Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Radiomics and Deep Learning: Bridging Breast Cancer Imaging Phenotypes and Genomic Heterogeneity
Authors Yi G, Deng L ![]() , Su L, Jie H, Huang C
, Su L, Jie H, Huang C ![]() , Wang Y
, Wang Y
Received 17 April 2026
Accepted for publication 23 June 2026
Published 30 June 2026 Volume 2026:18 617698
DOI https://doi.org/10.2147/BCTT.S617698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Guangming Yi1, Lihua Deng 2, Liping Su3, Huan Jie4, Cong Huang5, Yujun Wang6
1Department of Oncology, The Third Hospital of Mianyang (Sichuan Mental Health Center), Mianyang, Sichuan, 621000, People’s Republic of China; 2Department of Radiology, The First People’s Hospital of Neijiang, Neijaing, Sichuan, 641000, People’s Republic of China; 3Department of Radiology, Yongchuan Hospital of Chongqing Medical University, Yongchuan, Chongqing, 402160, People’s Republic of China; 4Department of Oncology, No. 926 Hospital, Joint Logistics Support Force of PLA, Kaiyuan, Yunnan, 661699, People’s Republic of China; 5Department of Radiology, No. 926 Hospital, Joint Logistics Support Force of PLA, Kaiyuan, Yunnan, 661699, People’s Republic of China; 6Department of Radiology, The First Affiliated Hospital of Zhejiang Chinese Medicine University (Zhejiang Provincial Hospital of Chinese Medicine), ZheJiang, Hangzhou, 310006, People’s Republic of China
Correspondence: Yujun Wang, Email [email protected]; Cong Huang, Email [email protected]
Abstract: Breast cancer is a highly heterogeneous malignancy. Radiomics, combined with deep learning techniques, harnesses the power of advanced medical imaging to extract rich quantitative features that noninvasively capture tumor imaging phenotypes. This approach facilitates the integration of macroscopic imaging data with genomic heterogeneity, thereby bridging the gap between tumor radiographic appearance and underlying molecular profiles. This review systematically outlines the radiomics workflow in breast cancer, encompassing image acquisition, tumor segmentation, feature extraction, feature selection, and modeling strategies. Emphasis is placed on the role of deep learning in automating feature extraction and enabling multimodal data fusion to enhance predictive accuracy. By examining current research progress, we elucidate methods to uncover latent information related to gene mutations, immune microenvironment characteristics, and other genomic alterations from imaging data. This synthesis highlights the potential of radiogenomics to provide novel insights and tools for precision medicine, ultimately fostering personalized diagnosis, prognosis, and treatment planning in breast cancer care.
Keywords: radiomics, deep learning, breast cancer, imaging phenotypes, genomic heterogeneity, radiogenomics, precision medicine
Introduction
Breast cancer is a highly heterogeneous disease, characterized by marked variability in clinical presentation, molecular subtypes, and therapeutic responses. This heterogeneity manifests both intertumorally, across different patients, and intratumorally, within a single tumor mass. For instance, triple-negative breast cancer (TNBC), which accounts for approximately 15–20% of all breast cancers, exemplifies this complexity with diverse molecular subtypes such as basal-like, mesenchymal-like, luminal androgen receptor, and immunomodulatory subtypes. These subtypes exhibit distinct radiologic features, underscoring the challenges in early diagnosis and tailored therapy.1,2 Furthermore, HER2-positive breast cancers demonstrate heterogeneity in HER2 amplification, which is associated with resistance to targeted therapies like trastuzumab emtansine, emphasizing the need for precise assessment of HER2 heterogeneity to guide treatment decisions.3,4 Intratumoral heterogeneity also extends to genomic alterations such as chromosomal instability and clonal diversity, which drive tumor evolution, progression, and therapeutic resistance.5 These complexities are further compounded by the heterogeneity of circulating tumor cells and clusters, which vary across breast cancer subtypes and impact metastatic potential and prognosis.6 Collectively, these findings highlight the intrinsic biological diversity of breast cancer, which poses significant challenges to the development of effective, personalized treatment strategies.
In recent years, the emergence of imaging genomics—or radiogenomics—has provided a promising avenue to bridge the gap between non-invasive imaging phenotypes and underlying genomic heterogeneity in cancer. Radiogenomics integrates quantitative imaging features with genomic data to uncover associations that can inform disease characterization, prognostication, and therapeutic response prediction. This approach leverages advances in radiogenomics to extract high-dimensional, reproducible imaging features that capture tumor heterogeneity beyond the limits of human visual assessment.7,8 In breast cancer, radiogenomics has been applied to identify imaging biomarkers correlated with molecular subtypes, gene expression profiles, and mutation status, facilitating non-invasive and spatially comprehensive tumor profiling.9 Moreover, the integration of radiomics and deep learning techniques has enhanced the ability to predict clinically relevant outcomes such as axillary lymph node metastasis.10–12 These methodologies enable capturing both intratumoral and peritumoral features, enhancing the performance of breast cancer diagnostic models.13 By combining imaging data with genomic information, radiogenomics offers the potential to overcome limitations of invasive biopsies and sampling bias, providing a holistic view of tumor biology that informs precision oncology.
The convergence of radiomics and deep learning technologies thus opens new opportunities for precision diagnosis and personalized treatment in breast cancer. Large-scale imaging and genomic datasets have been utilized to explore complex tumor heterogeneity and molecular characteristics, providing insights into molecular subtypes and gene expression signatures.14,15 These approaches have demonstrated superior performance compared to traditional radiomics models in predicting axillary lymph node status.16 Furthermore, the integration of clinical data with radiogenomic signatures enhances predictive accuracy and supports individualized treatment planning.17 The application of radiogenomics extends beyond breast cancer to other malignancies, illustrating its broad utility in oncology.18,19 Despite these advances, challenges remain regarding standardization of feature extraction, model interpretability, and validation.20 Addressing these issues is critical to translate radiogenomic insights into routine clinical practice, ultimately improving patient outcomes through more precise and non-invasive tumor characterization. This review will systematically explore the intersection of radiomics and deep learning in building the bridge between breast cancer imaging phenotypes and genomic heterogeneity, highlighting current progress, challenges, and future directions for advancing precision medicine in breast oncology.
The Relationship Between Imaging Phenotypes and Genomic Heterogeneity of Breast Cancer
Molecular Subtypes of Breast Cancer and Their Genomic Characteristics
Breast cancer is widely recognized as a heterogeneous disease characterized by diverse molecular subtypes with distinct genomic landscapes and clinical implications. The classification into molecular subtypes, notably through the PAM50 gene expression assay, has become a cornerstone in understanding breast cancer biology and tailoring therapeutic strategies. Molecular stratification of breast cancers includes intrinsic subtypes such as Luminal, HER2-enriched, and Basal-like, each exhibiting unique gene expression patterns and clinical outcomes.21 Basal-like and triple-negative breast cancers (TNBCs) are more aggressive and lack targeted treatment options, whereas luminal subtypes have distinct molecular characteristics.22,23 Molecular assays such as MammaPrint, TargetPrint, and BluePrint complement traditional immunohistochemical (IHC) classifications, improving risk stratification and guiding treatment decisions.24
The molecular heterogeneity of breast cancer extends beyond expression profiles to encompass a complex landscape of genomic alterations, including somatic mutations, copy number variations (CNVs), and epigenetic modifications. Key driver mutations including TP53, PIK3CA, and BRCA1/2 have been studied for their prevalence and distribution across breast cancer subtypes.25,26 PIK3CA mutations are frequently observed in canine mammary tumors with molecular subtypes analogous to human breast cancer, though specific associations with Luminal or Basal-like subtypes are not established.26 Copy number alterations on chromosome 17 involving ERBB2 and adjacent genes reveal molecular differences in HER2-negative breast cancers, though their role in defining HER2-enriched subtypes and tumor behavior requires further investigation.27 Genomic instability, measured by tumor mutational burden and mutant-allele tumor heterogeneity, varies among subtypes and associates with clinical features, though direct correlations with prognosis and therapeutic response remain to be fully elucidated.28 These genomic features underscore the biological complexity and necessitate integrated molecular profiling for precision medicine.
Recent advances have also revealed the significance of non-coding RNAs, including long non-coding RNAs (lncRNAs), in modulating gene expression and contributing to subtype-specific phenotypes. Comprehensive transcriptome analyses have identified novel lncRNAs associated with hormone receptor status and immune microenvironment modulation, linking them to breast cancer progression.29 Moreover, necroptosis-related lncRNA signatures have been proposed as prognostic markers and potential therapeutic targets, reflecting the interplay between cell death pathways and tumor heterogeneity.30 These findings suggest that integrating coding and non-coding genomic elements enriches our understanding of subtype biology.
The angiogenesis-related molecular subtypes represent another layer of heterogeneity, with distinct immune landscapes and genomic alterations influencing tumor microenvironment and treatment response. For example, angiogenesis subtypes identified through consensus clustering of TCGA data demonstrate differential expression of immune checkpoints and mutation burdens, which may affect immunotherapy efficacy.31 Similarly, proteomic and phosphoproteomic profiling has delineated subtypes with unique kinase activation patterns, providing insights into neoadjuvant treatment stratification.32 These multi-omic approaches highlight the dynamic interplay between genomic alterations and tumor microenvironment across subtypes.
Furthermore, cross-species genomic comparisons have identified parallels between human basal-like breast cancer and canine mammary tumors, reinforcing the molecular characteristics of aggressive subtypes and offering translational models for research.33,34 This comparative oncology approach may facilitate the discovery of conserved oncogenic pathways and therapeutic vulnerabilities.
Machine learning and deep learning techniques applied to multi-modal data, including genomic, transcriptomic, and imaging features, have enhanced the accuracy of molecular subtype prediction and prognosis assessment. Graph convolutional networks have demonstrated superior performance in classifying breast cancer subtypes, while integrative bioinformatics tools contribute to molecular characterization and prognostic gene signature identification.35–37 These computational advances enable the integration of heterogeneous data sources, capturing the complexity of breast cancer heterogeneity.
In summary, the molecular subtyping of breast cancer, grounded in comprehensive genomic characterization, provides critical insights into tumor biology and clinical management. The heterogeneity in gene mutations, copy number variations, expression profiles, and epigenetic regulation across subtypes underpins differences in prognosis and therapeutic response. Integrating multi-omic data with advanced computational methods holds promise for refining subtype classification and advancing precision oncology. It is crucial to continue validating these molecular features across diverse patient cohorts and exploring their functional implications to optimize subtype-specific interventions.
Diversity of Imaging Phenotypes and Their Biological Basis
Imaging phenotypes in breast cancer encompass a wide range of quantitative features extracted from medical images, capturing tumor morphology, texture heterogeneity, and dynamic contrast enhancement patterns. Tumor shape and size, as fundamental morphological characteristics, provide essential information on tumor aggressiveness and growth patterns. For example, MRI phenotypes such as tumor size, shape, and margin characteristics have been associated with molecular and cellular features, though direct correlations with invasiveness or benignity require further validation.38 Texture features derived from radiomic analysis quantify intratumoral heterogeneity by assessing gray-level variations, entropy, and spatial distribution of pixel intensities. These studies have modeled cellular plasticity and spatial diversity related to epithelial-mesenchymal transition in breast cancer organoids using imaging and deep learning approaches.39 Dynamic contrast-enhanced (DCE) imaging enriches phenotypic characterization by capturing spatial and kinetic heterogeneity relevant to tumor microenvironment features.40 The integration of these imaging features through artificial intelligence models enables more precise tumor subtyping and prognostication.
The biological basis of imaging phenotypes is increasingly elucidated by correlating radiomic features with histopathological and molecular data. Tumor morphology and texture heterogeneity often mirror variations in cellular density, extracellular matrix composition, and angiogenesis within the tumor microenvironment (TME). For instance, MRI-derived texture features correlate with gene expression profiles related to cell cycle regulation, DNA repair, and extracellular matrix remodeling.38 Dynamic enhancement patterns reflect vascular density and permeability.41 Moreover, imaging phenotypes such as heterogeneity in enhancement patterns have been associated with immune cell infiltration and immune checkpoint expression, indicating an interplay between tumor vascularity and immune microenvironment.40 These imaging biomarkers thus serve as non-invasive surrogates for complex biological processes within tumors.
Importantly, imaging phenotypes are closely linked to the tumor microenvironment and immune status. Multiplexed imaging studies have demonstrated spatial heterogeneity in tumor and immune cell populations, highlighting phenotypic diversity without direct linkage to imaging features or immune microenvironment classifications.42 Radiomics signatures derived from DCE-MRI have successfully distinguished breast tumors with high innate and adaptive immune cell infiltration from those with sparse immune presence, correlating with differential expression of hormone receptors and immune checkpoint molecules.40 The spatial distribution of cancer-associated fibroblasts (CAFs) has been characterized, though its influence on imaging texture and enhancement patterns remains to be established.43 This association underscores the potential of imaging phenotypes to non-invasively assess the immunological landscape of tumors, which is critical for predicting response to immunotherapy.
Emerging computational frameworks leverage multiplexed tissue imaging and advanced machine learning to dissect the spatial organization of tumor ecosystems at single-cell resolution, providing deeper insight into the biological underpinnings of imaging phenotypes. Spatially resolved single-cell analysis integrates morphological and topological features to classify tumor, stromal, and immune cells, revealing microecological modules associated with molecular features and patient prognosis.44 These approaches facilitate the identification of prognostic spatial biomarkers, such as lymphocyte infiltration patterns and fibroblast neighborhoods.45 The convergence of high-dimensional imaging data with molecular profiling thus bridges the gap between radiological phenotypes and the biological complexity of the tumor microenvironment.
In addition to static imaging, longitudinal and dynamic imaging techniques capture temporal heterogeneity and phenotypic plasticity within tumors. Functional 4-D imaging modalities, such as dynamic FDG PET, characterize kinetic intratumor heterogeneity by identifying distinct subpopulations with unique metabolic activity profiles, revealing tumor biology and prognostic information.46 Simulation-based methods further link PET-derived radiomic features to microscopic tumor parameters, including hypoxia and necrosis, enhancing the biological interpretability of imaging phenotypes.47 These dynamic imaging phenotypes reflect the evolving tumor biology and microenvironmental interactions, providing a more comprehensive understanding of tumor heterogeneity.
Collectively, the diversity of imaging phenotypes in breast cancer arises from complex biological processes involving tumor cell morphology, microenvironmental composition, vascular characteristics, and immune infiltration. The integration of radiomics, multiplexed imaging, and machine learning enables the dissection of these phenotypes and their biological basis, offering promising avenues for non-invasive tumor characterization, prognostication, and personalized therapy selection.48 This multidisciplinary approach advances the potential of imaging biomarkers to serve as surrogates for molecular and cellular heterogeneity, ultimately bridging the gap between imaging phenotypes and tumor biology.
The Bridging Role of Radiogenomics
Radiogenomics serves as a critical bridge connecting imaging phenotypes with genomic heterogeneity in breast cancer, enabling noninvasive characterization of tumor biology and providing insights into the molecular underpinnings of imaging features (Figure 1). Imaging phenotypes, derived from modalities such as dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI), capture spatial and temporal heterogeneity within tumors, reflecting variations in cellular architecture, microenvironment, and metabolic activity. These phenotypes represent a macroscopic manifestation of underlying genomic heterogeneity, which includes diverse gene expression patterns, mutational landscapes, and pathway activations that drive tumor progression and therapeutic response. For instance, deep learning radiomics (DLR) models applied to DCE-MRI have demonstrated high accuracy in predicting lymph node metastasis (LNM) in invasive breast cancer, with the associated imaging features correlating significantly with classical tumor signaling pathways related to immune response, signal transduction, and cell death. The identification of hub genes linked to these imaging phenotypes facilitates the calculation of gene expression scores (eg., RadDeepGene), which strongly predict metastatic risk, thereby underscoring the biological relevance of radiomic signatures as surrogates of genomic alterations.49
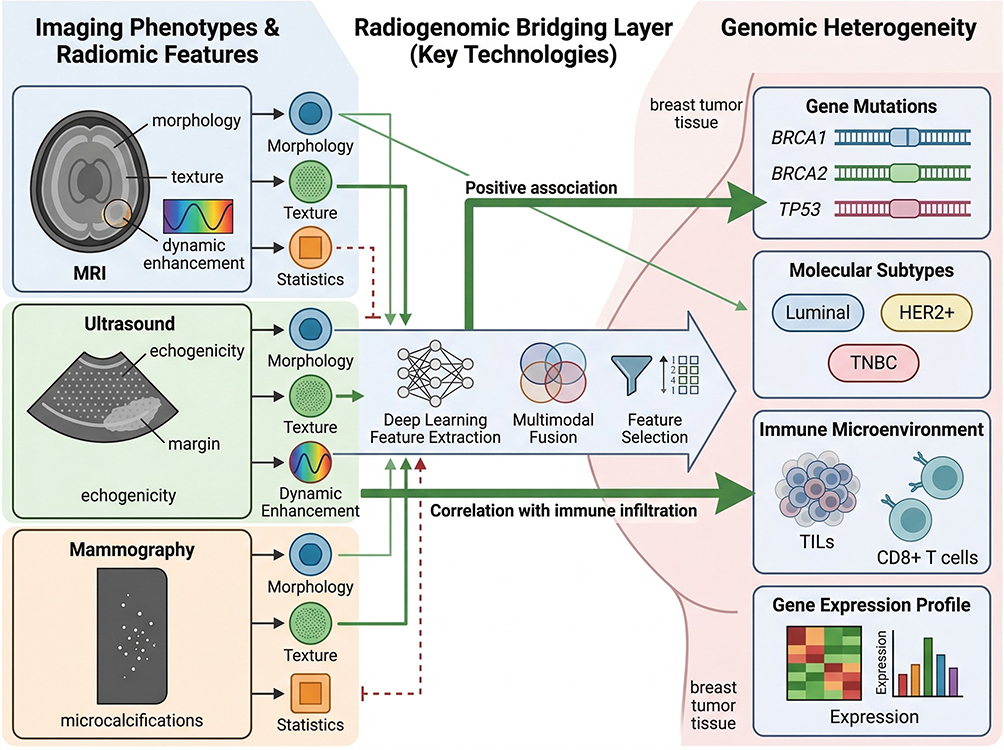 |
Figure 1 Schematic diagram of radiogenomics bridging imaging phenotypes and genomic heterogeneity in breast cancer. This schematic illustrates the core mechanism of radiogenomics in linking breast cancer imaging phenotypes to genomic heterogeneity. On the left, typical imaging phenotypes (MRI morphological/texture/dynamic enhancement features, ultrasound echo/border features, mammography microcalcification features) and extracted radiomic features (morphological, texture, statistical features) are shown. The middle radiogenomics bridge layer displays key technologies including deep learning-based feature extraction, multimodal fusion, and feature selection. On the right, genomic heterogeneity dimensions (gene mutations (BRCA1/2/TP53), molecular subtypes (Luminal/HER2+/TNBC), immune microenvironment (TILs/CD8+ T cells), and gene expression profiles) are presented, with core associations (e.g., texture features positively correlated with TP53 mutation) annotated with corresponding references. |
The integration of radiomic and genomic data has advanced the understanding of breast cancer heterogeneity beyond what either modality can achieve alone. Radiomics extracts quantitative features from imaging data that characterize tumor shape, texture, and intensity, while genomics provides molecular insights at multiple levels, including gene mutations, transcriptomics, and pathway activities. Studies utilizing multi-omics approaches have revealed that deep radiomic features outperform traditional handcrafted features in predicting clinical characteristics such as tumor size, hormone receptor status, and lymph node involvement, with stronger associations to risk genes and biological pathways. This enhanced predictive power is attributed to the ability of deep learning frameworks to capture high-order, complex imaging patterns that better reflect the tumor’s molecular landscape. Moreover, the spatial heterogeneity captured by imaging corresponds with intratumor heterogeneity observed at the genomic level, which is a major determinant of prognosis and therapeutic resistance. Imaging intratumor heterogeneity (IITH) assessed by radiomics correlates with genomic heterogeneity and clinical features, providing insights into tumor biology.50,51
Current research on radiogenomics emphasizes the synergy between imaging and genomics to develop multidimensional models for precision breast cancer management. Integrative analyses link radiomic features with transcriptomic and genomic profiles to stratify patients, predict treatment response, and forecast outcomes. For instance, interpretable imaging phenotypes derived from AI-driven analysis of 4D DCE-MRI data have been shown to correlate with tumor microenvironment markers and molecular signatures, including hormone receptor and immune checkpoint protein expression, offering prognostic value superior to conventional radiomics or black-box deep learning methods. This interpretability enhances clinical relevance by elucidating the biological basis of imaging features and facilitating personalized treatment decisions.40 Additionally, radiogenomic models have been developed to noninvasively estimate immune cell infiltration, such as γδT cell abundance in triple-negative breast cancer, which is linked to favorable prognosis and differential benefit from chemo- or immunotherapy. The ability to infer immune landscape from imaging further exemplifies the bridging role of radiogenomics in connecting phenotype with genotype and immune contexture.52
Despite promising advances, challenges remain in integrating imaging and genomic data effectively. Variability in imaging protocols, feature extraction methods, and genomic data processing complicate standardization and reproducibility. Moreover, many radiogenomic studies rely on retrospective cohorts with limited sample sizes, underscoring the need for large-scale, multicenter datasets and external validations to ensure generalizability. Recent efforts to develop user-friendly computational tools, such as MuSA, facilitate multi-omics data integration and analysis, enabling researchers without programming expertise to explore radiogenomic associations and generate hypotheses. These tools support modular workflows encompassing data preprocessing, normalization, clustering, and feature selection, thereby promoting broader adoption of radiogenomics in breast cancer research.53 The evolving landscape of artificial intelligence, including deep learning and multimodal data fusion, holds promise for improving the accuracy and interpretability of imaging models in breast cancer diagnosis and treatment.54,55
In summary, radiogenomics acts as a vital conduit linking imaging phenotypes with genomic heterogeneity in breast cancer, facilitating noninvasive tumor characterization, prognostication, and personalized therapy. The integration of advanced radiomics, deep learning, and multi-omics data continues to refine our understanding of tumor biology, offering new avenues for precision oncology. Continued methodological improvements, standardization efforts, and validation studies are essential to translate radiogenomic insights into routine clinical practice, thereby bridging the gap between imaging and genomics for improved patient outcomes.
