Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Quality Improvement in Stroke Rehabilitation: A Scoping Review
Authors Shafei I, Karnon J, Crotty M
Received 23 September 2022
Accepted for publication 30 November 2022
Published 22 December 2022 Volume 2022:15 Pages 2913—2931
DOI https://doi.org/10.2147/JMDH.S389567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ingy Shafei,1,2 Jonathan Karnon,1,3 Maria Crotty3
1School of Public Health, Faculty of Health and Medical Sciences, The University of Adelaide, Adelaide, South Australia, Australia; 2College of Business, Government and Law, Flinders University, Adelaide, South Australia, Australia; 3College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia
Correspondence: Ingy Shafei, Faculty of Health and Medical Sciences, The University of Adelaide, GPO Box 2100, Adelaide, South Australia, 5001, Australia, Tel +61 0458715670, Email [email protected]
Background: Quality improvement interventions are used extensively in health care, aiming to improve delivery and promote best practice. The impact of quality improvement interventions implemented in stroke rehabilitation remains unclear.
Objective: The aim of this scoping review is to examine the different types of published quality improvement interventions in stroke rehabilitation and their impact on improving the quality of care.
Materials and Methods: A scoping review was performed in the PubMed, Embase and CINAHL databases. QI studies evaluating interventions for stroke rehabilitation patients that were published up to August 2020 were included. The review looked at the types of quality improvement interventions that have been evaluated as well as the improvements/impacts reported for quality improvement interventions for stroke patients in rehabilitation.
Results: We reviewed 1580 studies, twelve quality improvement interventions met inclusion criteria and were included in the current study. Six studies involved organizational change, three studies involved provider education and audit-feedback and three studies involved provider education. Of the twelve quality improvement interventions that have been included, > 90% reported improvements (91.6%). In the majority of cases, improvements were noted through implementation of a myriad of interventions. Several facilitators and barriers were noted during implementation and contributed to success or failure of the intervention.
Conclusion: There is paucity of full-text peer-reviewed published research investigating quality improvement interventions for improving the quality of care in stroke rehabilitation. The current review offers value to healthcare providers in terms of key success factors, contextual factors, barriers and facilitators associated with improvements in stroke rehabilitation.
Keywords: scoping review, review, stroke rehabilitation, quality improvement, quality interventions
Introduction
There is clear evidence on the gap between effective practice (obtained from evidence and research) and what happens in practice. This variation in practice has a significant impact on patient outcomes and processes of care.1 Poor quality of care has attributed to nearly 60% (5 Million of the 8.6 million deaths) preventable through health care.2 Decreasing unwarranted variations in clinical practice is important both from a safety and a quality perspective.1 Healthcare leaders use quality improvement (QI) interventions to improve the delivery of healthcare services and promote best practice implementation, thus contributing significantly to greater efficiencies in healthcare delivery.1 Principles and benefits of quality improvement (QI) have been well established through literature and practice. While typically the health sector was slow in embracing quality initiatives, in the more recent years, QI approaches have become more widespread with the use of different approaches to enact change and improvement.3
Many strategies have been proposed to improve quality amongst healthcare providers, including greater standardization of processes and using a myriad of strategies ensuring evidence-based practices are applied in the organization, thus contributing significantly to greater efficiencies in healthcare delivery. Bravata et al in “Closing the Gap” series defined QI strategies as
Interventions aimed at reducing the quality gap the difference between health care processes or outcomes observed in practice and those potentially obtainable on the basis of current professional knowledge for a group of patients representative of those encountered in routine practice.
The authors developed a taxonomy of nine QI strategies, including patient and provider education, organizational change, audit and feedback, patient and provider reminders, transfer of clinical data to providers, incentives including financial and legislative, and encouraging self-monitoring or self-management.4 In addition, developing and putting clinical guidelines and evidence-based pathways into practice also contribute towards decreasing unwanted variation and despite having guidelines in place, unwanted variation still exists.1
Furthermore, contextual factors have been ascertained to influence QI success and the Model for Understanding Success in Quality (MUSIQ) details such contextual factors for health. MUSIQ extolls QI implementers undergoing efforts throughout the QI initiatives to optimize contextual factors for the success and effectiveness of QI initiatives.5 Contextual factors are further categorized into external factors (external motivators, project sponsorships), organizational factors (leadership, senior leader sponsorship, culture, maturity of QI, physician payment structures) microsystem (leadership, culture, capability for improvement, motivation), as well as QI support and capacity (data infrastructure, resource availability, workforce focus), QI team (diversity, physician involvement, expertise, team tenure, prior experience in QI, leadership, decision-making process, QI skills and team norms), and some miscellaneous factors (eg, triggering events, importance of QI tasks).5 Implementation teams typically involve multiple stakeholders and cross-functional teams of medical teams, administration staff, consumers of health care, pharmacists and many others.6 Another key to quality improvements in health is involvement of frontline workers where health care is delivered.2
Stroke is a healthcare condition that is prevalent and disabling. It is the second most common cause of death in many countries.7 In addition, the economic consequence of stroke is enormous with annual costs estimated to be $320.1 billion globally for stroke and cardiovascular disease.8 One of the main issues with stroke is the resultant acquired disability. While most patients survive the initial stroke episode, there are usually longer term consequences and acquired adult disabilities that occur.7 The majority of post-stroke care is dependent on accessing rehabilitation, which has a significant effect in reducing mortality and dependency. Stroke rehabilitation typically follows a cyclical process that involves assessment, goal-setting, intervention and reassessment.7
Given previous studies of QI programs across many medical specialties, it is clear that rehabilitation services are particularly primed to benefit from such programs. Typically, in both acute and subacute rehabilitation facilities, outcome measurements are used for measuring quality, while many factors including multidisciplinary team members, goal setting, communication, the appropriateness of care among others are critical to patient needs.9 However, there is limited evidence in literature as to the QI initiatives and indicators for stroke rehabilitation.10,11 In addition, despite the interest in QI in healthcare context, there is a gap in research with little published literature evaluating the use of QI and its impacts within medical contexts, where success was seen and what changes have been observed due to QI.12 A search for existing reviews on this topic was performed. This included the Joanna Briggs Institute (JBI) Database of Systematic Reviews and Implementation Reports, the Cochrane Database of Systematic Reviews, MEDLINE and CINAHL. No relevant reviews (published or in progress) were identified. Thus, to address this gap in literature, the reported study aims to perform a scoping review to assess the extent to which QI interventions have been reported for stroke patients in rehabilitation, as well as the reported impacts of QI interventions on the rehabilitation of stroke patients.
Methods
Objectives
The objective of the scoping review is to identify and examine the available literature on quality improvement interventions utilized for stroke patients in rehabilitation. The review questions include:
- What QI interventions have been evaluated for stroke patients in rehabilitation?
- What improvements/impacts have been reported for quality improvement interventions for stroke patients in rehabilitation?
- What were the reported barriers and facilitators to the QI interventions improving the quality of care for stroke patients in rehabilitation?
