Back to Journals » Patient Preference and Adherence » Volume 20
Qualitative Study of Learned Helplessness in Colorectal Cancer Patients with Colostomy: A Social-Ecological Perspective
Authors Wei X, Wu L, Chen X, Ding J, Hua Q
Received 16 October 2025
Accepted for publication 24 December 2025
Published 7 January 2026 Volume 2026:20 574914
DOI https://doi.org/10.2147/PPA.S574914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Xianqi Wei,1 Lujuan Wu,1 Xuan Chen,1 Jinxia Ding,1,2 Qingling Hua2
1School of Nursing, Anhui Medical University, Hefei, People’s Republic of China; 2Department of Medical Oncology, The First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China
Correspondence: Jinxia Ding, School of Nursing, Anhui Medical University, Hefei, People’s Republic of China, Email [email protected]
Purpose: To explore the experience of learned helplessness among colorectal cancer ostomy patients within the theoretical framework of social ecosystems, and to provide a theoretical basis for developing targeted nursing interventions for this population.
Methods: Employing purposive sampling, semi-structured in-depth interviews were conducted with 16 colorectal cancer patients with ostomies at the First Affiliated Hospital of Anhui Medical University between March and June 2024. Data analysis was performed using Colaizzi’s phenomenological methodology.
Results: A total of three main themes and nine sub-themes were identified, as follows: (1) Micro-level systems: fear and negative cognition, self-care barriers and dependency, and self-regulation fatigue and loss of control; (2) Meso-level systems: heavy economic burden, the importance of family support, and social avoidance and stigma; (3) Macro-level systems: insufficient medical information and services, social cognitive bias, and the importance of social security policies.
Conclusion: Learned helplessness in colorectal-cancer patients is driven by synergistic systemic factors. Healthcare providers should implement multifaceted, individualized interventions that target psychological distress and mitigate helplessness across the entire care trajectory.
Keywords: colorectal cancer, stoma, learned helplessness, social-ecological theory, qualitative research
Introduction
Colorectal cancer (CRC) is one of the most common gastrointestinal malignancies worldwide. Global cancer statistics for 2022 indicate that CRC accounted for roughly 9.6% of all new cancer cases, placing it third in incidence and second in mortality.1 In China alone, approximately 517,000 new cases were recorded in the same year, representing 10.7% of the national cancer incidence and ranking second among newly diagnosed malignancies.2 Surgery remains the curative mainstay, and over one million Chinese patients now live with a colostomy, with an additional 100,000 created annually.3 The operation diverts a segment of colon to an abdominal stoma, replacing the anus as the route of defecation.4 Although the procedure prevents disease progression5 and prolongs survival,6 it inevitably alters body anatomy and function. Patients therefore endure not only post-operative pain but also multifaceted physiological, psychological, social, and spiritual challenges7 that can precipitate learned helplessness.
Learned helplessness is a psychological concept proposed by Martin Seligman in 1975.8 LH refers to the psychological state of powerlessness or self-abandonment experienced by individuals when they perceive a lack of controllable connection between their own behaviors and outcomes, which is manifested as cognitive impairment, reduced motivation, and emotional disturbance.9 Studies have shown that LH is a common psychological phenomenon among most patients with chronic diseases.10–13 When LH levels are high, patients lack confidence in their ability to effectively manage their disease and daily lives, and are more likely to give up efforts or struggle to persist with long-term interventions.14 In addition, as a persistent negative psychological state, LH may induce more severe psychological problems (eg, cognitive bias, distress, anxiety, and depression) and even increase the risk of suicide,15 which has a significant negative impact on patients’ disease recovery and quality of life. Notably, most patients in China participate in peer support groups. When patients witness negative events (eg, family breakdown or the death of fellow patients), they tend to project these negative events onto themselves out of empathy, leading to increased learned helplessness. The Healthy China Action (2019–2030) also emphasizes the importance of cancer prevention and control, as well as promoting the mental health of cancer patients.16 Therefore, timely identification and intervention of LH to prevent or delay adverse outcomes are of great clinical and social significance. However, current interventions for learned helplessness mainly focus on patients with rheumatoid arthritis, systemic lupus erythematosus, and other chronic diseases, which lack pertinence. There is an urgent need to develop tailored intervention programs for colorectal cancer patients with colostomies, tailored to their disease-specific characteristics. Thus, it is particularly important to deeply explore the internal experiences of learned helplessness among colorectal cancer patients with colostomies during disease treatment. By exploring these internal experiences and underlying influencing factors, we can provide more targeted psychological support for patients, help them cope with the disease more effectively, and improve their treatment compliance and quality of life.
Social-ecosystems theory provides a holistic, systems-level lens for examining interactions between individuals and society, highlighting the dynamic reciprocity among personal attributes, immediate settings, and larger social structures. It distinguishes three nested tiers: (1) the microsystem—the person’s unique biological and psychological characteristics; (2) the mesosystem—face-to-face contexts such as family, work, and peer networks that directly shape experience; and (3) the macrosystem—overarching cultural beliefs, community norms, institutions, and policy environments.17 Today, this framework has been widely applied in fields such as chronic disease management18 and health promotion.19 Research suggests that learned helplessness (LH) is not a direct result of traumatic events but rather emerges through interactive learning shaped by multiple factors encountered during an individual’s coping process.20 Therefore, a systematic socio-ecological examination of how patient-level and contextual factors shape learned helplessness is both warranted and timely.
To date, learned helplessness in colorectal-cancer ostomy patients has received little empirical attention, and qualitative inquiries embedded in socio-ecological theory are virtually absent. To address this gap, we conducted a qualitative study that blends phenomenological methods with a socio-ecological lens to illuminate patients’ lived experience of helplessness. By expanding the depth and breadth of current knowledge, our findings offer an evidence-based reference for developing tailored interventions for this underserved population.
