Back to Journals » OncoTargets and Therapy » Volume 15
Rapid and Efficient Response to Gilteritinib and Venetoclax-Based Therapy in Two AML Patients with FLT3-ITD Mutation Unresponsive to Venetoclax Plus Azacitidine
Authors Zhang LS, Wang J, Xu MZ, Wu TM, Huang SM ![]() , Cao HY, Sun AN, Liu SB
, Cao HY, Sun AN, Liu SB ![]() , Xue SL
, Xue SL ![]()
Received 4 November 2021
Accepted for publication 27 January 2022
Published 18 February 2022 Volume 2022:15 Pages 159—164
DOI https://doi.org/10.2147/OTT.S336715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Federico Perche
Lei-Si Zhang,1,2,* Jun Wang,1,2,* Ming-Zhu Xu,1,2,* Tian-Mei Wu,1,2 Si-Man Huang,1,2 Han-Yu Cao,1,2 Ai-Ning Sun,1,2 Song-Bai Liu,3 Sheng-Li Xue1,2
1National Clinical Research Center for Hematologic Diseases, Jiangsu Institute of Hematology, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China; 2Institute of Blood and Marrow Transplantation, Collaborative Innovation Center of Hematology, Soochow University, Suzhou, People’s Republic of China; 3Suzhou Key Laboratory of Medical Biotechnology, Suzhou Vocational Health College, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Song-Bai Liu, Suzhou Key Laboratory of Medical Biotechnology, Suzhou Vocational Health College, No. 28, Kehua Road, Suzhou, 215009, People’s Republic of China, Tel +86-13862145806, Email [email protected] Sheng-Li Xue, National Clinical Research Center for Hematologic Diseases, Jiangsu Institute of Hematology, The First Affiliated Hospital of Soochow University, No. 188, Shizi Street, Suzhou, 215006, People’s Republic of China, Tel +86-512-67781856, Email [email protected]
Abstract: The presence of FLT3-ITD mutation is associated with relapse and poor survival in AML patients. Venetoclax combined with hypomethylating agents (VEN+HMA) was approved for the frontline treatment of elderly or unfit AML patients, which leads to noteworthy impacts on AML management. The combination therapy is associated with encouraging efficacy in FLT3-mutated AML among both newly diagnosed unfit and relapsed/refractory patients. However, we found that two AML patients with FLT3-ITD mutation did not respond to venetoclax plus azacitidine (VEN+AZA). Given that the combined efficacy of venetoclax and the FLT3 inhibitor has been proved in pre-clinical models of FLT3+ AML, it is a scientific rationale to investigate venetoclax combined with the FLT3 inhibitor in AML patients with FLT3-ITD mutation. This is the first report of assessing the safety and response of gilteritinib (the first and only targeted second-generation FLT3 tyrosine kinase inhibitor approved by the US FDA) and venetoclax-based therapy in two AML patients with FLT3-ITD mutation unresponsive to VEN+AZA, which may bring new hope to FLT3 mutated patients who are unresponsive to VEN+HMA.
Keywords: acute myeloid leukaemia, FLT3-ITD, gilteritinib, venetoclax
Introduction
Acute myeloid leukaemia (AML) is a life-threatening disease harbouring variable genetic mutations that can influence therapy outcome and prognosis. The presence of the FLT3-ITD mutation is associated with relapse and poor survival in AML patients. Venetoclax combined with hypomethylating agents (VEN+HMA) has been approved as a frontline treatment for elderly or unfit AML patients, which leads to noteworthy impacts on AML management. Combination therapy is associated with encouraging efficacy in FLT3-mutated AML among both newly diagnosed unfit and relapsed/refractory patients, with CR/CRi rates of 94% and 42%, respectively.1
Herein, we describe two patients with FLT3-ITD AML who were unresponsive to venetoclax plus azacitidine but showed a rapid response with good safety following gilteritinib and venetoclax-based therapy. The patients’ characteristics and treatment details are summarized in Table 1.
