Back to Journals » Clinical Ophthalmology » Volume 17
Reduced Size of Telangiectatic Capillaries After Intravitreal Injection of Anti-Vascular Endothelial Growth Factor Agents in Diabetic Macular Edema
Authors Itou J, Furushima K, Haruta M ![]() , Kato N
, Kato N ![]() , Arai R, Mori K, Ishikawa K, Yoshida S
, Arai R, Mori K, Ishikawa K, Yoshida S ![]()
Received 19 October 2022
Accepted for publication 6 December 2022
Published 19 January 2023 Volume 2023:17 Pages 239—245
DOI https://doi.org/10.2147/OPTH.S393360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Junichi Itou,1,* Kei Furushima,1,* Masatoshi Haruta,1 Nobuhiro Kato,1 Rikki Arai,1 Kenichiro Mori,2 Keijiro Ishikawa,2 Shigeo Yoshida1
1Department of Ophthalmology, Kurume University School of Medicine, Kurume, Japan; 2Department of Ophthalmology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan
*These authors contributed equally to this work
Correspondence: Shigeo Yoshida, Department of Ophthalmology, Kurume University School of Medicine, 67 Asahi-machi, Kurume, Fukuoka, 830-0011, Japan, Tel +81-942-317574, Fax +81-942-370324, Email [email protected]
Purpose: Intravitreal injection of anti-vascular endothelial growth factor (anti-VEGF) agents reduces microaneurysms in patients with diabetic macular edema (DME). However, residual anti-VEGF-resistant telangiectatic capillaries (TelCaps) have been reported. In this study, we investigated changes in the size of TelCaps after intravitreal injection of anti-VEGF agents in DME.
Patients and Methods: Indocyanine green angiography (IA) and optical coherence tomography were performed before and 3 months after the intravitreal injection of anti-VEGF agents (pro re nata regimen after three monthly loading doses) in 12 eyes of 12 patients (7 males and 5 females, mean age 65.2 ± 8.8 years) with DME. The number and size of TelCaps within a 6-mm diameter macular region of the edema were measured using optical coherence tomography B-scan images overlaid on IA images.
Results: There were significant reductions in the number and size of TelCaps between the baseline and 3 months after anti-VEGF agent administration (P < 0.05 and P < 0.0001, respectively). The maximum corrected visual acuity (logMAR visual acuity) and the central macular thickness after anti-VEGF therapy were significantly improved (P < 0.01 and P < 0.02, respectively). The TelCaps remaining after loading three consecutive anti-VEGF agents had a significantly larger mean size at baseline than the TelCaps that resolved after the treatment (P < 0.03).
Conclusion: Our study demonstrated that intravitreal injection of anti-VEGF agents could reduce TelCap size in patients with DME. We propose that larger-sized TelCaps detected by IA might be useful predictors of refractory DME, which could thus be principal targets of laser photocoagulation.
Keywords: anti-VEGF therapy, diabetic retinopathy, TelCap, indocyanine green angiography, microaneurysm, optical coherence tomography
Introduction
Diabetic macular edema (DME) is a major complication in patients with diabetes mellitus that can lead to severe vision reduction.1,2 The pathogenesis of DME is due to diabetic blood–retinal barrier breakdown and intraretinal fluid leakage from microaneurysms (MAs).3
Vascular endothelial growth factor (VEGF) has been identified as a critical mediator of retinal neovascularization and permeability in eyes with diabetic retinopathy (DR).4 The management of DME has changed considerably in recent years, especially following the development of intravitreal anti-VEGF therapy, which has emerged as a first-line therapy for center-involved DME. Laser treatment,5 intravitreal steroid therapy, and vitrectomy are also important treatment options for DME.1 Many randomized clinical trials have demonstrated that intravitreal injection of anti-VEGF agents (eg, ranibizumab and aflibercept) showed improved visual acuity and macular swelling.6,7 However, macular edema (ME) did not improve but rather persisted in a significant number of patients, even after repeated intravitreal anti-VEGF injections.8,9
Microvascular abnormalities such as MAs are the most characteristic signs of DR, and extravascular leakage from these can cause DME.10 Regarding the relationship between VEGF and MAs, we11 and others12–15 have recently demonstrated that intravitreal injection of anti-VEGF agents can reduce the number of MAs present in DME patients. Sugimoto et al further demonstrated that the reduction in the number of MAs correlated with a reduction in the central retinal thickness.12 However, there were non-responding MAs even after three consecutive loading injections.11,12 Thus, it remains unclear as to what type of MA responds to anti-VEGF agents and which is associated with recurrent DME.
