Back to Journals » Nature and Science of Sleep » Volume 18

Racial Differences in Self-Reported Sleep Continuity Disturbance, Problem Endorsement, and Daytime Dysfunction Among Black and White Non-Hispanic Adults in the United States
Authors Thompson MG ![]() , Boyle JT, Muench A
, Boyle JT, Muench A ![]() , Lampe EW, Chung D
, Lampe EW, Chung D ![]() , Grandner MA
, Grandner MA ![]() , Jemmott III JB, Seixas AA
, Jemmott III JB, Seixas AA ![]() , Jean-Louis G
, Jean-Louis G ![]() , Perlis ML
, Perlis ML ![]()
Received 10 April 2025
Accepted for publication 30 September 2025
Published 21 February 2026 Volume 2026:18 530373
DOI https://doi.org/10.2147/NSS.S530373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Michelle G Thompson,1 Julia T Boyle,2– 4 Alexandria Muench,5 Elizabeth W Lampe,6 Debbie Chung,7 Michael A Grandner,8 John B Jemmott III,9,10 Azizi A Seixas,7,11 Girardin Jean-Louis,7 Michael L Perlis10,12,13
1Department of Community and Global Health, College of Health, Lehigh University, Bethlehem, PA, USA; 2Office of Research and Development, VA Boston Healthcare System, Boston, MA, USA; 3New England Geriatric Research Education and Clinical Center, VA Boston Healthcare System, Boston, MA, USA; 4Department of Psychiatry, Harvard Medical School, Boston, MA, USA; 5Hematology-Oncology, Penn Medicine, Princeton Health, Plainsboro, NJ, USA; 6Center for Weight, Eating and Lifestyle Sciences, Department of Psychological and Brain Sciences, Drexel University, Philadelphia, PA, USA; 7Center for Translational Sleep & Circadian Sciences, Department of Psychiatry & Behavioral Sciences, University of Miami Miller School of Medicine, Miami, FL, USA; 8Sleep and Health Research Program, Department of Psychiatry, University of Arizona College of Medicine, Tucson, AZ, USA; 9Annenberg School for Communication, University of Pennsylvania, Philadelphia, PA, USA; 10Department of Psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 11Department of Informatics and Health Data Science, University of Miami Miller School of Medicine, Miami, FL, USA; 12Behavioral Sleep Medicine Program, Department of Psychiatry, University of Pennsylvania, Philadelphia, PA, USA; 13Chronobiology and Sleep Institute, Department of Medicine, University of Pennsylvania, Philadelphia, PA, USA
Correspondence: Michelle G Thompson, Department of Community and Global Health, Lehigh University, 124 E Morton Street, Suite #155, Bethlehem, PA, 18015, USA, Tel +1 610-758-1806, Email [email protected]
Background: Few studies have assessed sleep across all sleep continuity variables (eg, sleep latency [SL], number of awakenings [NWAK], wake after sleep onset [WASO], early morning awakenings [EMA], total sleep time [TST], total wake time [TWT]) concurrently, at the community level, leading to gaps in understanding racial sleep disparities. Moreover, many studies do not examine sleep-related problem endorsement and daytime function.
Purpose: To examine race differences in insomnia symptom severity (eg, sleep continuity disturbance [SCD]), problem endorsement, and daytime dysfunction among Black and White non-Hispanic adults.
Participants and Methods: Participants (N=8172) living in Greater Philadelphia completed an online community survey about their sleep between 2011 and 2021. Chi-square and t-test analyses were used to compare sleep-related differences by race. Multiple regression analyses were conducted to investigate the effect of race on sleep, controlling for age, sex, BMI, and education.
Results: Black non-Hispanics had significantly worse SL (Δ> 3 min), WASO (Δ> 8.4 min), and TWT (Δ > 12.1 min) but not NWAK (Δ< 0.4). Black non-Hispanics also reported substantially lower TST (Δ> 36.8 min). Appreciable effect sizes ranged from .01 to .44. White non-Hispanics consistently endorsed greater daytime dysfunction with small effects ranging from .07 to .14.
Conclusion: Findings suggest that Black non-Hispanics experience less restorative sleep, which can lead to impaired cognitive function, mood disturbances, and increased risk of chronic illness. Observed differences in TST may be due to the unmeasured effects of EMA or to reduced time in bed, underscoring the importance of comprehensive approaches to understanding sleep disturbances like insomnia. Addressing insomnia severity using multidimensional approaches and with targeted interventions, such as Cognitive Behavioral Therapy for Insomnia and/or systematic sleep extension, could help improve sleep health. Moreover, examining differences in sleep across sociodemographic characteristics leads to nuanced understandings that highlight the importance of developing targeted, precision-based behavioral health interventions.
Keywords: insomnia, sleep differences, sleep quality, sleep health disparities, Black or African Ancestry
Introduction
At the epidemiologic level, race and ethnicity are frequently associated with poor sleep among individuals living in the United States.1–6 Racial and ethnically minoritized individuals are more than twice as likely to suffer from sleep disturbances, with Black/African Americans experiencing some of the worst sleep.7–9 Yet comparatively little attention has been paid to the evaluation of racial and ethnic differences in insomnia illness profiles like sleep continuity disturbance (SCD),10,11 as few consider the full spectrum of variables that define sleep continuity (eg, sleep onset latency [SL], number of awakenings [NWAK], wake-after-sleep-onset [WASO], early morning awakenings [EMA], total sleep time [TST], and sleep efficiency [SE%]). Moreover, many studies, if any, concurrently assess sleep continuity, problem endorsement, and sleep-related daytime function.
Importantly, race as a socially conceptualized category used in the United States and based on phenotypic presentation, is not the driving factor for sleep health. Historically discriminatory actions and/or policies based on race are what result in severely consequential psychosocial and environmental determinants that drive disparate sleep health outcomes.12,13 Individuals most strongly impacted are Black/African Americans, as Black/African Americans (henceforth referred to as “Blacks”) are often overrepresented in health disparities overall and in sleep health disparities, in particular.10,14 Therefore, it stands to reason that assessing differences in sleep continuity, problem endorsement, and sleep-related daytime function empirically may provide important insight into conceptualizing insomnia and SCD differences across racial and ethnic groups, and more importantly, how these issues are assessed and treated in underrepresented populations in general and among Blacks specifically. Moreover, while objectively measuring sleep, such as in polysomnography (PSG; the gold standard), may provide a more precise estimation of individual sleep patterns, assessing sleep continuity and quality via self-report is equally important in understanding sleep. Subjective measures may capture subtle nuances in sleep that other methods cannot detect, and these differences may be significantly associated with health outcomes.15,16 The following section provides a brief overview of subjectively measured differences in sleep continuity, sleep continuity problem endorsement, and sleep-related daytime function.
In a scoping review by Ahn et al,10 only 45 studies examined one or more sleep continuity variables. Of these studies, only two provided a full complement of the primary sleep continuity variables (ie, SL, WASO, and TST).17,18 The data suggest that Blacks differ from Whites (with respect to race and not inclusive of ethnicity) on at least one SCD measure.2,4,6,19 Specifically, Blacks tend to report longer latencies (SL)20–22 and exhibit about 10–20 minutes more of middle insomnia (WASO) than Whites.23–25 While quantitative comparisons have not been reported for EMA; Blacks are more likely to experience late insomnia (ie, EMA).20,23 For TST, race is also a significant predictor of insufficient sleep.1,2 Among the studies that report minute estimates of sleep duration, Blacks experience the shortest sleep durations (20–40 min less)22,23,26,27 irrespective of an insomnia diagnosis.28 Similar findings have been corroborated in nationally representative samples.29,30
Beyond racial differences in sleep continuity (eg, SL, NWAK, WASO, EMA, and TST) is the issue of whether Black and White individuals differ in sleep satisfaction and/or the consequences of sleep disturbances. This is particularly important when group differences in SCD are relatively marginal, for one group may have a higher sleep need and thus “suffers more from less”.31,32 The literature on race differences in “sleep complaint” reveals that Blacks tend to report fewer sleep complaints4,5,22,31 but the results across studies are mixed.6,33 In one study, there were no significant differences in sleep complaints between Black and White individuals,34 whereas other studies have found that Blacks were more likely to be classified as noncomplaining poor sleepers35 or were more likely to reduce their complaints or sleep satisfaction with age when compared to Whites.36
One reason for the lack of clarity may be that the measures used across studies differ substantially. In some instances, daytime performance measures (eg, sleepiness and fatigue questionnaires) are used to make inferences about the consequences of SCD. In other cases, problem status is directly assessed (eg, the last 4 items of the Insomnia Severity Index [ISI] regarding sleep-related: satisfaction; worry; interference; and effects that others might notice). Sometimes, the participants are queried directly about their quantitative judgments (eg, on sleep diaries, where one may subjectively report on their sleep). Accordingly, any conclusion regarding sleep problem endorsement (sleep satisfaction) must be considered tentative.
