Back to Journals » Psychology Research and Behavior Management » Volume 19
Experiences Related to Learned Helplessness and Support Needs Among Patients with Recurrent Implantation Failure Undergoing in vitro Fertilization and Embryo Transfer: A Qualitative Study
Authors Guo S ![]() , Peng X
, Peng X ![]() , Xie C, Leng W, Zhou L, Zhang M, Cai S
, Xie C, Leng W, Zhou L, Zhang M, Cai S
Received 27 April 2026
Accepted for publication 2 June 2026
Published 16 June 2026 Volume 2026:19 620415
DOI https://doi.org/10.2147/PRBM.S620415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Einar Thorsteinsson
Shimin Guo,1 Xiaocui Peng,1 Chunying Xie,1 Weiwei Leng,1 Liping Zhou,2 Maoling Zhang,2 Shu Cai1
1School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Nursing, Guangdong Women and Children Hospital, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Shu Cai, School of Nursing, Guangdong Pharmaceutical University, 283 Jianghai Avenue, Haizhu District, Guangzhou, Guangdong, 510310, People’s Republic of China, Email [email protected]
Purpose: This qualitative study aimed to explore experiences related to learned helplessness and support needs among patients with recurrent implantation failure undergoing in vitro fertilization and embryo transfer, and to provide evidence for targeted psychological support and nursing interventions in clinical practice.
Patients and Methods: A descriptive phenomenological study was conducted. Using purposive sampling, 17 patients with recurrent implantation failure undergoing in vitro fertilization and embryo transfer were recruited from the Reproductive Medicine Center of a tertiary Grade A hospital in Guangzhou between December 2025 and March 2026. Data were collected through semi-structured interviews and analyzed using Colaizzi’s seven-step phenomenological method, supported by NVivo 15.0 software.
Results: The analysis identified four themes and 13 subthemes, covering perceived sources of learned helplessness, manifestations in daily life and psychological well-being, participants’ coping responses, and external support needs. These themes reflected how repeated treatment failure, invasive procedures, uncertainty about pregnancy outcomes, and medical and family-related pressures shaped participants’ helplessness experiences, influenced daily life and psychological well-being, and generated needs for information, emotional support, continuity of care, and supportive family and peer communication.
Conclusion: Patients with recurrent implantation failure undergoing in vitro fertilization and embryo transfer described learned helplessness as a multifaceted experience related to repeated treatment failure, invasive procedures, uncertainty about pregnancy outcomes, and medical and family-related pressures. This experience was closely associated with disruptions in daily life, persistent psychological distress, differentiated coping patterns, and multidimensional support needs. Healthcare professionals are encouraged to identify feelings of helplessness early and provide continuous, individualized nursing support based on patients’ coping patterns and support needs.
Keywords: recurrent implantation failure, learned helplessness, nursing, qualitative research
Introduction
Infertility is an important condition affecting the reproductive health of people of childbearing age and is increasingly recognized as a threat to human health.1 In vitro fertilization and embryo transfer (IVF-ET) is an important treatment for infertility and one of the core technologies in assisted reproduction.2 However, despite the increasing maturity of assisted reproductive technologies, some patients undergoing in vitro fertilization and embryo transfer still fail to achieve a clinical pregnancy after multiple embryo transfers, a condition referred to as recurrent implantation failure (RIF), which affects approximately 10% of IVF-ET treatment outcomes worldwide.3 During treatment, patients with RIF are required to undergo repeated invasive procedures, while continually facing the psychological distress caused by repeated implantation failure and bearing substantial medical and family-related burdens.4,5 As a result, they are particularly vulnerable to feelings of helplessness.
Learned helplessness is one of the important indicators reflecting an individual’s psychological state. It refers to a cumulative psychological state and behavioral tendency characterized by powerlessness or self-abandonment that gradually develops after prolonged exposure to negative events that are unpredictable or uncontrollable.6 Unlike broader psychological distress, which includes general emotional responses such as anxiety, sadness, fear, and treatment-related fatigue, learned helplessness specifically emphasizes the belief that one’s actions or repeated efforts may not influence outcomes after exposure to uncontrollable or repeatedly unsuccessful events.7 The attributional reformulation of learned helplessness further suggests that, after uncontrollable negative events, individuals’ explanations for failure may influence whether helplessness becomes persistent or extends beyond the original event. This is especially relevant when repeated failure is perceived as personal, stable, or broadly difficult to change.8 In patients with RIF, repeated treatment failure despite sustained physical, emotional, and financial investment may gradually weaken confidence in future treatment outcomes and increase vulnerability to feelings of helplessness. This process may be understood as a gradual weakening of the perceived link between effort and outcome, in which repeated unsuccessful treatment attempts make patients feel that further effort may not necessarily change the result. Learned helplessness may affect patients’ self-management and is also closely related to psychological suffering, highlighting the need to understand this experience in clinical care.9,10 In reproductive health research, existing studies have mainly focused on psychological distress, anxiety, depression, or fertility-related quality of life.11 However, limited qualitative attention has been paid to learned helplessness among patients with RIF, including how they experience repeated treatment failure, how helplessness affects their daily life and coping, and what support needs they express during this process. Therefore, this study adopted a descriptive phenomenological design to explore experiences related to learned helplessness and support needs among patients with RIF, with the aim of providing evidence for targeted health education and psychological support.