Pathologic studies have shown that the cellular components in the lumens of the MAs are erythrocytes or polymorphonuclear leukocytes and intramural cells, endothelial cells, or pericytes,16,17 and that dense hyalinized MAs are often acellular, whereas hypercellular MAs have a thin wall.16 The association between the vascular wall and the cellular content in MAs indicates that there are multiple types of MAs in vivo. This led us to hypothesize that the pace of reducing the size of MA in response to anti-VEGF may vary depending on each different pathology of MA.
Occasionally, microvascular abnormalities reach several hundreds of microns in diameter, and such large lesions have been termed capillary MAs.15,18 Castro-Farías et al recently proposed the name ‘telangiectatic capillaries’ (TelCaps) to describe capillary abnormalities >150 µm to avoid confusion with the term “retinal arterial microaneurysm”.19,20
TelCaps are often detected by fluorescein- and indocyanine green angiography (IA). The fluorescein molecule is only 60% to 80% bound to proteins and leaks through vessels, whereas the indocyanine green molecule is 98% bound to proteins and does not leak through vessels.21 This allows IA to better visualize TelCaps in DME.11,19 In this study, we investigated changes in the size of TelCaps after intravitreal injection of anti-VEGF agents in DME, and examined the characteristics of anti-VEGF-resistant TelCaps.
Materials and Methods
Patients and Study Design
This study was approved by the Institutional Ethics Committee of Kurume University Hospital (Fukuoka, Japan) with the number (22191) and was conducted in accordance with the tenets of the Declaration of Helsinki regarding biomedical research involving human subjects. Written informed consent was obtained from all patients.
Twelve eyes of 12 patients with center-involved DME were included in this retrospective study. The mean age of the patients was 65.2 ± 8.8 years. All patients were examined at Kurume University Hospital and were followed for a minimum of 3 months during the period between October 2020 and October 2022. All patients received an initial loading dose of three injections of anti-VEGF agents administered monthly; thereafter, they received a pro re nata regimen for a minimum of 1 month of follow-up. The pro re nata regimen was applied until an improvement in the central macular edema was confirmed by optical coherence tomography (OCT) or until stable visual acuity was achieved.11 IA images were obtained for all patients before and at 3 months after the initial injection. The exclusion criteria were (1) a history of vitreoretinal surgery; (2) previous treatment with anti-VEGF agents or sub-tenon triamcinolone acetonide injection within 3 months; (3) active intraocular inflammation; (4) uncontrolled glaucoma; and (5) the presence of epiretinal membrane or vitreomacular traction syndrome.
We assessed the best-corrected visual acuity (BCVA) using Landolt decimal visual acuity charts at 5 m (CV-6000, Tomey, Nagoya, Japan; or AVC-36, Kowa, Nagoya, Japan) or single Landolt test cards (HP-1258, Handaya, Tokyo, Japan). The BCVA was converted to the logarithm of the minimum angle of resolution (logMAR).