 |
Table 1 Patient Characteristics, Treatment Details and Response to Therapy |
Case 1
Patient 1 was a 24-year-old man diagnosed with MDS-EB2 in August 2020, and 15.8% blasts with FLT3-ITD (AR = 0.064) were detected in his bone marrow. After 2 cycles of azacitidine, he was referred for a haploidentical haematopoietic stem cell transplantation (HSCT) from his father in October 2020. Unfortunately, five months later, he was diagnosed with AML progressing from MDS after HSCT, and the bone marrow biopsy revealed 48% blasts with FLT3-ITD (AR = 0.673). Disappointingly, 92.5% blasts with FLT3-ITD (AR = 7.141) were present in his bone marrow after two cycles of venetoclax + azacitidine. When the patient had an FLT3 mutation, a reinduction therapy comprising gilteritinib, venetoclax and azacitidine (Figure 1A) was administered in April 2021. The patient achieved a morphologic leukaemia-free state at the end of the induction therapy (+1 d) with MRD 8.5*10−4 and FLT3-ITD (AR = 0.058). The patient continued gilteritinib and venetoclax combined therapy (Figure 1A) as consolidation treatment on day 21 when the neutrophil count exceeded 0.5×109/L. Afterwards, he achieved CR with FLT3-ITD negative for the first time since consolidation treatment in June 2021. No serious adverse events occurred during the treatment, although haematological toxicity was observed (Figure 1B, Table 1). The patient is in good condition till now, almost eight months after reinduction therapy, and waiting for a second HSCT.
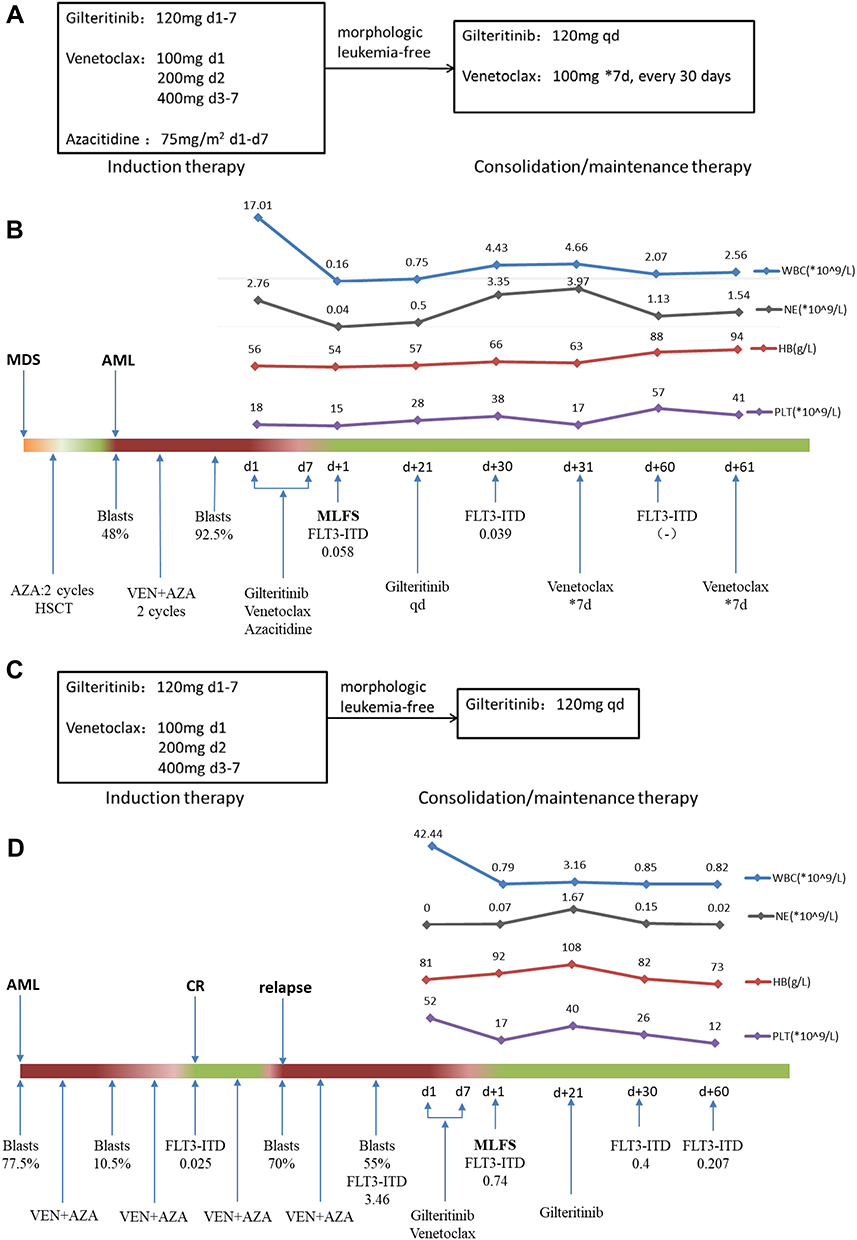 |
Figure 1 (A) Induction therapy and consolidation/maintenance therapy in Patient 1. (B) Treatment process of patient 1. (C) Induction therapy and consolidation/maintenance therapy in Patient 2. (D) Treatment process of Patient 2. *The dose of venetoclax was adjusted because of posaconazole treatment. |
Case 2