Materials and Methods
Participants
Purposive sampling was used to recruit patients with recurrent implantation failure undergoing in vitro fertilization and embryo transfer from the Reproductive Medicine Center of a tertiary Grade A hospital in Guangzhou between December 2025 and March 2026. To ensure sample diversity and richness of the data, participants were selected according to the principle of maximum variation, with consideration given to age, educational level, duration of infertility, and number of failed embryo transfers. The sample size was determined with reference to the recommendations for qualitative research proposed by Hennink et al,12 and the principle of data saturation was followed. Data saturation was discussed within the research team during the process of data collection and preliminary analysis. Recruitment was stopped when no new themes or substantially new information emerged from the interviews.
The inclusion criteria were as follows: (1) meeting the definition of recurrent implantation failure according to the 2023 Chinese Expert Consensus on the Clinical Diagnosis and Management of Recurrent Implantation Failure;13 and (2) ability to communicate normally and willingness to participate in the study.
The exclusion criteria were as follows: (1) severe dysfunction of major organs, such as the heart, liver, or kidneys, or other serious physical illnesses; (2) mental disorders, cognitive impairment, or disturbance of consciousness; and (3) self-reported experience of other major stressful life events within the past year apart from recurrent implantation failure and its related treatment experiences.
Study Design and Data Collection
This descriptive phenomenological study used semi-structured interviews for data collection. Before the interviews, the researchers obtained support from the reproductive medicine center and consulted the clinical staff to understand the participants’ treatment status and establish initial trust. Eligible participants were fully informed of the study purpose, interview procedures, audio-recording arrangements, and confidentiality principles, and written informed consent was obtained prior to the interviews. One-on-one in-depth interviews were conducted in a quiet and private setting, such as a consultation room or meeting room, and each interview lasted approximately 20–40 minutes. With participants’ permission, the interviews were audio-recorded. During the interviews, the researchers maintained a neutral and non-judgmental attitude, avoided evaluative responses, and paid close attention to non-verbal cues such as facial expressions, tone of voice, pauses, and emotional changes. Follow-up questions were asked when appropriate to encourage participants to describe their experiences in greater depth. Given that patients with recurrent implantation failure may be emotionally sensitive when discussing repeated treatment failure, uncertainty about pregnancy outcomes, or family-related pressure, the researchers paid particular attention to emotional reactions during the interviews. If participants showed obvious distress, such as crying, prolonged silence, or emotional agitation, the interview was paused or slowed down according to their wishes. Emotional reassurance was provided when necessary to ensure their comfort and safety throughout the interview process. The interview guide was initially developed based on a literature review and group discussions within the research team. To ensure the scientific rigor and sensitivity of the interview questions, the guide was reviewed by two experts in qualitative research methodology and one clinical expert. Before the formal interviews, the interviewers received standardized training and established rapport with the participants. Subsequently, three eligible patients were selected for pilot interviews. Based on the pilot interview results, the guide was further revised and refined, and the final interview guide was then established. The key questions included: (1) What was your most immediate feeling after experiencing recurrent implantation failure? (2) During this process, did you ever experience feelings of helplessness or a gradual loss of confidence after repeated efforts? Please describe your experiences in detail. (3) How have these experiences and feelings affected your daily life, family, and treatment process? (4) When you feel helpless or emotionally distressed, what strategies do you usually use to cope? (5) During this process, who or what has provided you with support? (6) What changes would you like healthcare professionals to make in terms of communication, emotional support, or treatment-related care to help you better cope with the helplessness associated with recurrent implantation failure? In addition, is there anything else about recurrent implantation failure and the feelings it has brought you that we have not mentioned but that you consider important?
Data Analysis
Within 24 hours of each interview, audio recordings were transcribed verbatim into text. Data were managed and analyzed using Colaizzi’s seven-step phenomenological approach,14 supported by NVivo 15.0 software. This study strictly adhered to the ethical principles of confidentiality and non-maleficence. We followed the Consolidated Criteria for Reporting Qualitative Research (COREQ).15
Research Team and Reflexivity
To enhance the rigor, trustworthiness, and reflexivity of the study, the following measures were implemented. All researchers completed systematic training in qualitative research methods, covering fundamental theories, interview techniques, data coding, and analytical procedures. This training helped improve the researchers’ interview skills and familiarity with qualitative research procedures. The research team consisted of two master’s students in nursing, two full-time senior nurses, one associate professor, and one professor. Prior to data collection, the two nursing master’s students communicated with the head nurses to understand the general condition of potential participants, facilitate recruitment, and ensure smooth coordination throughout the study period. Each interview was conducted by the two nursing master’s students, with one responsible for leading the interview and the other providing on-site assistance. To reduce the influence of personal bias, the research team engaged in reflexive analysis during data collection and analysis. Before data collection, the interviewers discussed their prior understanding of recurrent implantation failure, infertility treatment, and learned helplessness within the research team. The research team recognized several potential preconceptions before and during analysis. For example, because some team members had nursing and reproductive health-related backgrounds, they might have expected patients with RIF to mainly describe distress, helplessness, and needs for psychological support. The team also recognized the possibility of interpreting general infertility-related distress or treatment fatigue too readily as learned helplessness. To manage these preconceptions, the researchers repeatedly returned to the original transcripts and participant quotations during coding and theme development, and paid particular attention to whether participants’ narratives reflected perceived uncontrollability, self-blame, weakened effort–outcome beliefs, and reduced confidence after repeated failure. Reflective notes and team discussion records were used to document emerging assumptions, researchers’ reflections, and key analytic decisions during coding and theme development. Differences in interpretation were discussed within the team until the themes were grounded in participants’ accounts rather than in researchers’ prior assumptions. The interviewers had no treatment, supervisory, or decision-making relationship with the participants, which helped reduce the potential influence of power imbalance or role conflict. In addition, the interviewers used open-ended questions, avoided evaluative responses, and encouraged participants to describe their experiences in their own words.