Indocyanine Green Angiography and Optical Coherence Tomography
IA images were obtained using the Heidelberg SPECTRALIS HRA2 + OCT device (Heidelberg Engineering, Heidelberg, Germany) with a 30° field of view. IA was performed after intravenous injection of 5 mL indocyanine green and late phases were included in the analysis (>10 min). TelCaps were defined as isolated or clustered large punctiform lesions (>100 microns) that were hypercyanescent on late-phase IA (>10 min) (Figure 1), as previously described.19,22
 |
Figure 1 Representative optical coherence tomography (OCT) and indocyanine green angiography (IA) for calculating TelCap size. Spectralis OCT image (6 × 6 mm) (A) and late-phase IA at baseline (B). Retinal topographic map of the OCT was overlaid onto the late-phase IA (C). A single TelCap is shown (B–D; yellow arrow). Spectralis OCT image (6 × 6 mm) (E) and late-phase IA (F). Retinal topographic map overlaid onto the late-phase IA (G) after three consecutive treatments. A TelCap of reduced size is shown (F–H; yellow arrow). The area of the TelCap was reduced from 16,733.06 µm2 to 4779.94 µm2. The number of the TelCaps was decreased from 5 to 2. Areas of the retina where the thickness was >400 µm are depicted as Orange-red to white in the retinal topographic map. |
In each eye, we automatically overlaid the retinal thickness topographic map (6 × 6 mm) obtained by the SPECTRALIS HRA2 + OCT device (Figure 1A) onto the images of late-phase IA (Figure 1B) obtained using the same device (Figure 1C). We defined the area where the retinal thickness was >400 µm (orange-red to white in the SPECTRALIS color chart) as the area of the macular edema. The number of TelCaps as hyperfluorescent spots on late-phase IA in the area with macular edema was determined using Image J software (National Institutes of Health; available at http://rsb.info.nih.gov/ij/index.html), as previously described.19,23,24 On spectral-domain optical coherence tomography, TelCaps appeared as hyper-reflective, round, or oval cockade lesions with clearly visible parietal thickening (Figure 1D). OCT allowed measurement of the TelCaps size using the caliper placed on the longest axis.19,22 The same analyses were performed at 1 month after three consecutive anti-VEGF injections (Figures 1E–1H). The presence of TelCaps was evaluated by two experienced retinal specialists (KI and SY) based primarily on size and the IA staining pattern.
Statistical Analysis
