Back to Journals » Clinical Interventions in Aging » Volume 20
Real-World Comparative Study of Ultra-Low-Dose Rivaroxaban in Very Elderly Patients with Atrial Fibrillation
Authors Han D, Ni Q, Qi J ![]() , Ni H, Wang B
, Ni H, Wang B ![]()
Received 24 July 2025
Accepted for publication 2 December 2025
Published 9 December 2025 Volume 2025:20 Pages 2467—2480
DOI https://doi.org/10.2147/CIA.S555943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Maddalena Illario
Dan Han,1 Qian Ni,2 Jialin Qi,2 Huanyu Ni,1 Baoyan Wang1
1Department of Pharmacy, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 2Department of pharmacy, Nanjing Drum Tower Hospital, Nanjing Drum Tower Hospital Clinical College, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Baoyan Wang, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, No. 321 Zhongshan Road, Nanjing, Jiangsu, 210008, People’s Republic of China, Tel +86-15161477178, Email [email protected]
Background: Optimal dosing of rivaroxaban in very elderly (≥ 80 years) nonvalvular atrial fibrillation (AF) patients remains debated, particularly concerning ultra-low-dose (5 mg daily) regimens derived from clinician judgement. This study aimed to describe real-world comparative outcomes associated with these clinician-selected dosing regimens.
Methods: The study included 1389 very elderly nonvalvular AF patients (≥ 80 years) who received rivaroxaban between January 2018 and December 2022, with 373, 604, and 412 patients receiving 5 mg, 10 mg, and 15/20 mg daily, respectively. Baseline characteristics were balanced using stabilized inverse probability of treatment weighting (IPTW). The outcomes included composite efficacy outcomes (stroke, systemic embolism, myocardial infarction and cardiovascular death) and major bleeding. Subgroup analysis and plasma trough level comparisons were conducted to further assess consistency and pharmacokinetics.
Results: The composite efficacy event rates were 9.3%, 6.6%, and 7.0% for the 5 mg, 10 mg, and 15/20 mg groups, respectively. After IPTW, there was no statistically significant difference in composite efficacy outcomes between three groups (HR for 10 mg vs 5 mg: 0.71, 95% CI: 0.44– 1.15; HR for 15/20 mg vs 5 mg: 0.91, 95% CI: 0.52– 1.59). However, major bleeding occurred in 1.6%, 3.6%, and 6.1% of patients, exhibited a dose-dependent increase. The 15/20 mg group had a 4.27-fold higher risk compared to the 5 mg group (HR: 4.27, 95% CI: 1.66– 10.97), while the 10 mg group showed no significant elevation (HR: 2.11, 95% CI: 0.82– 5.40). Subgroup analysis confirmed consistent efficacy and safety trends across specified subgroups. Plasma trough concentrations were significantly higher in the 15/20 mg group compared to the 5 mg group, with no significant difference between the 10 mg and 5 mg groups.
Conclusion: In very elderly AF patients, ultra-low-dose rivaroxaban (5 mg daily) provided comparable efficacy to higher doses while significantly reducing major bleeding. This regimen may be a balanced option for high-risk elderly populations.
Keywords: atrial fibrillation, very elderly patients, rivaroxaban, ultra-low-dose
Introduction
Atrial fibrillation (AF) is the most prevalent sustained cardiac arrhythmia globally, with epidemiological studies projecting its prevalence to escalate in parallel with population aging trends.1 Notably, individuals aged ≥80 years demonstrate an age-specific AF prevalence exceeding 10%.2 This vulnerable population presents distinct clinical challenges in AF management due to the confluence of age-associated physiological decline, multi-morbidity profiles (eg, hypertension, renal insufficiency), polypharmacy, and heightened predisposition to hemorrhage-factors that collectively complicate anticoagulation decision-making.3
The non-vitamin K antagonist oral anticoagulants (NOACs) have fundamentally transformed thromboembolic prophylaxis in AF by offering superior safety profiles and elimination of routine monitoring compared to conventional vitamin K antagonists. Rivaroxaban, a direct factor Xa inhibitor, has emerged as a cornerstone therapy endorsed by international guidelines.4,5 Current ACC/AHA and ESC guidelines recommended standard-dose rivaroxaban (20 mg once daily or 15 mg daily for reduced renal function) for stroke prevention in nonvalvular AF and did not endorse further dose reductions.6,7 However, in real-world practice, considerable variation in rivaroxaban dosing exists globally, where physicians often prescribe lower doses to mitigate bleeding risk in frail elderly patients.8,9 This divergence highlights an ongoing clinical controversy regarding whether underdosing compromises thromboembolic protection while enhancing safety, underscoring the need for real-world evidence to guide individualized anticoagulation strategies in very elderly populations. Given these competing risks, determining the optimal anticoagulant dose in elderly patients remains clinically challenging.
Emerging pharmacodynamic investigations have posited that modified rivaroxaban dosing regimens might optimize benefit-risk ratios in Asian populations. The trial (J-ROCKET AF) demonstrated non-inferior stroke prevention with reduced rivaroxaban dose (15 mg daily, 10 mg daily for creatinine clearance < 50 mL/min) versus warfarin in Japan, coupled with no significant increase in major bleeding.10 Additionally, age-related decreases in hepatic cytochrome P450 isoenzyme (CYP450) activity and renal clearance may prolong the half-life of rivaroxaban in elderly populations, as confirmed by several pharmacokinetic studies,11,12 suggesting potential for further dose de-escalation.
Notwithstanding these advances, a critical evidence gap persists regarding the efficacy-safety equilibrium of ultra-low-dose rivaroxaban (<10 mg daily) in systematically evaluated elderly AF cohorts. Current clinical practice relies primarily on empirical dose adjustments rather than evidence-based protocols tailored to extreme age groups. Given the increasing number of elderly AF patients, there is an urgent need to explore whether ultra-low-dose rivaroxaban can provide an effective and safe alternative to standard dose, particularly in this vulnerable population. This study therefore aimed to describe the real-world utilization patterns and report comparative outcomes across different physician-selected rivaroxaban doses (standard, low, ultra-low) in nonvalvular AF patients aged ≥80 years.