Patient 2 was a 77-year-old woman diagnosed with AML in August 2020, with 77.5% myoblasts and FLT3-ITD (AR = 1.75). ASXL1 and CSMD1 and ETV6 mutations were detected in her bone marrow. She achieved morphologic CR with FLT3-ITD (AR = 0.025) after two cycles of venetoclax + azacitidine. Disappointingly, she experienced relapse before the commencement of the fourth cycle. The bone marrow aspirate indicated 70% myoblasts with the FLT3-ITD mutation (AR = 1.49) in March 2021. After the fourth cycle of venetoclax + azacitidine, the patient still did not achieve CR, with 55% blasts with the FLT3-ITD mutation (AR = 3.46). As she had a FLT3 mutation, a reinduction therapy combining gilteritinib and venetoclax (Figure 1C) was administered in April 2021. She achieved a morphologic leukaemia-free state at the end of the induction therapy (+1 d) with MRD 1.1*10−3 and FLT3-ITD (AR = 0.74). Her peripheral blood recovered to normal levels on day 2. Because of financial concerns, she continued with gilteritinib as maintenance therapy (Figure 1C). Following-up at 2 months after gilteritinib alone, she remained morphologic CR. No serious adverse events occurred during the treatment, although haematological toxicity was observed (Figure 1D, Table 1). The latest follow-up is November, 2021, seven months after gilteritinib and venetoclax combined therapy, and gilteritinib was still adopted as maintenance therapy.
Discussion
FLT3-ITD triggers leukaemogenesis alone or in combination with other mutations, suggesting that FLT3-ITD is a candidate therapeutic target for pursuing long-lasting remission.2 The rate of FLT3-ITD mutation in the MDS population is less than 10%, and those with the mutation have a higher AML transformation rate, quicker disease progression, and shorter survival time.3 Patient 1 underwent AML progression with the FLT3-ITD mutation five months after HSCT. As venetoclax + azacitidine is a viable salvage option for relapsed/refractory patients with AML or MDS,4 we chose the combination as reinduction therapy. Patient 2 was an elderly woman with high-risk factors who could not undergo traditional chemotherapy. According to NCCN guidelines, venetoclax-based therapy is a good option for her. However, patient 1 did not respond to the treatment, and the response diminished in Patient 2 during the treatment.
