")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Quality of Life and Glucose Regulation in Pediatric Patients with Type 1 Diabetes: A Study in the Ningxia Hui Autonomous Region
Authors Bai H, He N, Zhang Y, Ahmad A, Yang XX, Ma Y, Liang LJ
Received 24 October 2023
Accepted for publication 24 February 2024
Published 12 March 2024 Volume 2024:17 Pages 1267—1278
DOI https://doi.org/10.2147/DMSO.S446387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Hua Bai,1 Na He,2 Yan Zhang,3 Aqsa Ahmad,3 Xing-Xing Yang,3 Yan Ma,3 Li-Jun Liang1
1Department of Pediatrics, General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China; 2PKUFH-NINGXIA Women Children’s Hospital, Yinchuan, 750001, People’s Republic of China; 3The First Clinical Medical College of Ningxia Medical University General Hospital, Yinchuan, 750004, People’s Republic of China
Correspondence: Li-Jun Liang, Department of Pediatrics, General Hospital of Ningxia Medical University, 804 Shengli South Street, Yinchuan, Ningxia, 750004, People’s Republic of China, Tel +86 137 0959 6527, Email [email protected]
Objective: In this study, we aimed to evaluate the current status of the quality of life (QOL) of pediatric patients and plasma glucose concentration regulation in children with type 1 diabetes (T1DM) in the Ningxia Hui autonomous region.
Methods: The study involved children with T1DM admitted to the General Hospital of Ningxia Medical University between October 2011 and October 2021. The children and their parents completed general information and quality of life (QOL) questionnaires. The regulation of plasma glucose concentration was assessed based on HbA1c levels, and plasma glucose and QOL-influencing components were investigated.
Results: Among the 136 pediatric patients diagnosed with T1DM, the mean glycated hemoglobin (HbA1c) level was recorded at 8.7% (7.2%, 10.5%). A breakdown of the patient cohort revealed that 44 patients (32.4%) demonstrated good regulation of plasma glucose, 33 patients (24.3%) exhibited acceptable glycemic control, and 59 patients (43.3%) displayed poor regulation of plasma glucose. The control of plasma glucose in pediatric patients diagnosed with T1DM was affected by the duration of the disease, the patient’s age, the frequency of daily plasma glucose measurements, the use of CGM, diabetic ketoacidosis (DKA), and the education level of the mother. The control of plasma glucose, dietary management, DKA, the ability to learn, and health education are interfering factors of quality of life in children diagnosed with T1DM. Effective control of plasma glucose may ensure the QOL in children with T1DM, and DKA was the risk factor for QOL.
Conclusion: In Ningxia, the regulation of plasma glucose in pediatric and adolescent patients with T1DM remains suboptimal, leading to poor QOL. There is a pressing need to enhance glucose regulation and QOL through comprehensive strategies, which include reinforced dietary management, rigorous monitoring of plasma glucose levels, and heightened health education levels.
Keywords: current status of regulation of plasma glucose concentration, influencing factors, QOL, type 1 diabetes
Introduction
Type 1 diabetes mellitus (T1DM) is a prevalent chronic metabolic disorder observed predominantly in children and adolescents.1 This disease emerges due to the immune-driven selective obliteration of pancreatic β-cells, influenced by both genetic predispositions and environmental factors. Characterized as an autoimmune disease, it results in absolute insulin deficiency.2 In many developed nations, patients diagnosed with T1DM constitute approximately 90% of the pediatric and adolescent diabetic population, and an upswing in cases among the youth continues to be reported.3,4 Clinical presentations of T1DM can be severe and include rapid onset of ketoacidosis, hyperosmolar hyperglycemic states, and lactic acidosis. Prolonged suboptimal glucose regulation can pave the way for microvascular complications such as diabetic retinopathy, neuropathy, and nephropathy, along with macrovascular ailments like coronary artery disease and peripheral vascular disorders.5 Given the early onset in pediatric populations, these patients are at an elevated risk of acute and chronic complications across multiple organ systems. These complications, in turn, significantly affect the health and quality of life (QOL) of pediatric patients, thereby imposing economic and societal burdens on their families.6 Existing studies underscore the pivotal role of efficacious diabetes management in preserving optimal QOL, stalling the progression of complications, and curtailing treatment costs.7–9 Therefore, along with refining glucose regulation and curtailing complications, it is imperative to enhance the QOL and prognosis.
