Back to Journals » International Journal of General Medicine » Volume 19
Public Knowledge and Acceptance of Artificial Intelligence–Assisted Physicians in Saudi Arabia: A Cross-Sectional Study
Authors Alhindi Y ![]() , Almoqati H, Alsaadi R, Alabbas LM, Alhuzali M, Alamoudi R, Khawaji H, Alharbi AA, Fallatah A, Muharrij A, Alluhaybi MB, Alotaibi WS, Alahmadi B, Alqurashi N, Fairaq A
, Almoqati H, Alsaadi R, Alabbas LM, Alhuzali M, Alamoudi R, Khawaji H, Alharbi AA, Fallatah A, Muharrij A, Alluhaybi MB, Alotaibi WS, Alahmadi B, Alqurashi N, Fairaq A
Received 14 January 2026
Accepted for publication 14 March 2026
Published 25 March 2026 Volume 2026:19 591213
DOI https://doi.org/10.2147/IJGM.S591213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Yosra Alhindi,1 Hatoun Almoqati,2 Reema Alsaadi,2 Lujain Mohammad Alabbas,2 Munayfah Alhuzali,2 Raghad Alamoudi,2 Huda Khawaji,2 Azam Amin Alharbi,2 Alaa Fallatah,2 Abrar Muharrij,2 Maram Bakheet Alluhaybi,2 Waad Saleh Alotaibi,3 Bashaer Alahmadi,4 Najwa Alqurashi,4 Arwa Fairaq5
1Department of Pharmacology and Toxicology, Faculty of Medicine, Umm Al Qura University, Makkah, Saudi Arabia; 2College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia; 3Riyadh Pharmacies, Riyadh, Saudi Arabia; 4Family Physician Consultants, Albohyrat Primary Care Center, Makkah, Saudi Arabia; 5Pharmaceutical Practice Department, Faculty of Pharmacy, Umm Al Qura University, Makkah, Saudi Arabia
Correspondence: Yosra Alhindi, Email [email protected]
Background: Artificial intelligence (AI) technologies are increasingly integrated into healthcare systems worldwide. However, successful implementation depends largely on public trust and acceptance. Limited evidence is available regarding public perceptions of AI-based medical consultation in Saudi Arabia.
Objective: This study aimed to assess public knowledge and acceptance of artificial intelligence doctors as a partial alternative to human physicians in Saudi Arabia and identify demographic factors influencing these perceptions.
Methods: A cross-sectional online survey was conducted among members of the general public in Saudi Arabia. The questionnaire assessed demographic characteristics, awareness of AI technologies, knowledge of AI healthcare applications, perceptions of AI doctors, and willingness to use AI-assisted medical consultation. Descriptive statistics were used to summarize responses, and Chi-square tests were performed to examine associations between demographic factors and participants’ acceptance levels.
Results: A total of 303 participants completed the survey. Most respondents reported prior awareness of artificial intelligence applications in healthcare. However, acceptance of AI as a partial substitute for human physicians remained cautious. Participants acknowledged potential benefits such as efficiency and diagnostic support but expressed concerns regarding trust, reliability, and ethical considerations.
Conclusion: While awareness of AI technologies in healthcare appears relatively widespread among the Saudi public, acceptance of AI-based medical consultation remains moderate. Educational initiatives and transparent regulatory frameworks may enhance public trust and facilitate responsible integration of AI technologies into healthcare systems.
Keywords: artificial intelligence, healthcare, public perception, acceptance, Saudi Arabia, physicians
Introduction
Artificial intelligence (AI) has rapidly emerged as a transformative technology in modern healthcare.1 AI-based systems have demonstrated potential in medical imaging interpretation, disease diagnosis, clinical decision support, and drug discovery. These technologies may enhance healthcare efficiency, reduce diagnostic errors, and support physicians in providing personalized patient care.2,3 One of AI’s key strengths is its ability to analyse vast amounts of medical data quickly, enabling faster and more objective decision-making compared to human practitioners.4
The integration of AI in healthcare offers numerous benefits. For instance, AI-based diagnostic systems can detect early signs of diseases such as cancer and cardiovascular conditions with high precision, often outperforming traditional diagnostic methods. AI is also being used in telemedicine, predictive analytics, and robotic-assisted surgeries, enhancing both the quality and accessibility of healthcare. Moreover, AI technologies support healthcare management systems by optimizing resource allocation and reducing operational costs. However, despite these advancements, challenges such as data bias, ethical considerations, and the need for human oversight remain major concern.5
Despite these potential advantages, successful implementation of AI in healthcare depends not only on technological performance but also on public acceptance and trust.6 Patients’ willingness to interact with AI-powered systems plays a crucial role in determining how effectively these technologies can be adopted in clinical settings. Concerns regarding data privacy, reliability, ethical issues, and lack of human interaction may influence public perceptions of AI in healthcare.5–7
Globally, several studies have investigated public perceptions of AI technologies in medicine. However, findings vary across countries due to differences in healthcare systems, cultural factors, and levels of technological exposure.8 In Saudi Arabia, digital health technologies are increasingly being promoted as part of national healthcare transformation initiatives aligned with Vision 2030. Nevertheless, limited research has explored public knowledge and acceptance of AI-driven medical consultation within the Saudi population.8
Understanding public perceptions of AI in healthcare is essential for policymakers, healthcare providers, and technology developers. Such information may help identify barriers to adoption and guide strategies to enhance trust and responsible integration of AI technologies into healthcare services.
