Back to Journals » Journal of Pain Research » Volume 18
Real-World Outcomes of Spinal Cord Stimulation: A Consecutive Institutional Experience with 505 Trials, Trial-to-Implant Ratio, Long-Term Efficacy, and Explantation Risk Factors
Authors Gheith R, Wortmann M, Najjar M ![]() , Oliver C, Whitlow B, Raterman B, Shackelford KR
, Oliver C, Whitlow B, Raterman B, Shackelford KR
Received 9 July 2025
Accepted for publication 15 November 2025
Published 28 November 2025 Volume 2025:18 Pages 6381—6395
DOI https://doi.org/10.2147/JPR.S552361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Dawood Sayed
Ramis Gheith, Mindy Wortmann, Michel Najjar, Christian Oliver, Bryan Whitlow, Briana Raterman, Kenneth R Shackelford
Pain Management Department, Interventional Pain Institute, St. Louis, MO, USA
Correspondence: Michel Najjar, Interventional Pain Institute, 500 Chesterfield Center Suite 250, Chesterfield, MO, 63017, USA, Tel +1636-519-8889, Fax +1 636-536-0120, Email [email protected]
Objective: This study aimed to evaluate the real-world outcomes of spinal cord stimulation (SCS) therapy in chronic pain management. Specifically, it investigated trial success rates, trial-to-permanent implant conversion, sustained post-implant efficacy, opioid use reduction, and risk factors for device explantation.
Materials and Methods: In this single-center retrospective observational cohort study, 505 adult patients who underwent SCS trials between January 2022 and January 2024 at a specialized pain management center were included. Demographic, clinical, and procedural data were extracted from electronic medical records. Trial success was defined as ≥ 50% pain relief at the time of lead pull. Permanent implant success was defined as ≥ 50% improvement in pain and function at final follow-up without explantation. Logistic regression was used to identify predictors of explantation.
Results: The mean age was 67.5 ± 12.4 years, and 64.2% of patients were female. Overall, 86.1% of patients achieved trial success, and 77.0% proceeded to permanent implantation. At follow-up (range: 3– 34 months), 76.6% of implanted patients maintained significant improvement. Patients diagnosed with diabetic neuropathy showed the highest success rate (83.3%), while patients living with CRPS had the lowest (67.6%). Opioid use decreased in 58.9% of patients. The overall explant rate was 14.1%, with loss of efficacy as the leading cause. Lead migration and infection were the most frequent complications. Tobacco use, depression, chronic opioid use, and post-implant falls were statistically significant predictors of explantation (p < 0.05).
Conclusion: SCS continues to be a clinically effective treatment for chronic refractory pain, with high trial success and durable benefit for most patients. However, certain patient-specific factors are associated with an increased likelihood of device failure and explantation. Identifying these risk factors may improve patient selection and long-term outcomes. Further prospective studies are warranted.
Plain Language Summary: Chronic pain can be life-changing and is often difficult to treat. For many people, common treatments such as medications, physical therapy, or injections do not offer enough relief. One treatment option is spinal cord stimulation (SCS), a technique where a small device is placed near the spine to send electrical signals that block pain messages from reaching the brain. We carried out this study to understand how well SCS works in the real world. We looked at the records of 505 patients who had SCS trials at a pain clinic between 2022 and 2024. First, patients tried the device temporarily. If it helped reduce their pain by at least half, they were given a permanent implant. We followed up with these patients for up to three years to see how well the treatment worked over time. We found that most patients—over 86%—felt enough pain relief during the trial to move forward with a permanent implant. Of those who received the implant, more than three-quarters continued to benefit from it at their last check-up. Many patients were able to reduce their use of opioid pain medications. However, around 14% had their devices removed, usually because the device stopped helping. Some patients also experienced complications like lead movement or infection. We also found that people with a history of depression, smoking, opioid use, or falls after the procedure were more likely to have their device removed. This study shows that SCS can be a valuable tool for people with chronic pain, especially when other treatments have not worked. It also highlights which patients may need extra care when considering this option.
Keywords: spinal cord stimulation, chronic pain, trial-to-implant ratio, explantation, neuromodulation, opioid reduction, device outcomes, lead migration
Introduction
Chronic pain remains a major global public health concern, affecting approximately 1.5 billion people worldwide.1 In the United States alone, nearly one in four adults experiences chronic pain, according to a recent report by the Centers for Disease Control and Prevention (CDC),2 with an estimated annual economic burden of $560–635 billion due to direct medical expenses and lost productivity.3 Despite the availability of pharmacological, nonpharmacological, and interventional treatment options, up to 77% of individuals report inadequate relief.4 Chronic pain has been consistently linked to increased rates of anxiety, depression,5,6 opioid misuse,7 impaired mobility, activity limitations, and diminished quality of life.8,9 These findings highlight the significant and multifaceted burden chronic pain imposes on patients, emphasizing the urgent need for more effective and sustainable treatment strategies.
Spinal cord stimulation (SCS) is an established neuromodulation therapy that has demonstrated efficacy in managing chronic pain over the past several decades.10,11 The field continues to expand, with the global SCS market projected to reach $2.8 billion by 2025.12 SCS involves the implantation of a subcutaneous pulse generator connected to electrodes via leads that traverse the epidural space over the dorsal columns of the spinal cord. By delivering controlled electrical impulses, the system disrupts nociceptive signal transmission, preventing pain signals from ascending to the brain. Patients considered for SCS typically undergo a temporary trial phase using externalized leads and a test stimulator to assess therapeutic benefit.13 Adjustable electrical stimulation is administered during this period to optimize pain control. During the study timeframe, multiple waveform modalities were available across devices, including traditional tonic stimulation, burst stimulation, and high-frequency (10 kHz) stimulation. These waveforms represent some of the most widely studied programming paradigms in contemporary spinal cord stimulation.14 Programming during the trial phase was individualized, with clinicians optimizing stimulation parameters to maximize pain relief and minimize side effects, consistent with best practices in SCS therapy. Trials are deemed successful if patients report at least a 50% reduction in pain, after which a permanent implant is considered. Trials are deemed successful if patients report at least a 50% reduction in pain, after which a permanent implant is considered.
SCS has been used to treat a variety of chronic pain conditions, including failed back surgery syndrome (FBSS, now classified as Persistent Spinal Pain Syndrome Type II [PSPS II]),15,16 complex regional pain syndrome (CRPS),17 and nonsurgical back pain (NSRBP, also referred to under PSPS II).18 Evidence for SCS efficacy in FBSS is particularly robust, with randomized controlled trials demonstrating its superiority over repeat surgery and conservative treatments for both low back and radicular leg pain.19,20 Encouraged by these findings, investigators have expanded SCS indications to include painful diabetic neuropathy,21 postherpetic neuralgia,22 intractable headache disorders,23 and chemotherapy-induced pain,24 with promising early results. Nonetheless, the long-term efficacy and sustainability of SCS remain debated. While its use continues to grow worldwide, some studies have raised concerns regarding potential placebo effects and waning therapeutic benefit over time.25,26
A particularly important challenge in SCS practice is device explantation,27 often performed when patients lose therapeutic benefit after already undergoing the risks of surgery and the substantial costs associated with implantation. Explantation for loss of efficacy represents the ultimate failure of SCS therapy, as the patient has been exposed to the burden of surgery and device expense without sustained benefit. Thus, identifying the clinical and demographic factors associated with explantation is critical for improving patient selection and optimizing long-term outcomes.
To address these uncertainties, we will conduct a retrospective review of 505 SCS trials performed at our pain management center, with patient follow-up extending up to three years. Given the range of SCS devices available on the market, the expanding list of clinical indications, and conflicting evidence regarding long-term efficacy and cost-effectiveness,12 this study will provide a broad overview of real-world SCS outcomes, including trial success, trial-to-permanent implant conversion, sustained efficacy, and risk factors for explantation.