Methods
Study Design
This descriptive phenomenological study collected data through semi-structured interviews and analysed them using Colaizzi’s method, while adhering to the Consolidated Criteria for Reporting Qualitative Research (COREQ).21
Participants
We used purposive sampling to recruit colorectal cancer patients with ostomies who attended the Department of Oncology or the Wound and Ostomy Care Clinic of the First Affiliated Hospital of Anhui Medical University between March and June 2024. To maximize sample diversity, participants with varying ages, educational levels, stoma types, and complications were included. Inclusion criteria: (1) Patients meeting the diagnostic criteria of the Chinese Diagnosis and Treatment Standards for Colorectal Cancer (2023 Edition);22 (2) Age ≥ 18 years; (3) History of intestinal ostomy surgery ≥ 1 month; (4) Demonstrates a high level of learned helplessness (assessed using the Learned Helplessness Scale (LHS),23 which has high reliability and validity and is one of the most commonly used psychological assessment tools for learned helplessness in China, with a Cronbach’s α coefficient of 0.930; a total score ≥ 62 indicates a high level); (5) Possession of normal communication abilities; (6) Signed informed consent. Exclusion Criteria: (1) Patients with other severe illnesses or comorbid psychological/psychiatric disorders; (2) Tumor recurrence, metastasis, or presence of other malignancies. Recruitment continued until data saturation was reached (ie, no new themes emerged during analysis).
Data Collection
Semi-structured face-to-face interviews were conducted by researchers trained in qualitative research methods and possessing interview experience. Interviews took place in quiet, comfortable private hospital rooms or offices. Before commencing, researchers introduced themselves, explained the purpose and significance of the interview, clarified that recordings were solely for nursing research and would not disclose any private information, and guided participants to sign a paper informed consent form after obtaining consent. Throughout the interview, the researcher maintained focused listening, flexibly adjusting techniques based on the situation, while observing and documenting the participant’s facial expressions, body language, and changes in tone of voice. Each interview lasts approximately 30 to 40 minutes. If no new information emerges during the interview, it will be concluded.
Grounded in social-ecological theory, we drafted an initial interview guide from the literature, clinical experience, and consultations with gastrointestinal surgeons and ostomy-care nurses. After pilot interviews with two colorectal-cancer ostomy patients, we refined the guide to match participants’ comprehension, producing the final version (Figure 1).
 |
Figure 1 Final version of the interview guide. |
Data Analysis
All recordings were transcribed within 24 h of each interview, and each transcript was checked and assigned an anonymous ID. The texts were imported into NVivo 12.0 for management and analysed according to Colaizzi’s seven-step phenomenological approach.24
- Familiarization: Carefully reread interview content multiple times to ensure thorough understanding of the material;
