure sociocultural appropriateness and semantic clarity of the translated terms, a pool of experts was involved in the translation process, as recommended by Kalfoss.34 This step aligns with best practices for addressing the semantic and cultural challenges inherent in adapting questionnaires to different populations. Furthermore, a content validity approach was employed, consistent with recommendations by Colina et al,35 to verify that the translated content accurately reflected the original questionnaire’s constructs and maintained its validity.
The AKT questionnaire was published by K. O. Obamiro et al in 201631 to provide a validated tool to assess patients’ knowledge (KN) about OA therapy. This questionnaire, unlike those already in the literature, is the only one that has been psychometrically validated to be administered not only to patients on VKA therapy but also to patients on DOAC therapy. It consists of twenty-eight questions and is divided into sections: part A (20 items), applicable to both VKAs and DOACS, and part B (8 items) applicable only to VKAs. According to K. O. Obamiro and collaborators, the AKT may also be used to evaluate the effects of therapeutic education interventions and to investigate the association between knowledge and clinical outcomes.19 The Italian version of the AKT (I-AKT), similarly to the original AKT, has good psychometric properties and can be used in clinical practice and research.29,36 The AKT score for part A is calculated, by assigning a maximum of 3 points to items 18 and 19, a maximum of 2 points to item 6, and a maximum of 1 point to all other items (for a total of a maximum of 25 points). The AKT score for part B is calculated by assigning a maximum of 3 points to item 6b and a maximum of 1 point to all other items, for a total maximum of 10 points.
The EuroQol-5D-5L is a questionnaire used worldwide and designed to be self-administered by the patient, aimed at measuring health status. The EuroQol-5D-5L questionnaire has been validated in Italian for telemedicine. EuroQol-5D-5L consists of a short descriptive questionnaire and a visual analog scale (EQ VAS) that do not require cognitive engagement and can be completed in a few minutes. The instrument investigates five dimensions: mobility (MO), self-care (SC), usual activities (UA), pain/discomfort (PD), and anxiety/depression (AD). Each dimension has 5 levels: no problems, mild problems, moderate problems, severe problems, and extreme problems. These five scored dimensions a 5-digit code that indicates health status. Scores can also be used to calculate a summarized utility score, weighting each dimension by the EuroQol-5D-5L value set calculated for Italy37 and subtracting parameter estimates for each dimension level of the health state from 1. The EQ VAS records the patient’s self-rated health on a 100-point vertical visual analog scale, where the endpoints are labeled as “The best health you can imagine” (100) and “The worst health you can imagine” (0).38
Statistical Methods
Data was analysed using descriptive statistical techniques. Quantitative variables were reported as mean and standard deviation (SD), scale scores were reported as median and interquartile range (IQR), but also as mean and SD for better readability, and categorical data were described by frequencies and percentages.
Data were compared using the nonparametric Mann–Whitney and Kruskal–Wallis tests. The Dunn test was used for Kruskal–Wallis post hoc multiple comparisons, with p-values adjusted using the Benjamini-Hochberg method. Regression models were applied to test if selected variables could predict AKT part A and TABS scores. Spearman correlation was used to assess the association between the two scales (TABS and AKT). All tests were two-tailed with a significance level set at α = 0.05.
If a patient missed the second study visit, data from the first visit were considered only for study objectives that did not require comparison with follow-up data.
Results
One hundred and twenty-four patients were enrolled, 48 receiving DOAC therapy and 76 receiving VKA therapy. The average age was 69.6 ± 12.9. The other demographic characteristics are reported in Table 1.
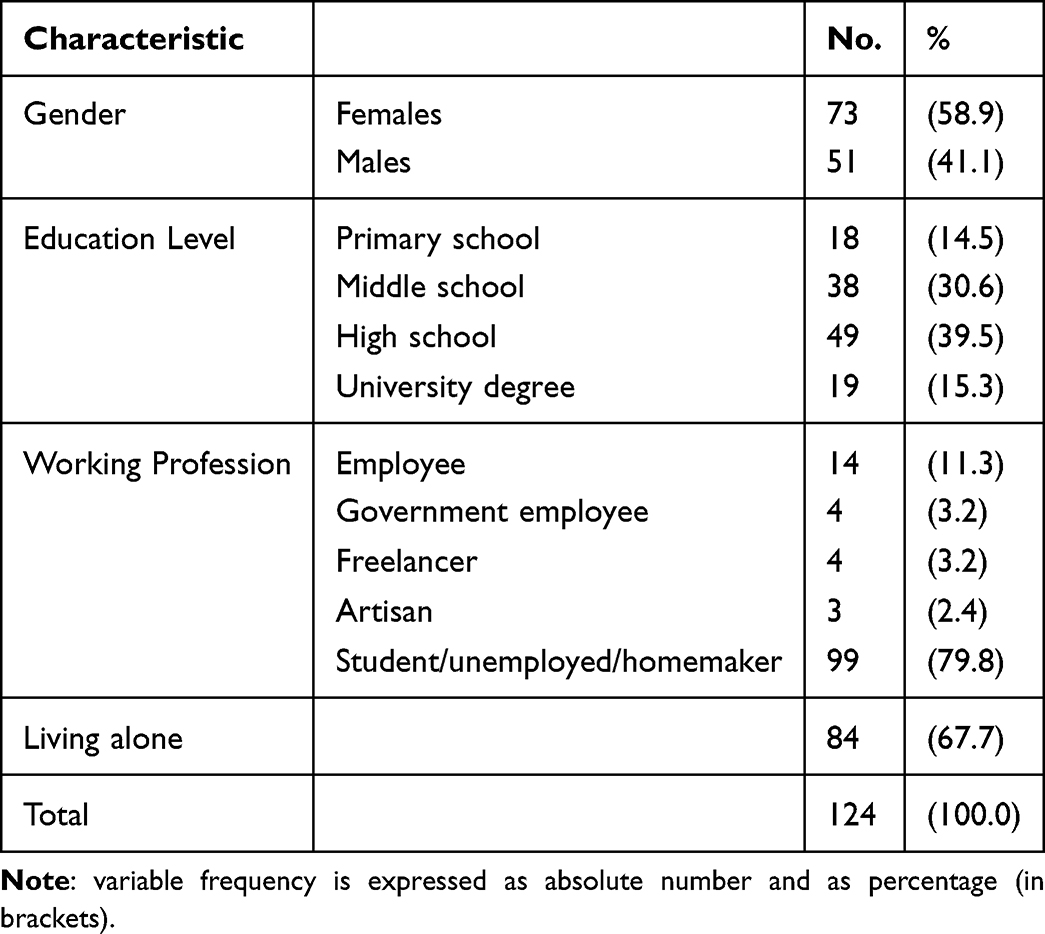 |
Table 1 Demographic Data of Enrolled Patients (n = 124) |