Objectives
The primary objectives of this study were to evaluate SCS trial success rates across different device brands and diagnoses, determine the trial-to-permanent implant conversion rate, and identify factors associated with both successful and unsuccessful permanent implantation. The secondary objective was to examine potential risk factors associated with device explantation.
Study Design
This was a retrospective chart review of spinal cord stimulation (SCS) trials conducted at the Interventional Pain Institute (IPI) between January 2022 and January 2024 using a convenience sampling strategy to select participants.
Setting
The study was conducted at a single pain management center specializing in interventional treatments for chronic pain.
Methods
Patient data were extracted using the eClinicalWorks electronic medical record (EMR) system and identified through relevant Current Procedural Terminology (CPT) codes for SCS procedures. Eligible participants were adult patients aged 18 to 99 who underwent an SCS trial within the study period. Exclusion criteria included: (1) loss to follow-up after the trial; (2) incomplete data; and (3) failure to reach a minimum of three months post-implant follow-up. These inclusion and exclusion criteria were selected to ensure data reliability and consistency. The age range focused on adult patients, consistent with the approved indications for SCS. The 3-month follow-up threshold allowed for the evaluation of early treatment outcomes and complications. Excluding cases with incomplete records or lack of follow-up minimized the risk of bias due to missing data. Similarly, excluding procedures performed by providers no longer at IPI ensured standardization of clinical and documentation practices across the study sample. All included patients underwent a trial SCS procedure prior to permanent implantation, in accordance with standard recommendations. Patients were also screened using validated instruments for psychosocial factors, including depression, as part of the pre-procedural workup.28 Patients were assessed pre-procedurally and at their last known follow-up (up to January 2, 2025), using the Visual Analog Scale (VAS) for pain (0 = no pain, 10 = worst pain), Oswestry Disability Index (ODI) for functional disability (0% = no disability, 100% = maximum disability), and opioid consumption, based on medication history. For patients who underwent more than one SCS trial, only the first was included to allow for a longer and more consistent follow-up period. Improvements in VAS and ODI scores were calculated using the equation:  . A trial was defined as successful if the patient experienced a ≥50% reduction in pain at the time of lead pull. A permanent implant was considered successful if the patient sustained ≥50% improvement at the last known follow-up, without requiring device explantation. Clinical data extracted included demographic data (age, sex, BMI, smoking status, marijuana use, and opioid use), medical history (including depression and chronic opioid use), diagnosis based on ICD-10 codes [Post-Laminectomy Syndrome (PLS, historically referred to as Failed Back Surgery Syndrome [FBSS], now classified under Persistent Spinal Pain Syndrome Type II [PSPS II]), Complex Regional Pain Syndrome (CRPS), Non-Surgical Refractory Back Pain (NSRBP, also categorized under PSPS II), and Diabetic Neuropathy (DN)], type of device used, trial success, post-implant pain and function improvement, post-implant falls, and reasons for explantation if applicable. Non-Surgical Refractory Back Pain (NSRBP) includes patients with chronic back pain who have not undergone major back surgery or are not considered suitable candidates for surgery, and in whom conventional medical management (CMM) provides limited relief. This term was first introduced in a publication by Patel et al.29 Patients were followed systematically: 7 days after trial, with permanent implantation typically scheduled 3–4 weeks later if trial success criteria were met. For patients not proceeding to implant, follow-up occurred at 4 weeks to review and discuss alternative care plans. After permanent implantation, follow-ups were scheduled at 1 week, 3 weeks, then monthly for patients remaining on opioids, or at 3 months for those not using opioids, with subsequent visits every 6 to 12 months depending on ongoing clinical needs.
. A trial was defined as successful if the patient experienced a ≥50% reduction in pain at the time of lead pull. A permanent implant was considered successful if the patient sustained ≥50% improvement at the last known follow-up, without requiring device explantation. Clinical data extracted included demographic data (age, sex, BMI, smoking status, marijuana use, and opioid use), medical history (including depression and chronic opioid use), diagnosis based on ICD-10 codes [Post-Laminectomy Syndrome (PLS, historically referred to as Failed Back Surgery Syndrome [FBSS], now classified under Persistent Spinal Pain Syndrome Type II [PSPS II]), Complex Regional Pain Syndrome (CRPS), Non-Surgical Refractory Back Pain (NSRBP, also categorized under PSPS II), and Diabetic Neuropathy (DN)], type of device used, trial success, post-implant pain and function improvement, post-implant falls, and reasons for explantation if applicable. Non-Surgical Refractory Back Pain (NSRBP) includes patients with chronic back pain who have not undergone major back surgery or are not considered suitable candidates for surgery, and in whom conventional medical management (CMM) provides limited relief. This term was first introduced in a publication by Patel et al.29 Patients were followed systematically: 7 days after trial, with permanent implantation typically scheduled 3–4 weeks later if trial success criteria were met. For patients not proceeding to implant, follow-up occurred at 4 weeks to review and discuss alternative care plans. After permanent implantation, follow-ups were scheduled at 1 week, 3 weeks, then monthly for patients remaining on opioids, or at 3 months for those not using opioids, with subsequent visits every 6 to 12 months depending on ongoing clinical needs.
Ethical Considerations
An IRB waiver was granted by BeyondBound IRB (IRB ID#: BB2506RG-130) on June 17, 2025. All patient data collected were de-identified to ensure confidentiality and compliance with the Declaration of Helsinki. As the study involves a retrospective review of de-identified data, a waiver of informed consent was requested and granted, in accordance with exemption criteria.
Statistical Analysis
Data were collected from medical records and entered into Google Forms, then analyzed using the Statistical Package for the Social Sciences (SPSS) software, version 25. Descriptive statistics were used to summarize the characteristics of patients who underwent spinal cord stimulation (SCS) trials. Categorical variables were reported as frequencies and percentages, and continuous variables as means with standard deviations. Associations between variables and permanent implant success or failure were assessed using Pearson’s Chi-Square (χ2) test, Fisher’s exact test, or independent t-tests, as appropriate. A one-sample t-test was used to compare baseline and last follow-up VAS scores among patients who underwent permanent implantation. Variables that showed significant associations with implant failure in the previous statistical tests were included in a multivariable logistic regression model to identify predictors of device explantation (vs no explantation). The covariates included in the model were: age <65 years (vs ≥65), female sex (vs male), positive tobacco use history (vs negative tobacco history), positive drug use history (vs negative drug use history), obesity (vs non-obesity), baseline Visual Analog Scale (VAS) score (continuous variable), history of depression (vs non-depression), chronic opioid use (vs no chronic opioid use), and falls after implantation (vs no falls after implant). All p-values < 0.05 were considered statistically significant.