Statistical analyses were performed using a commercial statistical software package (JMP ver.16; SAS Institute, Cary, NC, USA). The results were expressed as the mean ± standard deviation. Paired t-tests were used to compare the BCVA and central macular thickness (CMT) before and at 3 months after the initial injection. The Wilcoxon signed-rank test was performed to compare the number and size of TelCaps detected before and at 3 months after the initial injection. The Mann–Whitney U-test was applied to compare the size of TelCaps between two groups.
Results
A total of 12 eyes from 12 patients met the inclusion criteria for this study. Table 1 presents baseline and 3-month measurements of all patients eligible for inclusion in this study. No patients were excluded from the analyses. Patients received three consecutive injections between the initial and follow-up IA. All 12 eyes received aflibercept, while one of the eyes also received ranibizumab. The mean BCVA improved from 0.24 ± 0.04 logMAR before treatment to 0.16 ± 0.06 logMAR at 3 months after treatment initiation (P < 0.01). The mean CMT significantly decreased from 470 ± 135 µm at baseline to 356 ± 79 µm at 3 months (P < 0.02). All 12 eyes showed partially decreased retinal thickness but persistent thickening located selectively around the remaining TelCaps after three consecutive anti-VEGF injections.
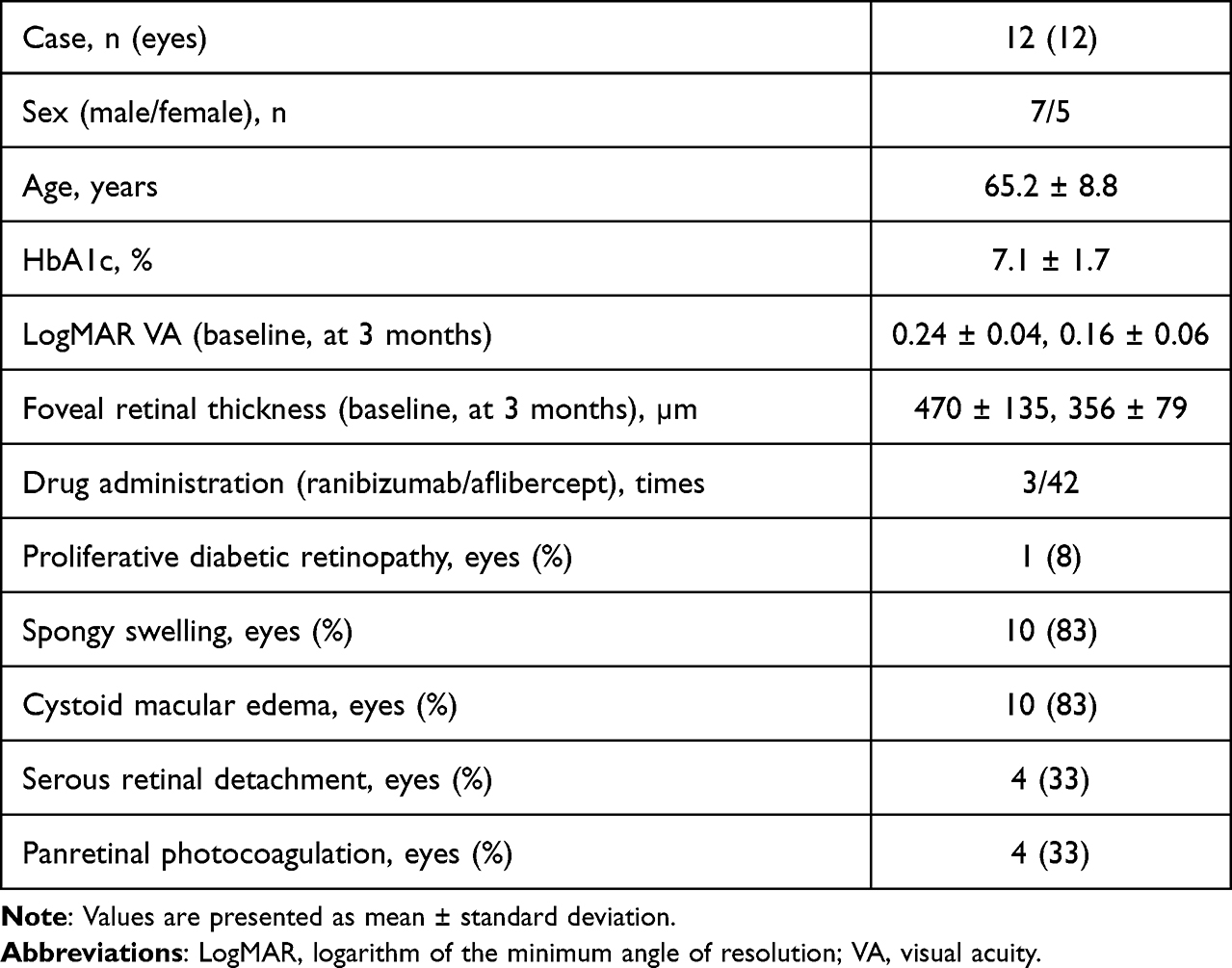 |
Table 1 Baseline and 3-Month Characteristics of Patients Included in the Study |
At baseline, the mean number of TelCaps was 3.75 ± 1.60 in the late phase (>10 min) IA. At 3 months, the mean number of TelCaps was 2.25 ± 1.48 in late-phase IA. Therefore, at 3 months, the number of TelCaps had significantly decreased from baseline (P < 0.05; Figure 2).
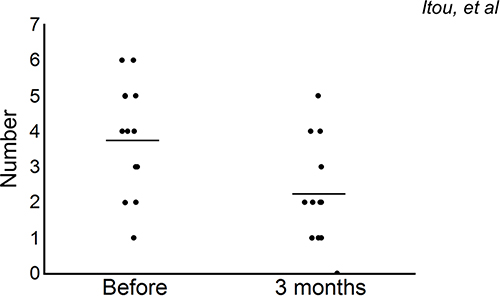 |
Figure 2 Effects of intravitreal injection of anti-VEGF agents on the number of TelCaps. The number of TelCaps in late-phase IA is visualized by dot plots at baseline and at 3 months after the initial treatment. The horizontal line in each plot indicates the median score. There were significant reductions in TelCaps between the baseline and at 3 months (P<0.05). |
We subsequently determined whether the TelCap size was altered after anti-VEGF treatment. At baseline, the mean TelCap size was 19,762.72 ± 6548.61 µm2 in late-phase IA. At 3 months, the mean TelCap size was 12,939.88 ± 5965.86 µm2 in late-phase IA, which was significantly decreased compared with the baseline (P < 0.0001; Figure 3).