Methods
Study Design
A cross-sectional survey was conducted among members of the general public in Saudi Arabia between February 10 and April 28, 2025.
Study Population
The study targeted adults residing in Saudi Arabia. Participants were eligible if they were aged 18 years or older and able to complete the online questionnaire. Electronic consent was taken before starting the survey.
Survey Instrument
The questionnaire was adapted from previously published studies examining awareness and attitudes toward artificial intelligence in healthcare.9 The survey included sections assessing demographic characteristics, awareness of AI technologies, knowledge of AI healthcare applications, perceptions toward AI doctors, and acceptance of AI-assisted medical consultation.
Data Collection
The survey was distributed online through social media platforms and community networks. Participation was voluntary and anonymous.
Sample Size Calculation
The minimum required sample size was calculated using a 95% confidence level and 5% margin of error. The estimated sample size was 384 participants. However, 303 completed responses were obtained and included in the final analysis.
Instrument Development and Validation
The questionnaire was originally developed in Arabic to ensure linguistic and cultural relevance. It was subsequently translated into English and back-translated into Arabic by bilingual experts to verify translation accuracy and conceptual equivalence. The survey instrument was adapted from previously validated questionnaires identified in related literature and was reviewed by academic experts in health informatics and medical ethics to confirm clarity, content validity, and alignment with the study objectives.
The final version of the instrument comprised five sections:
1. Sociodemographic characteristics: including age, gender, education level, occupation, and whether the respondent worked in healthcare.
2. Knowledge of AI: assessing participants’ awareness, understanding, and prior exposure to AI technologies.
3. Acceptance and trust in AI: measuring willingness to engage with or rely on AI-assisted healthcare tools.
4. Concerns and barriers: evaluating apprehensions regarding AI, including data privacy, accuracy, and the absence of human empathy.
5. Perceived impact: exploring opinions on how AI may influence the quality, accessibility, and efficiency of healthcare services.
Attitudinal items were rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree).
Ethical Considerations
The questionnaire link was disseminated digitally to reach a diverse population across Saudi Arabia. No personally identifiable information was collected. Participation was voluntary, and all responses were treated with strict confidentiality. Electronic informed consent was obtained at the beginning of the survey. The study adhered to the ethical principles outlined in the Declaration of Helsinki (2013 revision) and received ethical approval from the appropriate institutional review committee. Ethical approval was taken from Umm Al-Qura University IRB committee with the Approval No. (HAPO-02-K-012-2025-04-2636).
Data Analysis
Data were cleaned, coded, and analysed using IBM SPSS Statistics, Version 31.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics—including frequencies, percentages, means, and standard deviations—were used to summarize participants’ demographic characteristics and survey responses. The relationships between sociodemographic variables and levels of knowledge or acceptance of AI were examined using Chi-square (χ2) tests. A p-value of <0.05 was considered statistically significant for all inferential analyses.
Operational Definitions
Awareness: Participants’ prior familiarity with artificial intelligence technologies in healthcare.
Knowledge: Participants’ understanding of AI applications in medical diagnosis, treatment support, and healthcare management.
Acceptance: Participants’ willingness to use AI-based medical consultation or allow AI systems to assist physicians in healthcare decision-making.
Results
Participant Characteristics
A total of 303 individuals participated in the study. The majority were female (63.0%), while males accounted for 37.0%. The age distribution revealed that most respondents were between 18–27 years (24.1%), 28–37 years (21.5%), and 38–47 years (21.5%), whereas only 22.4% were older than 50 years. Most participants held a bachelor’s degree (68.3%), followed by those with a master’s degree or higher (11.9%). Regarding occupation, 36.6% were employed in non-healthcare sectors, 20.8% were healthcare professionals, 15.2% were students, and 17.2% were unemployed. Only 27.7% reported working in healthcare-related professions, including 3.0% specialist physicians, 1.3% general practitioners, and 23.4% other healthcare professionals (Table 1).
