")
Back to Journals » Cancer Management and Research » Volume 13
Recurrent Laryngeal Nerve Injury Near the Nerve Entry Point in Total Endoscopic Thyroidectomy: A Retrospective Cohort Study
Authors Liu N, Chen B , Li L, Zeng Q, Sheng L , Zhang B, Liang W , Lv B
Received 9 September 2021
Accepted for publication 22 November 2021
Published 1 December 2021 Volume 2021:13 Pages 8979—8987
DOI https://doi.org/10.2147/CMAR.S338551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Nan Liu, Bo Chen, Luchuan Li, Qingdong Zeng, Lei Sheng, Bin Zhang, Weili Liang, Bin Lv
Department of Thyroid Surgery, General Surgery, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: Bin Lv
Department of Thyroid Surgery, General Surgery, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China
Email [email protected]
Background: Recurrent laryngeal nerve injury (RLNI) still occurs in total endoscopic thyroidectomy (TET) by using intraoperative neuromonitoring (IONM). As the region where most injuries occur, more attention should be paid to RLNI near the nerve entry point (NEP) in TET.
Materials and Methods: This cohort study collected retrospectively data from 415 patients who underwent TET between February 2012 and December 2019. The functions of the recurrent laryngeal nerve (RLN) in TET were recorded by IONM. The patients with RLNI near the NEP were followed up by laryngoscopies. The demographic and clinical characteristics, the mechanisms of RLNI, and the outcomes of RLNI were recorded and analyzed.
Results: There were a total of 444 at-risk nerves in 405 patients were analyzed. The incidence of RLNI near the NEP was 7.9%. RLNs with extralaryngeal branches were more likely to be injured near the NEP (P = 0.037). The incidences of different types of RLNI, in order of frequency, were 68.8% for thermal injury (n = 22), 28.1% for traction/compression injury (n = 9), and 3.1% for transverse injury (n = 1). A total of 93.8% (n = 30) of RLNI patients had complete recovery of vocal cord activity function.
Conclusion: The extralaryngeal branch was a risk factor for RLNI near the NEP in TET. Thermal injury caused by an ultrasonic scalpel was the most common cause of RLNI near the NEP. Most RLNIs near the NEP would eventually recover.
Keywords: thyroid surgery, total endoscopic thyroidectomy, recurrent laryngeal nerve injury, intraoperative neuromonitoring, recovery time
Introduction
Surgery is the main method for the treatment of thyroid cancer, but conventional open thyroidectomy (COT) can leave an obvious, permanent scar in the front of the neck. Surgeries are needed for an increasing number of young women with thyroid cancer. These patients are concerned about not only the safety of surgery but also the postoperative cosmetic effect. In 1996 and 1997, Gagner1 and Hüscher2 completed the first endoscopic parathyroid and thyroid surgeries, respectively. Total endoscopic thyroidectomy (TET) can provide a good neck cosmetic effect and improve the postoperative quality of life because of the small and hidden incisions.
Recurrent laryngeal nerve injury (RLNI) is one of the common complications of thyroidectomy, which can lead to postoperative vocal cord palsy (VCP). In thyroid surgery, the incidence of RLNI can be reduced by routine visual identification of the recurrent laryngeal nerve (RLN).3–6 The literature shows that the overall incidence of VCP after thyroid surgery is 4–8%, and the incidence of permanent VCP is 1–2%.7,8 In addition, the use of intraoperative neuromonitoring (IONM) can also help to identify RLNI and reduce the risk of RLNI.9–14
RLNI still occurs at times in TET with the help of routine visual identification and IONM. Some studies have confirmed that the incidence of RLNI in TET is higher than that in COT.15–22 In addition, it was found that the nerve entry point (NEP) into the larynx was a common region of nerve injury in COT.23 However, RLNIs near the NEP in TET have rarely been studied, and the mechanisms of RLNI in TET might be different from those in COT. Therefore, the purpose of this study was to describe the potential mechanisms of RLNI near the NEP in TET and to provide instruction for the thyroid surgeons.
Materials and Methods
Patient Selection
This retrospective cohort study collected data from a total of 415 patients who underwent TET due to thyroid papillary carcinoma between February 2012 and December 2019. Patients were informed of the study content in both written and oral forms before the operation and signed informed consents. All patients underwent laryngoscopies before the operations so that the movements of the vocal cord were determined. The research protocol has been approved by the Medical Ethics Committee of Qilu Hospital of Shandong University (Project identification code: 2018149). This study has been registered in the ResearchRegistry (UIN: researchregistry5594). This study complied with the Declaration of Helsinki.
In this study, an RLNI near the NEP was defined as a nerve injury occurring within 1 cm from the NEP. The inclusion and exclusion criteria of TET and RLNI near the NEP are shown in Table 1. The demographic data, surgical anatomy, postoperative VCP, and recovery time were recorded in this study. According to whether RLNI occurred or not, patients were divided into two groups to evaluate the risk factors for RLNI near the NEP. Then, the mechanisms of RLNI and the subsequent outcomes of VCP were analyzed. To further determine the effect of left and right thyroidectomy on RLNI near the NEP, a subgroup analysis was performed in the patients who underwent total lobectomy. The retrospective cohort study was designed according to the flow chart in Figure 1.