The two full-time senior nurses were responsible for checking the transcripts and assisting with preliminary organization of the textual data based on the audio recordings and verbatim transcripts. The data were independently coded and analyzed with the support of NVivo 15.0 software to enhance analytic rigor. When differences arose in coding or interpretation, the research team engaged in further discussion until consensus was reached. During these discussions, the team also examined potential assumptions and differences in interpretation to reduce the influence of individual preconceptions on theme development. The associate professor and professor reviewed and validated the themes to strengthen the credibility of the findings. The professor, as the principal investigator, oversaw the entire research process. All members of the research team were familiar with one another and maintained regular communication and timely feedback through telephone calls and face-to-face meetings to ensure consistency in data collection, analysis, and interpretation.
Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. This study was approved by the hospital ethics committee (Approval No. 20250101). Written informed consent was obtained from all participants, including consent for the publication of anonymized responses and direct quotations.
Results
No participants withdrew from this study. Guided by the principle of data saturation, a total of 17 participants were ultimately included. The demographic characteristics of the participants are presented in Table 1. Overall, the participants ranged in age from 24 to 39 years. They varied in place of residence, educational level, household monthly income per capita, duration of marriage, duration of infertility, type of infertility, childbirth history, and number of failed embryo transfers, thus ensuring diversity in both demographic and treatment-related characteristics.
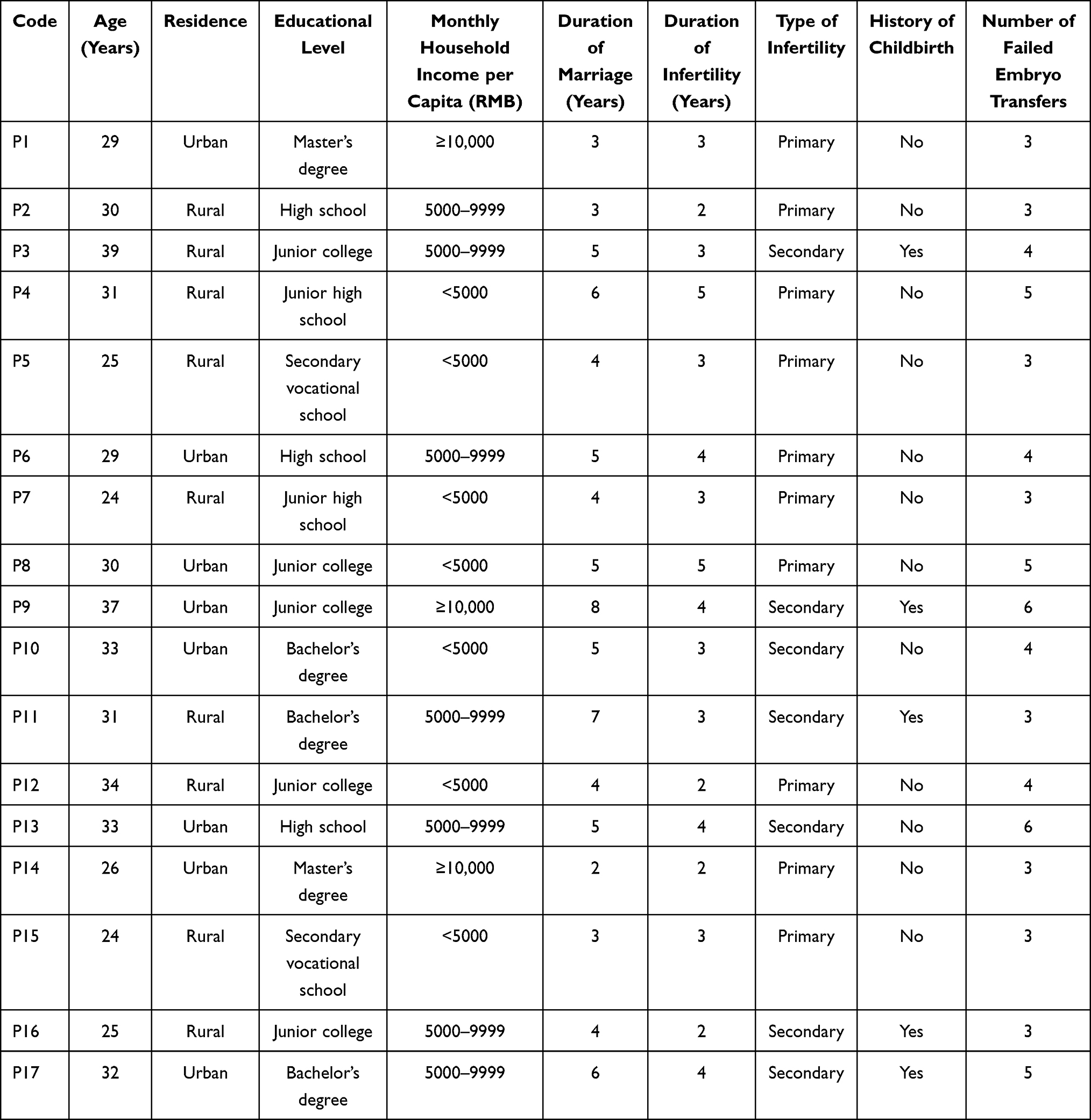 |
Table 1 General Characteristics of Participants (n = 17) |
Four core themes and thirteen subthemes were identified from participants’ accounts of experiences related to learned helplessness and support needs. The themes and subthemes are shown in Table 2.
