Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Critical Care Nurses’ Experiences with Endotracheal Suctioning in Critically Ill Older Adults Patients: A Phenomenological Study
Authors Tang J, Lyv J, Wu NH, Chen X, Bai JJ
Received 5 December 2025
Accepted for publication 18 February 2026
Published 7 March 2026 Volume 2026:19 586847
DOI https://doi.org/10.2147/JMDH.S586847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Jun Tang,1,* Jing Lyv,2,* Ni-Hui Wu,3 Xu Chen,4 Jiao-Jiao Bai1
1Department of Nursing, Huadong Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 2Department of Geriatric Critical Care Unit, Huadong Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 3Department of Geriatric Respiratory Intensive Care Unit, Huadong Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 4Department of Respiratory Intensive Care Unit, Huadong Hospital, Fudan University, Shanghai, 200040, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiao-Jiao Bai, Department of Nursing, Huadong Hospital, Fudan University, No. 221 Yananxi Road, Jingan District, Shanghai, 200040, People’s Republic of China, Tel +86 13331806987, Email [email protected]
Objective: This study aimed to explore nurses’ experiences with endotracheal suctioning in critically ill older adults and to generate evidence to support the development of targeted standardized protocols.
Methods: A phenomenological approach was applied to conduct in-depth interviews with 15 nurses at a tertiary hospital in Shanghai from February to March 2025. Participants met predefined inclusion and exclusion criteria. Data were analyzed using Colaizzi’s method.
Results: Three themes were identified: the unique characteristics of endotracheal suctioning in critically ill older adults; challenges encountered during suctioning and corresponding coping strategies; and nurses’ needs and recommendations for establishing standardized protocols.
Conclusion: The results of this study underscore the necessity of establishing age-specific suction parameters (such as pressure and depth) and individualized operational procedures tailored to comorbidities (such as coagulopathy), providing crucial evidence for the development of standardized protocols focused on airway fragility and complication prevention in elderly patients.
Keywords: critical ill patients, endotracheal suctioning, experience, nurse, older adults, qualitative research
Introduction
With the acceleration of population aging, critically ill older adults comprise an increasing proportion of intensive care populations. Reported data indicated that older adults accounted for 68.24% of intensive care unit patients in China.1,2 Artificial airways serve as critical interventions to maintain ventilation in this population and were essential for reducing the risk of airway obstruction and ensuring airway patency.3 However, as an invasive procedure, suctioning through an artificial airway poses greater risks for elderly patients. On one hand, the airway mucosa of elderly patients is fragile, and their blood vessels are more brittle, making improper suctioning prone to mucosal damage and bleeding. On the other hand, elderly patients often have multiple underlying diseases such as chronic obstructive pulmonary disease and cardiovascular disease, and incorrect suctioning can lead to adverse reactions such as hypoxemia and hemodynamic instability. Findings indicated that nonadherence to best practice standards during suctioning could result in mucosal damage, ventilator-associated pneumonia (VAP), atelectasis, oxygen desaturation, sympathetic stimulation, bradycardia, and increased intracranial pressure.4 The current literature lacks standardized protocols specifically addressing endotracheal suctioning in critically ill older adults. Published evidence indicates that nurses’ clinical experiences are vital for optimizing suctioning procedures, enhancing care quality, and ensuring patient safety.5,6 Nevertheless, investigations exploring nurses lived experiences and perceptions regarding endotracheal suctioning in this population remain limited. Accordingly, this study aimed to explore the experience and cognition of nurses regarding endotracheal suction in critically ill elderly patients through descriptive phenomenological research, with the goal of providing evidence-based standardized operational procedures to enhance nursing quality and reduce complications.
Participants and Methods
This study adopts the phenomenological method in qualitative research and follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) for reporting.
Participants
This study adopts purposive sampling. This study recruited registered nurses from the care departments for elderly patients with severe conditions in a tertiary hospital in Shanghai in 2025. These departments included the respiratory intensive care unit, coronary heart disease care unit, emergency intensive care unit, emergency department, respiratory medicine department, and geriatrics department. Additionally, nurses with different demographic characteristics (education, age, and years of work experience) were included using maximum variation sampling to enhance the generalizability of the research results. The determination of sample size was based on the principle of data saturation, which means to stop interviewing when no new themes emerge. No new themes emerged during interviews with nurses 16–18 in this study, resulting in the final inclusion of 15 nurses. Their demographic and clinical characteristics are shown in Table 1.