AKT- part A, regardless of the type of OA taken, revealed a mean (±SD) knowledge score of 18.1 ± 4.1 (median = 19). The maximum score of 25 was not achieved by any patient, while only 2.4% of the patients scored 24 (3 out of 124 patients). The knowledge score was slightly higher among patients treated with VKAs compared with those receiving DOACs (mean 18.3 vs 17.6) and slightly higher among those with higher levels of education (17.5 for patients up to the middle school level vs 18.5 for those with a high school and or university degree, although the differences were not statistically significant. No differences were detectable for other socio-demographic variables such as working profession and age. However, the knowledge score was significantly higher in female patients (18.9, median 20) than in male patients (16.9, median 18) (p=0.0117, Mann–Whitney test), for both DOACs (18.6, median 20 vs 16.8, median 18) and VKA (19.0, median 20 vs 17.0, median 17.5) (Figure 1). A multiple regression model used to evaluate whether gender, type of OA therapy (DOACs or VKAs), and education level, independently predicted the knowledge score confirmed gender as the only statistically significant predictor, although the model explained only a small portion of the variance. The simple linear regression including gender was overall statistically significant overall (R2=0.059, F (1, 122) =7.695, p=0.006), and the fitted regression equation was knowledge =14.84 + 2.03*gender.
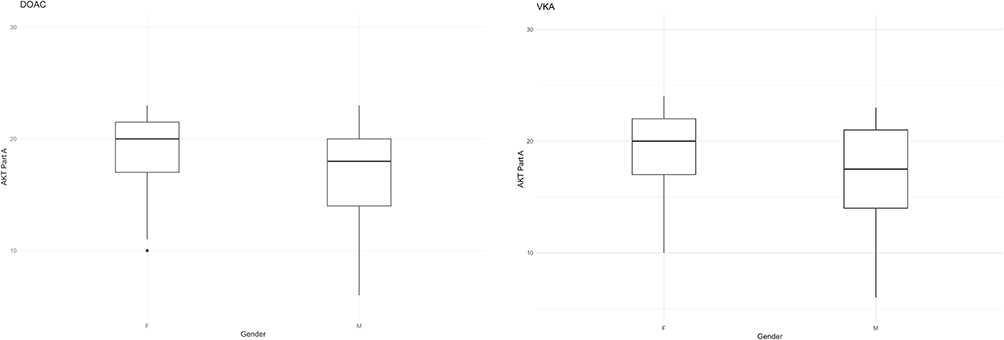 |
Figure 1 AKT - part A scores by gender and type of oral anticoagulant (OA). Notes: Notes: AKT Part A scores are displayed for direct oral anticoagulant (DOAC) users on the left and for vitamin K antagonist (VKA) users on the right. F = females; M = males. For DOAC users, the comparison is shown between females (F, N = 23) and males (M, N = 25). The comparison for VKA users is shown on the right for 50 females and 26 males. The boxes represent the interquartile range (IQR), with the median shown as the horizontal line, whiskers extending to 1.5 × IQR, and dots indicating outliers. |
AKT - part B, designed to assess specific aspects of treatment understanding in patients treated with VKAs, yielded a mean ± SD score of 8.2 ± 2.3 indicating a generally good level of patient awareness regarding key aspects of their medication regimen. The maximum score of 10 was achieved by 22 out of 75 patients receiving VKA therapy who completed the questionnaire (29.3%). Females scored higher than males, however, this difference did not reach statistical significance.
TABS questionnaire showed a mean score (± SD) of adherence to therapy of 37.1 ± 2.7 (median =38), with the maximum score of 40 achieved by 26 out of 124 patients (21.0%). There was no significant difference between males and females. Patients treated with VKAs achieved significantly higher adherence scores than those receiving DOACs (37.5 ± 2.6, median =38 vs 36.5 ± 2.9, median = 37; p=0.0369, Mann–Whitney test) (Figure 2), with also a slightly higher percentage of perfect adherence answers among VKA patients (23.7%; 18 out of 76 patients) compared with DOAC patients (16.7%; 8 out of 48 patients).
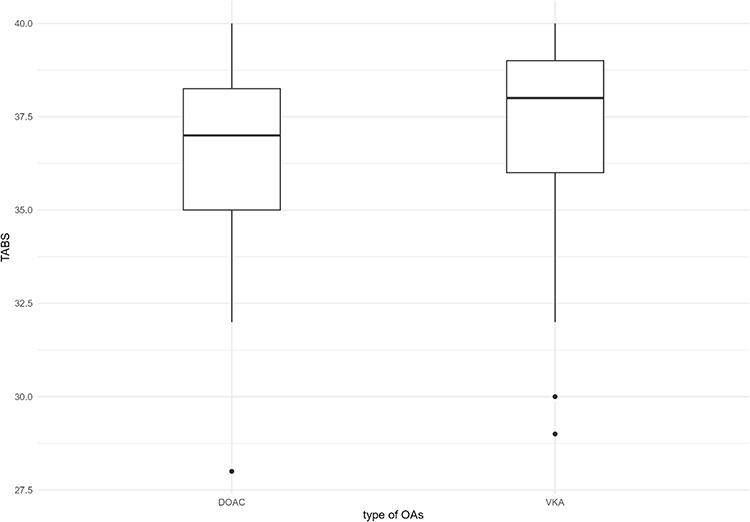 |
Figure 2 TABS scores by type of oral anticoagulant (OA). Notes: The TABS score distribution for direct oral anticoagulant (DOAC) and vitamin K antagonist (VKA) users are shown as boxplots, with the central line in each box representing the median, the box limits corresponding to the first (Q1) and third (Q3) quartiles. The whiskers extend to 1.5 × IQR, while the points beyond the whiskers are outliers. |
Correlation between the AKT and TABS assessed using Spearman’s test shows the presence of a weak but significant correlation. As the AKT result increases, TABS scores also increase (Spearman coefficient =0.190, p=0.035). This finding was more evident in the subgroup of patients taking DOACs, although the result was borderline with statistical significance (rs=0.280, p=0.053) (Figure 3). The multiple regression model that included the type of OAs and AKT- part A poorly but significantly predicted the TABS score (R2=0.077, p=0.008; TABS=33.09+0.88*OAs+0.15*AKT). Both the type of OAs (b=0.788, p=0.076) and AKT part A (b=0.145, p=0.015) contributed to improving the model. Table 2 shows the average results of the three separate questionnaires based on the drug taken by the patient. No significant differences were found in terms of adherence or knowledge among the different drugs within the same therapeutic class (VKAs or DOACs).