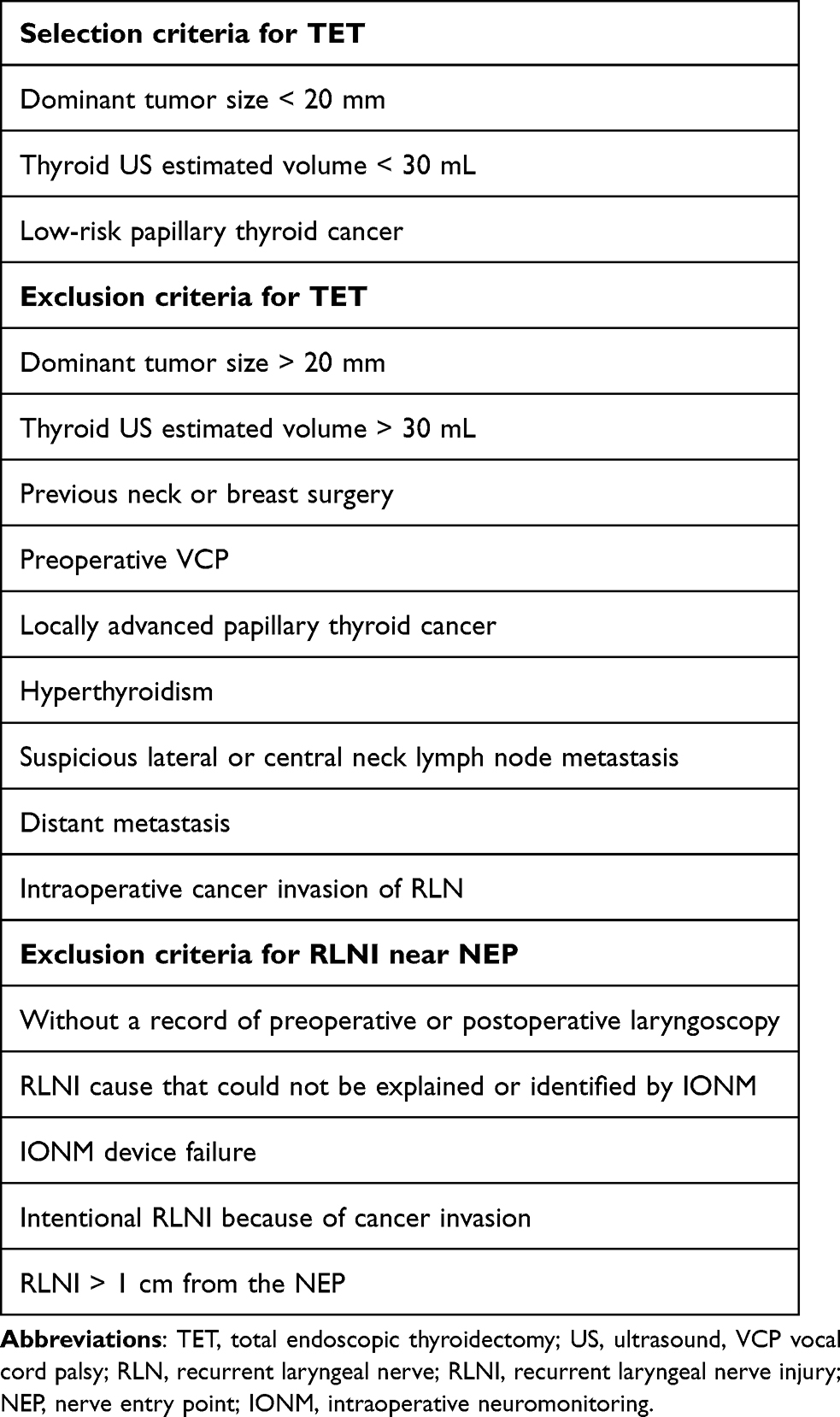 |
Table 1 Eligibility and Exclusion Criteria for the Study |
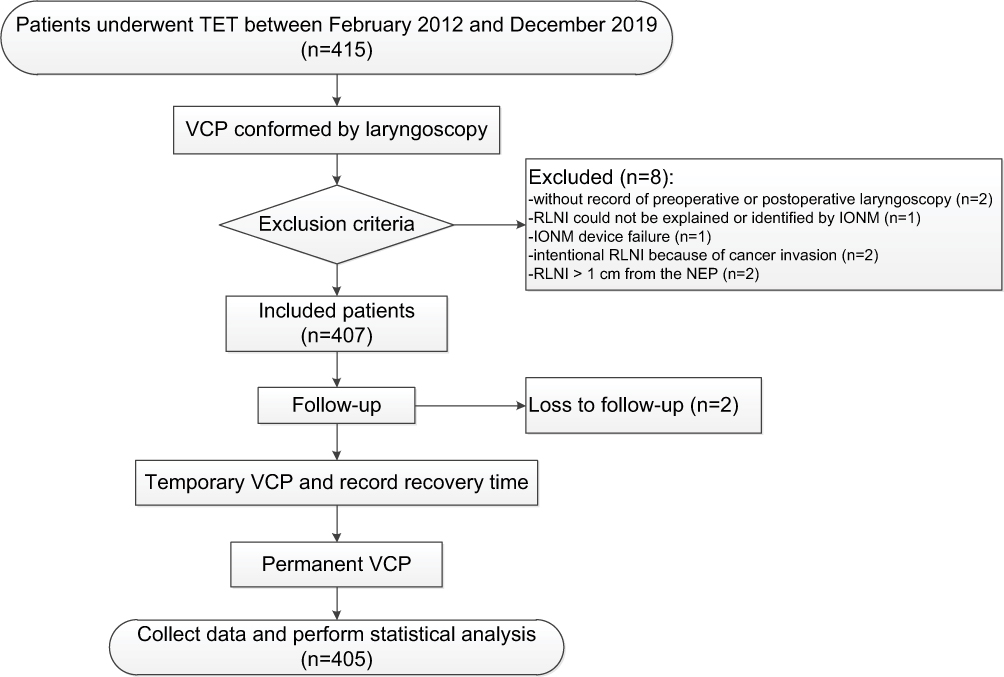 |
Figure 1 The flow chart of the study. Abbreviations: TET, total endoscopic thyroidectomy; VCP, vocal cord palsy; RLNI, recurrent laryngeal nerve injury; IONM, intraoperative neuromonitoring; NEP, nerve entry point. |
Surgical Technique and IONM Equipment
All TETs were performed by the same surgical team, including an experienced thyroid surgeon and two assistants. The operation was performed under general anesthesia, and a half dose of neuromuscular blocker was used during anesthesia induction. A 1-cm vertical incision was made near the sternum or the inner edge of the right mammary areola to serve as the observation hole, and a 5-mm incision was made at the edges of the left and right areola borders respectively as the operation hole. After the strap muscles were pulled laterally using special retractors, a monopolar stimulator probe was percutaneously punctured 3 cm above the ipsilateral clavicle to help identify and locate the RLN. After the RLN was found at the lower pole of the thyroid gland, it was dissected to the NEP. In order to minimize traction injury, excessive pulling of the thyroid lobe was avoided as much as possible. The RLN was bluntly dissected and then the fiber bundles or blood vessels were cut off, until the whole nerve was exposed to further avoid traction injury. The ultrasonic scalpel was fired when the distance between it and the RLN was at least 3 mm.
