Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Real-World Assessment of Transcranial Direct Current Stimulation (tDCS) Combined with Sertraline in the Treatment of Depression in Vietnam
Authors Do TX, Bui HQ, Dinh HV, Nguyen LV, Pham TT, Nguyen DT, Nguyen DT, Huynh LN, Pham TQ ![]() , Pham TN, Tran TN, Nguyen XT
, Pham TN, Tran TN, Nguyen XT ![]()
Received 8 October 2025
Accepted for publication 2 February 2026
Published 12 February 2026 Volume 2026:22 567022
DOI https://doi.org/10.2147/NDT.S567022
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Tinh Xuan Do,1 Huy Quang Bui,1 Hung Viet Dinh,1 Linh Van Nguyen,1 Thu Thi Pham,1 Dao Trong Nguyen,1 Dinh Tat Nguyen,1 Lang Ngoc Huynh,1 Toan Quoc Pham,2 Thao Ngoc Pham,3 Tuan Ngoc Tran,4 Xuan Thanh Nguyen5
1Department of Psychiatry, 103 Military Hospital, Vietnam Military Medical University, Hanoi, Vietnam; 2Department of Nepherology and Dialysis, 103 Military Hospital, Vietnam Military Medical University, Hanoi, Vietnam; 3Department of Functional Diagnosis, 103 Military Hospital, Vietnam Military Medical University, Hanoi, Vietnam; 4Department of Community Health, Vietnam Military Medical University, Hanoi, Vietnam; 5Senior Officer Department, 103 Military Hospital, Vietnam Military Medical University, Hanoi, Vietnam
Correspondence: Xuan Thanh Nguyen, Senior Officer Department, 103 Military Hospital, Vietnam Military Medical University, Hanoi, Vietnam, Email [email protected]
Background: Major depressive disorder (MDD) is a leading cause of disability worldwide. While selective serotonin reuptake inhibitors (SSRIs) such as Sertraline are widely used, a substantial proportion of patients achieve only partial remission. Transcranial direct current stimulation (tDCS), a non - invasive neuromodulation technique, has been approved and implemented as a clinical procedure in Vietnam. This study aimed to assess the real - world effectiveness of combining tDCS with Sertraline in patients with MDD.
Methods: This open-label, randomized real-world study was conducted at 103 Military Hospital. A total of 140 inpatients with MDD were allocated to receive either Sertraline alone (n = 70) or Sertraline plus tDCS (n = 70) as part of routine care. Depression severity was evaluated using the Beck Depression Inventory (BDI) and Hamilton Depression Rating Scale (HAMD), and serum serotonin levels were measured at baseline and after a three - week treatment period. Statistical analyses included repeated - measures ANOVA and ordinal logistic regression.
Results: Both groups demonstrated significant reductions in BDI and HAMD scores over time (p < 0.001). However, the Sertraline + tDCS group exhibited a significantly greater increase in serum serotonin (+ 30.3 vs + 20.0 ng/mL, p < 0.0001) and greater symptom improvement. Logistic regression indicated a higher likelihood of clinical response in the tDCS group (BDI: OR ≈ 4.3, p = 0.032; HAMD: OR ≈ 6.5, p = 0.018).
Conclusion: In a real - world clinical setting in Vietnam, adjunctive tDCS combined with Sertraline was associated with enhanced biological and clinical outcomes in MDD patients. These findings provide supportive evidence for the integration of tDCS into standard psychiatric care, although further controlled studies are warranted.
Keywords: depression, sertraline, transcranial direct current stimulation, tDCS, serotonin, adjunctive therapy, real-world study
Introduction
Major depressive disorder (MDD) is a common psychiatric condition affecting more than 300 million individuals globally, posing a substantial socioeconomic and public health burden. Alarmingly, depression ranks as the third leading cause of suicide-related mortality among individuals aged 15–29 years.1 In Vietnam, the prevalence of depression has been increasing-particularly in the aftermath of the COVID-19 pandemic—with long-term consequences for both individuals and society.2
Current standard treatment primarily relies on pharmacological intervention. Among available antidepressants, Sertraline-a selective serotonin reuptake inhibitor (SSRI)-is widely prescribed due to its established efficacy and favorable safety profile.3 Nonetheless, approximately 30–40% of patients fail to achieve full remission with monotherapy, and many experience adverse effects or relapse after initial clinical improvement.4 These limitations underscore the need for effective, safe, and practical adjunctive treatment strategies in clinical settings.
