Back to Archived Journals » Pathology and Laboratory Medicine International » Volume 14
Rare Case Report on Hydatid Cyst of Breast
Authors Kassahun Tadele A ![]() , Israel Korga T
, Israel Korga T ![]() , Melis Nisiro A
, Melis Nisiro A ![]() , Abebe Ayele S
, Abebe Ayele S
Received 2 August 2022
Accepted for publication 29 November 2022
Published 8 December 2022 Volume 2022:14 Pages 33—36
DOI https://doi.org/10.2147/PLMI.S380081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Paul Zhang
Abraham Kassahun Tadele,1 Tesfalem Israel Korga,2 Abebe Melis Nisiro,1 Selamawit Abebe Ayele1
1Department of Pathology, Hawassa University Comprehensive Specialized Hospital, Hawassa, Sidama, Ethiopia; 2Department of Pathology, Wolaita Sodo University Teaching Hospital, Wolayta, SNNP, Ethiopia
Correspondence: Abraham Kassahun Tadele, Tel +251910194890, Email [email protected]
Abstract: Hydatid cyst of the breast is a very rare disease that predominantly affects endemic regions. Breast hydatid cysts can occur alone or as a component of widespread hydatidosis. Histopathology is the best diagnostic method for hydatid cysts of the breast, but fine needle aspiration cytology can be utilized in preoperative diagnosis. Here we report, a case of a female patient who was diagnosed with Hydatid cyst of the breast Postoperatively in Wolaita Sodo University teaching hospital, southern Ethiopia. Preoperatively the patient was diagnosed with tuberculous mastitis and she took the full course of Anti Tuberculous treatment. After completing the treatment there was no improvement. The cyst was removed surgically and histopathology confirmed the disease to be Hydatid cyst of the breast.
Keywords: hydatid cyst, benign breast lesion
Introduction
Hydatid disease is caused by ingestion of eggs of Echinococcus species and formation of cysts in organs where the parasite larvae are deposited. Dog and fox are the definitive hosts for Echinococcus granulosus and Echinococcus multilocularis respectively. Sheep are the usual intermediate hosts for Echinococcus multilocularis whereas rodents are intermediate hosts for Echinococcus multilocularis. Humans are accidental intermediate hosts, infected by ingestion of food tainted with eggs shed by dogs or foxes.1
Several Echinococcus species can infect humans. The most prevalent type, Echinococcus granulosus, causes cysts most frequently in the liver and lungs. Echinococcus multilocularis, which causes an invasive tumor-like replacement of liver tissue, is far less frequent. Even in endemic places, hydatid cysts of the breast are relatively uncommon; they only make up 0.27% of all occurrences.2
A breast hydatid cyst can resemble a number of benign breast lesions. Physical examination, radiologic examinations, serologic tests, and Fine needle aspiration cytology cannot reliably differentiate Hydatid cyst of the breast from other benign breast lesions. Histopathology is required for definitive diagnosis.3
Ethical Review
After receiving approval from the Hawassa University Institutional Review Board in the form of a letter, the patient provided written informed consent for this case report to be published (IRB).
Case Presentation
Our case was 18 years old female residing in the rural part of Wolaita, southern Ethiopia Region. She presented with a left breast mass of 02 years duration. There was no associated pain, discharge, or bleeding. She had no history of contact with any animal. She was evaluated at surgical outpatient department in Wolaita Sodo University Teaching hospital, southern Ethiopia. During the evaluation, she had 6x5cm mass in the left upper quadrant of the left breast. There was no skin color change, nipple retraction, or palpable ipsilateral axillary lymphadenopathy. No abnormality was detected in the contralateral breast. Breast ultrasound revealed oval cystic mass. Fine needle aspiration cytology was done and the conclusion was granulomatous inflammation of the breast.
On laboratory examination, the Complete blood count and Erythrocyte sedimentation rate were under the normal range.
On abdominal ultrasound, any pathology was not identified. After the above investigation with the impression of granulomatous inflammation secondary to tuberculous mastitis, the patient was put on anti-Tuberculous treatment. After completing the full course of the treatment there was no improvement then the managing team agreed to excise the mass both for diagnostic and treatment reasons.
The patient was taken to the operation room and complete excision of the tumor with clear surgical margins was done. Intraoperative there was an intact cystic mass measuring 6x5x3cm and lytic lesion of the adjacent rib. The sample was sent for histopathologic examination. On Gross Examination there was 6x5x3cm cystic tissue with a gray-white outer surface. On the cut section, there were daughter cysts and grayish material. Under microscopic evaluation, hydatid cyst wall surrounded by granulomatous inflammation along with tubulo-lobular unit of breast was identified (Figure 1). Another medium power microscopic examination revealed germinative and acellular laminated layers of hydatid cyst (Figure 2).