To date, there is no review focused on quality improvement interventions for stroke rehabilitation, their impact on improving the quality of care and the facilitators and barriers to the QI interventions improving quality of care. Given the potential impacts of QI interventions on patient outcomes and processes of care, the current study aimed to address the gap.
Search Strategy
The researchers conducted a scoping review using the Joanna Briggs Institute (JBI) methodology for scoping reviews. Databases searched for scholarly peer-reviewed articles included PubMed and Academic Search Complete/EBCSCO, Embase, CINAHL, JBI Library, Cochrane Library and Grey Literature sources including Google Scholar, Open-Grey and the Grey Literature Report.
Included were studies that evaluated quality improvement interventions for stroke rehabilitation patients that were published from the inception of the databases to August 2020. Data was extracted by one reviewer, and thirty percent of the studies were verified by the second reviewer.
An initial search of PubMed, Academic Search Complete/EBCSCO and CINAHL was done, followed by analysis of the text words in the title and abstract and of the index terms used to describe articles. Secondly, another search was undertaken utilizing the identified keywords and index terms across relevant databases. Thirdly, the reference lists of selected studies were searched for other relevant articles. All studies irrespective of their date of publication were considered for inclusion in the review. Studies translated into English were also considered for inclusion in the review.
The search terms were composed of two constructs. The first construct related to population and was limited to studies focusing on stroke rehabilitation. The second construct related to the intervention and was limited to implementation of a quality improvement intervention. A combination of the two constructs was used to conduct the search. The search strategy used in each of the three databases is detailed in Appendix A.
Inclusion and Exclusion Criteria