Methods
Study Design and Participants
This retrospective cohort study utilized data from a tertiary hospital-based nonvalvular AF registry, spanning from 1 January 2018 to 31 December 2022. Eligible patients were included based on the following criteria: (1) nonvalvular AF documented on an electrocardiogram and echocardiography during hospitalization; (2) Age ≥ 80 years; (3) Currently receiving rivaroxaban therapy. Exclusion criteria included the following: (1) Use of oral anticoagulants other than rivaroxaban (eg, warfarin, dabigatran, apixaban, or edoxaban); (2) Patients who discontinued rivaroxaban and switched to alternative oral anticoagulants during follow-up were excluded; (3) Creatinine clearance (CrCl) < 15 mL/min; (4) Liver disease with Child-Pugh class B or C (eg, acute clinical hepatitis, chronic active hepatitis, cirrhosis);4 (5) Concomitant use of drugs with both CYP3A4 and p-glycoprotein inhibitors (eg, ketoconazole, voriconazole, itraconazole, ritonavir) or strong inducers of CYP3A4 (eg, rifampin, carbamazepine, phenytoin).
Anticoagulant therapy was systematically reviewed and recorded. According to the National Medical Products Administration (NMPA)-approved prescribing information for rivaroxaban in China, the recommended dosage is 20 mg once daily (CrCl ≥50 mL/min) or 15 mg once daily (CrCl <50 mL/min). In this study, the prescribed rivaroxaban dose was based on the initial prescribed daily dose as determined by the physician according to clinical judgment. Patients were categorized into three groups based on dosage: standard dose (20/15 mg daily), low dose (10 mg daily), and ultra-low dose (5 mg daily). Medication adherence was verified through electronic prescription records, outpatient prescription reconciliation, and telephone follow-ups.
Covariates
Data were extracted from electronic medical records, including patient demographics, comorbidities, medication history, FRAIL Scale scores, CHA2DS2-VASc scores, HAS-BLED scores and renal function. The FRAIL Scale scores are a simple, validated tool used to assess frailty in older adults.13 It evaluated five key domains: fatigue, resistance, ambulation, illness and weight loss. Scores classify patients into three categories: not frail (0 points), pre-frail (1–2 points) and frail (3–5 points). The CHA2DS2-VASc score, a clinical tool to stratify stroke risk in atrial fibrillation,4 incorporates the following factors: congestive heart failure, hypertension, age ≥75 years, diabetes, prior stroke/transient ischemic attack (TIA), vascular disease, age 65–74 years, and female sex. Each factor contributes a predefined score, with cumulative totals guiding anticoagulation decisions. The HAS-BLED score estimates bleeding risk in anticoagulated AF patients,4 accounting for uncontrolled hypertension, abnormal renal/hepatic function, prior stroke, bleeding history or predisposition, labile international normalized ratio (INR), advanced age (>65 years), and concomitant use of alcohol or drugs predisposing to hemorrhage. Renal function was assessed by calculating CrCl using Cockcroft-Gault formula: CrCl = [(140 − age) × weight (kg) × 1.23/serum creatinine (μmol/L)] (×0.85 for females). Actual body weight was used for all patients due to lack of standardized adjustments in the dataset.
Study Outcomes
The efficacy outcome comprised a composite of stroke, systemic embolism, myocardial infarction and cardiovascular death, as well as each individual outcome. The safety outcome was major bleeding according to the definition of the International Society on Thrombosis and Haemostasis (ISTH) criteria.14 Patients could experience multiple outcomes during the study period, but only the first event was included in the analysis. All outcomes were blindly adjudicated by two independent clinicians. Discrepancies were resolved by a third-party senior specialist through a centralized review. The follow-up period was defined as the interval from initiation of anticoagulant therapy to the first occurrence of any outcome or the study end date (31 December 2024), whichever occurred first. The study was designed with a planned 2-year observation period.
Stroke was defined as sudden onset of a focal neurologic deficit consistent with a major cerebral artery territory, persisting >24 hours and not attributable to other causes (eg, metabolic disorders or trauma).15 Strokes were categorized as ischemic, hemorrhagic, or unspecified and confirmed by computed tomography (CT) or magnetic resonance imaging (MRI). Systemic embolism was characterized by the sudden abrupt vascular insufficiency, accompanied by clinical or radiological evidence of arterial occlusion, in the absence of other probable etiologies such as atherosclerosis, invasive procedures, or trauma.16 Acute myocardial infarction was defined according to the Fourth Universal Definition of Myocardial Infarction, including elevated cardiac troponin (≥99th percentile upper reference limit) and at least one of the following: (1) symptoms of acute myocardial ischemia (eg, chest pain, shortness of breath); (2) new ischemic electrocardiogram (ECG) changes (eg, ST-segment elevation/depression, T-wave inversion); (3) imaging evidence of loss of viable myocardium or new regional wall motion abnormalities; (4) identification of a coronary thrombus via angiography or autopsy.15 Cardiovascular death was classified as sudden cardiac arrest, acute myocardial infarction, ischemic stroke, heart failure, cardiogenic shock, immediate complications from a cardiovascular procedure, and other cardiovascular causes.15
Major bleeding was defined as clinically overt bleeding associated with any of the following: fatal outcome, involvement of critical site (eg, intracranial, spinal, ocular, articular or retroperitoneal), hemoglobin drop >2 g/dL, transfusion of >2 units of whole blood or red blood cells, or permanent disability.14
Statistical Analysis
Study participants were classified according to the initial dose of rivaroxaban prescribed at cohort entry. This first exposure carried forward (FECF) assignment was maintained throughout follow-up, regardless of subsequent dose modifications or temporary interruptions. This approach aligns with the objective to evaluate outcomes associated with the initial dosing decisions of clinicians for elderly AF patients, which represent a key therapeutic choice point in real-world practice.
To evaluate clinical outcomes between different groups, the stabilized inverse probability of treatment weighting (IPTW) approach was implemented to enhance covariate balance and improve comparability. Propensity scores were calculated via multivariable logistic regression incorporating baseline covariates. Subsequently, stabilized weights derived from these scores were applied to generate a pseudo-population maintaining the original cohort size. Covariate balance was assessed by standardized mean differences (SMD) before and after stabilized IPTW, with imbalance defined as SMD >10%. Differences in clinical outcomes between different groups were analyzed through Kaplan–Meier method, using Log Rank test for survival curve difference. The proportional hazards assumption was verified through diagnostic analysis of Schoenfeld residuals, confirming adherence for all models. Hazard ratios (HRs) were calculated using the multivariate Cox proportional risk model, with the 5 mg group as reference.
In survival analysis, competing risks (eg, non-cardiovascular deaths) may bias traditional estimates. We utilized competing risk regression (Fine and Gray method) to account for the presence of non-cardiovascular deaths as competing events. Cumulative incidence functions (CIFs) were estimated using the Aalen-Johansen estimator, and Gray’s test was applied to compare CIFs between treatment groups. Sub-distribution HRs and 95% CIs were calculated via multivariable regression adjusted for the covariates (Table S1).