Intermittent IONM (3.0 Nim response system EMG endogenous tube; Medtronic, Minneapolis, MN, USA) was used to help identify the RLN and evaluate the function of the RLN in a standard four-step procedure.24 Standard equipment setup for induction and maintenance of anesthesia, tube positioning verification tests, EMG definitions, and troubleshooting algorithms were implemented and managed following the guidelines of the International Neural Monitoring Study Group.25
Identification and Mechanisms of RLNI
Intraoperative loss of signal (LOS) is defined as an absence of biphasic waveform EMG with a stimulation intensity of 1.0 mA and an event threshold of 100 mV. During the surgery, the function of the RLN was repeatedly evaluated after each step of dissecting the RLN or cutting off the Berry’s ligament to determine the time and location of nerve injury and the corresponding injury mechanism (such as traction/compression, thermal, transection, or clamp injury). When the interruption point of nerve conduction was verified, the RLN function was detected from the NEP of the RLN at the current intensity of 1.0 MA.24,25 If the signal was obtained, the RLN at the proximal position continued to be tested until a response could not be elicited. Conversely, the exposed RLN was then tested from the proximal portion to the distal portion until a monitoring signal was obtained.24,25
The RLNI was defined as thermal injury when LOS occurred immediately after the use of an ultrasonic scalpel near the RLN. Additionally, an ultrasonic scalpel was used after the function of RLN was verified normal. If nerve discontinuity was found, the RLNI was defined as transverse injury. For the patient with LOS after inadvertent clamping of the RLN, the RLNI was classified as clamp injury. It can be difficult to strictly distinguish traction and compression injuries in TET, as both can occur at the same time. If the RLNI could not be explained by the above injury mechanisms, especially when the RLN passed through the Berry’s ligament or the RLN had an upward inflection point, the RLNI was defined as traction/compression injury.
Follow-Up
All patients with RLNI were followed up by laryngoscopies for 6 months. The laryngoscopy was performed initially within 7 days after the operation. If the vocal cord activity decreased, it was defined as postoperative VCP. During the first month of follow-up, the patients were followed up once a week, and subsequently once every two weeks until the vocal cord activity recovered. Permanent VCP was considered if the vocal cord activity did not recover by the 6-month follow-up visit. Recovery time was measured as the time interval (days) from surgery to the recovery of vocal cord activity.
Statistical Analysis
Assuming a 10% loss due to follow-up, at least 374 at-risk nerves were needed to achieve 90% power at a 5% significance level on the basis of the practical experience and the rate of RLNI in TET described in previous publications.15–22
Statistical analysis was carried out using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, N.Y., USA). Continuous variables were statistically described as the mean ± standard deviation and statistically inferred by a T-test or Mann–Whitney U-test. Categorical variables were statistically described as frequency (percentage), and the statistical inference was carried out by a Chi-square test or Fisher’s exact test. Statistical significance was defined as P value <0.05.
Results
A total of 415 patients received TET, of which 8 patients were excluded (Figure 1). During the follow-up period, 2 patients were lost because they could not be contacted. Ultimately, a total of 405 patients (444 at-risk nerves) met the inclusion criteria and completed the follow-up (404 females and 1 male, with an average age of 34.6 ± 7.1 years and a range of 19–48 years). The results showed that age, sex, operation method, gland lobe volume, tumor size, operative time, and Hashimoto’s thyroiditis were not related to RLNI near the NEP (Table 2). However, patients with branched RLN were prone to suffer from RLNI near the NEP (P=0.037). In addition, the length of hospital stay of patients with RLNI near the NEP was increased (P=0.025).