Currently, mean glycated hemoglobin (HbA1c) levels are recognized as the definitive standard for evaluating plasma glucose regulation. Noteworthy associations have been unearthed between QOL and HbA1c levels in pediatric patients diagnosed with T1DM. A study by Frøisland et al elucidated a direct correlation between deteriorated QOL and elevated HbA1c levels.10 In a similar vein, Rechenberg et al explored correlations between plasma glucose control, self-care practices, and familial income brackets.11 Their findings underscored significantly reduced HbA1c levels in children and adolescents from affluent backgrounds compared to their counterparts from lower and middle-income families, thereby underscoring the intricate nexus between HbA1c levels and QOL. Furthermore, empirical data suggests that chronic T1DM can precipitate considerable psychological strain on affected children, manifesting in debilitating emotional responses like anxiety and depression, which severely impinge on their QOL.12
While international research landscapes are replete with studies focusing on the QOL of patients diagnosed with T1DM, there are few studies in China regarding this domain. The present study endeavors to assess both QOL and plasma glucose regulation in pediatric patients diagnosed with T1DM, concurrently dissecting the salient influencing factors. By enhancing disease awareness, optimizing glucose regulation, and assessing patient QOL, this study seeks to lay the groundwork for refined therapeutic strategies for pediatric T1DM, ultimately enhancing patient QOL.
Materials and Methods
Participants
The study involved children diagnosed with T1DM admitted to the General Hospital of Ningxia Medical University between October 2011 and October 2021.
Diagnostic Criteria
As stipulated in the “Expert Consensus on the Standardized Diagnosis and Management of Type 1 Diabetes Mellitus in Chinese Children (2020)”, a diagnosis of diabetes mellitus can be affirmed if any of the following criteria are met:13
Inclusion Criteria
Exclusion Criteria
Methods
Collection and Data Entry
Patients and guardians jointly completed the questionnaire. Data were independently entered by two persons, which were then cross-checked to ensure accuracy.
Statistical Analysis
All collected data were analyzed utilizing the SPSS 26.0 software package. Descriptive statistics for the general demographic details of the participants are represented as case numbers (n) and percentages (%). Given that neither glycated hemoglobin levels nor QOL scores followed a normal distribution, they are expressed using median values accompanied by their respective quartiles. To discern the factors impacting the plasma glucose levels and QOL, both nonparametric tests and logistic regression analyses were employed. The Pearson’s correlation analysis was used to determine relationships between various parameters, with P < 0.05 indicating statistical significance.
Results
General Information
A total of 145 questionnaires seeking information on patient demographics were disseminated. Out of these, 136 were returned, reflecting a response rate of 93.8%. From the pool of pediatric patients diagnosed with T1DM who participated, 61 were males (constituting 44.9% of the total) while 75 were females (representing 55.1% of the total). Age-wise distribution was as follows: 5 patients (3.7%) were aged 6 years or below, 90 patients (66.2%) fell in the 6 to 14-year age bracket, and 41 patients (30.1%) were aged above 14 years. Notably, a significant majority, totaling 108 patients or 79.4% of the sample, were administered treatment via continuous subcutaneous insulin infusion (CSII). Comprehensive details can be found in Table 1.
 |
Table 1 Analysis of Factors Influencing Plasma Glucose Regulation in Children Diagnosed with T1DM (M (P25, P75)) |
Status Quo of Regulation of Plasma Glucose in Patients Diagnosed with T1DM
Brief Description of Regulation of Plasma Glucose
For the 136 pediatric patients diagnosed with T1DM, the median HbA1c level was recorded at 8.7%, with an interquartile range spanning from 7.2% to 10.5%. When analyzing the plasma glucose regulation, 44 patients (32.4%) demonstrated good regulation, as evidenced by their HbA1c levels being below 7.5%; 33 patients (24.3%) exhibited acceptable regulation, with HbA1c levels ranging from 7.5% to 9.0%; and 59 patients (43.3%) manifested poor regulation, as their HbA1c levels exceeded 9.0%. It is pertinent to note that an HbA1c level of 9.0% or below was deemed indicative of effective plasma glucose regulation. Conversely, an HbA1c value surpassing 9.0% was categorized as indicative of failed regulation.
Regulation of Plasma Glucose of Groups of Age
All 5 patients younger than 6-years of age had effective glycemic management; good, moderate, and poor regulation of plasma glucose were reported in 31 cases, 28 cases, and 31 cases, respectively, among 90 patients aged 6 to 14 years; 8 out of 41 patients older than 14 years were found to have good regulation of plasma glucose, 5 had acceptable regulation, and 28 had poor regulation. Details are illustrated in Figure 1A.