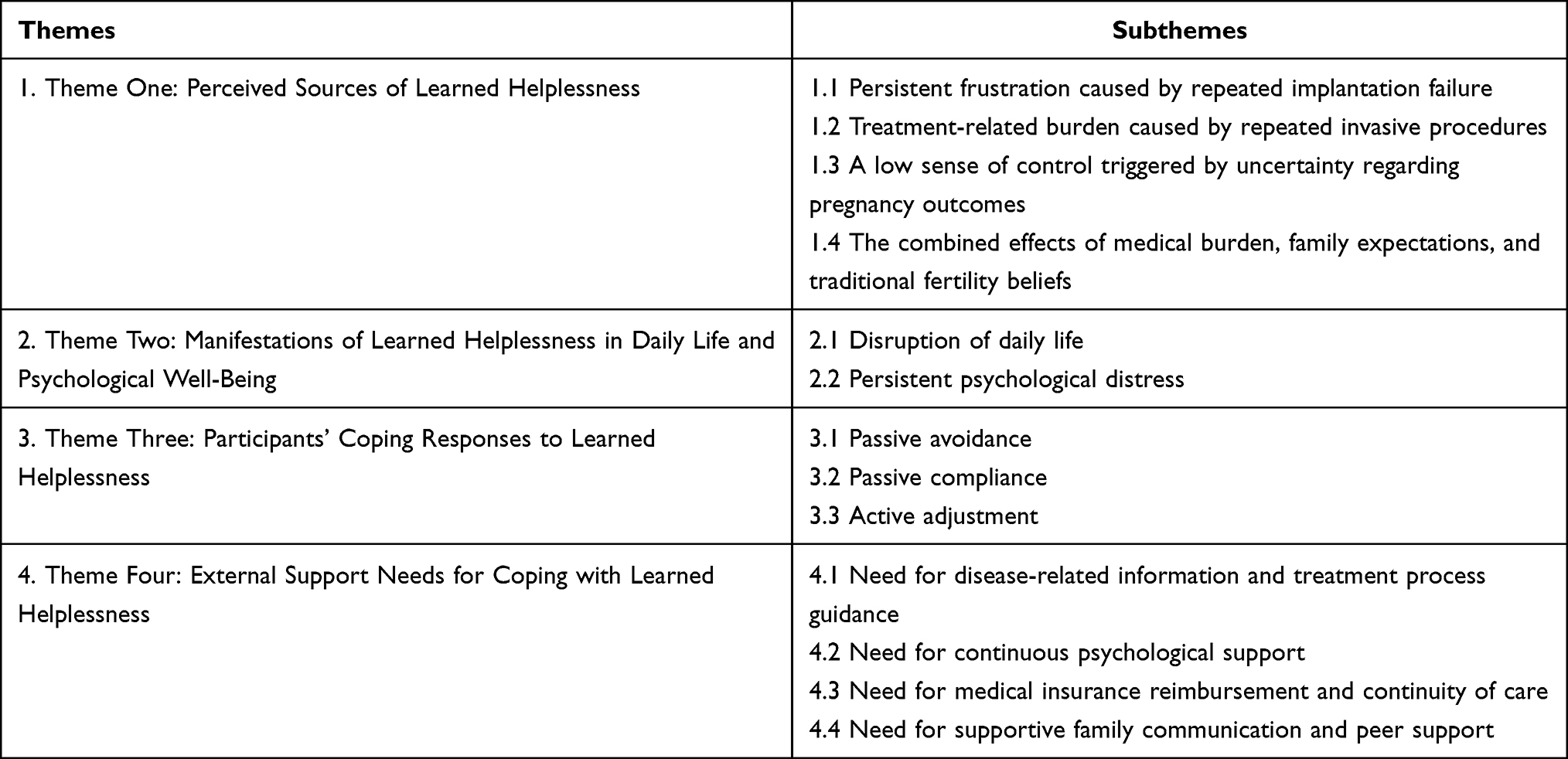 |
Table 2 Themes and Subthemes |
Theme One: Perceived Sources of Learned Helplessness
Subtheme 1: Persistent Frustration Caused by Repeated Implantation Failure
Most participants reported that, after repeatedly entering treatment cycles and experiencing repeated failure, the cumulative sense of frustration gradually led them to believe that continued effort might still not result in the desired outcome.
P2:The previous attempts all failed, so I just kept feeling uncertain and quite anxious.
P3:I have gone through so many cycles, done all the tests, taken all the medications, and spent so much money, but still there has been no real good result.
Subtheme 2: Treatment-Related Burden Caused by Repeated Invasive Procedures
Some participants described having to undergo repeated invasive procedures, such as oocyte retrieval, embryo transfer, and related examinations, during the course of treatment. The accumulation of physical pain and fear of repeated procedures not only intensified the suffering associated with treatment, but also increased their overall physical and emotional burden.
P6:Every time I think about having to go through those examinations and procedures again, I immediately feel tense. It’s not only fear of a bad result, but also fear of the process itself. Physically, it is really uncomfortable.
P8:After treatment, my menstrual pain became so severe that it even made me think about giving up, because I really did not want to keep going through this kind of pain again and again. It was just too painful.
Subtheme 3: A Low Sense of Control Triggered by Uncertainty Regarding Pregnancy Outcomes
For most participants, helplessness was described as being related not only to implantation failure itself, but also to the prolonged uncertainty surrounding treatment outcomes. Even when they tried their best to cooperate with treatment, they still found it difficult to gain any sense of control over whether pregnancy would ultimately be achieved.
P1:This is not something I can control myself. If it were like an exam, at least you could improve through effort, but with this, I just do not know what to do. I still feel very helpless.
P2:This is something you simply cannot control. If that’s the case, then there is nothing you can do except accept it and let things take their course.
P4:In the end, I can only listen to the doctors. I do not really understand it myself, so it just feels completely beyond my control.