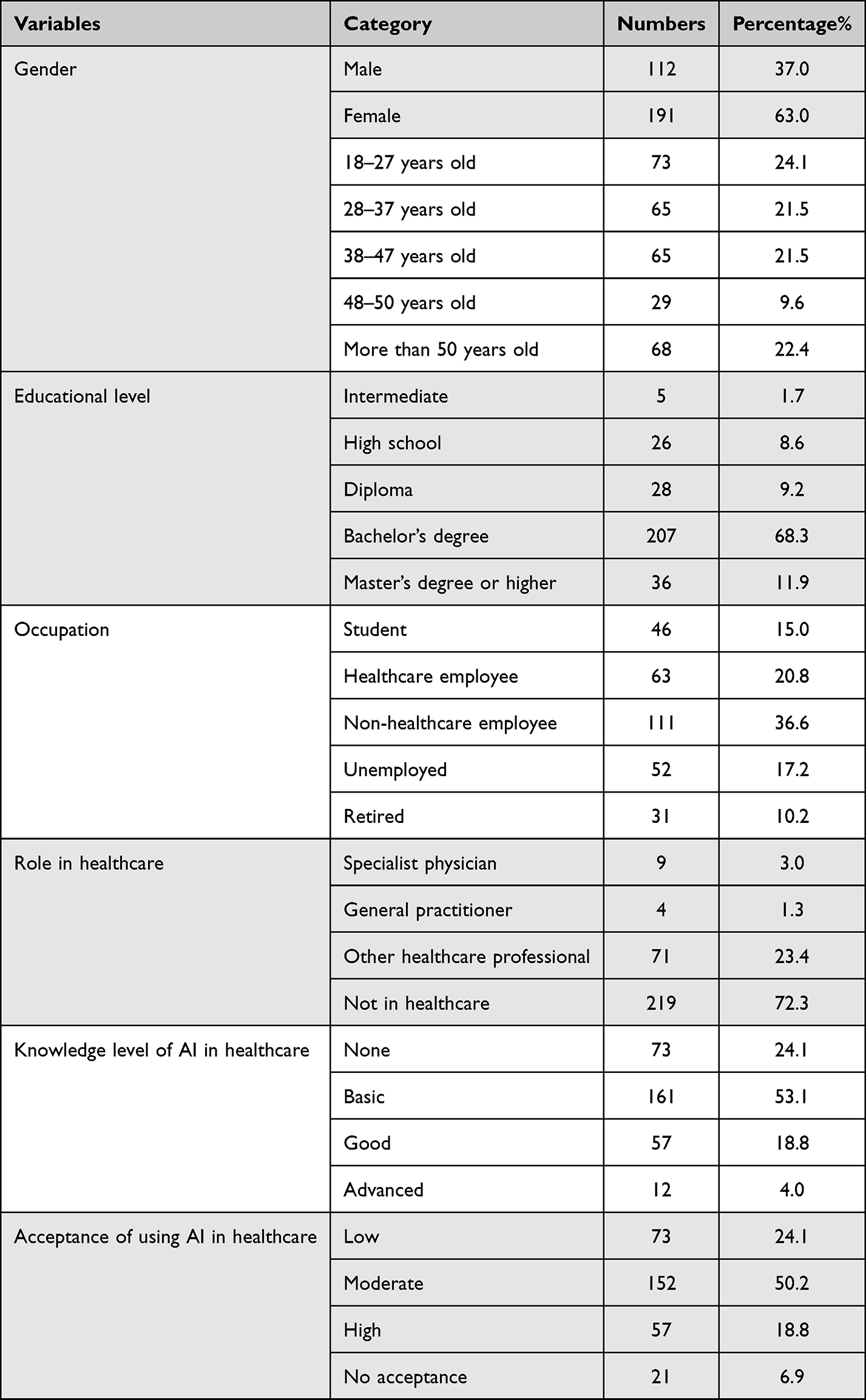 |
Table 1 Participants Demographics (n=303) |
Knowledge and Awareness of Artificial Intelligence in Healthcare
More than half of the respondents (53.1%) demonstrated basic knowledge of artificial intelligence (AI), while 18.8% had good knowledge, 24.1% reported no knowledge, and only 4.0% indicated an advanced level. Most participants (80.5%) had prior awareness of AI, and 75.9% recognized that AI is currently utilized in healthcare settings. Social media was identified as the primary information source for AI in healthcare (58.4%), followed by news or scientific journals (11.9%), educational courses (6.9%), and university training (5.3%) (Table 2).
 |
Table 2 Participants’ Knowledge and Awareness About Artificial Intelligence (n=303) |
Attitudes and Acceptance of AI in Healthcare
Regarding acceptance of AI in healthcare, approximately half of the participants (50.2%) reported moderate acceptance, while 18.8% expressed high acceptance, 24.1% low acceptance, and 6.9% no acceptance at all. Most respondents (62.7%) believed that AI in medicine would be beneficial, and 61.7% agreed that AI could enhance healthcare efficiency. However, 48.2% disagreed with the idea of AI serving as a partial substitute for human physicians, reflecting persistent skepticism toward AI-driven medical decision-making (Table 3).
