Back to Journals » Patient Preference and Adherence » Volume 19
Improving Medication Adherence and Lifestyle Changes: An Image-Based Educational Tool for Patients with Heart Failure
Authors Gao L ![]() , Xie Q, Liu T, Liu H, Yan S
, Xie Q, Liu T, Liu H, Yan S ![]() , Han Y, Zhang M, Zhu D, Guo N, Nicholas S
, Han Y, Zhang M, Zhu D, Guo N, Nicholas S ![]() , Maitland E, Wang D
, Maitland E, Wang D ![]()
Received 7 April 2025
Accepted for publication 23 July 2025
Published 30 July 2025 Volume 2025:19 Pages 2251—2262
DOI https://doi.org/10.2147/PPA.S530695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Lingyan Gao,1 Qing Xie,1 Tiantian Liu,1 Hua Liu,1 Suying Yan,1 Yalei Han,2 Meijing Zhang,2 Dawei Zhu,3 Na Guo,4 Stephen Nicholas,5,6 Elizabeth Maitland,7 Dongxiao Wang1
1Department of Pharmacy, Aerospace Center Hospital, Beijing, People’s Republic of China; 2Department of Cardiology, Aerospace Center Hospital, Beijing, People’s Republic of China; 3International Research Center for Medicinal Administration, Peking University, Beijing, People’s Republic of China; 4Department of Strategic Research, China Population and Development Research Center, Beijing, People’s Republic of China; 5Health Services Research and Workforce Innovation Centre, Newcastle Business School, University of Newcastle, Newcastle, NSW, Australia; 6Australian National Institute of Management and Commerce, 1 Central Avenue Australian Technology Park, Sydney, Australia; 7School of Management, University of Liverpool, Liverpool, UK
Correspondence: Dongxiao Wang, Department of Pharmacy, Aerospace Center Hospital, No. 15 Yuquan Road, Haidian District, Beijing, 100049, People’s Republic of China, Tel +86 13520109984, Email [email protected]
Background: A lack of disease-specific knowledge in heart failure (HF) patients is associated with poor adherence to complex medication regimens and non-pharmacological recommendations, especially among individuals with low health literacy. Existing educational tools have been shown to be inadequate, highlighting the need for more accessible and effective alternatives.
Purpose: To develop an educational tool that improves HF knowledge in a more accessible and effective way.
Methods: An image-based educational tool was created by healthcare professionals and HF patients, drawing on the Health Belief Model (HBM) and utilizing both qualitative and quantitative approaches. Project objectives were defined and content was guided by a literature review and focus group interviews. The tool was refined through iterative optimization using feedback and questionnaires.
Results: Thirteen healthcare professionals and eight HF patients participated in the development and refinement of the educational tool. The final tool consisted of seven A3-sized images and accompanying text, addressing the following topics: (1) Cognition of HF; (2) Cause and classification of HF; (3) Inducing factors and prevention of HF; (4)-(5) Medication treatments of HF; (6) Exercise and self-management of HF; (7) “We are on the same journey” - a supportive theme for HF patients. The final version of the tool demonstrated high accuracy, readability, usability, and overall satisfaction, with all categories receiving scores of ≥ 4.5 on a 5-point Likert scale.
Conclusion: The image-based educational tool, developed using HBM, effectively meets the needs of HF patients. It shows strong performance in terms of accuracy, readability, usability, and satisfaction, which may ultimately help improve adherence to both pharmacological treatments and non-pharmacological recommendations for HF management.
Keywords: patient education, image-based educational tool, patient engagement, heart failure, medication adherence, lifestyle changes
Introduction
Heart failure (HF) is a serious world-wide chronic cardiac disease characterized by high morbidity, hospitalization, and mortality, carrying a significant burden to families, the health system and society.1,2 Poor adherence to complex drug regimens and non-pharmacological recommendations, such as lifestyle modifications, low-sodium diets, restricted fluid intake, daily weighing, and regular exercise, is associated with a higher incidence of multimorbidity, intensive healthcare and death.3,4 Evidence suggests that most HF patients adhere to less than two-thirds of their prescribed medications5,6 and have low compliance with non-pharmacological guidelines, such as sodium restriction (43–70%),7,8 body weight monitoring (8.4–60%),8,9 and fluid restriction (23–73%).10,11
Lack of disease-specific knowledge in HF patients has been shown to be associated with poor adherence to medication and non-pharmacological treatments, particularly in individuals with low health literacy.12 Current educational interventions for HF patients include face-to-face communication,13 telephone follow-ups,14 printed materials such as flyers and books,15 and computer-based video resources.16 These approaches have been shown to have limited success in improving patients’ self-care behaviours. A meta-analysis found that the educational interventions helped to improve medication adherence, but not self-care, in HF patients.17
The current unsatisfactory education interventions for HF patients partly reflect the lack of suitable educational tools.12 First, the complexity of HF treatment and self-care often renders medical instructions and educational materials dense with specialized terminology, which can be challenging for patients to comprehend, even for those with well-developed language skills.18 Especially for the poorly or uneducated, medical instructions and educational materials can create a barrier to understanding and implementing treatment guidelines effectively. Second, healthcare professionals frequently underestimate the emotional distress and anxiety experienced by HF patients, which undermines patients’ confidence and self-efficacy in managing their condition.18,19 Finally, the traditional one-way delivery of health information limits patient engagement, reducing their ability to internalize and act on the guidance. Developing easy-to-understand and interactive educational tools addresses these challenges and improving adherence among HF patients. We develop such an easy-to-understand, interactive educational tool for HF patients.