Risk of clinical outcomes in specified subgroups (age, gender, CrCl category, FRAIL Scale scores, CHA2DS2-VASc scores and HAS-BLED scores) was assessed. For subgroup analysis, multivariate Cox proportional hazards regression and propensity score methods were employed. The significance of interaction between the treatment group and subgroup was defined as P-for-interaction <0.05.
To assess the robustness of causal effect estimates, we conducted a sensitivity analysis using Targeted Maximum Likelihood Estimation (TMLE). As a doubly robust approach, TMLE provides consistent estimation of the causal effect of exposure factors on clinical outcomes. Given the inherent risk of unmeasured confounding in observational retrospective designs, TMLE simultaneously fits an outcome regression model and a propensity score model. This approach exhibits double robustness: consistent estimators are attained when either model is correctly specified. The risk difference (RD) and relative risk (RR) were calculated. Data analysis was conducted using R software (version 4.5.0).
Results
Patient Characteristics
Between 2018 and 2022, a total of 1389 patients were enrolled in the study and categorized into three treatment groups: 373 patients receiving 5 mg, 604 patients receiving 10 mg, and 412 patients receiving 15/20 mg (Table 1). Patients in the 5 mg group had older age, greater use of antiplatelet agents, and elevated HAS-BLED scores. Conversely, the 10 mg group showed a higher prevalence of congestive heart failure, along with higher FRAIL scale scores. Furthermore, significant differences were observed in the distribution of renal function among the three groups. After IPTW, all baseline characteristics were effectively balanced between the three groups, ensuring a more reliable comparative analysis (Table 2).
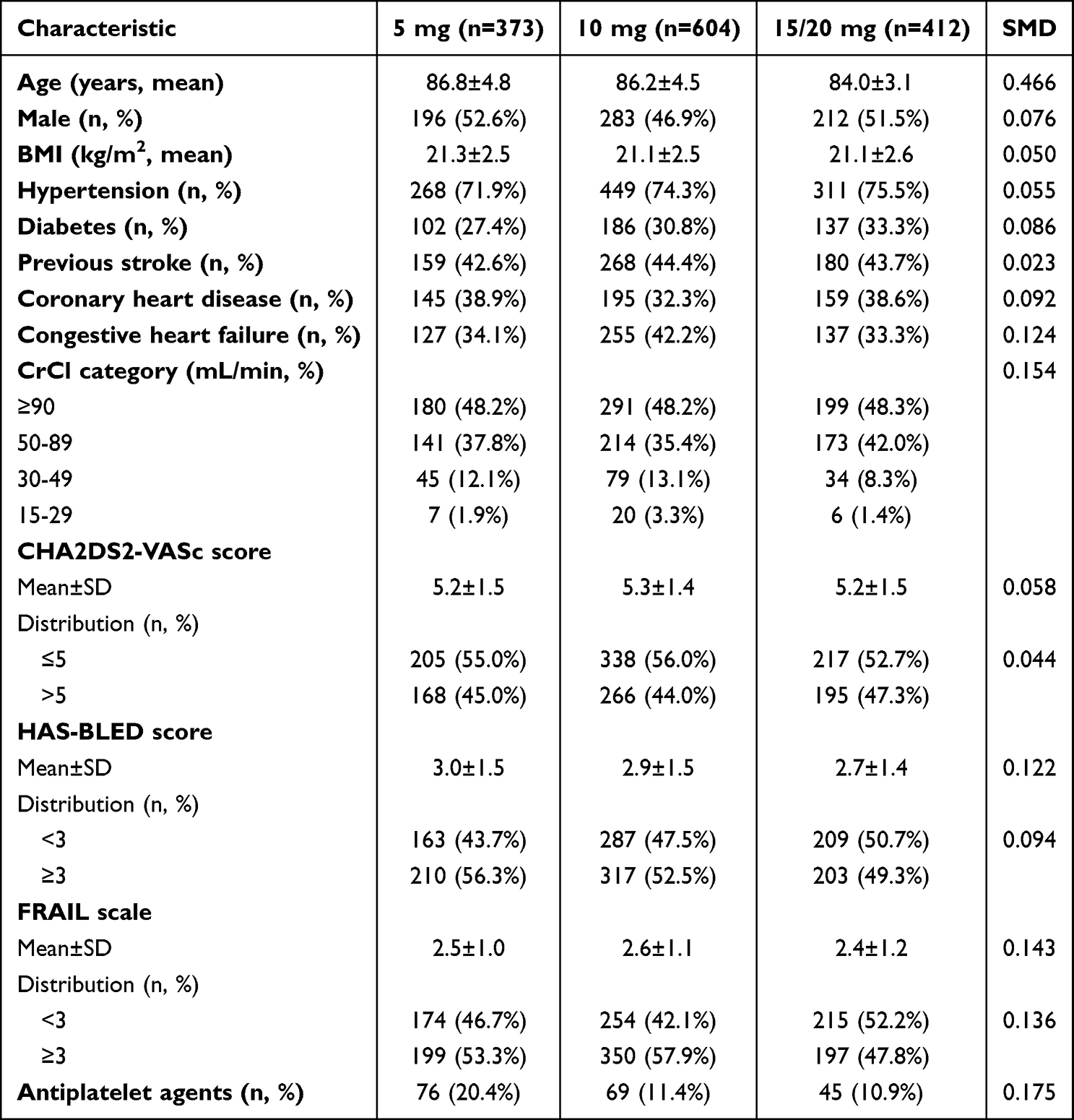 |