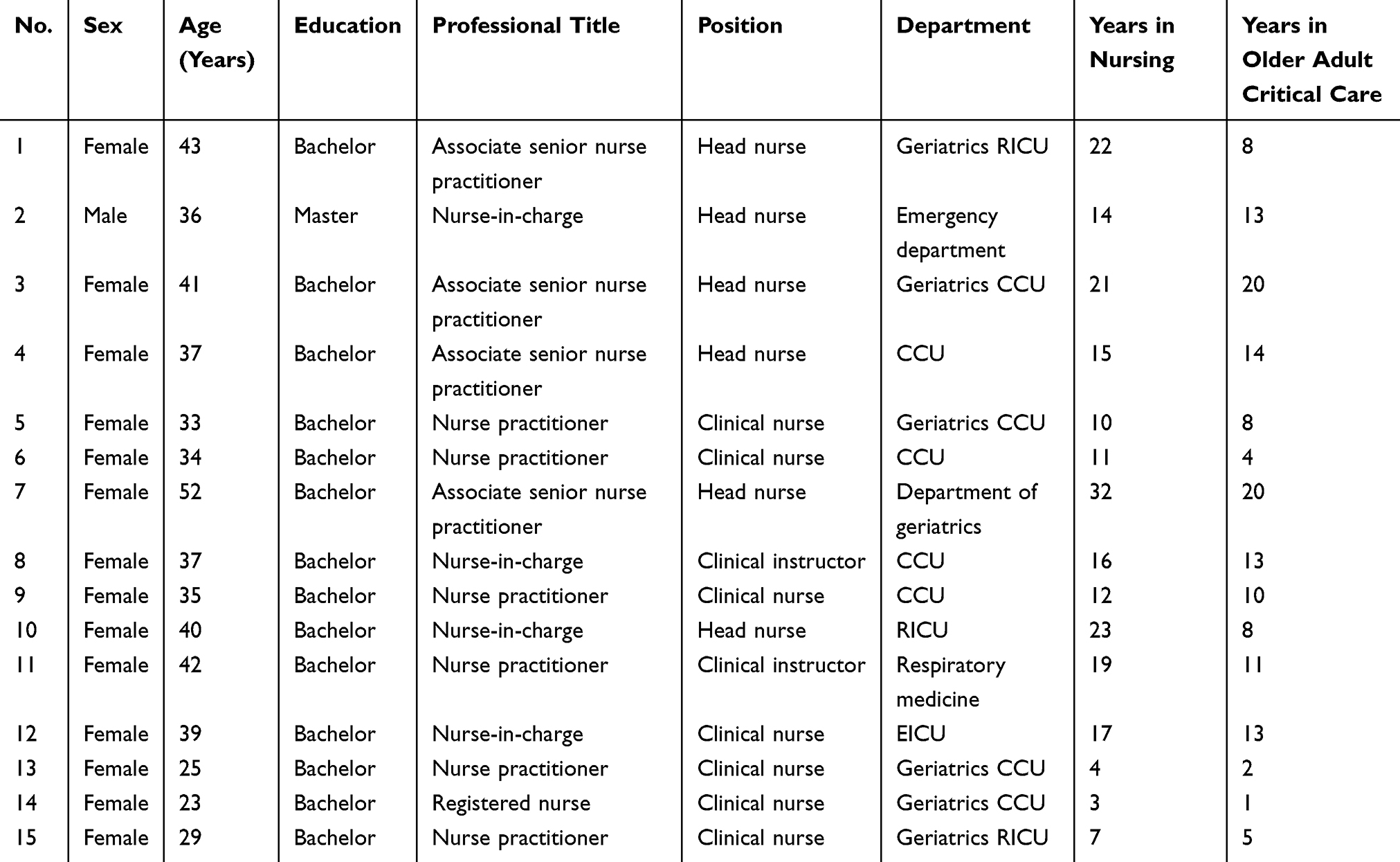 |
Table 1 Demographic and Clinical Characteristics of Critical Care Nurse Participants (n = 15) |
Inclusion criteria comprised: registered nurses with ≥1 year of experience in their current department, participation in endotracheal suctioning for critically ill older adults within the past three months, and willingness to participate.
Exclusion criteria were: student nurses, nurses on temporary training assignments or short-term clinical fellowships, and nurses absent from clinical practice for six months due to extended leave.
The Ethics Committee of Huadong Hospital, Fudan University approved the study (No. 20250015). Demographic and Clinical Characteristics of Critical Care Nurse Participants (n = 15).
