Back to Journals » Journal of Pain Research » Volume 15
Radiofrequency Ablation for the Knee Joint: A Survey by the American Society of Pain and Neuroscience
Authors Abd-Elsayed A, Strand N ![]() , Gritsenko K
, Gritsenko K ![]() , Martens J, Chakravarthy K, Sayed D
, Martens J, Chakravarthy K, Sayed D ![]() , Deer T
, Deer T ![]()
Received 29 December 2021
Accepted for publication 14 April 2022
Published 27 April 2022 Volume 2022:15 Pages 1247—1255
DOI https://doi.org/10.2147/JPR.S342653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Alaa Abd-Elsayed,1 Natalie Strand,2 Karina Gritsenko,3 Joshua Martens,1 Krishnan Chakravarthy,4 Dawood Sayed,5 Timothy Deer6
1University of Wisconsin, School of Medicine and Public Health, Department of Anesthesiology, Madison, WI, USA; 2Division of Pain Medicine, Mayo Clinic, Phoenix, AZ, USA; 3Montefiore Multidisciplinary Pain Program, Bronx, NY, USA; 4University of California San Diego, San Diego, CA, USA; 5University of Kansas Medical Center, Kansas City, KS, USA; 6The Spine and Nerve Center of the Virginias, Charleston, WV, USA
Correspondence: Alaa Abd-Elsayed, University of Wisconsin School of Medicine and Public Health, Department of Anesthesiology, 600 Highland Avenue, B6/319 CSC, Madison, WI, 53792-3272, USA, Tel +1 608-263-8100, Fax +1 608-263-0575, Email [email protected]
Background: Genicular nerve radiofrequency ablation (RFA) is an effective, minimally invasive procedure often used to treat patients with intractable knee pain secondary to knee osteoarthritis and failed knee replacements. The prevalence of knee pain in adults has been estimated to be as high as 40% and is continuously increasing with an aging population. Over the past two decades, proceduralists have adopted variations in patient preparation, procedural steps, and post-operative care for genicular nerve RFA procedures. A survey was dispensed via the American Society of Pain and Neuroscience (ASPN) to gain a popular assessment of common practices for genicular nerve RFA.
Methods: A 29 question survey was dispensed via SurveyMonkey to all members of ASPN. Members were able to respond to the survey a single time and were unable to make changes to their responses once the survey was submitted. After responses were compiled, each question was assessed in order to determine common practices for genicular nerve RFA.
Results: A total of 378 proceduralists responded to the survey. There was high consensus with the three most commonly targeted nerves. The inferomedial, superomedial, and superolateral genicular branches were treated by 95– 96% of respondents, while other targets were less commonly treated. There remains some debate among proceduralists regarding the need for a second diagnostic nerve block and the type of steroid used for diagnostic nerve blocks.
Conclusion: Pain physicians use a wide variety of methods to perform genicular nerve ablations. The data offered by the survey show that there is no standardized protocol when it comes to treating knee pain via genicular nerve block and ablation and highlights controversies among proceduralists that ought to serve as the targets of future clinical research aimed at establishing a standardized protocol.
Keywords: genicular nerve ablation, knee radiofrequency ablation, genicular nerve survey, genicular nerve block, radiofrequency ablation
Introduction
Genicular nerve radiofrequency ablation is a minimally invasive procedure that is often used to treat patients with intractable knee pain secondary to knee osteoarthritis (OA) and failed knee replacements.1 Knee OA represents one of the most common joint diseases in adults, with a prevalence as high as 40% in adults between the ages of 70 and 75, and remains one of the leading causes of pain and disability in elderly populations.2,3 Overall, the prevalence of knee pain, independent of age and BMI has increased substantially over the past few decades, nearly doubling among women and tripling among men over a 20-year period.4 Genicular nerve ablation offers an effective, low risk alternative for patients who have failed conservative treatment of their knee pain, such as weight loss, physical therapy, and pharmacotherapy, who may not be good surgical candidates or may prefer to avoid surgery.1 The procedure has been shown to offer patients effective pain relief along with improvements in quality of life, daily function, and patient satisfaction, with a low risk of serious side effects.2 A recent retrospective study conducted by Iannaccone et al found that, on average, genicular nerve ablation offers patients with intractable knee pain 60% pain relief lasting for as long as 6 months.5
Over the past two decades, proceduralists have adopted variations in patient preparation, procedural steps, and post-operative care for genicular nerve ablations. These variations include, but are not limited to, the types of imaging guidance used during electrode placement, the use of diagnostic nerve blocks along with the type of nerve block used, the type of ablation, and the type of cannula used in procedural approach. While there is a growing breadth of literature investigating differences in effectiveness for certain approaches, the impact on variation across proceduralists remains poorly understood. There are very little data available on which variations are most common and whether a plurality of proceduralists conduct genicular nerve ablations a certain way.6–8 To gain a popular assessment of the common practices of genicular nerve ablation in the modern interventional pain world and to identify areas in clinical practice that lack consensus as potential targets of future research, a 29 question survey was dispensed via the American Society of Pain & Neuroscience (ASPN) with anonymous responses compiled by a database.