- Identify significant statements: Extract sentences that directly address the research questions;
- Formulate meanings: Translate each excerpt into concise codes that capture its essence;
- Cluster themes: Group related codes to create an initial thematic framework;
- Develop Detailed Descriptions: Provide comprehensive descriptions for each theme generated in step (4), incorporating representative participant statements as supporting evidence;
- Synthesize the framework: Iteratively compare and merge similar themes to produce a coherent structure;
- Validate findings: Return the final framework to participants for confirmation of accuracy and resonance.
Quality Control
Audio recordings were transcribed within 24 h by two master’s-prepared nursing students who cross-checked each transcript. The full research team subsequently discussed the data to reach consensus, and each participant was asked to confirm that the transcript accurately reflected his or her intended meaning.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Anhui Medical University (Approval Number: PJ 2024-10-58). Participants were informed that their involvement was voluntary and that they could decline or withdraw at any time without consequences. All data were collected anonymously, privacy was strictly protected, and written informed consent was obtained from all participants, which included permission for the publication of anonymized responses and direct quotes.
Results
Participant Characteristics
Based on the principle of data saturation, this study ultimately included 16 colorectal cancer ostomy patients, comprising 9 males and 7 females aged between 35 and 79 years. Detailed demographic information is presented in Table 1. To protect subject privacy, participants were identified using coded designations P1 through P16.
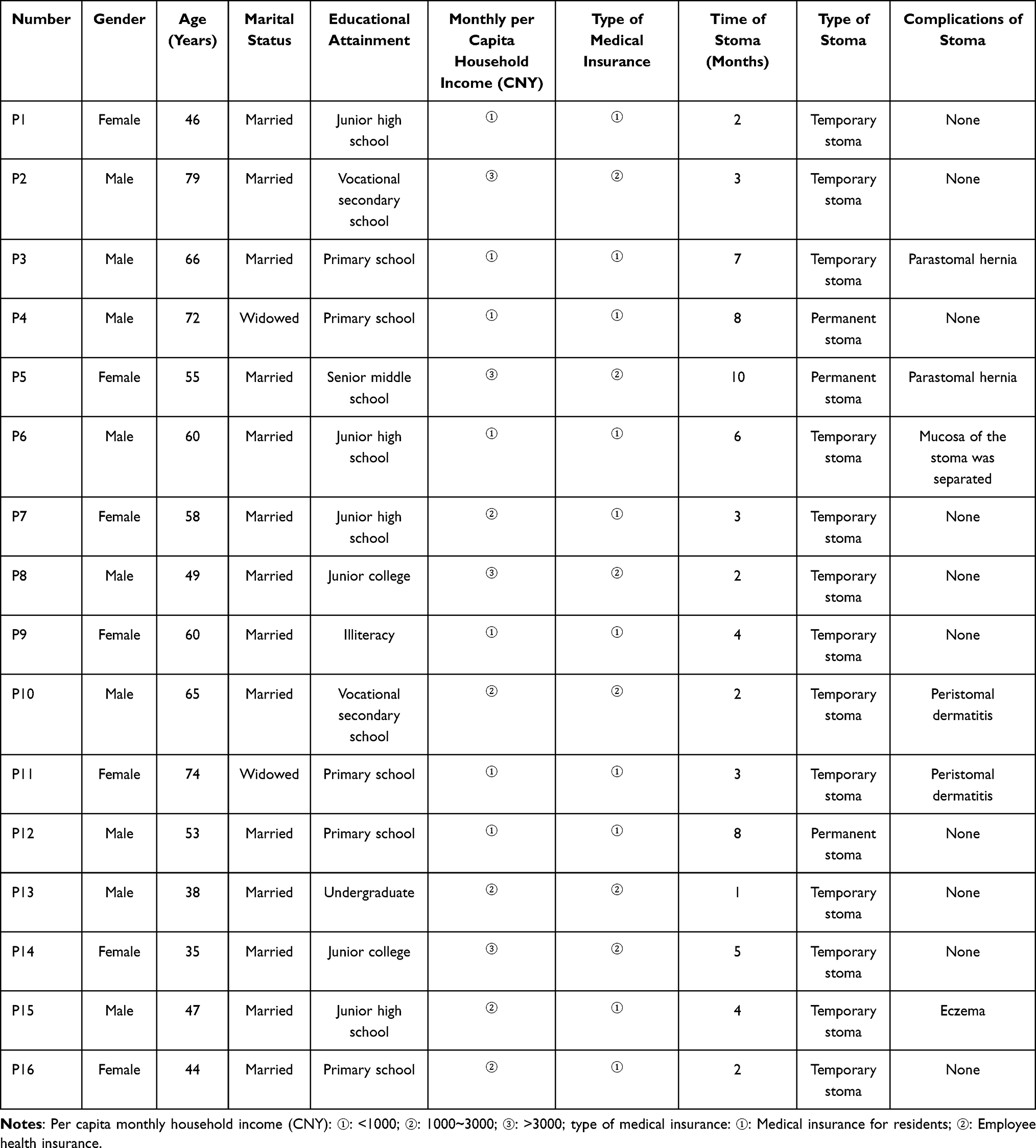 |
Table 1 Characteristics of Participants (N =16) |
Phenomenological Findings
Three themes and nine subthemes emerged from the interviews (Table 2): (1) Micro-system: Physiological and psychological adaptation dilemmas (fear and negative cognition, inadequate self-care and dependency, self-regulation fatigue and sense of loss of control); (2) Meso-system: Support and challenges within family and social networks (heavy economic burden, importance of family support, social avoidance and stigma associated with illness); (3) Macro System: The Interplay of Social Policies and Cultural Environment (Insufficient Medical Information and Services, Social Cognitive Biases, Importance of Social Security Policies).
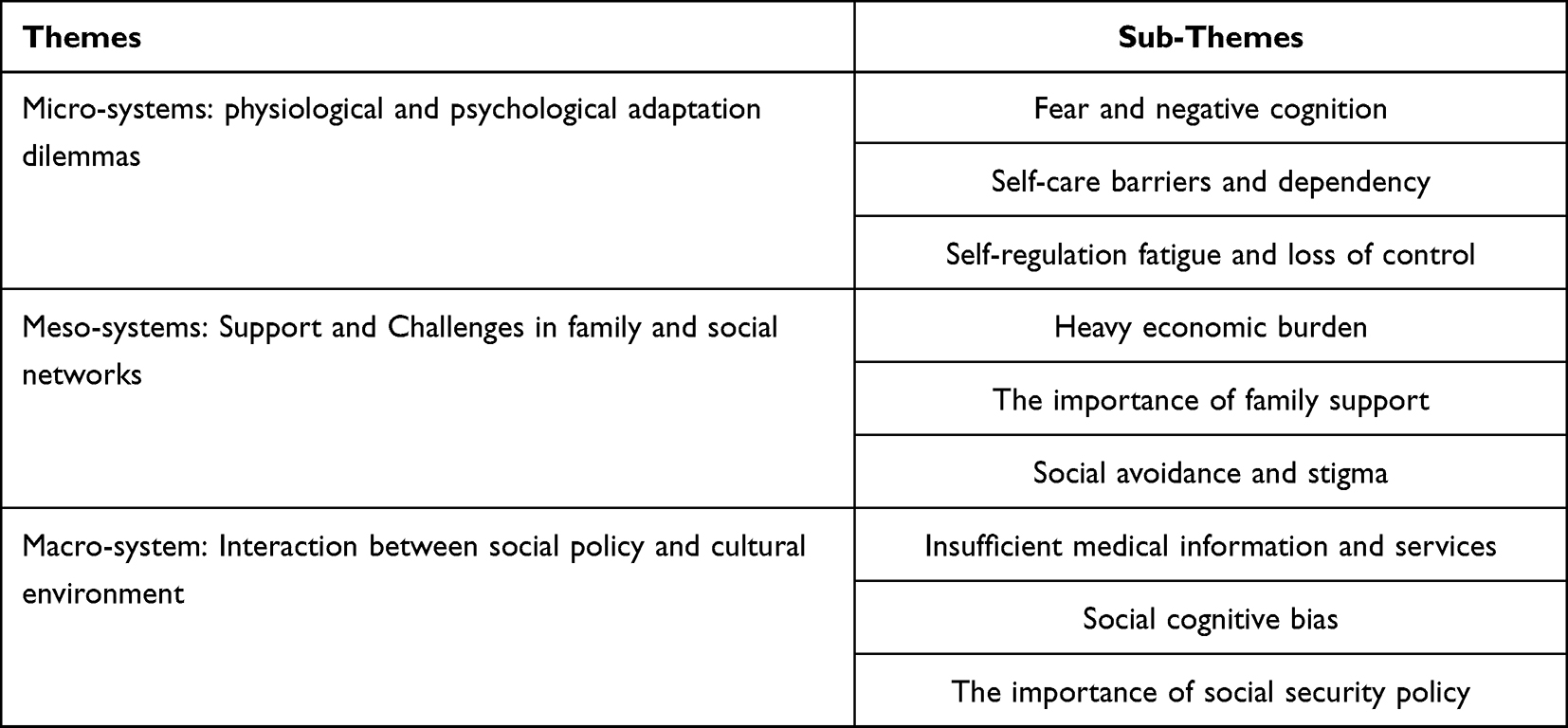 |
Table 2 Themes and Sub-Themes of Learned Helplessness Experience in Colorectal Cancer Patients with Colostomy |
Microsystem: Physiological and Psychological Adaptation Dilemmas
Fear of Disease Progression and Negative Cognition
Most participants reported pronounced fear and anxiety about recurrence or metastasis; their worries centred on disease progression, treatment failure, and poor survival prognosis. Because colorectal cancer is associated with high rates of recurrence, metastasis, and mortality, stoma patients carry an additional psychological burden that is fuelled by post-operative alterations in body image.