Subtheme 4: The Combined Effects of Medical Burden, Family Expectations, and Traditional Fertility Beliefs
Most participants reported that, during repeated treatment, they had to bear multiple pressures at the same time, including financial burden, time costs, and family expectations. Some were also influenced by traditional beliefs such as “women should have children soon after marriage” and “childbearing is a family responsibility,” which placed them under long-term pressure related to family roles and reproductive expectations, making them more likely to experience self-blame, guilt, and low mood.
P1:Especially in this society, I personally like children very much. If I really could not have a child in the future, I think it would be very hard for me to accept.
P5:My husband has never said it directly, but I know he definitely wants a child too.
P7:The financial pressure is quite heavy, because with this treatment, you really do not know how much money you will have to spend before getting a result.
P14:The older people in the family always think that once you get married, you should have a child as soon as possible. After trying for so long without success, I worry that they may think there is something wrong with me.
Theme Two: Manifestations of Learned Helplessness in Daily Life and Psychological Well-Being
Subtheme 1: Disruption of Daily Life
Most participants reported that, during repeated treatment, they often had to take repeated leave from work and adjust their work arrangements because of oocyte retrieval, embryo transfer, and related examinations. Their daily lives also had to be organized around treatment. Meanwhile, the pain and physical discomfort caused by repeated invasive procedures further affected their daily activities and overall living state. In addition, concern about another failed attempt made some participants more cautious about exercise, diet, and everyday behaviors, thereby disrupting their previous life routines.
P3:Sometimes, just to keep up with treatment, I have to take leave again and again, and my work arrangements get completely disrupted.
P8:I used to go out to exercise and meet friends, but now I have stopped doing many of those things. It feels as if my whole life revolves around treatment.
P4:I used to drink things like milk tea, but now I do not dare anymore. I have become very cautious about what I eat.
Subtheme 2: Persistent Psychological Distress
After repeated treatment failure, learned helplessness was often manifested as persistent low mood, emotional suppression, and self-denial. Some participants gradually began to attribute failure to themselves and also experienced sleep disturbance and difficulty regulating their emotions.
P1:Every time I think back on it, I feel both helpless and deeply frustrated.
P3:At night, I keep thinking about it and cannot fall asleep. During that period after failure, I was only sleeping three or four hours a night.
P6:On the surface, I may look fine, but actually I keep it all inside. Especially when I am alone and quiet, I keep replaying all those previous failures in my mind, and after thinking too much, I start to wonder whether the problem is really with me.
Theme Three: Participants’ Coping Responses to Learned Helplessness
Subtheme 1: Passive Avoidance
Under the influence of learned helplessness, some participants tended to withdraw during the treatment process and adopted avoidant coping in response to others’ concern and to topics related to fertility and childbearing.
P10:My friends and I try not to bring up this topic.
P11:Sometimes, the more my family tries to comfort me, the worse I feel. I just want to avoid it, and I do not want to listen or explain anymore.
P15:After going through all of this, I have even become somewhat resistant to going to the hospital.
Subtheme 2: Passive Compliance
Influenced by learned helplessness, some participants showed passive compliance with subsequent treatment. Although they continued to undergo examinations and treatment, their initiative was clearly reduced. They were more likely to follow the existing arrangements and adopt a more resigned attitude toward the outcome.
P4:In the end, I can only follow what the doctors say, because I do not really understand it myself.
P9:Usually, I just see the doctor and do whatever the doctor tells me to do.
P16:To put it simply, I am just going along with it. I do not dare think too much about whether it will work or not.
Subtheme 3: Active Adjustment
Some participants attempted to cope in a relatively positive way after repeated treatment failure. They tried to relieve learned helplessness by actively seeking disease- and treatment-related information, using other activities to distract themselves, and obtaining emotional support from family members or peers with similar experiences.
P2:When I try to get through these feelings, I exercise, listen to audiobooks, read, or listen to music. That’s how I distract myself.
P5:I would search online to find out why implantation failed and what could be done to avoid failure next time.
P9:There was another woman next to me who was also receiving treatment here. After talking with her, I would feel a bit better.
Theme Four: External Support Needs for Coping with Learned Helplessness
Subtheme 1: Need for Disease-Related Information and Treatment Process Guidance
After repeated treatment failure, some participants reported feeling confused and helpless because they lacked a clear understanding of the reasons for failure, did not fully understand the meaning of examination results, and were uncertain about how subsequent treatment would be arranged. They hoped not only to receive accurate and clear professional information, but also to obtain more specific explanations from healthcare professionals regarding precautions during treatment and the next steps in the treatment plan, so as to reduce uncertainty and strengthen their confidence in continuing treatment.
P1:I hope the hospital can give more special attention to my situation and really tell me what I should do.
P2:If someone could explain more to me before the results came out, I probably would not feel so panicked.
P17:Every time I finish an examination, I really want to know what the result means and what the next step will be. If no one explains it clearly, I just keep worrying.
Subtheme 2: Need for Continuous Psychological Support
Participants’ need for psychological support was not limited to brief comfort immediately after a failed treatment result. Rather, they hoped to receive ongoing attention and support throughout the entire treatment process. Because learned helplessness often extended into treatment intervals and daily life, participants reported a clear need for emotional support while waiting for examination results, before entering the next treatment cycle, and during periods of emotional fluctuation.
P6:It’s not enough just to comfort me once after the result comes out. I hope there can be more attention and support throughout the whole treatment process.
P11:Sometimes the hardest part is not the moment of failure itself, but what comes afterward, when I have to process it all by myself.
P13:I think this kind of psychological support should be ongoing. It should not be limited to just a few comforting words at the moment things go wrong.