Inclusion criteria considered the participants, the concept, quality rating and the context of the studies. To be included, the study must include a QI intervention applied within the area of stroke rehabilitation. QI interventions were defined utilizing the nine definitions of the QI strategies used in the “Closing the Gap” series.4 Facilitators and barriers were categorized utilizing the Model for Understanding Success in Quality (MUSIQ), which ascertains 25 contextual factors that could influence QI success.5 There were no exclusions to any healthcare settings and geographic areas. Studies from high- as well as low- and middle-income countries were considered. In addition, the review considered all types of qualitative and quantitative studies of QI interventions in health care including non-randomized controlled studies, quasi-experimental/before and after studies, prospective and retrospective cohort studies, case–control studies, cross-sectional studies and observational studies. The review also considered descriptive epidemiological study designs such as case series, individual case reports and descriptive cross-sectional studies as well as systematic reviews and literature reviews that meet the criteria. Excluded studies included studies that did not include a quality improvement intervention, or only considered organizational audits with no quality improvement intervention, or only considered guideline adherence with no quality improvement intervention, or only looked at the design of a quality improvement intervention or developed a tool and did not include the quality improvement intervention or only implemented a new model of care with no quality improvement intervention.
Quality Rating
All papers that met inclusion criteria were appraised by two independent critical appraisers for methodological quality. Methodological quality was based on using the standardized critical appraisal instruments for Qualitative Research, Quasi-Experimental Studies and Randomized Controlled Trials from JBI to ensure the extent to which studies dealt with the likelihood of bias in design, conduct and analysis.
Results
The initial search yielded 1580 studies. After removing duplicates (146), citations were imported into Rayyan. Both reviewers screened all titles only to determine relevance resulting in 174 articles selected and 1260 excluded. Both reviewers (IS & JK) then reviewed and assessed all titles and abstracts in Rayyan resulting in excluding 135 articles, with 39 remaining. Full-text articles were obtained for included articles. Reviewers excluded 27 studies as per eligibility criteria. No authors were contacted for additional information. Twelve articles remained for inclusion in the current study as demonstrated in PRISMA Diagram in Figure 1.