In recent years, non-invasive brain stimulation (NIBS) techniques-particularly transcranial direct current stimulation (tDCS)-have gained growing attention as promising adjunctive modalities for depression. tDCS applies a low-intensity electrical current (1–2 mA) through scalp electrodes, aiming to modulate cortical excitability, enhance neuroplasticity, and improve the function of neural circuits involved in emotion regulation.5 Emerging evidence from international studies has demonstrated that tDCS can significantly alleviate depressive symptoms, particularly when used in conjunction with antidepressant medications.6,7
In Vietnam, tDCS has been officially approved by the Ministry of Health as a clinical neuromodulation procedure and is currently implemented in several psychiatric hospitals. However, domestic clinical data remain scarce, with limited real-world evaluations of its effectiveness.
Therefore, this study aims to assess the clinical and biological efficacy of combining tDCS with Sertraline in patients with depression, using validated depression rating scales (Beck Depression Inventory - BDI, Hamilton Depression Rating Scale - HAMD) and a biological marker (serum serotonin levels). The findings are expected to contribute meaningful evidence for the broader clinical adoption of tDCS in Vietnam’s mental health services.
Materials And Methods
Participants
This randomized, open-label controlled trial enrolled 140 inpatients diagnosed with Major Depressive Disorder (MDD) according to the DSM-5 (2013) criteria.8 All participants were admitted for inpatient treatment at the Department of Psychiatry, 103 Military Hospital, Hanoi, Vietnam, between May 2022 and March 2023.
Sample size was calculated using the single-proportion formula, assuming a 95% confidence level (Z = 1.96), expected proportion p=0.5, and margin of error d=0.12, yielding a minimum of 69 participants. We selected 70 patients per group to ensure sufficient power, accounting for potential dropout, although no participants withdrew.
Study Design
Participants were randomly assigned (1:1 allocation) using simple randomization without stratification into two groups:
- Control group (n = 70): Received Sertraline monotherapy.
- Intervention group (n = 70): Received Sertraline plus transcranial direct current stimulation (tDCS).
Randomization was conducted by an independent clinician not involved in assessments. Outcome raters were not blinded, due to the nature of the intervention, constituting a limitation of the study design.
Inclusion Criteria
Patients were eligible if they met the following: Age 18–65 years; DSM-5 diagnosis of moderate to severe MDD; Baseline BDI ≥ 20 and HAMD-17 ≥ 19; No acute physical illness; stable medical condition; Provided written informed consent after receiving full explanation of the study procedures.
Exclusion Criteria
Diagnosis of other major psychiatric disorders (eg, schizophrenia, bipolar disorder); Neurological comorbidities (eg, epilepsy, brain injury); Intellectual disability or developmental delay; Substance abuse or dependence; Pregnancy or lactation; Concurrent use of non-study antidepressants or psychotropic agents; Severe medical conditions (eg, cardiovascular, hepatic, renal failure).
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of 103 Military Hospital (approval No. 42/CNchT-HĐĐĐ).The tDCS procedure utilized in this research has been approved by the Ministry of Health of Vietnam and officially implemented at 103 Military Hospital in accordance with Decision No. 3679/QĐ-BVQY103 (dated 20 October 2023).
Intervention
Both groups were administered Sertraline, starting at 50 mg/day, titrated up to 100 mg/day based on clinical response. For the tDCS group, stimulation was applied using a DC-STIMulator Plus (NeuroConn, Germany). Protocol: Electrodes: 25 cm2 rubber electrodes soaked in 0.9% saline; Placement: Anode at F3 (left DLPFC), cathode between P3–T3 (left parietotemporal region), based on 10–20 EEG system; Current: 2 mA for 20 minutes; Schedule: 5 sessions/week for 2 weeks (total 10 sessions); Ramp-up/down: 30 seconds at start and end. All sessions were supervised, and any side effects were documented. The stimulation protocol was adapted from previous clinical studies.9
Outcome Measures
Clinical: Depression severity was assessed using three standardized scales: (1) Beck Depression Inventory (BDI));10,11 (2) Hamilton Depression Rating Scale (HAMD-17));11 (3) Zung Self-Rating Depression Scale (ZUNG).12 Assessments were conducted at four time points: baseline, after the first, second, and third treatment sessions.
Biological: Serum serotonin levels were measured using an enzyme-linked immunosorbent assay (ELISA) at baseline and after the third treatment session.
Statistical Analysis
All analyses were performed using SPSS 25.0 and Python (statsmodels).
Variables were described as:
- Continuous: mean ± standard deviation (SD).
- Categorical: frequency and percentage.
Statistical methods:
- Baseline comparisons: Independent t-test and Chi-square test.
- Within- and between-group changes: Repeated-measures ANOVA.