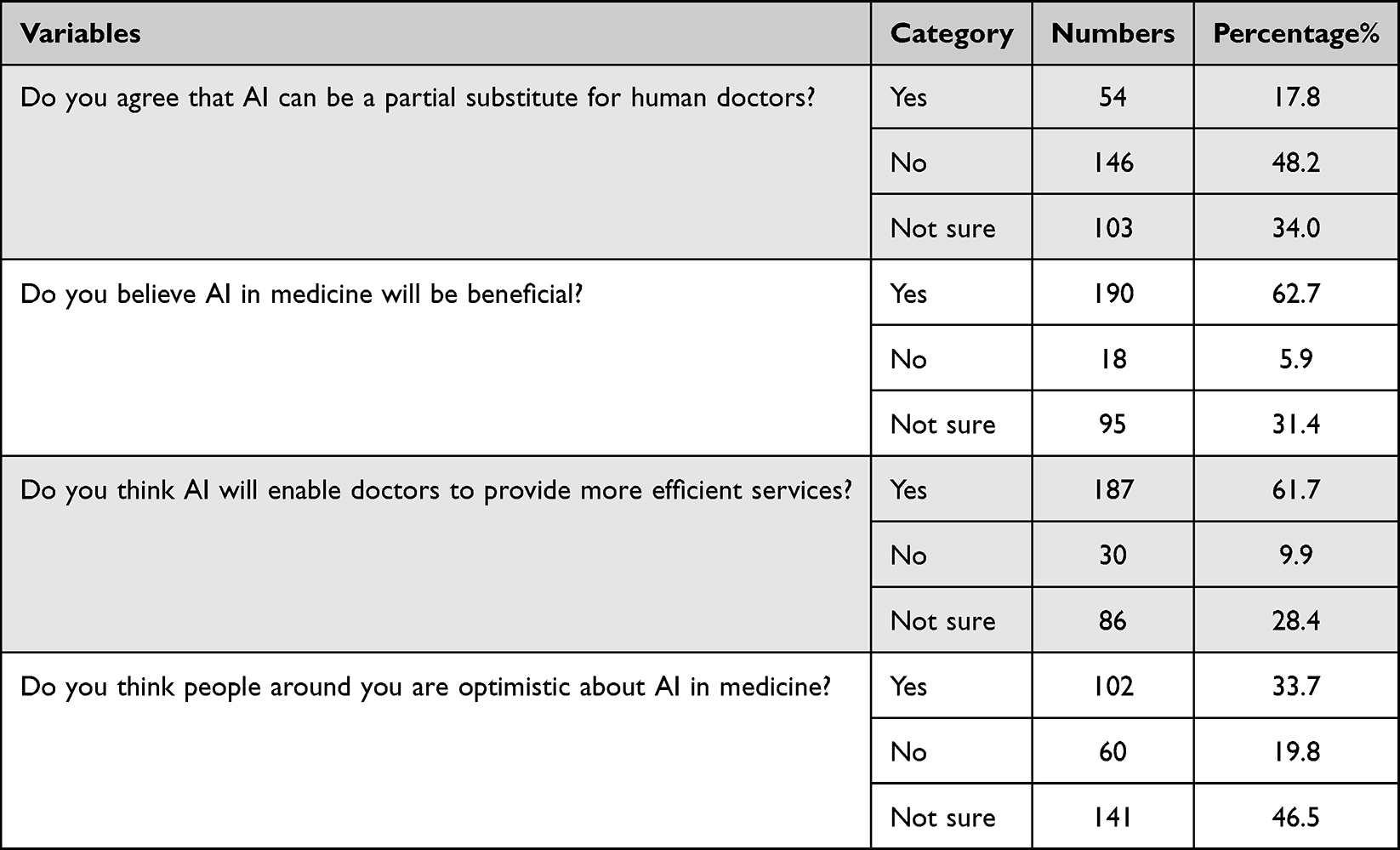 |
Table 3 Participants’ Perspectives About the Use of an Artificial Intelligence Doctor as a Partial Alternative for a Human Physician (n = 303) |
Perceived benefits of AI-powered virtual doctors included improved access to care in remote areas, reduced workload for human clinicians, decreased medical errors, provision of unbiased consultations, and lower healthcare costs (Figure 1). Conversely, the most frequently reported concerns were the lack of human empathy, risk of misdiagnosis due to limited contextual understanding, data privacy issues, and fear of AI replacing human physicians (Figure 2).