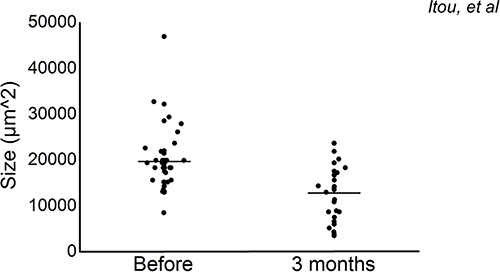 |
Figure 3 Effects of intravitreal injection of anti-VEGF agents on the size of TelCaps. The TelCaps size is visualized by dot plots at baseline and at 3 months after the initial treatment. The horizontal line in each plot indicates the median score. There were significant reductions in the TelCaps between the baseline and at 3 months (P<0.0001). |
Of the 45 TelCaps from all examined patients, the size at baseline was 21,613.18 ± 7509.17 µm2 in the 27 TelCaps that remained, even after the three consecutive injections, and 16,987.04 ± 3340.47 µm2 in the 18 TelCaps that were resolved, which was statistically significantly different (P < 0.03; Figure 4).
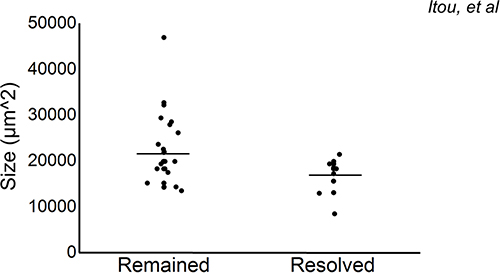 |
Figure 4 Relationship between recurrent macular edema and the size of TelCaps at baseline. The TelCaps size is visualized by dot plots at the baseline. The horizontal line in each plot indicates the median score. We classified TelCaps at 3 months after the start of treatment into two groups: remained and resolved groups. The TelCaps size in late-phase IA at baseline was significantly larger in the remained group than in the resolved group (P<0.03). |
Discussion
To the best of our knowledge, this is the first report to demonstrate significant reductions in TelCap size between the baseline and 3 months after treatment with anti-VEGF agents. The absence of pericytes is characteristic of MAs, possibly because VEGF abolishes pericyte coverage of nascent vascular sprouts, leading to vessel destabilization,25 although some researchers have reported that VEGF is required for pericyte survival.26 We postulated that the injection of anti-VEGF agents may accelerate pericyte recruitment around the retinal vascular endothelial cells in TelCaps.27 These pericytes subsequently produce type IV collagen and multiple laminin isoforms,28 which reduce the depth of each TelCap. These may subsequently stabilize retinal vascular endothelial cells and reduce TelCap size.29
We found that those TelCaps that remained after three consecutive anti-VEGF agent injections had a significantly larger mean size at baseline (Figure 4). We speculated that relatively new TelCaps that occur with endothelial proliferation are smaller and more sensitive to anti-VEGF agents. In contrast, larger TelCaps may represent a more chronic and advanced stage with intraluminal material such as hyaline and fat deposition,17 which may possess affinity for IA. These larger TelCaps may be closely associated with less sensitive recurrent or refractory macular edema. This is consistent with a previous report that greater TelCap size (outer and inner diameters) and wall thickness correlated with increased endothelial dysfunction in non-proliferative DR,30 and that late IA staining is an indicator of severe breakdown of the blood–retinal barrier.19
It was reported that eyes receiving both ranibizumab and deferred laser photocoagulation for DME exhibited better long-term vision improvement than eyes receiving ranibizumab with prompt laser photocoagulation.31 Together with the results of recent studies including ours,32 our findings in the current study suggest that deferred laser photocoagulation should first be performed only for some of the largest TelCaps detected by IA after TelCaps reduction by injection of anti-VEGF agents, especially when the number of TelCaps is high. In this manner, we expect to achieve a more effective minimally invasive DME therapy by selective targeting of “refractory, anti-VEGF therapy-resistant TelCaps” with lesser impaired visual function. In parallel, laser photocoagulation may be performed in some cases before anti-VEGF therapy in which single or a few isolated TelCaps are easily reachable and clearly visible to spare some injections.33
Although the detection of refractory TelCaps by IA appears to be useful, the routine clinical use of IA could be challenging in real-world practice because it is invasive, costly, and time-consuming. Recently, OCT angiography (OCTA) has been gaining interest because of its capacity to non-invasively document the retinal vasculature, and it has been reported to be able to record features of DR.34 However, OCTA detection of TelCaps in DR may depend on intra-aneurysmal blood flow, rather than their size or leakage.34 The decrease in blood flow due to the vessel wall thickening and intraluminal material accumulation has been considered as the cause of the poor detection of some of the largest TelCaps.19 OCTA is, therefore, not a sufficient imaging technique for cases with TelCaps.