Moreover, irrespective of illness severity and/or problem endorsement, is the question of whether the individual (or the racial and ethnic group) experiences sleep-related daytime dysfunction. Here again, the measures used across studies differ. In what is perhaps the largest study of its kind (n = 6139), Blacks, compared to Whites, reported significantly greater sleep-related daytime difficulties with concentration, memory, hobbies, or work.22 Using the Epworth Sleepiness Scale (ESS), similar findings were reported by Chen et al26 and Carnethon et al.23
In summary, the literature suggests two primary concerns that require further exploration: 1) Blacks may experience worse sleep continuity (particularly TST, which can be taken as an indirect or reciprocal measure of total wake time [TWT]), less problem endorsement, and worse daytime function; and 2) Blacks may be more prone to relapse or experience recurrences of insomnia. These gaps underscore the need to assess clinical domains concurrently and explore how they vary by race. The lack of such data limits our ability to know whether assessment and/or treatment for insomnia needs to be modified to account for race. Accordingly, the present study serves as the first large-scale study to concurrently assess at the community level SCD, sleep problem endorsement, and sleep-related daytime functioning among Black and White non-Hispanic individuals with sleep disturbance complaints.
Methods
Data Source
The data used for this study were extracted from a continuously running online survey (https://sleeplessinphilly.com)37 primarily used as a recruitment and screening tool for community-based insomnia research studies in the greater Philadelphia area in the United States, which includes parts of southeastern Pennsylvania, southern New Jersey, northern Delaware, and the northern Eastern Shore of Maryland. Potential respondents are recruited via ResearchMatch; Facebook; Google; and various other forms of social media (eg, advocacy groups and/or listservs dedicated to sleep disorders or other conditions of interest), advertisements in local newspapers, cable TV ads, and radio announcements. The screening survey includes items that pertain to socio-demographics, medical and mental health, and sleep and sleep disorders; the sleep-related items were developed based on standard clinical queries, typical item construction for retrospective assessments, literature review, and expert consensus (see Figure 1). Additionally, each sleep-related item in the survey is augmented with questions about problem endorsement (ie, “Do you consider this a problem?”). Informed consent was obtained from all participants. Respondents who access the survey are required to provide consent via a University of Pennsylvania Institutional Review Board (IRB) approved online informed consent form. Data collection from the survey was approved as a protocol and subsequently approved by the IRB (IRB 809272). Deidentified, archival data were extracted from this survey and used for this study. Important to note, this data source oversamples from the central northeast region of the United States and oversamples individuals with insomnia complaints; data from the survey have demonstrated utility as represented in prior studies.31,38 Survey data were extracted from a decade cohort (2011 to 2021) for use in the present study. Inclusion criteria were individuals over the age of 18 years who identified as Black or White, and who presented with one or more insomnia symptoms. Of note, the purpose of this study was to examine race-related differences in SCD, problem endorsement, and daytime dysfunction, and therefore the extracted data did not include measures on variables such as physical or mental health comorbidities, the use of medications (incl. sleep-specific medications), or other factors that influence sleep. As a result, individuals with comorbid disorders or conditions (eg, self-reported sleep disorders, medical and mental health conditions, or substance abuse) were not excluded from the analyses. Some co-morbid illnesses may have residual confounding effects. Results from the analyses in this study should be interpreted with caution.
 |
Figure 1 Survey Items of Sleep Continuity Disturbance, Sleep Continuity Problem Endorsement, and Sleep-Related Daytime Dysfunction. Note: aTST was asked in hours but converted to minutes for analytic purposes. bItem was reverse-scored, where “yes” was counted as 0 and “no” was counted as 1. |
Measures
The survey questions relevant to the present analysis (See Figure 1) included the following: basic socio-demographics (eg, age, sex, race, education level, etc).; severity and frequency of SCD; problem endorsement of SCD; and sleep-related daytime dysfunction.
SCD
“Sleep continuity” refers to the class or set of variables that represent “sleep performance”. That is, it is a class term (vs sleep architecture or sleep microarchitecture) for variables that represent latency to, and duration and efficiency of, the sleep that occurs during the sleep period, including SL, NWAK, WASO, EMA, TST, and SE%. When one or more of these variables are pathological, this may be referred to as SCD. More, the use of this class term promotes a level of specificity that is unconfounded with the many denotations and connotations of the vernacular term “insomnia”.38 Questionnaire items required that individuals quantify the following: length of time it takes them to fall asleep (SL in min), frequency of nocturnal awakenings (NWAK in number of incidents), duration of wakefulness in the middle of the night (WASO in min), and time awake earlier than intended (EMA in min). Individuals were also asked to quantify their typical sleep durations (TST in hours and minutes). For analysis purposes, TST was converted to minutes for comparability to SL, WASO, and EMA. All SCD queries are shown in Figure 1. To determine the severity of total wakefulness during an intended sleep period, the variable, total wake time (TWT), was calculated as follows: TWT = SL+WASO+EMA.
Sleep-Related Problem Endorsement
Following the provision of each sleep continuity estimate (eg, SL, NWAK, WASO, EMA, and TST), respondents were prompted to self-assess whether the quantified estimate (eg, SL of 45 minutes) was a problem for them (eg, “Do you consider this a problem?”). Response options were “Yes” or “No”. “No” was coded as a value of “0” and “Yes” was coded as a value of “1”. These data were used to estimate overall problem endorsement (ranging from 0 to 5) and to evaluate specific item frequencies (see Figure 1).
Sleep-Related Daytime Dysfunction
Survey items for sleep-related daytime dysfunction included questions that assessed for the presence of 1) concentration difficulties, 2) irritability, 3) feeling unrested upon waking, 4) impaired daytime function due to trouble sleeping, 5) daytime fatigue, and 6) daytime sleepiness (see Figure 1). Response options were “Yes” or “No”. Each “No” was coded as a value of “0” and each “Yes” was coded as a value of “1.” These data were used to estimate overall daytime impairment (ranging from 0 to 6). The question “Do you feel rested upon waking?” was reverse-scored.
Data Management and Statistical Analyses
Participants/Analysis Sample
The initial extracted dataset contained 8449 individuals, including 277 individuals who self-identified as Hispanic, representing less than 5% of the total sample and too small for any meaningful analyses. As a result, these individuals were removed from the final analysis sample, resulting in a total sample of 8172 Black and White non-Hispanics. Race was assessed categorically, where individuals reported whether they identified as “White” or “Black.” That is, participants were not categorized with respect to self-identified region of origin (eg, Caribbean vs African Blacks or Scandinavian vs Australian Whites). Respondents were also grouped by age as follows: young adults (YA; 18–29 years); adults (A; 30–44 years); young older or middle-aged adults (YO; 45–64 years); and older adults (OA; 65+ years).39,40 Survey entries with extreme values for SCD variables were identified and removed prior to matching (n = 35). Less extreme outliers were included to accurately depict the severity of sleep disturbances within this sample (eg, a survey entry reporting 99 nocturnal awakenings was removed, while another entry reporting 8 nocturnal awakenings was kept). An a priori power analysis regarding our variables of interest was not conducted, and all available survey records were used in analyses.
Mean Comparisons of SCD, Problem Endorsement, and Sleep-Related Daytime Dysfunction
Descriptive statistics and independent samples t-tests and chi-square tests were conducted to assess for mean differences by race group for age, sex, body mass index (BMI), and education. Independent samples t-tests and/or chi-square tests were also run to determine any significant differences in SCD variables (SL [minutes], NWAK [frequency], WASO [minutes], EMA [minutes], TST [minutes], and TWT [minutes]), SCD problem endorsement (ie, SL, NWAK, WASO, EMA, and TST), and sleep-related daytime dysfunction (ie, self-reported concentration, irritability, restedness, general daytime impairment, fatigue, and daytime sleepiness). A Bonferroni correction was applied to p-values, with an adjusted alpha level of 0.001. Continuous variables were presented as means and standard deviations (SD), and categorical variables were expressed as total numbers and percentages. Effect sizes were determined using Cohen’s d values for mean differences by race group and with indices for chi-square tests.