 |
Figure 1 PRISMA diagram. Notes: PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health careinterventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons.13 |
Synthesis of Results and Methods of Analysis
Twelve peer-reviewed journal articles were included. Study characteristics (author, year, location, study design, population, intervention details and primary outcomes) are described in Table 1. Narrative descriptions of the studies are provided.
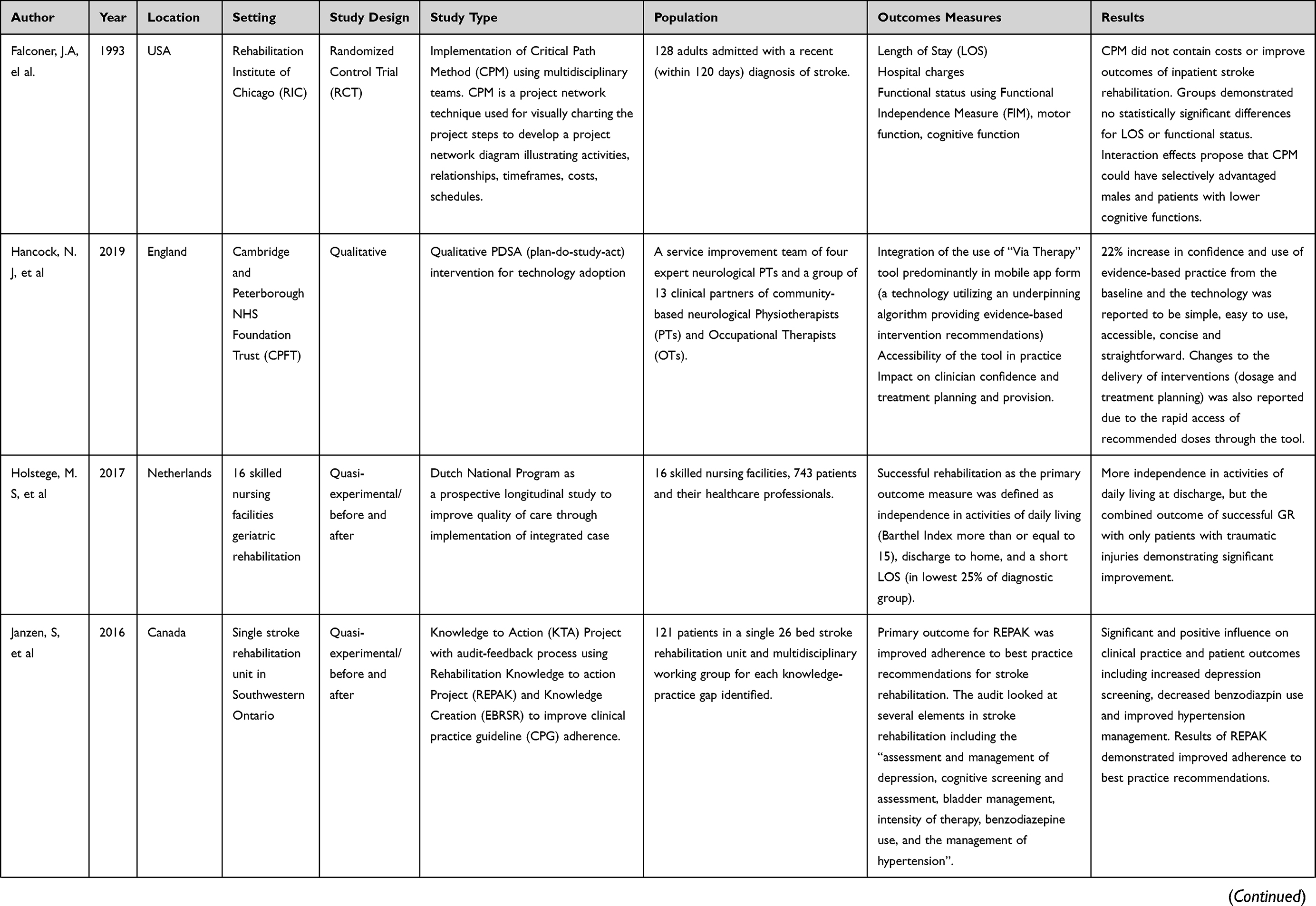 | 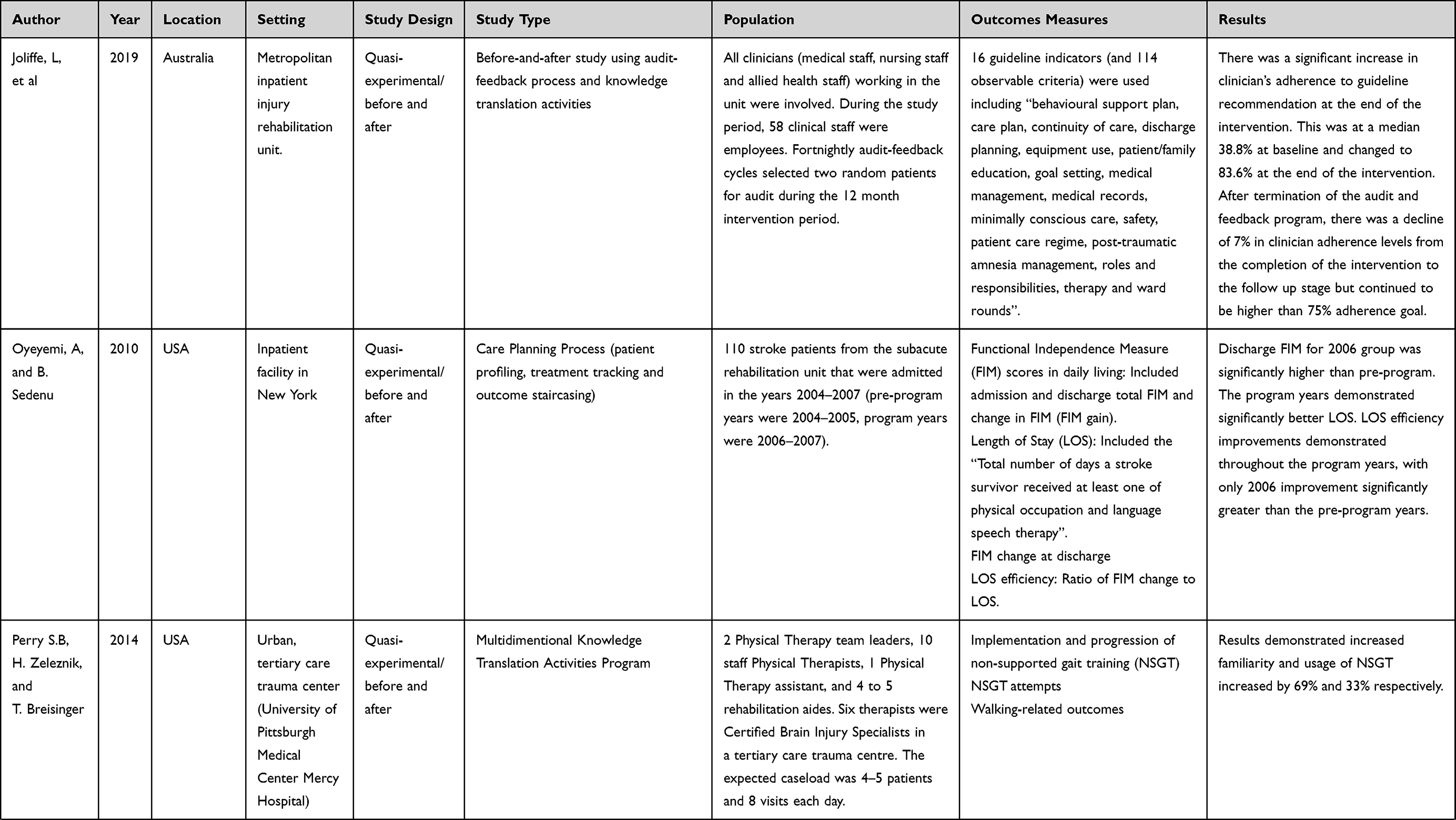 | 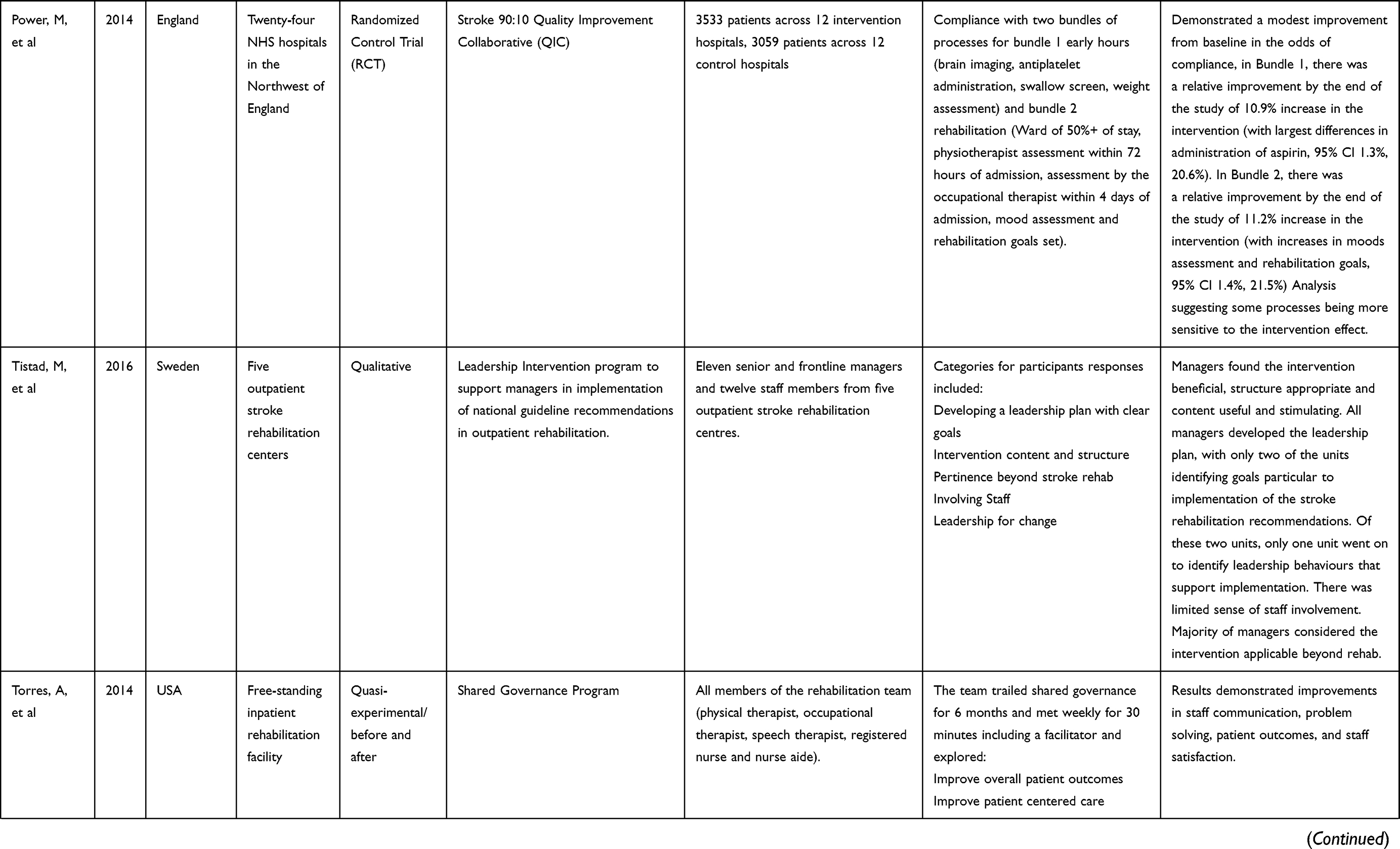 | 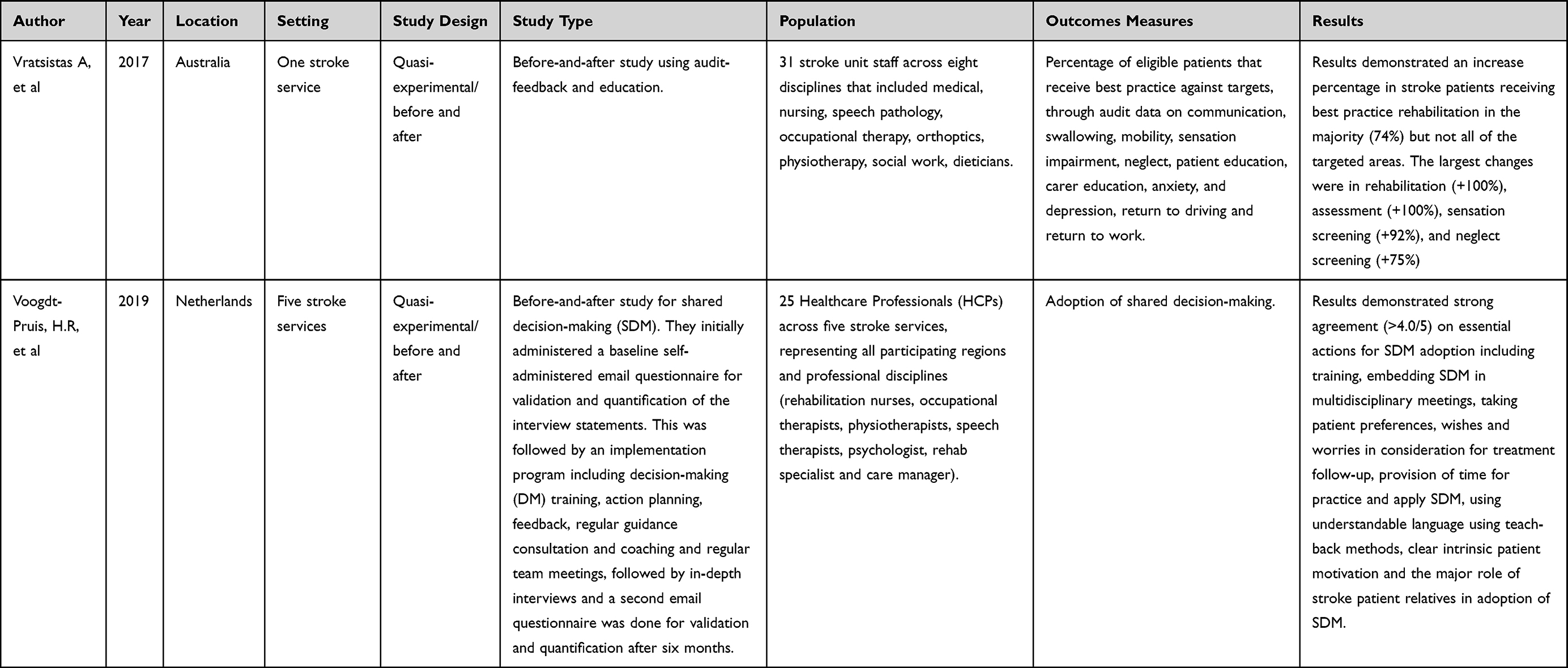 |
Table 1 Study Characteristics (Design, Type, Population and Primary Outcomes) |
Results of Search
The search was purposively broad aiming to scope the current literature, and the included studies were published between 1993 and 2020, with 9 of the 12 (75%) studies published in the last five years. The studies were located in North America; USA and Canada14–19 as well as Europe; Sweden, England and the Netherlands20–23 and Australia.24,25
Bravata et al’s QI definitions4 were used for the quality interventions, the included studies evaluated interventions involving Organizational Change,14–17,20,22 Provider Education and Audit-Feedback process19,24,25 and Provider Education.18,21,23
Study Methods and Results
Twelve studies were included, and study intervention descriptors are summarized in Table 1. One study demonstrated no improvement in patient outcomes with the QI intervention15, and eleven studies demonstrated improvements following program implementation.14,16–25 Results of the study demonstrated a wide variety and heterogeneity of QI initiatives in stroke rehabilitation; thus, a narrative approach was undertaken in the analysis to address the first and second research question on the types of QI interventions that have been evaluated for stroke patients in rehabilitation and their improvements and impacts and summarised in Tables 1 and 2.