Methods
Interview Guide Development
Following a review of the relevant literature and discussions within a multidisciplinary research team, a semi-structured interview guide was developed. The guide was pilot-tested with two critical care nurses to assess clarity, relevance, and feasibility; data from these pilot interviews were not included in the final analysis. Minor refinements were made before finalizing the guide. The final interview guide consisted of five open-ended questions: (1) Can you describe your experiences and key considerations when performing endotracheal suctioning in critically ill older adult patients? (2) What differences, if any, do you perceive between older and younger adult patients during endotracheal suctioning, and what factors contribute to these differences? (3) What challenges or difficulties have you encountered during suctioning, and how did you manage them? (4) Are there existing protocols for endotracheal suctioning in critically ill older adults in your unit, and what limitations, if any, have you identified? (5) In your opinion, is there a need for specialized protocols for endotracheal suctioning in critically ill older adults? Please explain and provide recommendations.
Data Collection
After contacting the research subjects, the researchers arrange a mutually convenient time and place (eg a conference room or a propaganda classroom) for face-to-face interviews. After the study purpose was introduced and informed consent obtained, semi-structured interviews were conducted and audio-recorded, while nonverbal cues were documented in field notes. Participants were encouraged to express their perspectives freely. Interviewers maintained neutrality, avoided leading questions, and sought clarification when required. Interview duration ranged from 20 to 40 minutes. At the end of the interview, the researchers will transcribe the audio recording word for word into text and import it into NVIvo software (version 12) within 24 hours. During this period, the two researchers involved in the interview will repeatedly recall and verify the content and promptly seek clarification from the interviewer to address any suspicious points, to ensure that the transcribed text matches the content expressed by the participant.
Data Analysis
Data collection and analysis were conducted concurrently in this study. The Colaizzi seven-step analysis method was employed to analyze and code the interview transcripts sentence by sentence.7 The specific steps are as follows: (1) The researcher repeatedly read the collected data to become thoroughly familiar with the content provided by the participants. (2) Two researchers (the first and second authors) independently analyzed the interview data sentence by sentence, identifying key statements related to the research question. (3) The two researchers independently summarized recurring themes and constructed the meaning of codes. (4) Summarize the coded themes, identify meaningful common viewpoints, and initially form themes. (5) The researcher provided a detailed explanation for each theme formed in step 4, including typical original statements from the participants. (6) Similar themes and statements were grouped to construct a short and meaningful phrase, termed as a theme. (7) The generated theme structure was returned to the participants for verification, asking whether it accurately described their true feelings to ensure the accuracy of the results. All authors participated in this process. To ensure the objectivity of the analysis results during data analysis, a dual coding method was adopted in this study. All data were independently coded by two researchers with experience in critical care nursing and research. After the initial coding stage, potential differences were resolved through consensus discussion, thus ensuring coding consistency.
Results
Unique Characteristics of Endotracheal Suctioning in Critically Ill Older Adults
Increased Procedural Risks from Pathophysiological Changes
All participants reported that age-related pathophysiological changes substantially increased suctioning risks in older adults. Airway mucosal fragility intensified with age, heightening the likelihood of injury during suctioning. Concurrently, diminished ciliary function and reduced respiratory muscle strength contributed to the deep accumulation of airway secretions.
P8 stated, Older adults have weaker cough ability than younger adults. Their cough reflex and force are insufficient to move deep secretions from lower to upper airways.
Older adults commonly presented with multiple comorbidities, further increasing complication risks during suctioning. Patients with coronary artery disease or stroke who received long-term anticoagulation demonstrated impaired coagulation, which increased mucosal bleeding risk. Patients with chronic obstructive pulmonary disease produced viscous secretions prone to crusting, resulting in potential airway obstruction, infection, or asphyxia. Patients with cardiopulmonary disease exhibited diminished oxygen reserves, leading to lower baseline oxygen saturation.
P12 noted, Older adults have more chronic diseases than younger adults, like chronic bronchitis or chronic obstructive pulmonary disease. Years of disease impair lung function, produce thick sputum, and cause deep accumulation and frequent pulmonary infections.
Procedure-Specific Characteristics
Participants indicated that older adults required suctioning techniques that differed from those used in younger adults. Because baseline oxygen saturation was frequently reduced, pre-oxygenation was often necessary. To manage viscous secretions, nurses optimized airway humidification and adjusted room temperature and humidity to reduce sputum viscosity and facilitate secretion removal.
Nurses applied a dual mucosal protection strategy involving reduced suction pressure and limited catheter depth. Suction pressure was adjusted based on patient condition, with shallow suctioning preferred. When deep suctioning was unavoidable, lower pressure was selected.
P10 explained, For older adults, we cannot use the higher pressure range tolerated by younger patients. We select pressure at the lower end of the acceptable range to prevent mucosal bleeding.