Unadjusted and Adjusted Multiple and Logistic Regressions of the Effect of Race on SCD, Problem Endorsement, and Sleep-Related Daytime Dysfunction
Unadjusted and adjusted multiple regressions assuming a normal distribution were used to examine the effect of race (Black vs White) on SCD (ie, SL, NWAK, WASO, EMA, TST, and TWT). Unadjusted and adjusted logistic regressions assuming binomial distribution were used to examine the effect of race (Black vs White) on the odds of SCD problem endorsement and sleep-related daytime complaints. Adjusted multiple and logistic regression analyses controlled for age, sex, BMI, and education level. Odds ratios were calculated as a measure of effect size for logistic regression models. All data management and statistical analyses were conducted using IBM SPSS Statistics (Version 27)41 and/or R (Version 4.3.2).42
Results
Participant Demographics
Table 1 summarizes the participant characteristics for the overall sample and by race group. Participants (N = 8172) were between the ages of 18–90 years (Mage = 47.9±14.9) and primarily of middle-age (ie, between 45 and 64 years; 48.3%), identified their biological sex at birth as female (67.4%), were overweight (M = 28.7±7.2) and had completed high school/GED or higher (98.7%). Significant differences between Blacks and Whites were found by age, BMI, and education. Whites were older, t(2585.6) = 13.795, p <0.001, had a lower BMI, t(2121) = 14.163, p <0.001), and were more likely to have a 2- or 4- year degree or higher (X2(3) = 800.88, p <0.001) compared to Blacks. No significant differences were found by sex between the respective groups, X2(1) = 0.029, p =0.865.
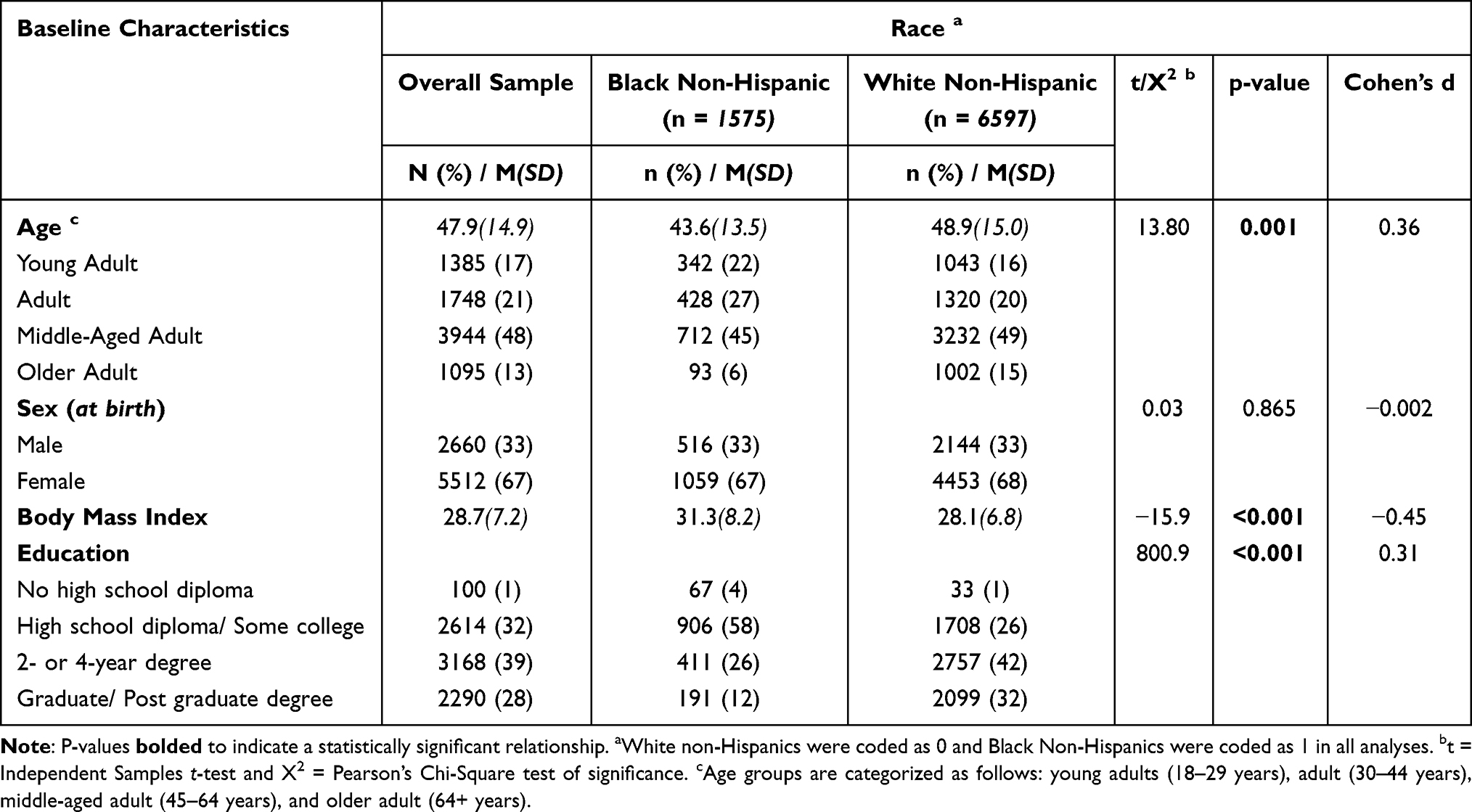 |
Table 1 Participant Demographics by Race (N=8172) |
SCD
Mean Comparisons of SCD
Mean SCD for the overall sample and differences by race group are reported in Table 2; mean SCD differences by race only are visually represented in Figures 2–7. Independent samples t-tests revealed statistically significant by group differences for all SCD variables except EMA. Specifically, Blacks took longer to fall asleep (SL; M = 49.7±38.8) than Whites (M = 46.7±40.8). While Blacks reported to wake up less often during the night (NWAK; M = 2.7±1.7), when awakened, they remained awake for longer periods (WASO; M = 47.7±51.8) before returning to sleep than Whites (M = 3.1±2.5; M = 39.3±45.1, respectively) (p < 0.01). The total amount of awake time during the night for Blacks lasted significantly longer than Whites: (TWT; M = 155.8±101.0 and M = 143.7±88.9, respectively), t(2192.1) = −4.364, p < 0.001. As a result, Blacks also slept significantly less (by ~40 minutes) than Whites (TST; M = 316.2±94.1 and M = 353.0±80.7, respectively), t(2160.7) = 14.311, p < 0.001.