- Response rate (≥50% reduction): Binary logistic regression.
- Improvement categories (<25%, 25–50%, 50–75%, >75%): Ordinal logistic regression.
- Serotonin changes: Independent t-test.
Results were reported as Odds Ratios (OR) with 95% Confidence Intervals (CI). Statistical significance was defined as p < 0.05 (two-tailed).
Results
Baseline Characteristics
A total of 140 patients diagnosed with major depressive disorder (MDD) were enrolled and randomly assigned to two equal groups: the Sertraline-only group (n = 70) and the Sertraline plus tDCS group (n = 70). No statistically significant differences were observed between the groups in terms of demographic, clinical, or biological baseline variables, including age, sex, Beck Depression Inventory (BDI) score, Hamilton Depression Rating Scale (HAMD) score, or serum serotonin levels (p > 0.05). These results suggest that the two groups were comparable at baseline, thereby supporting the validity of subsequent comparisons (Table 1).
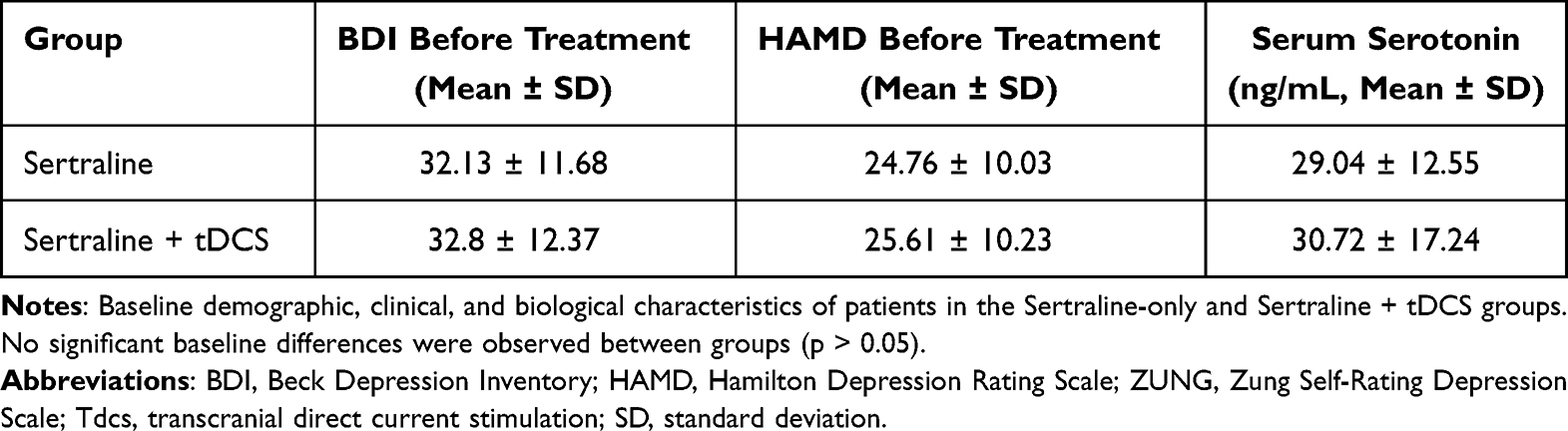 |
Table 1 Baseline Clinical and Biological Characteristics of Study Groups |
Clinical Outcomes and Serum Serotonin Changes
After three assessment time points, both groups exhibited significant reductions in BDI and HAMD scores (p < 0.001). The Sertraline + tDCS group showed a more rapid and pronounced decline, particularly evident after the second time point. Repeated-measures ANOVA revealed a significant main effect of time (p < 0.001) and a significant group × time interaction (p < 0.05), suggesting a potential additive effect of tDCS when combined with Sertraline.
As shown in Figure 1, the reduction in mean BDI and HAMD scores was steeper in the combined group, indicating a faster clinical response to treatment. Further details are provided in Supplementary Figure 1.