Detailed Workflow of Radiomics
Image Acquisition and Preprocessing
Breast cancer imaging employs multiple modalities, each offering unique advantages for diagnosis and treatment planning. The most commonly used imaging techniques include Magnetic Resonance Imaging (MRI), mammography (breast X-ray), ultrasound (US), and positron emission tomography (PET). MRI is useful in detecting breast lesions and provides detailed soft tissue contrast, aiding in the evaluation of tumor extent and multifocality.56 Mammography is widely used for breast cancer detection and plays a role in identifying microcalcifications and masses, though sensitivity may be affected by breast density.57 Ultrasound is utilized in breast cancer detection and classification, with advances in deep learning improving image segmentation and classification accuracy.58 PET imaging, often combined with CT (PET/CT), offers metabolic information that aids in staging and treatment response assessment.59 The integration of these modalities enhances the overall diagnostic accuracy and provides comprehensive phenotypic information necessary for personalized treatment strategies.
Preprocessing of imaging data is critical to ensure the reliability and reproducibility of subsequent radiomic and deep learning analyses. Standardization techniques such as image normalization, noise reduction, and registration are routinely applied to reduce variability introduced by different scanners, acquisition protocols, and patient motion. Intensity normalization methods, including Z-score normalization within organ masks, have demonstrated superiority in harmonizing images across different MRI vendors and field strengths, ensuring comparable intensity distributions essential for robust feature extraction.60 Noise removal techniques, including Wiener filtering and speckle noise filtering with block-matching three-dimensional filtering, are applied in ultrasound image preprocessing and contribute to improved classification performance.58,61 Multimodal deep learning frameworks combining MRI and ultrasound data have demonstrated effectiveness in predicting axillary lymph node metastasis.62
Advanced preprocessing includes image enhancement techniques such as contrast-limited adaptive histogram equalization (CLAHE), which improve the visibility of subtle lesions and texture patterns critical for radiomic analysis.63,64 Segmentation of regions of interest (ROIs), such as breast parenchyma, is often performed using deep convolutional neural networks like U-Net variants, enabling precise delineation and optimizing feature extraction.65 The combination of these preprocessing steps lays a solid foundation for extracting high-quality quantitative imaging biomarkers that reflect underlying tumor biology and heterogeneity.
The choice of imaging modality and preprocessing protocol can significantly impact the extracted radiomic features and the performance of predictive models. Radiomic features extracted from T2-weighted axillary MRI have been studied for their role in lymph node metastasis prediction, though sensitivity to segmentation and acquisition variability requires further investigation.66 Similarly, the reproducibility of radiomic features from mammography can be influenced by imaging physics parameters such as kV and mAs settings, necessitating the selection of robust features less susceptible to such variations.67,68 Harmonization techniques like ComBat have been employed to mitigate batch effects arising from multi-center datasets, enhancing the generalizability of machine learning models across heterogeneous imaging sources.69
Recent advances in deep learning have further refined preprocessing workflows by integrating automated denoising, normalization, and segmentation into end-to-end pipelines. Transfer learning approaches leveraging pretrained convolutional neural networks (CNNs) on large mammography or ultrasound datasets have improved lesion detection and classification accuracy, even with limited annotated data.58,70 Moreover, the development of multimodal deep learning models that fuse MRI and ultrasound features has demonstrated superior predictive performance for clinically relevant endpoints such as axillary lymph node metastasis.62 These models benefit from meticulous preprocessing that ensures data consistency and feature reliability.
In summary, the acquisition of breast cancer imaging data across multiple modalities combined with rigorous preprocessing steps such as normalization, noise reduction, and registration is fundamental to extracting meaningful imaging biomarkers. These processes enable the development of robust radiomics and deep learning models that can bridge imaging phenotypes with underlying genomic heterogeneity, ultimately contributing to personalized breast cancer management. The continuous refinement of preprocessing techniques tailored to specific imaging modalities and clinical tasks is essential to maximize the potential of radiomics and artificial intelligence in breast cancer diagnostics and prognostics.
Tumor and Region of Interest (ROI) Delineation
Accurate delineation of tumors and regions of interest in breast cancer imaging is a critical step in radiomics and deep learning workflows, as it directly influences the quality of feature extraction and subsequent analyses. Traditionally, manual contouring by expert radiologists has been the gold standard for tumor segmentation. Manual delineation is subject to inter-observer variability, which can introduce inconsistencies in radiomic feature quantification and affect reproducibility of predictive models.71 To mitigate these limitations, semi-automatic and fully automatic segmentation methods have been developed, leveraging advances in deep learning architectures such as U-Net, Transformer-based models, and their variants.
Semi-automatic segmentation approaches typically combine initial manual inputs, such as seed points or bounding boxes, with algorithmic refinement to delineate tumor boundaries. For example, a semi-automatic segmentation method based on a seeded region growing algorithm has been applied to breast MRI images, enabling efficient tumor area delineation that balances accuracy and user effort.72 Despite reducing workload, semi-automatic methods may still require expert involvement and can be influenced by the initial inputs, potentially affecting reproducibility.
Fully automatic segmentation methods harness deep learning to achieve rapid and consistent tumor delineation without manual intervention. Transformer-based segmentation models have demonstrated superior performance compared to traditional convolutional neural networks like U-Net in mammographic tumor segmentation, achieving high Dice Similarity Coefficients (DSC) around 0.92 in test datasets.73 These models not only improve segmentation accuracy but also enhance downstream radiomic feature extraction, leading to improved classification of breast lesions into benign and malignant categories. Similarly, deep learning architectures such as dense U-Net, recurrent residual U-Net (R2UNet), and dense R2UNet have been successfully applied to segment triple-negative breast cancer patient-derived tumor xenografts on preclinical MRI images, yielding F1-scores exceeding 0.94 and high correlation of extracted radiomic features with expert consensus segmentations.74
The accuracy of segmentation profoundly impacts the robustness and reproducibility of radiomic features. Studies have shown that inter-observer variability in manual segmentation can result in significant differences in feature extraction; for instance, only about 33–42% of radiomic features were identified as robust against inter-observer variability in breast MRI tumor segmentations.71 Automated segmentation methods can reduce such variability, providing more consistent tumor masks that improve the reliability of radiomic analyses. Moreover, features extracted from automatically segmented tumor regions have been demonstrated to retain prognostic value, such as predicting disease-free survival in invasive breast cancer using multi-modal imaging signatures derived from ultrasound and MRI.75
In addition to tumor segmentation, delineation of peritumoral regions has gained attention due to their biological significance and contribution to radiomic signatures. Radiomic features extracted from peritumoral areas on MRI and PET imaging have been shown to enhance prediction of pathological complete response to neoadjuvant chemotherapy in breast cancer.76,77 Accurate segmentation of both intra- and peritumoral regions is thus essential for comprehensive tumor phenotyping.
Recent advances also include weakly supervised and weak annotation strategies that reduce the need for precise manual annotations while maintaining segmentation performance. For example, a 3D U-Net transformer model trained with bounding box annotations achieved median DSCs of 0.75 for whole breast and 0.89 for ROI segmentations on DCE-MRI, demonstrating the feasibility of efficient segmentation with limited annotation effort.78 Such approaches facilitate scaling to large datasets and integration into clinical workflows.
Furthermore, the choice of imaging modality and segmentation method can influence the downstream predictive models. For instance, Transformer-based segmentation coupled with radiomic feature selection and ensemble classifiers outperformed U-Net-based segmentation in mammographic breast cancer diagnosis, achieving classification accuracies above 90% compared to 84%.73 This suggests that segmentation quality directly affects the diagnostic utility of radiomics and deep learning models.
In summary, the evolution from manual to semi-automatic and fully automatic segmentation techniques has substantially improved the accuracy, reproducibility, and efficiency of tumor and ROI delineation in breast cancer imaging. High-quality segmentation is foundational for reliable radiomic feature extraction and robust predictive modeling. Continued integration of advanced deep learning architectures, combined with strategies to reduce annotation burden, promises to further enhance tumor delineation and enable scalable, precise breast cancer imaging phenotyping. Segmentation approaches based on deep learning have been developed and evaluated across various breast imaging modalities, demonstrating potential for clinical application.73–75
Feature Extraction
Feature extraction is a fundamental step in radiomics and deep learning workflows, involving the quantitative characterization of breast cancer imaging data to capture tumor heterogeneity and relevant phenotypic traits. In breast cancer imaging analysis, extracted features generally fall into several categories: morphological features, texture features, and statistical features. Morphological features describe the shape, size, and geometric properties of the lesion, such as tumor volume, sphericity, and surface area. Texture features quantify patterns of pixel intensity variations within the tumor region, capturing heterogeneity that may correlate with cellular architecture and microenvironmental factors. Statistical features include first-order histogram-based metrics reflecting intensity distribution within the lesion, though specific metrics such as mean intensity, variance, skewness, and kurtosis require further specification.79
Traditionally, handcrafted radiomics features are extracted using predefined algorithms and mathematical descriptors applied to segmented regions of interest. For example, texture features derived from gray-level co-occurrence matrices (GLCM), gray-level run-length matrices (GLRLM), and wavelet transforms have been widely used to characterize breast tumors on modalities such as MRI, ultrasound, and mammography. These handcrafted features provide interpretable metrics and have demonstrated associations with clinical outcomes.80,81 However, handcrafted features are limited by their dependence on accurate lesion segmentation and may not fully capture complex tumor patterns.
In contrast, deep learning-based feature extraction leverages convolutional neural networks or other architectures to automatically learn high-level abstract features directly from imaging data without manual feature engineering. Deep learning features are often extracted from intermediate layers of pretrained or task-specific networks, capturing hierarchical representations of tumor characteristics. Studies have shown that deep learning features outperform traditional handcrafted radiomics in predicting clinical endpoints such as axillary lymph node metastasis, pathological complete response (pCR) to neoadjuvant chemotherapy, and distant metastasis risk.51,82,83 MRI-based deep radiomic features extracted via DenseNet architectures have demonstrated predictive performance in lymph node metastasis prediction, with associations to clinical features.51,84
Comparative analyses between traditional radiomics and deep learning feature extraction reveal complementary strengths. Traditional radiomics provides interpretable, handcrafted features that can be linked to known imaging biomarkers, while deep learning extracts complex, high-dimensional features that capture subtle imaging phenotypes. Fusion models integrating both feature types have achieved improved diagnostic and prognostic accuracy in breast cancer. For example, combining handcrafted radiomics with deep learning signatures in a nomogram significantly enhanced prediction of axillary lymph node metastasis compared to either feature set alone.16,85 Similarly, fusion of radiomics and deep learning features from intra-tumoral and peri-tumoral regions improved discrimination between breast cancer lung metastases and primary lung cancer.86
Moreover, deep learning feature extraction benefits from end-to-end training and can incorporate multimodal imaging data, such as combining ultrasound radiomics with clinical parameters or PET/CT radiomics, to boost predictive performance.17,87 Transfer learning techniques have been applied to breast imaging tasks, where pretrained CNNs like ResNet and DenseNet are fine-tuned on breast cancer datasets to extract robust features.55,88 The integration of radiomics and deep learning features within a unified framework enables the capture of both global and local tumor characteristics, facilitating more accurate and generalizable models for breast cancer diagnosis, treatment response prediction, and metastasis risk stratification.
Additionally, the inclusion of peritumoral region features alongside intratumoral features has been shown to enhance model performance, as the tumor microenvironment contributes important biological information. Deep learning models incorporating peritumoral regions extracted from ultrasound or mammography images achieved higher AUCs for distinguishing malignant from benign lesions.13,89 This suggests that deep learning-based feature extraction can effectively mine rich phenotypic information beyond the tumor core.
In summary, feature extraction in breast cancer radiomics encompasses a spectrum from handcrafted morphological, texture, and statistical features to automatically learned deep learning features. While traditional radiomics offers interpretability and established imaging biomarkers, deep learning provides powerful hierarchical representations that capture complex tumor heterogeneity. Combining these approaches through fusion models consistently yields superior predictive accuracy, supporting their integration in clinical decision support systems for breast cancer management.16,17,85
The evolving evidence indicates that leveraging both traditional and deep learning feature extraction methods can better characterize the phenotypic and genomic heterogeneity of breast cancer, potentially enabling more personalized and precise diagnosis and treatment strategies (Table 1). Future research should focus on optimizing feature fusion strategies and model validation in breast cancer imaging studies.90
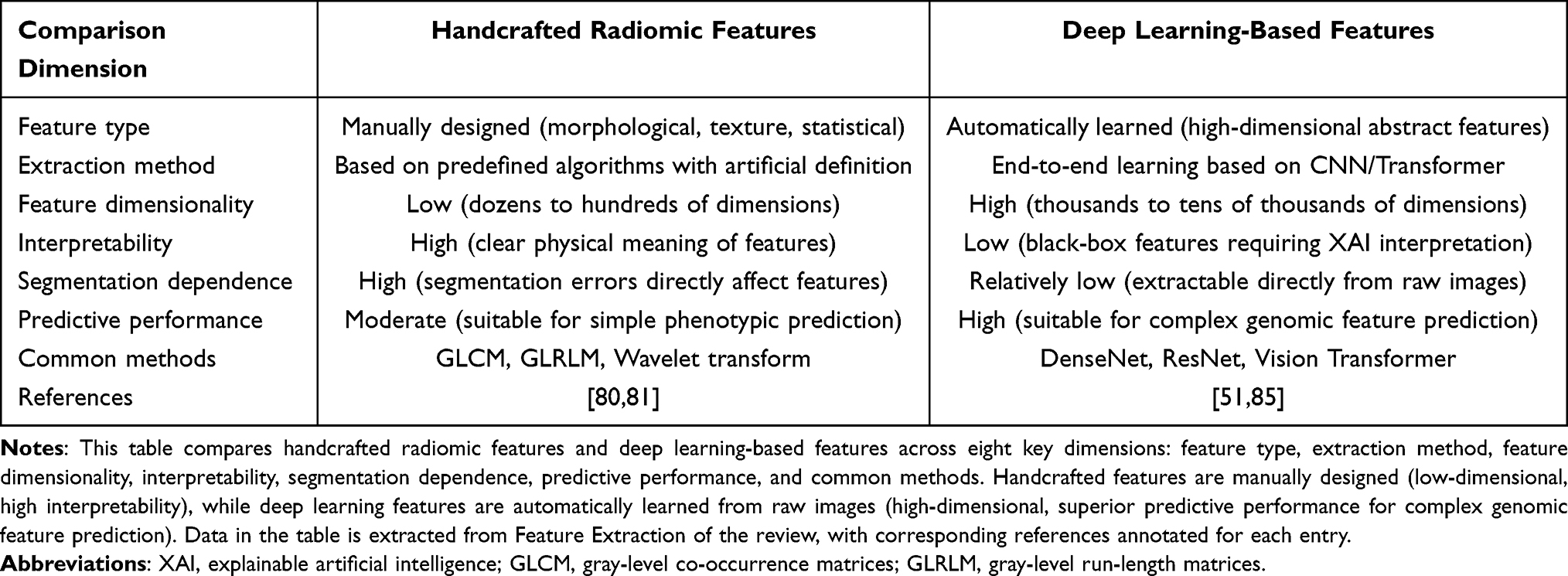 |
Table 1 Comparison of Handcrafted Radiomic Features and Deep Learning-Based Features in Breast Cancer Radiomics |
Feature Selection and Dimensionality Reduction
Feature selection and dimensionality reduction are critical steps in radiomics and deep learning pipelines for breast cancer imaging analysis, serving to enhance model efficiency, reduce computational burden, and improve generalization by avoiding overfitting. Several established methods, including correlation analysis, principal component analysis (PCA), and least absolute shrinkage and selection operator (LASSO), have been widely applied to identify the most informative features from high-dimensional datasets.
Correlation analysis is often employed as an initial screening step to remove redundant features that exhibit high pairwise correlation, thereby reducing multicollinearity within the dataset. For example, in a study integrating B-mode ultrasound (BMUS) and color Doppler ultrasound (CDUS) imaging for sentinel lymph node (SLN) metastasis prediction in breast cancer, Pearson correlation analysis was used to filter features before applying LASSO regression for further selection.91 This two-step process ensures that the final model includes features that are both independent and predictive, enhancing robustness.
Principal component analysis is a widely used unsupervised dimensionality reduction technique that transforms the original feature space into a smaller set of orthogonal components capturing the majority of variance. In a radiomics model based on dynamic contrast-enhanced MRI for predicting SLN metastasis, PCA was utilized after normalization to reduce feature dimensionality before classification with support vector machines (SVM), resulting in improved model performance.92 PCA helps to condense complex radiomic data into principal components that retain essential information while minimizing noise, which is particularly beneficial when sample sizes are limited relative to feature numbers.
LASSO regression, a regularization method that imposes an L1 penalty on feature coefficients, effectively shrinks less important feature weights to zero, thus performing both feature selection and regularization. Multiple studies have demonstrated the utility of LASSO in breast cancer radiomics. For instance, in a multimodal mammography and MRI study predicting axillary lymph node metastasis, LASSO was employed to select key features from combined radiomics and deep learning outputs, which contributed to a combined model achieving an area under the curve (AUC) of 0.846.93 Similarly, in MRI radiomics models assessing HER2 expression status, LASSO facilitated the selection of discriminative features from multiparametric sequences, improving prediction accuracy.94 LASSO’s ability to prevent overfitting by penalizing excessive complexity is crucial for developing generalized models applicable to diverse patient cohorts.
Beyond these traditional techniques, hybrid and ensemble approaches have also been explored. For example, a study predicting chemotherapy response in locally advanced breast cancer combined matrix rank-based filtering to remove dependent features with a genetic algorithm coupled to SVM for optimal feature subset selection and hyperparameter tuning, achieving an accuracy of 88%.95 This highlights the trend towards integrating multiple feature selection strategies to balance dimensionality reduction and model optimization.
Importantly, effective feature selection and dimensionality reduction directly contribute to avoiding overfitting—a common pitfall when models are trained on high-dimensional radiomic data with relatively small sample sizes. By reducing irrelevant or redundant features, models are less likely to capture noise or spurious correlations, thereby enhancing their ability to generalize to independent datasets. For instance, in ultrasound-based radiomics combined with immune status to predict SLN metastasis, LASSO-selected features enabled logistic regression models to achieve AUCs of 0.91 and 0.79 in training and validation cohorts, respectively, demonstrating strong reproducibility.96
Moreover, combining features from multiple imaging modalities or tumor regions often necessitates dimensionality reduction to manage the increased feature space. Studies integrating intratumoral and peritumoral radiomics features have applied LASSO to identify optimal predictive signatures, improving the performance of neoadjuvant chemotherapy efficacy prediction models.97 This approach underscores that dimensionality reduction is not only a technical necessity but also a strategic step to capture biologically relevant heterogeneity while maintaining model parsimony.
In summary, feature selection and dimensionality reduction methods such as correlation analysis, PCA, and LASSO are indispensable tools in breast cancer radiomics and deep learning workflows. These methods help distill high-dimensional imaging data into concise, informative feature sets that improve model accuracy and robustness while mitigating overfitting risks. The integration of multiple techniques and consideration of multimodal data further enhance model generalizability and clinical utility.
The consistent success of LASSO-based feature selection across diverse imaging modalities and prediction tasks suggests that sparsity-inducing regularization is particularly well-suited for managing the complexity of radiomic data in breast cancer. This supports the continued development of hybrid feature selection frameworks that combine statistical filtering, dimensionality reduction, and machine learning optimization to refine predictive models for personalized breast cancer management.91,93,94
Modeling and Validation
The construction of predictive models in radiogenomic studies of breast cancer integrates advanced machine learning and deep learning techniques to capture the complex relationships between imaging phenotypes and genomic heterogeneity. Traditional machine learning models such as Support Vector Machines and Random Forests (RF) have been widely employed for classification and prediction tasks due to their robustness and interpretability. For instance, SVM classifiers have been effectively used to predict gene expression levels such as CXCL9 from MRI radiomic features, achieving AUC values of 0.748 in training and 0.711 in validation cohorts, demonstrating moderate predictive capability.98 Similarly, RF models have been applied in ultrasound imaging for breast cancer diagnosis, yielding classification accuracies near 78.5% when combined with deep radiomic features extracted through convolutional autoencoders.99 These models typically rely on handcrafted or semi-automatically extracted radiomic features, which, while interpretable, may not fully capture the high-dimensional heterogeneity of tumor phenotypes.