Educational materials that incorporate visual aids can better communicate complex health information.20 A prominent example is Healthy Interactions’ Diabetes Conversation Maps (CM), developed in collaboration with the International Diabetes Federation.21,22 CM uses pictorial guides to convey health information, facilitating patients’ understanding of diabetes,23,24 improving medication adherence,25 promoting self-care,26 enhancing self-efficacy, and reducing disease-related distress.27 Despite its success in diabetes education, the CM tool has not been widely applied to other diseases.
The integration of CM-style tools with theory-driven methods to design effective educational interventions remains under explored. Behavioral change theories, such as the Health Belief Model (HBM), provide a framework for explaining and predicting health behaviors.28 The HBM identifies six key constructs that influence health behaviors: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.29 By incorporating these constructs, our “image dialogue” HF educational tool was designed to address the specific beliefs and motivators that drive HF patient behavior. Combining colorful, real-world visual representations with a narrative framework to convey essential knowledge about medication and disease management, the ultimate goal of our HF educational tool is to provide patients with a user-friendly resource that enables them to understand complex information to improve their medication adherence and self-management capabilities.
Methods
Study Design
We adopted an exploratory mixed methods approach, conducted in two distinct phases. In the first phase, a qualitative approach was used to identify the educational content based on the HBM. A preliminary sketch of the tool and accompanying language was then developed. In the second phase, the tool was refined and optimized using a combination of quantitative questionnaires and qualitative interviews.
Participants
In Phase 1, a focus group 1 “creative team” was assembled to advise on HF educational content. The creative team consisted of 13 healthcare professionals and 2 HF patients. The healthcare professionals included: five cardiologists (one chief physician, two deputy chief physicians, and two attending physicians; four from Aerospace Center Hospital and one from a community health center), three cardiovascular nurses (one deputy chief nurse and two supervising nurses; all from Aerospace Center Hospital) and five clinical pharmacists (one chief pharmacist, three deputy chief pharmacists, and one supervising pharmacist; four from three different tertiary hospitals and one from a community health center). For Phase 2, six additional HF patients joined the creative team to form focus group 2 to assist in refining the HF educational tool. An illustrator was also engaged to visually represent the ideas in the form of images. All participants completed a brief demographic survey before participating in the study.
Theoretical Framework
HBM is used in a wide range of health-related actions, including adherence and compliance to medical treatments, preventive and screening behaviors, self-management of chronic conditions, and health promotion and prevention of diseases.30 The basic elements and contents of HBM are shown in Table 1. HBM provides a comprehensive framework for understanding the psychological factors that influence health-related behaviors and its application in health education can contribute to the development of more effective interventions. Kam et al demonstrated that HBM-based health education in hypertensive patients effectively improved blood pressure control and medication adherence31 and Saffari et al showed HBM-based behavior modification program improved both lifestyle and clinical measures in patients with coronary heart disease (CHD).32 In patients with chronic obstructive pulmonary disease (COPD), a nursing intervention based on HBM increased patients’ health belief and self-efficacy in disease management, reduced dyspnoea, and improved exercise tolerance and activity of daily living.33 Guided by HBM, Bordes et al created an educational website on bone health that proved to be useful, helpful and able to raise awareness of bone health among prostate and breast cancer survivors.34
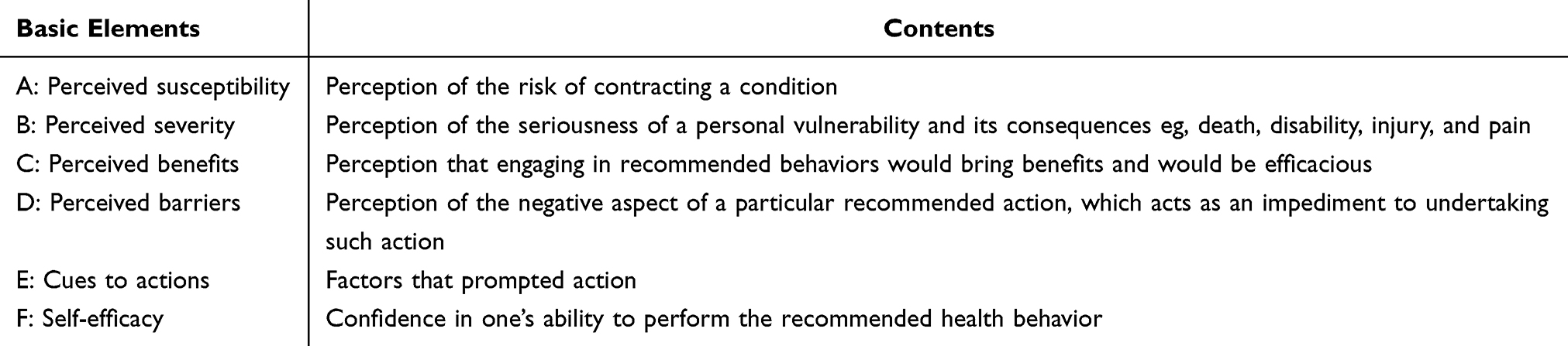 |
Table 1 The Basic Elements and Contents of HBM29 |
Research Procedure
Figure 1 shows Phase 1 involved developing the educational tool and Phase 2 improved the tool.