Methods
This research was completed using a survey developed by the American Society of Pain and Neuroscience (ASPN) using expert opinion. Several society members with expertise in developing surveys participated in drafting and finalizing the questionnaire. The survey contained all elements of voluntary informed consent. The survey consisted of 29 questions that aimed to address the respondent’s demographics, background in pain medicine, clinical practice, procedure details, and post-procedure details. Questions were presented in multiple-choice format; however, respondents were offered an “other” or “NA” selection, when applicable, and permitted to free-text a response. A multilingual survey for respondents outside of the US was not used. The survey was administered via SurveyMonkey to all members of ASPN. In order to receive the survey, members needed to have a valid email on file with the society. The survey was delivered via email to all members with an email on file with ASPN on three separate occasions. Survey invitations were sent on May 10, May 14, and the survey was closed on May 18, 2021.
Members were able to respond to the survey a single time only. Once members submitted the survey, they were unable to make additional edits to their responses. Members of ASPN who answered any question within the survey were documented as respondents. Instances where members of ASPN responded to at least one question in the survey, but did not respond to all questions, were marked as “skipped” for the questions that lacked a response. Once the survey was closed, all responses were compiled for data analysis. Members who had started the survey but did not submit their responses were excluded from data analysis. ASPN members who took part in the survey design did not participate in the study.