P8: Sometimes when I feel unwell, I get really worried, afraid it might be a recurrence.
P7: Ever since this surgery, I can’t sleep a wink every night. I’m such a scaredy-cat—why did this disease have to happen to me?
P14: I’m still young. What if it comes back? Just thinking about it keeps me up at night (sighs). I still want to go back to work.
P6: I don’t know if this stoma can be reversed. The intestine and skin are separated. The doctor said to let the wound heal first. Last time I came, the wound was almost healed, but after this round of chemo, it’s not healing again. It’s so torturous.
P5: After getting this disease, I don’t know how much longer I have. Online sources say it’s incurable.
P12: Someone in my village had this disease before too. They passed away within a few years.
P2: At my age, I’m just grateful for each day I get to live.
P16: I didn’t do chemotherapy after surgery, but I felt uneasy. So I sought out traditional Chinese medicine. I’ve been taking herbal medicine for a while now.
Self-Care Impairment and Dependency
Limited knowledge and hands-on skills leave many patients ill-equipped to manage their stomas, predisposing them to incorrect technique and subsequent complications. Advanced age, declining memory, and diminished adaptive capacity further hinder older adults from acquiring the necessary information, compounding the risk of stoma-related problems.
P13: I tried learning to change it myself, but I just can’t get the hang of it. Sometimes I’m in the middle of changing it and stool leaks out—it’s so frustrating.
P1: Applying this ostomy pouch is such a hassle, and I can never get it to stick properly. It leaks all the time.
P14: I can’t bring myself to look at that area. My spouse changes my pouch every day. I really wish I could get the reversal surgery done sooner.
P15: I rarely take baths. What if the water soaks into the stoma and causes an infection? Then I’d suffer again. I can only wipe it with a towel before bed.
P4: I’m too scared to change it myself. I’m getting older and don’t know how to handle it.
P10: I don’t change the bag as often at home. My skin got inflamed, so now I have to come here every week for the nurses to treat it.
P6: I have to come here twice a week. The intestine and skin haven’t healed properly yet, so I don’t dare change it myself.
Self-Regulation of Fatigue and Sense of Loss of Control
Patients with lower educational attainment are less likely to seek out disease-related information, understand medical instructions, or apply stress-management techniques, leaving them ill-prepared to cope with unexpected events and precipitating self-regulatory fatigue and imbalance. Compounding these difficulties, stoma care itself poses a major challenge: recurrent leakage can embarrass patients, restrict social contact, disrupt adherence to recommended diet and activity regimens, and ultimately erode overall quality of life.
P10: When I got discharged and went home, all sorts of problems popped up. The bag leaked and wasn’t secure. My skin itched, but I dared not scratch it. It was so frustrating. Sigh.
P13: After the surgery, my stamina clearly isn’t what it used to be. I get tired so easily now.
P14: Once I woke up in the middle of the night to find stool leaking all over the bed. Ugh, it was unbearable. I could only lie flat and dared not turn over, just stayed in bed until dawn.
P1: I never sleep well—waking up multiple times each night, worried it might suddenly leak.
P9: Every time I see the bag getting full, I feel anxious.
P15: My wife usually changes the bag very diligently, but I don’t know why she suddenly developed eczema.
P2: What bothers me most is the itching at night. It itches all night, and I can’t sleep well.
P8: We’ve gone through a lot of detours.
P5: Before, when my stomach was cramping, I handled it myself. I bought an electric moxibustion device online to dispel the cold.
Mesosystem: Support and Challenges in Family and Social Networks
Heavy Economic Burden
Colorectal-cancer stoma patients shoulder a dual financial load: high upfront oncology costs plus lifelong expenditure on appliances and post-operative care. Co-morbidities such as hypertension or diabetes add further chronic medication expenses, while tumour- or treatment-related work incapacity reduces household income, compounding the economic strain.
P9: After a lifetime of farming, I have no retirement pension. I rely entirely on my children, and since they have to care for me, my spouse can’t work either.
P4: I need chemotherapy at the hospital once a month. Between meals, transportation, and lodging, it costs thousands. I also have hypertension and require medication.
P6: I come to the hospital weekly to change this stoma. They also placed an IV port in my chest that needs regular dressing changes,
P7: I can’t earn money now, and my son already has heavy burdens—like his mortgage payments,
P12: There are so many expenses. We borrowed money from relatives for previous surgeries, and I don’t know when we’ll ever pay it back,
P16: “A base plate costs tens of yuan, and the ostomy base and pouch together cost tens of yuan per day”.
The Importance of Family Support
Many patients remain dependent on family care after discharge, making the home environment pivotal to recovery. Strong family support provides emotional reassurance and practical assistance, fosters adaptive emotional expression, reduces psychological burden, and prevents the accumulation of distress.
P9: I often snap at my husband. He bustles about taking care of me every day, never complaining or showing any sign of resentment.
P5: My husband is very meticulous. I never have to worry about anything—he even changes my bag for me. I’ve never had to do it myself. He supports me both physically and emotionally, always encouraging me: ‘It’s okay, take it slow. You’ll get better.
P10: My children are very busy with work and don’t have time to care for me. Usually, it’s all up to my spouse. She has sacrificed so much for this family. Every time I need a follow-up checkup, my son has to drive me to the hospital.