 |
Figure 1 The process of developing image-based educational tool. |
Development of Preliminary Image-Based Educational Tool
Literature Review
Using PubMed, Web of Science, China National Knowledge Infrastructure (CNKI), and Wanfang databases, a comprehensive literature review was conducted on educational tools for HF patients, including the keywords “heart failure”, “health education”, “patient compliance”, and “patient adherence”. Based on the literature review, the research team derived the relevant HF guidelines, which were then reviewed and assessed for content development.
Focus Groups
Moderated by a pharmacist in the research team, the 15 participants in the focus group 1 creation team scoped the HF educational content. Based on the literature review, the moderator summarized the key content of existing HF education materials and introduced the advantages of our educational tool. The focus group participants then shared their required HF educational content. Based on the HF literature review and HF participants’ needs, an open discussion identified the main content and specific items for the HF educational tool. To ensure all voices were heard, the moderator encouraged each participant to share their opinions, minimizing the influence of dominant participants. Participants received a RMB50 gift for their involvement.
The discussion was conducted in Mandarin, audio-recorded, and transcribed verbatim, with the data anonymized. The anonymized data were analyzed by 2 pharmacists from the team to finalize the content items two days after the discussion.
Development of Drafts
Based on the research team draft, the focus group moderator drew a preliminary sketch of the educational tool and a professional illustrator was then hired to refine the tool’s visual elements. Since misinterpretations can occur when cultural background factors can influence individuals’ interpretation of the images, an accompanying language description, informed by the focus groups discussions, was also developed.35 The whole research team approved the initial HF educational tool.
Improvement of the Image-Based HF Educational Tool
Focus group 2 comprised the original creative team focus group 1 team and six additional HF patients to evaluate the initial HF educational tool. Each participant received a one-to-one explanation of the image-based educational tool from a member of the research team.
Over three rounds of individual sessions, participants assessed the tool for accuracy, readability, usability, and overall satisfaction using a five-point Likert scale, with higher scores indicating greater performance in each category.36 During the one-to-one survey sessions, the clinical pharmacist interviewer also collected qualitative feedback on areas for improvement.
All interviews were audio-recorded and transcribed verbatim. The research team analyzed both the quantitative scores and qualitative feedback, identifying areas for refinement. Suggestions were conveyed to the illustrator for revisions, with iterative rounds between the research team and the illustrator leading to the final version of the educational tool.
The educational tool comprises seven A3-sized images paired with explanatory text (eFigures 1–7 in Supplementary material 1). It was designed to help HF patients better understand complex medication regimens and lifestyle modifications through the use of relatable imagery, vivid cartoons, a first-person narrative, and face-to-face communication.
Ethical Considerations
This study was approved by the Medical Ethics Committee of Aerospace Center Hospital (Approval No.2023(005)). Written informed consent was obtained from all participants, including permission for publication of anonymized responses and direct quotes.
Data Analysis
Descriptive statistics were calculated using Microsoft word 2017 software. Two authors independently coded the transcripts, resolving any discrepancies through discussion. Quantitative data were processed using SPSS 27 software, with continuous variables expressed as means and standard deviations ( ).
).
Results
Literature Review
A total of 244 English and 32 Chinese articles were reviewed, along with published HF guidelines from the American College of Cardiology,37 European Society of Cardiology,38 the Chinese Society of Cardiology,39 and Chinese Society of Rehabilitation Medicine.40 Common themes across the educational content emerged, comprising disease cognition (symptoms, classification, cause, and prevention of HF), medication treatments, and self-care practices (exercise, sodium restriction, weight monitoring, fluid management and alcohol restriction).