Results
Baseline Demographics and Characteristics of Study Participants
Out of 597 medical records reviewed for patients who underwent spinal cord stimulation (SCS) trials at the Interventional Pain Institute (IPI) between January 2022 and January 2024, 505 participants met the inclusion criteria and were included in the final analysis. A total of 92 patients were excluded based on the study’s exclusion criteria: 23 due to loss to follow-up after the trial, 28 due to incomplete data, and 41 because they did not reach the minimum 3-month post-implant follow-up requirement. A flowchart of study participants and their outcomes is shown in (Figure 1). The average age of the cohort was 67.5 ± 12.4 years (range: 22–91 years), with the majority being 65 years or older (325 patients, 64.4%). Females comprised 324 patients (64.2%) of the sample. The average body mass index (BMI) was 31.9 ± 7.4, with 282 patients (55.8%) classified as obese at the time of the trial. A total of 136 patients (26.9%) had a positive history of smoking. Regarding diagnoses at the time of the SCS trial, 333 patients (65.9%) had Post-Laminectomy Syndrome (PLS), 209 (41.4%) had Non-Surgical Refractory Back Pain (NSRBP), 135 (26.7%) had Complex Regional Pain Syndrome (CRPS), and 78 (15.4%) had Diabetic Neuropathy (DN). Nevro was the most used device brand (397 patients, 78.6%), followed by Abbott (93 patients, 18.4%), Boston Scientific (7 patients, 1.4%), Medtronic (6 patients, 1.2%), and Biotronik (2 patients, 0.4%). The overall pre-trial Visual Analog Scale (VAS) score averaged 8.6 ± 2.6, while the Oswestry Disability Index (ODI) was 40.3 ± 17.4. Baseline demographics and outcomes of participants who underwent SCS trials are summarized in (Table 1).
 |
Table 1 Trial Participants’ Demographics and Baseline Characteristics (N=505) |
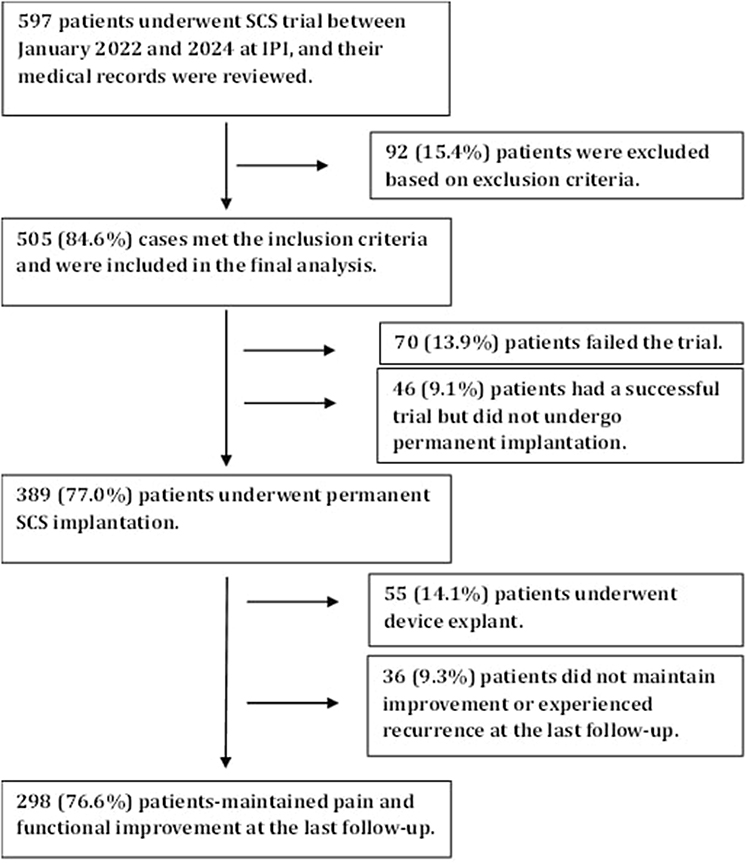 |
Figure 1 Flowchart of study participants who underwent SCS trials at IPI between January 2022 and January 2024. Out of 597 patients screened, 505 met inclusion criteria and 389 proceeded to permanent implantation after meeting the ≥50% pain relief threshold at trial completion. |
SCS Trial Outcomes
Among the 505 patients who underwent SCS trials, the overall trial success rate was 86.1%, with 435 patients experiencing at least 50% pain relief at the time of lead removal. The average percentage of pain relief following the trial was 66.2 ± 14.9%. Specifically, 175 patients (34.7%) reported 61–80% improvement, while 95 patients (18.8%) reported 81–90% improvement. The percentage of pain relief reported at lead pull is illustrated in (Figure 2). Trial success rates varied by diagnosis and device type, as shown in (Figure 3). Individuals living with NSRBP had the highest trial success rate (94.7%) followed by DN (89.7%), PLS (88.9%), and CRPS (80.0%).
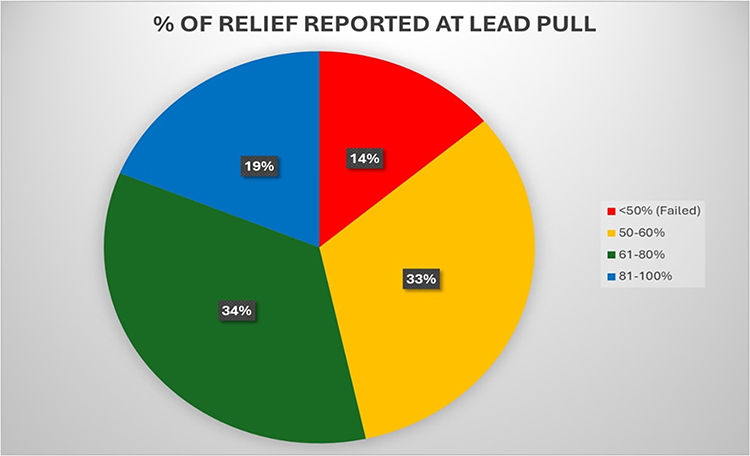 |
Figure 2 Percentage of pain relief reported at lead pull following SCS trial in 505 patients treated at IPI between January 2022 and January 2024. Trial success was defined as achieving ≥50% pain relief. |
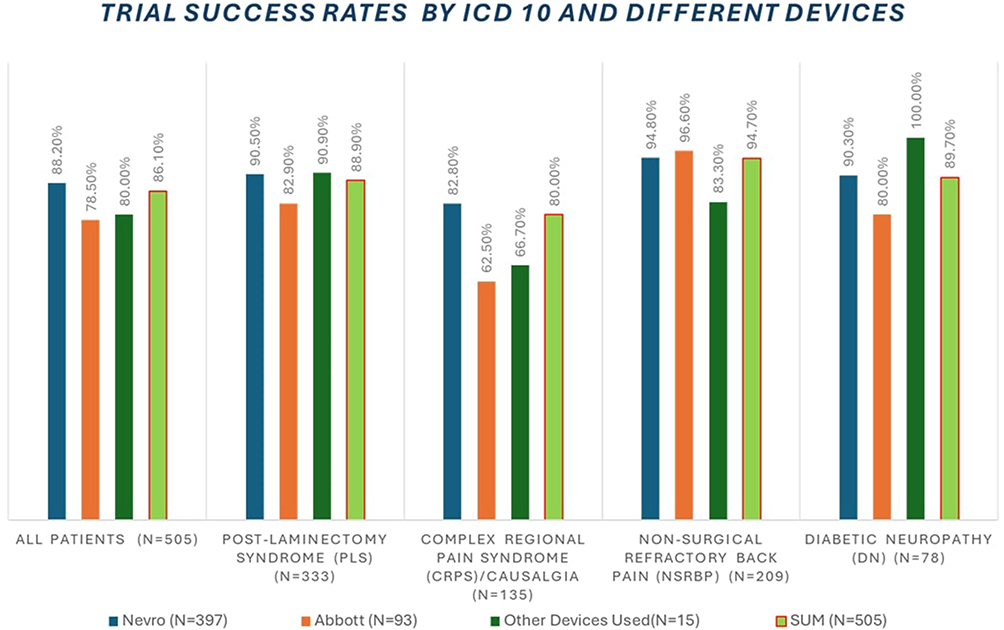 |
Figure 3 Trial success rates by diagnosis (ICD-10 classification: Post-Laminectomy Syndrome [PLS], Complex Regional Pain Syndrome [CRPS], Non-Surgical Refractory Back Pain [NSRBP], and Diabetic Neuropathy [DN]) and device manufacturer for 505 patients. Notes: Other devices used included Boston Scientific (N=7), Medtronic (N=6), and Biotronik (N=2). |
Permanent SCS Implant Outcomes
Of the 505 patients who underwent an SCS trial, 389 proceeded to permanent implantation, yielding a trial-to-implant conversion rate of 77.0% (Figure 1). These patients were retrospectively followed for an average of 13.4 ± 8.3 months (range: 3–34 months). For the 389 patients who proceeded to permanent implantation, all met the requirement of at least 3 months of follow-up. Patients who were lost before that point were excluded at the outset. Permanent implant outcomes are detailed in (Table 2). At last known follow-up, 298 of the 389 patients maintained improvement in pain and function, resulting in a permanent implant success rate of 76.6%. The mean baseline VAS pain score was 8.5 ± 0.9, which significantly improved to 4.8 ± 2.7 at the last follow-up (p < 0.001). The average improvement in pain and function was 56.5 ± 28.0%. Additionally, 229 patients (58.9%) were using less opioid medication than before implantation. Success rates for permanent implants by diagnosis are shown in (Figure 4). Individuals living with diabetic neuropathy who received SCS implants had the highest success rate (83.3%), followed by NSRBP (79.6%), PLS (77.5%), and CRPS (67.6%). At the last known follow-up, 55 patients had undergone device explantation, representing an explant rate of 14.1%. The most common reason for explantation was loss of efficacy (30 patients, 7.7%), while the most frequent complications leading to explant included lead migration (7 patients, 1.8%) and infection (5 patients, 1,3%) (Table 2). A comparison of outcomes by follow-up duration (<18 months vs ≥18 months) showed that although explantations and complications were more frequent in the <18-month group, the differences were not statistically significant (Supplementary Table 2).