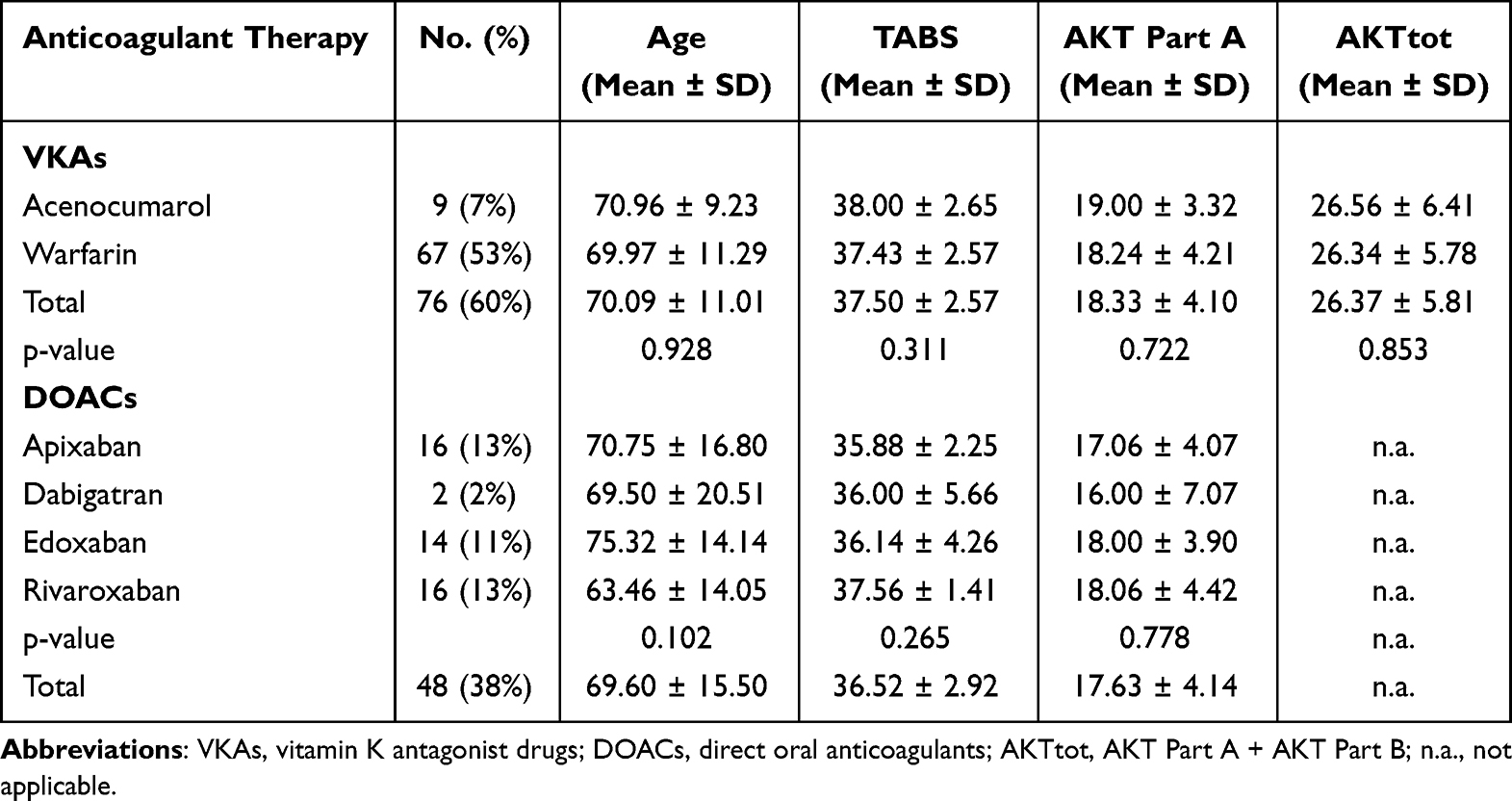 |
Table 2 Adherence and Knowledge Scores Broken Down by Type of Anticoagulant Medication |
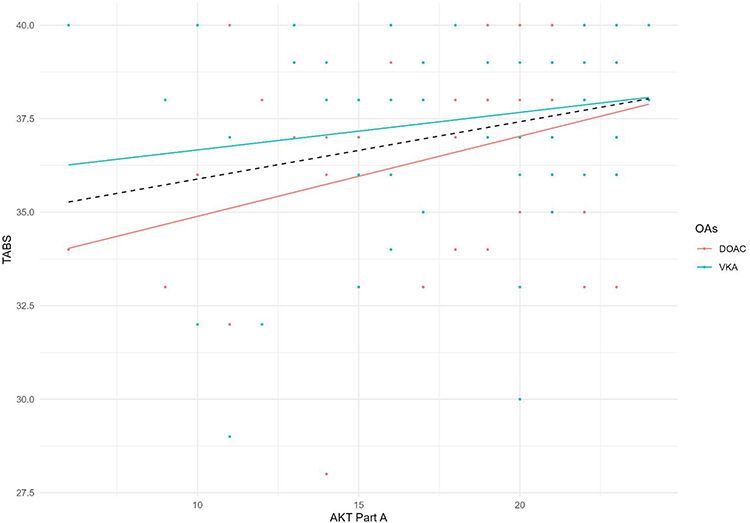 |
Figure 3 Scatterplot of the correlation between TABS and AKT Part A scores. Notes: The individual scores on the two variables are in dark-grey dot for direct oral anticoagulant (DOAC) users and in light-grey triangle for vitamin K antagonist (VKA) users. The positive association is shown by the simple regression lines; the dark-grey line is for DOAC users, the light grey for VKA users, and the dotted black line for the overall data. |
No significant differences were found in terms of adherence or knowledge regarding the different therapy used within the same category of drugs (VKAs or DOACs).