Subtheme 3: Need for Medical Insurance Reimbursement and Continuity of Care
Participants described that unclear reimbursement policies and insufficient support after leaving the hospital could intensify their feelings of helplessness and uncertainty. Some assisted reproductive procedures had not yet been incorporated into medical insurance coverage, and the required reimbursement materials, procedures, and eligibility conditions were not sufficiently clear. As a result, participants experienced considerable financial pressure during long-term treatment and felt anxious about reimbursement issues. In addition, after returning home and during treatment intervals, guidance regarding follow-up examinations, medication use, and lifestyle management was difficult to sustain, leaving participants uncertain about the subsequent treatment process.
P5:The cost of repeated tests and treatment is really high. After a long time, the pressure becomes very obvious. If more of it could be reimbursed, I would feel much more relieved.
P9:A lot of the time, after finishing one step, you just go home. But once you are back home, there are still so many questions, and you do not know who to ask or what to do next.
P14:Once I am back home, it’s actually easier to start overthinking. If someone could continue to follow up with me, I would feel much more reassured.
Subtheme 4: Need for Supportive Family Communication and Peer Support
Participants’ need for supportive family communication and peer support was closely related to their perceived lack of companionship and understanding during long-term treatment. Participants generally hoped to receive more emotional support and practical companionship from family members in order to reduce the helplessness and psychological stress caused by long-term treatment. At the same time, they also hoped to obtain experiential sharing and emotional resonance from peers with similar experiences, which helped to alleviate anxiety about subsequent treatment and pregnancy outcomes.
P6:Sometimes the hardest part is not the treatment itself, but feeling that I am carrying all of this alone. If my family could spend more time with me and listen to me, I would feel much better.
P11:My husband has always accompanied me to the hospital. Even though there are many things he cannot actually help with, as long as someone is facing it with me, I do not feel so helpless.
P12:If you talk to people who have never gone through it, they really do not understand. It is much more helpful to talk to someone who has had the same experience.
Discussion
Recognizing the Multiple Sources of Learned Helplessness and Strengthening Early Identification and Targeted Intervention
This study found that participants’ experiences related to learned helplessness appeared to be shaped by multiple stressors, including repeated implantation failure, invasive procedures, uncertainty regarding outcomes, and medical and family-related pressures. This suggests that learned helplessness in this population may be related to the long-term accumulation of multiple stressors, which is consistent with theoretical explanations linking recurrent exposure to uncontrollable stressors with learned helplessness.16 Possible explanations include the erosion of patients’ belief in the relationship between effort and outcome after repeated implantation failure; the cumulative burden of procedure-related pain and anticipatory fear associated with repeated invasive treatments; the reduced sense of control caused by prolonged treatment cycles and uncertain outcomes; and the way in which financial burden and traditional fertility beliefs reinforce personal responsibility attribution, thereby intensifying negative emotions. From the perspective of the attributional reformulation of learned helplessness, these findings suggest that participants’ experiences involved more than general distress after treatment failure. Repeated unsuccessful treatment attempts, perceived uncontrollability, self-blame, and weakened effort–outcome beliefs helped explain why these experiences were interpreted as learned helplessness rather than only infertility-related distress or treatment fatigue. Previous studies have shown that learned helplessness may reduce treatment adherence, whereas targeted health education and psychological support can improve psychological well-being.17 These findings suggest that healthcare professionals may need to be attentive to patients who repeatedly describe treatment failure, invasive procedures, uncertainty, and family-related pressure as sources of helplessness. In clinical communication, clearer explanations of treatment uncertainty and sensitive responses to family-related blame may help reduce patients’ perceived lack of control. These implications should be interpreted as preliminary.
Focusing on Manifestations of Learned Helplessness in Daily Life and Psychological Well-Being
Participants described learned helplessness-related experiences as closely intertwined with disruptions in daily life and persistent emotional distress. Some patients had to take repeated leave from work and adjust their work arrangements because of ongoing treatment. They also became more cautious about exercise, diet, and daily activities, resulting in disruption of their usual life routines, together with persistent low mood, self-denial, and sleep disturbance. This may be related to the restriction of daily role functioning caused by repeated treatment. The continued accumulation of life disruption and emotional distress may reinforce each other and further affect patients’ fertility-related quality of life and willingness to continue treatment.11,18,19 Previous studies have shown that psychological distress among infertile women and patients undergoing assisted reproductive technology is associated with poorer quality of life and coping difficulties.20,21 These findings indicate that nursing assessment may need to consider both emotional distress and disruptions in daily functioning. For patients reporting persistent distress or serious sleep disturbance, timely referral to psychological services may be considered when appropriate.
Understanding the Differentiated Characteristics of Coping Patterns and Strengthening Patients’ Positive Coping Resources
This study found that patients did not cope with repeated treatment failure in a single way; rather, differentiated coping patterns emerged under the continued influence of helplessness, which is consistent with previous findings.22 Patients’ coping patterns are closely related to infertility-related stress and psychological status,23 and may also influence their subsequent participation in treatment and their use of support resources. The three coping responses identified in this study—avoidance, passive compliance, and active adjustment—suggest that support may need to be tailored to patients’ coping patterns rather than delivered in a uniform manner.
For participants who described avoidance, non-judgmental communication and a low-pressure environment may help reduce resistance to discussing treatment-related experiences. For those showing passive compliance, clearer explanations of treatment goals and available options may help increase their sense of participation in the treatment process. For those showing active adjustment, reliable information channels and appropriate use of family or peer support may help reinforce existing coping resources. These findings suggest that future supportive care may need to consider differences in coping patterns, although the effectiveness of tailored support should be examined in further studies.