 |  |  |  |
Table 2 Summary of Abstracts on Quality Interventions in Stroke Rehabilitation |
Two studies involved clinician education QI interventions.18,21 Clinician/provider education includes any intervention that encompasses any of educational workshops, meetings, lectures, educational outreach visits, or distribution of educational materials.4 One study,18 looked at multidimensional knowledge translation activities, defined as a process for “moving research findings into action”18, aiming to encourage behavioral changes in clinical practice for neurologic physical therapists’ utilization of a novel gait training method for patients with hemiparesis for inpatients in rehabilitation.18 In the mid-year survey before the quality improvement project, Perry et al established that 19% and 33% of the therapists were moderate/very familiar and almost always/often used non-supported gait training (NSGT), as opposed to 78% and 66% at the 6 months point.18 Another study21 used an exploratory design and involved process evaluation to study a leadership intervention for five outpatient stroke rehabilitation centers in Sweden. The objective was supporting managers with the implementation of guidelines in outpatient stroke rehabilitation settings. Tistad et al showed that managers considered the intervention beneficial with all managers developing a leadership plan. However, just two units identified specific implementation goals.21
Several studies involved audit and feedback as well as clinician education QI interventions.19,24 Audit and feedback involves “providing a summary of the healthcare provider’s or the institution’s clinical performance that is reported publicly or confidentially to or about the clinician or institute”.4 Using audit-feedback process and knowledge translation activities, one study24 looked at 16 overarching guideline indicators, with a target for staff adherence to guideline indicators per patient set at a minimum of 75%. Jolliffe et al24 demonstrated a significantly increased adherence to guideline recommendation. The other study by Janzen et al involving clinician education as well as audit-feedback involved a “Knowledge to Action Project” involving the audit-feedback process with both a knowledge creation cycle and an action cycle. Janzen et al demonstrated considerable success in changing clinical practice and developing a culture supporting using evidence-based practices in stroke rehabilitation.19 Vratsistas-Curto et al25 involved clinician education and an audit-feedback intervention. The study involved audit-feedback process, identification of practice determinants, provision of educational materials and education. Audit data explored eleven areas, and the study demonstrated meeting or exceeding the 10% target improvement in 20 out of the 27 areas targeted (74%).
Six studies involved organizational change.4,14–17,20,22,23 Organizational change involves “any intervention that involves changes in the structure or delivery of care designed to improve the efficiency or breadth and depth of clinical care”.4
Two studies utilized shared governance and shared decision-making. One study17 looked at shared governance with a goal to discuss any issues and problems and develop proposed solutions to improve patient-centered care. Torres et al demonstrated improvements in patient outcomes, staff communication, staff satisfaction and problem solving as a result of the QI intervention.17 Another study23 using shared decision-making (SDM) in five stroke units. Voogdt-Pruis et al demonstrated the feasibility of implementation of SDM in integrated stroke care23 and developed an additional eight recommendations for adoption of shared decision-making in stroke care. This included awareness campaigns, organizational ambassadors, essentiality of training, investigating patient personal preferences before treatment as well as involving relatives, implementation through stroke services and embedding shared decision-making in current care chains with clear roles and responsibilities as well as having informative overviews of primary healthcare professionals (HCPs) in the region to support in shared decision-making transfer to primary care.23
Two studies were utilizing randomized controlled trials. One study15 looked at the use of the Critical Path Method (CPM) for containing costs and improving patient outcomes. Falconer et al demonstrated that using the CPM for QI intervention showed no improvement in patient outcomes.15 No statistical significance was evident between groups for length of stay or hospital charges. Another study22 evaluated the effects of the “Stroke 90:10 Quality Improvement Collaborative” (QIC) on the uptake of two evidence-based bundles of care (early hours and rehabilitation). The collaborative aimed to improve compliance and reliability of nine processes across early hours and rehabilitation from 72% to an average of 90%. Power et al demonstrated a modest improvement from baseline in the odds of compliance corresponding to a relative improvement of 10.9% in the Early Hours Bundle and 11.2% in the Rehabilitation Bundle.22
Another study16 evaluated improvements in geriatric rehabilitation service delivery through a national quality improvement program aiming to incite self-organizing capacity to develop integrated care through developing or improving the care pathway for the patient group. Holstege et al used two cohorts of patients, baseline and one-year post-implementation follow-up cohort.16 At 1-year post-implementation, there was similarity in successful rehabilitation between the cohorts for stroke rehabilitation, but with additional independence in activities of daily living in the follow-up cohort. Another study14 looked at improving care planning aiming for the most efficient resource utilization to maximize outcomes for stroke survivors. After implementing the program, Oyeyemi and Sedenu demonstrated a significantly decreased length of stay as well as a consistent improvement in length of stay efficiency.14 Finally, one study20 using a PDSA (plan-do-study-act) intervention for technology adoption investigated the integration of the use of a “Via Therapy” tool predominantly as a mobile app with clinical partners. Hancock et al demonstrated a 22% increase in confidence and use of evidence-based practice from the baseline. The technology was found to be concise, straightforward, accessible, simple and easy to use with changes to intervention delivery reported.20
In addition, twenty-three quality improvement studies in stroke rehabilitation were documented in abstracts only.26–48 The studies demonstrated a mix of QI initiatives including twelve quasi-experimental/before and after studies, two qualitative studies, five plan-do-study-act (PDSA) cyclical studies, one action research study and three lean methodology studies. All studies reported positive outcomes and conclusions. The studies are summarized in Table 2 (Summary of Abstracts on Quality Interventions in Stroke Rehabilitation).
To address the third research question, the researchers subsequently considered the role of different barriers and facilitators to the QI interventions in improving the quality of care for stroke patients in rehabilitation utilizing narrative analysis and summary in Table 3. The Model for Understanding Success in Quality (MUSIQ) was used to ascertain contextual factors that could influence QI success.5 One study did not report improvement, while the rest of the studies reported improvements following the intervention, with many reporting on the impact of contextual factors impacting the intervention results. When assessing contextual factors, several authors agreed on the impacts of external environment,16,22 as well as organizational factors.16,19–21,24 In addition, QI support and capacity,14,23 microsystem21 and the QI team14,17,18,24,25 were seen to also have an impact on QI initiatives in the current research.