Since the patient’s recruitment was carried out in three centers belonging to two hospitals, the data were also analyzed based on the enrolling center: Thrombosis Center of the E.O. Ospedali Galliera of Genoa (TC-GH), anticoagulation clinics (AC) of the E.O. Ospedali Galliera (AC-GH) and IRCCS Ospedale Policlinico San Martino of Genoa (AC-SM), respectively. There was a significant difference between the results obtained on the AKT and TABS in the three centers (p=0.0037 and p<0.0001, respectively, Kruskal–Wallis test); the average scores were higher for patients treated at the AC-GH, lower at the TC-GH, and lowest at the AC-SM for both AKT and TABS (Table 3). These differences were mainly due to the difference between the two Galliera and the San Martino center, rather than between the two Galliera (AC vs TC).
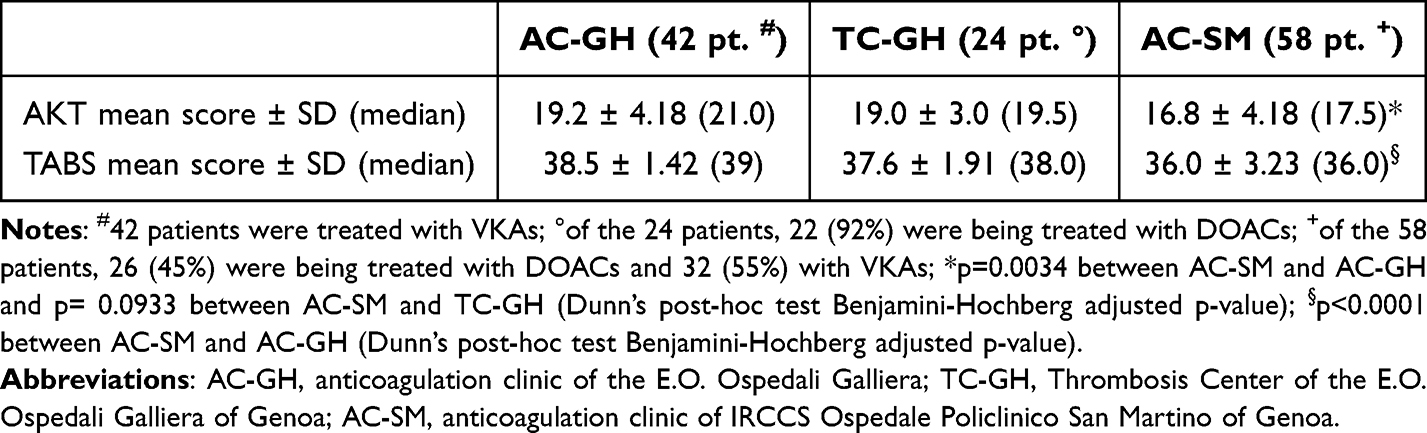 |
Table 3 AKT and TABS Results in the Three Hospital Centers |
The analysis conducted using a multiple regression model confirmed that AKT part A was influenced by both patient gender and recruitment center. Both variables were significant predictors in the model (b=1.793 and p=0.014 for gender; b=−1.097 and p=0.007 for the recruitment center), which overall explained 11.5% of the variation in AKT part A (p=0.001).
The three recruitment centers and the OAs treatment were collinear, as the two Ospedali Galliera’ s centers (GH) were specialized, with AC-GH patients all treated with VKAs and TC-GH patients mostly treated with DOACs (Table 3). However, patients at San Martino (SM) were equally treated with both OAs (VKA for 55% of patients), so that the type of OAs was no longer associated with Hospital, GH and SM, when centers were grouped at Hospital level, allowing both variables to be included in the regression model. This model confirmed the association of the hospitals but not of type of OAs, with AKT part A scores.
The scores obtained from the analysis of the EuroQol-5D-5L questionnaire by dimension and level are shown in Table 4. The overall utility score was 0.79 ± 0.28 (mean ± SD). Significant differences were found according to gender (0.75 in females, 0.84 in males, p=0.0351, Mann–Whitney test), education level (ranging from 0.54 with primary school to 0.89 with a university degree, p=0.0021, Kruskall-Wallis test), working occupation (p=0.0156, Kruskall-Wallis test), living alone (p=0.0410, Mann–Whitney test). The utility score was different also according to the different classes of and age (p=0.012 Kruskal–Wallis test), showing a decline after 80 years of age, in addition to a general negative correlation (rs= −0.274, p=0.0022). The utility score was slightly higher among patients receiving VKAs, although this difference was not statistically significant. No differences were found between the enrolling centers.