In recent years, deep learning models, especially convolutional neural networks, have revolutionized the field by enabling automatic feature extraction and hierarchical representation learning from raw imaging data. CNN-based architectures such as ResNet and DenseNet have been adapted for breast cancer imaging tasks, including prediction of molecular subtypes, treatment response, and recurrence risk. For example, a 3-block DenseNet deep learning classifier applied to ultrasound images predicted HER2 expression with accuracies exceeding 80% and AUCs around 0.84, outperforming traditional radiomics models.100 Moreover, multimodal deep learning fusion models integrating features from intratumoral and peritumoral ultrasound regions have demonstrated high predictive performance for early tumor response to neoadjuvant chemotherapy, with AUCs reaching up to 0.965 in internal validations.101 These deep learning models often employ stacking or ensemble strategies to combine features from multiple image regions or modalities, enhancing robustness and generalizability.
Beyond CNNs, graph neural networks (GNNs) and attention-based deep graph clustering models have emerged to model the spatial heterogeneity and interactions within the tumor microenvironment, which are critical for understanding breast cancer heterogeneity. An unsupervised dual-attention deep graph clustering model (DGCLM) was developed to segment breast tumors into spatially distinct phenotypic subclusters using 4D dynamic contrast-enhanced MRI data. This model leverages human-interpretable imaging phenotypes and achieves superior accuracy and transparency compared to conventional radiomics and black-box deep learning methods.40 The application of GNNs allows for capturing complex spatial dependencies and intercellular interactions that conventional CNNs might overlook, providing a more biologically relevant representation of tumor heterogeneity.
Model performance evaluation in breast cancer radiogenomic studies commonly utilizes metrics such as the area under the receiver operating characteristic curve, accuracy, sensitivity, specificity, and calibration curves. Cross-validation strategies, including nested and stratified k-fold cross-validation, are implemented to ensure robustness and reduce overfitting. For example, in predicting axillary lymph node metastasis, radiomics models based on dynamic contrast-enhanced MRI achieved AUCs up to 0.99 in training and 0.86 in validation cohorts, with decision curve analysis confirming clinical benefits.102 Similarly, radiomics models for predicting pathological complete response after neoadjuvant chemotherapy have been validated using independent external cohorts, with AUCs exceeding 0.90 in some studies.103 The integration of clinical variables with radiomic or deep learning features through nomograms or combined models often enhances predictive accuracy, as demonstrated in HER2 status classification and recurrence risk prediction.104,105
Furthermore, explainability and interpretability have become critical aspects of model validation. Techniques such as SHapley Additive exPlanations (SHAP) and Gradient-weighted Class Activation Mapping (Grad-CAM) are employed to elucidate feature contributions and model decision-making processes. For instance, SHAP analysis quantified the importance of radiomic features in predicting treatment response, linking imaging features to underlying biological pathways such as immune activation and cell proliferation.106 Grad-CAM has been applied in ultrasound image classification models to provide visual explanations of model decisions.107 These interpretability methods facilitate the translation of complex models into clinically actionable tools.
The combination of radiomic and genomic data—radiogenomics—further refines predictive modeling by incorporating molecular-level insights. Radiogenomic models integrating MRI radiomics and transcriptomic data have shown non-significant trends toward improved performance in predicting axillary lymph node metastasis and neoadjuvant chemotherapy response compared to unimodal models.108,109 Machine learning algorithms, including logistic regression, random forests, and support vector machines, are used to select and integrate multimodal features. Although some studies report modest improvements without statistical significance, the potential for enhanced individualized treatment planning is evident.109 The interpretability of such models is augmented by linking imaging features with gene expression pathways, providing a biological rationale for model predictions.
In summary, the modeling and validation of breast cancer radiogenomic predictive models have evolved from traditional machine learning approaches to sophisticated deep learning and graph-based models that capture spatial and phenotypic tumor heterogeneity. Performance evaluation employs rigorous cross-validation and multiple metrics, while interpretability techniques ensure clinical relevance. The integration of multimodal data promises more precise and personalized predictions, although further large-scale validation is necessary to confirm clinical utility. Future research should focus on harmonizing datasets, improving model generalizability across diverse populations, and enhancing explainability to facilitate adoption in routine clinical practice (Figure 2).
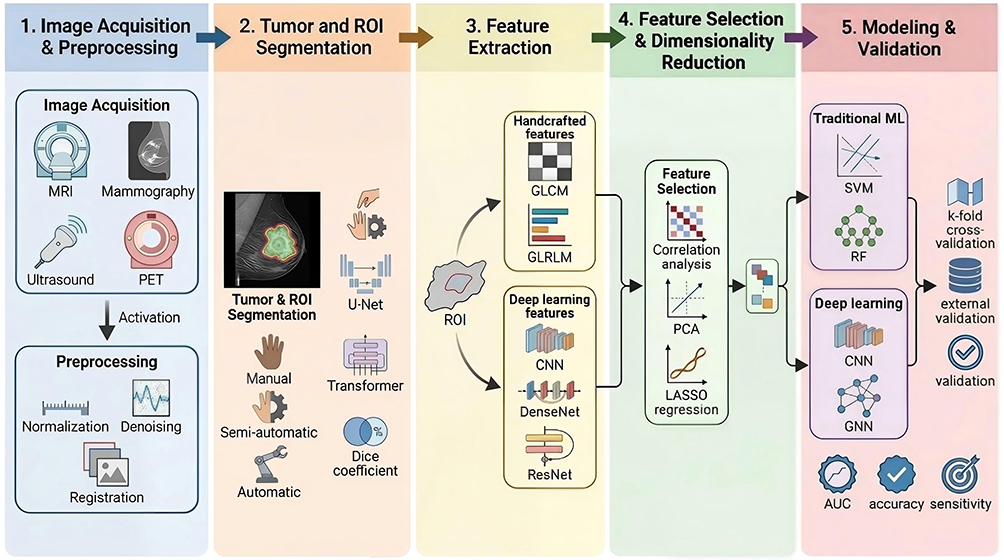 |
Figure 2 Technical workflow of breast cancer radiomics from image acquisition to model validation. This flow chart depicts the complete technical workflow of breast cancer radiomics, divided into five core steps: (1) Image acquisition and preprocessing (modalities including MRI/mammography/ultrasound/PET, preprocessing operations: normalization, denoising, registration); (2) Tumor and ROI segmentation (manual/semi-automatic/automatic segmentation with U-Net/Transformer models, evaluated by Dice similarity coefficient); (3) Feature extraction (handcrafted features: GLCM/GLRLM; deep learning features: CNN/DenseNet/ResNet); (4) Feature selection and dimensionality reduction (methods: correlation analysis, PCA, LASSO regression); (5) Modeling and validation (traditional machine learning: SVM/RF; deep learning: CNN/GNN; validation methods: k-fold cross-validation, external validation; evaluation metrics: AUC/accuracy/sensitivity). Key references for each step are annotated to ensure scientific rigor. |
Application of Deep Learning in Breast Cancer Radiomics
Automatic Feature Learning and Representation
Convolutional Neural Networks have revolutionized the field of medical image analysis by their ability to automatically learn hierarchical and high-level features directly from imaging data, bypassing the need for manual feature engineering. In breast cancer imaging, CNNs can extract complex patterns from modalities such as ultrasound, mammography, MRI, and CT, enabling improved differentiation between benign and malignant lesions, as well as prediction of metastatic status. CNN architectures like DenseNet121, ResNet50, and VGG16 have been utilized to learn discriminative features for breast cancer diagnosis and axillary lymph node metastasis prediction, with combined models showing improved performance.85,110 This automatic feature extraction capability allows CNNs to capture subtle imaging phenotypes that may be imperceptible to human observers, thereby enhancing diagnostic accuracy and aiding clinical decision-making.
The integration of deep learning features with radiomics and clinical data has shown synergistic effects in improving model performance. Studies have demonstrated that combining CNN-extracted features with radiomics and patient clinical parameters yields higher area under the curve values and better sensitivity and specificity compared to models using either feature set alone.17,85,110 This suggests that CNNs can complement traditional radiomics by capturing additional abstract representations of tumor heterogeneity and microenvironment characteristics. Deep learning features extracted from both intratumoral and peritumoral regions have been shown to provide comprehensive tumor information, enhancing classification performance in differentiating breast cancer lung metastases from primary lung cancer.13,86 The peritumoral region, often overlooked in conventional analyses, contains valuable contextual information reflecting tumor-host interactions, which CNNs can effectively exploit through automatic feature learning.
Transfer learning and the use of pretrained models constitute another major advantage in breast cancer imaging applications. Given the limited availability of large annotated medical imaging datasets, leveraging CNNs pretrained on large-scale natural image datasets such as ImageNet has become a standard approach. Transfer learning allows models pretrained on large datasets to be fine-tuned for breast imaging tasks, demonstrating feasibility though effects on training efficiency and generalization require further study.88 ResNet50 and DenseNet201 pretrained models have been adapted for digital breast tomosynthesis classification tasks, achieving moderate performance despite relatively small sample sizes.17,88 This approach reduces the risk of overfitting and enables rapid development of robust diagnostic tools.
Furthermore, advanced training strategies such as curriculum learning guided by radiomics scores have been proposed to enhance CNN training by incorporating domain knowledge. In one study, a radiomics-informed deep curriculum learning framework weighted the loss function based on radiomics-derived difficulty scores for each sample, allowing the CNN to focus progressively on harder cases during training. This method improved breast cancer classification performance compared to standard CNN training or direct use of radiomics features as inputs.111 Such hybrid training paradigms exemplify the potential of combining handcrafted and automatically learned features to optimize model learning dynamics and robustness.
In summary, CNNs enable automatic extraction of high-level imaging features that capture complex tumor phenotypes and microenvironmental context, which are critical for accurate breast cancer diagnosis and prognosis prediction. The use of transfer learning with pretrained models facilitates effective model training on limited datasets, while integration with radiomics and clinical data further enhances predictive performance. Emerging training techniques that incorporate radiomics knowledge into deep learning frameworks offer promising avenues to improve model generalizability and clinical applicability. These advances collectively contribute to bridging the gap between breast cancer imaging phenotypes and underlying genomic heterogeneity, supporting precision oncology efforts.
Multimodal Imaging Data Fusion
The integration of diverse imaging modalities such as magnetic resonance imaging, positron emission tomography, and ultrasound has become a pivotal strategy in enhancing the diagnostic accuracy and prognostic assessment of breast cancer. Multimodal imaging data fusion leverages the complementary strengths of each modality to capture comprehensive tumor characteristics, including morphological, functional, and molecular information, which are often unattainable through single-modality imaging. For instance, MRI offers superior soft tissue contrast and functional imaging capabilities, PET provides metabolic and molecular insights, while ultrasound is widely accessible and effective for real-time imaging of breast lesions. Methods for multimodal data fusion typically fall into early fusion, intermediate fusion, and late fusion strategies, each differing in the stage at which data integration occurs within the analytical pipeline.
Early fusion approaches combine raw or preprocessed data from multiple modalities before feature extraction, allowing models to learn joint representations that capture inter-modality correlations. Intermediate fusion integrates features extracted independently from each modality, merging them for joint analysis. Late fusion combines decisions or predictions derived separately from each modality, often through ensemble learning techniques. Studies have demonstrated that ensemble and stacking strategies in late fusion can significantly improve classification performance for distinguishing benign and malignant breast tumors, achieving accuracies up to 96.8% and area under the curve values nearing 0.997 when combining ultrasound, mammography, and MRI features.112 This indicates that sophisticated fusion strategies can effectively harness the complementary diagnostic information of multimodal imaging.
Deep learning has substantially advanced multimodal feature integration by enabling automated, hierarchical feature extraction and complex pattern recognition from heterogeneous data sources. Convolutional neural networks and transformer-based architectures have been employed to extract deep features from each imaging modality, which are then fused using attention mechanisms or graph-based models to capture interdependencies across modalities. For example, in breast cancer subtype prediction, a multimodal neural network combining radiomic and deep learning features from dynamic contrast-enhanced MRI achieved a mean accuracy of 83% and further improved to 97% with uncertainty estimation modules, outperforming traditional radiomics or standalone deep learning models.113 Similarly, hybrid frameworks integrating radiomic texture analysis with deep learning segmentation have enhanced myocardial infarction detection, demonstrating the utility of multimodal fusion beyond oncology.114
The role of deep learning in multimodal fusion extends beyond feature extraction to include sophisticated fusion strategies such as cross-modal transformers, attention-weighted networks, and graph convolutional layers that model spatial and semantic relationships between modalities. A deep learning-based multimodal feature interaction-guided fusion framework integrated CT radiomic macrofeatures with whole-slide histopathological microfeatures to predict EGFR mutation status in lung adenocarcinoma, achieving AUC values above 0.85 on internal validation and 0.817 on external validation sets.115 This highlights the potential of deep learning to bridge imaging phenotypes with molecular heterogeneity, a critical aspect in precision oncology.
Moreover, multimodal fusion models that combine imaging data with clinical, genomic, or pathological information have demonstrated superior prognostic and diagnostic performance compared to unimodal models. For example, integrating deep learning-derived tumor radiomics with mediastinal adiposity metrics improved postoperative survival prediction in non-small cell lung cancer patients, achieving concordance indices exceeding 0.82.116 In breast cancer, multimodal models fusing histopathological whole-slide images with clinical features via multiple instance learning significantly enhanced prognostic risk stratification, outperforming models based on clinical data alone.117 These findings suggest that deep learning-based multimodal fusion not only consolidates imaging data but also synergistically integrates heterogeneous data types to capture tumor heterogeneity and improve individualized patient management.
In thyroid nodule diagnosis, the fusion of radiomics and deep learning features extracted from B-mode and power Doppler ultrasound images has led to classification models with accuracy rates up to 84%, demonstrating the value of combining morphological and vascular information.118 Additionally, hybrid quantum-classical frameworks have been explored for integrating mammography and genomic data, achieving an AUC of 0.96 and highlighting emerging computational paradigms in multimodal fusion.119 These advances underscore the growing importance of deep learning in managing the complexity and high dimensionality of multimodal datasets, facilitating more accurate and interpretable diagnostic tools.
The integration of multimodal imaging data through deep learning also addresses challenges related to tumor heterogeneity and microenvironmental complexity. For example, multimodal diagnostic models incorporating MRI, proteomic, genomic, and clinical data have identified distinct breast cancer subtypes with differential responses to neoadjuvant therapy, informing personalized treatment strategies.120 Furthermore, explainable AI techniques such as Grad-CAM and SHAP have been employed in multimodal fusion frameworks to enhance the interpretability of model decisions, thereby increasing clinician trust and facilitating clinical translation.121
In summary, multimodal imaging data fusion, empowered by deep learning methodologies, represents a transformative approach in breast cancer imaging phenotyping. By integrating MRI, PET, ultrasound, and complementary clinical and molecular data, these models capture the complex biological heterogeneity of tumors and improve diagnostic accuracy, prognostic assessment, and therapeutic decision-making. Continued advancements in fusion strategies, model interpretability, and large-scale validation are essential to fully realize the clinical potential of multimodal deep learning frameworks in breast cancer management.
End-to-End Genomic Prediction Models
End-to-end genomic prediction models represent a cutting-edge approach in radiogenomics, where deep learning frameworks are designed to directly predict gene mutations and expression profiles from imaging data without the need for intermediate handcrafted feature extraction. This paradigm leverages the ability of convolutional neural networks and other deep architectures to automatically learn hierarchical representations from raw medical images, such as whole slide histopathology images (WSIs) or dynamic contrast-enhanced magnetic resonance imaging, that correlate with underlying genomic alterations. The direct prediction of genomic traits from imaging phenotypes offers a noninvasive, cost-effective alternative to traditional molecular assays, potentially enabling more rapid and widespread genomic characterization in breast cancer management.
Numerous studies have demonstrated the feasibility and effectiveness of such models. For instance, a deep learning model trained on WSIs from breast carcinoma patients successfully predicted point mutations in six key genes with area under the curve values ranging from 0.68 to 0.85, as well as copy number alterations in another six genes with AUCs between 0.69 and 0.79. Moreover, this model extended its predictive capability to biological pathway activities, identifying three out of ten canonical pathways with AUCs from 0.65 to 0.79. The visualization of attention weight maps in this study provided insights into the spatial regions of tumor tissue influencing the model’s predictions, highlighting the interpretability of the approach.122 Such findings underscore the potential of end-to-end deep learning models to capture complex genotype-phenotype relationships embedded in histopathological images.
Similarly, deep learning applied to DCE-MRI has been utilized to predict lymph node metastasis and to associate imaging phenotypes with gene expression profiles. A study combining radiomics and deep learning features from DCE-MRI constructed nomograms that achieved high predictive performance for LNM (training cohort AUC = 0.98; validation cohort AUC = 0.87). Importantly, the deep learning phenotypes were linked to multiple classical tumor signaling pathways, including immune response and cell death, and a gene expression score derived from these phenotypes was strongly associated with high LNM risk (odds ratio = 164.00, P < 0.001).49 This integrative approach not only enhances prediction accuracy but also provides biological interpretability, bridging imaging features with molecular mechanisms.
The integration of multimodal data — combining imaging, clinical, and genomic information — further improves the predictive power of end-to-end models. For example, a multi-modal deep learning framework that incorporated H&E-stained WSIs, clinical data, and gene expression profiles achieved an AUC of 0.75 in predicting breast cancer recurrence and metastasis risk, outperforming models based on single data types. This approach utilized attention mechanisms to weight different image regions, integrating them with genomic and clinical features for comprehensive risk stratification.123 The synergistic use of diverse data modalities allows the model to capture complementary aspects of tumor biology, thereby enhancing prognostic precision.
In addition to mutation and expression prediction, end-to-end models have been applied to infer homologous recombination deficiency (HRD) status directly from routine histology images. Using attention-weighted multiple instance learning (attMIL), models achieved AUROCs up to 0.78 in breast cancer cohorts and demonstrated generalizability across multiple tumor types, indicating a shared HRD-like phenotype observable in histopathology. This capability suggests that deep learning models can uncover pan-cancer genomic features from imaging data, potentially guiding therapeutic decisions such as PARP inhibitor eligibility.124,125 The cross-cancer applicability highlights the robustness and translational potential of these models.
Despite the promising results, challenges remain in model generalization and interpretability. Studies have noted that deep learning models trained on specific datasets or imaging modalities may exhibit reduced performance when applied to external cohorts due to data heterogeneity and variations in imaging protocols. However, approaches such as transfer learning, multi-cohort training, and incorporation of explainable AI techniques are being developed to address these issues. Visualization of activation maps has been used to explore the biological significance of deep learning radiomic phenotypes in breast cancer lymph node metastasis prediction.49,122 Future work focusing on model robustness and interpretability is essential for clinical translation.
In summary, end-to-end genomic prediction models leverage deep learning to directly infer gene mutations, expression profiles, and pathway activities from breast cancer imaging data. By integrating multimodal information and employing advanced architectures, these models achieve high predictive accuracy and provide biologically meaningful insights. Their development marks a significant advance toward noninvasive, image-based genomic profiling, offering potential for personalized diagnosis, prognosis, and treatment planning in breast cancer care. Continued research is warranted to validate these models across diverse populations and imaging platforms to ensure broad clinical utility (Figure 3).