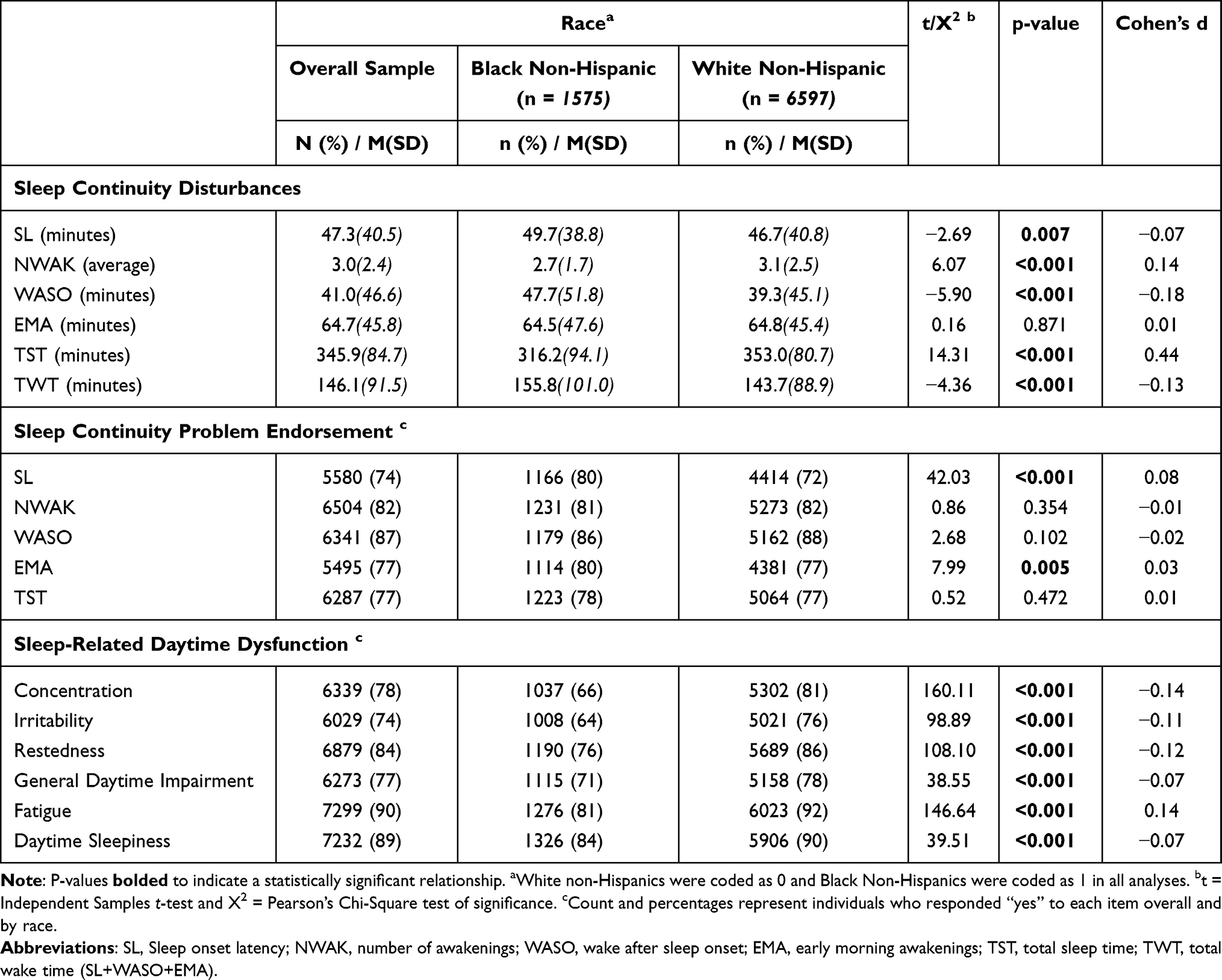 |
Table 2 Mean Differences of Sleep Continuity Disturbances, Sleep Continuity Problem Endorsement, and Sleep-Related Daytime Dysfunction by Race (N=8172) |
 |
Figure 2 Mean differences of sleep latency (SL) by race. Notes: This bar graph corresponds to SCD variables presented in Table 2. Error bars represent standard errors and are set at the 95% CI. |
 |
Figure 3 Mean differences of nighttime awakenings (NWAK) by race. Notes: This bar graph corresponds to SCD variables presented in Table 2. Responses are by count. Error bars represent standard errors and are set at the 95% CI. |
 |
Figure 4 This bar graph corresponds to SCD variables presented in Table 2. Mean differences of wake after sleep onset (WASO) by race. Notes: Responses are in minutes. Error bars represent standard errors and are set at the 95% CI. |
 |
Figure 5 This bar graph corresponds to SCD variables presented in Table 2 Table 1. Mean differences of early morning awakenings (EMA) by race. Notes: Responses are in minutes. Error bars represent standard errors and are set at the 95% CI. |
 |
Figure 6 This bar graph corresponds to SCD variables presented in Table 2. Mean differences of total sleep time (TST) by race. Notes: Responses are in minutes. Error bars represent standard errors and are set at the 95% CI. |
 |
Figure 7 This bar graph corresponds to SCD variables presented in Table 2 Table 1. Mean differences of total wake time (TWT) by race. Notes: A calculated variable (SL+WASO+EMA), displayed in minutes. Error bars represent standard error and are set at the 95% CI. |
Effect of Race on SCD
Table 3 summarizes results for the multiple regressions conducted to examine the effect of race (Black vs White [reference]) on SCD. Controlling for age, sex, BMI and education, race was negatively associated with SL (b = −2.62, p < 0.05), NWAK (b = −0.44, p<0.001), and TST (b = −28.57, p<0.001); race was positively associated with WASO (b = 9.46, p<0.001) and TWT (B = 9.33, p<0.001). Adjusting for age, sex, BMI, education and race was not significantly associated with EMA.
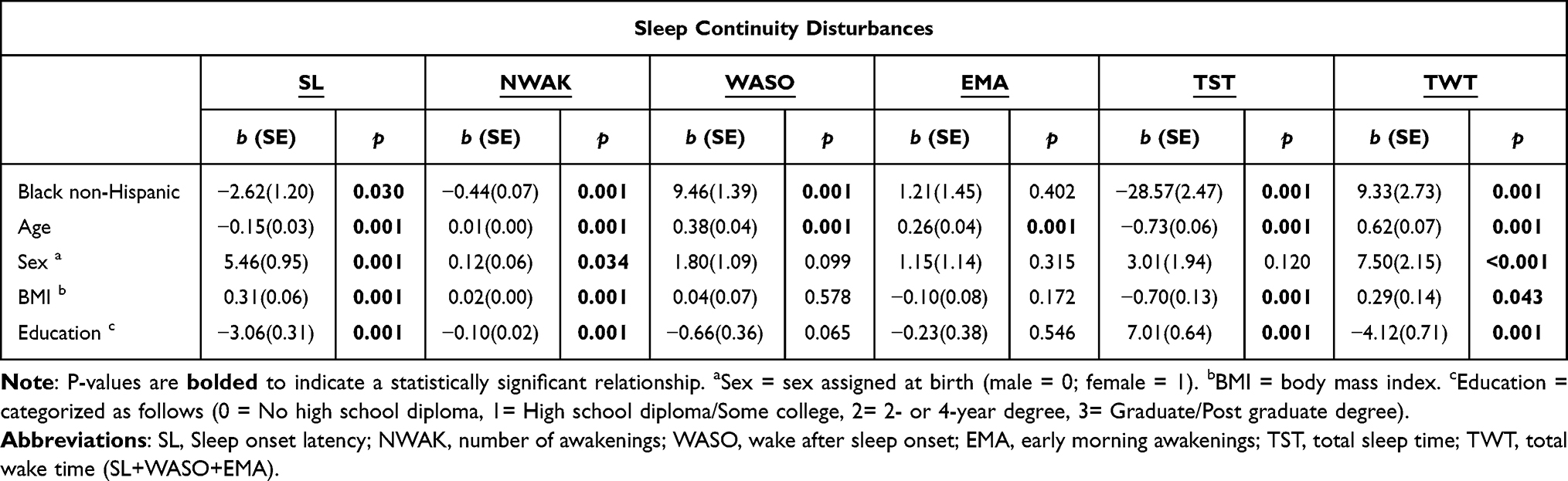 |
Table 3 Multiple Regression Results of the Effect of Race on Sleep Continuity Disturbances, Adjusted for Age, Sex, BMI, and Education (N=8172) |
Sleep Continuity Problem Endorsement
Mean Comparisons of Problem Endorsement
Rates of sleep-related problem endorsement for the overall sample and by race group are reported in Table 2. The chi-square tests for independence revealed statistically significant by group differences in problem endorsement for SL and EMA, whereas there were no significant by group differences for NWAK, WASO or TST. Blacks were significantly more likely to endorse SL as a problem, X2(1) = 42.03, p < 0.001. Although there were no significant differences in EMA duration between groups, Blacks were also more likely to endorse EMA as a problem, X2(1) = 7.987, p = 0.005.
Effect of Race on Problem Endorsement
Table 4 summarizes the adjusted odds ratios (OR) for each SCD problem endorsement, with race as a predictor, adjusted for age, sex, BMI, and education. Independent of any age, sex, BMI or education-related effects, race was most strongly associated with endorsing SL and EMA sleep continuity symptoms as a problem. Blacks had an approximate 22% increased odds of endorsing SL (OR = 1.22, 95% CI[0.05,0.35], p<0.01) and 39% increased odds of endorsing EMA (OR = 1.39, 95% CI [0.17,0.49], p<0.001) as a problem than Whites.