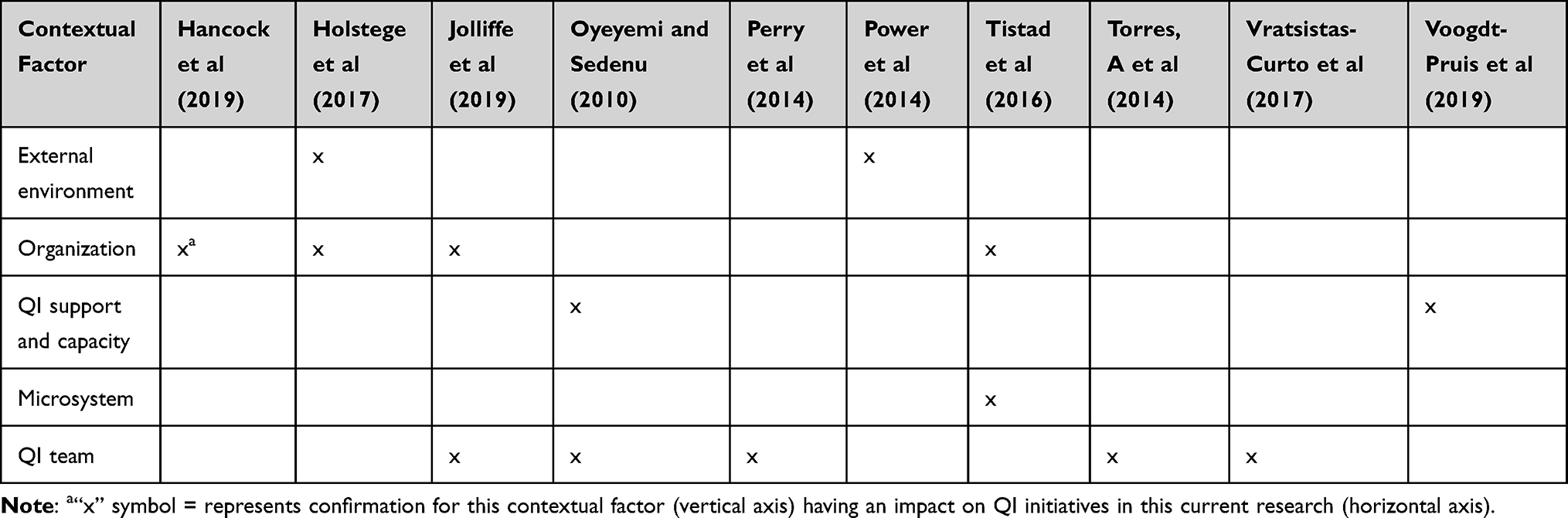 |
Table 3 Contextual Factors in the Research Utilizing MUSIQ |
Several authors in the current review report organizational factors were important facilitators of success including the role of senior leadership and sponsor support in contributing to the success of the intervention. Jolliffe et al concluded that the strong senior management support and organizational support facilitated success.24 Tistad et al suggested that mobilizing knowledge into clinical practice is complex and support from senior management especially for prioritization and discussion was integral for success.21 In addition, several authors concurred with Kaplan et al on the importance of the maturity of QI interventions and sophistication of programs and their contribution to success. Duration of programs was identified as important. Holstege et al recommended longer follow-up periods are sometimes necessary to detect changes in outcomes after quality interventions. They recommended that future studies should look at specific components of the quality interventions that contribute to specific outcome improvements.16 Jolliffe et al also advocated for high incidence of implemented cycles, a long 12-month program duration contributing to higher adherence (>75%) to the program and intervention success.24 In addition, clear prescribed guidelines and ease-of-use are important for success. Janzen et al also concluded that for QI success, clear, comprehensive and prescriptive guidelines are essential.19 Vague recommendations, which are difficult to apply and challenging to measure, contribute to lower success and compliance rates of interventions. Hancock et al concluded that the usability and accessibility of the used intervention contributed to success.20
Holstege et al confirmed that external factors (societal and organizational) could have affected the study outcome.16 Power et al also stated that national and regional attention to stroke at the time of the intervention contributed to improvement.22 They also stated that regulation, clinical leadership, and research implementation contributed to the better care for the stroke patients during the intervention. In addition, they concluded that the effects of interventions could be specific rather than generalizable; thus, certain care processes would have more improvement in collaborative programs such as simple, controllable, geographically bound changes, rather than others that could be less tractable.22
QI support and capacity were noted to be important contextual factors. Oyeyemi and Sedenu, concluded that incentives and fiscal factors could also have contributed to some of the improvements in the intervention.14 In addition, Voogdt-Pruis et al discussed the impact of the availability and ease-of-use of the intervention as well as access and training involved as facilitators for success.23 At the microsystem level, Tistad et al in the current study also concurred with MUSIQ as to the importance of leadership and culture for QI success and suggested that significant improvements could be made through formal training interventions being incorporated into the normal work settings.21 Furthermore, mentoring managers and tailoring interventions within specific contexts could also contribute to success. Identifying specific indicators for change relevant to the context as well as monitoring performances and outcomes were found to have a positive influence on the intervention.21
Finally, MUSIQ discussed extensively the role of QI teams in intervention success,5 which was further confirmed by many authors in the current study. Jolliffe et al mentioned that regular attendance of key staff in the intervention influenced the regularity of feedback during the intervention, however as they were looking at a sustainability in the program, this was an acceptable limitation during implementation.24 They also confirmed the importance of non-aversive clinician-led feedback as well as shared goals to QI success. Vratsistas-Curto et al also discussed team actors that contributed to lack of behavioral changes, which included lack of staff monitoring, staff turnover, smaller interventions, and absence of familiarity or concurrence with the proposed assessments and interventions.25 Oyeyemi and Sedenu concluded that improvements in staff expertise as a contributing factor for success.14 Torres et al also concluded that improved communication impacted intervention success.17 Perry et al discussed team diversity and norms, concluding that an “active” approach demonstrated better adherence that just relying on mailed guidelines, and that practice style traits (seekers, receptive, traditionalists and pragmatists) also influenced intervention success.18 The researchers also stressed the importance of change agents on-site. They concluded that some of the challenges included complexity of patient cases, time availability, the drive for persistence over longer periods of time and change resistance.
Discussion
The purpose of this review was to identify QI interventions used in stroke rehabilitation settings and the impacts and improvements reported in the QI interventions. Our search identified twelve studies with QI interventions in stroke rehabilitation that met review criteria.
In addition, there were twenty-three quality improvement studies in stroke rehabilitation where only conference abstracts were available. The types of intervention in these abstracts were briefly discussed in the results section of this review and are presented in Table 2. This suggests that quality interventions were implemented for stroke rehabilitation and discussed in relevant conferences, however no further endeavours were attempted to develop a full journal paper to further describe and discuss the interventions. This suggests there may be four categories of QI studies, those that are published as full papers in peer review journals, published as conference abstracts, presented at conferences but the abstracts are not published and even perhaps not published or presented, thus suggesting that the QI studies published as full papers are the tip of the iceberg. The studies reported in the identified abstracts were not included in the full review due to the lack of comparable detail on the interventions and study findings.
The review identified heterogeneous interventions with largely positive results. Less than 10% of the studies reported no improvement after a quality intervention. The majority of QI interventions were involving organizational change in the structure or delivery of care,4,14–17,20,22 two clinician education QI interventions18,21 and two audit and feedback as well as clinician education QI interventions.19,24 With the limitations and heterogeneity in intervention types, designs, contextual factors and outcomes in the reviewed primary studies of QI interventions that are typical in QI literature, the researchers encountered challenges in assessing of the evidence across heterogeneous studies with limited ability to quantitatively synthesize results and thus a narrative analysis approach was undertaken. In addition, the researchers summarized evidence, grouping evidence by settings, study design, type, population, methods, intervention results and outcome measures. On the other hand, this very heterogeneity reflects the wide diversity of interventions in practice for stroke rehabilitation QI interventions that are likely to impact improvements in practice and contributing significantly to this gap in literature.
Various contextual factors, barriers and facilitators throughout the studies contributed to the success of the interventions. Contextual factors in the QI interventions in the current review impacted on improvement outcomes following implementation. The characteristics of the setting in the study where no improvement after the quality improvement intervention could have impacted intervention effectiveness.15 This included specialization, professional (turf) issues, external regulations including cost-containing policies and procedures, goal flexibility, poorly defined outcomes, unclear relationship between services and outcomes as well as multiple, non-integrated patient care management may have contributed to limiting the effectiveness of the CPM intervention. The majority of the studies reported quality improvements with contextual factors including external environment, organizational factors, QI support and capacity, microsystem and the QI team impacting intervention success.14,16–25 Thus, researchers and clinicians implementing QI interventions would benefit from taking into consideration reported barriers and facilitators for quality improvement for stroke patients in rehabilitation.