P2: Staying home all day gets boring after a while, and I can’t do much work. My spouse keeps me company and chats with me daily to lift my spirits. My daughter also calls often, telling me not to overthink things.
P11: My son and daughter handle all the hospital expenses—I don’t have to worry about it.
Social Avoidance and Stigma
After ostomy surgery, alterations in body image can trigger feelings of inferiority, perceived discrimination, and social exclusion, accentuating a sense of deviance from the norm. The accompanying loss of bowel control further erodes self-esteem, leading some patients to withdraw from social contact as a self-protective measure against anticipated external harm.
P7: I used to be very conscious about my appearance and had a great figure I’d go downstairs every night to dance in the square. Now that I’ve gained weight and my body has changed, I don’t feel like dressing up anymore. Plus, carrying this ostomy bag is so inconvenient.
P13: I’ve given up many hobbies. I used to often meet friends for hiking or running. I don’t want them to know I have a stoma, afraid they’ll ask about my condition.
P14: I always feel like I smell, even after washing thoroughly. I spray on a lot of perfume beforehand, afraid others will notice the odor. So I rarely go out with people, have few friends, and don’t want to bother anyone.
P5: Wearing this bag makes dressing and showering inconvenient.
P10: Going out requires preparing so many things beforehand—it’s too much trouble.
P8: I just can’t accept it mentally.
Macro System: The Interplay Between Social Policy and Cultural Environment
Insufficient Medical Information and Services
Although Enhanced Recovery After Surgery (ERAS) protocols have shortened hospital stays, most patients are discharged with unmet needs across multiple domains. The limited time in hospital restricts education for both patients and their families, resulting in inadequate knowledge of stoma care that can negatively affect recovery and long-term quality of life.
P3: After being discharged and returning home, I wasn’t sure if I could move around. I was anxious to get back to work, which led to a hernia. At first, I didn’t even realize it was a hernia. Look at this big bulge—I didn’t understand it, and no one explained it to me. That’s why it’s crucial to clearly explain all precautions to patients after stoma creation.
P4: There were so many things I didn’t understand. I couldn’t eat freely, afraid that eating the wrong foods would make me uncomfortable When I felt unwell, I didn’t know if it was normal.
P13: My wife changes my ostomy pouch. She can’t get the baseplate size right—she doesn’t know how big to cut it.
P10: Once when changing it, the skin around the stoma was red and a bit sore. I didn’t know if that was normal.
P11: Sometimes the pouch fills up really fast. I don’t know why there’s so much gas inside. It worries me.
P13: My wife changes my ostomy pouch. She can’t get the baseplate cut to the right size—I don’t know how big it should be.
Social Cognitive Bias
The stoma’s visible location, altered appearance, and involuntary function collide with societal bodily ideals and entrenched norms of excretory privacy, marking patients as deviant. In traditional Chinese culture, where cancer is often equated with misfortune, this stigma amplifies psychological distress and fosters learned helplessness.
P6: My relatives and friends know I’m sick and have to go to the hospital often. I haven’t told them what I have, afraid they’ll look at me differently.
P16: I’ve been lying at home for over half a year now. Having cancer isn’t exactly good news—it makes people gossip. Word spreads quickly in the village, and soon everyone knew.
P14: When I occasionally run into neighbors in the elevator now, we just exchange greetings before going our separate ways. It’s not as warm as it used to be.
P3: People know I have cancer, and they’re afraid I might infect them.
P12: Because of this illness, the construction site boss doesn’t dare let me work anymore.
The Importance of Social Security Policies
Interviewees reported that current social-support mechanisms—medical-insurance provisions and the distribution of public facilities—are inadequate for their treatment and long-term rehabilitation needs. Reimbursement rates differ by region, so rural patients and those treated outside their home districts shoulder a disproportionate share of expenses, creating considerable financial strain.
P8: Whenever I go out, I am afraid the bag will suddenly leak on the street—there’s nowhere to change it and public toilets are hard to find.
P2: I live far from this hospital. The nurses at local facilities are not as skilled, so I do not feel confident going there.
P7: The nurses added me to a WeChat support group where patients share experiences and encourage one another.
P16: Each time I visit the hospital’s ostomy clinic I talk at length with the nurses; their guidance has been invaluable.
P1: I am from a rural area. I hope more employment opportunities can be created for people like us.
P12: The medical-insurance reimbursement rate is low; every chemotherapy cycle still costs several thousand yuan. It would help if a larger share were covered.
Discussion
Based on the social-ecological systems theory, this study adopted the descriptive phenomenological research method to deeply explore the real experiences of learned helplessness of colorectal cancer patients with colostomies in the context of Chinese culture. The results show that the learned helplessness of patients is affected by the micro, meso, and macro levels factors, and these systems interact with one another, thus affecting the physical and mental health of patients. This phenomenon needs to be paid attention to by medical staff and family members, who should identify the learned helplessness of patients in time, and provide targeted support and intervention based on the characteristics of each system, so as to reduce the adverse consequences and maintain the stability of their social-ecological system.
At the micro-system level, the study first established that the physiological and psychological distress experienced by colorectal-cancer ostomy patients is closely linked to learned helplessness (LH). Participants reported persistent psychological burdens, foremost among them fear of cancer progression, anxiety, and depression. A recent systematic review identified fear of recurrence or progression as the most prevalent unmet need among cancer survivors;25 without timely intervention, this fear often remains high and chronic.26 Sarkar et al27 further argue that excessive fear and stress can erode treatment adherence, impair social functioning, and drive up medical costs, ultimately precipitating a cascade of adverse outcomes. In addition, limited knowledge and hands-on skills related to stoma care among both patients and their families frequently result in improper management and severe daily challenges—findings that align with those of Alwi et al.28 As one participant succinctly described, “Nothing went wrong in the hospital, but once I got home everything started—bag leaks and itchy skin”. Despite multiple preventive efforts, such incidents could not be entirely avoided. The resulting sense of powerlessness in the face of adversity is a key trigger for LH.29 Our findings also reveal that LH in this population is associated with a sustained burden of coping, manifested as chronic fatigue and emotional exhaustion that intensify patients’ feelings of losing control. Similar observations have been reported by Xie et al30 in maintenance hemodialysis patients, who likewise demonstrated a strong link between LH and perceived lack of control. Multiple stoma-related complications and low self-care competence further erode patients’ sense of mastery. Prolonged exposure to these stressors leaves individuals feeling unable to influence their own physical and emotional states, thereby exacerbating LH.31 A qualitative study of older adults with temporary stomas found that limited self-care capacity at home markedly increased their dependence on healthcare professionals.32 Therefore, clinicians should deliver targeted education and continuous support to ensure patients and caregivers master essential stoma-care skills, promote independent self-management, and enhance perceived control. Concurrently, nurses must monitor patients’ emotional responses, promptly identify emerging distress and unmet needs, and tailor interventions to reduce the psychological burden imposed by learned helplessness.