For tube-fed patients, positioning adjustments were implemented to prevent reflux and aspiration.
P7 stated, Older adults have slower gastric emptying than younger adults. Suctioning triggers coughing, and with relaxed cardiac sphincter tone, this may cause reflux and aspiration. Therefore, we elevate the head of the bed and turn the patient’s head to one side.
Challenges and Coping Strategies in Suctioning
Complex Challenges in Suctioning Special Patient Populations
Participants described multiple challenges encountered when suctioning critically ill older adults. In patients with bronchial carcinoma in which tumor tissue extended into the bronchial lumen, suctioning risked contact with the tumor and consequent severe bleeding. In very old adults, loose or missing teeth complicated endotracheal tube fixation and increased the risk of foreign body obstruction. Patients with neurological conditions could experience airway spasm during seizures, and head movements further impeded suctioning.
P1 stated, Some bronchial cancer patients have tumors growing into the bronchus. These patients often require intubation for respiratory failure. Each time we suction, we may touch tumor tissue and cause serious bleeding.
P3 added, Older adults may have loose or missing teeth, making tube fixation difficult—it slides around.
Critically ill older adults frequently exhibited agitation and poor cooperation, which substantially increased the difficulty of suctioning.
P6 explained, Our patients are quite old. They don’t understand their disease and resist the tube, shaking their heads constantly. They don’t understand instructions, so experienced nurses must read their reactions.
Targeted and Effective Coping Strategies
Experienced nurses adapted strategies to individual patient needs. For patients with bronchial carcinoma, nurses collaborated with physicians and used bronchoscopy to guide suctioning under direct visualization, enabling accurate secretion localization while minimizing risk to the greatest extent possible. For patients with loose teeth, nurses secured teeth using surgical sutures affixed to the cheek to prevent aspiration or ingestion. For patients unable to communicate, clinical teams used written materials or pictures to explain procedures, encouraging expression through writing or gestures. Psychological support during suctioning helped reduce anxiety and improve cooperation.
P1 noted, Bronchoscopy allows us to see inside the airway and avoid repeated injury.
P5 stated, For resistant patients, two nurses work together—one suctions while the other provides psychological support and stabilizes the head and hands.
P12 described, Throughout suctioning, we offer psychological preparation, explaining each step to gain cooperation.
Persistent Clinical Dilemmas
Several participants reported persistent challenges despite endotracheal suctioning being widely used as a core airway management technique in critically ill older adults. First, closed suctioning systems raised concerns regarding secretion removal effectiveness.
P1 stated, For infection-prone older adults, we use closed suction catheters. While they maintain oxygenation and reduce contamination, they often feel inadequate for complete secretion removal, which is a common concern among nurses.
Second, balancing suctioning frequency with bleeding risk remained difficult. Frequent suctioning could prevent infection and improve oxygenation but simultaneously increased mucosal bleeding risk.
P5 explained, When older adults have severe infection and heavy secretions, frequent suctioning is needed. But the ventilator alarms again shortly after. If we suction two or three times within thirty minutes, mucosal bleeding easily occurs, yet delayed suctioning compromises airway patency.
Third, evidence regarding the optimal interval between suctioning and nasogastric feeding was lacking.
P2 stated, For patients with nasogastric tubes, we don’t know how long to wait between suctioning and feeding. We can only rely on experience since there is no relevant research. We typically wait at least thirty minutes, but we’re unsure if this is appropriate.
Nurses’ Needs and Recommendations for Standardized Suctioning Protocols
Limitations of Current Protocols
Participants consistently identified notable deficiencies in current suctioning protocols, which insufficiently addressed the needs of critically ill older adults. Existing protocols were primarily designed for general adult patients and lacked age-specific considerations. Given structural airway changes, altered secretion characteristics, and prevalent comorbidities, older adults differed substantially from younger adults, yet current protocols did not adequately reflect these distinctions.
P3 stated, Our current protocol is based on adult standards and it’s generic. Older adults are different. Many have chronic bronchitis or emphysema with thick, difficult secretions and fragile airways that bleed easily. We must be extremely careful. We really need a protocol designed specifically for them.
Existing protocols focused mainly on procedural steps while omitting essential components such as the prevention and management of mucosal injury and bleeding. As a result, nurses frequently relied on personal experience when complications occurred, which increased clinical risk.
P6 noted, We have an evaluation standard, but it mainly covers procedural steps, which involves telling you what to do at each stage. Many important aspects aren’t included.