Many limitations were discussed in the current studies, with size, generalizability and data issues emerging as the main themes. The majority of authors discussed size and generalizability as well as absence of cost analysis as limitation of the research. In the study by Hancock et al (2019), authors had only one PDSA cycle throughout the project, thus limitations of a small data set, inability to perform costs analysis as well as the use of one community setting were observed during application.20 Jolliffe et al mentioned that implementation in just one site limits the generalizability and possibility of scaling-up, adoption and delivery across multiple organizations. Finally, using multiple indicators might also limit implementation in multiple sites. They recommended implementing in both public and private hospitals as well as including cost/benefit analysis along with any evaluation of efficacy.24 Oyeyemi and Sedenu also confirmed that small sample size and a one-center study is a limitation in the study.14 Perry et al stated limitations in absence of control groups and non-randomization.18 Vratsistas-Curto et al also mentioned small file numbers as a study limitation.25 Power et al had limitations in not non-generalizability beyond the English context. They suggested further studies investigate causal mechanisms linking improved performance to improved outcomes, as well as more sophisticated evaluation mechanisms for collaboratives.22 Some of the limitations in Voogdt-Pruis et al including non-representation of the study population to the entire population, the possibility of missing certain barriers and facilitators by the late adopters and the absence of patient and patient-representative participation in the study.23 Data issues and missing data were also mentioned as limitations in several studies. Perry et al stated limitations in missing data and unclear documentation in the intervention.18 Vratsistas-Curto et al also recorded inaccuracy of written medical records.25 Power et al had limitations in not capturing additional processes of care, variation in completion rates as well as data collection bias.22
Thus, it could be said that the QI interventions undergone to date for stroke rehabilitation demonstrated improvements through implementation of the different interventions (>90%). However, despite the importance of QI interventions for improving the delivery of health care in stroke rehabilitation, many contextual factors, barriers and limitations in the implementation and evaluation of QI interventions can be seen influencing the effectiveness of the intervention. The current research concurred with MUSIQ on many of the contextual factors underlying success in QI, where more specifically the role of the organization and the QI team have been discussed by the majority of authors in the current study as playing a role in success. Designing and supporting QI interventions taking into consideration the facilitators, limitations, contextual factors and recommendations posed by the researchers in the current study would contribute to better and more generalisable QI interventions in stroke rehabilitation.
Limitations
There were limitations in the current study. Firstly, due to the limited number of studies as well as the quality of some studies that met review criteria, the strength of conclusions is limited. Secondly, there was a wide range of study types, settings and methods, leading to wide heterogeneity in the studies that met inclusion criteria, thus performing a meta-analysis for the results was not possible. Thirdly, our search might not have been exhaustive despite searching multiple databases using comprehensive and validated search strategies. Finally, categorizing articles by type of intervention even with assistance of predefined tools and classification schemes is partly subjective.
Conclusions
There is paucity of research investigating QI intervention for improving the quality of care in stroke rehabilitation. Reviewing 12 studies that included quality improvement interventions in stroke care can offer value to healthcare providers in terms of key success factors associated with improvements in this particular clinical setting of stroke rehabilitation. In more than 90% of cases, improvements were noted through implementation of multicomponent interventions, and the majority of studies raised the impact of contextual factors through intervention implementation.
IS made substantial contributions to the conception and design, acquisition, analysis, and interpretation of data and was involved in drafting the final manuscript. MC made substantial contributions to the conception and interpretation of data and was involved in drafting the final manuscript. JK made substantial contributions to the conception and design, analysis, and interpretation of data and was involved in drafting the final manuscript. All authors read and approved the final manuscript. JK is the overall guarantor.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Kennedy PJ, Leathley CM, Hughes CF. Clinical practice variation. Med J Austral. 2010;193(8):S97. doi:10.5694/j.1326-5377.2010.tb04021.x
2. Ng’ang’a R, Kimani KN, Okutoyi L, Adam MB. Evidence of interventions and strategies to bridge the quality improvement gap led by HCW at the frontline in SSA: a scoping review. IJQHC Commun. 2022;2(2):115.
3. Akmal A, Podgorodnichenko N, Foote J, Greatbanks R, Stokes T, Gauld R. Why is quality improvement so challenging? A viable systems model perspective to understand the frustrations of healthcare quality improvement managers. Health Policy. 2021;125(5):658–664. doi:10.1016/j.healthpol.2021.03.015
4. Bravata DM, Sundaram V, Lewis R, et al. Closing the quality gap: a critical analysis of quality improvement strategies (vol. 5: asthma care). 2010.
5. Kaplan HC, Provost LP, Froehle CM, Margolis PA. The Model for Understanding Success in Quality (MUSIQ): building a theory of context in healthcare quality improvement. BMJ Qual Saf. 2012;21(1):13–20. doi:10.1136/bmjqs-2011-000010
6. Curcin V, Woodcock T, Poots AJ, Majeed A, Bell D. Model-driven approach to data collection and reporting for quality improvement. J Biomed Inform. 2014;52:151–162. doi:10.1016/j.jbi.2014.04.014
7. Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet. 2011;377(9778):1693–1702. doi:10.1016/S0140-6736(11)60325-5
8. Latorre JGS, Flanagan S, Phipps MS, Shenoy AM, Bennett A, Seidenwurm D. Quality improvement in neurology Stroke and Stroke Rehabilitation Quality Measurement Set update. Neurology. 2017;89(15):1619–1626. doi:10.1212/WNL.0000000000004486
9. Dowla N, Chan L. Improving quality in stroke rehabilitation. Top Stroke Rehabil. 2010;17(4):230–238. doi:10.1310/tsr1704-230
10. Grube MM, Dohle C, Djouchadar D, et al. Evidence-based quality indicators for stroke rehabilitation. Stroke. 2012;43(1):142–146. doi:10.1161/STROKEAHA.111.627679
11. Zorowitz R. Stroke rehabilitation quality indicators: raising the bar in the inpatient rehabilitation facility. Top Stroke Rehabil. 2010;17(4):294–304. doi:10.1310/tsr1704-294