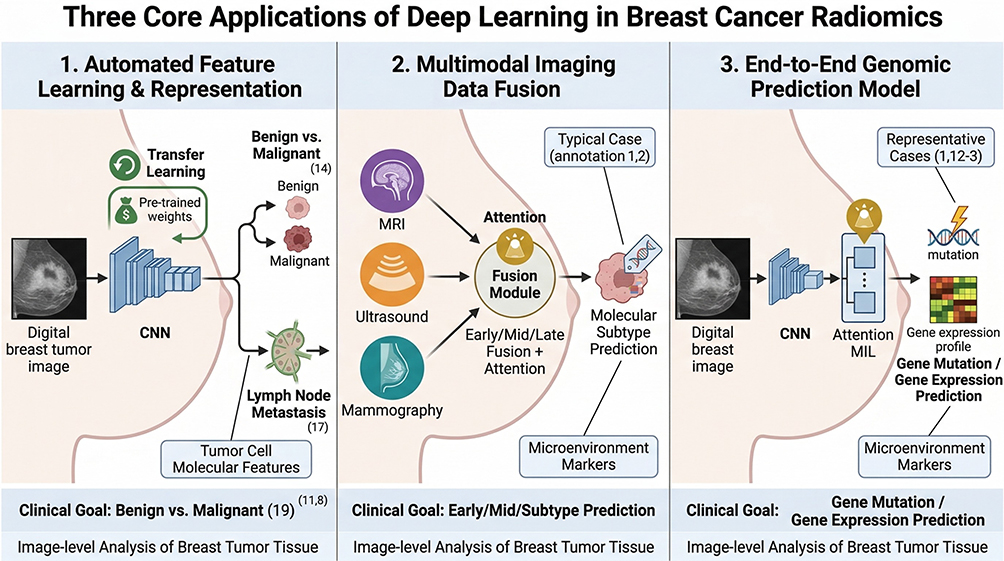 |
Figure 3 Schematic diagram of three core applications of deep learning in breast cancer radiomics. This three-panel schematic summarizes the three core applications of deep learning in breast cancer radiomics: (1) Automated feature learning and representation (technology: CNN/transfer learning; clinical goal: benign/malignant differentiation, lymph node metastasis prediction); (2) Multimodal imaging data fusion (technology: early/mid/late fusion, attention mechanism; clinical goal: molecular subtype prediction); (3) End-to-end genomic prediction model (technology: CNN/Attention MIL; clinical goal: gene mutation/gene expression profile prediction). Each panel includes technical principles, clinical goals, and typical cases with reference annotations. |
Correlation Analysis Between Imaging Features and Genomic Heterogeneity
Association Between Imaging Features and Gene Mutations
The relationship between imaging phenotypes and gene mutations in breast cancer has garnered increasing attention, particularly focusing on key genes such as BRCA1/2 and TP53, which are pivotal in hereditary breast cancer syndromes and tumor progression. Radiogenomic studies have demonstrated that imaging features extracted from modalities like ultrasound, MRI, and mammography can reflect underlying genetic alterations, thereby providing non-invasive biomarkers for mutation status prediction and personalized treatment planning. For instance, ultrasound-based radiomics models have been developed to predict germline BRCA mutations with promising accuracy. In a retrospective study involving 497 breast cancer patients who underwent germline BRCA genetic testing, radiomic features extracted from intratumoral and peritumoral ultrasound regions were combined with clinicopathological factors to construct a nomogram. This model achieved an area under the receiver operating characteristic curve of 0.824 in the validation cohort, outperforming the clinicopathological model alone.126 Similarly, another study using ultrasound images and radiomics features selected via multivariate logistic regression identified 10 significant features predictive of BRCA1/2 mutation, with the combined nomogram model reaching an AUC of 0.811 in validation, highlighting the complementary value of imaging and clinical data.127
Beyond BRCA mutations, TP53 and other high- and moderate-risk genes such as CHEK2, PALB2, and PTEN have been implicated in breast cancer pathogenesis, with distinct imaging phenotypes reported. Radiologists play a crucial role in recognizing these phenotypes and integrating genetic risk into screening protocols. Imaging features such as internal enhancement patterns on MRI and spiculated margins have been associated with pathogenic mutations and may predict recurrence or metastasis risk.128,129 Moreover, radiogenomic frameworks that analyze multi-angle ultrasound images in conjunction with gene mutation data have been proposed to capture complex many-to-many associations between imaging and genetic features across breast cancer subtypes, facilitating biological interpretation and targeted therapy development.130
Statistical and machine learning methods have been instrumental in elucidating these associations. Techniques such as least absolute shrinkage and selection operator regression, maximum relevance minimum redundancy (mRMR) feature selection, and deep convolutional neural networks (DCNNs) have been employed to identify imaging features most relevant to genetic mutations. For example, a DCNN model based on ultrasound images effectively predicted PIK3CA mutation status with an AUC of 0.775, outperforming classical machine learning models.131 Additionally, deep learning applied to whole-slide histopathology images has enabled prediction of BRCA gene mutations, with AUCs reaching up to 0.828, further underscoring the potential of integrating imaging and molecular data through advanced computational approaches.132
Furthermore, multiview nonnegative matrix factorization (MVNMF) has been introduced as a novel method for radio-multigenomic analysis, linking dynamic contrast-enhanced MRI radiomic features with multi-omics data including DNA copy number alterations, mutations, and mRNA expression. This approach not only improved survival prediction in breast cancer patients but also enhanced understanding of the biological mechanisms underlying imaging phenotypes.133 Such integrative models highlight the evolving landscape where statistical and machine learning frameworks bridge imaging biomarkers and genomic heterogeneity.
In addition to mutation prediction, radiomics and radiogenomics provide insights into the tumor microenvironment and immune landscape. For example, the abundance of gamma-delta (γδ) T cells, which have antitumor roles in triple-negative breast cancer, has been correlated with MRI radiomic features, suggesting that imaging can non-invasively estimate immune cell infiltration and potentially guide immunotherapy.52 This demonstrates the multifaceted utility of imaging-genomic associations extending beyond mutation status to encompass broader tumor biology.
Collectively, these findings emphasize that imaging features can serve as surrogate markers for key gene mutations such as BRCA1/2 and TP53 in breast cancer. The integration of statistical methods and machine learning algorithms enhances the detection and interpretation of these associations, facilitating risk stratification, prognostication, and personalized therapy. Imaging-genomic correlation studies have demonstrated predictive capabilities for genetic mutations and prognosis in breast cancer, with ongoing methodological advancements.126,127,133
Imaging Features and Tumor Immune Microenvironment
The tumor immune microenvironment (TIME) plays a critical role in cancer progression and response to immunotherapies. Radiomics, by extracting quantitative imaging features, offers a non-invasive window into the complex interactions within the TIME, particularly immune cell infiltration and immune-related molecular pathways. Several studies have demonstrated significant correlations between radiomic features and immune cell infiltration levels, including tumor-infiltrating lymphocytes (TILs) and CD8+ T cells, which are pivotal for antitumor immunity.
In breast cancer, radiomic models derived from dynamic contrast-enhanced magnetic resonance imaging have been successfully developed to predict immune cell infiltration. For example, a study on triple-negative breast cancer utilized radiomic features to non-invasively estimate TIL levels, achieving an area under the curve of 0.79 in validation cohorts. This radiomic signature correlated with transcriptomic data indicating activated immune-related pathways and increased infiltration of CD8+ T cells, follicular helper T cells, and memory B cells in tumors with high radiomic-predicted TILs, reflecting a “hot” immune microenvironment.134 Similarly, machine learning-based radiomics models have predicted STAT3 expression, a key regulator of immune suppression, in breast cancer, with high radiomic scores linked to elevated immune-related gene signatures and longer overall survival, further underscoring the capacity of imaging features to characterize immune microenvironment phenotypes.135
The relationship between imaging texture features and immune infiltration extends beyond breast cancer. In non-small cell lung cancer (NSCLC), radiomic signatures from computed tomography (CT) and PET/CT scans have been associated with CD8+ T cell expression and immune-inflamed tumor phenotypes. A combined PET/CT radiomics-clinical model achieved an AUC of 0.93 for predicting CD8 expression, with higher radiomic scores corresponding to enhanced immune scores and activated immune pathways.136 Furthermore, unsupervised clustering of CT radiomic features in NSCLC identified subtypes with distinct immune microenvironment characteristics, where one subtype exhibited higher T cell, B cell, and natural killer (NK) cell infiltration and was associated with better immunotherapy response and survival.137 These findings suggest that radiomic features can capture the heterogeneity of immune cell infiltration and may serve as predictive biomarkers for immunotherapy efficacy.
The spatial heterogeneity of immune cells within tumors also influences prognosis and treatment response. Advanced radiomic analyses integrating multiparametric MRI and deep learning have enabled the prediction of immunophenotypes, such as immune-inflamed versus immune-desert phenotypes, in breast cancer. A machine learning-based radiomics signature distinguished these phenotypes with an AUC of approximately 0.85 and predicted response to anti-PD-1/PD-L1 immunotherapy.138 Radiomic features extracted from both intratumoral and peritumoral regions have shown diagnostic efficacy in evaluating immune cell infiltration levels, with peritumoral features often demonstrating higher accuracy, reflecting the importance of the tumor microenvironment beyond the tumor core.139
Radiomics also holds promise in predicting the tumor immune microenvironment in other cancers. In hepatocellular carcinoma (HCC), radiomic subtypes derived from contrast-enhanced CT scans correlated with immune-related pathways and immune cell infiltration patterns, with associations to prognosis.140,141 In murine tumor models, radiomics combined with immunological analyses has been utilized to non-invasively assess immune cell infiltration dynamics.142,143
The integration of radiomics with transcriptomic and single-cell sequencing data facilitates the biological interpretation of imaging features, linking them to immune cell populations and immune checkpoint expression. Radiomic features associated with macrophage infiltration and T cell exhaustion have been identified in glioma and breast cancer tumor microenvironments, providing insight into immune suppression mechanisms.144,145 Radiomics combined with deep learning and machine learning algorithms enhances feature extraction and model robustness, with applications in tumor classification and microenvironment characterization.146,147
Overall, radiomics offers a powerful, non-invasive approach to assess the tumor immune microenvironment by capturing imaging features reflective of immune cell infiltration, immune activation status, and immune suppression. These imaging biomarkers have the potential to guide immunotherapy decisions, predict treatment response, and enable personalized cancer management.
Summary
Radiomic imaging features quantitatively reflect the heterogeneity and composition of the tumor immune microenvironment across multiple cancer types. By correlating with immune cell infiltration, immune-related gene expression, and immunotherapy response, radiomics provides a non-invasive biomarker platform that bridges tumor phenotypes and immune status. Integrating radiomics with multi-omics data and advanced machine learning enhances the interpretability and predictive accuracy of these models, paving the way for precision oncology approaches that tailor immunotherapy and other treatments based on individual tumor immune profiles.
Integration Analysis of Imaging Features and Gene Expression Profiles
The integration of imaging phenotypes with genomic data has emerged as a pivotal approach to unravel the complex biological underpinnings of breast cancer heterogeneity and to enhance predictive accuracy for clinical outcomes. One fundamental aspect of this integration is elucidating the correspondence between gene expression subtypes and imaging phenotypes derived from modalities such as dynamic contrast-enhanced magnetic resonance imaging and computed tomography. Studies leveraging deep learning radiomics have demonstrated that imaging features extracted from DCE-MRI can predict lymph node metastasis with high accuracy, and these imaging phenotypes correlate with specific gene expression signatures and biological pathways associated with immune response, signal transduction, and cell death.49 This correspondence underscores that imaging phenotypes are not mere visual surrogates but reflect intrinsic molecular characteristics of tumors.
Moreover, the PAM50 intrinsic molecular subtypes of breast cancer, defined by gene expression profiles, have been found to associate significantly with certain MRI-based radiomic features such as maximum 2D diameter, degree of correlation, and inverse difference moment normalized. Although the correlations are modest, these imaging features provide noninvasive biomarkers that reflect underlying molecular heterogeneity.148 Such associations facilitate the stratification of patients into biologically relevant subgroups using imaging data, potentially reducing the need for invasive biopsies.
Beyond single-modality correlations, multi-omics data fusion strategies have been developed to integrate radiomics with transcriptomics and other genomic data, enhancing the predictive power for prognosis and therapeutic response. Multimodal deep learning frameworks combining gene expression and clinical variables have outperformed models based on any single data type in predicting survival outcomes in breast cancer patients.149,150 These frameworks employ advanced architectures such as multimodal transformers and deep bilinear networks to capture complex intra- and inter-modality relationships, enabling more nuanced modeling of tumor biology.
In breast cancer, radiogenomics nomograms integrating radiomics signatures with immune-related gene expression profiles have shown promising performance in predicting axillary lymph node metastasis, with underlying gene modules enriched in pathways related to metastasis, such as focal adhesion and extracellular matrix (ECM) receptor interaction.151 This integrative approach not only improves prediction accuracy but also elucidates biological mechanisms driving radiomic phenotypes, supporting the hypothesis that imaging features are manifestations of specific molecular alterations.
Additionally, spatial-temporal radiogenomics approaches have been proposed to capture dynamic changes in imaging features and their biological significance during neoadjuvant chemotherapy, providing insights into tumor heterogeneity and treatment response.152 By correlating imaging alterations with gene expression profiles before and after therapy, these methods enable the identification of temporal biomarkers that reflect evolving tumor states.
The integration of imaging and gene expression data also extends to the characterization of the tumor microenvironment. AI-driven interpretable imaging phenotypes derived from DCE-MRI have been linked to molecular signatures including hormone receptor status and immune checkpoint protein expression, demonstrating superior prognostic value compared to traditional radiomics or black-box deep learning models.40 These findings suggest that imaging features can serve as proxies for complex molecular interactions within the TME, facilitating noninvasive assessment of tumor biology.
From a methodological perspective, multi-omics data fusion strategies involve various levels of integration, including early fusion (combining raw data), intermediate fusion (combining extracted features), and late fusion (combining model outputs). Late fusion models have been shown to achieve superior generalizability and interpretability in survival prediction tasks by effectively leveraging complementary information from histopathology images, omics data, and clinical data.149 Furthermore, emerging quantum-classical hybrid frameworks have been explored to enhance feature selection and integration efficiency in radiogenomic analyses, achieving high diagnostic accuracy in breast cancer.119
Inferences drawn from these integrative studies indicate that radiomic features can serve as noninvasive biomarkers reflecting gene expression profiles and molecular subtypes, thereby bridging the gap between imaging phenotypes and tumor genomics. This integration facilitates personalized treatment planning, risk stratification, and monitoring of therapeutic response. However, the strength of these associations may vary depending on imaging modalities, tumor subtypes, and analytical methods, highlighting the need for standardized protocols and larger multi-center validation cohorts to establish robust radiogenomic biomarkers.
In summary, the integration of imaging features with gene expression profiles through advanced multi-omics fusion strategies holds significant promise for advancing precision oncology in breast cancer (Figure 4). By capturing the complex interplay between tumor morphology and molecular heterogeneity, these integrative approaches provide comprehensive insights that can improve diagnosis, prognostication, and individualized therapy selection.49,148,149,151,152
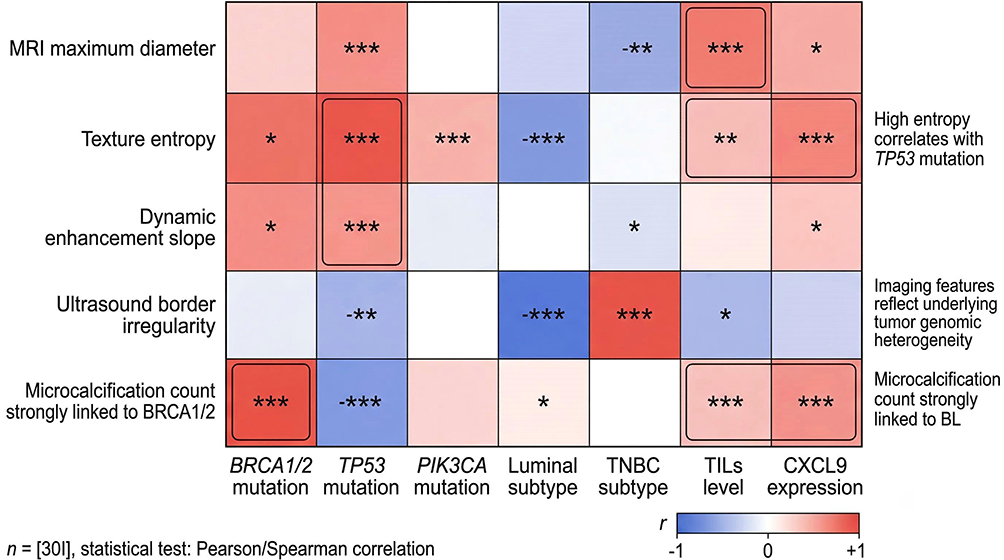 |
Figure 4 Heatmap of correlation analysis between imaging features and genomic heterogeneity in breast cancer. This heatmap visualizes the correlation strength between typical breast cancer imaging features (y-axis: MRI maximum diameter, texture feature entropy, dynamic enhancement curve slope, ultrasound border irregularity, mammography microcalcification count) and genomic heterogeneity indicators (x-axis: BRCA1/2 mutation, TP53 mutation, PIK3CA mutation, Luminal subtype, TNBC subtype, TILs level, CXCL9 gene expression). The color gradient represents Pearson/Spearman correlation coefficients (red: positive correlation, blue: negative correlation, white: no correlation), with P-values annotated (*P<0.05, **P<0.01, ***P<0.001). Strong correlation regions (|r|>0.6) are labeled with key conclusions from the review, and the sample size and statistical methods are specified in the figure annotation. |
Clinical Applications and Challenges
Application of Radiogenomics in Breast Cancer Diagnosis
Radiogenomics integrates imaging phenotypes with genomic profiles, offering a non-invasive approach to characterize breast cancer molecular subtypes and heterogeneity. This approach leverages advanced imaging modalities such as dynamic contrast-enhanced magnetic resonance imaging, ultrasound, and mammography to extract quantitative radiomic features that reflect underlying tumor biology. These imaging features are then correlated with genomic data, including gene expression, mutations, and multi-omics profiles, to develop predictive models for breast cancer diagnosis and classification.
One of the key applications of radiogenomics in breast cancer diagnosis is the non-invasive prediction of molecular subtypes. Breast cancer comprises distinct molecular subtypes—such as luminal A, luminal B, HER2-positive, and triple-negative breast cancer —each with unique prognostic and therapeutic implications. Radiogenomic studies have demonstrated that specific radiomic features extracted from MRI or ultrasound can differentiate these subtypes with moderate to high accuracy. Machine learning models trained on radiomic features have been used to distinguish triple-negative breast cancer subtypes from others, indicating that imaging phenotypes capture subtype-specific biological variations.153,154 Furthermore, deep learning approaches applied to multiparametric MRI have successfully decoded gene-phenotype associations, enabling prediction of receptor status such as estrogen receptor (ER), progesterone receptor (PR), and HER2 with AUCs around 0.65 to 0.70, thus supporting the feasibility of imaging-based genomic inference.155
Radiogenomics also enhances early diagnosis and risk assessment by linking imaging features with genetic alterations and tumor microenvironment characteristics. Studies integrating radiomic signatures with transcriptomic and proteomic data have identified imaging biomarkers associated with tumor heterogeneity, immune suppression, and metabolic pathways. For example, peritumoral heterogeneity quantified by radiomics correlates with immune evasion mechanisms and fatty acid synthesis in TNBC, serving as a prognostic factor for recurrence-free and overall survival.154 Additionally, radiogenomic models combining MRI features and gene expression data have improved prediction of axillary lymph node metastasis (ALNM), a critical factor in staging and treatment planning, with AUCs exceeding 0.80 in validation cohorts.108,151 These models reveal that radiomic phenotypes are driven by biological pathways involved in metastasis, such as focal adhesion and extracellular matrix interactions, underscoring the biological relevance of imaging features.
The integration of multi-omics data with radiomics further refines diagnostic accuracy and biological interpretability. Approaches employing multiview nonnegative matrix factorization have linked dynamic contrast-enhanced MRI features with DNA copy number alterations, mutations, and mRNA expression, enhancing survival prediction beyond imaging or genomics alone.133 Deep learning-based radiomic features extracted via autoencoders demonstrate stronger associations with genomic risk genes and biological pathways than traditional handcrafted features, yielding superior performance in predicting clinical characteristics like tumor size, lymph node status, and receptor expression.51 This highlights the potential of advanced computational methods to capture complex tumor biology from imaging data.
Moreover, radiogenomics offers promise in early risk stratification and personalized screening. Artificial intelligence (AI) models integrating imaging and genomic data can stratify patients by risk, facilitating tailored screening protocols and early intervention strategies.156 The non-invasive nature of radiogenomics circumvents limitations of biopsy-based molecular testing, reducing patient burden and enabling longitudinal monitoring of tumor evolution and treatment response.157 This is particularly valuable given the heterogeneity of breast cancer and the challenges in obtaining representative tissue samples.
Despite these advances, challenges remain in standardization, data harmonization, and clinical translation. Variability in imaging protocols, feature extraction methods, and genomic data integration can affect model reproducibility and generalizability. Large-scale, multi-institutional studies with diverse populations are needed to validate radiogenomic biomarkers and define their clinical utility. Enhancing the interpretability of radiogenomic models is an important consideration in their development.48,150
In summary, radiogenomics is transforming breast cancer diagnosis by providing non-invasive molecular subtype prediction and early risk assessment through integration of imaging and genomic data. The synergy between advanced imaging analytics, multi-omics integration, and AI-driven modeling holds promise for precision diagnostics that can guide individualized patient management. Continued methodological improvements and validation efforts will be pivotal in realizing the full clinical potential of radiogenomics in breast cancer care (Figure 5).