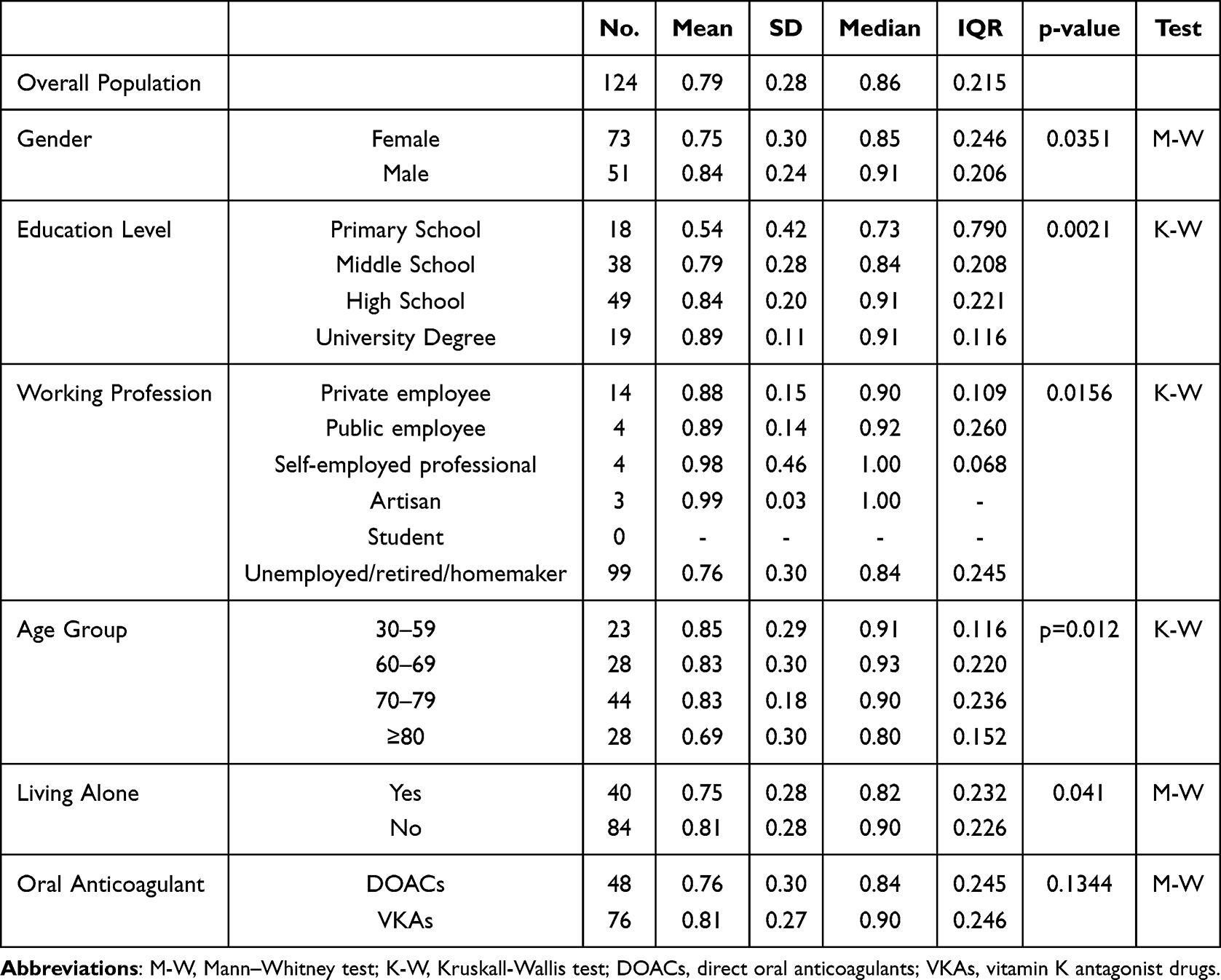 |
Table 4 EuroQol-5D-5L Questionnaire - Utility Score |
VAS score was 71.0 ± 16.86 (mean ± SD). No significant differences were observed according to gender (70.4 ± 17.11 and 71.8 ± 16.80 in females and males respectively, p=0.584, Mann–Whitney test). Education level showed an increasing trend, rising from 59.41 ± 21.06 with primary school to 75.72 ± 12.43 with a university degree (p=0.0411, Mann–Whitney test).
Adverse Events (AEs) monitoring revealed only three reported AEs: two in patients receiving VKAs (one male 79 years old, with scores of 40, 19, and 0.61 for TABS, AKT part A and EuroQol-5D-5L utility score respectively, and one female 51 years old, with scores of 30, 20, and 0.91 respectively) and one in a patient receiving DOAC therapy (male aged 93 years, with scores of 34, 18, and 0.77 for TABS, AKT part A and EuroQol-5D-5L utility score respectively).
Finally, we compared the TABS, AKT-part A and EuroQol-5D-5L scores between the first and second visits. Unfortunately, only 25 patients agreed to participate in the second study visit and completed the questionnaires again. In this group of patients, there was an increase in the AKT part A score (from 18.1 ± 4.1 (median = 19) to 21.7 ± 2.4 (median = 23), with a strong effect (Matched Rank-Biserial Correlation=0.91). Nonetheless, the very high attrition of 80% did not allow robust and not biased statistical tests.
In contrast, no relevant differences were observed in the TABS (from 37.1 ± 2.7 (median = 38) to 37.6 ± 2.1 (median = 38) or EuroQol-5D-5L (from 0.79 ± 0.28 (median = 0.86) to 0.80 ± 0.31 (median = 0.91) scores.
Discussion
Adherence to drug therapy is a fundamental issue in the management of patients undergoing chronic treatment. Chronic therapies impose a significant burden on patients, both in terms of organizational demands and psychological impact. Non-adherence to chronic therapy can lead to adverse events in cases of overdose and, conversely, to insufficient therapeutic coverage when medication is taken irregularly. It is currently estimated that less than 50% of the population undergoing chronic anticoagulant therapy is fully adherent to treatment.39 Several studies suggest that better knowledge of one’s disease and prescribed therapy can lead to improved treatment adherence. Another key factor that can promote adherence is the use of Patient Experience Data (PED), as reported in the literature. PEDs may not only promote adherence but also help identify possible causes of non-adherence.25 For these reasons, in our study, we assessed the level of knowledge and adherence among a group of outpatients undergoing chronic anticoagulation therapy for the prevention of thromboembolic events in order to investigate potential strategies to improve adherence and provide better support to patients receiving therapies that significantly affect their daily lives.
Due to the increasingly important role that PED plays in the evaluation of drug therapies, we considered the use of questionnaires to be a practical and cost-effective method for assessing patient adherence and knowledge. However, by definition, these tools are subjective, deriving, from data self-reported by patients/caregivers. To minimize the risks associated with the use of subjective measures, we used questionnaires that had previously been validated.
The literature shows that data on treatment adherence can vary greatly depending on whether they come from electronically reported measurements (44%) or patient-reported data (77%).40,41 Our results showed a moderate-to-high adherence rate of approximately 70%, which is consistent with data reported in the literature when adherence is assessed using patient-reported measures.