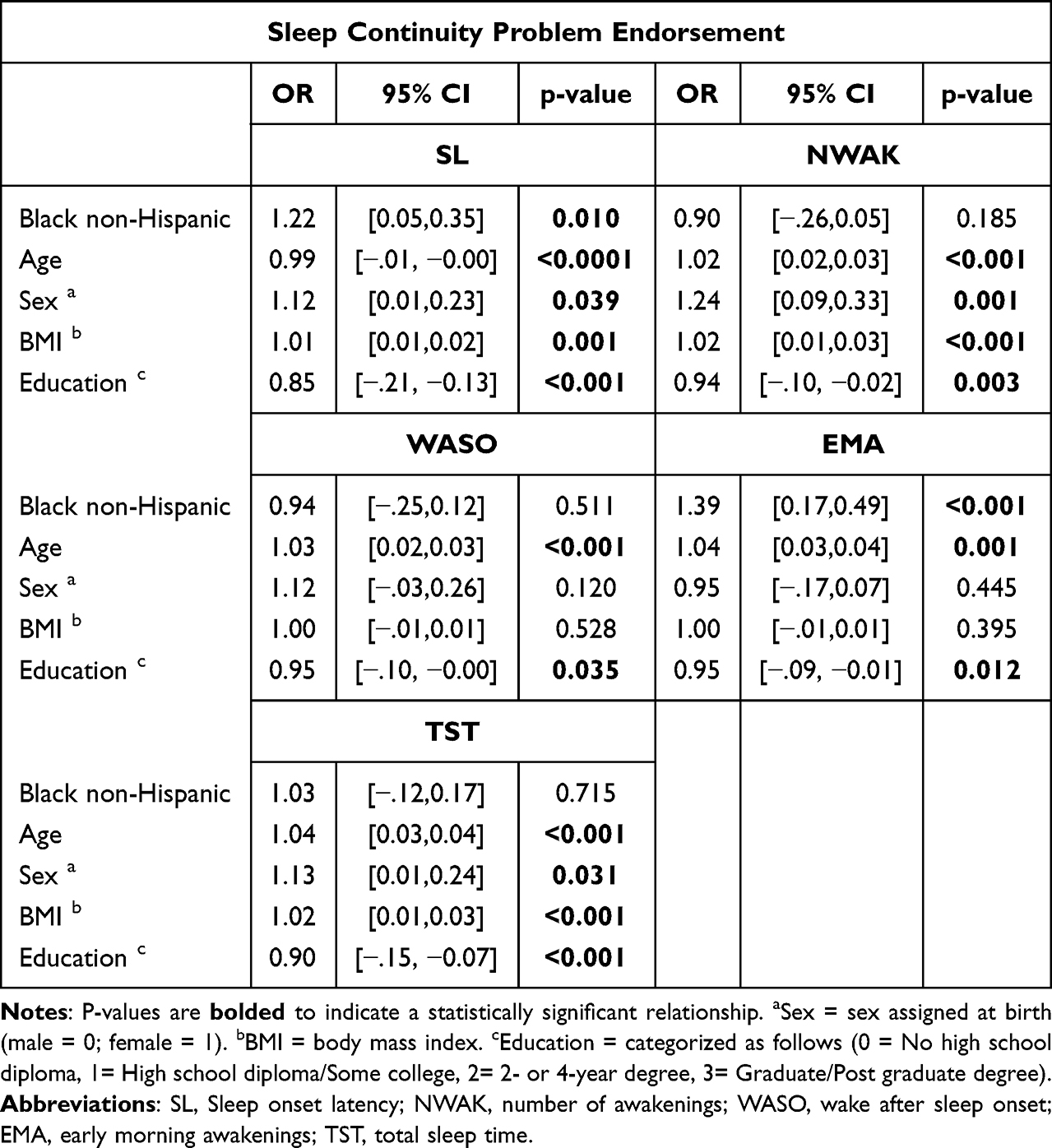 |
Table 4 Odds Ratios (OR) and 95% Confidence Intervals (CI) from Logistic Regression Results of the Effect of Race on Sleep Continuity Problem Endorsement, Adjusted for Age, Sex (at Birth), BMI, and Education (N=8172) |
Sleep-Related Daytime Dysfunction
Mean Comparisons of Sleep-Related Daytime Dysfunction
Rates of sleep-related daytime dysfunction for the overall sample and by race group are reported in Table 2. The chi-square tests for independence revealed significant by group differences for all symptoms of sleep-related daytime dysfunction, eg, concentration [X2 = 160.11, p<0.001], irritable [X2 = 98.89, p<0.001], restedness [X2 = 108.10, p<0.001], general daytime impairment [X2 = 38.55, p<0.001], fatigue [X2 = 146.64, p<0.001], and daytime sleepiness [X2 = 39.51, p<0.001]. In general, Whites endorsed sleep-related daytime dysfunction more frequently than Blacks.
Effect of Race on Sleep-Related Daytime Dysfunction
Table 5 summarizes the adjusted OR for each sleep-related daytime dysfunction variable, with race as a predictor, adjusted for age, sex, BMI, and education. Independent of any age, sex, BMI, or education-related effects, race remained strongly associated with each sleep-related daytime dysfunction. Blacks had decreased odds of endorsing concentration (OR = 0.41, 95% CI[−1.03,-0.77], p<0.001), irritability (OR = 0.44, 95% CI [−0.94,-0.68], p<0.001), restedness (OR = 0.47, 95% CI [0.24,0.46], p<0.001), general daytime impairment (OR = 0.61, 95% CI [0.64,-0.37], p<0.001), fatigue (OR = 0.37, 95% CI [−1.16,-0.82], p<0.001) and daytime sleepiness (OR = 0.55, 95% CI [−0.78,-0.43], p<0.001) than Whites.
 |
Table 5 Odds Ratios (OR) and 95% Confidence Intervals (CI) from Logistic Regression Results of the Effect of Race on Sleep-Related Daytime Dysfunction, Adjusted for Age, Sex (at Birth), BMI, and Education (N=8172) |
Discussion
To our knowledge, the present analysis is the first to concurrently assess racial differences between Blacks and Whites in sleep continuity (ie, insomnia severity), sleep continuity problem endorsement, and sleep-related daytime function in a large community sample. The results revealed that Blacks’ and Whites’ self-reported sleep were largely comparable across all three domains. The primary differences were that Black individuals took longer to fall asleep (SL), woke less frequently (NWAK), but stayed up longer during the night when awakened (WASO), and had substantially shorter sleep durations (TST). Blacks were also slightly more likely to endorse issues with the length of time it took them to fall asleep, and that they woke up earlier than desired. Interestingly, Black individuals were less likely to report any sleep-related daytime dysfunction and, while they were not significantly more likely to report waking up earlier than they planned (EMA), they were more likely to endorse the behavior as a problem. This remained true even after controlling for age, sex, BMI, and education. In our analysis, race seems to be the most important factor driving these outcomes. Although race (and ethnicity) often serves as a proxy for other social determinants of health and health disparities, the variable (race) appears to have its own independent function.
These findings can be compared to earlier results of studies that have shown that Black individuals, on average, tend to report longer SL and WASO, and shorter TSTs.6 Our results revealed an average SL of only three minutes difference between the two groups versus other studies that reported an average of 12 minutes or longer.21 While these differences are minute, any amount of reduced sleep can lead to health consequences. Insufficient sleep can reduce time spent in restorative sleep stages (eg, REM), leading to impaired cognitive function and mood disturbances during waking hours, and is associated with increased risk for severe and persistent chronic illnesses (eg, cardiovascular disease, Alzheimer’s disease, dementia, and diabetes).43,44 As such, our study findings support the need to further explore these differences in sleep-related outcomes. In our present study, this difference in time could be explained by how the data was collected, which was via self-reported survey and not corroborated with more systematic means such as daily diaries or objective measures like actigraphy. There are known discrepancies between objective and subjective measures of sleep, especially among racial and ethnic minority groups.6,45,46 Despite this, our study builds on the existing literature by examining the nuance of the between-group differences in SCD that may be missed when examining sleep (in general).
Additionally, in the present study, Blacks were more likely to report their SL and EMA as problems but less likely to report sleep-related daytime difficulties. At least one other study reported somewhat similar results. Tutek et al35 found that Blacks were more likely to be “non-complaining poor sleepers” compared to Whites. Some researchers have suggested that these contradictory outcomes among Blacks may be related to John Henryrism and/or Super Women Schema, whereby underrepresented groups develop excessive and overtly strong work ethics and suppress emotional reactions to avoid being associated with negative stereotypes typically linked with their community.47–49 From a measurement standpoint, the difference between our studies may be the way problem endorsement was assessed. In the present study, each sleep continuity variable was directly assayed to determine whether the reported value was a problem. In the Tutek35 study, individuals were assessed (in a general way) as to whether their overall sleep was a problem. Interestingly, that study concluded that medical co-morbidity and psychological distress were much stronger predictors of sleep complaint than race. While the literature on racial and ethnic differences in sleep complaints is largely inconsistent,6 our study contributes to the discourse on the importance of determining how sleep is defined and measured across studies.
The observed group differences were about 40 minutes for TST, about 4 minutes for SL, about 1 awakening for NWAK, and about 8 minutes for WASO. The TST difference is the most meaningful and is consistent with many other studies that show that Black Americans report lower TST than White Americans.1 Importantly, recent evidence shows that this disparity is widening27 and is related to population-level differences in cardiometabolic disease risk.43 The differences in sleep continuity variables were somewhat small, below the threshold of clinically meaningful differences. Previous work has shown that even small population-level differences in sleep variables (eg, just a few minutes) can have measurable impacts on health outcomes, especially when scaled up to the population level.50 Further, previous work shows that Black individuals who do not identify as having a problem falling asleep are more likely to take >30 minutes to fall asleep, relative to White individuals.50 Therefore, since the current sample consisted of individuals self-selected as having a sleep complaint, there may be different patterns in the wider population. Future work should clarify this.