Addressing External Support Needs and Optimizing Continuity of Nursing Care
The findings of this study showed that patients with RIF had external support needs while coping with learned helplessness. These needs included disease-related information and treatment process guidance, continuous psychological support, medical insurance reimbursement and continuity of care, and supportive family communication and peer support. If these needs remain unmet over time, they may intensify patients’ uncertainty regarding the treatment process and outcomes and may further contribute to feelings of helplessness. Family companionship and peer support were regarded as important sources of emotional buffering and may be strengthened through corresponding guidance to help reduce feelings of helplessness.24 Participants’ accounts suggested that psychological support was needed not only after an unsuccessful treatment result but also during treatment intervals and the waiting period for results. This finding highlights the importance of continuous psychological support across different stages of the RIF treatment pathway.
Based on participants’ expressed needs, future nursing support may consider clearer treatment-related communication, emotional support during treatment intervals and waiting periods, follow-up guidance after leaving the hospital, and family or peer support. Future studies may examine whether these support needs can be integrated into structured nursing-led supportive care interventions, such as care bundles.25
Relevance for Clinical Practice
The findings provide preliminary insights for reproductive nursing practice. Healthcare professionals may be attentive to feelings of helplessness among patients with RIF, especially when patients describe repeated treatment failure, uncertainty, self-blame, or reduced confidence. Supportive communication, individualized information, emotional support during treatment intervals and waiting periods, and appropriate family or peer support may be considered in routine care. Given the qualitative and single-site nature of this study, these practice implications should be interpreted cautiously. Future research is needed to develop and evaluate structured supportive care approaches for patients with RIF.
Study Limitations
First, the sample source and representativeness were limited. This study used purposive sampling, and all participants were recruited from the Reproductive Medicine Center of a single tertiary hospital, with a relatively small sample size. Differences in regional culture, family fertility beliefs, and access to reproductive healthcare resources may influence patients’ experiences of learned helplessness. Therefore, the transferability of the findings to other populations and settings needs to be interpreted with caution.
Second, the findings were based on participants’ self-reported experiences and may have been influenced by recall and expression differences. Because the interviews focused on emotionally sensitive experiences related to repeated treatment failure, some participants may have selectively recalled events or had difficulty fully articulating their inner feelings, which could have affected the depth and completeness of the data. In addition, although the interview guide was designed to explore participants’ experiences related to learned helplessness, one interview question explicitly mentioned “feelings of helplessness” and “loss of confidence.” This may have shaped how some participants understood and described their experiences. Therefore, the themes should not be interpreted as having emerged from a fully inductive exploration of psychological experience, but rather as findings generated within an interview framework that included learned helplessness as a sensitizing concept. To reduce this potential influence, the interviewers used open-ended follow-up questions, avoided evaluative responses, and encouraged participants to elaborate on their experiences in their own words. Future studies may use more neutral opening questions before gradually exploring specific concepts related to learned helplessness.
Third, although the interviews provided useful descriptions of participants’ experiences, the interview duration of approximately 20–40 minutes may have limited further exploration of some deeply emotional and cumulative experiences related to repeated treatment failure. The interviewers used follow-up questions to encourage participants to elaborate on their experiences where appropriate. Future studies could consider longer interviews, repeated interviews, or longitudinal qualitative designs to obtain a more in-depth understanding of learned helplessness over time.
Fourth, this study explored learned helplessness only from the patients’ perspective and did not include the views of family members or healthcare professionals. Given that the experiences of patients with recurrent implantation failure are closely related to family interaction, medical communication, and treatment support, the absence of multiple perspectives may have limited a more comprehensive understanding of how feelings of helplessness developed and how supportive interventions could be designed.
Conclusions
This qualitative study of patients with RIF identified four themes: perceived sources of learned helplessness, manifestations of learned helplessness in daily life and psychological well-being, participants’ coping responses to learned helplessness, and external support needs for coping with learned helplessness. In clinical nursing practice, early identification, continuous psychological support, individualized informational guidance, and continuity of care may be important areas for further consideration. At the same time, greater attention may be paid to integrating family and peer support resources in order to improve patients’ psychological well-being. In the future, multidisciplinary collaboration among reproductive medicine, nursing, psychological services, and follow-up care teams may help support the development of structured and continuous patient care approaches for patients with RIF.
Data Sharing Statement
The datasets analyzed during the current study are not publicly available due to ethical and privacy reasons.
Ethics Statement
This study complied with the Declaration of Helsinki. Ethical approval for this study was granted by the Ethics Committee of Guangdong Women and Children Hospital on December 5, 2025 (Approval No. 20250101). All procedures were conducted in accordance with relevant guidelines and regulations. Written informed consent was obtained from all participants prior to their inclusion in the study.
Acknowledgments
We sincerely appreciate the medical staff and patients of the hospital for their invaluable support and assistance.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Akalewold M, Yohannes GW, Abdo ZA, Hailu Y, Negesse A. Magnitude of infertility and associated factors among women attending selected public hospitals in Addis Ababa, Ethiopia: a cross-sectional study. BMC Womens Health. 2022;22:11. doi:10.1186/s12905-022-01601-8
2. Tenchov R, Zhou QA. Assisted reproductive technology: a ray of hope for infertility. ACS Omega. 2025;10(22):22347–13. doi:10.1021/acsomega.5c01643
3. Coughlan C, Ledger W, Wang Q, et al. Recurrent implantation failure: definition and management. Reprod Biomed Online. 2014;28(1):14–38. doi:10.1016/j.rbmo.2013.08.011
4. Guo YB, Tang B, Zhang L, Wu X, Huang ZH. Anxiety and depression in recurrent implantation failure after frozen-thawed embryo transfer and efficacy of endometrial receptivity testing. World J Psychiatry. 2025;15(9):109175. doi:10.5498/wjp.v15.i9.109175
5. Ni Y, Tong C, Huang L, Zhou W, Zhang A. The analysis of fertility quality of life and the influencing factors of patients with repeated implantation failure. Health Qual Life Outcomes. 2021;19(1):32. doi:10.1186/s12955-021-01666-3
6. Seligman ME. Learned helplessness. Annu Rev Med. 1972;23:407–412. doi:10.1146/annurev.me.23.020172.002203
7. Maier SF, Seligman MEP. Learned helplessness at fifty: insights from neuroscience. Psychol Rev. 2016;123(4):349–367. doi:10.1037/rev0000033
8. Abramson LY, Seligman ME, Teasdale JD. Learned helplessness in humans: critique and reformulation. J Abnorm Psychol. 1978;87(1):49–74.