At the meso-system level, the study identified three interlocking forces—heavy economic burden, the pivotal role of family support, and social avoidance coupled with stigma—that jointly shape the lived environment of colorectal-cancer ostomy patients. Many participants described receiving robust assistance from immediate family—most notably spouses and children—and credited this backing with strengthening their resolve to continue treatment. Family is a complex, heterogeneous system whose functioning is influenced by the wider social environment, critical life events, and prevailing community norms.33 Previous research confirms that ostomy patients have an especially urgent need for family support,34 and, within Chinese culture, individuals are more inclined to seek emotional sustenance from relatives than from non-kin networks.35 Greater perceived family support is consistently associated with better physical and psychological well-being and with more active, constructive illness-coping behaviors.36 Yet, most respondents came from rural areas and reported formidable treatment-related expenses, corroborating earlier findings that financial strain and family support are two of the strongest predictors of learned helplessness in this population.37,38 Compounding these pressures, post-operative symptoms such as high-output stoma, pain, and fatigue markedly reduced patients’energy and mobility, severely restricting travel and social participation and leading to progressive social withdrawal.39 Participant P7 summarized the shift: “I used to go square-dancing with my neighbors every evening; now I hardly leave the house”. Such isolation intensifies feelings of helplessness. Family-function theory posits that the extent to which individuals feel understood and supported during recovery provides the scaffolding for broader social engagement.40 Accordingly, family members should accompany patients to community events, patient-group lectures, and peer-support activities. These joint ventures both expand patients’ access to information and encourage them to articulate their emotions and perspectives, thereby replenishing and enhancing their psychological resources.41
At the macro-system level, the broader social climate and national health policy form the decisive context for patients’learned helplessness (LH). Previous studies consistently identify social support as a key external resource for cancer patients and a significant negative predictor of LH.14 Huang et al likewise showed that higher social support attenuates helplessness in lung-cancer patients.15 In the present study, however, most respondents reported low social support coupled with heavy societal pressure. Limited public knowledge about ostomies, compounded by the cultural reticence prevalent in Chinese society, renders cancer a “taboo” topic and discourages open discussion among patients and potential supporters.42 This silence reduces social contact, reinforces isolation, and amplifies helplessness. Conversely, successful societal reintegration can restore productivity, ease the financial burden of cancer, improve physical health, and foster positive affect, thereby enhancing quality of life.43 Yet China’s current policy environment provides insufficient coverage and quality of medical insurance, social services, and rehabilitation resources for colorectal-cancer ostomy patients. Limited access to specialized care and information erodes patients’sense of control and intensifies LH. As a developing country with a vast population, China faces chronically strained medical resources.44 Clinicians cannot offer lengthy, individualized health guidance to every patient, leaving an urgent unmet need for professional information and education. Therefore, in the future, knowledge about colorectal cancer stomas can be disseminated through education, training, and mass media to correct public misconceptions about this disease and foster an inclusive and supportive social environment. Simultaneously, basic public services in urban areas should be continuously improved. Relevant departments may consider providing convenient services for ostomates, such as installing dedicated restrooms, to alleviate concerns about going out and encourage them to step out of their homes with confidence. Furthermore, relevant authorities must optimize healthcare policies to expand stoma care coverage and reduce out-of-pocket expenses, thereby alleviating patients’ financial burdens. Concurrently, increased resource allocation and specialized training for primary healthcare facilities will address resource shortages, providing policy-level support to empower patients and ease their burdens.
Strengths and Limitations
To the best of our knowledge, this is the first qualitative study to explore the experience of learned helplessness among colorectal cancer patients with colostomies, using the social-ecological systems theory as a theoretical framework—which lays a solid foundation for subsequent research. Additionally, the study demonstrated methodological rigor by achieving data saturation and adhering to the COREQ reporting guidelines—all of which have enhanced the credibility of the findings. However, this study has some limitations. Firstly, the sample size of this study is relatively small, limited to a group of patients with colostomy cancer in a tertiary hospital in a provincial capital city of eastern China. This restricts the general applicability of the research results, as the sample fails to cover differences in medical levels or between urban and rural areas. Future research should expand the sample size and recruit participants from different regions and hospitals to enhance the representativeness of the sample and the general applicability of the results. Secondly, the interviews were conducted in Chinese and then translated into English, which may introduce language bias or loss of nuances. Thirdly, individual differences among interviewers may lead to potential interviewer bias. Fourthly, the learned helplessness scale used in this study is a general tool and may lack specificity for effectively identifying or accurately assessing learned helplessness in this specific population. Therefore, future research should develop and validate assessment tools specifically tailored to the unique characteristics of this population. Additionally, future studies should adopt longitudinal, multi-informant designs (including both patients and their family members) to generate richer, more nuanced insights.