Additionally, much of the protocol content originated from textbooks and individual experience, lacked evidence-based support, and was outdated.
Recommendations for Protocol Development
Most participants supported developing standardized suctioning protocols specifically for critically ill older adults to enhance care quality and patient safety. Many nurses recommended identifying key differences between older and younger adult patients and incorporating these distinctions into protocols to reduce reliance on experience-based judgment.
P11 stated, Complications during suctioning are more complex in critically ill older adults. If we include common scenarios—causes, observation points, and interventions—nurses would know how to respond.
P5 indicated, We could develop something like an SOP but more detailed, demonstrating how older adults differ from adults.
Some junior nurses, reflecting on the fast-paced clinical environment, recommended concise checklists for quick reference during busy shifts.
Participants emphasized that protocols should incorporate current guidelines and expert consensus to ensure clinical validity. They particularly highlighted the need for age-appropriate suctioning pressure and catheter depth specifications.
P8 observed, Adult consensus standards recommend −80 to −150 mmHg, and international guidelines indicate pressures not exceeding −200 mmHg. No standards specify values for older adults and hence we need clear guidance on appropriate depth and pressure.
Protocols should include assessments of vital signs, breath sounds, and secretion characteristics before and after suctioning, along with strategies for preventing and managing age-related complications.
P11 noted, Older adults experience more frequent and complex complications during suctioning. Including common complications and interventions would help nurses handle emergencies better.
Given the complexity of critical illness in older adults, some participants recommended incorporating respiratory therapist consultation into protocol development.
Discussion
Recognizing the Dual Special Characteristics of Endotracheal Suctioning in Critically Ill Older Adults
Participating nurses consistently described that age-related pathophysiological changes substantially increased suctioning risks in older adults. Published evidence indicated that deteriorating airway defense mechanisms and multimorbidity predisposed older adults to VAP and airway injury during suctioning.8,9 Nurses implemented several protective measures, including pre-oxygenation, reduced suction pressure, controlled catheter depth, optimized humidification, and positioning adjustments to minimize procedural risks.
There is evidence to support these practices. Liu et al reported that adjusting suction pressure according to secretion viscosity and using shallow suctioning reduced mucosal bleeding.10 The American Association for Respiratory Care recommended verifying suction pressure before each procedure and maintaining the lowest effective setting.11 However, only 22% of healthcare personnel were reported to routinely confirm pressure settings before suctioning.12 This discrepancy indicated a need for enhanced standardization in clinical practice. Pre-oxygenation was demonstrated to reduce the incidence of post-suctioning oxygen desaturation (>4% decrease) in older adults from 38.7% to 12.4%.13 Additionally, 88% of experienced nurses extended pre-oxygenation for high-risk patients.12 Heat-moisture exchangers improved cough symptoms and secretion characteristics and reduced equipment obstruction-related replacements by 40%.14 A 45-degree semi-recumbent position improved secretion drainage, enhanced patient tolerance, and reduced mucosal injury compared with the supine or the 90-degree lateral positions.15 These measures aligned with contemporary principles of minimally invasive suctioning and patient-centered safety.16,17 Collectively, these strategies reduced procedural risks and improved suctioning efficiency.
Nurses Face Multiple Challenges When Performing Endotracheal Suctioning in Critically Ill Older Adults
Findings from this investigation indicated that nurses encountered multiple patient-specific challenges, including bleeding risk in patients with bronchial carcinoma, loose teeth in very old adults, airway spasm in individuals with neurological conditions, inadequate catheter fixation, patient agitation, and sputum crust formation associated with prolonged intubation. Reduced cardiopulmonary reserve heightened vulnerability to transient hypoxia and arrhythmias.18 Immunosenescence further increased infection risk during invasive procedures such as suctioning.19
In response to the aforementioned risks, clinical studies have shown that while high-resolution chest CT can effectively identify concealed sputum crusts.20 Its ability to monitor dynamic airway changes is limited. Fiberoptic bronchoscopy plays a prominent role in this regard.21–23 Nurses therefore needed to assess tumor characteristics and airway status to select techniques that balanced reduced suction pressure, refined procedure steps, and multidisciplinary collaboration.22,24 For patients with neurological conditions and unstable intracranial pressure, limiting non-essential suctioning was recommended because excessive suctioning increased cerebral blood flow, triggered vasoconstriction, raised intracranial pressure, compromised cerebral perfusion, and could precipitate seizures.3 Pre-suctioning bronchodilator nebulization lowered airway spasm risk.25 Modified endotracheal tube fixation devices improved anatomical conformity, enhanced stability, and reduced tube displacement.26 For agitated patients, combining restraints, music therapy, and psychological support facilitated improved cooperation.27 Although dental splints stabilized loose teeth, their use in orally intubated patients remained limited and required further evaluation.28 Despite evidence supporting these interventions, substantial patient heterogeneity underscored the importance of individualized assessment.