Table 1 Baseline Characteristics of Patients Receiving Different Doses of Rivaroxaban Before IPTW |
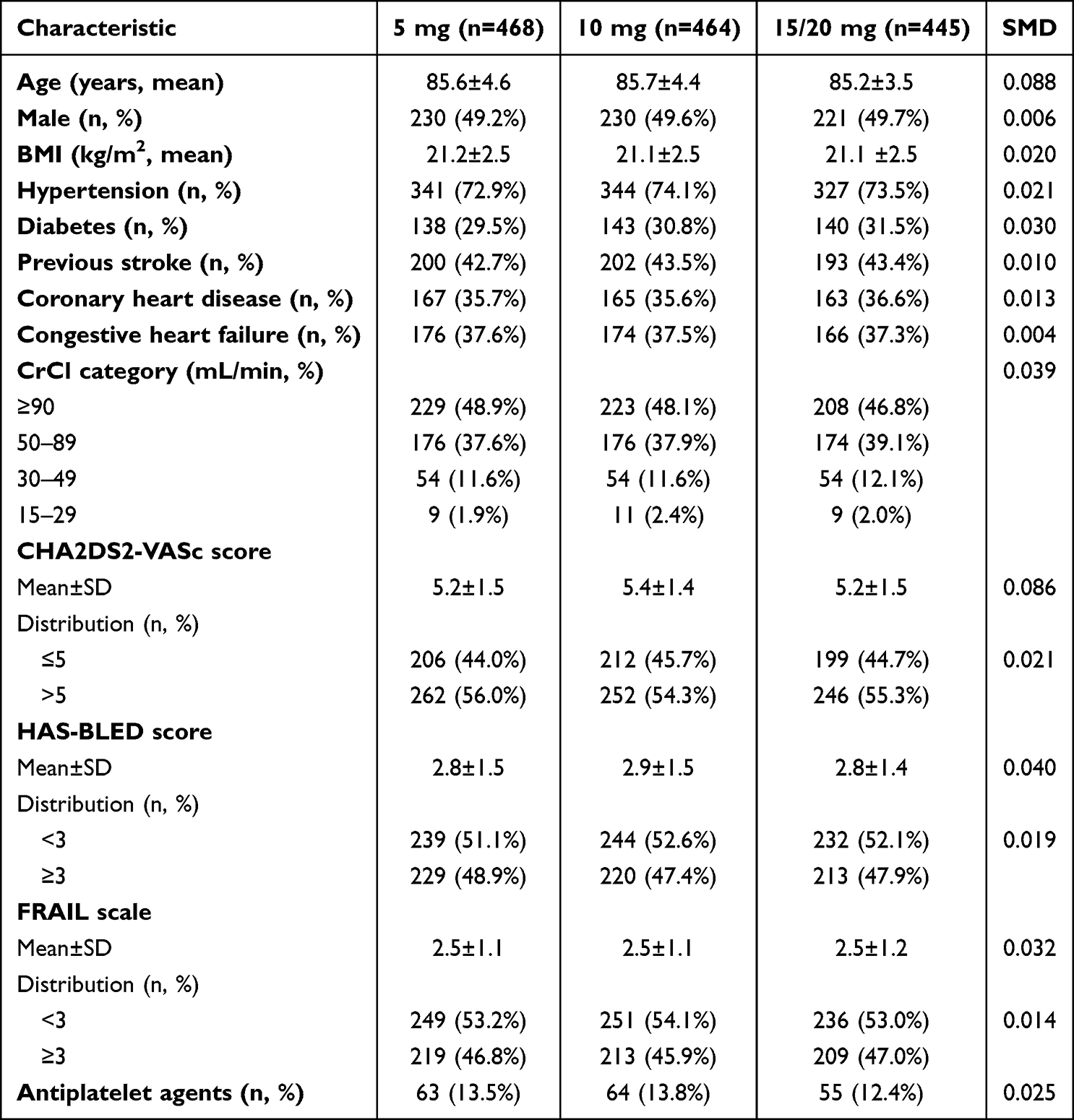 |
Table 2 Baseline Characteristics of Patients Receiving Different Doses of Rivaroxaban After IPTW |
Clinical Outcomes
The incidence rates for composite outcomes and major bleeding were presented in Figure 1. After adjustment, the cumulative incidence curves for composite outcomes showed no significant separation among the 5 mg, 10 mg, and 15/20 mg groups (Figure 2A). Compared to the 5 mg group, neither the 10 mg group (HR: 0.71, 95% CI: 0.44–1.15) nor the 15/20 mg group (HR: 0.91, 95% CI: 0.52–1.59) exhibited a statistically significant reduction in composite outcomes risk (Figure 1). Similarly, no dose-dependent differences were observed in individual components of the composite outcomes, including stroke, systemic embolism, myocardial infarction, or cardiovascular death.
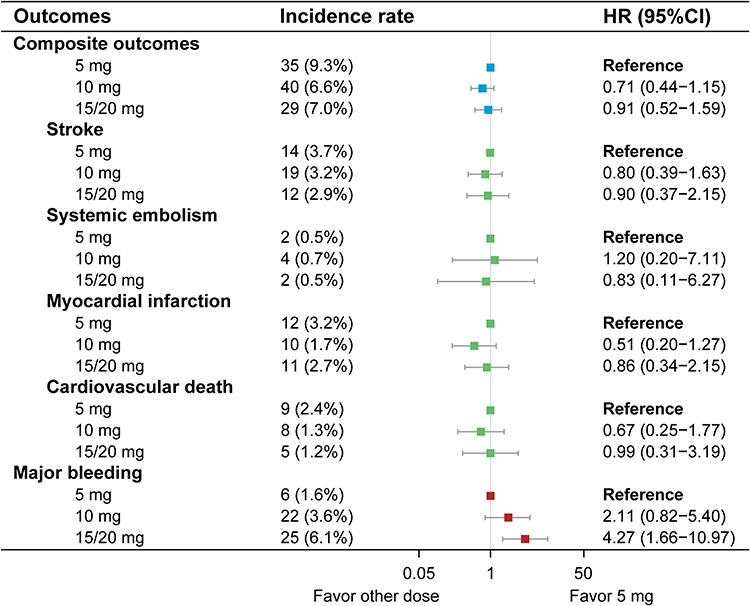 |
Figure 1 Forest plot showing hazard ratios for clinical outcomes comparing the 10 mg and 15/20 mg groups with the 5 mg reference group. |
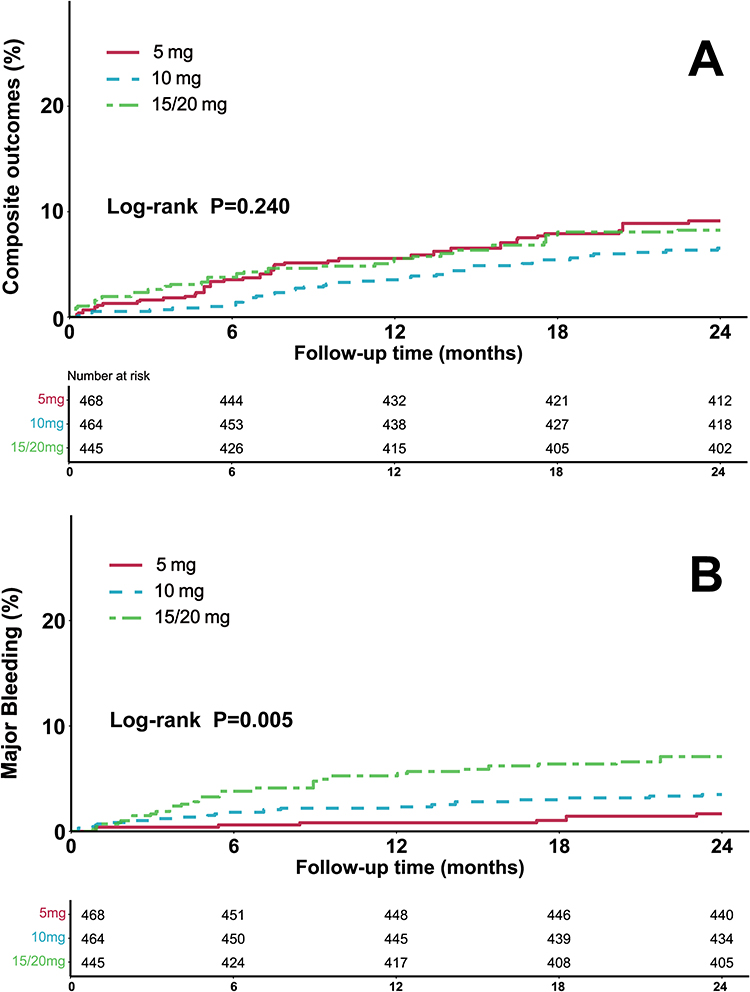 |
Figure 2 Cumulative incidence curves for composite outcomes (A) and major bleeding (B) in very elderly patients with nonvalvular AF taking different doses of rivaroxaban after IPTW. |
In contrast, the cumulative incidence curves for major bleeding demonstrated clear separation across dose groups (Figure 2B). The lowest cumulative incidence was observed in the 5 mg group, followed by the 10 mg group, with the highest incidence occurring in the 15/20 mg group, indicating a clear dose-dependent relationship with major bleeding risk. The 15/20 mg dose was associated with a 4.27-fold increased risk of major bleeding compared to the 5 mg group (95% CI: 1.66–10.97), whereas the 10 mg group showed no significant risk elevation (HR = 2.11, 95% CI: 0.82–5.40).