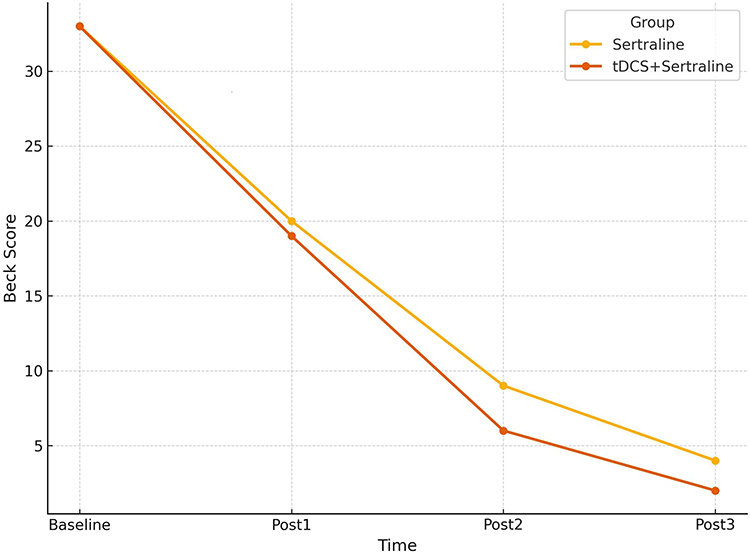 |
Figure 1 Mean Beck Depression Inventory (BDI) scores across treatment sessions. The line plot illustrates a progressive decline in BDI scores across the three assessment points. The Sertraline + tDCS group demonstrated a faster and more sustained reduction in depressive symptoms compared with the Sertraline-only group. Abbreviations: BDI, Beck Depression Inventory; tDCS, transcranial direct current stimulation. |
Biologically, serum serotonin levels increased significantly in both groups (p < 0.001). However, the mean increase was notably greater in the Sertraline + tDCS group (+30.3 ± 16.5 ng/mL) compared with the Sertraline-only group (+20.0 ± 13.5 ng/mL; p < 0.001), as illustrated in Figure 2 and detailed in Table 2. While this difference may reflect enhanced serotonergic modulation, interpretation should remain cautious due to the use of peripheral rather than central measures.
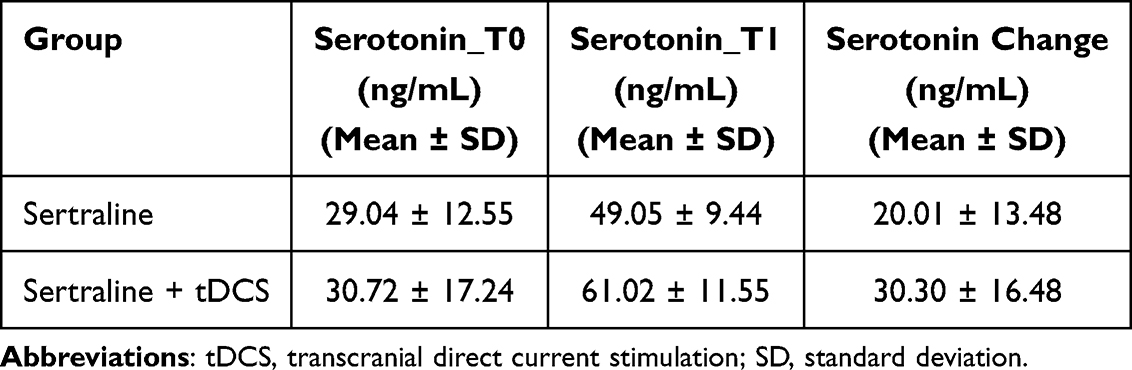 |
Table 2 Changes in Serum Serotonin Levels Before and After Treatment |
 |
Figure 2 Mean Hamilton Depression Rating Scale (HAMD) scores across treatment sessions. The graph demonstrates consistent symptom improvement in both groups, with a more marked and sustained reduction in the Sertraline + tDCS group. These findings correspond with the significant group × time interaction effects observed in the analysis. Abbreviations: HAMD, Hamilton Depression Rating Scale; tDCS, transcranial direct current stimulation. |
These findings were further supported by logistic regression analysis, which indicated an increased likelihood of clinical response in the combined group (see Tables 3 and 4).