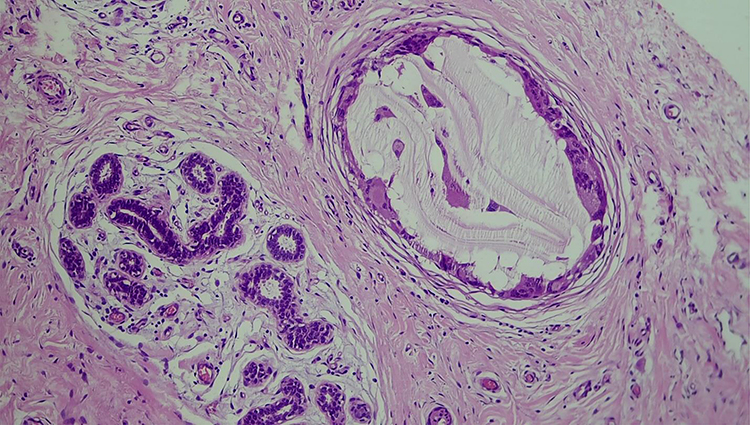 |
Figure 1 Medium power microscopic examination demonstrating hydatid cyst wall surrounded by giant cells and granuloma. Adjacent tubulolobular unit of breast is also evident. |
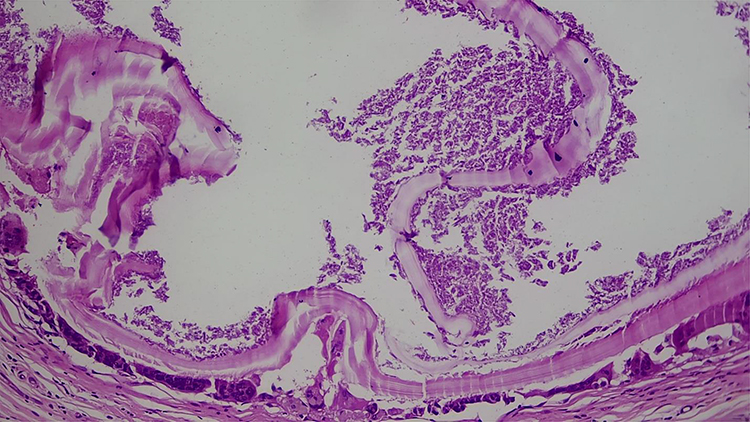 |
Figure 2 Medium power microscopic examination demonstrating germinative layer and acellular laminated layer of hydatid cyst surrounded by Giant cells. |
There was no intraoperative or postoperative complication. The Patient received post-operative Albendazole treatment and recurrence was not observed in the last 06 months after the surgery.
Discussion
Echinococcosis is an infection caused by cestodes of the genus Echinococcus. Carnivores are the definitive hosts, and adult worms are found in their intestines. Echinococcus eggs, which are excreted by definitive hosts, hatch when consumed by suitable intermediate hosts, such as humans. The freed embryos then go to parenteral locations and mature into the metacestode (larval) forms. The transmission of Echinococcus species from intermediate to definitive hosts is the result of predator-prey relationship interaction between hosts. Established risk factors for human infection include intimate contact between humans and dogs, the unrestrained slaughter of cattle, and unhygienic living circumstances.2
The prevalence of the parasite differs from region to region, being higher in sheep-raising, developing, and underdeveloped countries around the Mediterranean Sea, the Middle East, South America, and Asia & East Africa.4
Echinococcus granulosus cysts are typically found in the liver in roughly two-thirds of cases, the lung in 5–15% of cases, and the bones, brain, or other organs in the remaining cases. The larvae dwell inside the capillaries of the various organs and first trigger an inflammatory response made up primarily of mononuclear leukocytes and eosinophils.1
Hydatid disease of the breast is rare and accounts for only 0.27% of all cases. The breast can be a primary site or part of a disseminated hydatidosis. In non-endemic areas, hydatid cyst of the breast is not usually considered in the differential diagnosis of breast lesions.5,6
The patient typically develops a painless breast lump that steadily grows in size without involving any local lymph nodes. Women between the ages of 30 and 50 are typically affected. It may resemble phyllodes tumors, chronic abscesses, fibroadenoma, or even cancer. Therefore, especially in endemic locations, breast hydatid cyst should be included in the differential diagnosis of breast masses.6,7
Mammography and ultrasound may play important role in the preclinical evaluation of hydatid cyst but they are not conclusive. Mammography may reveal a ring-shaped structure inside a circumscribed mass lesion.8 The ultrasound results are variable depending on growth stage, associated complications, and affected organ. “Wheel-spoke” pattern which is characterized by multiple daughter cysts separated by a fluid matrix that contains a mixture of membranes of broken daughter vesicles, scolices, and hydatid sand with mixed echogenicity may be seen in unruptured hydatid cyst of breast. In ruptured hydatid cyst, folded membrane floating at the air-fluid interface may create ‘water lily sign’ on ultrasound.9,10 In our case breast ultrasound was done preoperatively and it revealed a cyst lesion measuring 6x5x3 cm but further features that suggest Hydatid cyst was not reported. For diagnosis and patient follow-up, serological studies with an indirect hemagglutination test may be performed.7
Previously there was controversy regarding the use of Fine needle aspiration cytology (FNAC) in the preoperative diagnosis of Hydatid cyst but recent literature concluded the procedure to be fast, inexpensive, and safe.5,11 In very rare conditions puncturing of the cyst may result in an anaphylactic reaction and spillage of hydatid fluid with secondary cyst development.12 On Fine needle aspiration cytology, laminated membrane with parallel striations, dispersed retractile booklets, granular debris, and multinucleated giant cell is consistent with the diagnosis of a hydatid cyst.11 Preferably Fine needle aspiration cytology should be done under ultrasound guidance.13 We performed Fine needle aspiration cytology in our case and the findings were Granuloma, multinucleated giant cells, and heterogeneous lymphoid cells. Features suggestive of Hydatid cyst were not identified. There was no complication following the procedure. Similar to our case the definitive diagnosis of most of the reported cases were made through histopathologic examination.