Strengths, Limitations, and Future Directions
One key strength of this study is that it evaluated differences by race in self-reported SCD, sleep problem endorsement, and sleep-related daytime dysfunction – few studies have assessed these variables concurrently, at the community-level. This allows for an exploration of relationships among different elements of community sleep health as they differ between groups. Moreover, the large sample size allowed for a level of statistical power that ensured even small differences were accounted for in the analysis.
The study also had some important limitations. Necessarily, we used single-item measures of complex constructs. While a common practice in epidemiologic sleep research,51 multi-item, independently validated instruments (eg, the Insomnia Severity Index to assess insomnia severity, the Epworth Sleepiness Scale to assess excessive daytime sleepiness, and the Functional Outcomes of Sleep Questionnaire to assess the impact of sleepiness on daily function), high-density prospective sampling of sleep continuity (ie, daily sleep diaries) over periods of weeks to months and/or objectively assessed sleep data (eg, wearable devices) would have provided more resolution and reduced some measurement error. While any combination of these efforts could have strengthened the reliability of our findings, there are existing known racial and ethnic differences in the concordance between self-report and objectively measured sleep, inviting the potential for additional biases.52 Also of note, while common potential misclassifications of sleep and wake periods do occur with the use of wearable devices, additional factors such as skin tone and even weight are particularly important when conducting research with certain groups.53 This said, the database used for this study was extracted from a screening survey archive that was developed by experts in the behavioral sleep medicine field (supporting construct validity) and was deliberately brief to minimize respondent burden (and improve internal validity). As such, the data and analyses performed were limited to the factors available.
Another limitation is that the study exclusively assessed individuals with self-identified sleep complaints, meaning that the observed race-based variations may not extend to individuals who may not identify as having a sleep-related complaint. Prior work shows that Black adults tend to complain less about sleep in general,34 though this is possibly corrected by wording questions in a more neutral manner,20 as was attempted in this study. In the future, including a general sample of individuals with and without sleep complaints would be informative.
Third, the original survey did not include time in bed (TIB) or measures of time to sleep (vs time to bed), or time of final awakening (vs time out of bed). This absence prohibits a calculated measure of total sleep time (TST = TIB - [SL + WASO + EMA]) vs a self-reported estimate; a calculated TST would have provided a more internally valid measure of TST. The absence of a TIB measure also makes it difficult to determine whether reduced time in bed accounts for the majority of the observed TST findings. Previous work shows that self-reported TST is often confounded with TIB.20 If this is the case, then the observed reduction in TST among Blacks may have more to do with sleep insufficiency than SCD.
This being the case, cognitive behavioral therapy for insomnia (CBT-I) with Blacks may need to be tailored to focus more on extending sleep duration via titration than is typically allowed in 4–8 sessions (ie, the standard treatment). This is of particular importance, as this suggests that Blacks may require more treatment sessions to reach (and maintain) desired outcomes. Moreover, irrespective of whether sleep profiles differ by race, future research should explore whether there are racial differences in CBT-I treatment response or relapse rates. To our knowledge, there are only two studies that have addressed these issues.54,55
Fourth, the study assessed racial associations that were limited to Black and White participants only, as other groups (American Indian/Alaska Native, Asian, Native Hawaiian/Pacific Islander, or Other) were not part of the original inclusion criteria due to known small sample sizes that would limit any meaningful analyses. Additionally, less than 5% of the extracted sample identified their ethnicity as Hispanic. As a result, analyses exploring ethnicity as a contributing factor to sleep health were beyond the scope of this study. Given the importance of ethnic and cultural considerations in sleep research,56 future studies would benefit by taking into account within-group differences (eg, ethnicity and/or ancestry) and the intersections of other marginalized identities.
Fifth, Blacks, when compared to Whites, were more likely to be categorized as “obese” (as assessed by BMI). While we accounted for these differences statistically in our analyses, the purpose of this study was not to diagnose. Therefore, we did not account for individuals who may be diagnosed with other sleep-related disorders like obstructive sleep apnea (OSA), a common sleep disorder diagnosed in underserved communities. Considering additional medical conditions that could potentially exacerbate SCD may further explain these sleep-related differences.
Finally, the observed differences by race may not represent racial differences and instead represent effects of unmeasured variables that co-aggregate or intersect with race (eg, social determinants of health disparities such as the effect of neighborhood safety, racism, lower income, and multiple jobs status and/or shift work).20 Of note, the extracted data did not include measures of physical or mental health comorbidities, the use of medications (including sleep-specific medications), income, occupation, or other physical, mental, or environmental factors (ie, noise, light, greenspace) that influence sleep.57 As a result, we did not control for these sleep-related factors in our analyses. Future studies should assess these things directly and evaluate whether they potentially mediate or moderate observed effects.
These limitations point to additional future implications and directions. For example, qualitative methods, such as interviews, may offer valuable complements to the use of validated instruments, as they often provide context by way of the individual’s subjective experience of the sleep disturbance and its impact on daily functioning and quality of life. Especially given the measurement issues inherent in assessing sleep across racial and ethnic groups,10 a follow-up prospective study with sleep diaries, wearables, and qualitative data may yield important insights regarding individuals’ relationships with sleep that may underlie these findings.58
These results also reiterate the multidimensional nature of sleep health59 – sleep health is more than just sleep duration. A series of recent scientific statements by the American Heart Association highlight that sleep health is an integral part of overall cardiometabolic health, included alongside other dimensions such as diet and physical activity in the “Life’s Essential 8” framework.60 Further, sleep health as a key factor in cardiometabolic health consists of multiple dimensions, including sleep duration but also sleep continuity disturbances,61 highlighting the importance of factors such as SL and WASO. In addition, sleep health is known to be inextricably linked with upstream social determinants of health.60,61 This study points to the importance of including these additional sleep dimensions in sleep disparities research and community-based interventions. Sleep health has been identified as a key factor to consider in designing and implementing community-based cardiometabolic behavioral health promotion programs,62 and these findings suggest potential targets beyond sleep duration for these efforts. Taken together, the present study identifies possible community-level sleep health disparities beyond sleep duration, which have already been identified as important aspects of multidimensional sleep health – which itself has been identified as an important factor in population cardiometabolic health. Future work should incorporate these and other dimensions of sleep health into community-based health promotion efforts.
Abbreviations
SCD, Sleep continuity disturbance; SL, Sleep latency or sleep onset latency; NWAK, Number of awakenings; WASO, Wake after sleep onset; EMA, Early morning awakenings; TST, Total sleep time; SE, Sleep efficiency; TWT, Total wake time; TIB, Time in bed; PSG, Polysomnography; ESS, Epworth Sleepiness Scale; CBT-I, Cognitive Behavioral Therapy for Insomnia.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors on request. Please refer all data requests to the senior author at [email protected].
Ethics Approval and Informed Consent
Deidentified archival data extracted for use in this study was approved as a protocol and followed the ethical approval guidelines provided by the University of Pennsylvania School of Medicine Institutional Review Board (IRB No. 809272). Informed consent was obtained from all individual participants included in the study. This research was performed in accordance with the ethical standards of the Declaration of Helsinki.
Acknowledgments
We would like to thank the members of the Behavioral Sleep Medicine Program at the University of Pennsylvania for making this data available and for their collaboration.
Author Contributions
All coauthors significantly contributed to the work reported in this paper and met criteria for authorship. All co-authors have drafted or written or substantially revised or critically reviewed the paper and have agreed on the final contents of the paper, including the journal to which the paper is submitted and acceptance of responsibility for the scientific content of the paper. The co-authors certify that this submission is original work and is not under review for publication at any other source.
Michelle G. Thompson: conceptualization, formal analysis, methodology, visualization, writing – original draft, writing – review and editing, project administration
Julia T. Boyle: conceptualization, data curation, formal analysis, methodology, visualization, writing – original draft, writing – review and editing
Alexandria Muench: conceptualization, writing – original draft, writing – review and editing
Elizabeth Lampe: formal analysis, methodology, validation, visualization, writing – review and editing
Debbie Chung: visualization, writing – review and editing, supervision
Michael A. Grandner: conceptualization, methodology, writing – original draft, writing – review and editing
John B. Jemmott III: formal analysis, methodology, writing – original draft, writing – review and editing
Azizi A. Seixas: conceptualization, writing – review and editing
Girardin Jean-Louis: conceptualization, funding acquisition, supervision, writing – review and editing
Michael L. Perlis: data curation, funding acquisition, supervision, writing – original draft, writing – review and editing.