Fine-Gray competing risk model test revealed that the 15/20 mg group had the highest cumulative risk of major bleeding than that of the 5 mg group (Fine-Gray P = 0.005, Figure S1), while no statistically significant difference was observed between the different dose groups for composite outcomes (Fine-Gray P = 0.245). The results of the sub-distribution hazard function in the Fine-Gray model were shown in Table S1, and the results were consistent with the multivariate COX proportional risk model.
Subgroup Analysis
Subgroup analysis was performed based on age, gender, CrCl category, FRAIL Scale scores, CHA2DS2-VASc scores and HAS-BLED scores to evaluate the differences in composite outcomes and major bleeding risk across patient populations (Figures 3 and 4). Patients aged ≤85 years receiving the 10 mg group demonstrated a statistically significant 64% reduction in composite outcomes risk compared to the 5 mg group (HR: 0.36, 95% CI: 0.16–0.81). A similar benefit was observed in patients with normal renal function, where 10 mg administration was associated with a 56% lower risk of composite outcomes (HR: 0.44, 95% CI: 0.22–0.90). Conversely, the 15/20 mg group exhibited substantial heterogeneity in major bleeding risk. Patients ≤85 years experienced a 4.87-fold increased major bleeding risk (HR: 4.87, 95% CI: 1.09–21.86), with amplified hazards observed in female patients (HR: 5.34, 95% CI: 1.45–19.68) and those with renal insufficiency (HR: 4.38, 95% CI: 1.39–13.77). This elevated major bleeding propensity was extended to other distinct populations including those with FRAIL Scale scores ≥3 (HR: 5.00, 95% CI: 1.35–18.49), CHA2DS2-VASc scores ≤5 (HR: 4.94, 95% CI: 1.30–18.76), and HAS-BLED scores ≥3 (HR: 7.93, 95% CI: 1.00–63.12). Although, subgroup analysis demonstrated variable risks of composite outcomes and major bleeding across clinically stratified populations, no significant dose-dependent interaction effects were observed between treatment groups and subgroup stratifications (P-interaction >0.05 for all).
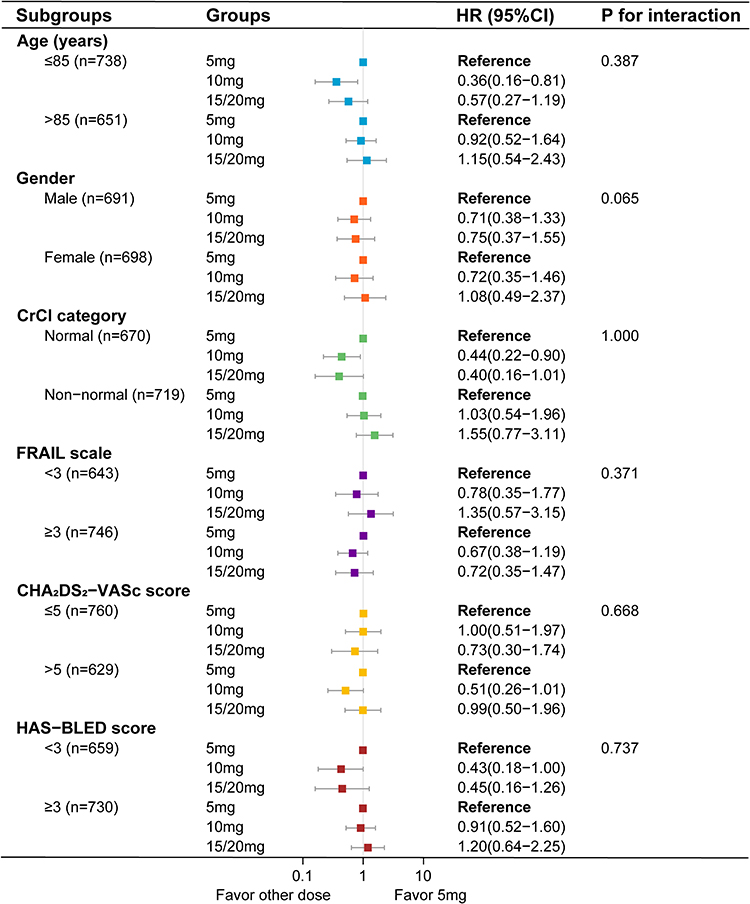 |
Figure 3 Risk of composite outcomes for the 10 mg and 15/20 mg groups compared with the 5 mg reference group, according to various subgroups. |
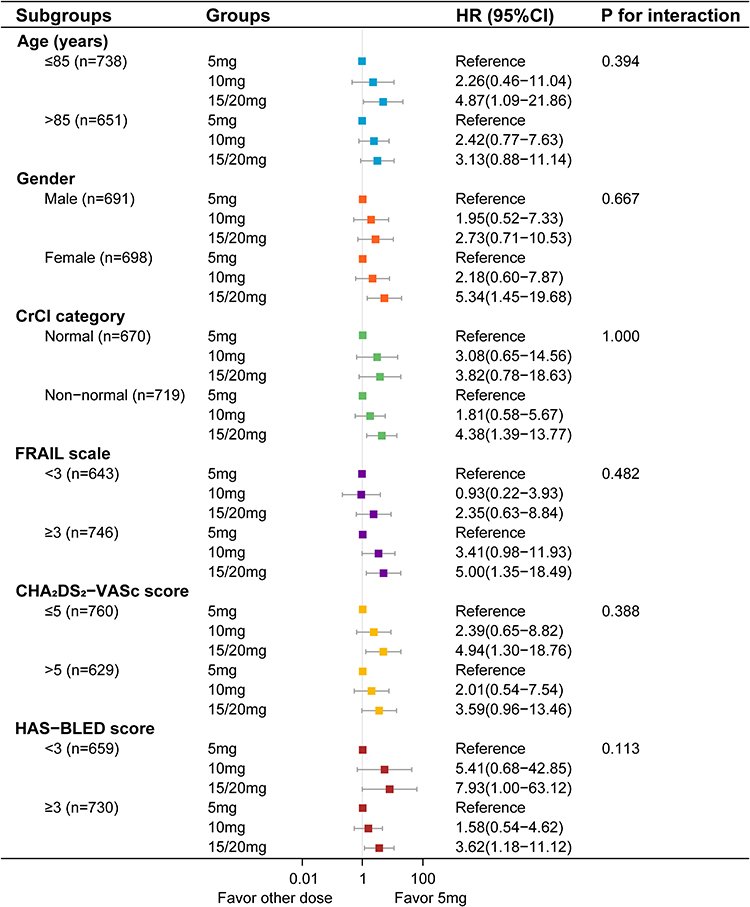 |
Figure 4 Risk of major bleeding for the 10 mg and 15/20 mg groups compared with the 5 mg reference group, according to various subgroups. |
Sensitivity Analysis