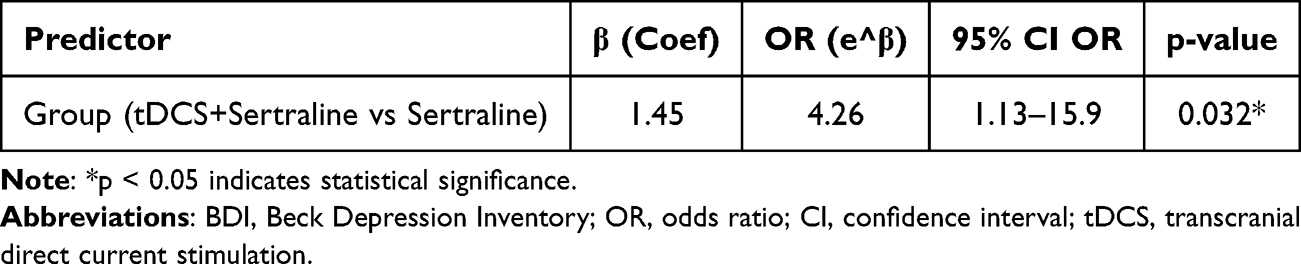 |
Table 3 Clinical Improvement in Beck Depression Inventory (BDI) Scores Between Groups |
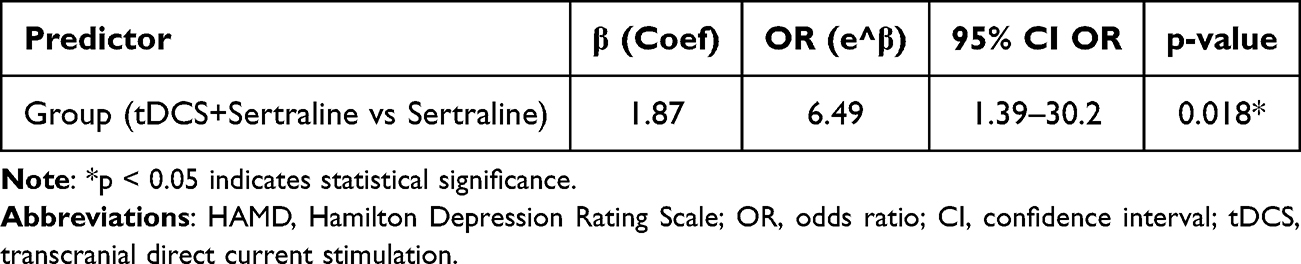 |
Table 4 Clinical Improvement in Hamilton Depression Rating Scale (HAMD) Scores Between Groups |
Treatment Efficacy Based on BDI and HAMD Scales
To further assess treatment outcomes, ordinal logistic regression models were applied to evaluate the likelihood of clinical improvement. The results indicated that patients in the Sertraline + tDCS group were significantly more likely to achieve higher levels of improvement compared to those receiving Sertraline alone (Tables 3 and 4): BDI: OR = 4.26 (β = 1.45; 95% CI: 1.13–15.9; p = 0.032); HAMD: OR = 6.49 (β = 1.87; 95% CI: 1.39–30.2; p = 0.018). No significant associations were found between clinical response and baseline age or sex (p > 0.05). Additional details are provided in Supplementary Figure 2. These results suggest that tDCS may serve as an independent predictor of enhanced clinical response when used adjunctively with pharmacotherapy.
Serum Serotonin Level Dynamics
Following treatment, serum serotonin concentrations increased significantly in both groups (p < 0.001). However, the increase was more pronounced in the combined treatment group (+30.3 ± 16.5 ng/mL vs +20.0 ± 13.5 ng/mL; p < 0.001). Figure 2 illustrates this divergence. Further exploratory analysis of the relationship between serotonin change and symptom improvement is presented in Supplementary Figure 3.
Although not statistically significant, this trend may point toward a potential interaction between neuromodulation and serotonergic pathways, meriting further exploration in future studies.
Discussion
Clinical Efficacy of Sertraline Combined with tDCS
Our findings demonstrated that both treatment regimens significantly improved depressive symptoms, as reflected by substantial reductions in Beck (BDI) and Hamilton (HAMD) scores after three assessment time points. However, the Sertraline + tDCS group exhibited a faster and deeper decline in scores, particularly from the second treatment phase onward. Repeated-measures ANOVA confirmed a significant group-by-time interaction (p < 0.05), suggesting a potential adjunctive benefit of tDCS when combined with antidepressant therapy.
These results are consistent with previous international studies. Wang et al (2021),13 reported in a meta-analysis that tDCS combined with Sertraline achieved greater clinical improvement than monotherapy. Similarly, Tao et al (2024),14 confirmed the efficacy of tDCS as an adjunct in major depression, though the magnitude of effect depended on the type of antidepressant used. Hausman et al (2024),15 found that tDCS significantly reduced depressive and anxiety symptoms in older adults. In addition, Ren et al (2025),16 demonstrated that tDCS improved both depressive and comorbid psychiatric symptoms compared with pharmacotherapy alone.
In our study, ordinal logistic regression revealed that patients receiving tDCS had markedly higher odds of achieving greater clinical improvement (OR ≈ 4.26 for BDI; OR ≈ 6.49 for HAMD). These statistical findings support the possibility of an augmentative effect of tDCS, although interpretation should remain cautious due to the open-label nature of the study. Supplementary Figures 1 and 2 illustrate this trend, showing a higher proportion of responders achieving >50% and >75% improvement in the combined group.