After responses were compiled from SurveyMonkey, data was extracted into an Excel file and analyzed on a question-by-question basis. Questions were stratified into four buckets: provider demographics, pre-procedure details, procedure details, and post-procedure details. The total count of responses from each question within each bucket was then summarized into tables for review (Tables 1–4). Each question was assessed by the total number of respondents who answered the question, the total number of respondents who skipped the question, and the percent of total respondents who selected each answer within the question. The data was summarized into a series of tables, which demonstrate the total number of respondents who selected each response per each question. This article received an IRB exemption from the University of Wisconsin in Madison as the survey was anonymous and did not include any patient subjects. The study was conducted in accordance with the principles embodied in the Declaration of Helsinki. All study participants provided consent for the use of their responses in the research study.
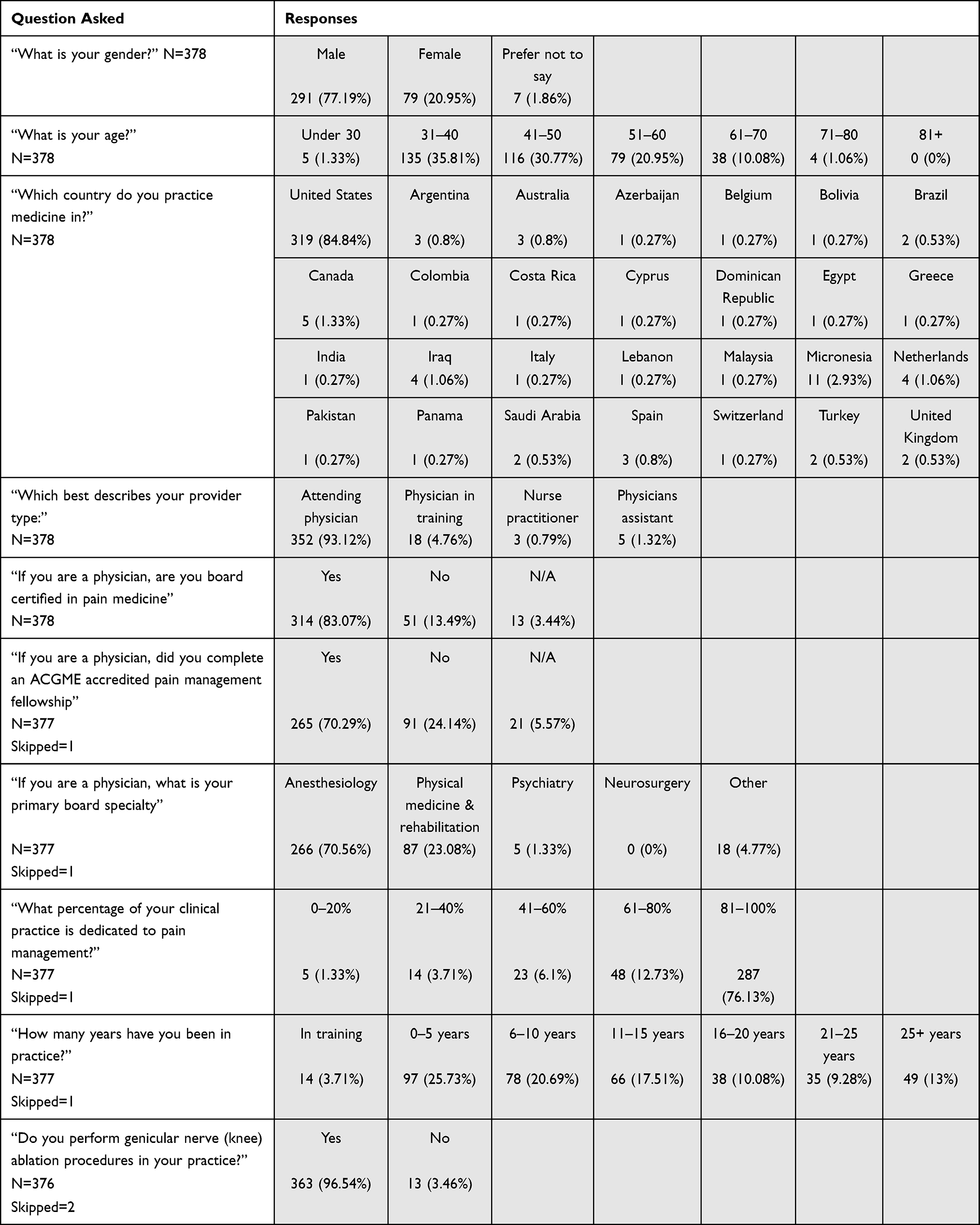 |
Table 1 Provider Demographics |
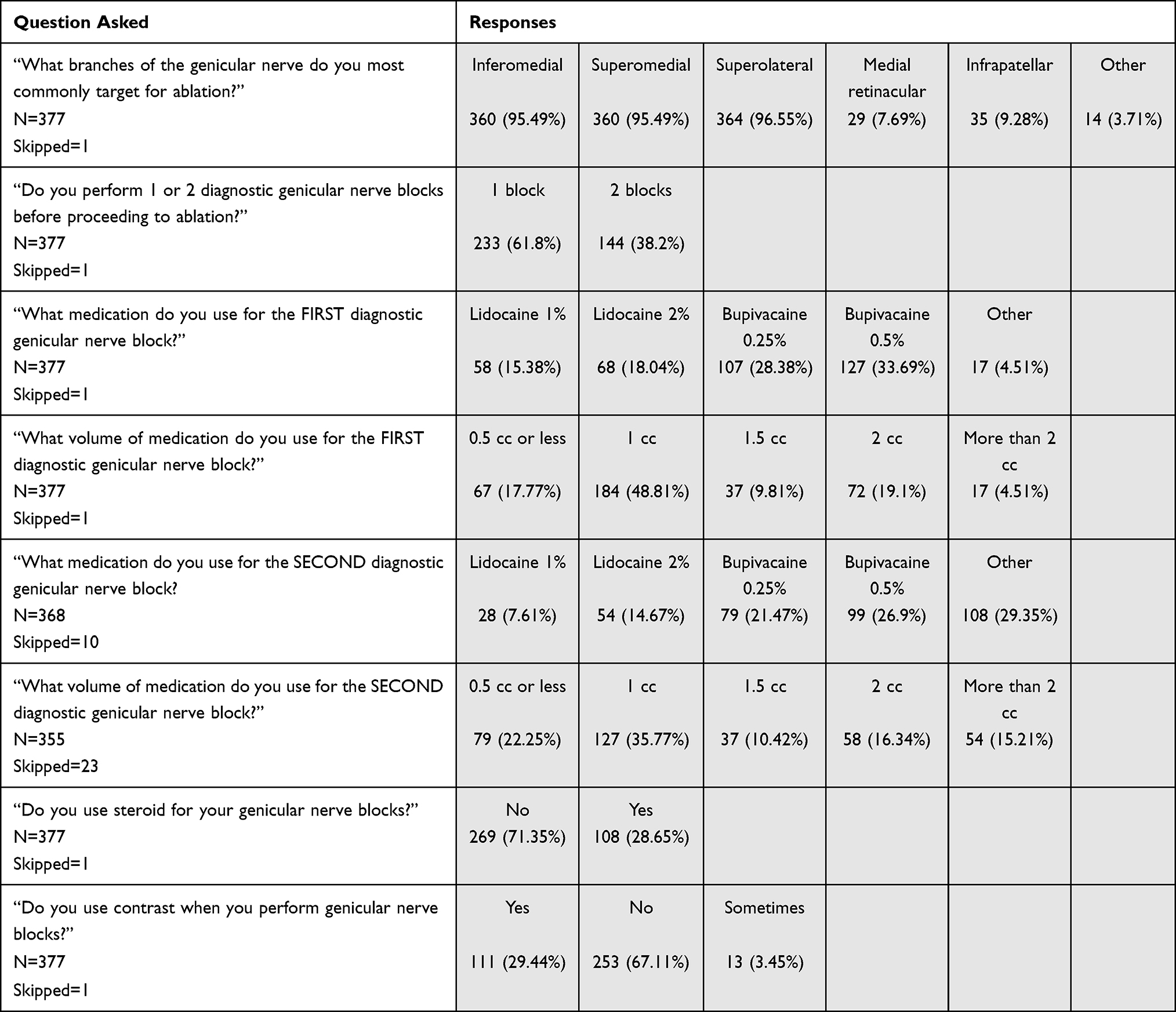 |
Table 2 Pre-Procedure Details |
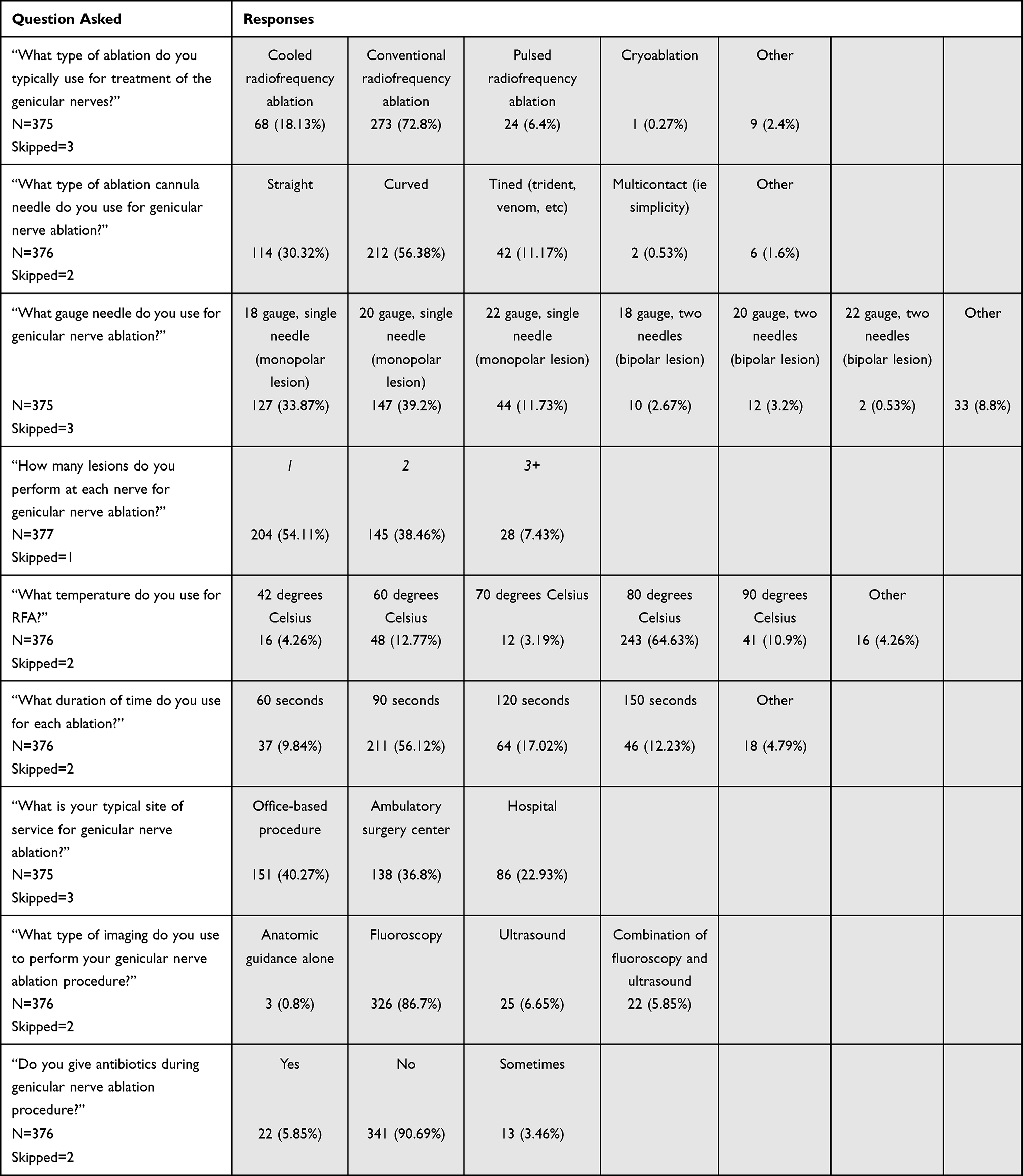 |
Table 3 Procedure Details |
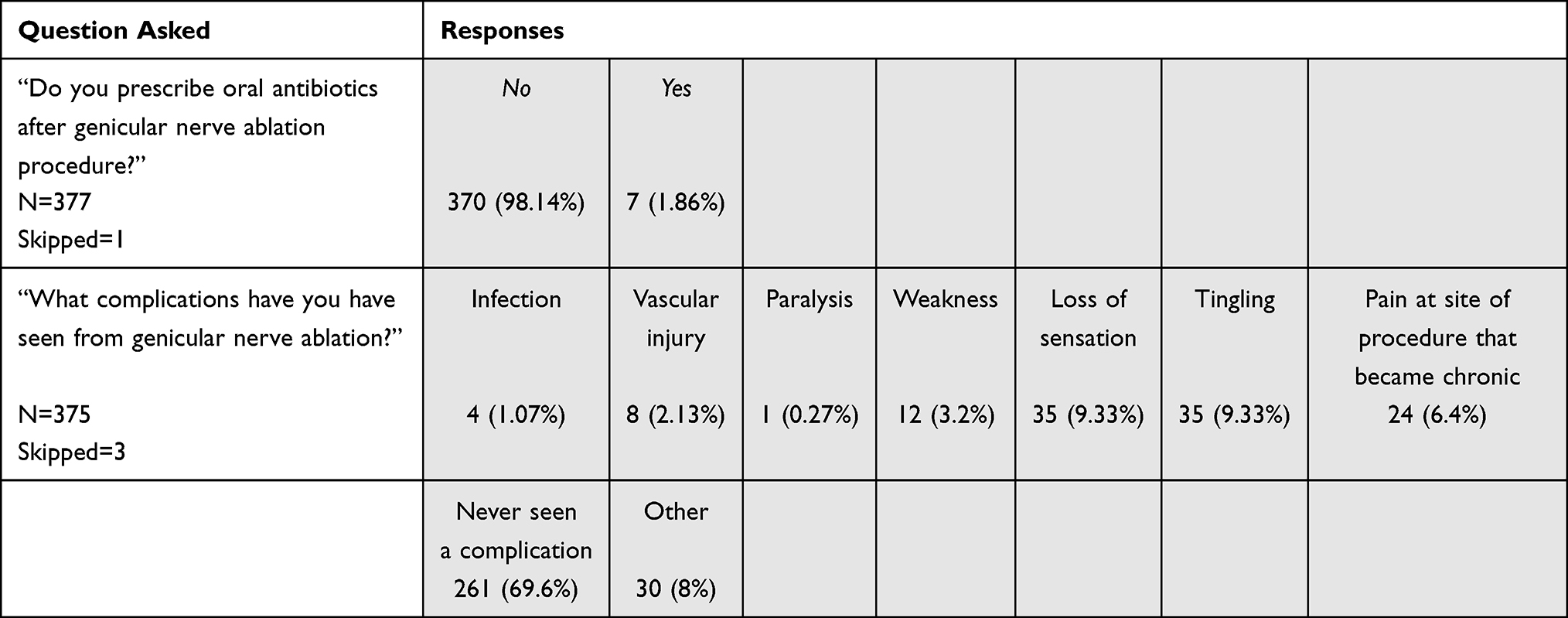 |
Table 4 Post-Procedure Details |
Results