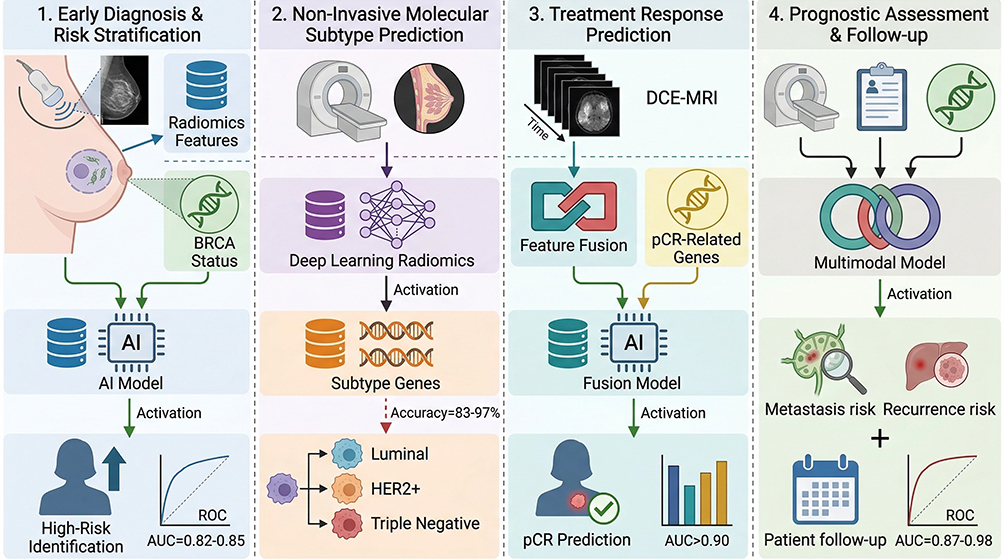 |
Figure 5 Schematic diagram of clinical application scenarios of radiogenomics in breast cancer. This schematic outlines four core clinical application scenarios of breast cancer radiogenomics along the clinical diagnosis and treatment pathway: (1) Early diagnosis and risk stratification (technology: ultrasound/mammography radiomics model; AUC=0.82–0.85 for BRCA mutation prediction); (2) Non-invasive prediction of molecular subtypes (technology: MRI deep learning radiomics; accuracy=83–97% for subtype classification); (3) Treatment response prediction (technology: DCE-MRI multi-phase feature fusion; AUC>0.90 for pCR prediction of neoadjuvant chemotherapy); (4) Prognostic assessment and follow-up (technology: multimodal model integrating imaging/clinical/genomic data; AUC=0.87–0.98 for lymph node metastasis/ distant recurrence prediction). Each scenario includes technical details, clinical goals, and application efficacy with reference annotations. |
Radiogenomics Guiding Personalized Therapy
Radiogenomics has emerged as a pivotal tool in the realm of personalized oncology, particularly in guiding targeted therapy and immunotherapy by linking imaging phenotypes with underlying molecular and genetic tumor characteristics. This integrative approach enables non-invasive, spatially resolved insights into tumor heterogeneity, which is crucial for selecting and optimizing individualized treatment regimens. For instance, in glioblastoma, radiogenomic markers have been identified that correlate with key molecular alterations such as MGMT methylation status, IDH mutations, and EGFR amplification, which are known to influence prognosis and therapeutic response.158 These imaging-genomic correlations facilitate stratification of patients into risk groups and can predict recurrence, thereby informing clinical decisions on aggressive versus conservative treatment strategies.
In breast cancer, radiogenomic testing platforms like Oncotype DX and MammaPrint have revolutionized risk stratification and treatment planning by integrating genomic signatures with imaging features. However, the psychological impact of such testing, including anxiety and decision conflict, underscores the necessity for comprehensive patient education and counseling to support personalized medicine effectively.159 Advanced imaging combining dynamic contrast-enhanced MRI radiomics with deep learning features enables early prediction of pathological complete response to neoadjuvant therapy.160 These predictive capabilities allow for timely treatment adjustments, minimizing exposure to ineffective therapies and associated toxicities.
Targeted therapies and immunotherapies benefit significantly from radiogenomic insights that reveal tumor microenvironment characteristics, such as immune infiltration and metabolic activity. For example, in clear cell renal cell carcinoma, radiomic models have been linked with immunometabolic subtypes that predict immunotherapy responsiveness, highlighting the crosstalk between metabolism and immune activity.161 Similarly, in non-small cell lung cancer, integration of PET/CT radiomics with glucose metabolism-related gene signatures has led to prognostic models that not only stratify patients by survival risk but also inform on immune checkpoint expression and potential drug sensitivities, thereby guiding personalized treatment selection.162
Radiogenomics also plays a critical role in head and neck cancer, where radiogenomic markers derived from hybrid imaging and whole-exome sequencing enable risk stratification by inferring mutational pathway states, including cellular senescence pathways. These integrated markers outperform prognostic models based solely on genetic or imaging data, facilitating the identification of high-risk patients who may benefit from intensified or targeted therapeutic interventions.163 Furthermore, the combination of advanced imaging modalities with radiogenomics has been proposed to identify radioresistant tumor regions, allowing for dose escalation and precision radiotherapy tailored to individual tumor biology.164
In the context of immunotherapy, radiogenomics contributes to the identification of biomarkers predictive of response by characterizing tumor heterogeneity and the immune microenvironment dynamically and non-invasively. AI-driven analyses of radiomic features extracted from imaging modalities such as CT, MRI, and PET/CT can uncover imaging biomarkers associated with tumor heterogeneity and treatment response, enabling real-time monitoring and personalized therapeutic strategies.165 This integration is particularly valuable given the complex interplay between tumor genomics, immune modulation, and treatment efficacy.
The predictive power of radiogenomics extends to monitoring treatment response and prognosis. For example, in breast cancer patients undergoing neoadjuvant therapy, combining radiomic and deep learning features from multiple imaging phases has yielded models with high predictive accuracy for therapeutic outcomes, supporting personalized treatment planning.160 Similarly, in gliomas, radiogenomic signatures derived from multiparametric MRI and genomic data enable the prediction of oncogenic signaling pathway deregulations, which can inform targeted therapy decisions and improve patient outcomes.166
While radiogenomics holds great promise for guiding personalized therapy, challenges such as the need for methodological standardization, prospective validation, and integration into clinical workflows remain. The heterogeneity of data sources, imaging protocols, and patient populations necessitates rigorous multi-institutional studies to confirm the robustness and generalizability of radiogenomic biomarkers. Advancements in AI, machine learning, and multi-omics integration hold potential to facilitate the translation of radiogenomics into clinical practice, though challenges remain.167
In summary, radiogenomics serves as a critical bridge between imaging phenotypes and genomic heterogeneity, offering valuable biomarkers for targeted therapy and immunotherapy selection, predicting treatment response, and assessing prognosis. By enabling a non-invasive, comprehensive characterization of tumor biology, radiogenomics enhances the precision of personalized oncology and supports dynamic treatment adaptation tailored to individual patient profiles.
Current Technical and Clinical Challenges
The integration of radiomics and deep learning into breast cancer imaging and management holds great promise, yet several technical and clinical challenges must be addressed to realize their full potential (Table 2). One of the foremost technical issues is the heterogeneity of data and the need for standardization. Medical imaging data used for radiomic and deep learning analyses often come from diverse sources, including different imaging modalities (eg., MRI, mammography, ultrasound), various acquisition protocols, and multiple centers. This variability can introduce inconsistencies in image quality, resolution, and contrast, which subsequently affect the extracted features and model performance. For instance, studies have shown that radiomic features can be sensitive to imaging physics parameters such as contrast, noise, and image sharpness, leading to variability in feature robustness.68 Similarly, multiparametric MRI radiomics performance can significantly decrease when imaging sequences are missing or vary across centers.168 These factors complicate the reproducibility and generalizability of radiomic models. Efforts toward harmonization of imaging protocols and development of robust feature extraction methods that minimize the influence of acquisition variability are critical. Moreover, large-scale multi-center datasets with standardized imaging and annotation protocols are essential to train and validate models that are clinically applicable.
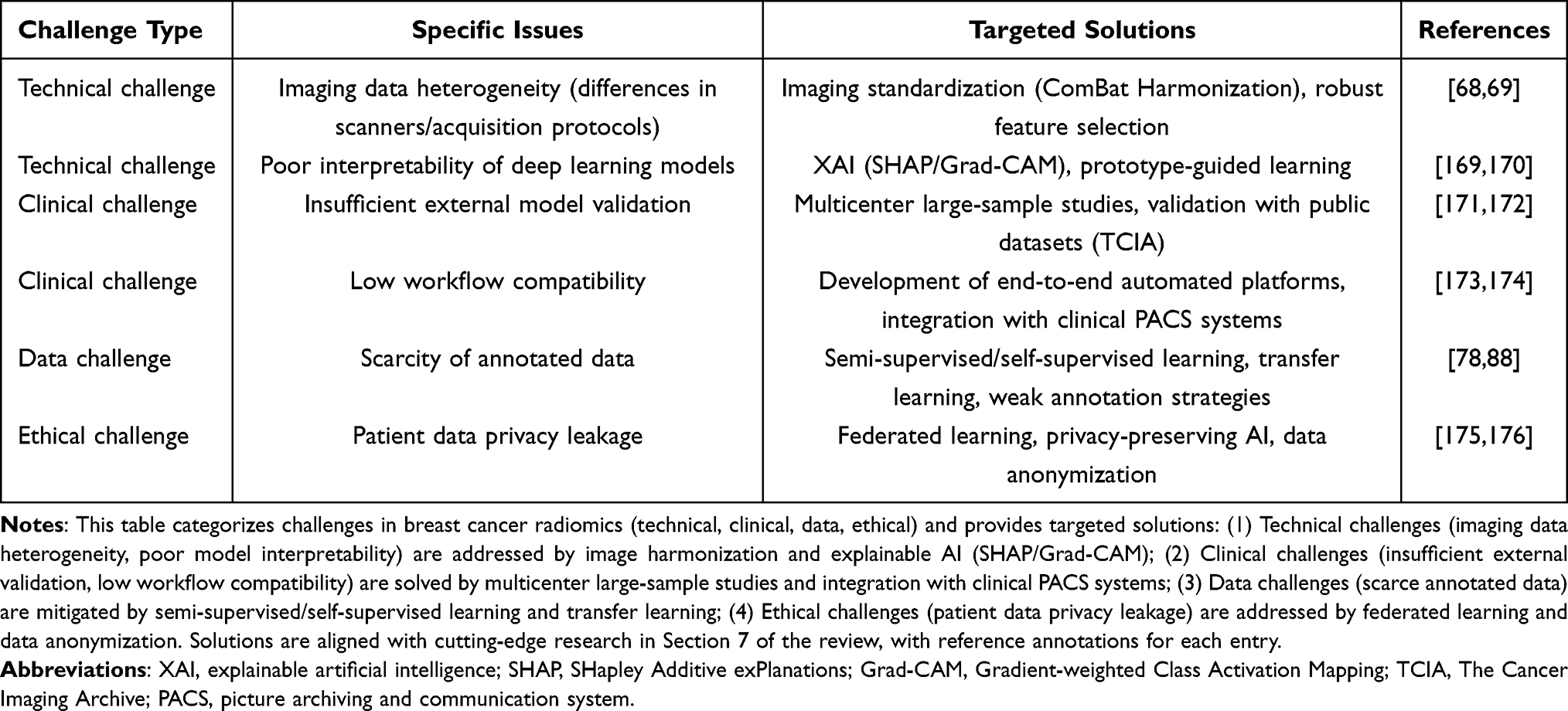 |
Table 2 Comparison of Technical and Clinical Challenges and Corresponding Solutions in Breast Cancer Radiomics and Deep Learning |
Another significant challenge lies in the interpretability of deep learning models and their clinical trustworthiness. Deep learning approaches have demonstrated performance in predicting breast cancer clinical features, though their “black-box” nature limits clinicians’ confidence in adopting these tools.51,150 Explainable AI techniques, including Grad-CAM visualizations and prototype-guided learning, have been proposed to provide insights into model decision-making processes.169,170 For example, interpretable imaging phenotypes derived from deep learning have been linked to molecular signatures and survival outcomes, enhancing transparency.40 Despite these advances, achieving a balance between model complexity and interpretability remains a challenge. Clinicians require models that not only perform well but also offer understandable rationales for their predictions to integrate them safely into clinical workflows.
Clinically, a pressing need exists for large-scale, multi-center validation of radiomics and deep learning models before widespread adoption. Many existing studies are retrospective, single-center, or based on relatively small cohorts, limiting the assessment of model robustness across diverse patient populations and imaging settings.171,172 The scarcity of publicly available, well-annotated datasets with comprehensive clinical and genomic information hampers external validation efforts. For instance, although large datasets like The Cancer Imaging Archive (TCIA) provide valuable resources, expert annotations and harmonized clinical data are often limited.172 Multi-center studies that encompass different ethnicities, imaging devices, and clinical practices are essential to evaluate model generalizability and identify potential biases. Furthermore, regulatory approval processes demand rigorous validation to ensure safety and efficacy. Without such validation, the translation of radiomics and deep learning tools from research to routine clinical practice will remain constrained.
In addition to these challenges, addressing data privacy and ethical concerns is paramount when dealing with multi-center data sharing and AI model development. Federated learning and privacy-preserving AI frameworks are emerging as potential solutions to enable collaborative model training without compromising patient confidentiality. However, these methods require further technical refinement and clinical validation.
Collectively, overcoming data heterogeneity through standardization, enhancing model interpretability to build clinical trust, and conducting extensive multi-center validations are critical steps toward integrating radiomics and deep learning into breast cancer care. Research trends in AI and radiomics in breast cancer highlight growing interest and potential for future clinical applications.150,171,177
Latest Research Progress and Technological Innovations
Emerging Deep Learning Architectures and Their Advantages
The rapid advancement of deep learning architectures has significantly impacted radiomics, especially in the context of complex image analysis tasks such as cancer imaging phenotyping. Among these architectures, Transformer models and graph neural networks have emerged as powerful tools that offer distinct advantages over traditional convolutional neural networks in capturing long-range dependencies and relational information, respectively. Transformers, originally developed for natural language processing, utilize self-attention mechanisms that enable the model to weigh the importance of different parts of the input data effectively. This characteristic is particularly beneficial in radiomics, where spatial heterogeneity and subtle imaging features must be integrated to characterize tumor phenotypes and their underlying genomic heterogeneity. For instance, Transformer-based fusion models have been successfully applied to integrate multi-dimensional imaging features, such as 2D and 3D deep learning features along with radiomics and clinical data, leading to improved performance in lesion bioactivity identification.178 The ability of Transformers to model complex interactions among diverse feature sets enhances their discriminative power in clinical tasks.
Graph neural networks extend deep learning capabilities by explicitly modeling the relationships among entities through graph structures. In radiomics, GNNs can represent spatial and functional interactions within tumor microenvironments or brain networks, capturing the intricate connectivity patterns that are often lost in grid-based CNNs. For example, multi-task graph neural networks have been employed to localize eloquent cortex regions in brain tumor patients using resting-state fMRI connectivity, demonstrating superior generalization and robustness compared to conventional machine learning and fully connected deep learning models.179 The graph-based approach allows for the incorporation of domain knowledge about anatomical and functional connectivity, which is critical for precise phenotypic characterization.
Another notable advancement is self-supervised learning, which addresses the challenge of limited annotated medical imaging data by leveraging unlabeled data to pre-train models. This approach enhances feature representation capabilities without relying heavily on manual annotations. Self-supervised techniques enable models to learn intrinsic data structures and patterns, which can be fine-tuned for specific downstream tasks such as tumor segmentation, classification, or mutation status prediction. Deep learning and machine learning models have been applied to COVID-19 detection from chest X-ray images, with ongoing research into training strategies.180 This improvement is critical in radiomics, where the scarcity of large, well-annotated datasets often hampers model generalizability.
The integration of these emerging architectures with radiomics enables the extraction of high-dimensional, biologically relevant imaging features that reflect tumor heterogeneity and molecular characteristics. For instance, combining radiomics with Vision Transformer (ViT) architectures has been demonstrated to yield superior predictive performance in lung adenocarcinoma EGFR mutation status compared to radiomics or deep learning alone.181 This synergy leverages the complementary strengths of handcrafted features and learned representations, facilitating a more comprehensive phenotypic-genotypic correlation.
In addition to improved accuracy, these architectures offer enhanced interpretability and explainability, which are paramount for clinical adoption. Attention mechanisms in Transformers and node-level relevance scoring in GNNs provide insights into which image regions or features contribute most to the model’s decision, aiding clinicians in understanding and trusting AI-driven diagnostics. For example, attention-based models have been used to identify tumor microenvironment elements from multiplex-stained images, linking imaging phenotypes to clinical outcomes in breast cancer.182
Collectively, the adoption of Transformer architectures, graph neural networks, and self-supervised learning in radiomics represents a paradigm shift toward more accurate, interpretable, and data-efficient models. These advances facilitate the bridging of imaging phenotypes with underlying genomic heterogeneity, ultimately enhancing personalized medicine approaches in oncology. Future research is encouraged to explore multimodal data fusion, incorporating imaging and molecular data within these architectures to further improve predictive capabilities.183
In summary, emerging deep learning architectures such as Transformers and GNNs, combined with self-supervised learning strategies, provide substantial advantages in radiomics by improving feature representation, enabling effective integration of heterogeneous data, and enhancing model interpretability. Transformer architectures and attention mechanisms have advanced genomic and transcriptomic data analysis, providing potential for future applications.184
Big Data and Cloud Computing Platform Support
The integration of big data and cloud computing platforms is pivotal for advancing radiomics and deep learning in breast cancer research. Multi-center data sharing enables the aggregation of diverse imaging and genomic datasets, enhancing model robustness and generalizability through collaborative analysis. Cloud-based infrastructures facilitate scalable storage and high-performance computing, significantly accelerating model training and deployment. This synergy allows researchers to efficiently handle vast heterogeneous data, optimize computational workflows, and rapidly translate imaging phenotypes into clinically actionable genomic insights.
Integration of Liquid Biopsy and Radiomics in Multimodal Studies
The integration of circulating tumor DNA (ctDNA) analysis with radiomic features extracted from medical imaging represents a promising frontier in precision oncology, particularly for breast cancer. Liquid biopsy offers a minimally invasive approach to capture tumor-derived genetic and epigenetic information, including mutations, methylation patterns, and fragmentomics, which reflect tumor heterogeneity and dynamics in real time. Radiomics, on the other hand, quantitatively characterizes tumor phenotypes and microenvironmental heterogeneity by extracting high-dimensional features from imaging modalities such as mammography, ultrasound, MRI, and PET/CT. Combining these modalities leverages complementary biological and spatial information, enhancing diagnostic accuracy and personalized treatment strategies.
Several studies have demonstrated the synergistic potential of this multimodal approach. In breast cancer management, ctDNA provides molecular insights, and radiomics captures morphological and textural heterogeneity, representing promising future directions.185 The complementary nature of these data modalities enables the development of integrated predictive models that outperform single-modality analyses. Models incorporating deep learning-based radiomic features from multimodal imaging have shown improved discrimination between benign and malignant breast lesions.112 Furthermore, the integration facilitates non-invasive monitoring of treatment response and early detection of recurrence, potentially reducing the need for invasive biopsies.
The development of multimodal biomarkers involves sophisticated machine learning frameworks that fuse data at different levels, including feature-level fusion and decision-level fusion. Transformer-based fusion models have demonstrated improved predictive accuracy in biological activity recognition of hepatic cystic echinococcosis by integrating clinical variables, radiomics, and deep learning features.178 These models can effectively capture complex interactions between imaging phenotypes and molecular alterations detected by liquid biopsy. For example, in gliomas, the combination of MRI radiomics and circulating tumor cell (CTC) parameters has been explored to achieve non-invasive integrated diagnosis aligned with the 2021 WHO CNS tumor classification, highlighting the potential to refine molecular subtype prediction preoperatively.186
Moreover, the use of artificial intelligence, particularly deep learning algorithms, facilitates the extraction of robust and high-level features from both imaging and liquid biopsy data, enabling the construction of comprehensive multimodal models. Studies in pancreatic cancer have shown that AI-supported radiomics and liquid biopsy technologies improve early detection and treatment response prediction, highlighting their clinical utility.187,188 This integrative strategy aligns with the goals of precision medicine by providing dynamic, patient-specific insights that guide tailored therapeutic interventions.
However, challenges remain in standardizing data acquisition, harmonizing multimodal datasets, and validating models across diverse populations and clinical settings. The heterogeneity of liquid biopsy analytes and imaging protocols necessitates rigorous methodological frameworks and multicenter collaborations to ensure reproducibility and generalizability. Additionally, interpretability of AI-driven models is crucial for clinical translation, requiring transparent algorithms and integration with existing clinical workflows.
