Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Red Blood Cell Distribution Width as a Biomarker in Type 2 Diabetes Mellitus: Technical Notes [Letter]
Authors Frater JL ![]()
Received 2 February 2023
Accepted for publication 4 February 2023
Published 17 February 2023 Volume 2023:16 Pages 479—481
DOI https://doi.org/10.2147/DMSO.S406885
Checked for plagiarism Yes
Editor who approved publication: Dr Konstantinos Tziomalos
John L Frater
Department of Pathology and Immunology, Washington University, St. Louis, MO, USA
Correspondence: John L Frater, Department of Pathology and Immunology, Washington University School of Medicine, 660 South Euclid Avenue, Box 8118, St. Louis, MO, 63110-1093, USA, Tel +1 314 362-1553, Email [email protected]
View the original paper by Mr Arkew and colleagues
A Response to Letter has been published for this article.
Dear editor
Arkew et al have published an article entitled “Red Blood Cell Parameters and Their Correlation with Glycemic Control Among Type 2 Diabetic Adult Patients in Eastern Ethiopia: A Comparative Cross-Sectional Study” in Diabetes, Metabolic Syndrome and Obesity.1 I congratulate the authors on their work, which adds to the already extensive literature on the use of the red blood cell distribution width (RDW) as a surrogate biomarker of systemic inflammation in the setting of type 2 diabetes mellitus (T2DM). I would like to add some technical details about the RDW which would be of interest to the readership of the journal who are considering the use of the RDW for this or related purposes.
Commercially available blood analyzers calculate the RDW as the standard deviation (RDW-SD) or the coefficient of variability (RDW-CV) of the red blood cell histogram. Like any other complete blood cell count (CBC) analyte, the RDW may be impacted by preanalytical and analytical phase variables. In the case of the RDW, the most important of these appear to be; 1) time between phlebotomy and analysis, 2) storage temperature, 3) tube type and anticoagulant, and 4) transport conditions, including pneumatic tube transport.2 Moreover, the determination of the RDW is not standardized among the different instrumentation manufacturers, and in the absence of a recognized RDW standard, there is an additional analytical phase issue.2 Therefore, when setting up a clinical study that uses CBC data, including the RDW, it is important to consider the potential biases introduced into the data by these preanalytical and analytical phase variables.
To assess the degree to which these issues have been addressed in the study of Arkew et al and the other studies cited in their paper, I extracted the relevant data which are summarized in Table 1.1,3–8 The preanalytical variables that may impact the RDW were largely unreported, with time between phlebotomy and analysis reported in 1/7 studies and no reporting of storage temperature and transport conditions in any of the studies. It is not surprising that these variables are underreported, since guidelines such as the Standards for Reporting of Diagnostic Accuracy Studies (STARD) do not mandate the reporting of preanalytical and analytical phase variables, despite their obvious importance in the outcomes of many laboratory tests, including the RDW.9 This is unfortunate, since information about these potential sources of bias are largely unreported outside the laboratory medicine literature and may have important clinical implications. For example, a potential source of error in the RDW is delay between phlebotomy and analysis. Since 6/7 of the studies used outpatient data, a potential time delay may occur if specimens were collected in doctors’ offices and/or outpatient clinics and analyzed in a central laboratory. Daves et al have reported that time delays as short as 3 hours have resulted in an erroneous RDW result.10 A lack of control for these preanalytical phase variables may account in part for the different cutoffs for the RDW and the lack of statistical significance in the study of Adane et al.3 Due to the lack of standardization of the RDW across different instrumentation platforms, the wide variety of instruments used in these studies, including devices manufactured by Sysmex (Kobe, Japan),3,6 Abbott (Chicago, IL, USA),4 Beckman Coulter (Brea, CA, USA),1,5 and Horiba (Kyoto, Japan),7 may add additional biases.