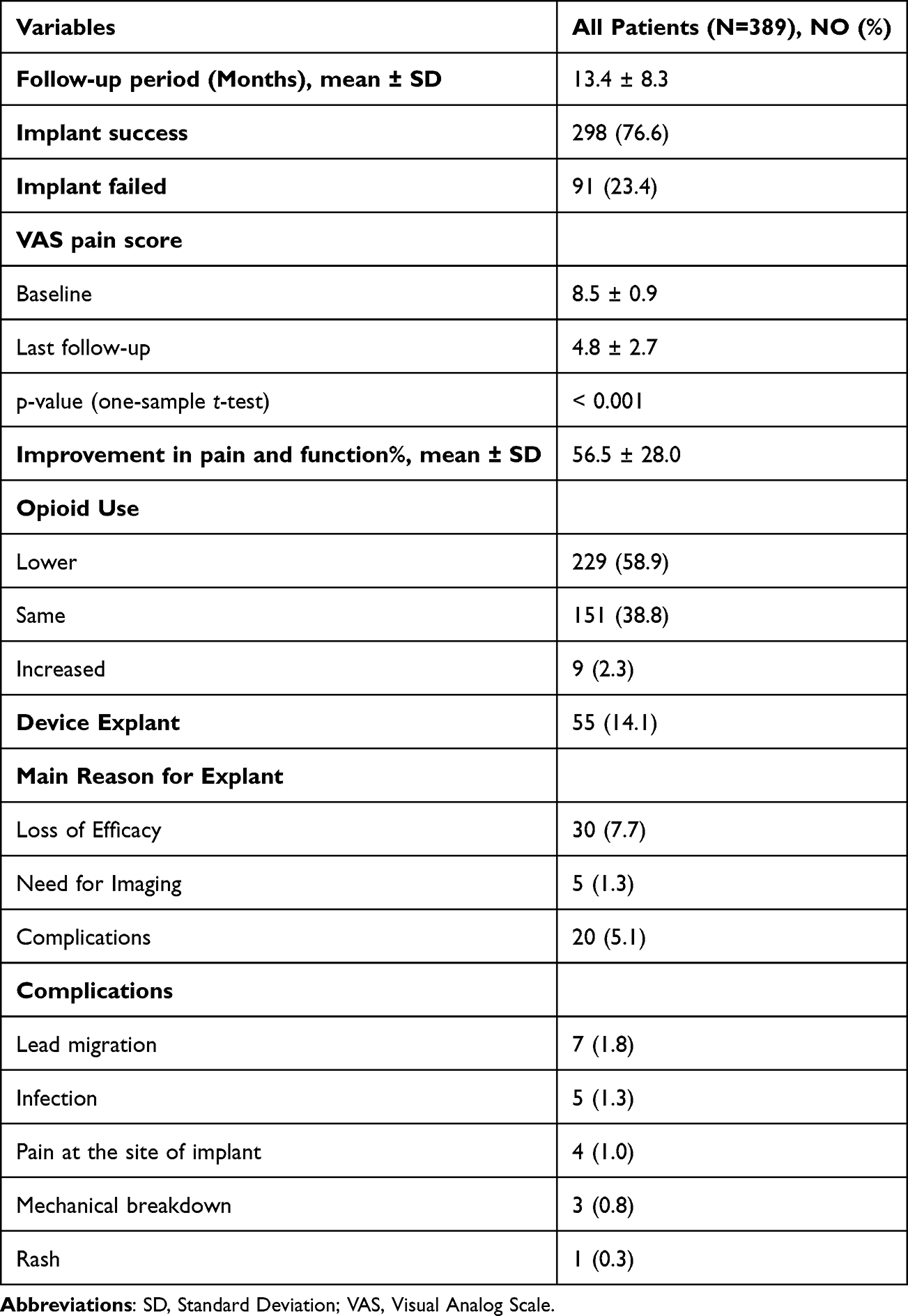 |
Table 2 Permanent Implant Outcomes |
 |
Figure 4 Permanent spinal cord stimulation (SCS) implant success rates by diagnosis (ICD-10 classification: PLS, CRPS, NSRBP, and DN) in 389 patients who underwent implantation at IPI between January 2022 and January 2024. Implant success was defined as ≥50% sustained improvement in pain and function at last follow-up (range 3–34 months) without explantation. |
Implant Explant Risk Factors
For exploring risk factors associated with permanent implant failure, participants were also divided based on permanent implant success/fail status at the last known follow-up, and comparisons of demographics and baseline characteristics between the two groups were conducted (Supplementary Table 1). Factors linked to implant failure were studied in a multivariate logistic regression analysis to identify the variables including age, sex, smoking history, drug use history, baseline VAS score, depression, chronic opioid use, and falls after implantation and their association with SCS device explant. The logistic regression model was statistically significant for the following factors: positive tobacco use history (vs negative tobacco history OR: 4.038, p-value = 0.002), history of depression (vs non-depression OR: 6.106, p-value <0.001), chronic opioid use (vs no chronic opioid use OR: 10.485, p-value <0.001), and falls after implantation (vs no falls after implant OR: 9.507, p-value <0.001), all of which were significantly associated with implant explant (Table 3).