Demographics of the Participants
Thirteen healthcare professionals and eight HF patients participated in the development and refinement of the educational tool. The vast majority of healthcare professionals were between 30 and 50 years old (92.3%), with a bachelor degree or higher (92.3%). In terms of work experience, the proportions of medical staff with more than 10 years was 38.5%; 46.2% had 5–10 years’ experience and 15.4% had less than 5 years’ experience. The vast majority of patients were over 50 years old (87.5%) and had a specialist degree or below (87.5%). Regarding the duration of HF, the proportions of patients with more than 10 years was 25%; 37.5% had 5–10 years’ HF duration; and 37.5% had less than 5 years’ HF duration. Detailed participant demographics are provided in Table 2.
 |
Table 2 Demographic Characteristics of Participants |
Development of Core Educational Content for HF Patients
Based on the literature review and focus group 1 creative team discussions, the educational content was divided into three categories and 20 subcategories. As shown in Table 3, the three categorized comprised cognition of HF: specifically symptoms, grading, cause, trigger and prevention of HF; medication treatments of HF: specifically the pharmacological effect, adverse reactions, and monitoring indicator of 8 types of drugs (eg, RASI, beta-blockers, diuretics, digoxin); and HF exercise and management of HF: specifically exercise, fluid management, dietary guidance, lifestyle advice, psychological support, and follow-up.
 |
Table 3 Content of the Educational Tool |
Development of Preliminary Image-Based Educational Tool
Based on HBM and focus group 1, a draft of an educational tool, presented in eFigures 8–13 in Supplementary material 1, was developed, comprising six A3-sized colour images, covering (1) Cognition of HF; (2) Causes and classification of HF; (3) Inducing factors and prevention of HF; (4) Medication treatments of HF; (5) Exercise and self-management of HF; (6) “We are together” – a supportive message for HF patients.
Improvement of Image-Based Educational Tool
Quantitative Results from Questionnaires
Using focus group 2, three sections were selected for detailed critical analysis: cognition of HF, medication treatment of HF, and self-care management. As shown in Table 4, in the first round of testing, scores ranged from 2.4±0.8 to 3.4±0.5, reflecting suboptimal scores for accuracy, readability, usability, and satisfaction, especially in the medication treatment section. By the third round, all categories scored ≥4.5 points, indicating high levels of accuracy, readability, usability, and satisfaction.
 |
Table 4 Focus Group 2 Evaluation of the Educational Tool |
Qualitative Results from Interviews
Revisions were undertaken using focus group 2’s 26 qualitative comments, comprising 5 on recognition of HF, 13 on drug treatment of HF and 8 on management of HF. eTable 1 in Supplementary material 1 shows detailed entries.
Development of Final Draft of the Educational Tool
Presented in eFigures 1–7 in Supplementary material 1, the final educational tool consisted of seven A3-sized images. eFigure 1 compares the heart to a pump, illustrating its structure and function. This analogy helps patients grasp the symptoms and underlying mechanisms of HF. eFigure 2 highlights various diseases that can lead to HF, emphasizing the importance of managing primary conditions to prevent HF progression. eFigure 3 identifies common daily life factors that can trigger HF episodes and provides corresponding preventive measures. eFigures 4 and 5 use simple, engaging cartoons to explain the operation and benefits of eight key HF medications, aiming to strengthen patients’ intrinsic motivation to adhere to treatment. Adverse effects and precautions associated with these medications are also clearly outlined. eFigure 6 offers targeted guidance on self-care strategies, including effective exercise routines, fluid management, and dietary recommendations tailored to HF patients. eFigure 7 likens the HF journey to a shared expedition, portraying patients, healthcare professionals, family, and friends as allies working together to overcome challenges.
The following section provides a detailed examination of how the key elements of HBM are integrated into the design of the educational tool.
A: Perceived Susceptibility
To provide patients a more comprehensive understanding of HF, perceived susceptibility in HBM, shown in Table 1, theory section, was explained in eFigures 1–3. By using vivid language and images to contrast the characteristics of a normal heart with a HF heart, the possible symptoms of HF, such as chest tightness, edema and fatigue, are depicted and contrasted with normal behavior, involving exercise and sleep. The left hand side of eFigure 2 shows the causes of HF, alerting potential HF patients to identify, prevent and manage HF. The left hand side of eFigure 3 shows factors such as infections, excessive salt and fluid intake, and the arbitrary discontinuation of medication that trigger HF episodes in daily life, so that HF patients take routine precautions which include getting vaccinated on time, adhering to a low-salt diet, avoiding overexertion, and taking medication as prescribed (right hand side of eFigure 3).
B: Perceived Severity
The right hand side of eFigure 2 shows how HBM perceived severity in Table 1 can be depicted. The severity of HF is progressive, increasing from stage I to stage IV. When HF is not actively managed, patients may become unable to perform even the most basic daily activities, such as eating and sleeping.
C: Perceived Benefits
To prevent HF attacks, it is essential that patients perceive the benefits of regular exercise, taking medication, managing low-salt diets, and adhering to fluid restrictions. eFigures 4–6 depict the HBM perceived benefits in Table 1. For medication adherence, easy-to-understand cartoons are used to explain how medicines work and the long-term benefits of taking them in eFigures 4–6 shows that adherence to exercise improves HF patients’ quality of life. A low-sodium diet reduces the risk of excess water in the body, which can prevent HF attacks. Keeping blood pressure and heart rate under control, controlling body weight, quitting smoking and limiting alcohol, and maintaining a healthy lifestyle are shown to control HF in eFigure 6.