The FLT3-ITD mutation is associated with a relatively lower response rate to venetoclax treatment and might be acquired after venetoclax treatment, indicating that FLT3-mutated clones may lead to resistance to venetoclax-based therapy.5 As venetoclax is a specific Bcl2 inhibitor that has little effect on other antiapoptotic proteins, such as BCL-XL and MCL-1,6 apoptotic evasion during venetoclax treatment occurs via apoptotic proteins modulated by oncogenic signalling. FLT3-ITD regulates multiple survival pathways and is linked to increased BCL-XL and MCL-1 expression, which might promote venetoclax resistance.7 In vivo and in vitro analyses indicated that FLT3 inhibitors could downregulate BCL-XL and MCL-1 expression, priming cells towards BCL-2 dependence for survival.8 Thus, it is a scientific rationale to investigate venetoclax combined with FLT3-ITD inhibition. In vitro analyses indicated that venetoclax and FLT3 inhibitors (midostaurin, gilteritinib and quizartinib) could synergistically induce apoptosis in FLT3-mutated AML cell lines and primary patient samples.8,9 Although the combination induced similar tumour regressions as the FLT3 inhibitor alone in vivo, the combination can truly increase durability and prevent leukaemia re-emergence.5
Gilteritinib is the first and only targeted second-generation FLT3 tyrosine kinase inhibitor that was approved by the US FDA in November 2018 for the treatment of adult patients with relapsed or refractory FLT3-mutated AML. In clinical trials, gilteritinib was well tolerated and prolonged survival by inducing deep molecular responses with FLT3-ITD clearance in FLT3-ITD+ relapsed/refractory AML patients.10,11 Consequently, the 2018 NCCN guidelines recommend gilteritinib as a category 1 treatment option for patients with relapsed/refractory FLT3-mutated AML. It is demonstrated that Gilteritinib could enhance the antileukaemic effects of venetoclax in vitro and in vivo by abolishing the induction of p-ERK by venetoclax and downregulating Mcl-1 protein expression levels.9
It is reported that the median overall survival (mOS) after VEN+HMA failure for elderly AML patients was 2.4 months, and those who received salvage therapy had better survival (mOS: 2.9 months).12 In our reports, after receiving gilteritinib and venetoclax-based re-induction therapy, patient 2, a 77-year-old woman, survived 7 months after VEN+AZA failure; while patient 1, a young patient, was in good conditions for 8 months and is waiting for HSCT. This is the first report assessing the safety and response of gilteritinib and venetoclax-based therapy in AML patients with FLT3-ITD unresponsive to VEN+HMA. The fact that the two patients achieved a rapid response without side effects indicated that gilteritinib and venetoclax-based therapy is a promising salvage therapy for those who are unresponsive to venetoclax plus azacitidine. A phase 1b multicentre study (NCT03625505) evaluated the safety and efficacy of venetoclax in combination with gilteritinib. As is reported in ASH 2021, the combined therapy is well tolerated and achieved high mCRc (74.5%) in patients with R/RFLT3+ AML (patients who failed at least 1 line of prior therapy). Patient 1 achieved CR and was FLT3-ITD-negative after gilteritinib and venetoclax combined consolidation therapy, while Patient 2 achieved sustained morphologic CR with gilteritinib consolidation therapy. We speculate that gilteritinib combined with venetoclax might be better than gilteritinib alone for consolidation/maintenance therapy. The results of a clinical trial (NCT02752035) also indicated that gilteritinib plus azacitidine induces antileukaemic responses in newly diagnosed FLT3-mutated AML patients with no unexpected AEs.13 Our two patients had similar agranulocytosis and neutropenia durations after induction therapy, although azacitidine was only added to the treatment regimen of patient 1. It is thought that azacitidine is appropriate for induction therapy, but more clinical data are needed to assess its toxicity and efficiency. In addition, a Phase I/II Study (NCT05010122) of ASTX727 (oral cedazuridine and decitabine), Venetoclax, and Gilteritinib for the Treatment of Newly Diagnosed, Relapsed or Refractory FLT3-Mutated Acute Myeloid Leukemia or High-Risk Myelodysplastic Syndrome is recruiting, which means the combination of HMA, venetoclax and gilteritinib is widely concerned and investigated. Thus, we propose a protocol (Figure S1) that could be delivered to FLT3-mutated AML patients unresponsive to venetoclax plus azacitidine.
Data Sharing Statement
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University and was conducted in accordance with the Declaration of Helsinki. Both patients provided written informed consent, and they consented to the publication of their clinical details.
Funding
This work was supported by grants from the National Natural Science Foundation of China [Grant No. 81970138], Translational Research Grant of NCRCH [Grant No. 2020ZKMB05], Jiangsu Province “333” project, Social Development Project of the Science and Technology Department of Jiangsu (Grant No. BE2021649), Gusu Key Medical Talent Program [Grant No. GSWS2019007], and China Scholarship Council(No. 202106920030).