Funding
This work was supported by a University of Pennsylvania Penn Provost Fellows postdoctoral fellowship and by the National Institutes of Health (NIH [grant numbers 1T32HL166609, L24AG0556021, R01HL142066, and R01AG067523]). The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH. Dr Boyle is supported by funding from VA Rehabilitation Research and Development (RR&D), USA (CDA-1; IK1RX004762-01).
Disclosure
Some material within this paper is the result of work supported with resources and use of facilities at VA Boston Healthcare System. The contents do not represent the views of the US Department of Veterans Affairs or the United States Government. Michelle Thompson and Girardin Jean-Louis report grants from the National Institutes of Health during the conduct of the study. Julia Boyle reports that this work was supported with resources and facilities of VA Boston Healthcare System during the conduct of the study. Michael Grandner reports personal fees from Google, Natrol, Smartypants Vitamins, Kenvue, Haleon, and WNDR HLTH outside the submitted work. The other authors do not have any financial conflicts of interest to disclose.
References
1. Jean-Louis G, Grandner MA, Youngstedt SD, et al. Differential increase in prevalence estimates of inadequate sleep among black and white Americans. BMC Public Health. 2015;15(1). doi:10.1186/s12889-015-2500-0
2. Williams NJ, Grandner MA, Wallace DM, et al. Social and behavioral predictors of insufficient sleep among African Americans and Caucasians. Sleep Med. 2016;18:103–18. doi:10.1016/j.sleep.2015.02.533
3. Xu J, Luo L, Gamaldo A, et al. Trends in sleep duration in the U.S. from 2004 to 2018: a decomposition analysis. SSM Popul Health. 2024;25:101562. doi:10.1016/j.ssmph.2023.101562
4. Petrov ME, Lichstein KL. Differences in sleep between black and white adults: an update and future directions. Sleep Med. 2016;18:74–81. doi:10.1016/j.sleep.2015.01.011
5. Ruiter ME, DeCoster J, Jacobs L, Lichstein KL. Sleep disorders in African Americans and Caucasian Americans: a meta-analysis. Behav Sleep Med. 2010;8(4):246–259. doi:10.1080/15402002.2010.509251
6. Johnson DA, Jackson CL, Williams N, Alcántara C. Are sleep patterns influenced by race/ethnicity – a marker of relative advantage or disadvantage? Evidence to date. Nat Sci Sleep. 2019;Volume 11:79–95. doi:10.2147/nss.s169312
7. Song Y, Ancoli-Israel S, Lewis CE, Redline S, Harrison SL, Stone KL. The association of race/ethnicity with objectively measured sleep characteristics in older men. Behav Sleep Med. 2012;10(1):54–69. doi:10.1080/15402002.2012.636276
8. Kaufmann CN, Mojtabai R, Hock RS, et al. Racial/ethnic differences in insomnia trajectories among US older adults. Am J Geriatric Psychiatry. 2016;24(7):575–584. doi:10.1016/j.jagp.2016.02.049
9. Cheng P, Casement MD, Cuellar R, et al. Sleepless in COVID-19: racial disparities during the pandemic as a consequence of structural inequity. Sleep. 2022;45(1). doi:10.1093/sleep/zsab242
10. Ahn S, Lobo JM, Logan JG, Kang H, Kwon Y, Sohn M-W. A scoping review of racial/ethnic disparities in sleep. Sleep Med. 2021;81:169–179. doi:10.1016/j.sleep.2021.02.027
11. Grandner MA. Sleep, health, and society. Sleep Med Clin. 2022;17(2):117–139. doi:10.1016/j.jsmc.2022.03.001
12. Smedley A, Smedley BD. Race as biology is fiction, racism as a social problem is real: anthropological and historical perspectives on the social construction of race. Am Psychologist. 2005;60(1):16. doi:10.1037/0003-066X.60.1.16
13. Gillispie-Bell V. The contrast of color: why the black community continues to suffer health disparities. Obstetrics Gynecol. 2021;137(2):220–224. doi:10.1097/AOG.0000000000004226
14. Noonan AS, Velasco-Mondragon HE, Wagner FA. Improving the health of African Americans in the USA: an overdue opportunity for social justice. Public Health Rev. 2016;37(1). doi:10.1186/s40985-016-0025-4
15. Aili K, Åström-Paulsson S, Stoetzer U, Svartengren M, Hillert L. Reliability of actigraphy and subjective sleep measurements in adults: the design of sleep assessments. J Clin Sleep Med. 2017;13(1):39–47. doi:10.5664/jcsm.6384
16. Akre S, Cohen ZD, Welborn A, et al. Comparing self reported and physiological sleep quality from consumer devices to depression and neurocognitive performance. Npj Digital Med. 2025;8(1):92. doi:10.1038/s41746-025-01493-6
17. Mezick EJ, Matthews KA, Hall M, et al. Influence of race and socioeconomic status on sleep: pittsburgh sleep SCORE project. Psychosomatic Med. 2008;70(4):410. doi:10.1097/PSY.0b013e31816fdf21
18. Hall MH, Matthews KA, Kravitz HM, et al. Race and financial strain are independent correlates of sleep in midlife women: the SWAN sleep study. Sleep. 2009;32(1):73–82.
19. Durrence HH, Lichstein KL. The sleep of African Americans: a comparative review. Behav Sleep Med. 2006;4(1):29–44. doi:10.1207/s15402010bsm0401_3
20. Grandner MA, Petrov MER, Rattanaumpawan P, Jackson N, Platt A, Patel NP. Sleep symptoms, race/ethnicity, and socioeconomic position. J Clin Sleep Med. 2013;9(9):897–905. doi:10.5664/jcsm.2990
21. Suarez E, Fang SC, Bliwise D, Yaggi HK, Araujo A. Disentangling racial/ethnic and socioeconomic differences in self-reported sleep measures: the Boston Area Community health survey. Sleep Health. 2015;1(2):90–97. doi:10.1016/j.sleh.2015.02.003
22. Ram S, Seirawan H, Kumar SKS, Clark GT. Prevalence and impact of sleep disorders and sleep habits in the United States. Sleep Breath. 2010;14(1):63–70. doi:10.1007/s11325-009-0281-3
23. Carnethon MR, De Chavez PJ, Zee PC, et al. Disparities in sleep characteristics by race/ethnicity in a population-based sample: Chicago area sleep study. Sleep Med. 2016;18:50–55. doi:10.1016/j.sleep.2015.07.005
24. Matthews KA, Hall MH, Lee L, et al. Racial/ethnic disparities in women’s sleep duration, continuity, and quality, and their statistical mediators: study of women’s health across the nation. Sleep. 2019;42(5):zsz042. doi:10.1093/sleep/zsz042
25. Owens S, Hunte H, Sterkel A, Johnson DA, Johnson-Lawrence V. Association between discrimination and objective and subjective sleep measures in the MIDUS adult sample. Psychosomatic Med. 2017;79(4):469. doi:10.1097/PSY.0000000000000428
26. Chen X, Wang R, Zee P, et al. Racial/ethnic differences in sleep disturbances: the Multi-Ethnic Study of Atherosclerosis (Mesa). Sleep. 2015;38(6):877–888. doi:10.5665/sleep.4732
27. Sheehan CM, Frochen SE, Walsemann KM, Ailshire JA. Are U.S. adults reporting less sleep?: findings from sleep duration trends in the national health interview survey, 2004–2017. Sleep. 2019;42(2). doi:10.1093/sleep/zsy221
28. Kalmbach DA, Pillai V, Arnedt JT, Drake CL. DSM-5 insomnia and short sleep: comorbidity landscape and racial disparities. Sleep. 2016;39(12):2101–2111. doi:10.5665/sleep.6306
29. Wang S, Rossheim ME, Nandy RR. Trends in prevalence of short sleep duration and trouble sleeping among US adults, 2005–2018. Sleep. 2022;46(1). doi:10.1093/sleep/zsac231
30. Caraballo C, Mahajan S, Valero-Elizondo J, et al. Evaluation of temporal trends in racial and ethnic disparities in sleep duration among US adults, 2004-2018. JAMA Network Open. 2022;5(4):e226385–e226385. doi:10.1001/jamanetworkopen.2022.6385
31. Boyle J, Vargas I, Rosenfield B, Grandner MA, Perlis ML. Insomnia severity and degree of dysfunction: what is to be learned when these domains are discordant? Behav Sleep Med. 2021;1–9. doi:10.1080/15402002.2021.1895794
32. Scott H, Perlis M. The Sleep Opportunity, Need and Ability (SONA) theory. J Sleep Res. 2025;e70030. doi:10.1111/jsr.70030
33. Adenekan B, Pandey A, McKenzie S, Zizi F, Casimir GJ, Jean-Louis G. Sleep in America: role of racial/ethnic differences. Sleep Med Rev. 2013;17(4):255–262. doi:10.1016/j.smrv.2012.07.002
34. Grandner MA, Patel NP, Gehrman PR, et al. Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep Med. 2010;11(5):470–478. doi:10.1016/j.sleep.2009.10.006
35. Tutek J, Mulla MM, Emert SE, et al. Health and demographic discriminators of an insomnia identity and self-reported poor quantitative sleep. Sleep Health. 2019;5(3):221–226. doi:10.1016/j.sleh.2019.01.009
36. Tapia AL, Yu L, Lim A, et al. Race and sex differences in the longitudinal changes in multidimensional self-reported sleep health characteristics in aging older adults. Sleep Health. 2023;9(6):947–958. doi:10.1016/j.sleh.2023.08.008