Accordingly, Bourhis et al reported that structural OCT is highly sensitive for the detection of TelCaps and superior to IA because of the visualization of the TelCap wall.15 Therefore, multimodal imaging approaches other than OCTA, such as structural OCT,35 multicolor scanning laser ophthalmoscopy,36 and infrared reflectance imaging,20 may have a better therapeutic effect on DME in a less time- and labor-consuming manner.
The limitations of the present study were the small number of evaluated patients and the short follow-up period. It is also possible that some of the TelCaps defined in this study were MAs, mainly because there is currently no consensus to differentiate MAs from TelCaps as well as there probably being a continuum between these lesions.22 Because these factors may have biased our results, prospective studies are required with a larger number of patients and a longer follow-up period.
Conclusions
Our study showed that intravitreal injection of anti-VEGF agents could reduce TelCap size in patients with DME. We propose that larger-sized TelCaps detected by IA might be useful predictors of refractory DME, which could thus be principal targets of laser photocoagulation.
Ethics Approval and Informed Consent
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We thank H. Nikki March, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
This research was supported in part by grants from the JSPS KAKENHI (grant number 21K09734).
Disclosure
Mr Junichi Itou reports personal fees from Novartis Japan, outside the submitted work. Dr Kei Furushima reports grants from Government, during the conduct of the study. The authors declare that they have no other conflicts of interest in this work.
References
1. Yoshida S, Murakami T, Nozaki M, et al. Review of clinical studies and recommendation for a therapeutic flow chart for diabetic macular edema. Graefes Arch Clin Exp Ophthalmol. 2021;259(4):815–836. doi:10.1007/s00417-020-04936-w
2. Das A, McGuire PG, Rangasamy S. Diabetic macular edema: pathophysiology and novel therapeutic targets. Ophthalmology. 2015;122(7):1375–1394. doi:10.1016/j.ophtha.2015.03.024
3. Klein R, Meuer SM, Moss SE, Klein BE. Retinal microaneurysm counts and 10-year progression of diabetic retinopathy. Arch Ophthalmol. 1995;113(11):1386–1391. doi:10.1001/archopht.1995.01100110046024
4. Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med. 1994;331(22):1480–1487. doi:10.1056/NEJM199412013312203
5. Allingham MJ, Mukherjee D, Lally EB, et al. A quantitative approach to predict differential effects of anti-VEGF treatment on diffuse and focal leakage in patients with diabetic macular edema: a pilot study. Transl Vis Sci Technol. 2017;6(2):7. doi:10.1167/tvst.6.2.7
6. Ishibashi T, Li X, Koh A, et al. The REVEAL Study: ranibizumab monotherapy or combined with laser versus laser monotherapy in Asian patients with diabetic macular edema. Ophthalmology. 2015;122(7):1402–1415. doi:10.1016/j.ophtha.2015.02.006
7. Mitchell P, Bandello F, Schmidt-Erfurth U, et al. The RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology. 2011;118(4):615–625. doi:10.1016/j.ophtha.2011.01.031
8. Brown DM, Schmidt-Erfurth U, Do DV, et al. Intravitreal aflibercept for diabetic macular edema: 100-week results from the Vista and VIVID studies. Ophthalmology. 2015;122(10):2044–2052. doi:10.1016/j.ophtha.2015.06.017
9. Choi MY, Jee D, Kwon JW. Characteristics of diabetic macular edema patients refractory to anti-VEGF treatments and a dexamethasone implant. PLoS One. 2019;14(9):e0222364. doi:10.1371/journal.pone.0222364