The survey was sent to a total of 4515 recipients; however, only 40% opened the email. Our response rate is estimated to be 21%. Per question response rates varied between 93.9% and 100%. Respondents were broadly representative of pain providers in terms of age and years in practice. The majority of respondents were between the ages of 31 and 50 and ages 51 and 70 (Table 1). A large majority of respondents were attending physicians, while the remainder were physicians in training and physician assistants (Table 1). Most respondents were board certified physicians and were Accreditation Council for Graduate Medical Education (ACGME) fellowship trained (Table 1). A larger proportion of respondent pain providers were male than were female (Table 1). Seven respondents preferred not to provide their gender. The majority of respondents had a training background of anesthesiologists, followed by physiatrists (Table 1). A small number of neurologists and single psychiatrist were represented in the respondent pool. The majority of survey respondents dedicated more than 80% of their clinical care to chronic pain medicine, while smaller numbers of respondents dedicated 61–80% or less than 60% of their clinical care to chronic pain medicine (Table 1). Survey respondents covered a wide range when it came to length of practice. A slight majority of respondents had 10 years of training or less, while smaller, but comparable, numbers of respondents had between 11 and 20 years of training or 21 years of training of more (Table 1). Survey participants were primarily from the United States; however, the survey responses did include global representation. Survey participants also represented Canada, Mexico, Europe, South America, Asia, and Australia (Table 1). When it came to the site of service for respondents, most providers conducted procedures in an office-based setting, though a comparable number were conducted in an ambulatory surgery center, and a smaller proportion were hospital based (Table 1).
When it came to clinical practice experience, nearly all of respondents performed genicular nerve ablations in their practice. A similar, large majority performed both inferomedial and superomedial ablations as well as performed superolateral ablations, and a minority of respondents performed medial retinacular and infrapatellar respondents (Table 2). Prior to undergoing the RFA procedure, a slight majority of respondents perform 1 diagnostic genicular block, with a comparable, but smaller subset perform 2 diagnostic genicular nerve blocks (Table 2). In order to perform the first diagnostic nerve block, about 1/3 of respondents used lidocaine 1% or 2% and the remaining 2/3 used bupivacaine 0.25% or 0.5% (Table 2). When it came to the volume of medication used for the first diagnostic block, the majority of respondents used 1 cc of below (Table 2). There were smaller, but considerable numbers of respondents who use 2 or more cc or 1.5 cc (Table 2). There were comparable discrepancies between proceduralists for the second diagnostic nerve block, with about ¼ using lidocaine 1% or 2% and ½ using bupivacaine 0.25% or 0.5% (Table 2). In terms of volume of medication for the second diagnostic nerve block, over half of respondents used 1 cc or less, while smaller proportions used 2 or more cc or 1.5cc. The majority of survey respondents do not use steroids and do not use contrast (Table 2).