9. Xie C, Li L, Zhou L, Sun C, Zhang Y, Li Y. Mediating role of learned helplessness’ components in the association between health literacy/social support and self-management among maintenance haemodialysis patients in Changsha, China: a cross-sectional study. BMJ Open. 2023;13(8):e068601. doi:10.1136/bmjopen-2022-068601
10. Boddez Y, Van Dessel P, De Houwer J. Learned helplessness and its relevance for psychological suffering: a new perspective illustrated with attachment problems, burn-out, and fatigue complaints. Cogn Emot. 2022;36(6):1027–1036. doi:10.1080/02699931.2022.2118239
11. Braverman AM, Davoudian T, Levin IK, Bocage A, Wodoslawsky S. Depression, anxiety, quality of life, and infertility: a global lens on the last decade of research. Fertil Steril. 2024;121(3):379–383. doi:10.1016/j.fertnstert.2024.01.013
12. Hennink MM, Kaiser BN, Marconi VC. Code saturation versus meaning saturation: how many interviews are enough? Qual Health Res. 2017;27(4):591–608. doi:10.1177/1049732316665344
13. Reproductive Medicine Professional Committee of the Chinese Medical Doctor Association; Reproductive Medicine Professional Committee of the Chinese Women’s Medical Association. Expert consensus on diagnosis and treatment of recurrent implantation failure. Natl Med J China. 2023;103(2):89–100. doi:10.3760/cma.j.cn112137-20221105-02317
14. Colaizzi PF. Psychological research as the phenomenologist views it. In: Valle RS, King M, editors. Existential-Phenomenological Alternatives for Psychology. New York, NY: Oxford University Press; 1978:48–71.
15. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
16. Crielaard L, Nicolaou M, Sawyer A, Quax R, Stronks K. Understanding the impact of exposure to adverse socioeconomic conditions on chronic stress from a complexity science perspective. BMC Med. 2021;19(1):242. doi:10.1186/s12916-021-02106-1
17. Xie C, Li L, Li Y. “alive day is the day”: a qualitative study of experiences of learned helplessness in maintenance haemodialysis patients. Risk Manag Healthc Policy. 2023;16:231–245. doi:10.2147/RMHP.S401205
18. Swift A, Thomas E, Larson K, Swanson M, Fernandez-Pineda M. Infertility-related stress, quality of life, and reasons for fertility treatment discontinuation among US women: a secondary analysis of a cross-sectional study. Sex Reprod Healthc. 2024;39:100955. doi:10.1016/j.srhc.2024.100955
19. Ni Y, Huang L, Zhang E, et al. Psychosocial correlates of fertility-related quality of life among infertile women with repeated implantation failure: the mediating role of resilience. Front Psychiatry. 2022;13:1019922. doi:10.3389/fpsyt.2022.1019922
20. Bai J, Zheng J, Dong Y, Wang K, Cheng C, Jiang H. Psychological distress, dyadic coping, and quality of life in infertile clients undergoing assisted reproductive technology in China: a single-center, cross-sectional study. J Multidiscip Healthc. 2022;15:2715–2723. doi:10.2147/JMDH.S393438
21. Iordăchescu DA, Paica CI, Boca AE, et al. Anxiety, difficulties, and coping of infertile women. Healthcare. 2021;9(4):466. doi:10.3390/healthcare9040466
22. Zhao CX, Lu MT, Zhong XP, Chen JW, Chen LP. Coping strategies and influencing factors among infertile patients: a qualitative meta-synthesis. BMC Public Health. 2025;25(1):3144. doi:10.1186/s12889-025-24031-1
23. Ďurašková G, Hampl R, Dostál D. Infertility stress and coping strategies in women and men undergoing in vitro fertilization treatment. Ceska Gynekol. 2025;90(1):14–21. doi:10.48095/cccg202514
24. Martins MV, Peterson BD, Almeida VM, Costa ME. Direct and indirect effects of perceived social support on women’s infertility-related stress. Hum Reprod. 2011;26(8):2113–2121. doi:10.1093/humrep/der157
25. Sebastiani E, Scacchetti M, Cesare M, Maurici M, Loiudice MT. Identifying the bundle/care development process in clinical risk management: a systematic review. Healthcare. 2024;12(22):2242. doi:10.3390/healthcare12222242
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Shared Decision-Making in Hemophilic Arthropathy Rehabilitation: A Qualitative Study
Liu YQ, Guo YL, Xu J, Geng WJ, Li ZZ, Jia M, Liu YD, Zhao H
Patient Preference and Adherence 2023, 17:249-257
Published Date: 25 January 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Qualitative Study of Learned Helplessness in Colorectal Cancer Patients with Colostomy: A Social-Ecological Perspective
Wei X, Wu L, Chen X, Ding J, Hua Q
Patient Preference and Adherence 2026, 20:574914
Published Date: 7 January 2026