10. Murakami T, Nishijima K, Sakamoto A, Ota M, Horii T, Yoshimura N. Foveal cystoid spaces are associated with enlarged foveal avascular zone and microaneurysms in diabetic macular edema. Ophthalmology. 2011;118(2):359–367. doi:10.1016/j.ophtha.2010.03.035
11. Mori K, Yoshida S, Kobayashi Y, et al. Decrease in the number of microaneurysms in diabetic macular edema after anti-vascular endothelial growth factor therapy: implications for indocyanine green angiography-guided detection of refractory microaneurysms. Graefes Arch Clin Exp Ophthalmol. 2020;258(4):735–741. doi:10.1007/s00417-020-04608-9
12. Sugimoto M, Cutler A, Shen B, et al. Inhibition of EGF signaling protects the diabetic retina from insulin-induced vascular leakage. Am J Pathol. 2013;183(3):987–995. doi:10.1016/j.ajpath.2013.05.017
13. Leicht SF, Kernt M, Neubauer A, et al. Microaneurysm turnover in diabetic retinopathy assessed by automated RetmarkerDR image analysis--potential role as biomarker of response to ranibizumab treatment. Ophthalmologica. 2014;231(4):198–203. doi:10.1159/000357505
14. Cho HJ, Rhee TK, Kim HS, et al. Intravitreal bevacizumab for symptomatic retinal arterial macroaneurysm. Am J Ophthalmol. 2013;155(5):898–904. doi:10.1016/j.ajo.2012.12.003
15. Bourhis A, Girmens JF, Boni S, et al. Imaging of macroaneurysms occurring during retinal vein occlusion and diabetic retinopathy by indocyanine green angiography and high resolution optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2010;248(2):161–166. doi:10.1007/s00417-009-1175-6
16. De Venecia G, Davis M, Engerman R. Clinicopathologic correlations in diabetic retinopathy. I. Histology and fluorescein angiography of microaneurysms. Arch Ophthalmol. 1976;94(10):1766–1773. doi:10.1001/archopht.1976.03910040540013
17. Stitt AW, Gardiner TA, Archer DB. Histological and ultrastructural investigation of retinal microaneurysm development in diabetic patients. Br J Ophthalmol. 1995;79(4):362–367. doi:10.1136/bjo.79.4.362
18. Spaide RF, Barquet LA. Retinal capillary macroaneurysms. Retina. 2019;39:1889–1895. doi:10.1097/IAE.0000000000002406
19. Castro Farias D, Matsui Serrano R, Bianchi Gancharov J, et al. Indocyanine green angiography for identifying telangiectatic capillaries in diabetic macular oedema. Br J Ophthalmol. 2020;104(4):509–513. doi:10.1136/bjophthalmol-2019-314355
20. Roh HC, Lee C, Kang SW, Choi KJ, Eun JS, Hwang S. Infrared reflectance image-guided laser photocoagulation of telangiectatic capillaries in persistent diabetic macular edema. Sci Rep. 2021;11(1):21769. doi:10.1038/s41598-021-01183-9
21. Weinberger D, Kramer M, Priel E, Gaton DD, Axer-Siegel R, Yassur Y. Indocyanine green angiographic findings in nonproliferative diabetic retinopathy. Am J Ophthalmol. 1998;126(2):238–247. doi:10.1016/S0002-9394(98)00148-2
22. Chaperon M, Kodjikian L, Agard E, et al. Screening of telangiectatic capillaries in chronic macular edema based on multimodal imaging: a study of 101 eyes. LyoMAC1 study. Graefes Arch Clin Exp Ophthalmol. 2022;260(8):2501–2508. doi:10.1007/s00417-022-05592-y
23. Ogura S, Yasukawa T, Kato A, et al. Indocyanine green angiography-guided focal laser photocoagulation for diabetic macular edema. Ophthalmologica. 2015;234(3):139–150. doi:10.1159/000437360
24. Nozaki M, Kato A, Yasukawa T, Suzuki K, Yoshida M, Ogura Y. Indocyanine green angiography-guided focal navigated laser photocoagulation for diabetic macular edema. Jpn J Ophthalmol. 2019;63(3):243–254. doi:10.1007/s10384-019-00662-x