This investigation also identified perceived limitations of closed suctioning systems, concerns about balancing suctioning frequency with mucosal bleeding risk, and experience-based intervals between suctioning and enteral feeding. These issues highlighted gaps in current technology, limited evidence-based guidance, and insufficient multidisciplinary collaboration, particularly with respiratory therapists and nutrition specialists, to support comprehensive protocol development.29
Developing Standardized Endotracheal Suctioning Protocols for Critically Ill Older Adults Based on Pathophysiological Characteristics and Clinical Needs
Most participants emphasized the necessity of designing suctioning protocols tailored to the physiological characteristics and clinical needs of critically ill older adults. Several key elements were identified. First, optimizing protocol content and defining age-specific parameters were essential. Protocols should delineate pre- and post-suctioning assessments, appropriate suction pressure and catheter depth, and strategies for preventing and managing complications. The American Association for Respiratory Care recommended modifying suctioning techniques according to patient population characteristics.11 For older adults, guidance includes maintaining suction pressure between −80 and −150 mmHg, prioritizing shallow suctioning, extending pre-oxygenation to 2 to 3 minutes, and limiting suction pressure to −80 mmHg in individuals with coagulopathy. However, given the fragile airway mucosa and impaired cardiopulmonary function observed in older adults, individualized adjustment of these parameters remains critical to prevent secondary injury while maintaining procedural safety and effectiveness.
Second, a tiered protocol design could accommodate varying experience levels. Senior nurses preferred detailed guidance addressing complex scenarios, whereas junior nurses required concise checklists to navigate fast-paced clinical settings. This need aligned with a tiered training and protocol model.30 Basic checklists enhanced standardization and reduced errors among junior nurses, while supplementary information provided experienced nurses with comprehensive direction for managing complicated situations. Digital decision-support tools could further strengthen protocol implementation. By integrating patient data, clinical progression, and real-time monitoring, intelligent algorithms may identify risks such as bleeding or hypoxemia during suctioning.31 These systems can provide alerts, assist with decision-making, and support individualized care planning, ultimately improving the safety and quality of endotracheal suctioning in critically ill older adults.
Advantages and Limitations
This study is the first to explore the experience of nurses in suctioning sputum from the artificial airway of elderly critically ill patients, providing a reference basis for the development of standardized clinical training programs and operational procedures. From the perspective of nurses in this study, it is revealed that the development of a suction protocol for elderly patients not only requires adjustments to technical parameters but also necessitates a systematic consideration of the decision-making dilemmas arising from their comorbidities and decreased physiological reserves. However, there are still certain limitations: (1) The study only selected 15 nurses as research subjects, which is a relatively limited sample size. Although purposeful sampling and the maximization of diversity strategy were employed to accommodate subjects with different characteristics as much as possible, in order to enrich research information and enhance the depth and saturation of the study, it is still difficult to comprehensively cover the nurse population who care for elderly critically ill patients with artificial airway in different levels, different working years, and different departments. The representativeness of the sample is somewhat limited. (2) This study is a qualitative study, and the formation of its research results is closely related to background factors such as the clinical environment, nursing team atmosphere, and regional medical resources of the research subjects. In the future, the sample size can be expanded to include nurses from different regions and different levels of medical institutions to conduct quantitative research, in order to further enrich and verify the results of this study.
Conclusion
This qualitative investigation conducted interviews with 15 nurses to examine their experiences with endotracheal suctioning in critically ill older adults. Older adults demonstrated distinct airway characteristics that posed substantial challenges during suctioning procedures. These findings indicated the need for strengthened training, integration of digital decision-support tools, and the development of standardized protocols through multidisciplinary collaboration. Future research should extend beyond a single tertiary hospital in Shanghai by incorporating larger and more diverse samples and implementing evidence-based approaches to support comprehensive protocol development.
Abbreviations
CT, Computed Tomography; SOP, Standard Operating Procedure; VAP, Ventilator-associated Pneumonia.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Huadong Hospital, Fudan University (No. 20250015). This study was conducted in accordance with the declaration of Helsinki. Informed consent for publication of anonymized responses and direct quotes was obtained from all participants.
Acknowledgments
We thank the staff for their dedicated work in implementing the study’s intervention and evaluation.