Taken together, these findings suggest that tDCS may serve as a clinically useful adjunct to Sertraline in real-world settings. However, its safety and feasibility were not systematically assessed in this study, and such claims should be explored further in future trials.
Biological Effects and the Role of Serotonin
A noteworthy finding of this study was the significant post-treatment increase in serum serotonin levels in both groups, with a greater rise in the Sertraline + tDCS group (+30.3 vs +20.0 ng/mL; p < 0.001). This may indicate that tDCS could influence serotonergic activity, potentially augmenting the pharmacological effects of Sertraline, a selective serotonin reuptake inhibitor (SSRI).
However, the causal role of serotonin in depression remains debated. Recent large-scale reviews have questioned the classical “serotonin deficiency” hypothesis, suggesting that changes in serotonergic signaling may reflect adaptive or downstream processes rather than a primary etiological mechanism of depression.17,18 Therefore, the observed increase in peripheral serotonin in our study should be interpreted with caution, as it may not directly represent central serotonergic neurotransmission. Other mechanisms—such as enhanced neuroplasticity, modulation of neuroinflammatory pathways, and neurotrophic signaling via BDNF—may also contribute to the antidepressant effects observed with tDCS.
Previous neurobiological studies have demonstrated that stimulation of the left dorsolateral prefrontal cortex (DLPFC) can modulate subcortical circuits such as the raphe nuclei and basal ganglia, reduce neuroinflammatory activity, and suppress pro-inflammatory cytokine release,19 potentially enhancing serotonin synthesis and release, which are crucial for antidepressant response.20
As noted by Qi et al (2023),21 tDCS alters neuronal membrane potentials and promotes neuroplasticity and neurotransmitter release. The observed elevation in peripheral serotonin may reflect a synergistic interaction between tDCS-related cortical modulation and Sertraline’s serotonergic mechanism, contributing to improved depressive symptoms.
Nevertheless, the correlation between serotonin change and clinical improvement was weak (r ≈ 0.21, p > 0.05), suggesting that other biological mechanisms—such as neuroinflammation, neurotrophic signaling (eg, BDNF), or additional peripheral markers—may also play important roles and deserve further investigation.22
Clinical Implications and Study Limitations
Although the mean reductions in BDI and HAMD scores were not dramatically different between groups, the regression models and higher response rates in the tDCS group indicate a potentially meaningful adjunctive benefit. In clinical practice, achieving symptom relief even one to two weeks earlier may help reduce hospitalization duration, improve medication adherence, and lower risk of relapse or suicide, particularly among patients with moderate to severe depression.23
Compared with other neuromodulation techniques such as electroconvulsive therapy (ECT) and repetitive transcranial magnetic stimulation (rTMS), tDCS offers several advantages: it is nonconvulsive, anesthesia-free, low-cost, and relatively easy to implement in general hospital or community psychiatric settings.24 These features may make tDCS a viable option in resource-limited contexts such as Vietnam, where access to more advanced neurostimulation methods remains limited.
Nevertheless, this study has several limitations. First, the short follow-up period (3 weeks) precluded assessment of long-term outcomes and relapse risk. Second, the open-label design may have introduced subjective bias, although independent clinician ratings were used to reduce this risk. Third, the absence of a sham control group limits the ability to fully separate specific treatment effects from placebo or expectancy bias. Fourth, while the sample size (n=140) was relatively large for a single-center real-world study, it was not sufficient for detailed subgroup analyses. Finally, plasma serotonin levels represent peripheral—not central—neurotransmission, and their interpretation should therefore remain tentative in relation to central neurobiological mechanisms.
The large within-group improvements and high odds ratios observed in this study should be interpreted with caution, as non-specific therapeutic and expectancy effects cannot be fully excluded in an open-label setting. Although independent raters were used, the lack of blinding may have contributed to overestimation of perceived treatment gains.
Overall, while the present findings suggest that tDCS may enhance the clinical response to Sertraline, the limited sample size and open-label design restrict the generalizability of these results. Future sham-controlled and adequately powered studies with longer follow-up periods and sensitivity analyses are warranted to confirm the robustness and reproducibility of these findings.
Future Directions
Future studies should include larger sample sizes and longer follow-up periods to strengthen statistical power and evaluate long-term outcomes. Incorporating a sham tDCS control group would help control for placebo effects and strengthen internal validity.In addition, future research should integrate biological markers such as BDNF, CRP, and neuroimaging techniques (fMRI, PET) to elucidate the underlying mechanisms of tDCS.Further exploration of personalized treatment models is warranted to identify patient subgroups that respond best to tDCS, and to integrate this technique into psychiatric rehabilitation and community-based interventions.