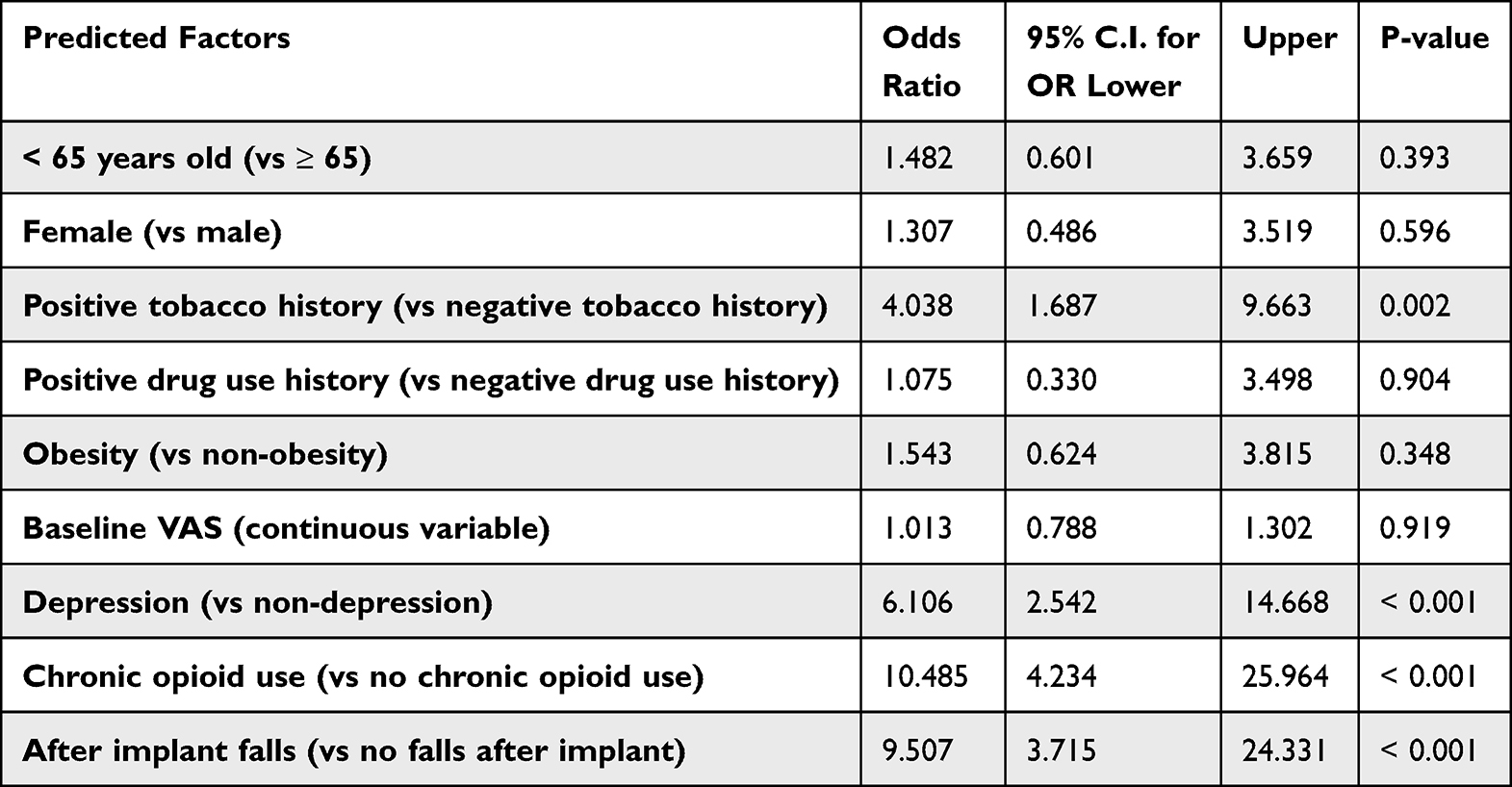 |
Table 3 Logistic Regression Analysis for the Factors Associated with Device Explant |
Discussion
Spinal cord stimulation (SCS) is a rapidly evolving field within pain medicine and has emerged as one of the most effective treatment options for chronic pain over the past five decades.20,30 Its use has grown significantly in recent years and has become a mainstay therapy for clinicians managing refractory pain conditions.31,32 For many patients, SCS offers transformative pain reduction, often succeeding in challenging clinical scenarios where other therapies have failed.33 Strong evidence supports its use in managing various chronic pain disorders, including persistent spinal pain syndrome type II (PSPS II), complex regional pain syndrome (CRPS), and peripheral neuropathies.34,35 However, its long-term efficacy has been debated, with some studies reporting diminishing benefits over time.36 Given the substantial costs associated with SCS systems, there is increasing interest in evaluating the long-term value and sustainability of this intervention.37 In this context, cost-effectiveness analyses have produced conflicting results: some studies conclude that SCS is cost-effective for conditions such as FBSS and CRPS,38 while others argue it may not offer sufficient economic value for broader chronic pain populations, especially when long-term outcomes are considered.39
Our patient demographics showed a mean age of 67.5 ± 12.4 years, with females comprising 64.2% of the cohort, consistent with prior registry data (mean age 59.1, 59.6% female).40 SCS remains an effective treatment for a variety of conditions in pain practice. At our institution, common indications included Post-Laminectomy Syndrome (PLS, now classified as Persistent Spinal Pain Syndrome Type II [PSPS II]), CRPS, Non-Surgical Refractory Back Pain (NSRBP, also referred to under PSPS II)), and Diabetic Neuropathy (DN), with PLS being the most frequent diagnosis. PLS, also known as failed back surgery syndrome, is the leading indication for SCS in the United States.41 A previous retrospective study found that CRPS and FBSS accounted for 82% of SCS cases.42 Today’s commercially available SCS devices offer various neurostimulation methods and waveform modalities.43,44 Nevro and Abbott were the predominant SCS devices used in our study. Nevro Corp.’s 10 kHz high-frequency SCS therapy has shown promising results in clinical studies, with several publications demonstrating long-term efficacy and durable pain relief for conditions like DN and NSRBP.45–47 Abbott has expanded its SCS portfolio with FDA approval for non-surgical back pain treatment.48 Abbott’s BurstDR™ stimulation also shows benefits in reducing analgesic use and improving quality of life.48,49
In our study, 86.1% of SCS trials achieved ≥50% pain relief, consistent with prior literature.40,50,51 NSRBP showed the highest trial success rate at 94.7%, aligning with reports by Kapural et al,52 who reported a 93% success rate among 145 NSRBP patients. Another RCT reported a 92.5% trial success rate in NSRBP patients.47 For PLS, our trial success rate was 88.9%, in line with a 2020 RCT,53 though lower rates have also been reported, such as 63.6% in a study by Son et al.54 Our overall trial-to-implant conversion rate was 77.0%, which is higher than the 72.4% conversion rate reported from a large digital health platform study of 7000 patients,40 and substantially above the 67% nationwide rate reported in earlier retrospective analyses.55–57 This suggests a trend toward improved conversion over recent years. The higher trial-to-permanent conversion rate at our specialized pain management center likely reflects integrated workflows, where both trial and permanent procedures were performed or closely coordinated by the same interventional team. This coordination reduces logistical delays associated with separate providers or facilities.58 Additionally, the high procedural volume and specialization of our center likely contributed to our higher conversion rates, consistent with findings that high-volume providers achieve better outcomes.56
In our cohort, 9.1% of patients had a successful trial but did not proceed to permanent implantation. From our experience, the most common reasons included fear of having a foreign device implanted in their body and other medical issues that took priority over SCS implantation.