Funding
1. Shanghai Shenkang Hospital Development Center Municipal Hospital Clinical Technology Promotion and Optimization Management Project (No. SHDC22022231); 2. Huadong Hospital (Nursing) Elite Talent Program (No. HLJY2203).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hu MY, Huang HY, Luo J, et al. Research progress of airway clearance in elderly patients with severe disease. J Nurses Train. 2023;38(3):233–10. doi:10.16821/j.cnki.hsjx.2023.03.009
2. Jiang J, Wang YE, Wang ZJ. Analysis of related factors of mechanical ventilation in EICU patients with severe respiratory disease at different ages. J Bengbu Med Coll. 2021;46(11):1616–8+22. doi:10.13898/j.cnki.issn.1000-2200.2021.11.030
3. Yu S, Yan L, Sheng TG, et al. Summary of evidence: sputum suctioning care in traumatic brain injury patients with artificial airways. Chin J Minimal Invas Neurosurg. 2024;28(09):563–568. doi:10.11850/j.issn.1009-122X.2024.09.012
4. Joshi PR. Pulmonary diseases in older patients: understanding and addressing the challenges. Geriatrics. 2024;9(2). doi:10.3390/geriatrics9020034
5. Han ML, Hu MM, Zhang SQ, et al. A qualitative study of the experience of mechanical ventilation in patients with artificial airways in the intensive care unit. Chin Gen Pract Nurs. 2014;12(34):3181–3183. doi:10.3969/j.issn.1674-4748.2014.34.005
6. Deng J, Huang S, Zou D, et al. Investigation of the airway management practice of emergency department ward nurses: a nationwide survey in China. BMJ Open. 2021;11(12):e049869. doi:10.3390/geriatrics9020034
7. Liu M. Using an example to illustrate Colaizzi′s phenomenological data analysis method. J Nurs Sci. 2019;34(11):90–92. doi:10.3870/j.issn.1001-4152.2019.11.090
8. Luo CX, Deng J, Liu XM, et al. Application of individualized nursing strategy in artificial airway management of elderly patients with critical illness. China Med Pharm. 2024;14(10):95–98. doi:10.20116/j.issn2095-0616.2024.10.23
9. Yang X, Cheng J, Wang Z, et al. High-flow nasal cannula oxygen therapy versus noninvasive ventilation for elderly chronic obstructive pulmonary disease patients after extubation: a noninferior randomized controlled trial protocol. BMC Pulm Med. 2024;24(1):539. doi:10.1186/s12890-024-03342-w
10. Liu W, Gu C, Li M, et al. Safe and effective pressure of endotracheal tube suctioning based on sputum viscosity grades during artificial airway open suctioning procedures: a double-blind randomized controlled trial. Nurs Crit Care. 2024. doi:10.1111/nicc.13203
11. Blakeman TC, Scott JB, Yoder MA, et al. AARC clinical practice guidelines: artificial airway suctioning. Respir Care. 2022;67(2):258–271. doi:10.4187/respcare.09548
12. Singh R, Bhalotra AR, Sharma S. Audit on practices of endotracheal suctioning in intensive care unit patients among Health Care Workers (HCWs). Indian J Crit Care Med. 2024;28(1):58–65. doi:10.5005/jp-journals-10071-24615
13. Maggiore SM, Lellouche F, Pignataro C, et al. Decreasing the adverse effects of endotracheal suctioning during mechanical ventilation by changing practice. Respir Care. 2013;58(10):1588–1597. doi:10.4187/respcare.02265
14. Ward EC, Hancock K, Boxall J, et al. Post-laryngectomy pulmonary and related symptom changes following adoption of an optimal day-and-night heat and moisture exchanger (HME) regimen. Head Neck. 2023;45(4):939–951. doi:10.1002/hed.27323
15. Fan H, Huang JS, Su WJ, et al. Comparison of the effects of different positions for expectoration in neurosurgical tracheotomy patients. Chin Gen Pract Nurs. 2023;21(32):4556–4560. doi:10.12104/j.issn.1674-4748.2023.32.022
16. Da L, Zhang K. Early pulmonary rehabilitation in ARDS patients: effects on respiratory function and long-term outcomes: a retrospective study. Medicine. 2024;103(51):e41023. doi:10.1097/MD.0000000000041023
17. Sontakke NG, Sontakke MG, Rai NK. Artificial airway suctioning: a systematic review. Cureus. 2023;15(7):e42579. doi:10.7759/cureus.42579