 |
Figure 1 Perceived advantages of AI-powered virtual doctors among participants (n=303). |
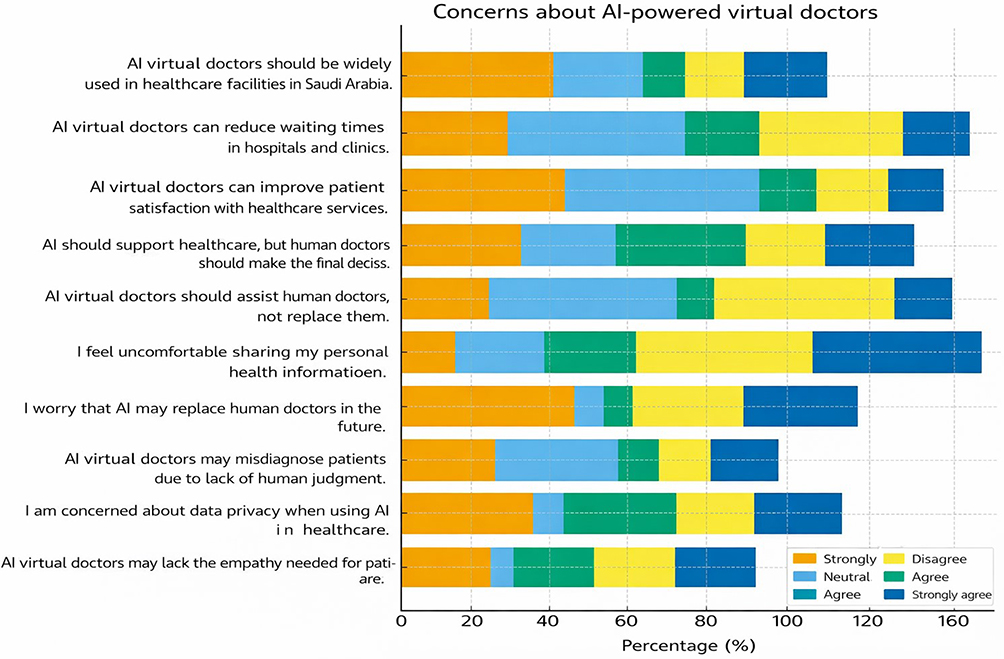 |
Figure 2 Concerns about AI-powered virtual doctors among participants (n=303). |
Factors Associated with Knowledge of AI
Chi-square analyses demonstrated that knowledge of AI was significantly associated with age group (p < 0.001), occupation (p < 0.001), and role in healthcare (p < 0.001). Participants aged above 38 years and those employed in healthcare or technical professions exhibited greater knowledge levels compared with younger or non-healthcare participants. No significant associations were observed between knowledge level and gender or educational attainment (Table 4).
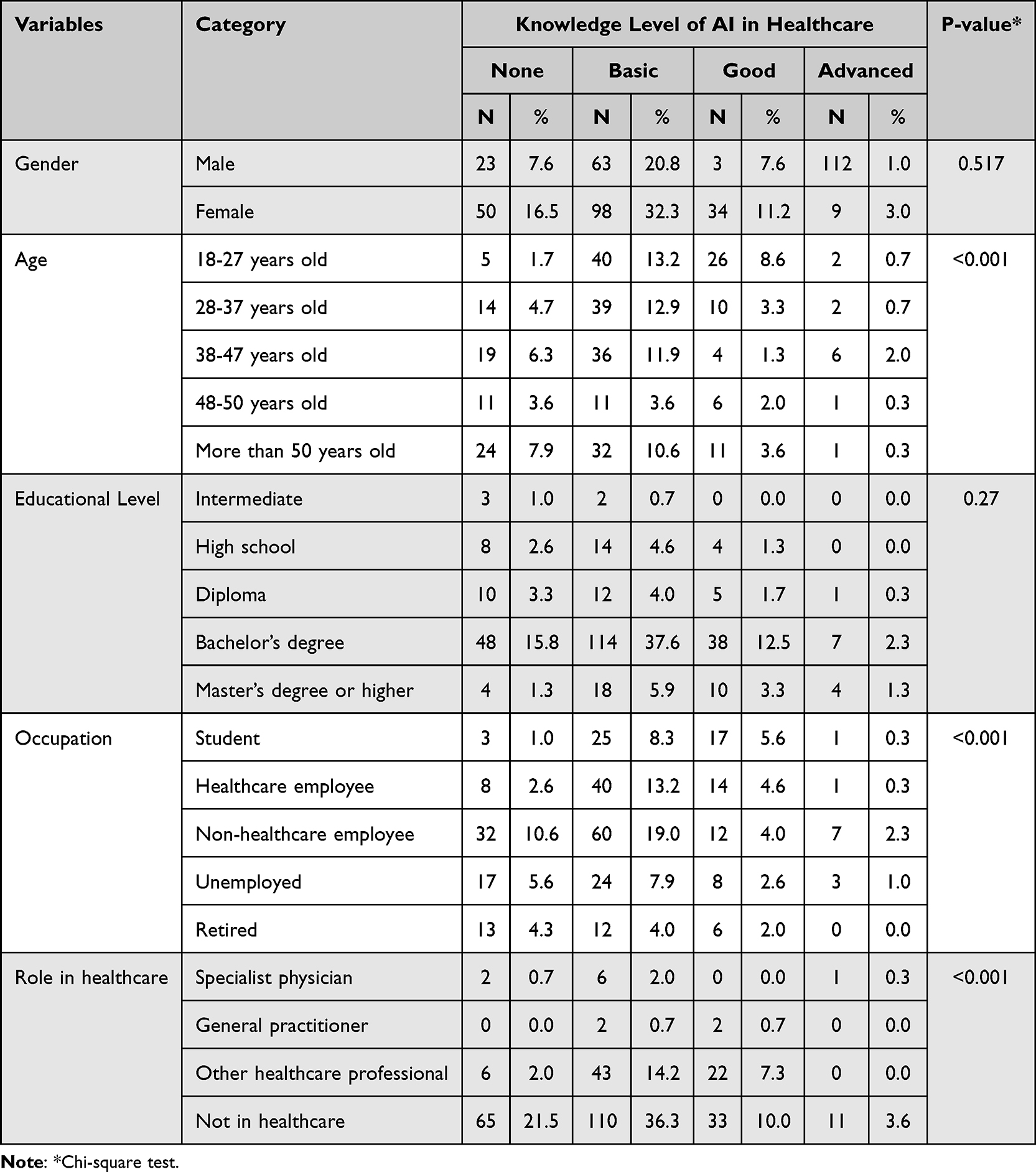 |
Table 4 Knowledge of Artificial Intelligence Based on Sociodemographic Characteristics |
Factors Associated with Acceptance of AI
Acceptance levels of AI in healthcare varied across sociodemographic categories. Although gender and age were not significantly associated with acceptance, occupation showed a borderline association (p = 0.051), suggesting that healthcare workers tended to have more favourable attitudes than non-healthcare participants (Table 5).