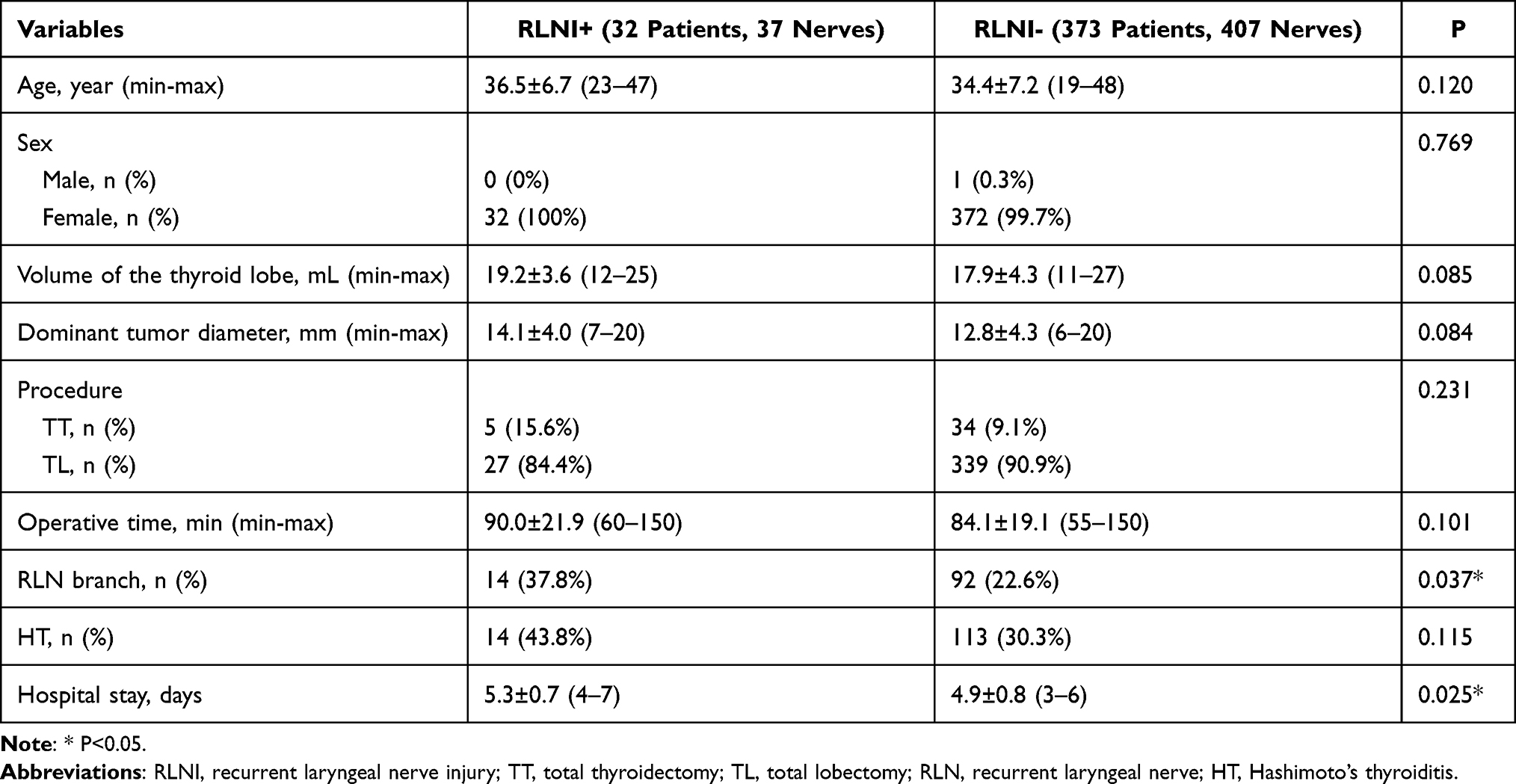 |
Table 2 Clinical Information of Enrolled Patients Grouped Based on RLNI |
A total of 32 patients (7.9%) had RLNI near the NEP (Table 3), though there was no patient with simultaneous bilateral RLNI. There was no patient with conversion to COT due to LOS. The order of RLNI near the NEP was thermal injury (68.8%; n=22), traction/compression injury (28.1%; n=9), and transverse injury (3.1%; n=1) (Table 4). No patients suffered from clamp injury. The incidence of temporary VCP was 7.4% (n=30), and there were 2 patients with permanent VCP. Out of the patients with thermal injury, there was one patient who suffered from permanent VCP, and the other patients suffered from temporary VCP. All the patients with traction/compression injury suffered from temporary VCP. The total recovery time of VCP was 28.2±22.4 days (Table 4). The recovery of the traction/compression injury group was faster than that of the thermal injury group, but there was no significant difference (P=0.066) (Table 4). The shortest recovery time of transient VCP was 10 days of traction injury, and the longest was 117 days of thermal injury. Although the only one patient with a transverse injury received endoscopic neuroanastomosis, the vocal cord movement had not recovered 6 months after the operation. In addition, there were 3 patients (8.6%; 3/35) for whom normal nerve signal transduction was restored during the operation by alleviating the traction of glands and changing the traction angle as soon as the LOS was found.