18. Eggen IB, Brønstad G, Langeland H, et al. Short-term effects of endotracheal suctioning in post-cardiac arrest patients: a prospective observational cohort study. Resusc Plus. 2022;10:100221. doi:10.1016/j.resplu.2022.100221
19. Blot S, Koulenti D, Dimopoulos G, et al. Prevalence, risk factors, and mortality for ventilator-associated pneumonia in middle-aged, old, and very old critically ill patients. Crit Care Med. 2014;42(3):601–609. doi:10.1097/01.ccm.0000435665.07446.50
20. Ng JKM, Cheung W, Li JJX, et al. Detection of early (T1) lung cancers and lepidic adenocarcinomas in sputum and bronchial cytology. Ann Diagn Pathol. 2023;67:152191. doi:10.1016/j.anndiagpath.2023.152191
21. Shu C, Liu YJ, Zheng KF, et al. Diagnosis and treatment of primary tracheobronchial tumors. Cancer Med. 2025;14(9):e70893. doi:10.1002/cam4.70893
22. Qian K, Wei Y, Liu X, et al. A missed diagnosis of sputum crust with fiberoptic bronchoscope causing extubation failure: a case report. BMC Pulm Med. 2023;23(1):153. doi:10.1186/s12890-023-02457-w
23. Huang YS, Chen JL, Ko WC, et al. Clinical variables and radiomics features for predicting pneumothorax in patients undergoing CT-guided transthoracic core needle biopsy. Radiol Cardiothorac Imaging. 2024;6(3):e230278. doi:10.1148/ryct.230278
24. Zheng PT, Ji CN, Wang YR, et al. Construction and validation of a postoperative lung infection prevention care program for lung cancer patients. Chin J Nurs. 2024;59(07):820–827. doi:10.3761/j.issn.0254-1769.2024.07.008
25. Kara S, Yildirim D. Analysis of youtube videos for artificial airway suctioning training of nurses: a content analysis. J Eval Clin Pract. 2025;31(2):e70053. doi:10.1111/jep.70053
26. Xie XH. Application and nursing effect of improved fixed method of tracheal intubation. Chin J Mod Drug App. 2019;13(07):166–168. doi:10.14164/j.cnki.cn11-5581/r.2019.07.095
27. Jiao XP, Wang ZW, Han SY. Progress of intervention research on agitated behaviour in elderly ICU patients. J Nurs. 2025;32(03):38–42. doi:10.16460/j.issn1008-9969.2025.03.038
28. Jiang W, Wang P. An analysis of the efficacy of intermaxillary traction combined with strong internal fixation in the treatment of facial comminuted fractures by arch splinting. Doctor. 2024;9(05):114–116. doi:10.3969/j.issn.2096-2665.2024.05.037
29. Rogalski E, Bona M, Esparza M, et al. Efficacy of Communication Bridge-2 for primary progressive aphasia: a randomized controlled trial of communication intervention. Alzheimers Dement. 2025;21(3):e70088. doi:10.1002/alz.70088
30. Wang Y, Wu JJ, Xu FF, et al. Effect of geriatric nutritional risk index (GNRI)-based stratified diet intervention onnutritional status and self-efficacy in elderly patients with maintenance hemodialysis. Chin J Blood Purif. 2022;21(07):536–540. doi:10.3969/j.issn.1671-4091.2022.07.016
31. Choi JY, Rhee CK. Predicting asthma exacerbation risk in the adult South Korean Population using integrated health data and machine learning models. J Asthma Allergy. 2024;17:783–789. doi:10.2147/JAA.S471964
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
A Qualitative Study of the Experience of Multidisciplinary Teamwork in Chronic Critical Illness Patients
Xu X, Jing M, Zhu Y, Jin H, Li L
Journal of Multidisciplinary Healthcare 2025, 18:827-836
Published Date: 13 February 2025
Transition from Hospital to Home-Based Care for Older Adults in Southwestern Uganda: Informal Caregiver’s Experiences
Owokuhaisa J, Wiens MO, Musinguzi P, Rukundo GZ
Journal of Multidisciplinary Healthcare 2025, 18:1461-1472
Published Date: 12 March 2025
Barriers to Home-Based Medication Self-Management Among Older Adults with Multimorbidity: A Qualitative Study Guided by Empowerment Theory
Zhang Z, Bai X, Hao L, Wang Y
Patient Preference and Adherence 2025, 19:3985-3998
Published Date: 11 December 2025
Qualitative Study of Learned Helplessness in Colorectal Cancer Patients with Colostomy: A Social-Ecological Perspective
Wei X, Wu L, Chen X, Ding J, Hua Q
Patient Preference and Adherence 2026, 20:574914
Published Date: 7 January 2026