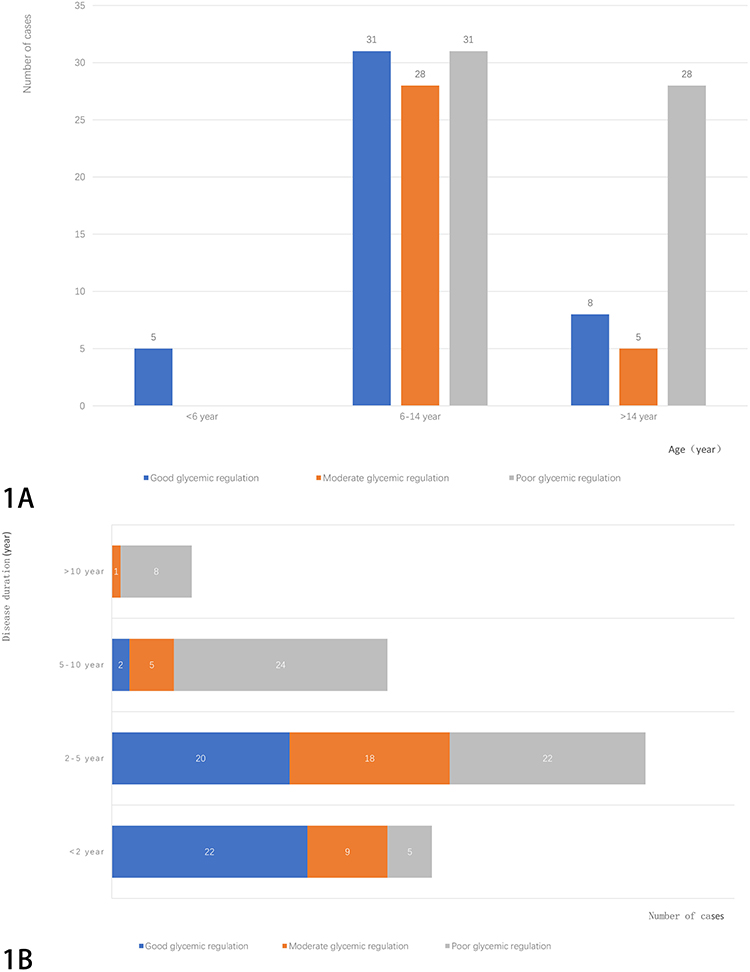 |
Figure 1 Age interval of children with T1DM (A), Regulation of plasma glucose in groups based on disease course (B). |
Regulation of Plasma Glucose Based on Disease Duration
For patients with a disease duration of ≤ 2 years (36 cases), 22 patients demonstrated good regulation, 9 patients revealed acceptable regulation, and 5 patients displayed poor regulation. In the patients with a disease duration spanning from 2 to 5 years (60 cases), 20 patients had good regulation, 18 patients manifested acceptable regulation, 22 patients evidenced poor regulation. For those with a disease course of 5 to 10 years (31 cases), only 2 patients achieved good regulation, 5 patients had acceptable regulation, while 24 patients displayed poor regulation. Among the longest duration category, with patients having a disease course exceeding 10 years (9 cases), 1 patient exhibited acceptable regulation, while the remaining 8 patients manifested poor regulation of plasma glucose. A comprehensive visual delineation of these findings, segmented by the duration of T1DM, is provided in Figure 1B.
HbA1c Distribution Based on Different Dosing Protocol
For the cohort of 108 patients undergoing continuous subcutaneous insulin infusion (CSII) therapy, the HbA1c value was reported as 8.7%, with an interquartile range from 7.2% to 10.3%. Conversely, for the 28 patients treated with multiple daily injections (MDI), the HbA1c value stood at 9.1% with an interquartile range spanning from 7.1% to 11.3%. Upon statistical comparison of the HbA1c distributions between the two treatment modalities, no statistically significant variance was observed (P > 0.05).
Analysis of Factors Affecting Regulation of Plasma Glucose in Children Diagnosed with T1DM
Based on the univariate analysis, the factors include the disease course (P < 0.001), age (P < 0.001), plasma glucose monitoring times daily (P < 0.001), use of CGM (P = 0.004), use of DKA (P=0.027), and education level of mother (P=0.003).
Survey on QOL
Results are as follows: The comprehensive assessment of the QOL yielded scores of 141.0 (128.3, 153.0) for children diagnosed with T1DM, 50.5 (45.0, 62.8) for satisfaction, and 90.0 (82.3, 98.0) for impact. The scores for the impact on interpersonal relationship, daily activity, mental state, and physiological activities were 13.0 (10.0, 15.0), 16.0 (13.0, 19.8), 24.0 (21.0, 27.0), 26.0 (22.0, 30.0), 11.0 (9.0, 13.0) respectively.
QOL for Different Plasma Glucose Regulation Levels
The QOL scores were 138.5 (124.0, 143.0), 141.0 (133.5, 151.0), and 144.0 (127.0, 173.0) for the groups with good, acceptable, and poor regulation, indicating significant difference in score among the three groups (P = 0.039). Figure 2 displays the line chart of the median QOL score (M) for the groups based on plasma glucose regulation.
 |
Figure 2 Median QOL score of children diagnosed with T1DM in groups based on of plasma glucose regulation. |
Impact of Plasma Glucose Regulation on Impact, Satisfaction, and Overall Score in Children Diagnosed withT1DM
In comparison to the group with poor regulation of plasma glucose, the group with effective regulation of plasma glucose had significantly lower scores for the impact on interpersonal relationships (P = 0.002), daily activities (P = 0.033), mental state (P = 0.007), and physiological activities (P = 0.036), impact of treatment on patients in 5 aspects (P = 0.003), impact of treatment on patients (P < 0.001), and overall score (P = 0.041). Although the QOL was greater in the group with successful glucose regulation compared to the group with poor glucose regulation, there was no significant difference in satisfaction between the two groups (P = 0.757). The detailed information is provided in Table 2 and Table 3.