Conclusion
This study provides preliminary evidence that combining tDCS with Sertraline may accelerate and enhance the improvement of depressive symptoms compared with Sertraline alone, and is associated with a greater increase in serum serotonin levels. Ordinal logistic regression analyses indicated a potential clinical relevance of these effects (OR Beck = 4.26; OR Hamilton = 6.49). However, given the open-label design, short follow-up period, and single-center setting, these results should be interpreted with caution. Overall, the findings contribute to the growing body of preliminary data supporting the possible adjunctive role of tDCS in depression treatment, while further large-scale, sham-controlled studies are warranted to confirm its efficacy, safety, and feasibility.
Abbreviations
ANOVA, Analysis of Variance; BDI, Beck Depression Inventory; BDNF, Brain-Derived Neurotrophic Factor; CI, Confidence Interval; COVID-19, Coronavirus Disease 2019; DLPFC, Dorsolateral Prefrontal Cortex; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; ECT, Electroconvulsive Therapy; EEG, Electroencephalogram; ELISA, Enzyme-Linked Immunosorbent Assay; Fmri, Functional Magnetic Resonance Imaging; HAMD, Hamilton Depression Rating Scale; MDD, Major depressive disorder; NIBS, Non-Invasive Brain Stimulation; OR, Odds Ratio; PET, Positron Emission Tomography; rTMS, Repetitive Transcranial Magnetic Stimulation; SD, Standard Deviation; SSRI, Selective Serotonin Reuptake Inhibitor; tDCS, Transcranial Direct Current Stimulation; ZUNG, Zung Self-Rating Depression Scale.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. Due to privacy and ethical restrictions, individual participant data are not publicly shared.
Ethics Approval and Consent to Participate
This study was conducted as an open-label observational study evaluating the clinical application of transcranial direct current stimulation (tDCS) combined with Sertraline in patients with depression.
The tDCS procedure utilized in this research has been approved by the Ministry of Health of Vietnam and officially implemented at 103 Military Hospital in accordance with Decision No. 3679/QĐ-BVQY103 (dated 20/10/2023) on the promulgation of technical procedures.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of 103 Military Hospital (approval No. 42/CNchT-HĐĐĐ).
Written informed consent was obtained from all participants and their legal guardians prior to participation.
Acknowledgments
The authors gratefully acknowledge all patients and their families who participated in this study, as well as the medical and nursing staff at the Department of Psychiatry, 103 Military Hospital, Vietnam Military Medical University, for their assistance in patient care and data collection.
Author Contributions
Tinh Xuan Do is the first author. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no external funding or financial support.
Disclosure
The authors declare no conflicts of interest related to the content of this work.
References
1. Global Burden of Disease (GBD) [online database]. Seattle (WA): Institute for Health Metrics and Evaluation; 2024. Available from: https://vizhub.healthdata.org/gbd-results/.
2. Tran QD, TQC V, Phan NQ. Depression prevalence in Vietnam during the COVID-19 pandemic: a systematic review and meta-analysis. Ethics Med Public Health. 2022;23:100806. doi:10.1016/j.jemep.2022.100806
3. Chu A, Wadhwa R. Selective serotonin reuptake inhibitors. [Updated 2023 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554406/.
4. Stern S, Linker S, Vadodaria KC, Marchetto MC, Gage FH. Prediction of response to drug therapy in psychiatric disorders. Open Biol. 2018;8(5):180031. doi:10.1098/rsob.180031
5. Rozisky JR, Antunes LC, Brietzke A, Sousa AC, Caumo W. Transcranial direct current stimulation and neuroplasticity. ResearchGate. 2016.