Using the TMLE method, there were no statistically significant differences between either the 10 mg group (RD: −0.023, 95% CI: −0.058–0.011; RR: 0.743, 95% CI: 0.485–1.140) or the 15/20 mg group (RD: 0.006, 95% CI: −0.044–0.055; RR: 1.067, 95% CI: 0.613–1.859) versus the 5 mg reference group for the composite outcomes (Table S2). In the analysis of major bleeding, the 10 mg group showed a non-significant elevated risk trend (RD: 0.019, 95% CI: −0.001–0.038; RR: 2.154, 95% CI: 0.891–5.207). A clinically significant increase was observed in the 15/20 mg high-dose group (RD: 0.049, 95% CI: 0.023–0.075; RR: 4.361, 95% CI: 1.727–11.010). Notably, the results derived through TMLE method demonstrated strong concordance with those from IPTW analysis.
Plasma Concentration
The steady-state trough concentration of rivaroxaban was measured in some patients (n = 222). Boxplot analysis revealed the distribution of rivaroxaban concentrations across the study groups (Figure 5). The median concentration in the 5 mg group was 18.8 ng/mL (IQR: 11.6–28.3 ng/mL). Higher doses corresponded to increased median concentrations: 26.0 ng/mL (IQR: 12.5–39.0 ng/mL) in the 10 mg group, and 34.9 ng/mL (IQR: 16.8–61.8 ng/mL) in the 15/20 mg group. Multiple linear regression, adjusted for covariates, confirmed significant differences between dosage groups. Compared to the 5 mg group, the 15/20 mg group had a significantly higher plasma concentration (P < 0.001), while no significant difference was observed in the 10 mg group (P = 0.084). The trough concentrations increased with declining renal function across all dose groups (Figure S2); however, the 5 mg group exhibited less pronounced fluctuations across CrCl category compared to other groups, with a weak correlation to CrCl.
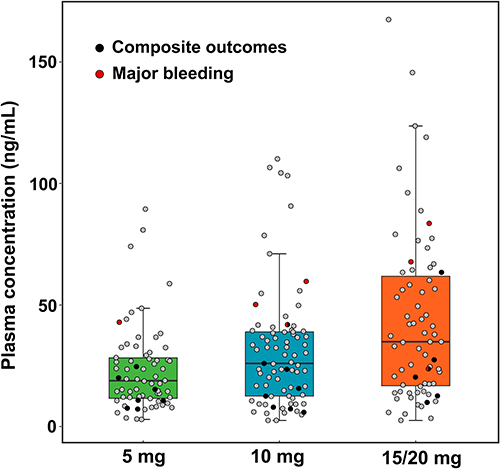 |
Figure 5 Steady-state trough concentrations of rivaroxaban at different doses. Black solid dots represent composite outcomes and red solid dots represent major bleeding. |
Discussion
The present study investigated the comparative outcomes of ultra-low-dose rivaroxaban (5 mg) compared to low/standard doses (10 mg and 15/20 mg) in very elderly patients with nonvalvular AF. The key findings demonstrated that although the composite efficacy outcomes did not differ significantly across dose groups. Specifically, a marked dose-dependent increase in major bleeding risk was observed, with the 15/20 mg group exhibiting a 4.27-fold higher risk than the 5 mg group. Notably, the 5-mg dose neither significantly increased composite outcomes nor elevated major bleeding. These results underscored the potential benefits of ultra-low-dose rivaroxaban in balancing stroke prevention and bleeding safety for this vulnerable population.