Since the primary endpoint was descriptive, no sample calculation was performed for the study. However, a sample size of 200 participants, estimated based on feasibility, would have been sufficient to achieve significance in finding small effects in the secondary objectives. Unfortunately, this number was not achieved, mainly due to a substantial loss to follow-up, with many patients unwilling to complete the questionnaires again at the time of the second visit. However, the sample size of 124 achieved for the cross-sectional endpoints was estimated at a sensitivity analysis to be enough to detect moderate effects. The longitudinal endpoints, instead, suffered from a very high drop in follow-up of 80%, in addition to the very reduced sample size. We believe that the addition of an extra commitment, such as that required by our study, which participation in a second questionnaire session, may have contributed to reduced patient participation in the follow-up visit. The patients who agreed to complete the questionnaires a second time may represent a subgroup of individuals who are more motivated and more engaged in their treatment, potentially introducing selection bias. In addition, given the observational nature of the study, the follow-up timeframes were dictated by clinical practice.42 This resulted in an imbalance in the follow-up intervals between the two patient groups (VKA and DOAC therapy). Undoubtedly, this temporal aspect, in addition to extreme attrition bias, made it difficult to evaluate the longitudinal effects of the therapeutic intervention; therefore, the improved knowledge scores that we detected after the educational session must be taken very cautiously as a mere exploratory result rather than confirmatory, possibly as hypothesis-generating for future trials. Treatment with OAs requires patients to follow a series of instructions that go beyond “simply” taking the medication. Whether patients are treated with VKAs or DOACs, they must follow certain behavioral recommendations. In particular, as widely known, patients on VKA therapy must also pay close attention to their diet to prevent the drug from falling outside the therapeutic range to drug-food-interactions. Although DOAC therapy requires less attention from the patient, the patient is still required to follow specific rules in order to achieve optimal anticoagulant coverage. In addition, the lack of mandatory close medical drug monitoring may expose patients receiving DOAC therapy to a greater risk of developing behaviors that compromise therapeutic coverage. Analysis of the results of our study on patients’ knowledge on OA therapy showed that patients generally had a good understanding of their treatment. Our results for the AKT questionnaire are consistent with other studies conducted in Europe and other countries.29,43 We also found that women had a statistically higher level of knowledge than men; this result was also observed among patients receiving VKA therapy. Patients appear to be more familiar with lifestyle aspects of therapy (eg, dietary restriction) than with more technical aspects of therapy, such as potential drug adverse effects) (data not shown). Our data show that patients taking VKAs are slightly more informed about their therapy than those taking DOACs. This difference may also reflect the fact that physicians tend to provide more detailed explanations when prescribing VKA therapy, given the need for careful management of interactions and monitoring. This finding underscores the need for prescribing physicians to pay greater attention to patients on DOAC therapy, with particular emphasis on educational information regarding the management of oral anticoagulant therapy, especially concerning the potential risks associated with the medication itself—particularly when taken incorrectly—and the risks of possible interactions with other substances or foods.
In several clinical centers, patients on VKA therapy are also provided with educational materials or small handbooks containing key rules or therapy management, which may further increase patient awareness of treatment. With regard to adherence to therapy, most patients in our study were found to be highly adherent according to the analysis of data obtained from the TABS questionnaire. Although questionnaire-based tools are relatively inexpensive and easy to administer, they rely on self-reported data and therefore may overestimate adherence compared with objective measurement methods. The assessment of adherence using a purely subjective method is a major limitation in our study, as the tool used is probably not effective in providing accurate data on patient adherence to oral anticoagulant therapy. In support of this assertion, the results of our study showed that both patient groups achieved excellent scores on the questionnaire as of the first administration, and it was not possible to demonstrate a significant improvement in adherence at follow-up. For this reason, future studies evaluating adherence to anticoagulant therapy may benefit from combining patient-reported tools with more objective methods, such as electronic monitoring or pharmacological measurements.
Analysis of our data also revealed only small differences in adherence according to the type of anticoagulant therapy used. In fact, even in this case, the patients with the best adherence were those on VKA therapy. This finding is consistent with the observation that these patients also demonstrated slightly higher levels of knowledge regarding their therapy, reinforcing the hypothesis that greater awareness and knowledge of the risks and benefits of therapy may lead to better adherence. Our analysis of the data showed also that patients attending the two centers at Galliera Hospital, a small hospital, scored better on both questionnaires than patients attending the San Martino Center, an IRCCS (Higher Institute for Research, Care and Assistance). This discrepancy could be explained by differences in organizational characteristics between the two hospitals. Patients attending smaller centers may benefit from longer consultation times and closer interaction with healthcare professionals, whereas centers with a higher patient turnover may have limited time available for each consultation. These findings suggest that the amount of time dedicated to patient education and communication may significantly influence patients’ understanding and management of chronic therapy for all those who need it. It is therefore clear that the time that can be dedicated to patients can significantly influence their approach to chronic therapy. Future studies could also collect data on the duration and content of visits, providing further information to better compare the management of patients on oral anticoagulant therapy in relation to the size of the clinical centre, and to test the hypothesis that the size of the clinical centre may influence patients’ adherence to treatment. If this hypothesis were to be confirmed, it would be important to consider a change in the management of patients on oral anticoagulant therapy within national policy.
Finally, in order to better assess the influence of anticoagulant therapy on the quality of life of the patients enrolled in the study, they were given a QoL questionnaire. A higher score was observed in men than in women, in patients with higher educational levels and in younger individuals. Being employed also seems to be associated with better perceived quality of life, as well as not living alone. The analysis of the data obtained from the EuroQoL-5D-5L questionnaire did not reveal any statistically significant correlations with the results of the other questionnaires administered in our study.
Conclusion
Our study revealed a generally good, but still not optimal, level of knowledge among patients receiving anticoagulant therapy. Patients who understand their medications and the reasons for their use seems to be more likely to adhere to prescribed regimens in agreement with literature. The exploratory results of our study suggest that the use of structured programs aimed at improving patient education regarding their therapy may help increase patients’ understanding of their treatment, thus their adherence and consequently, reduce the risks associated with inadequate management of anticoagulant therapy, including haemorrhagic or thrombotic complications.
Our findings suggest that there may be a positive association between knowledge and adherence; however, the tools used in the present study may not be sufficient to fully capture patient adherence behavior, and the use of more direct methods for measuring adherence should be considered in future research.