In summary, the combined analysis of circulating tumor DNA and radiomic features through advanced AI-driven multimodal models represents a transformative approach in breast cancer and other malignancies (Figure 6). This integration enhances the sensitivity and specificity of diagnosis, prognostication, and treatment monitoring, offering a non-invasive and comprehensive assessment of tumor biology and heterogeneity. Continued research focusing on standardized protocols, large-scale validation, and real-world implementation will be pivotal in establishing these multimodal biomarkers as routine clinical tools.185–187
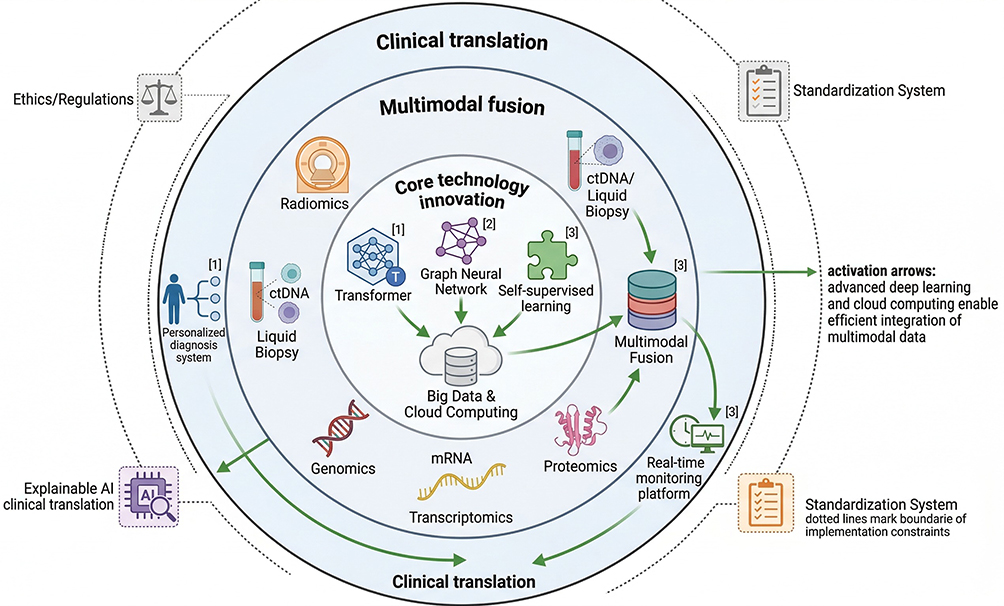 |
Figure 6 Schematic diagram of cutting-edge technologies and future development directions of breast cancer radiomics. This circular schematic illustrates the development trend of breast cancer radiomics based on the logic of “core technology innovation → multimodal fusion → clinical translation”. The inner circle shows underlying technical innovations (emerging deep learning architectures: Transformer/GNN/self-supervised learning; big data and cloud computing); the middle circle displays multimodal fusion (radiomics + liquid biopsy (ctDNA/CTC), radiomics + multi-omics (genomics/transcriptomics/proteomics)); the outer circle presents clinical translation (personalized diagnosis and treatment decision system, real-time efficacy monitoring platform, explainable AI clinical translation). Peripheral constraints (ethics/regulations, standardization system) are annotated to reflect practical clinical implementation considerations, with key references for cutting-edge technologies. |
Ethics, Regulations, and Future Prospects
Data Privacy and Ethical Issues
The integration of radiomics and deep learning in breast cancer imaging phenotyping and genomic heterogeneity analysis introduces critical challenges related to data privacy and ethical considerations. Medical imaging and genomic data are inherently sensitive, containing personal health information that requires stringent protection measures to prevent unauthorized access and misuse. The protection of patient privacy is paramount, as breaches can lead to discrimination, stigmatization, or psychological harm. Advanced AI systems, particularly those employing deep learning, rely on large-scale datasets that often encompass identifiable patient information embedded within imaging and genetic profiles. Data protection, privacy, and ethical considerations are critical in AI applications, though specific anonymization and encryption protocols require further emphasis.175 The complexity of combining imaging data with genomic information further amplifies privacy risks, necessitating the development of specialized frameworks that address the unique vulnerabilities of multi-modal datasets.
Informed consent represents a cornerstone of ethical data use in breast cancer research involving AI technologies. Patients must be adequately informed about how their imaging and genomic data will be collected, stored, analyzed, and potentially shared. This transparency fosters trust and aligns with ethical norms that respect patient autonomy. However, the dynamic nature of AI research, which may involve secondary data use and evolving analytic techniques, complicates the consent process. Traditional one-time consent may be insufficient, prompting the adoption of dynamic consent models that allow patients to update their preferences over time. Moreover, data sharing among institutions and researchers is crucial for enhancing AI model robustness and generalizability, but it must be balanced against privacy concerns. Ethical considerations in AI applications include privacy and regulatory compliance, with ongoing discussions on data sharing and access.176 The establishment of standardized ethical protocols can harmonize practices across institutions, promoting responsible data stewardship.
The ethical implications extend beyond privacy and consent to encompass fairness, transparency, and accountability in AI applications. Biases in training datasets, arising from unbalanced representation of demographic groups or imaging protocols, can perpetuate health disparities if not rigorously addressed. Ensuring equitable access to AI-driven diagnostic and prognostic tools is vital to prevent exacerbation of existing inequalities in breast cancer care. Transparency in AI algorithms, including clear documentation of model development, validation, and limitations, is essential to maintain clinician and patient confidence. Additionally, mechanisms to identify and attribute responsibility for AI errors must be established to uphold ethical standards in clinical practice.175 These considerations highlight the need for multidisciplinary collaboration among clinicians, ethicists, data scientists, and legal experts to create comprehensive frameworks that safeguard patient welfare in the era of AI-enhanced breast cancer management.
The deployment of AI in breast cancer diagnostics and treatment planning also raises questions about the impact on the healthcare workforce and patient-clinician relationships. While AI can augment radiologists and pathologists by improving accuracy and efficiency, it should not supplant the critical role of human judgment and empathy. Ethical frameworks advocate for AI systems that support shared decision-making and preserve patient-centered care. Continuous monitoring and evaluation of AI tools are necessary to detect unintended consequences and ensure alignment with ethical principles throughout their lifecycle. The evolving landscape of AI in breast cancer care demands proactive governance strategies that anticipate and mitigate ethical challenges, thereby fostering sustainable integration of these technologies into clinical practice.176 This approach will help maintain public trust and optimize the benefits of AI innovations for diverse patient populations.
In summary, addressing data privacy and ethical issues is fundamental to the responsible application of radiomics and deep learning in breast cancer imaging and genomics. Protecting sensitive information, securing informed consent, ensuring fairness and transparency, and preserving the human element of care are pivotal to harnessing AI’s potential while upholding ethical standards. Establishing robust, standardized ethical frameworks and regulatory oversight will be crucial to navigating these challenges and advancing precision oncology.
Regulatory Environment and Clinical Translation Barriers
The regulatory landscape for medical devices, including AI-driven radiomics and deep learning tools in breast cancer imaging, is a critical factor influencing their clinical translation. Medical device certification involves rigorous evaluation processes to ensure safety, efficacy, and quality before market approval. Regulatory bodies such as the U.S. Food and Drug Administration (FDA), European Medicines Agency (EMA), and other national agencies require comprehensive documentation covering device design, validation, clinical performance, and risk management. AI applications in medical imaging show promise, though challenges remain in addressing biases and ensuring reproducibility.189,190 The complexity of AI algorithms, especially deep learning models, poses unique challenges in regulatory review because these systems may evolve over time with continuous learning or updates, raising questions about the need for ongoing validation and post-market surveillance. Furthermore, demographic biases identified in computational pathology models underscore the necessity for regulatory frameworks to incorporate stratified evaluation to prevent disparities in diagnostic accuracy among different patient groups.191 This highlights that regulatory policies must evolve to consider not only traditional device safety but also algorithmic fairness and transparency.
Clinical trial design for AI and radiomics applications in breast cancer also faces significant regulatory and practical challenges. Trials must demonstrate not only diagnostic or prognostic accuracy but also clinical utility and impact on patient outcomes. AI and radiomics applications in breast cancer face challenges including data consistency, technical reproducibility, and clinical translation.54,176 Regulatory compliance requires adherence to Good Clinical Practice (GCP) standards, data privacy laws such as HIPAA or GDPR, and ethical considerations related to AI decision-making transparency. Moreover, validation studies should include external datasets to assess generalizability and mitigate domain shifts that can degrade model performance when applied to new clinical settings.176 The lack of standardized reporting and evaluation metrics further complicates regulatory approval and clinical acceptance. Hence, a collaborative approach involving regulators, clinicians, AI developers, and patients is necessary to establish consensus guidelines that balance innovation with patient safety and ethical responsibility.
In addition to regulatory and trial design hurdles, the integration of AI-driven radiomics into clinical practice is hindered by workflow compatibility and interpretability issues. AI adoption in clinical practice faces challenges including interpretability and workflow integration, with ongoing efforts to improve usability.173,174 The black-box nature of many deep learning models limits clinicians’ ability to understand the rationale behind predictions, which can impede adoption and raise medico-legal concerns. Efforts to develop explainable AI (XAI) frameworks and transparent algorithms are ongoing to enhance interpretability and regulatory acceptance.190 Furthermore, the heterogeneity of imaging devices, acquisition protocols, and patient populations necessitates robust calibration and continuous performance monitoring to maintain accuracy and safety post-deployment. These factors collectively represent significant translational barriers that must be addressed to realize the full potential of radiomics and deep learning in personalized breast cancer management.
The evolving regulatory environment is gradually adapting to the unique challenges posed by AI in medical imaging, with increasing emphasis on lifecycle management, real-world evidence collection, and adaptive regulatory pathways. For instance, the FDA has introduced frameworks for Software as a Medical Device (SaMD) that include provisions for AI/ML-based modifications and continuous learning systems. Technological innovation in AI is rapid, with ongoing considerations for regulatory frameworks to support clinical translation.189 Collaborative efforts to harmonize international regulatory standards and promote data-sharing initiatives are crucial to accelerate validation and approval processes. Additionally, addressing ethical concerns such as data privacy, informed consent, and algorithmic bias is integral to regulatory compliance and public trust. Given these challenges, it is anticipated that future regulatory policies will increasingly require comprehensive demographic and clinical validation to ensure equitable and effective AI applications in breast cancer imaging.
Overall, the regulatory environment and clinical translation barriers for AI-based radiomics in breast cancer imaging encompass device certification complexities, stringent clinical trial requirements, workflow integration challenges, and evolving policy frameworks. Addressing these multifaceted obstacles through interdisciplinary collaboration, transparent methodologies, and rigorous validation will be essential to bridge the gap between technological advances and routine clinical use. Continued efforts to standardize evaluation metrics, mitigate biases, and develop explainable models will facilitate regulatory approval and adoption, ultimately enhancing personalized breast cancer diagnosis and treatment.
Strategies to Promote Clinical Application of Radiogenomics
The clinical translation of radiogenomics in breast cancer faces multifaceted challenges that necessitate strategic approaches centered on interdisciplinary collaboration and standardization. Radiogenomics integrates imaging phenotypes with genomic data to characterize tumor heterogeneity and predict clinical outcomes, but the complexity of data types and analytic methods requires coordinated efforts among radiologists, oncologists, bioinformaticians, and molecular biologists. Establishing standardized protocols for image acquisition, feature extraction, and genomic data processing is critical to ensure reproducibility and comparability across studies and clinical settings. Variability in radiomic feature normalization methods can introduce bias and affect analysis in breast cancer studies.150,192 Collaborative consortia involving imaging device manufacturers, regulatory bodies, healthcare providers, and academic institutions have been proposed to develop consensus guidelines and shared databases that facilitate multicenter validation and benchmarking of radiogenomic models.48 Such initiatives can also address data heterogeneity by harmonizing imaging protocols and genomic assays, thereby enhancing the robustness of predictive models and their acceptance in clinical workflows.
In addition to technical standardization, education and training are pivotal for the successful integration of radiogenomics into clinical practice. Radiologists and oncologists must be equipped with foundational knowledge of artificial intelligence, machine learning, and genomics to interpret radiogenomic outputs effectively and incorporate them into decision-making processes. Training programs and interdisciplinary workshops can bridge the knowledge gap, fostering a culture of collaboration and innovation. Moreover, clinical promotion requires demonstrating the added value of radiogenomics in improving diagnostic accuracy, prognostication, and treatment planning through prospective clinical trials and real-world evidence. Models combining radiomics and genomic signatures have shown promise in predicting axillary lymph node metastasis in breast cancer patients, highlighting the potential of radiogenomics to refine risk stratification.108,151 These models, however, need to be validated in diverse populations and integrated with existing clinical parameters to gain regulatory approval and clinician trust.
Furthermore, addressing ethical, regulatory, and data privacy concerns is essential to facilitate clinical adoption. The sensitive nature of genomic data and the complexity of AI algorithms necessitate transparent, explainable models that comply with data protection regulations and ethical standards. Ethical challenges in AI applications include transparency and trust, with ongoing efforts to develop explainable AI frameworks.175,190 Engaging stakeholders, including patients, in the development and implementation of radiogenomic tools ensures that clinical applications align with patient-centered care principles.
Finally, leveraging multimodal data fusion approaches that integrate imaging, genomics, clinical, and pathological information can enhance the predictive power and clinical utility of radiogenomic models. Recent advances in deep learning and multimodal feature fusion have demonstrated improved diagnostic accuracy and robustness by combining heterogeneous data sources.55,119 These integrative strategies require cross-disciplinary expertise and infrastructure, underscoring the importance of sustained collaboration and resource sharing.
In summary, promoting the clinical application of radiogenomics in breast cancer hinges on fostering interdisciplinary collaboration, establishing standardized methodologies, advancing education and clinical validation, ensuring ethical and regulatory compliance, and embracing integrative multimodal analytics. These strategies collectively pave the way for radiogenomics to become a transformative tool in precision oncology.
Conclusion
In conclusion, the integration of radiomics with deep learning has emerged as a powerful approach to elucidate the intricate relationship between breast cancer imaging phenotypes and underlying genomic heterogeneity. From an expert perspective, this interdisciplinary synergy offers a transformative, non-invasive window into tumor molecular characteristics that were previously accessible only through invasive tissue sampling. By leveraging systematic workflows and cutting-edge modeling techniques, these methods have enabled the extraction of subtle yet clinically meaningful genomic mutations and immune microenvironment features directly from imaging data, thereby advancing the frontier of precision oncology.
Balancing the diverse research perspectives in this rapidly evolving field requires a nuanced understanding of both the technological capabilities and the biological complexities involved. On one hand, radiogenomic approaches have demonstrated remarkable potential to refine diagnostic accuracy, prognostication, and therapeutic stratification in breast cancer. On the other hand, challenges such as data heterogeneity, lack of standardized imaging and genomic protocols, and the often “black-box” nature of deep learning models necessitate cautious interpretation and rigorous validation. Ensuring model explainability and reproducibility remains critical to gaining clinical trust and facilitating integration into routine workflows.
Moreover, the translation of radiogenomic discoveries into clinical practice is contingent upon addressing ethical, regulatory, and practical considerations. The development of robust ethical frameworks and regulatory guidelines will be essential to safeguard patient privacy and data security, while fostering responsible innovation. Additionally, large-scale, multi-center validation studies are imperative to confirm the generalizability and robustness of radiomic biomarkers across diverse populations and imaging platforms. Such collaborative, multidisciplinary efforts will accelerate the maturation of this technology from promising research to reliable clinical tools.
Looking forward, the continued convergence of artificial intelligence, molecular biology, and medical imaging holds great promise to bridge the gap between phenotypic observations and genomic insights. This precision bridge has the potential not only to revolutionize breast cancer management by enabling truly personalized treatment but also to serve as a paradigm for other malignancies. Ultimately, the success of radiogenomics in breast cancer will depend on harmonizing technological innovation with clinical applicability, ethical responsibility, and collaborative validation—ensuring that these powerful tools are safely and effectively harnessed to improve patient outcomes in the era of precision medicine.
Funding
This work was supported by the Medical Science and Technology Project of the Sichuan Provincial Health Commission (No.25QNMP083) and the Neijiang Municipal Science and Technology Program (Grant Nos. Z2025041 and Z2025036).
Disclosure
The authors report no conflicts of interest int his work.
References
1. Müller M, Güth U, Varga Z, et al. Clinical imaging of the heterogeneous group of triple-negative breast cancer. Anticancer Res. 2020;40(4):2125–37. doi:10.21873/anticanres.14171
2. Mehraj U, Mushtaq U, Mir MA, et al. Chemokines in triple-negative breast cancer heterogeneity: new challenges for clinical implications. Semin Cancer Biol. 2022;86(Pt 2):769–783. doi:10.1016/j.semcancer.2022.03.008
3. Okines AFC, Turner NC. Heterogeneous HER2 amplification-a new clinical category of HER2-positive breast cancer? Cancer Discov. 2021;11(10):2369–2371. doi:10.1158/2159-8290.CD-21-0936
4. Li Z, Metzger Filho O, Viale G, et al. HER2 heterogeneity and treatment response-associated profiles in HER2-positive breast cancer in the NCT02326974 clinical trial. J Clin Invest. 2024;134(7). doi:10.1172/JCI176454
5. Meléndez-Flórez MP, Ortega-Recalde O, Rangel N, et al. Chromosomal instability and clonal heterogeneity in breast cancer: from mechanisms to clinical applications. Cancers. 2025;17(7):1222. doi:10.3390/cancers17071222
6. Hao L, Zheng L. Clinical significance and heterogeneity of circulating tumor cells and clusters in breast cancer subtypes. PeerJ. 2025;13:e19703. doi:10.7717/peerj.19703
7. Liu L, Yi X, Lu C, et al. Background, applications and challenges of radiogenomics in genitourinary tumor. Am J Cancer Res. 2021;11(5):1936–1945.
8. Wang SR, Shen YT, Huang B, et al. Ultrasound-based radiogenomics: status, applications, and future direction. Ultrasonography. 2025;44(2):95–111. doi:10.14366/usg.24152
9. He W, Huang W, Zhang L, et al. Radiogenomics: bridging the gap between imaging and genomics for precision oncology. MedComm. 2024;5(9):e722. doi:10.1002/mco2.722
10. Liu H, Zou L, Xu N, et al. Deep learning radiomics based prediction of axillary lymph node metastasis in breast cancer. NPJ Breast Cancer. 2024;10(1):22. doi:10.1038/s41523-024-00628-4
11. Zhang J, Yin W, Yang L, et al. Deep learning radiomics nomogram based on multiphase computed tomography for predicting axillary lymph node metastasis in breast cancer. Mol Imaging Biol. 2024;26(1):90–100. doi:10.1007/s11307-023-01839-0
12. Cheng C, Wang Y, Zhao J, et al. Deep learning and radiomics in triple-negative breast cancer: predicting long-term prognosis and clinical outcomes. J Multidiscip Healthc. 2025;18:319–327. doi:10.2147/JMDH.S509004
13. Shen JT, Chen GQ, Lun HM, et al. Key parameters in intratumoral-peritumoral region fusion models: optimizing deep learning radiomics for breast cancer diagnosis. Front Oncol. 2025;15:1587879. doi:10.3389/fonc.2025.1587879
14. Hartmann K, Sadée CY, Satwah I, et al. Imaging genomics: data fusion in uncovering disease heritability. Trends Mol Med. 2023;29(2):141–151. doi:10.1016/j.molmed.2022.11.002
15. Buda M, AlBadawy EA, Saha A, et al. Deep radiogenomics of lower-grade gliomas: convolutional neural networks predict tumor genomic subtypes using MR images. Radiol Artif Intell. 2020;2(1):e180050. doi:10.1148/ryai.2019180050
16. Li X, Yang L, Jiao X. Comparison of traditional radiomics, deep learning radiomics and fusion methods for axillary lymph node metastasis prediction in breast cancer. Acad Radiol. 2023;30(7):1281–1287. doi:10.1016/j.acra.2022.10.015
17. Hu M, Zhang L, Wang X, et al. Enhanced HER-2 prediction in breast cancer through synergistic integration of deep learning, ultrasound radiomics, and clinical data. Sci Rep. 2025;15(1):26992. doi:10.1038/s41598-025-12825-7
18. Zhong ME, Duan X, Ni-Jia-Ti MY, et al. CT-based radiogenomic analysis dissects intratumor heterogeneity and predicts prognosis of colorectal cancer: a multi-institutional retrospective study. J Transl Med. 2022;20(1):574. doi:10.1186/s12967-022-03788-8
19. Liu Q, Hu P. Extendable and explainable deep learning for pan-cancer radiogenomics research. Curr Opin Chem Biol. 2022;66:102111. doi:10.1016/j.cbpa.2021.102111
20. Gou X, Feng A, Feng C, et al. Imaging genomics of cancer: a bibliometric analysis and review. Cancer Imaging. 2025;25(1):24. doi:10.1186/s40644-025-00841-9
21. Guido LP, Gomez-Fernandez C. Advances in the molecular taxonomy of breast cancer. Arch Med Res. 2020;51(8):777–783. doi:10.1016/j.arcmed.2020.08.001
22. Zhao S, Zuo WJ, Shao ZM, et al. Molecular subtypes and precision treatment of triple-negative breast cancer. Ann Transl Med. 2020;8(7):499. doi:10.21037/atm.2020.03.194
23. Garmpis N, Damaskos C, Garmpi A, et al. Molecular classification and future therapeutic challenges of triple-negative breast cancer. Vivo. 2020;34(4):1715–1727. doi:10.21873/invivo.11965
24. López-Ruiz JA, Mieza JA, Zabalza I, et al. Comparison of genomic profiling data with clinical parameters: implications for breast cancer prognosis. Cancers. 2022;14(17):4197. doi:10.3390/cancers14174197
25. Testa U, Castelli G, Pelosi E. Breast cancer: a molecularly heterogenous disease needing subtype-specific treatments. Med Sci. 2020;8(1):18. doi:10.3390/medsci8010018
26. Kim TM, Yang IS, Seung BJ, et al. Cross-species oncogenic signatures of breast cancer in canine mammary tumors. Nat Commun. 2020;11(1):3616. doi:10.1038/s41467-020-17458-0
27. Loh JW, Lim AH, Chan JY, et al. Classification of HER2-negative breast cancers by ERBB2 copy number alteration status reveals molecular differences associated with chromosome 17 gene aberrations. Ther Adv Med Oncol. 2023;15:17588359231206259. doi:10.1177/17588359231206259
28. Li Y, Yang X, Geng C, et al. Identification of molecular subtypes based on chromatin regulator-related genes and experimental verification of the role of ASCL1 in conferring chemotherapy resistance to breast cancer. Front Immunol. 2024;15:1390261. doi:10.3389/fimmu.2024.1390261
29. Zhu W, Huang H, Hu Z, et al. Comprehensive transcriptome analysis expands lncRNA functional profiles in breast cancer. Int J Mol Sci. 2024;25(15):8456. doi:10.3390/ijms25158456
30. Zhang Y, Yue Q, Cao F, et al. Necroptosis-related lncRNA signatures determine prognosis in breast cancer patients. Sci Rep. 2022;12(1):11268. doi:10.1038/s41598-022-15209-3
31. Peng XF, Qin FL, Chen WJ, et al. The landscape of angiogenesis subtypes for breast cancer: a comprehensive analysis based on the Cancer Genome Atlas. J BUON. 2021;26(5):1975–1990.