We retrospectively followed participants from implantation for 3 to 34 months, and 76.6% sustained ≥50% improvement at the last follow-up. This is comparable to Kapural et al,14 who found that 79% of 10-kHz SCS patients achieved ≥50% back pain reduction at 12 months, with 77% maintaining this relief at 24 months. Another prospective multicenter study showed 60% of patients experienced ≥50% back pain relief and 71% experienced ≥50% leg pain relief at 24 months.51 However, the durability of SCS remains controversial.25,59 In our study, DN patients had the highest sustained success rate (83.3%), supported by a 2025 meta-analysis confirming SCS efficacy in DN,60 and a randomized study where 92.0% of DN patients reported satisfaction with SCS after 24 months.61 CRPS patients had the lowest success rate (67.6%), consistent with studies reporting diminished efficacy at 9- and 12-months,62 although a separate retrospective study found 70% continued SCS use over a median 8-year period despite limited reductions in opioid use.17
For the 389 patients who underwent permanent implantation, the mean baseline VAS pain score was 8.5 ± 0.9, which significantly improved to 4.8 ± 2.7 at the last follow-up (p < 0.001). This represents a statistically significant reduction in pain from baseline to follow-up. At last follow-up, patients reported an average 56.5 ± 28.0% pain reduction, with 58.9% using fewer opioids compared to pre-implant levels. Metzger et al63 reported 5.1- and 4.5-point reductions in pain scores at 3 and 12 months, respectively, and another study with 408-day follow-up reported sustained 5.0-point pain improvements.64 A nationwide analysis showed that 60.4% reduced opioid use, 34.2% transitioned to lower dosage groups, and 17.0% discontinued opioids.65 In contrast, a large real-world study reported no association between SCS and reduced opioid use at two years and noted increased costs and common complications.55 Another retrospective study reported loss of SCS efficacy over time, with VAS scores increasing by 1.95 points after two years.25 Our analysis yielded an explant rate of 14.1%. The most common reason for explantation was loss of efficacy, while the most frequent complications leading to explant included lead migration and infection. One of the most challenging complications to manage and mitigate has been lead migration,66 which often contributes to diminished therapeutic benefit and may necessitate revision or removal. A systematic review of 13,026 patients who underwent permanent SCS implantation between 1984 and 2024 across 25 studies found that 9.82% underwent explantation. The most common reason was lack of efficacy and inadequate pain relief (38%), followed by lead failure (15%) and infection (14%).67 In our study, we observed a higher rate of explantations among individuals with less than 18 months of follow-up, consistent with a 2025 study that reported most explantations occur within the first year.67 However, our analysis did not demonstrate any statistically significant differences in outcomes between the two follow-up groups.
Our logistic regression model showed that positive tobacco use history, history of depression, chronic opioid use, and falls after implantation were significantly associated with implant explantation (p-value <0.05). These findings are consistent with a previous retrospective database analysis,68 which also linked depression, chronic preoperative or postoperative opioid use, cannabis abuse, tobacco use, and coagulopathy to increased risk of explantation. A 2022 study has found that post-implantation falls are associated with an increased risk of poor benefit from SCS, which may indirectly contribute to explantation if patients perceive limited therapeutic value.69 Taken together, these factors highlight the interplay of both psychosocial and clinical risks in determining long-term SCS outcomes. For example, depression and chronic opioid use may reduce coping capacity, lower pain thresholds, and limit functional gains, thereby increasing the likelihood of treatment discontinuation. Tobacco use has been associated with impaired wound healing and higher infection rates, which may further elevate explant risk. Falls after implantation may cause mechanical complications such as lead migration, contributing to device failure. Previous survival analysis has also demonstrated that younger age and tobacco use are associated with an increased likelihood of SCS explantation.70 While our study found that age <65 years was associated with lower device success, it was not significantly linked to explantation in our logistic regression analysis.
Overall, our findings emphasize the importance of personalized patient selection, careful pre-implant evaluation, and coordinated care to maximize the long-term effectiveness of SCS therapy. Continued research is warranted to validate these predictors and enhance strategies that improve patient outcomes and device durability.
Study Limitations
This study has a few limitations. Its retrospective design makes it vulnerable to selection and reporting bias and relies on patient-reported outcomes, which may be subject to recall inaccuracies. Additionally, being conducted at a single high-volume center may limit the generalizability of the results to other practice settings. The absence of a control group prevents direct comparisons with other treatment modalities for chronic pain. Variability in follow-up duration (3 to 34 months; mean 13 months) may have affected the consistency of long-term outcome assessments and makes it difficult to perform more informative time-to-event analyses, such as Kaplan–Meier survival curves. Extending follow-up may be considered in future studies to provide a clearer picture of long-term efficacy and device durability. Another important limitation is the presence of potential confounding factors, as some patients may have had other sources of pain unrelated to their primary SCS indication, which could influence their reported outcomes. Prospective, multicenter studies with standardized protocols are needed to validate and expand upon these findings.
Conclusion
Overall, spinal cord stimulation remains an effective and valuable treatment option for managing chronic pain conditions, with high trial success and trial-to-permanent implant conversion rates observed in our specialized pain management center. The integrated care model and experienced providers likely contribute to these favorable outcomes. Sustained pain relief and opioid reduction were achieved in most patients, although certain factors such as tobacco use, depression, chronic opioid use, and post-implant falls were associated with increased risk of device explantation. These findings highlight the importance of careful patient selection and multidisciplinary management to optimize long-term success with SCS therapy. Further prospective studies are needed to confirm these results and refine strategies to improve durability and minimize complications.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the Ethical Principles for Medical Research Involving Human Subjects as outlined in the World Medical Association’s Declaration of Helsinki, revised in 2013. All patient data collected were de-identified to ensure confidentiality. An Institutional Review Board (IRB) waiver was granted by BeyondBound IRB (IRB ID#: BB2506RG-130) on June 17, 2025. Given that the study involved a retrospective review of de-identified data, a waiver of informed consent was requested and granted by BeyondBound IRB in accordance with the applicable exemption criteria.
Acknowledgments
We extend our sincere gratitude to everyone who participated in this study. A special thank you goes to the office manager and the entire clinical team at the Interventional Pain Institute (IPI) for their invaluable support and contributions, which were crucial to the success of this research. We also appreciate the editorial board of Pain Physician for their thorough review and constructive criticism, which greatly improved the manuscript.
Author Contributions
RG had full access to all the data in the study, participated in study design, and takes responsibility for the integrity of the data and the accuracy of the data analysis. MW participated in data collection, study design, and contributed to manuscript preparation. RG and MW provided revisions for intellectual content and final approval of the manuscript. MN wrote the study protocol, performed the statistical analysis, managed the literature review, and drafted the initial manuscript. RG, MW, CO, BW, BR, and KS participated in performing SCS trials and implants, followed up with patients, and assisted in data collection. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external funding was received for this research. All costs associated with the preparation and publication of this manuscript, including article processing charges and IRB fees, were covered by the Interventional Pain Institute (IPI). The authors did not receive any additional compensation beyond their regular salaries. IPI had no influence on the study after the protocol was finalized.
Disclosure
The authors declare no conflicts of interest related to this study. None of the authors received any remuneration beyond their regular salaries. Additionally, the authors have not received any reimbursement or honoraria in any form. All authors are affiliated with the Interventional Pain Institute.
References
1. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11(1). doi:10.1186/1471-2458-11-770
2. Lucas JW, Sohi I. Chronic pain and high-impact chronic pain among U.S. adults, 2023. 2024. doi:10.15620/cdc/169630
3. Us) M. Cover of Relieving Pain in America Relieving Pain in America: a Blueprint for Transforming Prevention, Care, Education, and Research. Nih.gov. 2015. https://www.ncbi.nlm.nih.gov/sites/books/NBK92510/.