A hydatid cyst is treated with total excision without any spillage and its recurrence is very rare. Albendazole treatment has been shown to reduce the incidence of recurrence.14 In our case, after complete excision of the cyst Albendazole was given postoperatively. Recurrence was not detected in the last six months after surgery.
Conclusion
Breast hydatid cysts are extremely uncommon. It is very difficult to distinguish it from other tumoral breast lesions. For patients who live in endemic areas, it should be considered in the differential diagnosis of breast masses. Fine Needle aspiration cytology can be used in preoperative diagnosis of hydatid cyst of the breast. The procedure is proved to be fast, inexpensive, and safe with very minimal complications. Rather than Computed tomography (CT) and mammography, sonography and Magnetic resonance imaging (MRI) plays a significant diagnostic role in preoperative diagnosis. The bulk of the reported instances was discovered after surgery. There have been cases of recurrence following surgical removal, but postoperative Albendazole may lower this rate.
Data Sharing Statement
The data used to support the findings of this study will be available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to acknowledge all the managing teams who participated in the betterment of this client and the accomplishment of this case report.
Author Contributions
All authors contributed significantly to the work that was published, whether it be in the ideation, study design, execution, data collection, analysis, and interpretation, or in each of these areas. They also participated in the writing, editing, and critical review of the article, gave their final approval for the version that would be published, decided on the journal to which the article would be submitted, and agreed to be held accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease.
2. Olano JP, Weller PF, Guerrant RL, Walker DH. Principles of parasitism: host-parasite interactions. Trop Infect Dis. 2006;1:1–12. doi:10.1016/B978-0-443-06668-9.50006-5
3. Koc A, Sarici IS, Vurdem UE, Karabiyik O, Gumus UO. Case report unusual presentation of hydatid cyst in breast with magnetic resonance imaging findings. Case Rep Med. 2017;2017:1–5. doi:10.1155/2017/6237435
4. Bekele A, Bekele A, Shifara A. A rare case of hydatid cyst disease of the breast: a case report and review of literature. Ethiop Med J. 2017;55(Suppl 1):15–31.
5. Alamer A, Aldhilan A, Makanjuola D, Alkushi A. Preoperative diagnosis of hydatid cyst of the breast: a case report. Pan Afr Med J. 2013;14:1–7. doi:10.11604/pamj.2013.14.99.2396
6. Acar T, Gömcel A, Güzel K, Yazgan A, Aydn R. Isolated hydatid cyst of the breast. Scott Med J. 2003;48(2):52–53. doi:10.1177/003693300304800208
7. Das DK, Choudhury U. Hydatid disease; an usual breast lump. J Indian Med Assoc. 2002;100(5):327–328.
8. Cavada A, Ortega E, Cavada A, Garijo F. Cyst of the breast. Am J Roentgenol. 1994;162(4):825–826. doi:10.2214/ajr.162.4.8140999
9. Mirdha BR, Biswas A. Echinococcosis: presenting as palpable lumps of breast. Indian J Chest Dis Allied Sci. 2001;43(4):239–241.
10. Dagli AF, Ozercan MR, Kocakoc E. Hydatid cyst of the breast mimicking inflammatory carcinoma and mastitis. J Ultrasound Med. 2006;25(10):1353–1356. doi:10.7863/jum.2006.25.10.1353
11. Cancelo MJ, Martín M, Mendoza N. Preoperative diagnosis of a breast hydatid cyst using fine-needle aspiration cytology: a case report and review of the literature. J Med Case Rep. 2012;6:2–5. doi:10.1186/1752-1947-6-293
12. Tukel S, Erden I, Eciffci S, Koçak S. Hydatid cyst of the breast: mRIimaging findings. Am J Roentgenol. 1997;168(5):1386–1387. doi:10.2214/ajr.168.5.9129460
13. Report C, Patmano M, Gümüş T. A Rare case; hydatid cyst of the breast. Int J Surg Case Rep. 2019;43:2018–2020. doi:10.4274/tpd.galenos.2018.5874
14. Report BAC. Primary hydatid cyst of the mediastinum. Eur J Cardiothorac Surg. 2007;4(3):159–162.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.