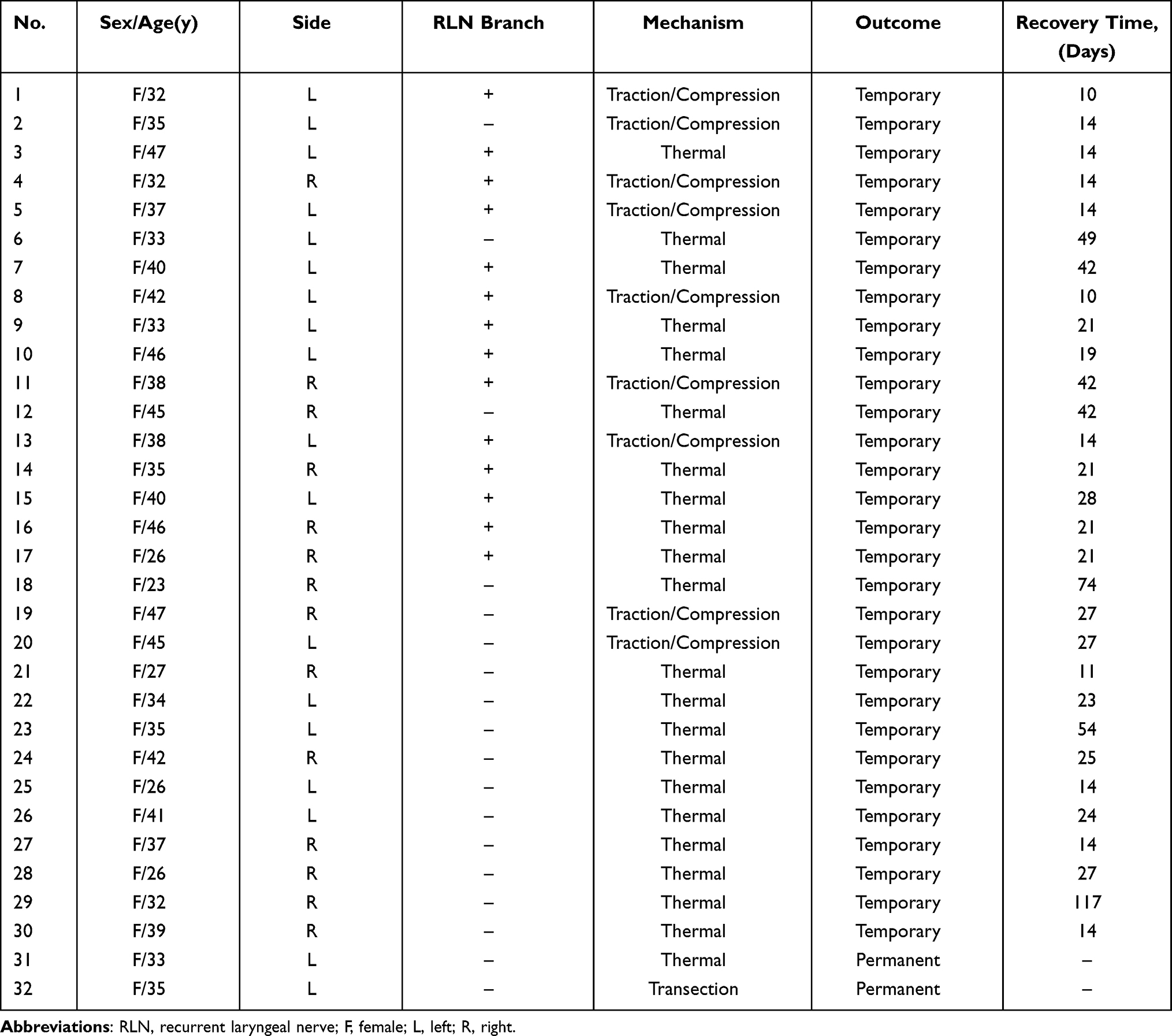 |
Table 3 Characteristics of the 32 Injured RLNs |
 |
Table 4 Mechanisms and Recovery Outcomes in RLNI |
There were more patients with left RLNI than with right RLNI. Therefore, to further investigate the effect of left and right thyroidectomy on RLNI near the NEP, the patients who underwent total lobectomy were further divided into a left lobectomy group and a right lobectomy group. Based on the statistical analysis, it was found that the age, sex, gland lobe volume, tumor size, RLN branch, operative time, Hashimoto’s thyroiditis, and hospital stay of both groups were comparable and that RLNI near the NEP was prone to occur in left lobectomy (P=0.023) (Table 5).
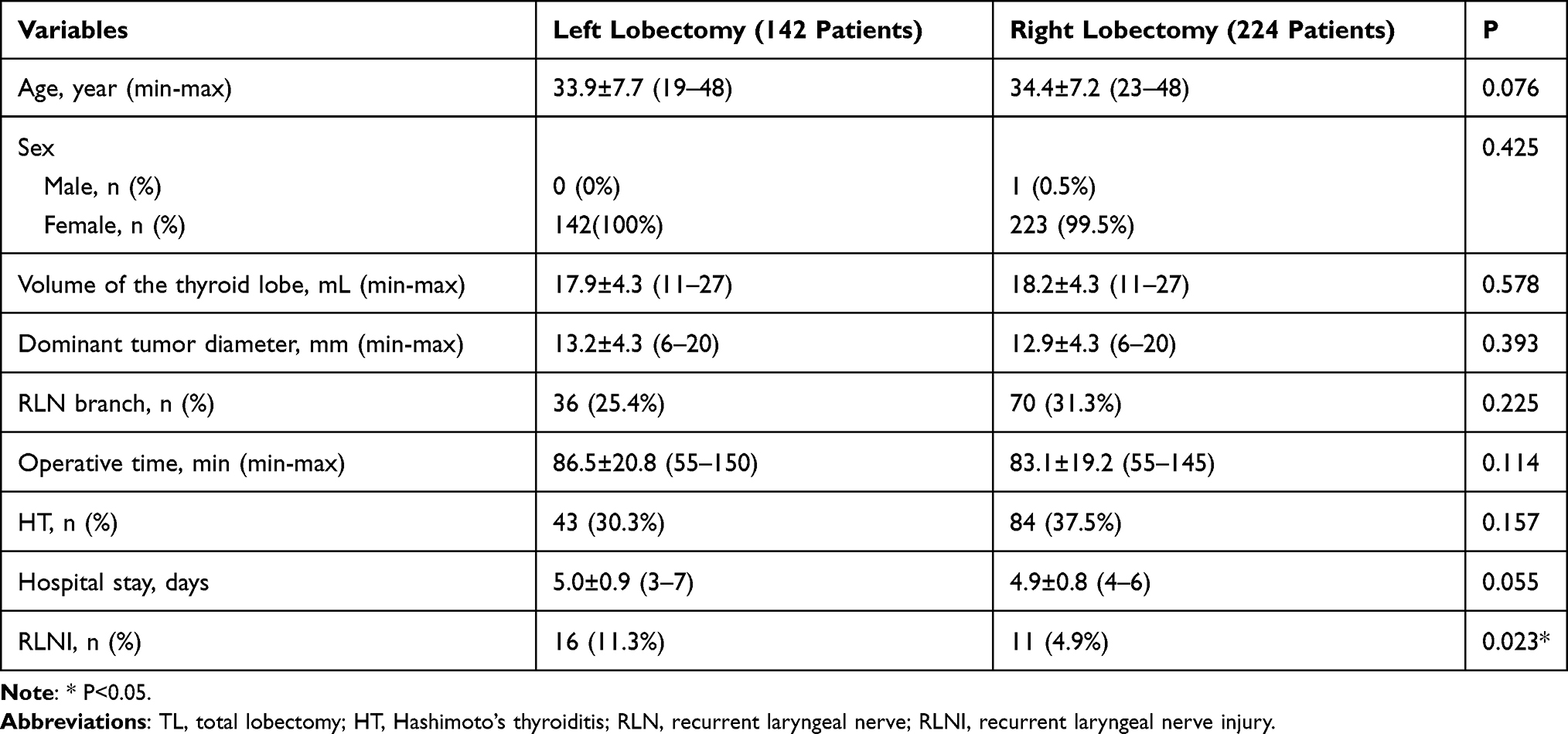 |
Table 5 Characteristics of Patients Stratified by Thyroidectomy Side (Only for the TL) |
Discussion
Although TETs were performed in patients with smaller gland lobe volume and tumor size, and hyperthyroidism was also excluded, the incidence of RLNI near the NEP (7.9%) was higher than the reported incidence of 5.1% in COT.23 In other studies, the overall incidence of RLNI in TET (2.1%-15%) was also higher than that in COT (0–4.6%).15–22 Extralaryngeal branch is the most common variant of the RLN. In this study, the incidence of extralaryngeal branch in the RLNI-positive group was higher. In previous studies, extralaryngeal branches of the RLN were found in 18.5–72% of patients.26–34 As reported in some studies, RLNI was more likely to occur if the RLN branched near the Berry’s ligament.35–37 The RLNs in about 25% of patients passed through the Berry’s ligament,38 which was more prone to injury during RLN dissection because the branched RLN was thinner and more fragile.
In this study, it was found that thermal injury was the most common cause of RLNI near the NEP in TET. Our result differed from the results from the previous studies on COT. Chiang et al described 15 cases of RLNI in 173 RLNs, of which 80% were caused by traction injury, 13% were caused by clamp injury and 7% were caused by compression injury, though there was no thermal injury.24 Snyder et al analyzed 25 cases of nerve injury in 680 RLNs and found that 56% were traction injuries, 12% were transverse or ligation injuries, 8% were compression injuries, and there was no thermal injury.39 The wide use of energy-based devices increased the number of cases of thermal injury.40 Although the RLN was more easily exposed and located with the help of the magnifying effect of the endoscope, the thermal injury of the ultrasonic scalpel during TET operation may cause RLNI.20 In addition, the dissection of the RLN in TET can only be carried out from caudal to cranial, with a