4. Majedi H, Dehghani SS, Soleyman-Jahi S, et al. Assessment of factors predicting inadequate pain management in chronic pain patients. Anesthesiol Pain Med. 2019. doi:10.5812/aapm.97229
5. De La Rosa JS, Brady BR, Ibrahim MM, et al. Co-occurrence of chronic pain and anxiety/depression symptoms in U.S. adults: prevalence, functional impacts, and opportunities. Pain. 2022;165(3). doi:10.1097/j.pain.0000000000003056
6. Mullins PM, Yong RJ, Bhattacharyya N. Associations between chronic pain, anxiety, and depression among adults in the United States. Pain Pract. 2023;23(6). doi:10.1111/papr.13220
7. Volkow ND, McLellan AT. Opioid abuse in chronic pain — misconceptions and mitigation strategies. N Engl J Med. 2016;374(13):1253–1263. doi:10.1056/nejmra1507771
8. Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being. JAMA. 1998;280(2):147. doi:10.1001/jama.280.2.147
9. Smith BH, Elliott AM, Chambers WA, Smith WC, Hannaford PC, Penny K. The impact of chronic pain in the community. Fam Pract. 2001;18(3):292–299. doi:10.1093/fampra/18.3.292
10. Deer TR, Grider JS, Lamer TJ, et al. A systematic literature review of spine neurostimulation therapies for the treatment of pain. Pain Med. 2020;21(7):1421–1432. doi:10.1093/pm/pnz353
11. Hara S, Andresen H, Solheim O, et al. Effect of spinal cord burst stimulation vs placebo stimulation on disability in patients with chronic radicular pain after lumbar spine surgery. JAMA. 2022;328(15):1506. doi:10.1001/jama.2022.18231
12. Knotkova H, Hamani C, Sivanesan E, et al. Neuromodulation for chronic pain. Lancet. 2021;397(10289):2111–2124. doi:10.1016/S0140-6736(21)00794-7
13. Frank, Soulanis K, Rtveladze K, Kamra S, Schlueter M. Spinal cord stimulation vs medical management for chronic back and leg pain. JAMA Network Open. 2024;7(11):e2444608–e2444608. doi:10.1001/jamanetworkopen.2024.44608
14. Kapural L, Yu C, Doust MW, et al. Comparison of 10-kHz high-frequency and traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain. Neurosurgery. 2016;79(5):667–677. doi:10.1227/neu.0000000000001418
15. Taylor RJ, Taylor RS. Spinal cord stimulation for failed back surgery syndrome: a decision-analytic model and cost-effectiveness analysis. Int J Technol Assessment Health Care. 2005;21(3):351–358. doi:10.1017/s0266462305050464
16. Rigoard P, Basu S, Desai M, et al. Multicolumn spinal cord stimulation for predominant back pain in failed back surgery syndrome patients: a multicenter randomized controlled trial. Pain. 2019;160(6):1410–1420. doi:10.1097/j.pain.0000000000001510
17. Hoikkanen T, Nissen M, Ikäheimo TM, Jyrkkänen HK, Huttunen J, von Und Zu Fraunberg M. Long-term outcome of spinal cord stimulation in complex regional pain syndrome. Neurosurgery. 2021;89(4):597–609. doi:10.1093/neuros/nyab239
18. Al-Kaisy A, Palmisani S, Smith TE, et al. Long-term improvements in chronic axial low back pain patients without previous spinal surgery: a cohort analysis of 10-kHz high-frequency spinal cord stimulation over 36 months. Pain Med. 2017;19(6):1219–1226. doi:10.1093/pm/pnx237
19. Palmer N, Guan Z, Chai NC. Spinal cord stimulation for failed back surgery syndrome -- patient selection considerations. Transl Perioper Pain Med. 2019;6(3):81.
20. Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132(1):179–188. doi:10.1016/j.pain.2007.07.028
21. Henson JV, Varhabhatla NC, Bebic Z, et al. Spinal cord stimulation for painful diabetic peripheral neuropathy: a systematic review. Pain Ther. 2021;10(2):895–908. doi:10.1007/s40122-021-00282-9
22. Isagulyan ED, Tkachenko V, Semenov D, et al. The effectiveness of various types of electrical stimulation of the spinal cord for chronic pain in patients with postherpetic neuralgia: a literature review. Pain Res Manag. 2023;2023:6015680. doi:10.1155/2023/6015680
23. Towne BV, Girgiss CB, Schuster NM. Use of spinal cord stimulation in treatment of intractable headache diseases. Pain Med. 2023;24(Supplement_2):S6–S10. doi:10.1093/pm/pnad090
24. Sheldon BL, Bao J, Khazen O, Pilitsis JG. Spinal cord stimulation as treatment for cancer and chemotherapy-induced pain. Front Pain Res. 2021;2:699993. doi:10.3389/fpain.2021.699993
25. Aiudi CM, Dunn RY, Burns SM, et al. Loss of efficacy to spinal cord stimulator therapy: clinical evidence and possible causes. Pain Physician. 2017;20(7):E1073.
26. Bianco GL, Al-Kaisy A, Natoli S, et al. Neuromodulation in chronic pain management: addressing persistent doubts in spinal cord stimulation. J Anesthesia Analgesia Crit Care. 2025;5(1). doi:10.1186/s44158-024-00219-6
27. Han JL, Murphy KR, Qasim M, et al. Explantation rates and healthcare resource utilization in spinal cord stimulation. Neuromodulation. 2017;20(4):331–339. doi:10.1111/ner.12567
28. Shanthanna H, Eldabe S, Provenzano DA, et al. Evidence-based consensus guidelines on patient selection and trial stimulation for spinal cord stimulation therapy for chronic non-cancer pain. Reg Anesth Pain Med. 2023;48(6):273–287. doi:10.1136/rapm-2022-104097
29. Patel N, Calodney A, Kapural L, et al. High‐frequency spinal cord stimulation at 10 kHz for the treatment of nonsurgical refractory back pain: design of a pragmatic, multicenter, randomized controlled trial. Pain Pract. 2020;21(2):171–183. doi:10.1111/papr.12945
30. Caylor J, Reddy R, Yin S, et al. Spinal cord stimulation in chronic pain: evidence and theory for mechanisms of action. Bioelect Med. 2019;5(12). doi:10.1186/s42234-019-0023-1
31. Jeon YH. Spinal Cord stimulation in pain management: a review. Korean J Pain. 2012;25(3):143. doi:10.3344/kjp.2012.25.3.143
32. Isagulyan E, Slavin K, Konovalov N, et al. Spinal cord stimulation in chronic pain: technical advances. Korean J Pain. 2020;33(2):99–107. doi:10.3344/kjp.2020.33.2.99
33. Deer TR, Mekhail N, Provenzano D, et al. The appropriate use of neurostimulation of the spinal cord and peripheral nervous system for the treatment of chronic pain and ischemic diseases: the neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):515–550. doi:10.1111/ner.12208
34. Taylor RS. Spinal cord stimulation in complex regional pain syndrome and refractory neuropathic back and leg pain/failed back surgery syndrome: results of a systematic review and meta-analysis. J Pain Sympt Manage. 2006;31(4):S13–S19. doi:10.1016/j.jpainsymman.2005.12.010
35. Fontaine D. Spinal cord stimulation for neuropathic pain. Revue Neurolog. 2021;177(7):838–842. doi:10.1016/j.neurol.2021.07.014
36. Traeger AC, Gilbert SE, Harris IA, Maher CG. Spinal cord stimulation for low back pain. Cochrane Database Syst Rev. 2023;2023(3). doi:10.1002/14651858.cd014789.pub2
37. Lad SP, Kalanithi PS, Arrigo RT, et al. A socioeconomic survey of spinal cord stimulation (SCS) surgery. Neuromodulation. 2010;13(4):
38. Niyomsri S, Duarte RV, Eldabe S, et al. A systematic review of economic evaluations reporting the cost-effectiveness of spinal cord stimulation. Value Health. 2020;23(5):656–665. doi:10.1016/j.jval.2020.02.005
39. Brill S, Defrin R, Aryeh IG, Zusman AM, Benyamini Y. Short‐ and long‐term effects of conventional spinal cord stimulation on chronic pain and health perceptions: a longitudinal controlled trial. Eur J Pain. 2022;26(9):1849–1862. doi:10.1002/ejp.2002
40. Venkatraman V, Bharmi R, Coletti F, et al. Real world characterization of chronic pain, success rates and implant rates: evidence from a digital health platform of patients undergoing spinal cord stimulation evaluations. J Pain. 2023;24(12):2228–2239. doi:10.1016/j.jpain.2023.07.008