When performing the RFA procedure, a wide majority of respondents used fluoroscopic guidance, followed by a small minority who used ultrasound or a combination of fluoroscopy and ultrasound, and an even smaller minority who used anatomic guidance alone, with no imaging (Table 3). Along with differences in the time of imaging guidance used, there was some variability in the techniques used in clinical practice. The majority of ablation techniques in clinical practice of those surveyed were conventional radiofrequency (Table 3). Cooled radiofrequency ablation was used in practice, and a minority of practitioners use pulsed radiofrequency ablation (Table 3). One person reported use of cryoablation. Majority of ablation cannula needles used for genicular nerve ablation are curved needles, followed by straight needles (Table 3). Smaller proportions of respondents use Tined – Trident/Venom, Simplicity 0.53%, and “other” types of cannula (Table 3). It is relevant to note that there are new techniques that may come to the market that would change the distribution of these data in the future. The majority of practitioners who responded to the survey reported the use of a single needle, monopolar lesion (Table 3). Less than 6% of practitioners prefer a bipolar, 2 needle approach to ablation. Additionally, the majority of practitioners report 1 lesion at each nerve for the ablation, compared to 2 lesions (Table 3). Only 7.41% of survey responses preferred 3 or more lesions.
The preferred temperature for lesioning was found to be 80 degrees Celsius (Table 3). This was followed by 60 degrees Celsius and 90 degrees Celsius (Table 3). The most common ablation time for each ablation was 90 seconds (Table 3). Smaller numbers of respondents completed 120 seconds, 150 seconds, and 60 seconds (Table 3). A large majority of practitioners did not provide antibiotics during nerve ablation procedures and a similar, large majority did not prescribe oral antibiotics following ablation procedures (Table 4). The majority of practitioners have not seen a complication, but complications that were reported by this survey include loss of sensation, tingling, pain at the site of procedure that became chronic, weakness, vascular injury, and infection (Table 4).
Discussion
Genicular Nerve (Knee) ablation is a growing procedure in the field of pain medicine for treatment of chronic knee pain. We surveyed 378 physicians to determine the variable practices when performing genicular nerve ablations in their practices. There is high consensus with the three most commonly targeted nerves, the inferomedial, superomedial, and superolateral genicular branches treated by 95–96% of responders. However, a substantial number of physicians also target the medial retinacular nerve (7.7%) and the infrapatellar nerve (9.3%). This is consistent with emerging knowledge of the innervation of the anterior knee joint. There are 10 nerves that innervate this region, and traditional ablation of the genicular nerves only capture 3 of them.9
There is some debate about the need for a second diagnostic genicular nerve block after one successful block. This is reflected in the results with 61.8% of physicians performing 1 diagnostic block, and 38.2% performing 2 diagnostic blocks. The usefulness of even one diagnostic block is debated in the literature as one study revealed over 80% of patients who had diagnostic blocks performed ended up responding to genicular ablation at the one month mark.10 With such a high amount of responders, the need for a diagnostic block prior to ablation is controversial. In our survey, all responders perform a diagnostic block, but there is significant variability in the type of local anesthetic used. The first block is performed with 0.5% Bupivacaine most of the time, but 0.25% bupivacaine, 1% lidocaine and 2% lidocaine are all commonly used. With no second block planned the majority of the time, there is no limited usefulness of a long acting local anesthetic compared to a short acting local anesthetic for prognostic value. The most commonly used dose for each diagnostic block is 1mL, but there is significant variability from 0.5m to 2mL. The risks and benefits of certain anesthetics used for blocks, as well as the dosage of blocks, represent an area of variability among proceduralists that should be further investigated with randomized control trials. While previous research has investigated the use of local anesthetic alone compared to local anesthetic with corticosteroids, there is no standardized recommendation for local anesthetic type or injectate volume. A comparison of the types of anesthetic as well as the dosage used for these nerve blocks should be conducted.
We continue to see variation when looking at the number of responders who use steroid for genicular nerve blocks, with a significant yet minority of responders using steroid. 71.4% use local anesthetic only. A randomized control study conducted by Kim et al found no clear clinic benefit of corticosteroid administration with local anesthetic compared to local anesthetic alone for genicular nerve blocks; however, the presence of a substantial minority of proceduralists who use steroids may justify additional case reports and randomized control trials on this topic.6 The variability in practice continues in use of contrast, as 29% of physicians use contrast for genicular nerve blocks, and 67% do not use contrast. While rare, vascular injury has been reported after placing needles for genicular nerve blocks and/or ablation.11 Kim et al reviewed the literature published involving genicular artery injuries and found that 40% of the time the medial superior genicular artery was involved, 33% of the time the medial inferior geniculate artery was involved, and 26% of the time the lateral superior genicular artery was involved.12 The use of contrast may aid in diagnosing a vascular injury early. Consistent with previous findings discussed by McCormick and Sperry, the results of this study indicate that there is no singular genicular prognostic block protocol in either volume, type of local anesthetic, inclusion of steroid, or use of contrast or number of blocks among proceduralists.13 These discrepancies should be further investigated by clinical researchers in order to help establish a standardized protocol for prognostic nerve blocks.