D: Perceived Barriers
eFigure 6 shows how HBM perceived barriers in Table 1 can be depicted. Exercise adherence can be difficult for HF patients, illustrating how starting with a few minutes can be gradually extended in duration. Various types of exercise, such as walking, Tai Chi, baduanjin, dancing and cycling, are correlated with patients’ physical condition, and hobbies are also shown. Adherence to daily record of fluid intake and output may be difficult for HF patients. eFigure 6 guides HF patients to measure their weight on an empty stomach after urinating early in the morning to keep weight within their target range.
E and F: Cues to Action and Self-Efficacy
eFigure 7 shows how HBM cues to action and self-efficacy in Table 1 are depicted. With the encouragement from doctors, nurses and pharmacists, and support from family and friends, “We are on the Same Journey” addresses patients’ negative emotions, to improve their confidence in managing their disease.
The HF educational tool provides a clear path forward to attenuating HF: recognising symptoms, taking preventive measures, eating a low-salt diet, taking medication and avoiding overexertion. While the educational tool was originally designed for older people with poor comprehension and low health literacy, we also provided in Supplementary material 1 an accompanying language text developed by healthcare professionals.
Discussion
Based on HBM, the development of the image-based HF educational tool involved a collaboration between multi-disciplinary healthcare professionals and HF patients. Through a combination of qualitative (focus group interviews and feedback) and quantitative (questionnaires) methods, the educational tool visualises HF information, which can be adapted for different populations, with different educational backgrounds, ethnicities and health literacy.
Our HF educational tool addresses two major hurdles: health-care providers do not have time or resources to deliver HF education and the complexity of HF treatment and self-care makes it challenging for patients to fully comprehend the information provided in routine doctor-patient interactions. To address these challenges, a pictorial series was chosen as an effective, simple and practical intervention. Using images closely related to the lives of the elderly can markedly increase attention and recall of health education information, especially for patients with low health literacy.18 Second, the use of exaggerated images, such as cartoon formats, can assist in enhancing patients’ comprehension of medical terminology.41 Third, the educational tool’s first-person narrative framework allows a close relationship between professional HF information and patients’ understanding of HF.42
Pictographic interventions need to be carefully developed and validated with both the targeted patient population and the clinical experts.35 Our educational tool directly involved HF patients from different age, disease stage and education level demographics and was continuously refined based on feedback from both healthcare professionals and HF patients. Using HBM as the organizing context, the content of our HF educational tool is divided into three key sections: disease knowledge, medication treatment, and self-care management. Each section posed challenges that were resolved through professional health experts and HF patient collaboration.
Section 1: Disease Knowledge
Knowledge plays an essential role in the promotion of self-care behaviours, especially for HF patients.12 Many HF patients, including those with a long history of HF disease, lack a comprehension of the disease and its associated symptoms,17 which is a major cause of high readmission rates.43 Providing patients with an understanding the heart’s structure and function can assist in the recognition of associated HF symptoms. When designing our educational tools, the introduction of “enlarged heart”, “weaker pumping function”, “less blood returning to the heart”, and “more blood remaining in the periphery (such as the lungs, liver, and lower extremities)” helps patients to better understand the causes and symptoms of shortness of breath, bloating, and lower extremity edema that occur during HF. The educational tool was validated by our expert creative team. For example, Doctor A stated:
The tool effectively demonstrates the distinguishing characteristics between a normal heart and a failing heart through the utilisation of images. When introducing knowledge about HF to patients, we inevitably use technical terminology which is more accurate and familiar to us. However, this may not be readily comprehensible to patients. We are also considering whether we can adopt a patient-friendly visual aids, such as images or simple heart models, with the objective of facilitating patient comprehension of intricate disease-related information. However, this requires a lot of time and effort, and it is very difficult.
Section 2: Medication Treatment
Patient understanding of the exact usage and dosage of their medications is key to HF prevention and treatment. A significant proportion of HF patients (87.5%) asserted that a comprehensive understanding of how their prescribed medication works to combat their illness was a crucial factor in maintaining long-term adherence to treatment.44 During the interviews, some HF patients (n=3) revealed the reason they stopped taking their medication was their belief that the medication prescribed by their doctor could not treat their disease. To combat HF drug misunderstandings, we expressed how HF drugs worked and their long-term benefits in a slightly exaggerated comic format with narrative language. This easy-to-understand and engaging approach promoted HF patients’ desire to take their medication and long-term medication compliance. For example, Patient A stated:
This image-based tool, combined with your explanation, is extremely vivid. I have had HF for seven years, and this is the first time anyone has explained the drug treatments clearly. I have always wanted to know how the medication I am taking treats HF. The doctor told me to take spironolactone, so I googled it and found out that it is a diuretic. But I did not urinate much even after taking it, so I stopped taking it. As a result, I was hospitalized for congestive HF. After communicating with you, I realized that the effect of spironolactone is not only diuresis, but also heart protection. I will never stop taking it!