 |
Table 2 Impact of Plasma Glucose Regulation on Influence, Satisfaction, and Overall Score in Children Diagnosed with T1DM |
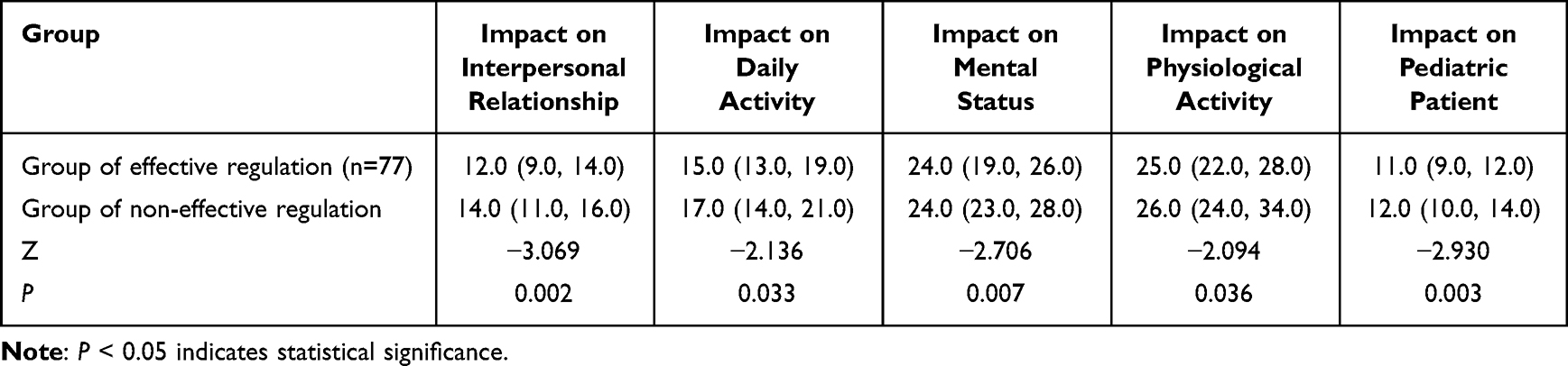 |
Table 3 Influence of Plasma Glucose Regulation on Different Aspects |
Pearson’s Correlation Analysis on Sub-Scores of QOL and HbA1c
There was a significant correlation between the HbA1c and the following: QOL score (rimpact = 0.431, P < 0.001), score of impact with respect to 5 aspects (rinterpersonal relationship = 0.254, P = 0.003; rdaily activities= 0.228, P = 0.008; rmental status = 0.336, P < 0.001; rphysiological activities = 0.349, P < 0.001; rimpact on pediatric patient = 0.343, P < 0.001) and overall score (roverall= 0.300, P < 0.001).
Univariate Analysis of QOL of Children with T1DM
Univariate analysis revealed that the factors influencing the QOL in children with T1DM were plasma glucose regulation (P = 0.041), diet management (P = 0.041), DKA (P = 0.046) and health education (P = 0.046). Details are listed in Table 4.
 |
Table 4 Descriptive Analysis of QOL in Children Diagnosed with T1DM (M (P25, P75)) |
Univariate Analysis of QOL of Children Diagnosed with T1DM
The overall QOL score was compared with the median value of 141.0 by transforming the score into a binary variable. If the QOL score of a patient was below this median, it was classified as “low”. Conversely, scores exceeding the median were deemed “high”. A binomial logistic regression analysis was conducted using these binary classifications. Based on the results of the analysis, effective regulation of plasma glucose was positively associated with the maintenance of a satisfactory QOL in children diagnosed with T1DM (P = 0.017, OR = 0.389, 95% CI: 0.179–0.843), and DKA was the risk factor for the QOL of children with T1DM (P = 0.034, OR = 2.424, 95% CI: 1.068–5.504). Details are provided in Table 5.