6. Lõokene M, Markov N, Nikander M, Neuvonen T, Dilkov D. Reduction of symptoms in patients with major depressive disorder after transcranial direct current stimulation treatment: a real-world study. J Affect Disord Rep. 2022;8:100347. doi:10.1016/j.jadr.2022.100347
7. Zheng EZ, Wong NML, Yang ASY, Lee TMC. Evaluating the effects of tDCS on depressive and anxiety symptoms from a transdiagnostic perspective: a systematic review and meta-analysis of randomized controlled trials. Transl Psychiatry. 2024;14(1):295. doi:10.1038/s41398-024-03003-w
8. First MB, Gaebel W, Maj M, et al. An organization- and category-level comparison of diagnostic requirements for mental disorders in ICD-11 and DSM-5. World Psychiatry. 2021;20(1):34–10. doi:10.1002/wps.20825
9. Sreeraj VS, Arumugham SS, Venkatasubramanian G. Clinical practice guidelines for the use of transcranial direct current stimulation in psychiatry. Indian J Psychiatry. 2023;65(2):289–296. doi:10.4103/indianjpsychiatry.indianjpsychiatry_496_22
10. Li X, Jin W, Han L, Chen X, Li L. Comparison and application of depression screening tools for adolescents: scale selection and clinical practice. Child Adolesc Psychiatr Ment Health. 2025;19(1):53. doi:10.1186/s13034-025-00908-2
11. Seemüller F, Schennach R, Musil R, et al. A factor analytic comparison of three commonly used depression scales (HAMD, MADRS, BDI) in a large sample of depressed inpatients. BMC Psychiatry. 2023;23(1):548. doi:10.1186/s12888-023-05038-7
12. Romera I, Delgado-Cohen H, Perez T, Caballero L, Gilaberte I. Factor analysis of the Zung self-rating depression scale in a large sample of patients with major depressive disorder in primary care. BMC Psychiatry. 2008;8:4. doi:10.1186/1471-244X-8-4
13. Wang J, Luo H, Schülke R, Geng X, Sahakian BJ, Wang S. Is transcranial direct current stimulation, alone or in combination with antidepressant medications or psychotherapies, effective in treating major depressive disorder? A systematic review and meta-analysis. BMC Med. 2021;19(1):319. doi:10.1186/s12916-021-02181-4
14. Tao Y, Liang Q, Zhang F, Guo S, Fan L, Zhao F. Efficacy of non-invasive brain stimulation combined with antidepressant medications for depression: a systematic review and meta-analysis of randomized controlled trials. Syst Rev. 2024;13(1):92. doi:10.1186/s13643-024-02480-w
15. Hausman HK, Alexander GE, Cohen R, et al. tDCS reduces depression and state anxiety symptoms in older adults: results from the Augmenting Cognitive Training in Older Adults Study (ACT). Brain Stimul. 2024;17(2):283–311. doi:10.1016/j.brs.2024.02.021
16. Ren C, Pagali SR, Wang Z, et al. Transcranial electrical stimulation in treatment of depression: a systematic review and meta-analysis. JAMA Network Open. 2025;8(6):e2516459. doi:10.1001/jamanetworkopen.2025.16459
17. Moncrieff J, Cooper RE, Stockmann T, et al. The serotonin theory of depression: a systematic umbrella review of the evidence. Mol Psychiatry. 2023;28:3243–3256. doi:10.1038/s41380-022-01661-0
18. Jauhar S, Arnone D, Baldwin DS, et al. A leaky umbrella has little value: evidence clearly indicates the serotonin system is implicated in depression. Mol Psychiatry. 2023;28:3149–3152. doi:10.1038/s41380-023-02095-y
19. Guo B, Zhang M, Hao W, et al. Neuroinflammation mechanisms of neuromodulation therapies for anxiety and depression. Transl Psychiatry. 2023;13:5. doi:10.1038/s41398-022-02297-y
20. Pannu A, Goyal RK. Serotonin and depression: scrutiny of new targets for future antidepressant drug development. Curr Drug Targets. 2023;24(10):816–837. doi:10.2174/1389450124666230425233727
21. Qi S, Cao L, Wang Q, Sheng Y, Yu J, Liang Z. The physiological mechanisms of transcranial direct current stimulation to enhance motor performance: a narrative review. Biology. 2024;13(10):790. doi:10.3390/biology13100790
22. Chmiel J, Stępień-Słodkowska M, Ramik-Mażewska I. Efficacy of transcranial direct current stimulation (tDCS) on neuropsychiatric symptoms in substance use disorder (SUD): a review and insights into possible mechanisms of action. J Clin Med. 2025;14(4):1337. doi:10.3390/jcm14041337
23. Kucuker MU, Almorsy AG, Sonmez AI, et al. A systematic review of neuromodulation treatment effects on suicidality. Front Hum Neurosci. 2021;15:660926. doi:10.3389/fnhum.2021.660926
24. Ruffini G, Salvador R, Castaldo F, et al. Multichannel tDCS with advanced targeting for major depressive disorder: a tele-supervised at-home pilot study. Front Psychiatry. 2024;15:1427365. doi:10.3389/fpsyt.2024.1427365
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Minimal Effects of Cariprazine on Prolactin Levels in Bipolar Disorder and Schizophrenia
Culpepper L, Vieta E, Kelly DL, Patel MD, Szatmári B, Hankinson A, Earley WR
Neuropsychiatric Disease and Treatment 2022, 18:995-1011
Published Date: 12 May 2022