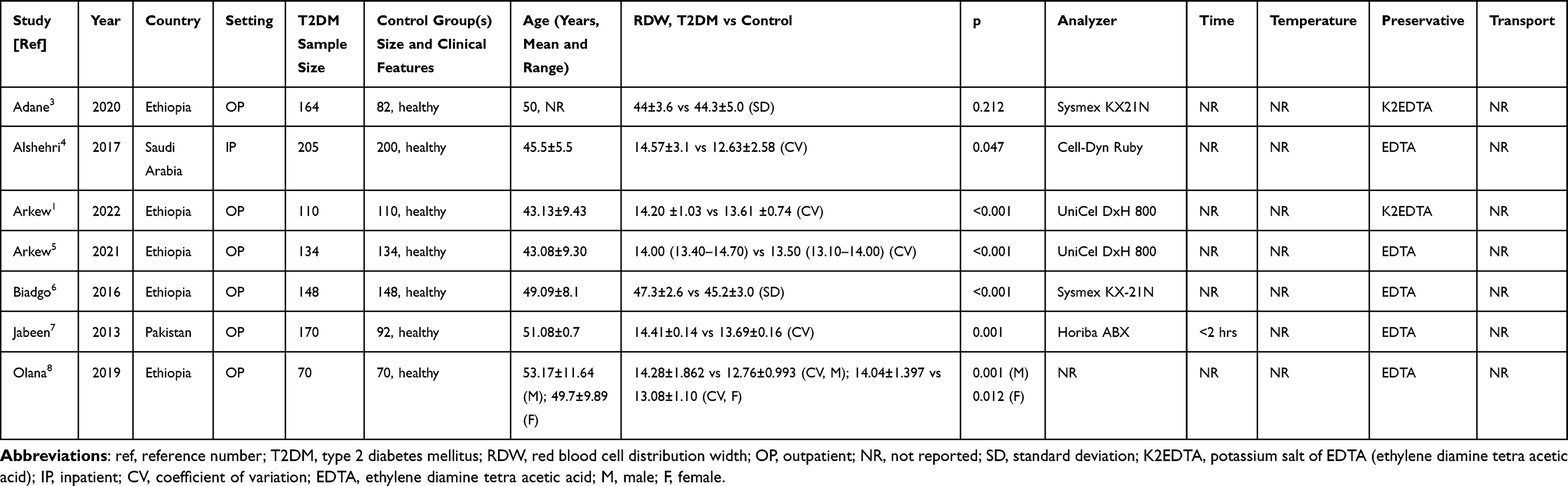 |
Table 1 Major Clinical and Laboratory Features of the Studies Cited by Arkew et al1 |
Another issue with the practical implementation of the RDW as a surrogate biomarker is its limited dynamic range, meaning that the difference between a normal and abnormal result may be quite small. Despite the differences in group means being statistically significant, there may be considerable overlap between individual results in the disease and control groups, impacting the meaningfulness of test results. This is particularly noteworthy for the studies of Arkew et al and Jabeen et al,1,5,7 where the differences in group means are ~1 fL, despite the statistically significant difference between the two cohorts. Without a rigorous control of the preanalytical and analytical phase variables, individual patient results may be difficult or impossible to interpret.
In summary, I thank Arkew et al for their thought-provoking study, that adds to our understanding of the potential clinical utility of the RDW in T2DM, and more broadly, its use as a surrogate marker of systemic inflammation. I hope that this assessment will add additional context to Arkew et al’s work and will be of interest to the readership of Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy who are considering the use of the RDW for this purpose.
Disclosure
The author reports no conflicts of interest in this communication.
References
1. Arkew M, Asmerom H, Tesfa T, et al. Red blood cell parameters and their correlation with glycemic control among type 2 diabetic adult patients in Eastern Ethiopia: a comparative cross-sectional study. Diabetes Metab Syndr Obes. 2022;15:3499–3507. doi:10.2147/DMSO.S386093
2. Frater JL. Red blood cell distribution width: the importance of preanalytical and analytical phase variables. Wien Klin Wochenschr. 2022. doi:10.1007/s00508-022-02099-8
3. Adane T, Getaneh Z, Asrie F. Red blood cell parameters and their correlation with renal function tests among diabetes mellitus patients: a comparative cross-sectional study. Diabetes Metab Syndr Obes. 2020;13:3937–3946. doi:10.2147/DMSO.S275392
4. Al Shehri ZS. The relationship between some biochemical and hematological changes in type 2 diabetes mellitus. Biomed Res Ther. 2017;4(11):1760–1774. doi:10.15419/bmrat.v4i11.382
5. Arkew M, Gemechu K, Haile K, Asmerom H. Red blood cell distribution width as novel biomarker in cardiovascular diseases: a literature review. J Blood Med. 2022;13:413–424. doi:10.2147/JBM.S367660
6. Biadgo B, Melku M, Abebe SM, Abebe M. Hematological indices and their correlation with fasting blood glucose level and anthropometric measurements in type 2 diabetes mellitus patients in Gondar, Northwest Ethiopia. Diabetes Metab Syndr Obes. 2016;9:91–99. doi:10.2147/DMSO.S97563
7. Jabeen F, Rizvi HA, Aziz F, Wasti AZ. Hyperglycemic induced variations in hematological indices in type 2 diabetics. IJAR. 2013;1(8):322–334.
8. Olana C, Seifu D, Menon MK, Natesan G. Abnormal hematological indices and anthropometric parameters associated with type 2 diabetes. Int J Biomed Adv Res. 2019;10(11):1–8.
9. Wu AH, Christenson RH. The standards for reporting diagnostic accuracy studies 2015 update: is there a missing link to the triumvirate? Ann Transl Med. 2016;4(3):44. doi:10.3978/j.issn.2305-5839.2015.12.41
10. Daves M, Zagler EM, Cemin R, et al. Sample stability for complete blood cell count using the Sysmex XN haematological analyser. Blood Transfus. 2015;13(4):576–582. doi:10.2450/2015.0007-15
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.