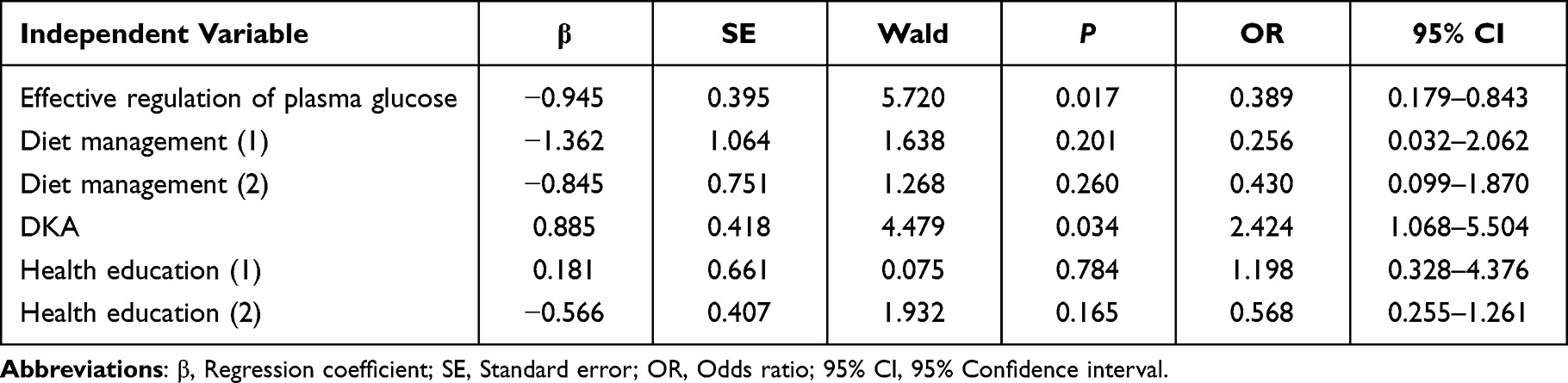 |
Table 5 Multivariate Analysis of QOL in Children Diagnosed with T1DM |
Discussion
The current therapeutic approach to T1DM aims to maintain optimal plasma glucose regulation and delay or prevent the onset of complications. HbA1c serves as the benchmark for assessing plasma glucose regulation. For pediatric patients diagnosed with T1DM, an HbA1c level below 7.5% is targeted.15 However, data spanning the past decade has shown an elevation in HbA1c levels from 7.8% (2010–2012) to 8.4% (2016–2018), indicating no significant improvement in plasma glucose regulation.16,17 In China, more than half of the younger demographic struggles to maintain acceptable plasma glucose levels.18 Of the 136 surveyed children diagnosed with T1DM, plasma glucose regulation results were as follows: 44 (32.4%) had good regulation, 33 (24.3%) had acceptable regulation, and 59 (43.3%) had poor regulation. This clearly portrays a significant challenge in regulating plasma glucose in pediatric patients diagnosed with T1DM in Ningxia.
Multiple factors could contribute to this. The secretion of growth hormone during puberty can induce insulin resistance, affecting plasma glucose regulation.19 Younger patients often face challenges with compliance and self-management due to their age, impacting diet management among other factors. Over an extended treatment period, caregivers and parents may develop negative attitudes, given the myriad precautions and challenges they confront, exacerbating the disease complications. Moreover, our study noted a trend where plasma glucose regulation deteriorated as the duration of the disease increased. In patients with a disease history exceeding 10 years, regulation was primarily poor. The shorter the disease course, the less the HbA1c, which is consistent with the results reported by Malerbi et al.20
Although parenteral insulin remains the primary therapeutic intervention for pediatric patients diagnosed with T1DM, treatment should be tailored to the patient, accounting for their age, physiological state, and daily routine. While CSII is commonly adopted by around 63% of pediatric patients diagnosed with T1DM in the USA and 5–15% in Europe, research by Pickup et al indicated that CSII enhanced plasma glucose regulation in pediatric patients diagnosed with T1DM.17,21,22 In our study, although CSII was linked with a slightly lower median HbA1c than MDI, the difference was not statistically significant, potentially due to the underrepresentation of MDI-receiving children.
Plasma glucose regulation is influenced by a plethora of factors. Our study identified several factors affecting this in pediatric patients diagnosed with T1DM, including the duration of the disease, patient age, frequency of plasma glucose monitoring per day, CGM, DKA, and the educational level of the mother.
Aeppli et al discovered that pediatric patients aged between 0 to 4 years exhibited effective regulation of plasma glucose within a span of five years post-diagnosis, implying a potential correlation between the trajectory of the disease and plasma glucose modulation.23 Further studies have indicated that T1DM concomitant with DKA correlates with prolonged suboptimal plasma glucose regulation in pediatric patients.24 Our own research identified a significant relationship between HbA1c concentrations and the presence of DKA. Additionally, the outcomes of our investigation revealed a discernible influence of the daily self-monitoring of blood glucose (SMBG) frequency on the regulation of plasma glucose levels. A plausible explanation is that frequent SMBG potentially serves as a reminder for patients to promptly regulate their plasma glucose through interventions such as dietary adjustments, physical activity, and appropriate insulin administration, subsequently optimizing HbA1c levels. In research focusing on pediatric patients diagnosed with T1DM, it was observed that an escalation in daily SMBG correlated with a notable decline in HbA1c levels and a decreased onset of acute sequelae like ketoacidosis.25 CGM is an innovative tool proficient in perpetually monitoring glucose concentrations in interstitial and subcutaneous tissues.26 This device not only exhibits instantaneous plasma glucose readings and their respective trends but also incorporates alert systems, rendering it crucial for T1DM patient management. Empirical evidence suggests that CGM aids in fine-tuning plasma glucose regulation, aligning with previous scholarly findings.27–30 Furthermore, the educational level of parents seems to have a consequential impact on the plasma glucose modulation in pediatric patients diagnosed with T1DM. Research conducted by AlAgha et al postulated that higher paternal educational level may be linked to enhanced plasma glucose regulation in children (reflected by HbA1c < 7%).31 Conversely, a lower educational level could be associated with suboptimal regulation. Wu et al inferred that the educational status of the parents significantly influences the plasma glucose regulation of children.32 Parents possessing advanced educational qualifications appear to exhibit heightened awareness regarding the implications of T1DM and the imperative nature of continuous glucose monitoring and management. In our findings, maternal education demonstrated a pronounced association with plasma glucose variations, whereas paternal education did not elicit a similar effect. This discrepancy may be attributed to the predominant role mothers tend to play in managing the treatment regimen of children diagnosed with T1DM.