When respondents perform the actual genicular nerve ablation for knee pain, the majority of the time conventional RFA is utilized (72.8%). Cooled radiofrequency ablation creates a larger lesion size via internal cooling.14 This is quite a desirable feature given the variation in genicular nerve anatomy, but there is more research needed about any difference in efficacy.9 The significant cost may explain why only 18.1% of responders report using this technology. Pulsed radiofrequency ablation is used 6.4% of the time. Gupta et al performed a systematic review to evaluate the effectiveness of cooled versus pulsed radiofrequency ablation and after reviewing 17 publications determined that there was only low-level evidence suggesting the use of any one ablation technique is better than another.15 In addition to type of ablation, we see diversity in needle gauge, number of lesions at each nerve, temperature setting, and duration of lesion. To date, no meta analysis has been conducted to compare the efficacy of genicular RFA by any of these data points. The variations between proceduralists within each of these areas, compounded by the fact that proceduralists show further variation in the combinations of needle gauge, number of lesions, temperature settings, and duration of lesions, reveal a need for further clinical research to compare the efficacy of each of these variables and protocols. By comparing the different needle gauges, number of lesions, temperatures, and duration of lesions commonly used in these procedures, clinical research might help to establish a standardized protocol in the future.
We found that the majority of physicians (86.7%) use fluoroscopy alone for this procedure. Approximately 12% of all physicians surveyed use ultrasound with or without fluoroscopy when performing this procedure. A small number of physicians use ultrasound guidance alone. Fluoroscopy and ultrasound each have benefits for use in this procedure. Kim et al sought to evaluate any differences in the efficacy of ultrasound guided and fluoroscopically guided genicular nerve ablations.7 Eighty patients were randomly assigned to have ultrasound or fluoroscopic guidance for this procedure. Ultimately, pain relief, functional improvement, and safety were similar between the two groups and the authors concluded that both imaging techniques were safe and effective.7 Huang et al performed a systematic review and meta-analysis to study the efficacy and safety of ultrasound guided radiofrequency ablation for knee pain and determined that ultrasound was safe and effective.16 In addition, they noted the benefits of reduced radiation and low barriers to use and application.16 El-Hakeim performed a single-blind randomized control trial to study the ability of fluoroscopically guided knee ablations to reduce pain. They concluded that ablation with fluoroscopic guidance was both safe and effective for reducing knee pain in patients with chronic knee osteoarthritis.17 Ultrasound imaging has been proposed for its ability to identify vascular structures and allow the pain medicine interventionalist to avoid insulting major blood vessels.11 In addition, ultrasound technology is less expensive and avoids radiation exposure. Fluoroscopic imaging has been proposed for visualization of bony landmarks for radiofrequency needle placement to target the intended genicular nerves.12 Although the literature tells us fluoroscopy and ultrasound each have benefits for users. Our results suggest that there is an overwhelming preference of physicians to use fluoroscopy. This may be explained as simply as pain physicians have more training with and are more comfortable performing these procedures under fluoroscopic guidance; however, the potential cost savings of the use of ultrasound guidance over fluoroscopy should not be ignored. Evidence shows that both visualization techniques are effective and safe; however, a further investigation into underlying drivers of physician preference should be conducted.
Limitations
The results of the survey are limited by the low response rate (21% of total respondents). While overall the respondent pool represents a diverse mix of proceduralists, the limited response rate exposes the survey to the possibility of response bias. The potential biases of those who did not respond were unable to be analyzed, given the inability to obtain responses from these proceduralists. While the majority of respondents were from the United States, representing the largest demographic discrepancy among respondents, the responses from proceduralists outside the United States were consistent with the variation present among those respondents from the US.
Conclusion
The results of the survey demonstrate that there is considerable variability among pain proceduralists in performing genicular nerve ablations. The data provided by this survey highlight commonly used approaches for genicular nerve RFA as well as controversies among proceduralists that ought to guide further investigation by clinical research.
Areas of Future Research
Future research should explore potential discrepancies between genicular nerve ablation practices of proceduralists outside of the United States. While this survey included respondents from a diverse array of countries outside the US, the vast majority of respondents were from the United States, limiting the ability to assess the practices of global proceduralists at a level of statistical significance. It is also critical that future research continues to assess for statistically significant benefits of using certain types of ablation, needle gauges, number of lesions, and duration of lesions. While some techniques are preferred by a majority of proceduralists, the results of this study identify areas of practice that lack a consensus among proceduralists. Additionally, future research investigating risks and benefits of the type and dosage of anesthetic used in genicular nerve blocks prior to procedure should be undergone. It is important for future research to evaluate these areas of variability to determine if certain techniques might provide greater benefit to patients. Additionally, future surveys and investigation should be conducted to evaluate similar preferences among proceduralists for other nerve ablation targets.