down-top view. In contrast, RLN recognition and dissection in COT can be achieved through more patterns and directions.41 In this study, the incidence of traction/compression injury decreased, possibly because the traction on the gland was not as strong as that in COT. A case of transverse RLNI was reported in this study. One possible explanation is that the visualization of the distal RLN near the NEP was limited, and the lifting of the thyroid gland might cause the upward movement of the RLN. Therefore, during TET, the RLN near the NEP should be fully exposed, and the ultrasonic scalpel should be kept as far from the RLN as possible, or gauze strips should be used to protect the RLN. In addition, near-total thyroidectomy is also a safe choice to reduce RLNI near the NEP.
This study confirmed that patients with RLNI near the NEP in TET might have different prognoses. It was noted that there was no permanent VCP in patients with traction/compression injury in this study, but one patient with thermal injury developed permanent VCP. Patients with traction/compression injury had a shorter recovery time than patients with thermal injury. Chiang et al reported that 94.6% of RLNIs maintaining nerve integrity could completely recover the vocal cord motor function after the operation.7 This experience was consistent with our results in which almost all patients with traction/compression injury and thermal injury ultimately recovered their normal vocal cord motor function.
In the subgroup analysis to explore the influence of left and right sides on RLNI near the NEP, it was found that the left lobectomy group had a relatively increased probability of RLNI. If some unknown confounding factors are excluded, this phenomenon may be explained by the fact that the left RLN is more within the tracheoesophageal groove42 and the visualization of the distal RLN near the NEP was limited; therefore, the surgeon may pull the left thyroid gland harder, resulting in the occurrence of traction/compression injury and temporary RLNI.
One limitation of this study is that the causes of RLNI might be multifactorial, especially for traction and compression injuries. It is sometimes difficult to determine exactly which injury leads to RLNI. Our study is also subject to its small sample size and lack of randomization. To verify our conclusion, a large-sample randomized controlled trial is needed.
Conclusion
The extralaryngeal branch was a risk factor for RLNI near the NEP in TET. Thermal injury caused by an ultrasonic scalpel was the most common cause of RLNI near the NEP in TET. Most RLNIs that maintained nerve integrity could lead to temporary VCP, and normal vocal cord activity would eventually restore.