Currently, the PedsQLTM instrument, developed by Varni et al at the Children’s Hospital and Health Center in San Diego, California, is extensively used in China to assess the QOL of children and adolescents diagnosed with T1DM.33 However, considering the pronounced disparities in dietary preferences, cultural backgrounds, lifestyles, and educational norms between Chinese and American children, there is a contention regarding the aptness of the PedsQLTM for the Chinese demographic. To cater to this specific context, and to more accurately gauge the QOL of pediatric patients diagnosed with T1DM, the “Questionnaire on Quality of Life of Children and Adolescents with Diabetes Mellitus in Chongqin”, designed by Prof. Zheng Lingling, was employed in our investigation.14
Our findings highlighted several factors influencing the QOL of children with T1DM. These encompassed aspects such as plasma glucose control, dietary management, the occurrence of DKA, the cognitive abilities of the child, and the provision of health education. Among these, proficient regulation of plasma glucose emerged as pivotal for maintaining optimal QOL. Conversely, the incidence of DKA was identified as a risk factor negatively affecting T1DM QOL. Corroborating studies have showcased an association between superior plasma glucose regulation and enhanced QOL.34 Evidently, children diagnosed with T1DM exhibiting inferior QOL typically manifested elevated HbA1c levels. Contrarily, those with reduced HbA1c levels not only demonstrated heightened QOL cognizance but also reduced vulnerability to acute complications, bolstering their overall QOL score.35 Relative to their healthy peers, children and adolescents with T1DM exhibited an increased propensity toward psychosocial challenges such as depression and anxiety. These mental health parameters, in turn, could potentially impinge upon both plasma glucose regulation and QOL.36 Our research ascertained diminished QOL in children diagnosed with T1DM with suboptimal plasma glucose regulation, juxtaposed against their better-regulated counterparts. Yet, it is paramount to note the nuanced relationship between reduced HbA1c levels and the holistic health perception, which typically corresponds to diminished disease impact, decreased anxiety, amplified satisfaction, and an augmented health cognizance. Moreover, daily routines, including dietary habits and glucose regulation, emerged as integral to QOL. Pervasive non-compliant diets and sedentary lifestyles predispose patients with T1DM to inferior plasma glucose regulation and resultant complications.37 Unquestionably, comprehensive and continuous interventions are mandated for patients diagnosed with T1DM to forestall extended or latent complications.
A study conducted by Zhu underlined correlations between the QOL of pediatric patients diagnosed with T1DM and factors such as age, disease duration, educational attainment, familial income, the quality of the parent-child bond, and the marital status of the parents—findings that resonated with ours38 Intriguingly, compared to an employed mother with advanced education, a lesser-educated mother might dedicate more time to overseeing the dietary and therapeutic needs of a T1DM child, ostensibly elevating the QOL of the children. Elevated parental expectations for academically proficient children could lead to more assiduous T1DM management. Socioeconomic factors, including parental unemployment, constrained income, and limited familial support, ostensibly undermine QOL. Compounded by poor glucose regulation and depressive symptoms, these socio-economic determinants exacerbate QOL degradation. Hence, while formulating T1DM management strategies, it is imperative to integrate socio-psychological considerations.
Limitation
The patient collection time is long, and the questionnaire is filled out jointly by the family members who take care of the child for a long time. Therefore, due to the cognitive differences between parents of different generations, there might be certain subjective biases.
Conclusion
The level of plasma glucose control in children and adolescents with T1DM in Ningxia is poor, and the QOL is lower. Several factors influence the control of plasma glucose in these patients, encompassing the duration of the disease, the age of the patients, the frequency of daily plasma glucose monitoring, the use of CGM, DKA, and the educational level of the mother. Various factors, such as plasma glucose control, dietary management, DKA, the ability to learn of the patients, and health education, are intrinsically linked to the QOL. To ameliorate both plasma glucose regulation and QOL, there is a need to fortify initiatives related to dietary management, meticulous monitoring of plasma glucose levels, and comprehensive health education.
Abbreviations
T1DM, Type 1 Diabetes Mellitus; QOL, Quality of Life; HbA1c, Glycosylated Hemoglobin; CGM, Continuous Glucose Monitoring; DKA, Diabetic Ketoacidosis; OGTT, Oral glucose tolerance test; CSII, Continuous Subcutaneous Insulin Infusion; MDI, Multiple Daily Injections; SMBG, Self-Monitoring of Blood Glucose.