An unexpected finding was that medical staff, especially nurses and non-cardiovascular pharmacists, in our creative team also showed a keen interest in the way HF drugs worked. We found that some of the focus group 1 medical creative team were unfamiliar with the latest developments in HF drugs, looking up the drug use instructions when faced with HF patient questions. These slightly exaggerated cartoons also help healthcare professionals to better understand how HF drugs work.
Section 3: Self-Care Management
Identifying barriers to self-care management in HF patients is a key attribute of our HF educational tool. For example, patients are told to limit salt in their diet to no more than 6g per day, but do not know how to achieve this goal. eFigure 6 in our educational tool uses beer bottle caps, a common object in everyday life, to visually represent the amount of salt needed per day. Similarly, eFigure 6 also shows that a simple method to limit daily fluid intake is to weigh yourself every morning to keep your weight within the target range. Told to exercise moderately, HF patients frequently fail to adhere to an exercise routine. Our educational tool in eFigure 6 illustrates with cartoon characters specific exercise routines with practical and easy to follow instruction appropriate to HF patients’ physical condition. For example, Patient E stated:
I thought heart failure meant the heart couldn’t beat anymore, so I definitely assumed it was impossible to exercise! Through this tool, I learned that exercise is still necessary for HF, which can improve heart function and enhance quality of life! And there are many ways to exercise. My body is still relatively weak, so I will first practice Tai Chi and respiratory muscle exercises at home, and then choose to walk or ride a bicycle when I am very well.
Simply distributing our HF educational tool directly to patients is not effective. First, our HF educational tool was designed for the elderly. Considering the decline in their visual and comprehension abilities, we do not use too much textual annotation, which inevitably affects the readability of the tool. Second, the extensive use of images can help people understand difficult technical knowledge, but it may also increase ambiguity, as images are more open to subjective interpretation compared to text. To address this limitation, we designed a supporting language. Also, only through interactive communication between medical staff and patients can we ensure that patients fully understand the content of the HF educational tool in a timely manner.
There are several other limitations. A randomized controlled trial is underway to validate long-term effects of using our educational tool in improving knowledge, medication adherence, non-pharmacological adherence, self-efficacy, and quality of life for HF patients. Second, our HF educational tool requires face-to-face communication between pharmacists and patients, which may hinder its promotion to a wider range of HF populations. We are exploring how our educational tool could be further optimized by developing a video format. Third, the current educational tool focuses primarily on HF-specific medications and does not address the challenges of managing complex polypharmacy regimens. Future research will aim to expand the tool to include comprehensive medication management for HF patients with multiple comorbidities.
Conclusion
Based on the Health Belief Model, our image-based HF educational tool was rated as accurate, readable, usable, and high satisfactory by HF patients and healthcare professionals. A randomized controlled trial (RCT) is being undertaken to validate the long-term benefits of this intervention in improving knowledge, medication adherence, and quality of life for HF patients.
Acknowledgments
The authors would like to thank all the healthcare professionals and patients interviewed by this study, and the Beijing Pharmaceutical Association, China funded this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Beijing Pharmaceutical Association, China [grant numbers LCYX-2022-21].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2023;118(17):3272–3287. doi:10.1093/cvr/cvac013
2. Greene SJ, Fonarow GC, Vaduganathan M, Khan SS, Butler J, Gheorghiade M. The vulnerable phase after hospitalization for heart failure. Nat Rev Cardiol. 2015;12(4):220–229. doi:10.1038/nrcardio.2015.14
3. Murray MD, Tu W, Wu J, Morrow D, Smith F, Brater DC. Factors associated with exacerbation of heart failure include treatment adherence and health literacy skills. Clin Pharmacol Ther. 2009;85(6):651–658. doi:10.1038/clpt.2009.7
4. van der Wal MH, Jaarsma T, van Veldhuisen DJ. Non-compliance in patients with heart failure; how can we manage it? Eur J Heart Fail. 2005;7(1):5–17. doi:10.1016/j.ejheart.2004.04.007
5. Chang LL, Xu H, DeVore AD, et al. Timing of postdischarge follow-up and medication adherence among patients with heart failure. J Am Heart Assoc. 2018;7(7):e007998. doi:10.1161/JAHA.117.007998
6. Qin X, Hung J, Teng TK, Briffa T, Sanfilippo FM. Long-term adherence to renin-angiotensin system inhibitors and beta-blockers after heart failure hospitalization in senior patients. J Cardiovasc Pharmacol Ther. 2020;25(6):531–540. doi:10.1177/1074248420931617
7. Artinian NT, Magnan M, Sloan M, Lange MP. Self-care behaviors among patients with heart failure. Heart Lung. 2002;31(3):161–172. doi:10.1067/mhl.2002.123672
8. Marti CN, Georgiopoulou VV, Giamouzis G, et al. Patient-reported selective adherence to heart failure self-care recommendations: a prospective cohort study: the Atlanta Cardiomyopathy Consortium. Congest Heart Fail. 2013;19(1):16–24. doi:10.1111/j.1751-7133.2012.00308.x
9. Seid MA, Abdela OA, Zeleke EG. Adherence to self-care recommendations and associated factors among adult heart failure patients. From the patients’ point of view. PLoS One. 2019;14(2):e0211768. doi:10.1371/journal.pone.0211768
10. Jaarsma T, Abu-Saad HH, Dracup K, Halfens R. Self-care behaviour of patients with heart failure. Scand J Caring Sci. 2000;14(2):112–119.