Emerging evidence has revealed a complex dose-response relation of NOACs therapy in elderly atrial fibrillation populations. While the J-ROCKET AF trial established the efficacy and safety profile of reduced-dose rivaroxaban (15 mg daily; 10 mg for CrCl <50 mL/min) in Asian cohorts, its subgroup analysis revealed heightened bleeding risks among elderly patients compared to warfarin (25.05% vs 16.95% per year; HR = 1.49, 95% CI: 1.02–2.16), with a significant age-dose interaction for safety outcomes.17 A retrospective cohort study demonstrated increased bleeding but equivalent effectiveness (all-cause mortality, myocardial infarction, stroke, systemic embolism and venous thromboembolism) between standard and reduced-dose NOACs in multimorbid elderly AF patients (≥65 years), supporting dose reduction strategies in frail populations.18 Although these studies differed in design and population characteristics from our analysis, their overall observations were conceptually consistent with our findings of no increase in composite efficacy outcomes between low- and standard-dose regimens, suggesting that bleeding susceptibility rather than thromboembolic protection may be the predominant dose-limiting factor in elderly patients. Nevertheless, a nationwide cohort study cautioned against excessive dose reduction in the elderly atrial fibrillation population (≥80 years), revealing that very-low-dose NOACs increased the risk of major adverse limb events (HR: 1.54, 95% CI: 1.09–2.18), venous thrombosis (HR: 3.75, 95% CI: 1.56–8.97), and all-cause mortality (HR: 1.21, 95% CI: 1.15–1.29) compared with regular-dosage NOACs, despite comparable ischemic stroke/systemic embolism and major bleeding.19 These discrepancies were corroborated by a systematic review demonstrating that off-label underdosing of NOACs elevated ischemic stroke or systemic embolism risk (HR: 1.17, 95% CI: 1.00–1.38) versus on-label dosing without reducing major bleeding (HR: 0.91, 95% CI: 0.76–1.10) in patients beyond elderly populations.20 Interestingly, the edoxaban low-dose for elder care atrial fibrillation patients (ELDERCAGE-AF) trial revealed that ultra-low-dose edoxaban (15 mg daily) demonstrated superior efficacy compared with placebo in reducing stroke or systemic embolism incidence while maintaining non-inferior safety profiles regarding major bleeding.21 Therefore, the lack of significant efficacy differences across doses in elderly patients contrasted with earlier reports of dose-dependent efficacy in younger cohorts. This discrepancy may reflect unique pathophysiological features in very elderly patients, including altered drug metabolism, frailty, or competing comorbidity-related risks, which attenuated the dose-response relationship for thromboprophylaxis while amplifying bleeding susceptibility. Our study extended these observations by exploring even lower doses (5 mg) in patients ≥80 years.
In this study, the annualized rate of stroke or systemic embolism was higher in all rivaroxaban dose groups than those reported in prior randomized controlled trials (RCTs) involving AF patients.10,22 This could be attributed to age being an independent risk factor for thromboembolic events in AF patients. The cumulative incidence of thromboembolism exhibited an age-dependent escalation: annual stroke incidence was approximately 1.5% in AF patients aged 50–59 years, rising to 23.5% in those aged 80–89 years.23 Notably, the ultra-low-dose rivaroxaban regimen evaluated in our study demonstrated no statistically significant reduction in thromboembolic events, including ischemic stroke or systemic embolism. Regarding safety outcomes, the annualized major bleeding rate observed with 15/20 mg rivaroxaban dosing aligned with standard-dose profiles from previous RCTs,10,22 whereas the ultra-low-dose rivaroxaban exhibited significantly reduced major bleeding, achieving a safety profile comparable to that of non-anticoagulated patients.23 Therefore, the ultra-low-dose rivaroxaban may be appropriate for selected high-risk elderly patients, particularly those with a hemorrhagic predisposition or extremely advanced age.
While subgroup analysis demonstrated numerical variations in composite outcomes and major bleeding risks across populations (eg, age, renal function, frailty), the absence of statistically significant interaction effects (P-interaction >0.05 for all subgroups) underscored the robustness of ultra-low-dose rivaroxaban (5 mg) as a universally applicable strategy for elderly AF patients. These findings suggested that the efficacy and safety of the 5 mg dose remained consistent regardless of age stratification, renal function, frailty status, or baseline stroke/bleeding risk scores. The lack of proven heterogeneity across subgroups reinforced the practicality of adopting a simplified dosing regimen for this highly vulnerable population, particularly given their frequent polypharmacy, impaired medication adherence, and limited tolerance for complex therapeutic adjustments.
The observed dose-dependent plasma concentration profile provided mechanistic insights into the clinical efficacy-safety tradeoffs identified in this study. Although the 15/20 mg group had significantly higher median steady-state trough concentrations than the 5 mg group, no reduction in composite outcomes was observed with escalating doses. Previous recommendations for laboratory measurement of NOACs mentioned that the expected trough concentration of rivaroxaban for stroke prevention in nonvalvular AF was 12–137 ng/mL.24 Despite ultra-low dose rivaroxaban administration in elderly patients, the plasma concentration range in this study remained within the therapeutic threshold required for thrombosis inhibition. Conversely, the dose-linear escalation in plasma concentrations amplified bleeding susceptibility. The broad interquartile range and extended upper distribution tail in 15/20 mg group likely reflected interindividual variability in drug metabolism or reduced clearance due to age-related renal/hepatic impairment. Such pharmacokinetic heterogeneity was associated with a significantly increased risk of major bleeding. Moreover, patients experiencing major bleeding (red solid dots) consistently exhibited elevated trough concentrations, whereas composite outcomes showed a wider distribution of trough concentrations (black solid dots) spanning lower to higher ranges. This observation suggested that composite outcomes were not solely driven by anticoagulant intensity in elderly patients. The concentration-dependent bleeding risk and dispersed composite outcomes patterns highlighted the complexity of anticoagulant management in elderly AF patients. Ultra-low-dose rivaroxaban, associated with reduced major bleeding and not excessively low trough concentrations, appeared advantageous in this population. Future strategies should prioritize individualized dosing guided by pharmacokinetic data and comprehensive risk assessment.
Although our findings provided real-world evidence, this study was exploratory and hypothesis-generating in nature. Moreover, this study has several limitations. First, its single-center, retrospective design limits generalizability beyond this Chinese cohort, although our tertiary medical center serves a wide regional catchment with diverse socioeconomic backgrounds. Second, rivaroxaban dosing was at physicians’ discretion, so patients perceived to be frail or at high bleeding risk likely received lower doses. Although IPTW and TMLE were used to adjust for known confounders, residual confounding by indication cannot be excluded due to unmeasured factors such as physician judgment and subtle frailty not captured by the FRAIL Scale. Finally, renal function was estimated using the Cockcroft-Gault formula, which may overestimate CrCl in very elderly, low-BMI patients with reduced muscle mass and low serum creatinine. Future studies should consider more accurate methods, such as cystatin C or eGFR equations like CKD-EPI, to better assess renal function in this population.
Conclusion
Our findings demonstrated that ultra-low-dose rivaroxaban (5 mg daily) achieved no significant increase in composite efficacy outcomes to standard/low-dose regimens while markedly mitigating major bleeding risks in elderly AF patients. These findings provided real-world evidence that may support the potential role of individualized dosing in frail or high-risk populations. However, ultra-low-dose rivaroxaban was not currently endorsed by major international guidelines, and the retrospective nature of our single-center study may limit the broader applicability of the results. Future prospective, multicenter studies are warranted to further confirm these observations.