41. Garcia K, Wray JK, Kumar S. Spinal Cord Stimulation. PubMed; 2021. https://www.ncbi.nlm.nih.gov/books/NBK553154/.
42. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN, Cheng J. Retrospective review of 707 cases of spinal cord stimulation: indications and complications. Pain Pract. 2010;11(2):148–153. doi:10.1111/j.1533-2500.2010.00407.x
43. Russo M, Brooker C, Cousins MJ, et al. Sustained long-term outcomes with closed-loop spinal cord stimulation: 12-month results of the prospective, multicenter, open-label avalon study. Neurosurgery. 2020;87(4):E485–E495. doi:10.1093/neuros/nyaa003
44. Veizi E, Hayek SM, North J, et al. Spinal cord stimulation (SCS) with anatomically guided (3D) neural targeting shows superior chronic axial low back pain relief compared to traditional SCS—LUMINA Study. Pain Med. 2017;18(8):1534–1548. doi:10.1093/pm/pnw286
45. Argoff CE, Armstrong DG, Kagan ZB, et al. Improvement in protective sensation: clinical evidence from a randomized controlled trial for treatment of painful diabetic neuropathy with 10 kHz spinal cord stimulation. J Diab Sci Technol. 2024. doi:10.1177/19322968231222271
46. Petersen E, Stauss T, Scowcroft J, et al. Long-term efficacy of high-frequency (10 kHz) spinal cord stimulation for the treatment of painful diabetic neuropathy: 24-Month results of a randomized controlled trial. Diabetes Res Clin Pract. 2023;203:110865. doi:10.1016/j.diabres.2023.110865
47. Patel NP, Jameson J, Johnson C, et al. Durable responses at 24 months with high-frequency spinal cord stimulation for nonsurgical refractory back pain. J Neurosurg Spine. 2023;40(2):229–239. doi:10.3171/2023.9.spine23504
48. Deer TR, Gilligan C, Falowski S, et al. Treatment of refractory low back pain using passive recharge burst in patients without options for corrective surgery: findings and results from the DISTINCT study, a prospective randomized multicenter controlled trial. Neuromodulation. 2023;26(7):1387–1399. doi:10.1016/j.neurom.2023.07.009
49. Ślusarczyk WT, Nejman TJ, Laskowski M, Koperczak A, Stanuszek A, Ciekalski M. Evaluation of patient’s quality of life before and after implantation of abbott’s proclaimTM XR spinal cord stimulator with BurstDRTM stimulation in chronic pain syndrome. Medicina. 2023;59(12):2192. doi:10.3390/medicina59122192
50. Pope JE, Antony A, Petersen EA, et al. Identifying SCS trial responders immediately after postoperative programming with ECAP dose-controlled closed-loop therapy. Pain Ther. 2024;13(5):1173–1185. doi:10.1007/s40122-024-00631-4
51. Al-Kaisy A, Van Buyten JP, Smet I, Palmisani S, Pang D, Smith T. Sustained effectiveness of 10 kHz high-frequency spinal cord stimulation for patients with chronic, low back pain: 24-month results of a prospective multicenter study. Pain Med. 2014;15(3):347–354. doi:10.1111/pme.12294
52. Kapural L, Wu C, Calodney A, et al. Demographics and PainDETECT as predictors of 24-month outcomes for 10 kHz SCS in nonsurgical refractory back pain. Pain Physician. 2024;27(3):129–139.
53. North RB, Calodney A, Bolash R, et al. Redefining spinal cord stimulation “trials”: a randomized controlled trial using single-stage wireless permanent implantable devices. Neuromodulation. 2020;23(1):96–101. doi:10.1111/ner.12970
54. Son B, Kim D, Lee S, Chough C. Factors associated with the success of trial spinal cord stimulation in patients with chronic pain from failed back surgery syndrome. J Kor Neurosurg Soc. 2013;54(6):501. doi:10.3340/jkns.2013.54.6.501
55. Hussaini SMQ, Murphy KR, Han JL, et al. Specialty-based variations in spinal cord stimulation success rates for treatment of chronic pain. Neuromodulation. 2017;20(4):340–347. doi:10.1111/ner.12582
56. Murphy KR, Han JL, Hussaini SMQ, et al. The volume-outcome effect: impact on trial-to-permanent conversion rates in spinal cord stimulation. Neuromodulation. 2017;20(3):256–262. doi:10.1111/ner.12526
57. Day W, Maloy GC, Winter AD, et al. Spinal cord stimulator utilization trends and predictors of unsuccessful trial-to-implant conversion. North Am Spine Soc J. 2025;22:100616. doi:10.1016/j.xnsj.2025.100616
58. Kumar K, Rizvi S, Nguyen R, Abbas M, Bishop S, Murthy V. Impact of wait times on spinal cord stimulation therapy outcomes. Pain Pract. 2014;14(8):709–720. doi:10.1111/papr.12126
59. Dhruva SS, Murillo J, Ameli O, et al. Long-term outcomes in use of opioids, nonpharmacologic pain interventions, and total costs of spinal cord stimulators compared with conventional medical therapy for chronic pain. JAMA Neurol. 2023;80(1):18–29. doi:10.1001/jamaneurol.2022.4166
60. Abbas A, Abouelmagd M, El-Moslemani M, et al. Assessing the efficacy of spinal cord stimulation in managing painful diabetic neuropathy: a systematic review and meta-analysis. Neuromodulation. 2025. doi:10.1016/j.neurom.2025.01.016
61. Petersen EA, Stauss TG, Scowcroft JA, et al. High-frequency 10-kHz spinal cord stimulation provides long-term (24-Month) improvements in diabetes-related pain and quality of life for patients with painful diabetic neuropathy. J Diab Sci Technol. 2024. doi:10.1177/19322968241268547
62. Levy RM, Mekhail N, Kramer J, et al. Therapy habituation at 12 months: spinal cord stimulation versus dorsal root ganglion stimulation for complex regional pain syndrome type I and II. J Pain. 2020;21(3–4):399–408. doi:10.1016/j.jpain.2019.08.005
63. Metzger CS, Hammond MB, Pyles ST, et al. Pain relief outcomes using an SCS device capable of delivering combination therapy with advanced waveforms and field shapes. Expert Rev Med Devices. 2020;17(9):951–957. doi:10.1080/17434440.2020.1812383
64. De Negri P, Paz-Solis JF, Rigoard P, et al. Real-world outcomes of single-stage spinal cord stimulation in chronic pain patients: a multicentre, European case series. Interventional Pain Med. 2023;2(3):100263. doi:10.1016/j.inpm.2023.100263
65. Adil SM, Charalambous LT, Spears CA, et al. Impact of spinal cord stimulation on opioid dose reduction: a nationwide analysis. Neurosurgery. 2020;88(1):193–201. doi:10.1093/neuros/nyaa353
66. Gupta M, Abd-Elsayed A, Hughes M, Rotte A. A retrospective review of lead migration rate in patients permanently implanted with percutaneous leads and a 10 kHz SCS device. Pain Res Manag. 2021;2021:6639801. doi:10.1155/2021/6639801
67. Wahezi SE, Yener U, Naeimi T, et al. Spinal cord stimulation explantation and chronic pain: a systematic review and technology recommendations. J Pain Res. 2025;18:1327–1340. doi:10.2147/jpr.s514732
68. Hussain N, Boulos R, Malik TM, et al. Identifying predictors for early percutaneous spinal cord stimulator explant at one and two years: a retrospective database analysis. Neuromodulation. 2022;26(1):124–130. doi:10.1016/j.neurom.2022.01.021
69. Graham DT, Lambert M, Mirzadeh Z, Ponce FA. Factors contributing to spinal cord stimulation outcomes for chronic pain. Neuromodulation. 2022;25(1):145–154. doi:10.1111/ner.13515
70. Dougherty MC, Woodroffe RW, Wilson S, Gillies GT, Howard MA, Carnahan RM. Risk factors and survival analysis of spinal cord stimulator explantation. Neuromodulation. 2021;24(1):61–67. doi:10.1111/ner.13173
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.