37. Program BSM. Welcome! University of Pennsylvania. Available from: http://www.sleeplessinphilly.com/.
38. Boyle JT, Rosenfield B, Di Tomasso RA, et al. Sleep continuity, sleep related daytime dysfunction, and problem endorsement: do these vary concordantly by age? Behav Sleep Med. 2023;21(4):436–447. doi:10.1080/15402002.2022.2124994
39. Lucas JW, Connor EM, Bose J. Back, lower limb, and upper limb pain among US adults, 2019. NCHS Data Brief. 2021;(415):1–8.
40. Villarroel MA, Terlizzi EP. Symptoms of Depression Among Adults: United States, 2019. US Department of Health and Human Services, Centers for Disease Control; 2020.
41. IBM SPSS statistics for windows. Version 27.0. IBM corp. 2020.
42. R: a language and environment for statistical computing. Version 4.3.2. R Foundation for Statistical Computing. 2023. http://www.R-project.org/.
43. Tubbs AS, Ghani SB, Valencia D, et al. Racial/ethnic minorities have greater declines in sleep duration with higher risk of cardiometabolic disease: an analysis of the U.S. National health interview survey. Sleep Epidemiol. 2022;2:100022. doi:10.1016/j.sleepe.2022.100022
44. Chaput J-P, Dutil C, Featherstone R, et al. Sleep timing, sleep consistency, and health in adults: a systematic review. Appl Physiol Nutr Metab. 2020;45(10):S232–S247. doi:10.1139/apnm-2020-0032
45. Jackson CL, Ward JB, Johnson DA, Sims M, Wilson J, Redline S. Concordance between self-reported and actigraphy-assessed sleep duration among African-American adults: findings from the Jackson heart sleep study. Sleep. 2020;43(3):zsz246. doi:10.1093/sleep/zsz246
46. Lehrer HM, Yao Z, Krafty RT, et al. Comparing polysomnography, actigraphy, and sleep diary in the home environment: the Study of Women’s Health Across the Nation (SWAN) sleep study. Sleep Adv. 2022;3(1). doi:10.1093/sleepadvances/zpac001
47. Erving CL, Zajdel RA, Blevins KM, et al. The association between Superwoman schema and subjective sleep quality among Black women. Sleep Health. 2024;10(3):302–307. doi:10.1016/j.sleh.2023.12.008
48. McLaurin-Jones TL, Anderson AS, Marshall VJ, Lashley M-B, Carter-Nolan PL. Superwomen and sleep: an assessment of black college women across the African diaspora. Int J Behav Med. 2021;28(1):130–139. doi:10.1007/s12529-020-09930-4
49. Bonham VL, Cooper K, Minniti CP, Abdallah K, Buscetta A. Clinical implications of active coping on sleep: john henryism in a sickle cell disease cohort. Blood. 2019;134(Supplement_1):1025. doi:10.1182/blood-2019-131240
50. Rezaei N, Grandner MA. Changes in sleep duration, timing, and variability during the COVID-19 pandemic: large-scale Fitbit data from 6 major US cities. Sleep Health. 2021;7(3):303–313. doi:10.1016/j.sleh.2021.02.008
51. Watson NF, Badr MS, Belenky G, et al. Joint consensus statement of the American academy of sleep medicine and sleep research society on the recommended amount of sleep for a healthy adult: methodology and discussion. Sleep. 2015;38(8):1161–1183. doi:10.5665/sleep.4886
52. Jackson CL, Patel SR, Jackson WB 2nd, Lutsey PL, Redline S. Agreement between self-reported and objectively measured sleep duration among white, black, hispanic, and Chinese adults in the United States: multi-ethnic study of atherosclerosis. Sleep. 2018;41(6). doi:10.1093/sleep/zsy057
53. de Zambotti M, Goldstein C, Cook J, et al. State of the science and recommendations for using wearable technology in sleep and circadian research. Sleep. 2024;47(4). doi:10.1093/sleep/zsad325
54. Cheng P, Luik AI, Fellman-Couture C, et al. Efficacy of digital CBT for insomnia to reduce depression across demographic groups: a randomized trial. Psychol Med. 2019;49(3):491–500. doi:10.1017/s0033291718001113
55. Zhou ES, Ritterband LM, Bethea TN, Robles YP, Heeren TC, Rosenberg L. Effect of culturally tailored, internet-delivered cognitive behavioral therapy for insomnia in black women: a randomized clinical trial. JAMA psychiatry. 2022;79(6):538–549. doi:10.1001/jamapsychiatry.2022.0653
56. Dubar RT. # NoJusticeNoSleep: critical intersections of race-ethnicity, income, education, and social determinants in sleep health disparities. Sleep Health. 2022;8(1):7–10. doi:10.1016/j.sleh.2021.12.007
57. Billings ME, Hale L, Johnson DA. Physical and social environment relationship with sleep health and disorders. Chest. 2020;157(5):1304–1312. doi:10.1016/j.chest.2019.12.002
58. Moloney ME, Moga DC, Grandner M, Schoenberg N. “No rest for me tonight”: a social-ecological exploration of insomnia in rural Appalachian women. Sleep Health. 2025;11(5):717–723. doi:10.1016/j.sleh.2025.04.009
59. Buysse DJ. Sleep health: can we define it? Does it matter? Sleep. 2014;37(1):9–17. doi:10.5665/sleep.3298
60. Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s essential 8: updating and enhancing the American heart association’s construct of cardiovascular health: a presidential advisory from the American heart association. Circulation. 2022;146(5):e18–e43. doi:10.1161/cir.0000000000001078
61. St-Onge M-P, Aggarwal B, Fernandez-Mendoza J, et al. Multidimensional sleep health: definitions and implications for cardiometabolic health: a scientific statement from the American heart association. Circulation. 2025;18(5):e000139. doi:10.1161/HCQ.0000000000000139
62. Tabak RG, Kandula NR, Angell SY, et al. Implementation of evidence-based behavioral interventions for cardiovascular disease prevention in community settings: a scientific statement from the American heart association. Circulation. 2025;152(9):e75–e87. doi:10.1161/cir.0000000000001349
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Latest Advances in Non-Invasive Neurostimulation for Insomnia: A Review
Liu W, Li G
Nature and Science of Sleep 2025, 17:947-957
Published Date: 15 May 2025
Poor Sleep Quality and Mood Disorders: Risk Factors of Increasing Chronic Pain in Patients with Insomnia

Liu L, Zhao X, Zhang X, Ren J, Zeng S, Dai Y, Zhang W, Zhou J
Nature and Science of Sleep 2025, 17:1447-1457
Published Date: 23 June 2025
Improving Sleep and Daytime Function with Tryptophan, Magnesium, Melissa and Lactuca Formulation: An Exploratory Study in Adults with Sleep Disturbances
Schmitt F, Weishaupt R, Katumba PKM, Vogt D, Meyer N, Feld M, Hellhammer J
Nutrition and Dietary Supplements 2025, 17:75-85
Published Date: 7 August 2025
Magnesium Bisglycinate Supplementation in Healthy Adults Reporting Poor Sleep: A Randomized, Placebo-Controlled Trial
Schuster J, Cycelskij I, Lopresti A, Hahn A
Nature and Science of Sleep 2025, 17:2027-2040
Published Date: 30 August 2025
Sleep-Related Problems and Problematic Smartphone Use in Young Adult Males: Findings from a Short-Term Behavioral Restriction Study
Özen Gökmuharremoğlu Ö, Çoban Taşkın A
Neuropsychiatric Disease and Treatment 2026, 22:597802
Published Date: 30 April 2026