12. Nunes JW, Seagull FJ, Rao P, Segal JH, Mani NS, Heung M. Continuous quality improvement in nephrology: a systematic review. BMC Nephrol. 2016;17(1):190. doi:10.1186/s12882-016-0389-1
13. Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health careinterventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10)
14. Oyeyemi A, Sedenu B. Using a classification process to optimize outcome of stroke rehabilitation. Phys Occup Ther Geriatr. 2010;28(4):376–386. doi:10.3109/02703181.2010.533819
15. Falconer JA, Roth EJ, Sutin JA, Strasser DC, Chang RW. The critical path method in stroke rehabilitation: lessons from an experiment in cost containment and outcome improvement. Qual Rev Bull. 1993;19(1):8–16. doi:10.1016/S0097-5990(16)30582-6
16. Holstege MS, Caljouw MA, Zekveld IG, et al. Successful geriatric rehabilitation: effects on patients’ outcome of a national program to improve quality of care, the SINGER study. J Am Med Dir Assoc. 2017;18(5):383–387. doi:10.1016/j.jamda.2016.10.011
17. Torres A, Kunishige N, Morimoto D, et al. Shared governance: a way to improve the care in an inpatient rehabilitation facility. Rehabil Nurs. 2015;40(2):69–73. doi:10.1002/rnj.143
18. Perry SB, Zeleznik H, Breisinger T. Supporting clinical practice behavior change among neurologic physical therapists: a case study in knowledge translation. J Neurol Phys Ther. 2014;38(2):134–143. doi:10.1097/NPT.0000000000000034
19. Janzen S, McIntyre A, Richardson M, Britt E, Teasell R. Building a knowledge to action program in stroke rehabilitation. Can J Neurol Sci. 2016;43(5):619–625. doi:10.1017/cjn.2016.258
20. Hancock NJ, Collins K, Dorer C, Wolf SL, Bayley M, Pomeroy VM. Evidence-based practice ‘on-The-go’: using ViaTherapy as a tool to enhance clinical decision making in upper limb rehabilitation after stroke, a quality improvement initiative. BMJ Open Qual. 2019;8(3):e000592. doi:10.1136/bmjoq-2018-000592
21. Tistad M, Palmcrantz S, Wallin L, et al. Developing leadership in managers to facilitate the implementation of national guideline recommendations: a process evaluation of feasibility and usefulness. Int J Health Policy Manag. 2016;5(8):477–486. doi:10.15171/ijhpm.2016.35
22. Power M, Tyrrell PJ, Rudd AG, et al. Did a quality improvement collaborative make stroke care better? A cluster randomized trial. Implement Sci. 2014;9(1):40. doi:10.1186/1748-5908-9-40
23. Voogdt-Pruis HR, Ras T, van der Dussen L, et al. Improvement of shared decision making in integrated stroke care: a before and after evaluation using a questionnaire survey. BMC Health Serv Res. 2019;19. doi:10.1186/s12913-019-4761-2
24. Jolliffe L, Morarty J, Hoffmann T, et al. Using audit and feedback to increase clinician adherence to clinical practice guidelines in brain injury rehabilitation: a before and after study. PLoS One. 2019;14(3):e0213525. doi:10.1371/journal.pone.0213525
25. Vratsistas-Curto A, McCluskey A, Schurr K. Use of audit, feedback and education increased guideline implementation in a multidisciplinary stroke unit. BMJ Open Qual. 2017;6(2):e000212. doi:10.1136/bmjoq-2017-000212
26. Allen L, Janzen SE, Mehta S, Britt E, Meyer M, Teasell R. The use of an audit-feedback loop to address adherence to stroke best practice recommendations for hypertension management. Stroke. 2013;44(12):e204.
27. Britt EJ, McHale H, Meyer M. A quality improvement initiative to reduce length of stay for an inpatient stroke rehabilitation program utilizing the RPG methodology. Stroke. 2010;41(7):e492.
28. Bassei M, Betita B, Martins A, Reid K, Pettapiece K. Look, touch, feel and learn: peer to peer knowledge translation of the Canadian Diabetes Association Guideline for hypoglycemia in a Rehab/CCC hospital with comprehensive stroke rehabilitation services. Int J Stroke. 2015;10:60–61.
29. Bayley MT, Wood-Dauphinee S, Mokry J, et al. Stroke Canada optimization of rehabilitation by evidence: implementation trial. Stroke. 2011;42(11):e590.
30. Bishev M. An interprofessional team approach to rehab intensity in inpatient stroke rehab at Sunnybrook Health Sciences Centre-St. John’s Rehab. Eur Stroke J. 2018;3(1):198–199.
31. Craven F, Noel S, Doyle R, et al. A quality improvement initiative in the stroke rehabilitation unit. Age Ageing. 2018;47:v13–v60. doi:10.1093/ageing/afy140.39
32. Garratt E, Bolton S. Stroke rehabilitation service quality improvement plan-a tale of 2 towns. Int J Stroke. 2018;13(3):39.
33. Hahn N. Physician-led quality improvement project to enhance delivery of stroke therapy in inpatient rehabilitation. Int J Stroke. 2019;14(3):33.
34. Halabi ML, Roberts J, MacQueen J, Amlani S, Hanna S. A team approach to quality improvement for an urban in-home stroke rehabilitation program. Int J Stroke. 2018;13(2):62.
35. Liang J, Adams E, Sivananthan D, Catapano M, Mayo A, MacNeill H. Streamlining completion of secondary stroke prevention investigation workup in inpatient stroke rehabilitation: a quality improvement project. Int J Stroke. 2019;14(3):36.
36. Lo A, Fancott C. Impact of quality and patient safety rounds in stroke rehabilitation. J Rehabil Med. 2016;48(1):100.
37. Lo A, Fortin J. Improving stroke rehab through interprofessional quality and patient safety rounds. Stroke. 2014;45(12):e289.
38. Lo Chang J, Aikman P. Stroke rehabilitation in BC: using action-research to identify gaps in care and promote improvements. Stroke. 2013;44(12):e218.
39. Morgan P, Cream A, West D. Osborne Park Hospital stroke rehabilitation unit: major changes achieved through teamwork and continuous improvement. Int J Stroke. 2012;7:56.
40. Pollard C, Ceglie D. Advancement of a rehab model of care: the designated stroke POD. Int J Stroke. 2018;13(2):113.
41. Pollard C, Ceglie D. Advancing Our Rehab Model: The Designated Stroke POD-Outcomes After One Year. International Journal of Stroke; 2019.
42. Robinson J, Trow K, McNicoll Whiteman R. Utilizing lean methodology to redesign stroke rehabilitation team rounds to improve efficiencies. Int J Stroke. 2018;13(2):170.
43. Savage J, Yang C, Mantha A, McDonnell L, Powell J. A quality improvement initiative to increase rehabilitation intensity. Int J Stroke. 2019;14(3):30.
44. Sheehan L, Ciavarra A, Hodgson S, et al. Using a LEAN approach to increase Rehabilitation Intensity (R.I.): a Focus on Environment. Int J Stroke. 2017;12(4):67–68.
45. Sureshkumar S. Enhancing teamwork to create a high-performance team in the acute stroke unit at Worcestershire Royal Hospital–quality improvement project. Future Healthc J. 2020;7(Suppl 1):s59–s. doi:10.7861/fhj.7.1.s59
46. Thornton M, MacKay-Lyons M, Dyks T, et al. Use of eLearning methods to evaluate best practice knowledge and self-efficacy of application of guidelines by Canadian physiotherapists: reporting of preliminary findings: RHB. Int J Stroke. 2015;10:194.
47. White J, Stager C. An integrated stroke unit model of care: leveraging the interdisciplinary team to improve acute length of stay, ACL days and referral to in-patient rehabilitation: RHB. Int J Stroke. 2015;10:200.
48. Yong-Jae K, Eun-Jung K. Development of an acute stroke care pathway following the FOCUS-PDCA model. Ann Acad Med Singapore. 2012;41(9):S260.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.