 |
Table 5 Acceptance of Artificial Intelligence Based on Sociodemographic Characteristics |
Furthermore, acceptance was significantly associated with knowledge level (p = 0.008), where participants with higher AI knowledge demonstrated greater acceptance and trust toward its implementation in healthcare practice (Table 6). This positive relationship underscores the importance of education and awareness in shaping public attitudes toward emerging digital health technologies.
 |
Table 6 Association Between Knowledge and Acceptance of Artificial Intelligence |
Discussion
This study explored public and professional awareness, acceptance, and perceived barriers regarding artificial intelligence (AI) integration in healthcare in Saudi Arabia. The results contribute to the growing body of literature assessing how demographic, occupational, and educational factors influence attitudes toward AI applications in medicine.10,11 The findings suggest that while awareness of AI in healthcare is relatively widespread, acceptance of AI doctors remains cautious due to concerns about trust, reliability, and ethical considerations.
Moreover, our results demonstrated a generally positive perception of AI in healthcare, consistent with previous Saudi and international studies reporting growing optimism toward AI-assisted medical technologies.9,11,12 Many participants, especially younger and highly educated individuals, exhibited greater awareness of AI applications, aligning with prior research linking technological literacy with education level.12,13 A 2025 survey of Saudi medical students similarly revealed that those with prior exposure to AI tools had higher readiness scores and more positive attitudes.12 Despite increasing awareness, several participants expressed uncertainty about the reliability and ethical use of AI-driven systems.14,15 This observation reinforces global findings that awareness does not necessarily translate into trust or readiness for clinical adoption.16,17
Acceptance of AI as a partial substitute for human doctors was primarily influenced by occupation, echoing earlier evidence that healthcare experience shapes attitudes toward AI.11,13 Healthcare professionals often express both enthusiasm and caution—acknowledging efficiency benefits but also fearing potential loss of clinical autonomy or human judgment.15,16, Public participants outside healthcare were more accepting of AI in administrative and diagnostic roles but less so in direct patient interaction, suggesting the persistence of concerns related to empathy and accountability.9,17, These attitudes mirror findings from other Gulf-region studies emphasizing the cultural and ethical dimensions of AI acceptance.9,18
Although participants recognized AI’s potential to improve diagnostic accuracy, reduce human error, and expand access to care, significant barriers remain. The most cited obstacles were limited AI education, lack of institutional support, and concerns about privacy and data security.5,8,19 This aligns with recent systematic reviews identifying workforce training, governance, and ethical uncertainty as major impediments to AI adoption.7,10,20 A Saudi review of the healthcare sector further found that only a small percentage of hospitals had implemented AI-based systems due to cost, infrastructure, and policy limitations.1,21 Globally, similar constraints persist in areas such as algorithm transparency, interoperability, and regulatory oversight.15,22 Building organizational readiness and developing AI governance frameworks are essential to ensure safe and equitable deployment.13,23
Moreover, the results underscore the need for national strategies promoting AI literacy, ethics, and infrastructure development. Integrating AI-focused education into medical and allied health curricula could enhance acceptance and preparedness.4,6,19 Structured training programs emphasizing clinical safety, patient communication, and ethical awareness can reduce misconceptions and build trust among practitioners.12,18 Additionally, collaboration between the Ministry of Health, academic institutions, and technology providers is vital to establish regulatory frameworks ensuring transparency, data protection, and algorithmic fairness.9,20,21,23
Longitudinal and qualitative studies are recommended to track evolving perceptions of AI as technologies advance. Further exploration of patient perspectives, particularly in diagnostic and decision-support contexts, will provide a more comprehensive understanding of societal readiness.15,22–27, Strengthening interdisciplinary cooperation and policy alignment with Vision 2030 can accelerate the safe, efficient, and ethical implementation of AI in Saudi healthcare.28–30
It should be noted that this study has a number of limitations. At first the cross-sectional survey design records respondents’ opinions at one particular moment in time, which might not accurately represent how attitudes about AI change as the technology develops. Second, there were only 303 participants in the sample, and a larger percentage of females and people not in the medical field may have impacted how broadly the results may be applied. Third, participants may overestimate or underestimate their level of acceptance and awareness about AI, which could lead to bias in reported results. Lastly, other potentially significant characteristics, such as cultural background, socioeconomic level, and past exposure to AI technologies, were not evaluated because this study concentrated on fundamental demographic information. Recommendations larger and more varied populations should be included in future research to enhance generalizability and enable subgroup analysis. As AI is increasingly incorporated into healthcare systems, longitudinal research approaches are advised for following variations in awareness and acceptance.