Disclosure
Lei-Si Zhang, Jun Wang, and Ming-Zhu Xu are co-first authors for this study. The authors declare that they have no conflicts of interest in this work.
References
1. Aldoss I, Zhang J, Mei M, et al. Venetoclax and hypomethylating agents in FLT3‐mutated acute myeloid leukemia. Am J Hematol. 2020;95(10):1193–1199. doi:10.1002/ajh.25929
2. Smith CC, Wang Q, Chin C, et al. Validation of ITD mutations in FLT3 as a therapeutic target in human acute myeloid leukaemia. Nature. 2012;485(7397):260–263. doi:10.1038/nature11016
3. Xu F, Han R, Zhang J, et al. The role of FLT3-ITD mutation on de Novo MDS in Chinese population. Clin Lymphoma Myeloma Leuk. 2019;19(2):e107–15. doi:10.1016/j.clml.2018.11.006
4. DiNardo CD, Rausch CR, Benton C, et al. Clinical experience with the BCL2-inhibitor venetoclax in combination therapy for relapsed and refractory acute myeloid leukemia and related myeloid malignancies. Am J Hematol. 2018;93(3):401–407. doi:10.1002/ajh.25000
5. Chyla B, Daver N, Doyle K, et al. Genetic biomarkers of sensitivity and resistance to venetoclax monotherapy in patients with relapsed acute myeloid leukemia. Am J Hematol. 2018;93(8):E202–5. doi:10.1002/ajh.25146
6. Ramsey HE, Fischer MA, Lee T, et al. A novel MCL1 inhibitor combined with venetoclax rescues venetoclax-resistant acute myelogenous leukemia. Cancer Discov. 2018;8(12):1566–1581. doi:10.1158/2159-8290.CD-18-0140
7. Bagrintseva K, Geisenhof S, Kern R, et al. FLT3-ITD-TKD dual mutants associated with AML confer resistance to FLT3 PTK inhibitors and cytotoxic agents by overexpression of Bcl-x(L). Blood. 2005;105(9):3679–3685. doi:10.1182/blood-2004-06-2459
8. Singh MR, Zhang Q, DeFilippis RA, et al. Venetoclax combines synergistically with FLT3 inhibition to effectively target leukemic cells in FLT3-ITD+ acute myeloid leukemia models. Haematologica. 2021;106(4):1034–1046. doi:10.3324/haematol.2019.244020
9. Ma J, Zhao S, Qiao X, et al. Inhibition of Bcl-2 synergistically enhances the antileukemic activity of midostaurin and gilteritinib in preclinical models of FLT3-mutated acute myeloid leukemia. Clin Cancer Res. 2019;25(22):6815–6826. doi:10.1158/1078-0432.CCR-19-0832
10. Pulte ED, Norsworthy KJ, Wang Y, et al. FDA approval summary: gilteritinib for relapsed or refractory acute myeloid leukemia with a FLT3 mutation. Clin Cancer Res. 2021;27(13):3515–3521. doi:10.1158/1078-0432.CCR-20-4271
11. Altman JK, Perl AE, Hill JE, Rosales M, Bahceci E, Levis MJ. The impact of FLT3 mutation clearance and treatment response after gilteritinib therapy on overall survival in patients with FLT3 mutation–positive relapsed/refractory acute myeloid leukemia. Cancer Med. 2021;10(3):797–805. doi:10.1002/cam4.3652
12. Maiti A, Rausch CR, Cortes JE, et al. Outcomes of relapsed or refractory acute myeloid leukemia after frontline hypomethylating agent and venetoclax regimens. Haematologica. 2021;106(3):894–898. doi:10.3324/haematol.2020.252569
13. Esteve J, Schots R, Bernal T, et al. Multicenter, open-label, 3-arm study of gilteritinib, gilteritinib plus azacitidine, or azacitidine alone in newly diagnosed FLT3 mutated (FLT3mut+) acute myeloid leukemia (AML) patients ineligible for intensive induction chemotherapy: findings from the safety Cohort. Blood. 2018;132:2736.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.