Further trials should explore personalized educational interventions in a larger patients’ population receiving anticoagulant therapy with additional use of Patient Experience Data, their impact on knowledge, adherence, and quality of life to confirm the positive longitudinal effects of the therapeutic intervention on patients’ adherence.
Data Sharing Statement
The clinical and laboratory data supporting this study’s findings are available from the corresponding author F.M. upon special request. The datasets generated or analyzed during the current study are not publicly available for ethical reasons per local guidelines.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Liguria Region - Territorial Ethics Committee (authorization nr. 387/2023). Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors are sincerely grateful to the patient for his/her participation in the present study and the precious help of the nursing staff.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heestermans M, Poenou G, Hamzeh-Cognasse H, Cognasse F, Bertoletti L. Anticoagulants: a short history, their mechanism of action, pharmacology, and indications. Cells. 2022;11(20):3214. doi:10.3390/CELLS11203214
2. AIFA - Ricerca Farmaco. Available from: https://medicinali.aifa.gov.it/it/#/it/dettaglio/0000004233.
3. Steffel J, Collins R, Antz M, et al. European heart rhythm association practical guide on the use of non-Vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. EP Europace. 2021;23(10):1612–14. doi:10.1093/EUROPACE/EUAB065
4. Nelson WW, Choi JC, Vanderpoel J, et al. Impact of Co-morbidities and patient characteristics on international normalized ratio control over time in patients with nonvalvular atrial fibrillation. Am J Cardiol. 2013;112(4):509–512. doi:10.1016/j.amjcard.2013.04.013
5. Orensky IA, Holdford DA. Predictors of noncompliance with warfarin therapy in an outpatient anticoagulation clinic. Pharmacother J Human Pharmacol Drug Ther. 2005;25(12):1801–1808. doi:10.1592/PHCO.2005.25.12.1801
6. Schein JR, White CM, Nelson WW, Kluger J, Mearns ES, Coleman CI. Vitamin K antagonist use: evidence of the difficulty of achieving and maintaining target INR range and subsequent consequences. Thromb J. 2016;14(1):1–10. doi:10.1186/S12959-016-0088-Y/TABLES/4
7. Mearns ES, Kohn CG, Song JS, et al. Meta-analysis to assess the quality of international normalized ratio control and associated outcomes in venous thromboembolism patients. Thromb Res. 2014;134(2):310–319. doi:10.1016/J.THROMRES.2014.05.035/ASSET/29DEE017-1F45-43A0-9254-94107B5CD448/MAIN.ASSETS/GR4.SML
8. Nelson WW, Wang L, Baser O, Damaraju CV, Schein JR. Out-of-range international normalized ratio values and healthcare cost among new warfarin patients with non-valvular atrial fibrillation. J Med Econ. 2015;18(5):333–340. doi:10.3111/13696998.2014.1001851
9. Eliquis | European Medicines Agency (EMA). Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/eliquis.
10. Lixiana | European Medicines Agency (EMA). Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/lixiana.
11. Rivaroxaban Viatris (previously Rivaroxaban Mylan) | european Medicines Agency (EMA). Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/rivaroxaban-viatris.
12. Pradaxa | European Medicines Agency (EMA). Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/pradaxa.
13. Chen A, Stecker E, Warden BA. Direct oral anticoagulant use: a practical guide to common clinical challenges. J Am Heart Assoc. 2020;9(13):17559. doi:10.1161/JAHA.120.017559/ASSET/9D03411E-2E57-44D7-81B6-4A6C6578E733/ASSETS/GRAPHIC/JAH35265-FIG-0003.PNG
14. Schwarb H, Tsakiris DA. New direct oral anticoagulants (DOAC) and their use today. Dentistry J. 2016;4(1):5. doi:10.3390/DJ4010005
15. Razouki Z, Ozonoff A, Zhao S, Jasuja GK, Rose AJ. Improving quality measurement for anticoagulation adding international normalized ratio variability to percent time in therapeutic range. Circ Cardiovasc Qual Outcomes. 2014;7(5):664–669. doi:10.1161/CIRCOUTCOMES.114.000804/-/DC1
16. Douxfils J, Adcock DM, Bates SM, et al. Update of the international council for standardization in haematology recommendations for laboratory measurement of direct oral anticoagulants. Thromb Haemost. 2021;121(8):1008–1020. doi:10.1055/A-1450-8178
17. AIFA: online il Rapporto OsMed 2023 “L’uso dei farmaci in Italia”. Available from: https://www.epicentro.iss.it/farmaci/rapporto-osmed-2023.
18. Potpara T, Markovic BG, Grygier M, et al. Adherence to oral thromboprophylaxis in atrial fibrillation: an overview for clinicians. Europace. 2025;27(11). doi:10.1093/EUROPACE/EUAF250
19. Rolls CA, Obamiro KO, Chalmers L, Bereznicki LRE. The relationship between knowledge, health literacy, and adherence among patients taking oral anticoagulants for stroke thromboprophylaxis in atrial fibrillation. Cardiovasc Ther. 2017;35(6). doi:10.1111/1755-5922.12304
20. Smet L, Heggermont WA, Goossens E, et al. Adherence, knowledge, and perception about oral anticoagulants in patients with atrial fibrillation at high risk for thromboembolic events after radiofrequency ablation在射频消融术后易患血栓的房颤患者中,对于口服抗凝血剂的依从性, 了解和认知的理解. J Adv Nurs. 2018;74(11):2577–2587. doi:10.1111/JAN.13780
21. Awwad O, Akour A, Al-Muhaissen S, Morisky D. The influence of patients’ knowledge on adherence to their chronic medications: a cross-sectional study in Jordan. Int J Clin Pharm. 2015;37(3):504–510. doi:10.1007/S11096-015-0086-3/TABLES/6
22. Sweileh WM, Zyoud SH, Abu Nab’A RJ, et al. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. BMC Public Health. 2014;14(1):1–8. doi:10.1186/1471-2458-14-94/TABLES/3
23. Najjar A, Amro Y, Kitaneh I, et al. Knowledge and adherence to medications among palestinian geriatrics living with chronic diseases in the west bank and East Jerusalem. PLoS One. 2015;10(6):e0129240. doi:10.1371/JOURNAL.PONE.0129240
24. Bertelsen N, Oehrlein E, Lewis B, et al. Patient engagement and patient experience data in regulatory review and health technology assessment: where are we today? Ther Innov Regul Sci. 2025;59(4):737–752. doi:10.1007/S43441-025-00770-6
25. Patient experience data (PED) reflection paper | european Medicines Agency (EMA). Available from: https://www.ema.europa.eu/en/patient-experience-data-ped-reflection-paper.