32. Ji F, Chen X, Yang C, et al. Multi-omic-based classification for identifying optimal neoadjuvant treatment strategies for high-risk early-stage breast cancer. Sci China Life Sci. 2025;68(10):2934–2949. doi:10.1007/s11427-024-2809-y
33. Watson J, Wang T, Ho KL, et al. Human basal-like breast cancer is represented by one of the two mammary tumor subtypes in dogs. Breast Cancer Res. 2023;25(1):114. doi:10.1186/s13058-023-01705-5
34. Watson J, Wang T, Ho KL, et al. Human basal-like breast cancer is represented by one of the two mammary tumor subtypes in dogs. bioRxiv. Preprint. 2023. doi:10.1101/2023.03.02.530622
35. Furtney I, Bradley R, Kabuka MR. Patient graph deep learning to predict breast cancer molecular subtype. IEEE. 2023;20(5):3117–3127. doi:10.1109/TCBB.2023.3290394
36. An Y, Liu X, Chen H, et al. Identification of breast cancer subtypes based on graph convolutional network. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2024;41(1):121–128. doi:10.7507/1001-5515.202306071
37. Das SC, Tasnim W, Rana HK, et al. Comprehensive bioinformatics and machine learning analyses for breast cancer staging using TCGA dataset. Brief Bioinform. 2024;26(1):bbae628. doi:10.1093/bib/bbae628
38. Bismeijer T, van der Velden BHM, Canisius S, et al. Radiogenomic analysis of breast cancer by linking MRI phenotypes with tumor gene expression. Radiology. 2020;296(2):277–287. doi:10.1148/radiol.2020191453
39. Bar-Hai N, Ben-Yishay R, Arbili-Yarhi S, et al. Modeling epithelial-mesenchymal transition in patient-derived breast cancer organoids. Front Oncol. 2024;14:1470379. doi:10.3389/fonc.2024.1470379
40. Lv T, Hong X, Liu Y, et al. AI-powered interpretable imaging phenotypes noninvasively characterize tumor microenvironment associated with diverse molecular signatures and survival in breast cancer. Comput Methods Programs Biomed. 2024;243:107857. doi:10.1016/j.cmpb.2023.107857
41. Klaassen R, Steins A, Gurney-Champion OJ, et al. Pathological validation and prognostic potential of quantitative MRI in the characterization of pancreas cancer: preliminary experience. Mol Oncol. 2020;14(9):2176–2189. doi:10.1002/1878-0261.12688
42. Kuett L, Bollhagen A, Tietscher S, et al. Distant metastases of breast cancer resemble primary tumors in cancer cell composition but differ in immune cell phenotypes. Cancer Res. 2025;85(1):15–31. doi:10.1158/0008-5472.CAN-24-1211
43. Cords L, Tietscher S, Anzeneder T, et al. Cancer-associated fibroblast classification in single-cell and spatial proteomics data. Nat Commun. 2023;14(1):4294. doi:10.1038/s41467-023-39762-1
44. Zhao S, Chen DP, Fu T, et al. Single-cell morphological and topological atlas reveals the ecosystem diversity of human breast cancer. Nat Commun. 2023;14(1):6796. doi:10.1038/s41467-023-42504-y
45. Eng J, Bucher E, Hu Z, et al. Robust biomarker discovery through multiplatform multiplex image analysis of breast cancer clinical cohorts. bioRxiv. 2023. doi:10.1101/2023.01.31.525753
46. Chitalia R, Viswanath V, Pantel AR, et al. Functional 4-D clustering for characterizing intratumor heterogeneity in dynamic imaging: evaluation in FDG PET as a prognostic biomarker for breast cancer. Eur J Nucl Med Mol Imaging. 2021;48(12):3990–4001. doi:10.1007/s00259-021-05265-8
47. Ahn HSH, Oloumi Yazdi Y, Wadsworth BJ, et al. Relating macroscopic PET radiomics features to microscopic tumor phenotypes using a stochastic mathematical model of cellular metabolism and proliferation. Cancers. 2024;16(12):2215. doi:10.3390/cancers16122215
48. Singh A, Chitalia R, Kontos D. Radiogenomics in brain, breast, and lung cancer: opportunities and challenges. J Med Imaging. 2021;8(3):031907. doi:10.1117/1.JMI.8.3.031907
49. Liu W, Chen W, Xia J, et al. Lymph node metastasis prediction and biological pathway associations underlying DCE-MRI deep learning radiomics in invasive breast cancer. BMC Med Imag. 2024;24(1):91. doi:10.1186/s12880-024-01255-y
50. Su GH, Xiao Y, You C, et al. Radiogenomic-based multiomic analysis reveals imaging intratumor heterogeneity phenotypes and therapeutic targets. Sci Adv. 2023;9(40):eadf0837. doi:10.1126/sciadv.adf0837
51. Liu Q, Hu P. Radiogenomic association of deep MR imaging features with genomic profiles and clinical characteristics in breast cancer. Biomark Res. 2023;11(1):9. doi:10.1186/s40364-023-00455-y
52. Wang G, Wang S, Song W, et al. Integrating multi-omics data reveals the antitumor role and clinical benefits of gamma-delta T cells in triple-negative breast cancer. BMC Cancer. 2025;25(1):623. doi:10.1186/s12885-025-14029-8
53. Zanfardino M, Castaldo R, Pane K, et al. MuSA: a graphical user interface for multi-OMICs data integration in radiogenomic studies. Sci Rep. 2021;11(1):1550. doi:10.1038/s41598-021-81200-z
54. Pesapane F, De Marco P, Rapino A, et al. How radiomics can improve breast cancer diagnosis and treatment. J Clin Med. 2023;12(4):1372. doi:10.3390/jcm12041372
55. Maruf NA, Basuhail A, Ramzan MU. Enhanced breast cancer diagnosis using multimodal feature fusion with radiomics and transfer learning. Diagnostics. 2025;15(17):2170. doi:10.3390/diagnostics15172170
56. Zhao X, Bai JW, Guo Q, et al. Clinical applications of deep learning in breast MRI. Biochim Biophys Acta Rev Cancer. 2023;1878(2):188864. doi:10.1016/j.bbcan.2023.188864
57. Ramadan SZ. Methods used in computer-aided diagnosis for breast cancer detection using mammograms: a review. J Healthc Eng. 2020;9162464. doi:10.1155/2020/9162464
58. L. C M, P. M JP. An optimal deep learning approach for breast cancer detection and classification with pre-trained CNN-based feature learning mechanism. J Biomol Struct Dyn. 2024;1–16. doi:10.1080/07391102.2024.2430454
59. Sollini M, Cozzi L, Ninatti G, et al. PET/CT radiomics in breast cancer: mind the step. Methods. 2021;188:122–132. doi:10.1016/j.ymeth.2020.01.007
60. SR D, SA B, AK L, et al. Comparison of intensity normalization methods in prostate, brain, and breast cancer multi-parametric magnetic resonance imaging. Front Oncol. 2025;15:1433444. doi:10.3389/fonc.2025.1433444/
61. Alotaibi M, Aljouie A, Alluhaidan N, et al. Breast cancer classification based on convolutional neural network and image fusion approaches using ultrasound images. Heliyon. 2023;9(11):e22406. doi:10.1016/j.heliyon.2023.e22406
62. Tang X, Zhang H, Mao R, et al. Preoperative prediction of axillary lymph node metastasis in patients with breast cancer through multimodal deep learning based on ultrasound and magnetic resonance imaging images. Acad Radiol. 2025;32(1):1–11. doi:10.1016/j.acra.2024.07.029
63. Al-Mnayyis AM, Gharaibeh H, Amin M, et al. (KAUH-BCMD) dataset: advancing mammographic breast cancer classification with multi-fusion preprocessing and residual depth-wise network. Front Big Data. 2025;8:1529848. doi:10.3389/fdata.2025.1529848
64. Samee NA, Alhussan AA, Ghoneim VF, et al. A hybrid deep transfer learning of CNN-Based LR-PCA for breast lesion diagnosis via medical breast mammograms. Sensors. 2022;22(13):4938. doi:10.3390/s22134938
65. Piantadosi G, Sansone M, Fusco R, et al. Multi-planar 3D breast segmentation in MRI via deep convolutional neural networks. Artif Intell Med. 2020;103:101781. doi:10.1016/j.artmed.2019.101781
66. Samiei S, Granzier RWY, Ibrahim A, et al. Dedicated axillary MRI-Based radiomics analysis for the prediction of axillary lymph node metastasis in breast cancer. Cancers. 2021;13(4):757. doi:10.3390/cancers13040757
67. Acciavatti RJ, Cohen EA, Maghsoudi OH, et al. Robust radiomic feature selection in digital mammography: understanding the effect of imaging acquisition physics using phantom and clinical data analysis. Proc SPIE Int Soc Opt Eng. 2020;11314:113140W. doi:10.1117/12.2549163
68. Acciavatti RJ, Cohen EA, Maghsoudi OH, et al. Incorporating robustness to imaging physics into radiomic feature selection for breast cancer risk estimation. Cancers. 2021;13(21):5497. doi:10.3390/cancers13215497
69. Whitney HM, Li H, Ji Y, et al. Multi-Stage harmonization for robust AI across breast MR databases. Cancers. 2021;13(19):4809. doi:10.3390/cancers13194809
70. Saba T, Abunadi I, Sadad T, et al. Optimizing the transfer-learning with pretrained deep convolutional neural networks for first stage breast tumor diagnosis using breast ultrasound visual images. Microsc Res Tech. 2022;85(4):1444–1453. doi:10.1002/jemt.24008
71. Granzier RWY, Verbakel NMH, Ibrahim A, et al. MRI-based radiomics in breast cancer: feature robustness with respect to inter-observer segmentation variability. Sci Rep. 2020;10(1):14163. doi:10.1038/s41598-020-70940-z
72. Park JH, Kwon LM, Lee HK, et al. Radiomic analysis of magnetic resonance imaging for breast cancer with TP53 mutation: a Single Center Study. Diagnostics. 2025;15(4):428. doi:10.3390/diagnostics15040428
73. Saadh MJ, Hussain QM, Albadr RJ, et al. Radiomics meets transformers: a novel approach to tumor segmentation and classification in mammography for breast cancer. J Xray Sci Technol. 2025;33(6):1039–1058. doi:10.1177/08953996251351624
74. Dutta K, Roy S, Whitehead TD, et al. Deep Learning segmentation of Triple-Negative Breast Cancer (TNBC) Patient Derived Tumor Xenograft (PDX) and sensitivity of radiomic pipeline to tumor probability boundary. Cancers. 2021;13(15):3795. doi:10.3390/cancers13153795
75. Xiong L, Tang X, Jiang X, et al. Automatic segmentation-based multi-modal radiomics analysis of US and MRI for predicting disease-free survival of breast cancer: a multicenter study. Breast Cancer Res. 2024;26(1):157. doi:10.1186/s13058-024-01909-3
76. Li C, Lu N, He Z, et al. A noninvasive tool based on magnetic resonance imaging radiomics for the preoperative prediction of pathological complete response to neoadjuvant chemotherapy in breast cancer. Ann Surg Oncol. 2022;29(12):7685–7693. doi:10.1245/s10434-022-12034-w
77. Aksu A, Güç ZG, Küçüker KA, et al. Intra and peritumoral PET radiomics analysis to predict the pathological response in breast cancer patients receiving neoadjuvant chemotherapy. Rev Esp Med Nucl Imagen Mol. 2024;43(3):500002. doi:10.1016/j.remnie.2024.500002
78. Park GE, Kim SH, Nam Y, et al. 3D Breast cancer segmentation in DCE-MRI using deep learning with weak annotation. J Magn Reson Imaging. 2024;59(6):2252–2262. doi:10.1002/jmri.28960
79. Li L, Tian H, Zhang B, et al. Prediction for distant metastasis of breast cancer using dynamic contrast-enhanced magnetic resonance imaging images under deep learning. Comput Intell Neurosci. 2022:6126061. doi:10.1155/2022/6126061
80. Wang X, Xie T, Luo J, et al. Radiomics predicts the prognosis of patients with locally advanced breast cancer by reflecting the heterogeneity of tumor cells and the tumor microenvironment. Breast Cancer Res. 2022;24(1):20. doi:10.1186/s13058-022-01516-0
81. Qi YJ, Su GH, You C, et al. Radiomics in breast cancer: current advances and future directions. Cell Rep Med. 2024;5(9):101719. doi:10.1016/j.xcrm.2024.101719
82. Wang Z, Li X, Zhang H, et al. Deep learning radiomics based on two-dimensional ultrasound for predicting the efficacy of neoadjuvant chemotherapy in breast cancer. Ultrason Imaging. 2024;46(6):357–366. doi:10.1177/01617346241276168
83. Miao S, An Y, Liu P, et al. Pectoralis muscle predicts distant metastases in breast cancer by deep learning radiomics. Acta Radiol. 2023;64(9):2561–2569. doi:10.1177/02841851231187373
84. Chen Y, Wang L, Dong X, et al. Deep learning radiomics of preoperative breast MRI for prediction of axillary lymph node metastasis in breast cancer. J Digit Imaging. 2023;36(4):1323–1331. doi:10.1007/s10278-023-00818-9
85. Wang D, Hu Y, Zhan C, et al. A nomogram based on radiomics signature and deep-learning signature for preoperative prediction of axillary lymph node metastasis in breast cancer. Front Oncol. 2022;12:940655. doi:10.3389/fonc.2022.940655
86. Li L, Zhou X, Cui W, et al. Combining radiomics and deep learning features of intra-tumoral and peri-tumoral regions for the classification of breast cancer lung metastasis and primary lung cancer with low-dose CT. J Cancer Res Clin Oncol. 2023;149(17):15469–15478. doi:10.1007/s00432-023-05329-2
87. Lu G, Tian R, Yang W, et al. Prediction of bone oligometastases in breast cancer using models based on deep learning radiomics of PET/CT imaging. Front Oncol. 2025;15:1621677. doi:10.3389/fonc.2025.1621677
88. Galati F, Maroncelli R, De Nardo C, et al. Deep learning with transfer learning on digital breast tomosynthesis: a radiomics-based model for predicting breast cancer risk. Diagnostics. 2025;15(13):1631. doi:10.3390/diagnostics15131631
89. Guo F, Li Q, Gao F, et al. Evaluation of the peritumoral features using radiomics and deep learning technology in non-spiculated and noncalcified masses of the breast on mammography. Front Oncol. 2022;12:1026552. doi:10.3389/fonc.2022.1026552
90. Zhao X, Wang M, Wei Y, et al. Overview of multimodal radiomics and deep learning in the prediction of axillary lymph node status in breast cancer. Acad Radiol. 2025;32(11):6623–6641. doi:10.1016/j.acra.2025.07.017
91. Yang ZQ, Zhang Y, Lu F, et al. Integrating multimodal ultrasound imaging for improved radiomics sentinel lymph node assessment in breast cancer. Gland Surg. 2025;14(7):1348–1365. doi:10.21037/gs-2025-223
92. Ma M, Jiang Y, Qin N, et al. A radiomics model for preoperative predicting sentinel lymph node metastasis in breast cancer based on dynamic contrast-enhanced MRI. Front Oncol. 2022;12:884599. doi:10.3389/fonc.2022.884599
93. Guo F, Sun S, Deng X, et al. Predicting axillary lymph node metastasis in breast cancer using a multimodal radiomics and deep learning model. Front Immunol. 2024;15:1482020. doi:10.3389/fimmu.2024.1482020
94. Zhang Y, Huang H, Yin L, et al. Preoperative prediction of HER-2 expression status in breast cancer based on MRI radiomics model. Zhonghua Zhong Liu Za Zhi. 2024;46(5):428–437. doi:10.3760/cma.j.cn112152-20230816-00086
95. Moslemi A, Osapoetra LO, Safakish A, et al. Hybrid feature selection for predicting chemotherapy response in locally advanced breast cancer using clinical and CT radiomics features. Integrat Matrix RankGenetic Algorithm Cancers. 2025;17(17):2738. doi:10.3390/cancers17172738
96. Zhao M, Zheng Y, Chu J, et al. Ultrasound-based radiomics combined with immune status to predict sentinel lymph node metastasis in primary breast cancer. Sci Rep. 2023;13(1):16918. doi:10.1038/s41598-023-44156-w
97. Wei C, Jia Y, Gu Y, et al. Predictive analysis of neoadjuvant chemotherapy efficacy in breast cancer using multi-region ultrasound imaging features combined with pathological parameters. Ultrasound Med Biol. 2025;51(12):2205–2216. doi:10.1016/j.ultrasmedbio.2025.08.027
98. Yan L, Chen Y, He J. Leveraging MRI radiomics signature for predicting the diagnosis of CXCL9 in breast cancer. Heliyon. 2024;10(19):e38640. doi:10.1016/j.heliyon.2024.e38640
99. Vigil N, Barry M, Amini A, et al. Dual-Intended deep learning model for breast cancer diagnosis in ultrasound imaging. Cancers. 2022;14(11):2663. doi:10.3390/cancers14112663
100. Xu Z, Yang Q, Li M, et al. Predicting HER2 status in breast cancer on ultrasound images using deep learning method. Front Oncol. 2022;12:829041. doi:10.3389/fonc.2022.829041
101. Liu J, Leng X, Yuan Z, et al. Predicting breast cancer response to neoadjuvant chemotherapy with ultrasound-based deep learning radiomics models – dual-center study. BMC Cancer. 2025;25(1):1737. doi:10.1186/s12885-025-15148-y
102. Tang Y, Chen L, Qiao Y, et al. Radiomic signature based on dynamic contrast-enhanced MRI for evaluation of axillary lymph node metastasis in breast cancer. Comput Math Methods Med. 2022:1507125. doi:10.1155/2022/1507125
103. Lim CH, Choi JY, Choi JH, et al. Development and external validation of 18F-FDG PET-Based radiomic model for predicting pathologic complete response after neoadjuvant chemotherapy in breast cancer. Cancers. 2023;15(15). doi:10.3390/cancers15153842
104. Deng Y, Lu Y, Li X, et al. Prediction of human epidermal growth factor receptor 2 (HER2) status in breast cancer by mammographic radiomics features and clinical characteristics: a multicenter study. Eur Radiol. 2024;34(8):5464–5476. doi:10.1007/s00330-024-10607-9
105. Fan W, Cui H, Liu X, et al. Machine learning-based ultrasound radiomics for predicting risk of recurrence in breast cancer. Front Oncol. 2025;15:1542643. doi:10.3389/fonc.2025.1542643
106. Hou J, Yang F, Gao Y, et al. MR imaging of breast cancer: interpretable radiomics analysis to assess treatment response and survival prognosis after neoadjuvant therapy. Int J Cancer. 2025;157(8):1723–1733. doi:10.1002/ijc.35514
107. Güler O. A dirichlet distribution-based complex ensemble approach for breast cancer classification from ultrasound images with transfer learning and multiphase spaced repetition method. J Imaging Inform Med. 2025. doi:10.1007/s10278-025-01515-5
108. Chen H, Lan X, Yu T, et al. Development and validation of a radiogenomics model to predict axillary lymph node metastasis in breast cancer integrating MRI with transcriptome data: a multicohort study. Front Oncol. 2022;12:1076267. doi:10.3389/fonc.2022.1076267
109. Oda S, Tokuda Y, Suzuki Y, et al. Integrative radiogenomics using MRI radiomics and microarray gene expression analysis to predict pathological complete response in patients with breast cancer undergoing neoadjuvant chemotherapy. Cureus. 2025;17(6):e86287. doi:10.7759/cureus.86287
110. Li C, Zhang H, Chen J, et al. Deep learning radiomics of ultrasonography for differentiating sclerosing adenosis from breast cancer. Clin Hemorheol Microcirc. 2023;84(2):153–163. doi:10.3233/CH-221608
111. Nebbia G, Dadsetan S, Arefan D, et al. Radiomics-informed deep curriculum learning for breast cancer diagnosis. Med Image Comput Comput Assist Interv. 2021;12905:634–643. doi:10.1007/978-3-030-87240-3_61
112. Lu G, Tian R, Yang W, et al. Deep learning radiomics based on multimodal imaging for distinguishing benign and malignant breast tumours. Front Med Lausanne. 2024;11:1402967. doi:10.3389/fmed.2024.1402967
113. Tang X, Zhu Y. RAE-Net: a multi-modal neural network based on feature fusion and evidential deep learning algorithm in predicting breast cancer subtypes on DCE-MRI. Biomed Phys Eng Express. 2025;11(2). doi:10.1088/2057-1976/adb494
114. Xu W, Shi X. Integrating radiomic texture analysis and deep learning for automated myocardial infarction detection in cine-MRI. Sci Rep. 2025;15(1):24365. doi:10.1038/s41598-025-08127-7