Data Sharing Statement
The raw data supporting the conclusion of this article will be available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol received approval from the Institutional Ethics Committees of Nanjing Drum Tower Hospital (Approval Number: 2022-097-01). The requirement for patient consent was waived due to the retrospective design. Patient information was de-identified to ensure confidentiality, and the study adhered to the Declaration of Helsinki.
Acknowledgments
The authors sincerely thank all patients and their families for their invaluable contributions to this study. We also extend our gratitude to the physicians and nursing staff at Nanjing Drum Tower Hospital for their dedicated collaboration throughout the research process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Clinical Trials from the Affiliated Drum Tower Hospital, Medical School of Nanjing University (2022-LCYJ-PY-32, 2021-LCYJ-PY-19).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Paludan-Müller C, Vad OB, Stampe NK, et al. Atrial fibrillation: age at diagnosis, incident cardiovascular events, and mortality. Eur Heart J. 2024;45(24):2119–2129. doi:10.1093/eurheartj/ehae216
2. Ding JC, Sun Y, Zhang K, et al. Effects of anticoagulant therapy and frailty in the elderly patients with atrial fibrillation. Clin Interv Aging. 2024;19:247–254. doi:10.2147/CIA.S453527
3. Stuby J, Haschke M, Tritschler T, Aujesky D. Oral anticoagulant therapy in older adults. Thromb Res. 2024;238:1–10. doi:10.1016/j.thromres.2024.04.009
4. Steffel J, Collins R, Antz M, et al. 2021 European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Europace. 2021;23(10):1612–1676. doi:10.1093/europace/euab065
5. Tzeis S, Gerstenfeld EP, Kalman J, et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. J Interv Card Electrophysiol. 2024;67(5):921–1072. doi:10.1007/s10840-024-01771-5
6. Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45(36):3314–3414. doi:10.1093/eurheartj/ehae176
7. Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2024;149(1):e1–e156. doi:10.1161/CIR.0000000000001193
8. Bawa D, Darden D, Ahmed A, et al. Lower-adherence direct oral anticoagulant use is associated with increased risk of thromboembolic events than warfarin. J Interv Card Electrophysiol. 2024;67(4):709–718. doi:10.1007/s10840-023-01585-x
9. Lin KJ, Singer DE, Ko D, et al. Frailty, home time, and health care costs in older adults with atrial fibrillation receiving oral anticoagulants. JAMA Network Open. 2023;6(11):e2342264. doi:10.1001/jamanetworkopen.2023.42264
10. Hori M, Matsumoto M, Tanahashi N, et al. Rivaroxaban vs. warfarin in Japanese patients with atrial fibrillation-the J-ROCKET AF study-. Circ J. 2012;76(9):2104–2111. doi:10.1253/circj.cj-12-0454
11. Liu XQ, Li ZR, Wang CY, et al. Is a lower dose of rivaroxaban required for Asians? A systematic review of a population pharmacokinetics and pharmacodynamics analysis of rivaroxaban. Pharmaceutics. 2023;15(2):588. doi:10.3390/pharmaceutics15020588
12. Zhang D, Chen WQ, Qin W, et al. Population pharmacokinetics and hemorrhagic risk analysis of rivaroxaban in elderly Chinese patients with nonvalvular atrial fibrillation. J Clin Pharmacol. 2023;63(1):66–76. doi:10.1002/jcph.2145
13. Ng YX, Cheng LJ, Quek YY, et al. The measurement properties and feasibility of FRAIL scale in older adults: a systematic review and meta-analysis. Ageing Res Rev. 2024;95:102243. doi:10.1016/j.arr.2024.102243
14. Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med. 2017;377(14):1319–1330. doi:10.1056/NEJMoa1709118
15. Chan YH, Kuo CT, Yeh YH, et al. Thromboembolic, bleeding, and mortality risks of rivaroxaban and dabigatran in Asians with nonvalvular atrial fibrillation. J Am Coll Cardiol. 2016;68(13):1389–1401. doi:10.1016/j.jacc.2016.06.062
16. Lin YC, Chien SC, Hsieh YC, et al. Effectiveness and safety of standard- and low-dose rivaroxaban in Asians with atrial fibrillation. J Am Coll Cardiol. 2018;72(5):477–485. doi:10.1016/j.jacc.2018.04.084
17. Hori M, Matsumoto M, Tanahashi N, et al. Rivaroxaban vs. warfarin in Japanese patients with non-valvular atrial fibrillation in relation to age. Circ J. 2014;78(6):1349–1356. doi:10.1253/circj.cj-13-1324
18. Hayes KN, Zhang T, Kim DH, et al. Benefits and harms of standard versus reduced-dose direct oral anticoagulant therapy for older adults with multiple morbidities and atrial fibrillation. J Am Heart Assoc. 2023;12(21):e029865. doi:10.1161/JAHA.122.029865
19. Chan YH, Chao TF, Chen SW, et al. Clinical outcomes in elderly atrial fibrillation patients at increased bleeding risk treated with very low dose vs. regular-dose non-vitamin K antagonist oral anticoagulants: a nationwide cohort study. Eur Heart J Cardiovasc Pharmacother. 2023;9(8):681–691. doi:10.1093/ehjcvp/pvad058
20. Mongkhon P, Singkham N, Ponok K, et al. Comparative effectiveness and safety of off-label underdosed direct oral anticoagulants in Asian patients with atrial fibrillation: a systematic review and meta-analysis. Drug Saf. 2025;48(1):25–42. doi:10.1007/s40264-024-01476-8
21. Okumura K, Akao M, Yoshida T, et al. Low-dose edoxaban in very elderly patients with atrial fibrillation. N Engl J Med. 2020;383(18):1735–1745. doi:10.1056/NEJMoa2012883
22. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883–891. doi:10.1056/NEJMoa1009638
23. Andersson C, Johnson AD, Benjamin EJ, Levy D, Vasan RS. 70-year legacy of the Framingham heart study. Nat Rev Cardiol. 2019;16(11):687–698. doi:10.1038/s41569-019-0202-5
24. Gosselin RC, Adcock DM, Bates SM, et al. International Council for Standardization in Haematology (ICSH) recommendations for laboratory measurement of direct oral anticoagulants. Thromb Haemost. 2018;118(3):437–450. doi:10.1055/s-0038-1627480
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Safety and Efficacy of Cryoballoon Pulmonary Vein Isolation and Left Atrial Appendage Closure Combined Procedure and Half-Dose Rivaroxaban After Operation in Elderly Patients with Atrial Fibrillation
Zhang X, Xing Z, Fang C, Yang M, Luo J, Ning Z
Journal of Multidisciplinary Healthcare 2023, 16:2603-2611
Published Date: 5 September 2023