Conclusions
Based on the theory of social ecological system, this study explored the real psychological experience of learned helplessness of 16 colorectal cancer patients with colostomy through qualitative interviews. Three core themes were extracted: physiological and psychological adaptation difficulties; Support and challenges in family and social networks; Interaction between social policy and cultural environment. The study found that patients’ learned helplessness is influenced by multiple factors—an insight that filled the gap in existing research in this field to a certain extent and provided a clear theoretical basis and practical direction for clinical healthcare professionals to implement targeted interventions. In the future, it is necessary to rely on the multi-level framework of social-ecological systems to construct a comprehensive, stable, and coordinated social support and intervention system. Specifically, efforts should focus on optimizing micro-system support strategies to enhance patients’ psychological empowerment; strengthening meso-system collaboration to promote patients’ social reintegration; and advancing the improvement of macro-system policies to alleviate patients’ psychological distress from multiple dimensions. These measures aim to mitigate the experience of learned helplessness in colorectal cancer patients with colostomies.
Abbreviations
COREQ, Consolidated Criteria for Reporting Qualitative Research; LHS, Learned Helplessness Scale.
Data Sharing Statement
The datasets analyzed herein are not publicly available for ethical and privacy reasons.
Ethics Statement and Consent to Participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Anhui Medical University (Approval Number: PJ 2024-10-58). All participants signed written informed consent after being fully informed of the study’s purpose and procedures prior to the interview.
Acknowledgments
The authors express their gratitude to all contributors for their diligent work on this study and to all participants who voluntarily took part in the research.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, data acquisition, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval to the version to be published; have reached a consensus on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by the Youth Program of Natural Science Foundation of Anhui Province (Project number: 2408085QH234) and the Graduate Seedling Cultivation Program of School of Nursing, Anhui Medical University (Project number: Hlqm12025078).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Lin L, Zheng J, Lin Z, Xiao H. Understanding the challenges of readiness for hospital discharge in stoma patients: a mixed-methods study. J Clin Nurs. 2025;34(5):1704–1712. doi:10.1111/jocn.17654
4. Krouse RS, Grant M, McCorkle R, et al. A chronic care ostomy self-management program for cancer survivors. Psychooncology. 2016;25(5):574–581. doi:10.1002/pon.4078
5. Alenezi A, Livesay K, McGrath I, Kimpton A. Ostomy-related problems and their impact on quality of life of Saudi ostomate patients: a mixed-methods study. J Clin Nurs. 2023;32(13–14):3707–3719. doi:10.1111/jocn.16466
6. Baykara ZG, Eyikara E, Hin AÖ, Acarlar H, Leventoğlu S. Changes in the lives of individuals with a stoma and their spouses: a qualitative study. Adv Skin Wound Care. 2022;35(5):281–288. doi:10.1097/01.ASW.0000823992.61032.ee
7. Alenezi A, McGrath I, Kimpton A, Livesay K. Quality of life among ostomy patients: a narrative literature review. J Clin Nurs. 2021;30(21–22):3111–3123. doi:10.1111/jocn.15840
8. Seligman ME. Learned helplessness as a model of depression. Comment and integration. J Abnorm Psychol. 1978;87(1):165–179. doi:10.1037/0021-843X.87.1.165
9. Camacho EM, Verstappen SM, Chipping J, Symmons DP. Learned helplessness predicts functional disability, pain and fatigue in patients with recent-onset inflammatory polyarthritis. Rheumatology. 2013;52(7):1233–1238. doi:10.1093/rheumatology/kes434
10. Mills SD, Azizoddin D, Gholizadeh S, Racaza GZ, Nicassio PM. The mediational role of helplessness in psychological outcomes in systemic lupus erythematosus. Lupus. 2018;27(7):1185–1189. doi:10.1177/0961203317751046
11. van der Werf SP, Evers A, Jongen PJ, Bleijenberg G. The role of helplessness as mediator between neurological disability, emotional instability, experienced fatigue and depression in patients with multiple sclerosis. Mult Scler. 2003;9(1):89–94. doi:10.1191/1352458503ms854oa
12. Smallheer BA, Vollman M, Dietrich MS. Learned helplessness and depressive symptoms following myocardial infarction. Clin Nurs Res. 2018;27(5):597–616. doi:10.1177/1054773816689752
13. Kuttner MJ, Delamater AM, Santiago JV. Learned helplessness in diabetic youths. J Pediatr Psychol. 1990;15(5):581–594. doi:10.1093/jpepsy/15.5.581
14. Xie C, Li L, Zhou L, Sun C, Zhang Y, Li Y. Mediating role of learned helplessness’ components in the association between health literacy/social support and self-management among maintenance haemodialysis patients in Changsha, China: a cross-sectional study. BMJ Open. 2023;13(8):e068601. doi:10.1136/bmjopen-2022-068601
15. Huang J, Shi Y, Chen Y, Tang L, Zhang Z. How social support influences learned helplessness in lung cancer patients: the chain mediation role of individual resilience and self-efficacy. Front Psychol. 2024;15:1436495. doi:10.3389/fpsyg.2024.1436495
16. Chen HY, Liao XY, Liu CM, et al. Key insights and implications from the major initiatives of the healthy China action (2019-2030): a general practitioner’s perspective. Chin Health Service Manag. 2020;37(12):958–960.
17. Han Y, Xing F, Huang J, Wang M. Associated factors of health-promoting lifestyle of the elderly based on the theory of social ecosystem. Aten Primaria. 2023;55(9):102679. doi:10.1016/j.aprim.2023.102679
18. Han MH, Zhao Q, Luo MY, et al. A qualitative study on the experiences of social isolation among patients with chronic obstructive pulmonary disease. Chin J Nurs. 2025;60(5):532–539.
19. Mei L, Chen S, Hu Y, Weng D, Zhou J. Caring experience of caregivers of children with short bowel syndrome based on the social ecological theory: a qualitative study. Chin J Nurs. 2022;57:718–723.
20. Seligman S. Dynamic systems theories as a metaframework for psychoanalysis. Psychoanal Dialogues. 2005;15(2):285–319. doi:10.1080/10481881509348832
21. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
22. Chinese Society of Medical Oncology; National Health Council of China; Department of Medical Affairs. Chinese colorectal cancer diagnosis and treatment standard (2023 edition). Med J Peking Union Med Coll Hosp. 2023;14:706–733.