11. van der Wal MH, Jaarsma T, Moser DK, Veeger NJGM, van Gilst WH, van Veldhuisen DJ. Compliance in heart failure patients: the importance of knowledge and beliefs. Eur Heart J. 2006;27(4):434–440. doi:10.1093/eurheartj/ehi603
12. Swiatoniowska-Lonc NA, Slawuta A, Dudek K, Jankowska K, Jankowska-Polańska BK. The impact of health education on treatment outcomes in heart failure patients. Adv Clin Exp Med. 2020;29(4):481–492. doi:10.17219/acem/115079
13. Navidian A, Mobaraki H, Shakiba M. The effect of education through motivational interviewing compared with conventional education on self-care behaviors in heart failure patients with depression. Patient Educ Couns. 2017;100(8):1499–1504. doi:10.1016/j.pec.2017.02.023
14. Boyne JJ, Vrijhoef HJ, Spreeuwenberg M, Weerd GD, Kragten J, Gorgels APM. Effects of tailored telemonitoring on heart failure patients’ knowledge, self-care, self-efficacy and adherence: a randomized controlled trial. Eur J Cardiovasc Nurs. 2014;13(3):243–252. doi:10.1177/1474515113487464
15. Hany A, Fadlila R, Lydia EP. The influence of reminder book to adherence of heart failure patients in Malang city. J Public Health Res. 2021;10(2):2158. doi:10.4081/jphr.2021.2158
16. Strömberg A, Dahlström U, Fridlund B. Computer-based education for patients with chronic heart failure. A randomised, controlled, multicentre trial of the effects on knowledge, compliance and quality of life. Patient Educ Couns. 2006;64(1–3):128–135. doi:10.1016/j.pec.2005.12.007
17. Tinoco J, Figueiredo L, Flores PVP, Padua BLR, Mesquita ET, Cavalcanti ACD. Effectiveness of health education in the self-care and adherence of patients with heart failure: a meta-analysis. Rev Lat Am Enfermagem. 2021;29:e3389.
18. Houts PS, Doak CC, Doak LG, Loscalzo MJ. The role of pictures in improving health communication: a review of research on attention, comprehension, recall, and adherence. Patient Educ Couns. 2006;61(2):173–190. doi:10.1016/j.pec.2005.05.004
19. Jia Z, Du X, Du J, et al. Prevalence and factors associated with depressive and anxiety symptoms in a Chinese population with and without cardiovascular diseases. J Affect Disord. 2021;286:241–247. doi:10.1016/j.jad.2021.02.006
20. Tiwari RR, Pandey B, Chaudhari KS. Image-based communication for strengthening patient health education in rural and underserved settings. Cureus. 2023;15(7):e41279. doi:10.7759/cureus.41279
21. Yang Q, Fang P. Impact of the conversation map tools in patients with type 2 diabetes mellitus: a PRISMA-compliant meta-analysis of randomized controlled trials. Medicine. 2016;95(40):e4664. doi:10.1097/MD.0000000000004664
22. Cardoso AF, Cardoso D, Felizardo H, et al. Effectiveness of educational programs using Diabetes Conversation Map tools on the health outcomes of people with type 2 diabetes: a systematic review protocol. JBI Evid Synth. 2021;19(5):1140–1147. doi:10.11124/JBIES-20-00144
23. Penalba M, Moreno L, Cobo A, et al. Impact of the «Conversation Map™» tools on understanding of diabetes by Spanish patients with type 2 diabetes mellitus: a randomized, comparative study. Endocrinol Nutr. 2014;61(10):505–515. doi:10.1016/j.endonu.2014.06.001
24. Defeudis G, Khazrai YM, Di Rosa C, et al. Conversation Maps™, an effective tool for the management of males and females with type 2 diabetes and mildly impaired glycemic control. Hormones. 2018;17(1):113–117. doi:10.1007/s42000-018-0005-9
25. Srulovici E, Leventer-Roberts M, Curtis B, et al. Long-term effectiveness of the Diabetes Conversation Map™ Program on health outcomes: a case-control retrospective cohort study. J Adv Nurs. 2020;76(9):2299–2310. doi:10.1111/jan.14439
26. Yang YS, Wu YC, Lu YL, et al. Adherence to self-care behavior and glycemic effects using structured education. J Diabetes Investig. 2015;6(6):662–669. doi:10.1111/jdi.12343
27. Li F, Yao P, Hsue C, Xu J, Lou Q. Impact of “Conversation Maps” on diabetes distress and self-efficacy of Chinese adult patients with type 2 diabetes: a pilot study. Patient Prefer Adher. 2016;10:901–908. doi:10.2147/PPA.S95449
28. Movahed E, Rezaee MM, Jadgal MS, Zareipour M, Azari MT. Effectiveness of the application of an educational program based on the Health Belief Model (HBM) in adopting. Invest Educ Enferm. 2022;40(3):e11. doi:10.17533/udea.iee.v40n3e11
29. Ullah F, Ragazzoni L, Hubloue I, Barone-Adesi F, Valente M. The use of the Health Belief Model in the context of heatwaves research: a rapid review. Disaster Med Public Health Prep. 2024;18:e34.