115. Xu J, Feng B, Chen X, et al. Deep learning-based multimodal feature interaction-guided fusion: enhancing the evaluation of EGFR in advanced lung adenocarcinoma. Acad Radiol. 2025;32(9):5585–5595. doi:10.1016/j.acra.2025.04.071
116. Niu Y, Xie HB, Jia HB, et al. Multimodal Deep learning integrating tumor radiomics and mediastinal adiposity improves survival prediction in non-small cell lung cancer: a prognostic modeling study. Cancer Med. 2025;14(15):e71077. doi:10.1002/cam4.71077
117. Wang Y, Zhang L, Li Y, et al. Predicting the prognosis of HER2-positive breast cancer patients by fusing pathological whole slide images and clinical features using multiple instance learning. Math Biosci Eng. 2023;20(6):11196–11211. doi:10.3934/mbe.2023496
118. Wen W, Zhang T, Zhao H, et al. Multimodal model enhances qualitative diagnosis of hypervascular thyroid nodules: integrating radiomics and deep learning features based on B-mode and PDI images. Gland Surg. 2025;14(8):1558–1571. doi:10.21037/gs-2025-183
119. P C, S SBK, R S, et al. Q RadFusion: hybrid quantum classical radiogenomic framework for breast cancer diagnosis. Res Sq. 2025:rs.3.rs–7657076. doi:10.21203/rs.3.rs-7657076/v1
120. Ye Z, Yuan J, Hong D, et al. Multimodal diagnostic models and subtype analysis for neoadjuvant therapy in breast cancer. Front Immunol. 2025;16:1559200. doi:10.3389/fimmu.2025.1559200
121. Abdullakutty F, Akbari Y, Al-Maadeed S, et al. Histopathology in focus: a review on explainable multi-modal approaches for breast cancer diagnosis. Front Med Lausanne. 2024;11:1450103. doi:10.3389/fmed.2024.1450103
122. Qu H, Zhou M, Yan Z, et al. Genetic mutation and biological pathway prediction based on whole slide images in breast carcinoma using deep learning. NPJ Precis Oncol. 2021;5(1):87. doi:10.1038/s41698-021-00225-9
123. Yao Y, Lv Y, Tong L, et al. ICSDA: a multi-modal deep learning model to predict breast cancer recurrence and metastasis risk by integrating pathological, clinical and gene expression data. Brief Bioinform. 2022;23(6):bbac448. doi:10.1093/bib/bbac448
124. Loeffler CML, El Nahhas OSM, Muti HS, et al. Prediction of homologous recombination deficiency from routine histology with attention-based multiple instance learning in nine different tumor types. BMC Biol. 2024;22(1):225. doi:10.1186/s12915-024-02022-9
125. Loeffler CML, El Nahhas OSM, Muti HS, et al. Direct prediction of homologous recombination deficiency from routine histology in ten different tumor types with attention-based multiple instance learning: a development and validation study. medRxiv. 2023. doi:10.1101/2023.03.08.23286975
126. Deng T, Liang J, Yan C, et al. Development and validation of ultrasound-based radiomics model to predict germline BRCA mutations in patients with breast cancer. Cancer Imaging. 2024;24(1):31. doi:10.1186/s40644-024-00676-w
127. Guo R, Yu Y, Huang Y, et al. A nomogram model combining ultrasound-based radiomics features and clinicopathological factors to identify germline BRCA1/2 mutation in invasive breast cancer patients. Heliyon. 2024;10(1):e23383. doi:10.1016/j.heliyon.2023.e23383
128. Shao Z, Yu J, Cheng Y, et al. MR imaging phenotypes and features associated with pathogenic mutation to predict recurrence or metastasis in breast cancer. BMC Cancer. 2023;23(1):97. doi:10.1186/s12885-023-10555-5
129. Bharucha PP, Chiu KE, François FM, et al. Genetic testing and screening recommendations for patients with hereditary breast cancer. Radiographics. 2020;40(4):913–936. doi:10.1148/rg.2020190181
130. Liang S, Xu S, Zhou S, et al. IMAGGS: a radiogenomic framework for identifying multi-way associations in breast cancer subtypes. J Genet Genomics. 2024;51(4):443–453. doi:10.1016/j.jgg.2023.09.010
131. Shen WQ, Guo Y, Ru WE, et al. Using an improved residual network to identify PIK3CA mutation status in breast cancer on ultrasound image. Front Oncol. 2022;12:850515. doi:10.3389/fonc.2022.850515
132. Wang X, Zou C, Zhang Y, et al. Prediction of BRCA gene mutation in breast cancer based on deep learning and histopathology images. Front Genet. 2021;12:661109. doi:10.3389/fgene.2021.661109
133. Guan J, Fan M, Li L. MVNMF: multiview nonnegative matrix factorization for radio-multigenomic analysis in breast cancer prognosis. Med Image Anal. 2025;103:103566. doi:10.1016/j.media.2025.103566
134. Su GH, Xiao Y, Jiang L, et al. Radiomics features for assessing tumor-infiltrating lymphocytes correlate with molecular traits of triple-negative breast cancer. J Transl Med. 2022;20(1):471. doi:10.1186/s12967-022-03688-x
135. Pan D, Zhang CY, Wang YF, et al. Machine learning-based integration of DCE-MRI radiomics for STAT3 expression prediction and survival stratification in breast cancer. Front Immunol. 2025;16:1619186. doi:10.3389/fimmu.2025.1619186
136. Tong H, Sun J, Fang J, et al. A machine learning model based on PET/CT radiomics and clinical characteristics predicts tumor immune profiles in non-small cell lung cancer: a Retrospective Multicohort Study. Front Immunol. 2022;13:859323. doi:10.3389/fimmu.2022.859323
137. Guo Y, Gong B, Li Y, et al. Non-invasive prediction of NSCLC immunotherapy efficacy and tumor microenvironment through unsupervised machine learning-driven CT radiomic subtypes: a multi-cohort study. Int J Surg. 2025;111(10):6592–6603. doi:10.1097/JS9.0000000000002839
138. Han X, Guo Y, Ye H, et al. Development of a machine learning-based radiomics signature for estimating breast cancer TME phenotypes and predicting anti-PD-1/PD-L1 immunotherapy response. Breast Cancer Res. 2024;26(1):18. doi:10.1186/s13058-024-01776-y
139. Qian H, Ren X, Xu M, et al. Magnetic resonance imaging-based radiomics was used to evaluate the level of prognosis-related immune cell infiltration in breast cancer tumor microenvironment. BMC Med Imag. 2024;24(1):31. doi:10.1186/s12880-024-01212-9
140. Gu Y, Huang H, Tong Q, et al. Multi-View radiomics feature fusion reveals distinct immuno-oncological characteristics and clinical prognoses in hepatocellular carcinoma. Cancers. 2023;15(8):2338. doi:10.3390/cancers15082338
141. Jin ZC, Wei J, Xiao YD, et al. Decoding tumor heterogeneity with imaging biomarkers predicts response to TACE plus Immunotherapy and targeted therapy in HCC. Hepatology. 2025. doi:10.1097/HEP.0000000000001593
142. Wang Z, Wang L, Wang Y. Radiomics in glioma: emerging trends and challenges. Ann Clin Transl Neurol. 2025;12(3):460–477. doi:10.1002/acn3.52306
143. Rifi AL, Raets C, Dufait I, De Ridder M, Barbé K. Integrating radiomics and immunology: non-invasive assessment of intratumoral CD8+ T cell levels in murine models. Comput Biol Med. 2025;190:110061. doi:10.1016/j.compbiomed.2025.110061
144. Fan X, Yuan C, Tao J, et al. CSF1R and macrophage infiltration: integrated magnetic resonance imaging radiomics and deep learning-driven models for the preoperative assessment of glioma. Chin Med J. 2025. doi:10.1097/CM9.0000000000003827
145. Lin G, Wang X, Ye H, et al. Radiomic models predict tumor microenvironment using artificial intelligence-the novel biomarkers in breast cancer immune microenvironment. Technol Cancer Res Treat. 2023;22:15330338231218227. doi:10.1177/15330338231218227
146. Ren Q, Xiong F, Zhu P, et al. Assessing the robustness of radiomics/deep learning approach in the identification of efficacy of anti-PD-1 treatment in advanced or metastatic non-small cell lung carcinoma patients. Front Oncol. 2022;12:952749. doi:10.3389/fonc.2022.952749
147. Cheng M, Guo Y, Zhao H, et al. CT-based deep learning radiomics analysis for preoperative Lauren classification in gastric cancer and explore the tumor microenvironment. Eur J Radiol Open. 2025;15:100667. doi:10.1016/j.ejro.2025.100667
148. Kim GR, Ku YJ, Kim JH, et al. Correlation between MR image-based radiomics features and risk scores associated with gene expression profiles in breast cancer. Taehan Yongsang Uihakhoe Chi. 2020;81(3):632–643. doi:10.3348/jksr.2020.81.3.632
149. Sucre A, Calle Sánchez X, Perez-Herrera LV, et al. Multimodal fusion strategies for survival prediction in breast cancer: a comparative deep learning study. Comput Struct Biotechnol J. 2025;27:4505–4516.P. doi:10.1016/j.csbj.2025.10.038
150. Wu X, Dai W. Beyond imaging: integrating radiomics, genomics, and multi-omics for precision breast cancer management. Cancers. 2025;17(21):3408. doi:10.3390/cancers17213408
151. Li X, Yang L, Jiang F, et al. Integration of radiomics and immune-related genes signatures for predicting axillary lymph node metastasis in breast cancer. Clin Breast Cancer. 2025;25(1):e40–e47e4. doi:10.1016/j.clbc.2024.06.014/
152. Zhang T, Zhao L, Cui T, et al. Spatial-temporal radiogenomics in predicting neoadjuvant chemotherapy efficacy for breast cancer: a comprehensive review. J Transl Med. 2025;23(1):681. doi:10.1186/s12967-025-06641-w
153. Davey MG, Davey MS, Boland MR, et al. Radiomic differentiation of breast cancer molecular subtypes using pre-operative breast imaging – A systematic review and meta-analysis. Eur J Radiol. 2021;144:109996. doi:10.1016/j.ejrad.2021.109996
154. Jiang L, You C, Xiao Y, et al. Radiogenomic analysis reveals tumor heterogeneity of triple-negative breast cancer. Cell Rep Med. 2022;3(7):100694. doi:10.1016/j.xcrm.2022.100694
155. Shiri I, Salimi Y, Mohammadi Kazaj P, et al. Deep radiogenomics sequencing for breast tumor gene-phenotype decoding using dynamic contrast magnetic resonance imaging. Mol Imaging Biol. 2025;27(1):32–43. doi:10.1007/s11307-025-01981-x
156. Cè M, Caloro E, Pellegrino ME, et al. Artificial intelligence in breast cancer imaging: risk stratification, lesion detection and classification, treatment planning and prognosis—a narrative review. Explor Target Antitumor Ther. 2022;3(6):795–816. doi:10.37349/etat.2022.00113
157. Wu J, Mayer AT, Li R. Integrated imaging and molecular analysis to decipher tumor microenvironment in the era of immunotherapy. Semin Cancer Biol. 2022;84:310–328. doi:10.1016/j.semcancer.2020.12.005
158. Corr F, Grimm D, Sass B, et al. Radiogenomic predictors of recurrence in Glioblastoma-A systematic review. J Pers Med. 2022;12(3):402. doi:10.3390/jpm12030402
159. Soliman AM. Psychological well-being in breast cancer: a literature review of the impact of precision oncology and radiogenomics. Cureus. 2025;17(8):e91210. doi:10.7759/cureus.91210
160. Zhang Y, Cai J, Cui C, Qi S, Zhao D. Predicting breast cancer response to neoadjuvant therapy by integrating radiomic and deep-learning features from early-and-peak phases of DCE-MRI. BMC Cancer. 2025;25(1):1747. doi:10.1186/s12885-025-15095-8
161. Wang Y, Zheng XD, Zhu GQ, et al. Crosstalk between metabolism and immune activity reveals four subtypes with therapeutic implications in clear cell renal cell carcinoma. Front Immunol. 2022;13:861328. doi:10.3389/fimmu.2022.861328
162. Wang C, Wang C, Zhang J, et al. Development and validation of a radiogenomics prognostic model integrating PET/CT radiomics and glucose metabolism-related gene signatures for non-small cell lung cancer. Eur J Nucl Med Mol Imaging. 2025;52(13):4924–4938. doi:10.1007/s00259-025-07354-4
163. Spielvogel CP, Stoiber S, Papp L, et al. Radiogenomic markers enable risk stratification and inference of mutational pathway states in head and neck cancer. Eur J Nucl Med Mol Imaging. 2023;50(2):546–558. doi:10.1007/s00259-022-05973-9
164. Shukla M, Forghani R, Agarwal M. Patient-Centric head and neck cancer radiation therapy: role of advanced imaging. Neuroimaging Clin N Am. 2020;30(3):341–357. doi:10.1016/j.nic.2020.04.005
165. Chang L, Liu J, Zhu J, et al. Advancing precision medicine: the transformative role of artificial intelligence in immunogenomics, radiomics, and pathomics for biomarker discovery and immunotherapy optimization. Cancer Biol Med. 2025;22(1):33–47. doi:10.20892/j.issn.2095-3941.2024.0376
166. Ahanger AB, Aalam SW, Masoodi TA, et al. Radiogenomics and machine learning predict oncogenic signaling pathways in glioblastoma. J Transl Med. 2025;23(1):121. doi:10.1186/s12967-025-06101-5
167. Dolciami M, Celli V, Panico C, et al. Unraveling tumor heterogeneity in gynecological cancer using a radiogenomics approach. Rofo. 2025. doi:10.1055/a-2698-8545
168. Hu Q, Whitney HM, Giger ML. Radiomics methodology for breast cancer diagnosis using multiparametric magnetic resonance imaging. J Med Imaging. 2020;7(4):044502. doi:10.1117/1.JMI.7.4.044502
169. Alom MR, Farid FA, Rahaman MA, et al. An explainable AI-driven deep neural network for accurate breast cancer detection from histopathological and ultrasound images. Sci Rep. 2025;15(1):17531. doi:10.1038/s41598-025-97718-5
170. Guo Y, Su Z, Koyun OC, et al. BPMambaMIL: a bio-inspired prototype-guided multiple instance learning for oncotype DX risk assessment in histopathology. Comput Methods Programs Biomed. 2025;272:109039. doi:10.1016/j.cmpb.2025.109039
171. Adam R, Dell’Aquila K, Hodges L, et al. Deep learning applications to breast cancer detection by magnetic resonance imaging: a literature review. Breast Cancer Res. 2023;25(1):87. doi:10.1186/s13058-023-01687-4
172. Garrucho L, Kushibar K, Reidel CA, et al. A large-scale multicenter breast cancer DCE-MRI benchmark dataset with expert segmentations. Sci Data. 2025;12(1):453. doi:10.1038/s41597-025-04707-4
173. Carriero A, Groenhoff L, Vologina E, et al. Deep learning in breast cancer imaging: state of the art and recent advancements in early 2024. Diagnostics. 2024;14(8):848. doi:10.3390/diagnostics14080848
174. Bhattacharya S, Saleem SM, Singh A, et al. Empowering precision medicine: regenerative AI in breast cancer. Front Oncol. 2024;14:1465720. doi:10.3389/fonc.2024.1465720
175. Singh A, Paruthy SB, Belsariya V, et al. Revolutionizing breast healthcare: harnessing the role of artificial intelligence. Cureus. 2023;15(12):e50203. doi:10.7759/cureus.50203
176. Ali A, Alghamdi M, Marzuki SS, et al. Exploring AI approaches for breast cancer detection and diagnosis: a review article. Breast Cancer. 2025;17:927–947. doi:10.2147/BCTT.S550307
177. Wu X, Xia Y, Lou X, et al. Decoding breast cancer imaging trends: the role of AI and radiomics through bibliometric insights. Breast Cancer Res. 2025;27(1):29. doi:10.1186/s13058-025-01983-1
178. Wang Z, Li F, Cai J, et al. Identification of lesion bioactivity in hepatic cystic echinococcosis using a transformer-based fusion model. J Infect. 2025;90(4):106455. doi:10.1016/j.jinf.2025.106455
179. Nandakumar N, Manzoor K, Agarwal S, et al. Automated eloquent cortex localization in brain tumor patients using multi-task graph neural networks. Med Image Anal. 2021;74:102203. doi:10.1016/j.media.2021.102203
180. Karthik R, Menaka R, Hariharan M, et al. AI for COVID-19 detection from radiographs: incisive analysis of state of the art techniques, key challenges and future directions. Ing Rech Biomed. 2022;43(5):486–510. doi:10.1016/j.irbm.2021.07.002
181. Jiang X, Sun Q, Wang C, et al. CT-based radiomics and deep learning to predict EGFR mutation status in lung adenocarcinoma. Front Oncol. 2025;15:1597548. doi:10.3389/fonc.2025.1597548/
182. Jiménez-Sánchez D, Ariz M, Chang H, et al. NaroNet: discovery of tumor microenvironment elements from highly multiplexed images. Med Image Anal. 2022;78:102384. doi:10.1016/j.media.2022.102384
183. Ballard JL, Wang Z, Li W, et al. Deep learning-based approaches for multi-omics data integration and analysis. BioData Min. 2024;17(1):38. doi:10.1186/s13040-024-00391-z
184. Choi SR, Lee M. Transformer architecture and attention mechanisms in genome data analysis: a comprehensive review. Biology. 2023;12(7):1033. doi:10.3390/biology12071033
185. Foffano L, Vida R, Piacentini A, et al. Is ctDNA ready to outpace imaging in monitoring early and advanced breast cancer? Expert Rev Anticancer Ther. 2024;24(8):679–691. doi:10.1080/14737140.2024.2362173
186. Hu P, Xu L, Qi Y, et al. Combination of multi-modal MRI radiomics and liquid biopsy technique for preoperatively non-invasive diagnosis of glioma based on deep learning: protocol for a double-center, ambispective, diagnostical observational study. Front Mol Neurosci. 2023;16:1183032. doi:10.3389/fnmol.2023.1183032
187. Cherukuri SP, Kaur A, Goyal B, et al. Artificial intelligence-enhanced liquid biopsy and radiomics in early-stage lung cancer detection: a precision oncology paradigm. Cancers. 2025;17(19):3165. doi:10.3390/cancers17193165
188. Rahdar A, Mhammadzadeh V, Razzaq S, et al. Physics-informed deep learning sharpens nano diagnostics for elusive pancreatic cancer. Semin Oncol. 2025;53(1):152427. doi:10.1016/j.seminoncol.2025.152427
189. Krengli M, Kruszyna-Mochalska MM, Pasqualetti F, et al. Can advances in artificial intelligence strengthen the role of intraoperative radiotherapy in the treatment of cancer? Cancers. 2025;17(19):3124. doi:10.3390/cancers17193124
190. Huang J, Xiang Y, Gan S, et al. Application of artificial intelligence in medical imaging for tumor diagnosis and treatment: a comprehensive approach. Discov Oncol. 2025;16(1):1625. doi:10.1007/s12672-025-03307-3
191. Vaidya A, Chen RJ, Williamson DFK, et al. Demographic bias in misdiagnosis by computational pathology models. Nat Med. 2024;30(4):1174–1190. doi:10.1038/s41591-024-02885-z
192. Castaldo R, Pane K, Nicolai E, Salvatore M, Franzese M. The impact of normalization approaches to automatically detect radiogenomic phenotypes characterizing breast cancer receptors status. Cancers. 2020;12(2):518. doi:10.3390/cancers12020518
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of an MRI Radiomics-Based Signature to Predict Histological Grade in Patients with Invasive Breast Cancer
Wang S, Wei Y, Li Z, Xu J, Zhou Y
Breast Cancer: Targets and Therapy 2022, 14:335-342
Published Date: 14 October 2022
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Bridging the Gap Between Imaging and Molecular Characterization: Current Understanding of Radiomics and Radiogenomics in Hepatocellular Carcinoma
Ren L, Chen DB, Yan X, She S, Yang Y, Zhang X, Liao W, Chen H
Journal of Hepatocellular Carcinoma 2024, 11:2359-2372
Published Date: 27 November 2024
Heterogeneity Assessment of Breast Cancer Tumor Microenvironment: Multiparametric Quantitative Analysis with DCE-MRI and Discovery of Radiomics Biomarkers
Ma W, Yang L, Zhang Y, Gao Y, Jie H, Huang C
Breast Cancer: Targets and Therapy 2025, 17:573-581
Published Date: 8 July 2025
Development and Validation of Machine Learning Models in Predicting Prognosis of Breast Cancer Patients with Lymph Nodes Metastasis Following Neoadjuvant Chemotherapy
Fan Y, Jin Y, Tian C, Zhang Y, Zhang C, Yu H, Liu S
Breast Cancer: Targets and Therapy 2025, 17:883-896
Published Date: 30 September 2025