23. Wu XY, Zeng H, Ma SB, et al. Development of the learned helplessness scale and its correlation with personality traits. J Sun Yat-sen Univers. 2009;30(3):357–360,361.
24. Liu M. The application of Colaizzi’s seven-step method in phenomenological research data analysis. J Nurs Sci. 2019;34(11):90–92.
25. Lisy K, Langdon L, Piper A, Jefford M. Identifying the most prevalent unmet needs of cancer survivors in Australia: a systematic review. Asia Pac J Clin Oncol. 2019;15(5):e68–e78. doi:10.1111/ajco.13176
26. Crist JV, Grunfeld EA. Factors reported to influence fear of recurrence in cancer patients: a systematic review. Psychooncology. 2013;22(5):978–986. doi:10.1002/pon.3114
27. Sarkar S, Sautier L, Schilling G, Bokemeyer C, Koch U, Mehnert A. Anxiety and fear of cancer recurrence and its association with supportive care needs and health-care service utilization in cancer patients. J Cancer Surviv. 2015;9(4):567–575. doi:10.1007/s11764-015-0434-2
28. Alwi F, Chiu YC, Ginting S. Self-care experiences of patients who have recently undergone colostomy: a qualitative study. Nurs Open. 2025;12(5):e70193. doi:10.1002/nop2.70193
29. Seligman ME. Helplessness: On Depression, Development, and Health. WH Freeman; 1975.
30. Xie C, Li L, Li Y. “Alive day is the day”: a qualitative study of experiences of learned helplessness in maintenance haemodialysis patients. Risk Manag Healthc Policy. 2023;16:231–245. doi:10.2147/RMHP.S401205
31. Yessick LR, Salomons TV. The chronic disease helplessness survey: developing and validating a better measure of helplessness for chronic conditions. Pain Rep. 2022;7(2):e991. doi:10.1097/PR9.0000000000000991
32. Wang SM, Jiang JL, Li R, et al. Qualitative exploration of home life experiences and care needs among elderly patients with temporary intestinal stomas. World J Gastroenterol. 2024;30(22):2893–2901. doi:10.3748/wjg.v30.i22.2893
33. Chen WJ, Shi YY, Dai SM, et al. The impact of bidirectional social support and family care on the overall well-being of community-dwelling older adults. Military Nurs. 2024;41(2):56–59.
34. Kafi L, Abu-Odah H, Xu Q. Experiences and needs of colorectal cancer survivors in resource-limited countries: a qualitative descriptive study in Syria. Eur J Oncol Nurs. 2024;73:102715. doi:10.1016/j.ejon.2024.102715
35. Tao H, Songwathana P, Isaramalai SA, Wang Q. Supportive communication to facilitate chinese patients’ adaptation to a permanent colostomy: a qualitative case study approach. Gastroenterol Nurs. 2016;39(5):366–375. doi:10.1097/SGA.0000000000000179
36. Kroenke CH, Michael YL, Shu XO, et al. Post-diagnosis social networks, and lifestyle and treatment factors in the after breast cancer pooling project. Psychooncology. 2017;26(4):544–552. doi:10.1002/pon.4059
37. Zeng JL, Dai Y, Lin CR, et al. The current status of learned helplessness among oral cancer patients after surgery and its influencing factors. Nurs Pract Res. 2024;21(8):1193–1198.
38. Liu Y, Li WD, Pei Q, et al. Analysis of learned helplessness in oral cancer patients after surgery and its influencing factors. J Nurs Sci. 2025;40(5):16–19.
39. Xu YC, Wang YJ, Wang GY, et al. A qualitative study on the causes of social isolation among patients with colorectal cancer stomas. J Nurs Sci. 2024;39(12):86–89.
40. Olson DH. Circumplex Model VII: validation studies and FACES III. Fam Process. 1986;25(3):337–351. doi:10.1111/j.1545-5300.1986.00337.x
41. Pickett SA, Diehl SM, Steigman PJ, et al. Consumer empowerment and self-advocacy outcomes in a randomized study of peer-led education. Community Ment Health J. 2012;48(4):420–430. doi:10.1007/s10597-012-9507-0
42. Liao Y, Liu X, Wu X, Li C, Li Y. Social isolation profiles and conditional process analysis among postoperative enterostomy patients with colorectal cancer. BMC Psychol. 2024;12(1):782. doi:10.1186/s40359-024-02304-5
43. Yuan WX, Kuang Y, Ruan JY, et al. A study on the mediating effects of cancer-related economic toxicity in social reintegration and quality of life. J Nurs Training. 2024;39(23):2472–2477.
44. Tang XY, Luo YL, Yang GQ, et al. Multi-indicator spatio-temporal joint evaluation of healthcare resources: an empirical analysis based on provincial panel data in China from 2009 to 2022. Health Economics Res. 2025;42(08):12–16+23.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
A Qualitative Study of the Experience of Multidisciplinary Teamwork in Chronic Critical Illness Patients
Xu X, Jing M, Zhu Y, Jin H, Li L
Journal of Multidisciplinary Healthcare 2025, 18:827-836
Published Date: 13 February 2025
Critical Care Nurses’ Experiences with Endotracheal Suctioning in Critically Ill Older Adults Patients: A Phenomenological Study
Tang J, Lyv J, Wu NH, Chen X, Bai JJ
Journal of Multidisciplinary Healthcare 2026, 19:586847
Published Date: 7 March 2026
Experiences Related to Learned Helplessness and Support Needs Among Patients with Recurrent Implantation Failure Undergoing in vitro Fertilization and Embryo Transfer: A Qualitative Study
Guo S, Peng X, Xie C, Leng W, Zhou L, Zhang M, Cai S
Psychology Research and Behavior Management 2026, 19:620415
Published Date: 16 June 2026