Data Sharing Statement
We declared that materials described in the manuscript, including all relevant raw data, will be freely available to any scientist wishing to use them for non-commercial purposes, without breaching participant confidentiality.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Medical research Ethics Review Committee of General Hospital of Ningxia Medical University (No. KYLL-2022-0242). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Disclosure
The authors declare that they have no competing interests.
References
1. Li H, Shi L. Advances in the diagnosis and treatment of type 1 diabetes. Chin J Diabetes. 2016;10:4. doi:10.3760/cma.j.issn.1674-5809.2016.10.004
2. Warshauer JT, Bluestone JA, Anderson MS. New frontiers in the treatment of type 1 diabetes. Cell Metab. 2020;31(1):46–61. doi:10.1016/j.cmet.2019.11.017
3. Mayer-Davis EJ, Kahkoska AR, Jefferies C, et al. ISPAD clinical practice consensus guidelines 2018: definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2018;19(Suppl 27):7–19. doi:10.1111/pedi.12773
4. Adeloye D, Chan KY, Thorley N, et al. Global and regional estimates of the morbidity due to type I diabetes among children aged 0–4 years: a systematic review and analysis. J Glob Health. 2018;8(2):021101. doi:10.7189/jogh.08.021101
5. McLarty RP, Alloyce JP, Chitema GG, Msuya LJ. Glycemic control, associated factors, acute complications of Type 1 Diabetes Mellitus in children, adolescents and young adults in Tanzania. Endocrinol Diabetes Metab. 2020;4(2):e00200. doi:10.1002/edm2.200
6. Weng Z. The Study on the Levels of Serum NO, ICAM-1 and VCAM-1 in Children with Type 1 Diabetes Mellitus in Different Course. Dalian Medical University; 2022. doi:10.26994/d.cnki.gdlyu.2021.001082
7. American Diabetes Association. 4. Lifestyle management: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl 1):S38–S50. doi:10.2337/dc18-S004
8. American Diabetes Association. 8. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl 1):S73–S85. doi:10.2337/dc18-S008
9. Davies MJ, D’Alessio DA, Fradkin J, et al; Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669–2701. doi:10.2337/dci18-0033
10. Frøisland DH, Graue M, Markestad T, Skrivarhaug T, Wentzel-Larsen T, Dahl-Jørgensen K. Health-related quality of life among Norwegian children and adolescents with type 1 diabetes on intensive insulin treatment: a population-based study. Acta Paediatr. 2013;102(9):889–895. doi:10.1111/apa.12312
11. Rechenberg K, Whittemore R, Grey M, Jaser S; TeenCOPE Research Group. Contribution of income to self-management and health outcomes in pediatric type 1 diabetes. Pediatr Diabetes. 2016;17(2):120–126. doi:10.1111/pedi.12240
12. Matziou V, Tsoumakas K, Vlahioti E, et al. Factors influencing the quality of life of young patients with diabetes. J Diabetes. 2011;3(1):82–90. doi:10.1111/j.1753-0407.2010.00106.x
13. Buse JB. Expert consensus on standardized diagnosis and treatment of type 1 diabetes in children in China (2020 edition). Chin J Pediatr. 2020;58(6):447–454. doi:10.3760/cma.j.cn112140-20200221-00124
14. Zheng L. Evaluation Quality of Life in Children and Adolescents with Diabetes Living in Chongqing. Chongqing Medical University; 2011.
15. Rewers M, Pihoker C, Donaghue K, Hanas R, Swift P, Klingensmith GJ. Assessment and monitoring of glycemic control in children and adolescents with diabetes. Pediatr Diabetes. 2009;10(Suppl 12):71–81. doi:10.1111/j.1399-5448.2009.00582.x
16. Miller KM, Foster NC, Beck RW, et al. Current state of type 1 diabetes treatment in the US: updated data from the T1D Exchange clinic registry. Diabetes Care. 2015;38(6):971–978. doi:10.2337/dc15-0078
17. Foster NC, Beck RW, Miller KM, et al. State of type 1 diabetes management and outcomes from the T1D Exchange in 2016–2018 [published correction appears in Diabetes Technol Ther. 2019 Apr; 21(4):230]. Diabetes Technol Ther. 2019;21(2):66–72. doi:10.1089/dia.2018.0384
18. McGuire HC, Ji L, Kissimova-Skarbek K, et al. Type 1 diabetes mellitus care and education in China: the 3C study of coverage, cost, and care in Beijing and Shantou. Diabet Res Clin Pract. 2017;129:32–42. doi:10.1016/j.diabres.2017.02.027
19. Hood KK, Peterson CM, Rohan JM, Drotar D. Association between adherence and glycemic control in pediatric type 1 diabetes: a meta-analysis. Pediatrics. 2009;124(6):e1171–e1179. doi:10.1542/peds.2009-0207