Although many participants acknowledged potential benefits of artificial intelligence in healthcare, their acceptance of AI as a substitute for human physicians remained cautious. This apparent discrepancy may reflect the distinction between perceived usefulness and trust in autonomous medical decision-making. While individuals may recognize the efficiency and analytical power of AI systems, many still prefer human physicians due to concerns about empathy, accountability, and ethical responsibility in clinical care. Further understanding of differences in public and professional perceptions may also be established by investigating the influence of contextual and cultural factors. Lastly, building confidence and acceptance of AI in medical practice will need to address issues with privacy, accuracy, and the doctor-patient relationship.
Conclusion
This study provides insight into public perceptions of artificial intelligence in healthcare within Saudi Arabia. Although awareness of AI technologies appears relatively widespread, acceptance of AI-based medical consultation as a partial alternative to human physicians remains moderate. Concerns regarding trust, reliability, and ethical implications continue to influence public attitudes. These findings highlight the need for public education, transparent communication, and appropriate regulatory frameworks to support the responsible integration of artificial intelligence technologies into healthcare systems.
Data Sharing Statement
Data is available upon request from the correspondence author.
Acknowledgments
The authors would like to thank all participants for their valuable time and contribution to this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding for this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al Kuwaiti A, Nazer K, Al-Reedy A, et al. A review of the role of artificial intelligence in healthcare. J Personal Med. 2023;13(6):951. doi:10.3390/jpm13060951
2. Alshutayli AAM, Asiri FM, Abutaleb YBA, et al. Assessing public knowledge and acceptance of using artificial intelligence doctors as a partial alternative to human doctors in Saudi Arabia: a cross-sectional study. Cureus. 2024;16(7):e73709. doi:10.7759/cureus.64461
3. Gao S, He L, Chen Y, Li D, Lai K. Public perception of artificial intelligence in medical care: content analysis of social media. J Med Inter Res. 2020;22(7):e16649. doi:10.2196/16649
4. Khanzode KCA, Sarode RD. Advantages and disadvantages of artificial intelligence and machine learning: a literature review. Int J Library Informat Sci. 2020;9(1):30–12. doi:10.17605/OSF.IO/GV5T4
5. Martinez R. Artificial intelligence: distinguishing between types & definitions. Nevada Law J. 2019;19(3):9.
6. Pedro AR, Dias MB, Laranjo L, Cunha AS, Cordeiro JV. Artificial intelligence in medicine: a comprehensive survey of medical doctor’s perspectives in Portugal. PLoS One. 2023;18(9):e0290613. doi:10.1371/journal.pone.0290613
7. Saeed A, Bin Saeed A, AlAhmri FA. Saudi Arabia health systems: challenging and future transformations with artificial intelligence. Cureus. 2023;15(4):e37826. doi:10.7759/cureus.37826
8. Sait SM, Alnasser M, Al-Dosary A. assessing public knowledge and acceptance of using Artificial intelligence doctors as a partial alternative to human doctors in Saudi Arabia: a cross-sectional study. Front Public Health. 2021;9:32561.
9. Aljehani NM, Al Nawees FE. The current state, challenges, and future directions of artificial intelligence in healthcare in Saudi Arabia: a systematic review. Front Artif Intell. 2025;8:1518440. doi:10.3389/frai.2025.1518440
10. Alhusseini A, Alkhawajah AA, Abuageelah BM, et al. The Saudi community view of the use of artificial intelligence in healthcare. Ann African Med. 2024;23(30).
11. Alsewari R, Alneami N, Almajnoni F, et al. Perceived Worries in the Adoption of Artificial Intelligence Among Healthcare Professionals in Saudi Arabia: A Cross-Sectional Survey Study. Nurs Rep. 2024; 14(4):3706–3721. doi:10.3390/nursrep14040271
12. Alkahtani A, Alkhamis MA, Khairallah FM, Choukou MA. A survey of medical and health sciences students’ perceived AI-readiness in Saudi Arabia. BMC Med Educ. 2025;25(69).