Abbreviations
COT, conventional open thyroidectomy; TET, total endoscopic thyroidectomy; RLNI, recurrent laryngeal nerve injury; VCP, vocal cord palsy; RLN, recurrent laryngeal nerve; IONM, intraoperative neuromonitoring; NEP, nerve entry point; LOS, loss of signal.
Acknowledgments
Supported by the Key Technology Research and Development Program of Shandong Province [grant No. 2019GSF108072].
Disclosure
The authors declare that there are no conflicts of interest related to this work.
References
1. Gagner M. Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism. Br J Surg. 1996;83(6):875. doi:10.1002/bjs.1800830656
2. Hüscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997;11(8):877. doi:10.1007/s004649900476
3. Kaplan EL, Salti GI, Roncella M, Fulton N, Kadowaki M. History of the recurrent laryngeal nerve: from Galen to Lahey. World J Surg. 2009;33(3):386–393. doi:10.1007/s00268-008-9798-z
4. Jatzko GR, Lisborg PH, Müller MG, Wette VM. Recurrent nerve palsy after thyroid operations–principal nerve identification and a literature review. Surgery. 1994;115(2):139–144.
5. Wagner HE, Seiler C. Recurrent laryngeal nerve palsy after thyroid gland surgery. Br J Surg. 1994;81(2):226–228. doi:10.1002/bjs.1800810222
6. Hermann M, Alk G, Roka R, Glaser K, Freissmuth M. Laryngeal recurrent nerve injury in surgery for benign thyroid diseases: effect of nerve dissection and impact of individual surgeon in more than 27,000 nerves at risk. Ann Surg. 2002;235(2):261–268. doi:10.1097/00000658-200202000-00015
7. Chiang F-Y, Wang L-F, Huang Y-F, Lee K-W, Kuo W-R. Recurrent laryngeal nerve palsy after thyroidectomy with routine identification of the recurrent laryngeal nerve. Surgery. 2005;137(3):342–347. doi:10.1016/j.surg.2004.09.008
8. Chan W-F, Lang B-H-H, Lo C-Y. The role of intraoperative neuromonitoring of recurrent laryngeal nerve during thyroidectomy: a comparative study on 1000 nerves at risk. Surgery. 2006;140(6):
9. Shindo M, Chheda NN. Incidence of vocal cord paralysis with and without recurrent laryngeal nerve monitoring during thyroidectomy. Arch Otolaryngol Head Neck Surg. 2007;133(5):481–485. doi:10.1001/archotol.133.5.481
10. Tomoda C, Hirokawa Y, Uruno T, et al. Sensitivity and specificity of intraoperative recurrent laryngeal nerve stimulation test for predicting vocal cord palsy after thyroid surgery. World J Surg. 2006;30(7):1230–1233. doi:10.1007/s00268-005-0351-z
11. Chan W-F, Lo C-Y. Pitfalls of intraoperative neuromonitoring for predicting postoperative recurrent laryngeal nerve function during thyroidectomy. World J Surg. 2006;30(5):806–812. doi:10.1007/s00268-005-0355-8
12. Witt RL. Recurrent laryngeal nerve electrophysiologic monitoring in thyroid surgery: the standard of care? J Voice. 2005;19(3):497–500. doi:10.1016/j.jvoice.2004.05.001
13. Marcus B, Edwards B, Yoo S, et al. Recurrent laryngeal nerve monitoring in thyroid and parathyroid surgery: the University of Michigan experience. Laryngoscope. 2003;113(2):356–361. doi:10.1097/00005537-200302000-00028
14. Pearlman RC, Isley MR, Ruben GD, et al. Intraoperative monitoring of the recurrent laryngeal nerve using acoustic, free-run, and evoked electromyography. J Clin Neurophysiol. 2005;22(2):148–152. doi:10.1097/01.wnp.0000158464.82565.32
15. Lee MC, Park H, Lee B-C, Lee G-H, Choi IJ. Comparison of quality of life between open and endoscopic thyroidectomy for papillary thyroid cancer. Head Neck. 2016;38(Suppl 1):E827–831. doi:10.1002/hed.24108
16. Kim WW, Kim JS, Hur SM, et al. Is robotic surgery superior to endoscopic and open surgeries in thyroid cancer? World J Surg. 2011;35(4):779–784. doi:10.1007/s00268-011-0960-7
17. Kim EY, Lee KH, Park YL, et al. Single-incision, gasless, endoscopic trans-axillary total thyroidectomy: a feasible and oncologic safe surgery in patients with papillary thyroid carcinoma. J Laparoendosc Adv Surg Tech A. 2017;27(11):1158–1164. doi:10.1089/lap.2016.0669
18. Xiang D, Xie L, Li Z, Wang P, Ye M, Zhu M. Endoscopic thyroidectomy along with bilateral central neck dissection (ETBC) increases the risk of transient hypoparathyroidism for patients with thyroid carcinoma. Endocrine. 2016;53(3):747–753. doi:10.1007/s12020-016-0884-y
19. Hong HJ, Kim WS, Koh YW, et al. Endoscopic thyroidectomy via an axillo-breast approach without gas insufflation for benign thyroid nodules and micropapillary carcinomas: preliminary results. Yonsei Med J. 2011;52(4):643–654. doi:10.3349/ymj.2011.52.4.643
20. Tan Z, Gu J, Han Q, et al. Comparison of conventional open thyroidectomy and endoscopic thyroidectomy via breast approach for papillary thyroid carcinoma. Int J Endocrinol. 2015;2015:239610. doi:10.1155/2015/239610