25. Kernt M, Cserhati S, Seidensticker F, et al. Improvement of diabetic retinopathy with intravitreal Ranibizumab. Diabetes Res Clin Pract. 2013;100(1):e11–13. doi:10.1016/j.diabres.2013.01.006
26. Dorrell MI, Aguilar E, Scheppke L, Barnett FH, Friedlander M. Combination angiostatic therapy completely inhibits ocular and tumor angiogenesis. Proc. Natl Acad Sci USA. 2007;104(3):967–972. doi:10.1073/pnas.0607542104
27. Greenberg JI, Shields DJ, Barillas SG, et al. A role for VEGF as a negative regulator of pericyte function and vessel maturation. Nature. 2008;456(7223):809–813. doi:10.1038/nature07424
28. Kohno R, Hata Y, Mochizuki Y, et al. Histopathology of neovascular tissue from eyes with proliferative diabetic retinopathy after intravitreal bevacizumab injection. Am J Ophthalmol. 2010;150(2):223–229 e221. doi:10.1016/j.ajo.2010.03.016
29. Elnahry AG, Abdel-Kader AA, Raafat KA, Elrakhawy K. Evaluation of changes in macular perfusion detected by optical coherence tomography angiography following 3 intravitreal monthly bevacizumab injections for diabetic macular edema in the IMPACT study. J Ophthalmol. 2020;2020:5814165. doi:10.1155/2020/5814165
30. Lee SN, Chhablani J, Chan CK, et al. Characterization of microaneurysm closure after focal laser photocoagulation in diabetic macular edema. Am J. Ophthalmol. 2013;155(5):905–912.
31. Bressler SB, Glassman AR, Almukhtar T, et al. Five-year outcomes of ranibizumab with prompt or deferred laser versus laser or triamcinolone plus deferred ranibizumab for diabetic macular edema. Am J Ophthalmol. 2016;164:57–68. doi:10.1016/j.ajo.2015.12.025
32. Mori K, Ishikawa K, Wada I, et al. Changes in metamorphopsia after the treat-and-extend regimen of anti-VEGF therapy for macular edema associated with branch retinal vein occlusion. PLoS One. 2020;15(10):e0241343. doi:10.1371/journal.pone.0241343
33. Paques M, Philippakis E, Bonnet C, et al. Indocyanine-green-guided targeted laser photocoagulation of capillary macroaneurysms in macular oedema: a pilot study. Br J Ophthalmol. 2017;101(2):170–174. doi:10.1136/bjophthalmol-2015-308142
34. Nakao S, Yoshida S, Kaizu Y, et al. Microaneurysm detection in diabetic retinopathy using OCT angiography may depend on intramicroaneurysmal turbulence. Ophthalmol Retina. 2018;2(11):1171–1173. doi:10.1016/j.oret.2018.06.001
35. Horii T, Murakami T, Nishijima K, Sakamoto A, Ota M, Yoshimura N. Optical coherence tomographic characteristics of microaneurysms in diabetic retinopathy. Am J Ophthalmol. 2010;150(6):840–848. doi:10.1016/j.ajo.2010.06.015
36. Sakono T, Terasaki H, Sonoda S, et al. Comparison of multicolor scanning laser ophthalmoscopy and optical coherence tomography angiography for detection of microaneurysms in diabetic retinopathy. Sci Rep. 2021;11(1):17017. doi:10.1038/s41598-021-96371-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relationship Between Risk Factors and Macular Thickness in Patients with Early Diabetic Retinopathy
Wei Q, Qiu W, Liu Q, Jiang Y
International Journal of General Medicine 2022, 15:6021-6029
Published Date: 5 July 2022
Intravitreal Faricimab for Previously Treated Neovascular Age-Related Macular Degeneration
Hang A, Ngo T, Virk JS, Moussa K, Moshiri A, Emami-Naeini P, Park SS
Clinical Ophthalmology 2024, 18:3781-3789
Published Date: 14 December 2024
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025
Analysis of OCT-Based Biomarkers and Recurrence in Eyes with Diabetic Macular Edema Following Anti-VEGF Therapy
Zhu T, Wang Y, Hua Y, Zha X, Xu T
International Journal of General Medicine 2025, 18:6941-6948
Published Date: 13 November 2025