26. Europe WHOrganizationRO for. Therapeutic patient education: an introductory guide. Rev Infirm. 2023;2023(193):53–54.
27. Correia JC, Waqas A, Assal JP, et al. Effectiveness of therapeutic patient education interventions for chronic diseases: a systematic review and meta-analyses of randomized controlled trials. Front Med Lausanne. 2023;9. doi:10.3389/FMED.2022.996528
28. Dager WEBM, Rose AE, Rudd KM. Considerations in educating patients receiving oral anticoagulation: quality over quantity. Am J Health Syst Pharm. 2025;82(15):e723–e731. doi:10.1093/AJHP/ZXAF024
29. Magon A, Arrigoni C, Roveda T, et al. Anticoagulation knowledge tool (AKT): further evidence of validity in the Italian population. PLoS One. 2018;13(8):e0201476. doi:10.1371/JOURNAL.PONE.0201476
30. George J, Mackinnon A, Kong DCM, Stewart K. Development and validation of the Beliefs and Behaviour Questionnaire (BBQ). Patient Educ Couns. 2006;64(1–3):50–60. doi:10.1016/J.PEC.2005.11.010
31. Obamiro KO, Chalmers L, Bereznicki LRE. Development and validation of an oral anticoagulation knowledge tool (AKT). PLoS One. 2016;11(6):e0158071. doi:10.1371/JOURNAL.PONE.0158071
32. Feng YS, Kohlmann T, Janssen MF, Buchholz I. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res. 2021;30(3):647–673. doi:10.1007/S11136-020-02688-Y/FIGURES/4
33. Savoia E, Fantini MP, Pandolfi PP, Dallolio L, Collina N. Assessing the construct validity of the Italian version of the EQ-5D: preliminary results from a cross-sectional study in North Italy. Health Qual Life Outcomes. 2006;4(1):1–9. doi:10.1186/1477-7525-4-47/TABLES/3
34. Kalfoss M. Translation and adaption of questionnaires: a nursing challenge. SAGE Open Nurs. 2019;5. doi:10.1177/2377960818816810.
35. Colina S, Marrone N, Ingram M, Sánchez D. Translation quality assessment in health research: a functionalist alternative to back-translation. Eval Health Prof. 2017;40(3):267–293. doi:10.1177/0163278716648191
36. Magon A, Arrigoni C, Moia M, et al. Determinants of health-related quality of life: a cross-sectional investigation in physician-managed anticoagulated patients using Vitamin K antagonists. Health Qual Life Outcomes. 2020;18(1):1–9. doi:10.1186/S12955-020-01326-Y/TABLES/4
37. Finch AP, Meregaglia M, Ciani O, Roudijk B, Jommi C. An EQ-5D-5L value set for Italy using videoconferencing interviews and feasibility of a new mode of administration. Soc Sci Med. 2022;292:114519. doi:10.1016/J.SOCSCIMED.2021.114519
38. Xu RH, Sun R, Tian L, ling CAW, Wong EL. Health-related quality of life in primary care patients: a comparison between EQ-5D-5L utility score and EQ-visual analogue scale. Health Qual Life Outcomes. 2024;22(1):1–11. doi:10.1186/S12955-023-02215-W/TABLES/4
39. Hernandez I, He M, Chen N, Brooks MM, Saba S, Gellad WF. Trajectories of oral anticoagulation adherence among medicare beneficiaries newly diagnosed with atrial fibrillation. J Am Heart Assoc. 2019;8(12). doi:10.1161/JAHA.118.011427/SUPPL_FILE/JAH34200-SUP-0001-SUPINFO.PDF
40. Patel S, Huang M, Miliara S. Understanding treatment adherence in chronic diseases: challenges, consequences, and strategies for improvement. J Clin Med. 2025;14(17). doi:10.3390/JCM14176034
41. Louise Foley, James Larkin, Richard Lombard-Vance, et al. Correction: prevalence and predictors of medication non-adherence among people living with multimorbidity: a systematic review and meta-analysis. BMJ Open. 2022;12(7). doi:10.1136/BMJOPEN-2020-044987CORR1
42. Galliazzo S, Bucciarelli P, Barcellona D, et al. Practical suggestions for an optimal management of vitamin k antagonists: italian federation of centers for the diagnosis of thrombotic disorders and the surveillance of the antithrombotic therapies (FCSA) position paper. Thromb Haemost. 2024;124(8). doi:10.1055/S-0044-1782688
43. Alajami HN, Alshammari SA, Al-Dossari DS, et al. Knowledge of anticoagulation among saudi patients with atrial fibrillation: a cross-sectional study. Cureus. 2021;13(11). doi:10.7759/CUREUS.19237
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Best Evidence Summary of Home Enteral Tube Feeding Care Management in the Elderly
Zhu H, Liu A, Han Z, Yang Y, Ma X, Shi H
Patient Preference and Adherence 2025, 19:49-63
Published Date: 7 January 2025
Improving Medication Adherence and Lifestyle Changes: An Image-Based Educational Tool for Patients with Heart Failure
Gao L, Xie Q, Liu T, Liu H, Yan S, Han Y, Zhang M, Zhu D, Guo N, Nicholas S, Maitland E, Wang D
Patient Preference and Adherence 2025, 19:2251-2262
Published Date: 30 July 2025
A Comparative Cross-Sectional Study Between Gestational Diabetes Mellitus and Preeclampsia: Medication Adherence, Depression and Quality of Life
Noor R, Abbas G, Khurram H, Aslam A, Randhawa FA, Assiri A, Shah S
International Journal of Women's Health 2026, 18:565083
Published Date: 8 January 2026
A Patient Education Intervention to Address Allergic Anaphylaxis-Related Quality-of-Life and Self-Efficacy
Belin C, Tomori C
Journal of Asthma and Allergy 2026, 19:573932
Published Date: 13 February 2026