21. Tae K, Ji YB, Cho SH, Kim KR, Kim DW, Kim DS. Initial experience with a gasless unilateral axillo-breast or axillary approach endoscopic thyroidectomy for papillary thyroid microcarcinoma: comparison with conventional open thyroidectomy. Surg Laparosc Endosc Percutan Tech. 2011;21(3):162–169. doi:10.1097/SLE.0b013e318218d1a4
22. Kim SK, Kang SY, Youn HJ, Jung SH. Comparison of conventional thyroidectomy and endoscopic thyroidectomy via axillo-bilateral breast approach in papillary thyroid carcinoma patients. Surg Endosc. 2016;30(8):3419–3425. doi:10.1007/s00464-015-4624-9
23. Liu N, Chen B, Li L, et al. Mechanisms of recurrent laryngeal nerve injury near the nerve entry point during thyroid surgery: a retrospective cohort study. Int J Surg. 2020;83:125–130. doi:10.1016/j.ijsu.2020.08.058
24. Chiang F-Y, Lu I-C, Kuo W-R, Lee K-W, Chang N-C, Wu C-W. The mechanism of recurrent laryngeal nerve injury during thyroid surgery—The application of intraoperative neuromonitoring. Surgery. 2008;143(6):743–749. doi:10.1016/j.surg.2008.02.006
25. Randolph GW, Dralle H; International Intraoperative Monitoring Study Group, et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011;121 Suppl 1:S1–16. doi:10.1002/lary.21119
26. Ardito G, Revelli L, D’Alatri L, Lerro V, Guidi ML, Ardito F. Revisited anatomy of the recurrent laryngeal nerves. Am J Surg. 2004;187(2):249–253. doi:10.1016/j.amjsurg.2003.11.001
27. Beneragama T, Serpell JW. Extralaryngeal bifurcation of the recurrent laryngeal nerve: a common variation. ANZ J Surg. 2006;76(10):928–931. doi:10.1111/j.1445-2197.2006.03899.x
28. Casella C, Pata G, Nascimbeni R, Mittempergher F, Salerni B. Does extralaryngeal branching have an impact on the rate of postoperative transient or permanent recurrent laryngeal nerve palsy? World J Surg. 2009;33(2):261–265. doi:10.1007/s00268-008-9832-1
29. Cernea CR, Hojaij FC, De Carlucci D, et al. Recurrent laryngeal nerve: a plexus rather than a nerve? Arch Otolaryngol Head Neck Surg. 2009;135(11):1098–1102. doi:10.1001/archoto.2009.151
30. Fontenot TE, Randolph GW, Friedlander PL, Masoodi H, Yola IM, Kandil E. Gender, race, and electrophysiologic characteristics of the branched recurrent laryngeal nerve. Laryngoscope. 2014;124(10):2433–2437. doi:10.1002/lary.24631
31. Kandil E, Abdel Khalek M, Aslam R, Friedlander P, Bellows CF, Slakey D. Recurrent laryngeal nerve: significance of the anterior extralaryngeal branch. Surgery. 2011;149(6):820–824. doi:10.1016/j.surg.2011.02.012
32. Kandil E, Abdelghani S, Friedlander P, et al. Motor and sensory branching of the recurrent laryngeal nerve in thyroid surgery. Surgery. 2011;150(6):1222–1227. doi:10.1016/j.surg.2011.09.002
33. Makay O, Icoz G, Yilmaz M, Akyildiz M, Yetkin E. The recurrent laryngeal nerve and the inferior thyroid artery–anatomical variations during surgery. Langenbecks Arch Surg. 2008;393(5):681–685. doi:10.1007/s00423-008-0320-8
34. Uludag M, Aygun N, Isgor A. Motor function of the recurrent laryngeal nerve: sometimes motor fibers are also located in the posterior branch. Surgery. 2016;160(1):153–160. doi:10.1016/j.surg.2016.02.003
35. Chiang F-Y, Lu I-C, Chen H-C, et al. Anatomical variations of recurrent laryngeal nerve during thyroid surgery: how to identify and handle the variations with intraoperative neuromonitoring. Kaohsiung J Med Sci. 2010;26(11):575–583. doi:10.1016/S1607-551X(10)70089-9
36. Scheid SC, Nadeau DP, Friedman O, Sataloff RT. Anatomy of the thyroarytenoid branch of the recurrent laryngeal nerve. J Voice. 2004;18(3):279–284. doi:10.1016/j.jvoice.2003.08.003
37. Snyder SK, Hendricks JC. Intraoperative neurophysiology testing of the recurrent laryngeal nerve: plaudits and pitfalls. Surgery. 2005;138(6):
38. Thompson NW, Olsen WR, Hoffman GL. The continuing development of the technique of thyroidectomy. Surgery. 1973;73(6):913–927.
39. Snyder SK, Lairmore TC, Hendricks JC, Roberts JW. Elucidating mechanisms of recurrent laryngeal nerve injury during thyroidectomy and parathyroidectomy. J Am Coll Surg. 2008;206(1):123–130. doi:10.1016/j.jamcollsurg.2007.07.017
40. Dionigi G. Energy based devices and recurrent laryngeal nerve injury: the need for safer instruments. Langenbecks Arch Surg. 2009;394(3):
41. Miccoli P, Dionigi G. Tailored approach for recurrent laryngeal nerve dissection according to different endoscopic endocrine surgery. Head Neck. 2019;41(11):4060–4061. doi:10.1002/hed.25901
42. Haller JM, Iwanik M, Shen FH. Clinically relevant anatomy of recurrent laryngeal nerve. Spine (Phila Pa 1976). 2012;37(2):97–100. doi:10.1097/BRS.0b013e31821f3e86
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.