Disclosure
Dr Karina Gritsenko is consultant for Avanos and Pacira. Dr Krishnan Chakravarthy reports Consultant to Biotronik, Bioventus, Mainstay Medical, Medtronic, SI Bone, Vertos Medical, Vivex Biologics. Dr Krishnan Chakravarthy reports consultant to Biotronik, Bioventus, Mainstay Medical, Medtronic, SI Bone, Vertos Medical, and Vivex Biologics. Dr Dawood Sayed reports personal fees from Medtronic and Abbott, outside the submitted work. Dr Timothy Deer reports grants and travel from American Society of Pain and Neuroscience, during the conduct of the study; personal fees for consultant from Abbott and research funding from Avanos, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Kidd VD, Strum SR, Strum DS, Shah J. Genicular nerve radiofrequency ablation for painful knee arthritis: the why and the how. JBJS Essent Surg Tech. 2019;9(1):e10. doi:10.2106/JBJS.ST.18.00016
2. Konya ZY, Akin Takmaz S, Başar H, Baltaci B, Babaoğlu G. Results of genicular nerve ablation by radiofrequency in osteoarthritis-related chronic refractory knee pain. Turk J Med Sci. 2020;50(1):86–95. doi:10.3906/sag-1906-91
3. van Saase JL, van Romunde LK, Cats A, Vandenbroucke JP, Valkenburg HA. Epidemiology of osteoarthritis: Zoetermeer survey. Comparison of radiological osteoarthritis in a Dutch population with that in 10 other populations. Ann Rheum Dis. 1989;48(4):271–280. doi:10.1136/ard.48.4.271
4. Nguyen US, Zhang Y, Zhu Y, Niu J, Zhang B, Felson DT. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: survey and cohort data. Ann Intern Med. 2011;155(11):725–732. doi:10.7326/0003-4819-155-11-201112060-00004
5. Iannaccone F, Dixon S, Kaufman A. A review of long-term pain relief after genicular nerve radiofrequency ablation in chronic knee osteoarthritis. Pain Physician. 2017;20(3):E437–E444. doi:10.36076/ppj.2017.E444
6. Kim DH, Choi SS, Yoon SH, et al. Ultrasound-guided genicular nerve block for knee osteoarthritis: a double-blind, randomized controlled trial of local anesthetic alone or in combination with corticosteroid. Pain Physician. 2018;21(1):41–52.
7. Kim DH, Lee MS, Lee S, Yoon SH, Shin JW, Choi SS. A prospective randomized comparison of the efficacy of ultrasound- vs fluoroscopy-guided genicular nerve block for chronic knee osteoarthritis. Pain Physician. 2019;22(2):139–146.
8. McCormick ZL, Korn M, Reddy R, et al. Cooled radiofrequency ablation of the genicular nerves for chronic pain due to knee osteoarthritis: six-month outcomes. Pain Med. 2017;18(9):1631–1641. doi:10.1093/pm/pnx069
9. McCormick ZL, Cohen SP, Walega DR, et al. Technical considerations for genicular nerve radiofrequency ablation: optimizing outcomes. Reg Anesth Pain Med. 2021;46:518–523. doi:10.1136/rapm-2020-102117
10. Santana Pineda MM, Vanlinthout LE, Moreno Martín A, et al. Analgesic effect and functional improvement caused by radiofrequency treatment of genicular nerves in patients with advanced osteoarthritis of the knee until 1 year following treatment. Reg Anesth Pain Med. 2017;42:62–68. doi:10.1097/AAP.0000000000000510
11. Strand N, Jorge P, Freeman J, D’Souza RS. A rare complication of knee hematoma after genicular nerve radiofrequency ablation. Pain Rep. 2019;4(3):e736. doi:10.1097/PR9.0000000000000736
12. Kim SY, Le PU, Kosharskyy B, Kaye AD, Shaparin N, Downie SA. Is genicular nerve radiofrequency ablation safe? A literature review and anatomical study. Pain Physician. 2016;19(5):E697–E705.
13. McCormick ZL, Sperry BP. Genicular nerve blocks: field tips on prognostic value and technical considerations. Pract Pain Manag. 2020;20(6):518–523.
14. Cosman ER, Dolensky JR, Hoffman RA. Factors that affect radiofrequency heat lesion size. Pain Med. 2014;15:2020–2036. doi:10.1111/pme.12566
15. Gupta A, Huettner DP, Dukewich M. Comparative effectiveness review of cooled versus pulsed radiofrequency ablation for the treatment of knee osteoarthritis: a systematic review. Pain Physician. 2017;20(3):155–171. doi:10.36076/ppj.2017.171
16. Huang Y, Deng Q, Yang L, et al. Efficacy and safety of ultrasound-guided radiofrequency treatment for chronic pain in patients with knee osteoarthritis: a systematic review and meta-analysis. Pain Res Manag. 2020;2020:2537075. doi:10.1155/2020/2537075
17. El-Hakeim EH, Elawamy A, Kamel EZ, et al. Fluoroscopic guided radiofrequency of genicular nerves for pain alleviation in chronic knee osteoarthritis: a single-blind randomized controlled trial. Pain Physician. 2018;21(2):169–177.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.