30. Alamer AS. Behavior change theories and models within health belief model research: a five-decade holistic bibliometric analysis. Cureus. 2024;16(6):e63143. doi:10.7759/cureus.63143
31. Kam BS, Lee SY. Integrating the health belief model into health education programs in a clinical setting. World J Clin Cases. 2024;12(33):6660–6663. doi:10.12998/wjcc.v12.i33.6660
32. Saffari M, Sanaeinasab H, Rashidi-Jahan H, et al. An intervention program using the health belief model to modify lifestyle in coronary heart disease: randomized controlled trial. Int J Behav Med. 2024;31(4):631–641. doi:10.1007/s12529-023-10201-1
33. Wang Y, Zang XY, Bai J, et al. Effect of a Health Belief Model-based nursing intervention on Chinese patients with moderate to severe chronic obstructive pulmonary disease: a randomised controlled trial. J Clin Nurs. 2014;23(9–10):1342–1353. doi:10.1111/jocn.12394
34. Des Bordes JKA, Suarez-Almazor ME, Volk RJ, Lu H, Edwards B, Lopez-Olivo MA. Online educational tool to promote bone health in cancer survivors. J Health Commun. 2017;22(10):808–817. doi:10.1080/10810730.2017.1360415
35. Wang T, Voss JG. Effectiveness of pictographs in improving patient education outcomes: a systematic review. Health Educ Res. 2021;36(1):9–40. doi:10.1093/her/cyaa046
36. Kim S, Ju MK, Son S, Jun S, Lee SY, Han CS. Development of video-based educational materials for kidney-transplant patients. PLoS One. 2020;15(8):e0236750. doi:10.1371/journal.pone.0236750
37. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2022;145(18):e895–e1032. doi:10.1161/CIR.0000000000001063
38. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
39. Heart Failure Group of Chinese Society of Cardiology of Chinese Medical Association. Chinese Heart Failure Association of Chinese Medical Doctor Association, Editorial Board of Chinese Journal of Cardiology. Chinese guidelines for the diagnosis and treatment of heart failure 2018. Chin J Cardiol. 2018;46(10):760–789.
40. Cardiovascular Disease Prevention and Rehabilitation Professional Committee of the Chinese Association Rehabilitation Medicine. Expert consensus on cardiac rehabilitation for chronic heart failure in China. Chin J Intern Med. 2020;59(12):942–952.
41. Brand A, Gao L, Hamann A, et al. Medical graphic narratives to improve patient comprehension and periprocedural anxiety before coronary angiography and percutaneous coronary intervention: a randomized trial. Ann Intern Med. 2019;170(8):579–581. doi:10.7326/M18-2976
42. Winterbottom A, Bekker HL, Conner M, Mooney A. Does narrative information bias individual’s decision making? A systematic review. Soc Sci Med. 2008;67(12):2079–2088. doi:10.1016/j.socscimed.2008.09.037
43. Lee CS, Bidwell JT, Paturzo M, et al. Patterns of self-care and clinical events in a cohort of adults with heart failure: 1 year follow-up. Heart Lung. 2018;47(1):40–46. doi:10.1016/j.hrtlng.2017.09.004
44. Ebrahimabadi M, Rezaei K, Moini A, Fournier A, Abedi A. Infographics or video; which one is more effective in asthmatic patients’ health? A randomized clinical trial. J Asthma. 2019;56(12):1306–1313. doi:10.1080/02770903.2018.1536143
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Its Associated Factors Among Outpatients with Heart Failure
Jarab AS, Al-Qerem WA, Hamam HW, Alzoubi KH, Abu Heshmeh SR, Mukattash TL, Alefishat E
Patient Preference and Adherence 2023, 17:1209-1220
Published Date: 8 May 2023
Advanced Practice Nurse–Led Cardiogeriatric Heart Failure Pathways: A Narrative, Practice-Based Description of an Integrated Care Model
Esser R, Farges C, Esteban M, Larbaneix M, Mondragon A, Nisse Durgeat S, Maurou O, Harboun M
Journal of Multidisciplinary Healthcare 2026, 19:599213
Published Date: 16 April 2026