13. Basu S, Dutta S. Artificial intelligence in healthcare: transforming patient safety with risk detection and mitigation. Front Med. 2024;11:1522554.
14. Assaf A, Chattopadhyay S. Towards secure and trusted AI in healthcare: a systematic review. Comput Biol Med. 2024;169:105003.
15. Campbell JP, Hom GL, Abramoff MD, et al. Current challenges and barriers to real-world artificial intelligence adoption for the healthcare system, provider, and the patient. Transl Vis Sci Technol. 2020;9(2):45. doi:10.1167/tvst.9.2.45
16. Hassan M, Kushniruk A, Borycki E Barriers to and facilitators of artificial intelligence adoption in health care: scoping review. JMIR Hum Factors. 2024;11:e48633. doi:10.2196/48633
17. Morone G, De Angelis L, Martino Cinnera A, et al. Artificial intelligence in clinical medicine: a state-of-the-art overview of systematic reviews with methodological recommendations for improved reporting. Front Digit Health. 2025;7:1550731. doi:10.3389/fdgth.2025
18. Li X, Zhao Y. Artificial Intelligence in primary care decision-making: survey of healthcare professionals in Saudi Arabia. Cureus. 2025;17(5):e361066.
19. Ayorinde A, Mensah DO, Walsh J, et al. Health care professionals’ experience of using AI: systematic review. J Med Internet Res. 2024;26:e55766.
20. Simoni J, Urtubia-Fernandez J, Mengual E, et al. Artificial intelligence in undergraduate medical education: an updated scoping review. BMC Med Educ. 2025;25(1):1609. doi:10.1186/s12909-025-08188-2
21. Chustecki M. Benefits and risks of AI in health care: narrative review. Interact J Med Res. 2024;13(1): e53616. doi:10.2196/53616
22. Radhakrishnan P, Chattopadhyay S. Artificial intelligence and decision-making in healthcare: a thematic review. JMIR AI. 2023;4(2):e53207.
23. Ruksakulpiwat S, Thorngthip S, Niyomyart A, et al. A systematic review of the application of artificial intelligence in nursing care: Where are we, and what’s next?. J Multidiscip Health. 2024;17:1603-1616. doi:10.2147/JMDH.S459946
24. Syed W, Babelghaith SD, Al-Arifi MN. Assessment of Saudi public perceptions and opinions towards artificial intelligence in healthcare. J Fam Community Med. 2024;31(3):155–163.
25. Eldesoky HA, AlThubaity D, Shalby AY, Mohammed FA Solicitude toward artificial intelligence among health care providers and its relation to their patient’s safety culture in Saudi Arabia. BMC HealthClass. 2025;25(1):889. doi:10.1186/s12913-025-13001-3
26. Watson H, Lee M. A systematic literature review of artificial intelligence in healthcare: applications, challenges, and ethical implications. Healthc Technol Lett. 2025;2(1):101–120.
27. Poon EG, Lemak CH, Rojas JC, Guptill J, Classen D. Adoption of artificial intelligence in healthcare: survey of health system priorities, successes, and challenges. J Am Med Inf Assoc. 2025;32(7):1093–1100. doi:10.1093/jamia/ocaf065
28. Khan MU. Saudi Arabia’s vision 2030. Def J. 2016;19:36.
29. Saudi Vision 2030. Available from: https://www.vision2030.gov.sa/en/.
30. Nurunnabi M. Transformation from an oil-based economy to a knowledge-based economy in Saudi Arabia: the direction of Saudi vision 2030. J. Knowl. Econ. 2017;8:536–564. doi:10.1007/s13132-017-0479-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Promise and Provisos of Artificial Intelligence and Machine Learning in Healthcare
Bhardwaj A
Journal of Healthcare Leadership 2022, 14:113-118
Published Date: 20 July 2022
Undergraduate Medical Students’ and Interns’ Knowledge and Perception of Artificial Intelligence in Medicine

Jha N, Shankar PR, Al-Betar MA, Mukhia R, Hada K, Palaian S
Advances in Medical Education and Practice 2022, 13:927-937
Published Date: 23 August 2022
Impact of AI-Powered Solutions in Rehabilitation Process: Recent Improvements and Future Trends
Khalid U, Naeem M, Stasolla F, Syed MH, Abbas M, Coronato A
International Journal of General Medicine 2024, 17:943-969
Published Date: 12 March 2024
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Serbaya SH, Khan AA, Surbaya SH, Alzahrani SM
Advances in Medical Education and Practice 2024, 15:269-280
Published Date: 5 April 2024
Challenges of Healthcare Systems in Saudi Arabia to Delivering Vision 2030: An Empirical Study From Healthcare Workers Perspectives
Al-Anezi FM
Journal of Healthcare Leadership 2025, 17:173-187
Published Date: 7 May 2025