20. Malerbi FE, Negrato CA, Gomes MB; Brazilian Type 1 Diabetes Study Group (BrazDiab1SG). Assessment of psychosocial variables by parents of youth with type 1 diabetes mellitus. Diabetol Metab Syndr. 2012;4(1):48. doi:10.1186/1758-5996-4-48
21. Naranjo D, Tanenbaum ML, Iturralde E, Hood KK. Diabetes technology: uptake, outcomes, barriers, and the intersection with distress. J Diabetes Sci Technol. 2016;10(4):852–858. doi:10.1177/1932296816650900
22. Pickup JC. Is insulin pump therapy effective in type 1 diabetes? Diabet Med. 2019;36(3):269–278. doi:10.1111/dme.13793
23. Aeppli TRJ, Mahler FL, Konrad D. Future glycemic control of children diagnosed with type 1 diabetes mellitus at toddler and preschool/school age. J Pediatr Endocrinol Metab. 2019;32(9):929–933. doi:10.1515/jpem-2019-0152
24. Duca LM, Wang B, Rewers M, Rewers A. Diabetic ketoacidosis at diagnosis of type 1 diabetes predicts poor long-term glycemic control. Diabetes Care. 2017;40(9):1249–1255. doi:10.2337/dc17-0558
25. Selvan C, Thukral A, Dutta D, Ghosh S, Chowdhury S. Impact of self-monitoring of blood glucose log reliability on long-term glycemic outcomes in children with type 1 diabetes. Indian J Endocrinol Metab. 2017;21(3):382–386. doi:10.4103/ijem.IJEM_342_16
26. Hoss U, Budiman ES. Factory-calibrated continuous glucose sensors: the science behind the technology. Diabetes Technol Ther. 2017;19(S2):S44–S50. doi:10.1089/dia.2017.0025
27. Dover AR, Stimson RH, Zammitt NN, Gibb FW. Flash glucose monitoring improves outcomes in a type 1 diabetes clinic. J Diabetes Sci Technol. 2017;11(2):442–443. doi:10.1177/1932296816661560
28. Al Hayek AA, Al Dawish MA. Assessing diabetes distress and sleep quality in young adults with type 1 diabetes using freestyle libre: a prospective cohort study. Diabetes Ther. 2020;11(7):1551–1562. doi:10.1007/s13300-020-00849-3
29. Al Hayek AA, Robert AA, Al Dawish MA. Evaluation of freestyle libre flash glucose monitoring system on glycemic control, health-related quality of life, and fear of hypoglycemia in patients with type 1 diabetes. Clin Med Insights Endocrinol Diabetes. 2017;10:1179551417746957. doi:10.1177/1179551417746957
30. Dunn TC, Xu Y, Hayter G, Ajjan RA. Real-world flash glucose monitoring patterns and associations between self-monitoring frequency and glycaemic measures: a European analysis of over 60 million glucose tests. Diabet Res Clin Pract. 2018;137:37–46. doi:10.1016/j.diabres.2017.12.015
31. AlAgha M A, Majdi W M, Aljefri HM, et al. Effect of parents’ educational level and occupational status on child glycemic control. J Patient Care. 2017;3(2):1–3. doi:10.4172/2573-4598.1000130
32. Wu T, Chen F, He Q, et al. Status quo and influencing factors of out-of-hospital blood glucose control in 118 children with type 1 diabetes. Chin General Pract Nurs. 2021;19(5):708–710. doi:10.12104/j.issn.1674-4748.2021.05.040
33. Varni JW, Burwinkle TM, Jacobs JR, Gottschalk M, Kaufman F, Jones KL. The PedsQL in type 1 and type 2 diabetes: reliability and validity of the Pediatric Quality of Life Inventory Generic Core Scales and type 1 Diabetes Module. Diabetes Care. 2003;26(3):631–637. doi:10.2337/diacare.26.3.631
34. Kalyva E, Malakonaki E, Eiser C, Mamoulakis D. Health-related quality of life (HRQoL) of children with type 1 diabetes mellitus (T1DM): self and parental perceptions. Pediatr Diabetes. 2011;12(1):34–40. doi:10.1111/j.1399-5448.2010.00653.x
35. Song H, Dong X, Chen Z, et al. Investigation and analysis of glycemic control and quality of life in children and adolescents with type 1 diabetes od Qingdao. Chin J Child Health Care. 2017;25(05):459–462. doi:10.11852/zgetbjzz2017-25-05-08
36. Paul J, Jani R, Davoren P, Knight-Agarwal C. Association between a low carbohydrate diet, quality of life, and glycemic control in Australian adults living with type 1 diabetes: protocol for a Mixed Methods Pilot Study. JMIR Res Protoc. 2021;10(3):e25085. doi:10.2196/25085
37. Mozzillo E, Zito E, Maffeis C, et al. Unhealthy lifestyle habits and diabetes-specific health-related quality of life in youths with type 1 diabetes. Acta Diabetol. 2017;54(12):1073–1080. doi:10.1007/s00592-017-1051-5
38. Zhu G. QOL satisfaction in children and adolescents with type I diabetes and its influencing factors. Diabetes World. 2020;17(7):177.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.