Back to Journals » International Journal of General Medicine » Volume 17
Impact of AI-Powered Solutions in Rehabilitation Process: Recent Improvements and Future Trends
Authors Khalid U ![]() , Naeem M
, Naeem M ![]() , Stasolla F
, Stasolla F ![]() , Syed MH, Abbas M, Coronato A
, Syed MH, Abbas M, Coronato A
Received 15 December 2023
Accepted for publication 5 March 2024
Published 12 March 2024 Volume 2024:17 Pages 943—969
DOI https://doi.org/10.2147/IJGM.S453903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Vinay Kumar
Umamah bint Khalid,1 Muddasar Naeem,2 Fabrizio Stasolla,2 Madiha Haider Syed,1,3 Musarat Abbas,1 Antonio Coronato2
1Department of Electronics, Quaid-I-Azam University, Islamabad, 44000, Pakistan; 2Research Center on ICT Technologies for Healthcare and Wellbeing, Università Telematica “Giustino Fortunato”, Benevento, 82100, Italy; 3Institute of Information Technology, Quaid-i-Azam University, Islamabad, 44000, Pakistan
Correspondence: Muddasar Naeem, Email [email protected]
Abstract: Rehabilitation is an important and necessary part of local and global healthcare services along with treatment and palliative care, prevention of disease, and promotion of good health. The rehabilitation process helps older and young adults even children to become as independent as possible in activities of daily life and enables participation in useful living activities, recreation, work, and education. The technology of Artificial Intelligence (AI) has evolved significantly in recent years. Many activities related to rehabilitation have been getting benefits from using AI techniques. The objective of this review study is to explore the advantages of AI for rehabilitation and how AI is impacting the rehabilitation process. This study aims at the most critical aspects of the rehabilitation process that could potentially take advantage of AI techniques including personalized rehabilitation apps, rehabilitation through assistance, rehabilitation for neurological disorders, rehabilitation for developmental disorders, virtual reality rehabilitation, rehabilitation of neurodegenerative diseases and Telerehabilitation of Cardiovascular. We presented a survey on the newest empirical studies available in the literature including the AI-based technology helpful in the Rehabilitation process. The novelty feature included but was not limited to an overview of the technological solutions useful in rehabilitation. Seven different categories were identified. Illustrative examples of practical applications were detailed. Implications of the findings for both research and practice were critically discussed. Most of the AI applications in these rehabilitation types are in their infancy and continue to grow while exploring new opportunities. Therefore, we investigate the role of AI technology in rehabilitation processes. In addition, we do statistical analysis of the selected studies to highlight the significance of this review work. In the end, we also present a discussion on some challenges, and future research directions.
Keywords: artificial intelligence, machine learning, rehabilitation, healthcare, cognitive skills, cognitive rehabilitation
Introduction
Cognitive decline is associated with loss of cognitive skills, and it is common with aging but it gets worse if it is caused by some medical conditions like neurocognitive disorder or neurodegenerative disorder. With the loss of cognitive skills like reasoning, thinking, executive functioning, attention, memory, and other abilities, an individual may face difficulty in the activities of daily life. The lack of necessary treatment for individuals with mental health issues is a significant concern. Therefore, an appropriate care and rehabilitation facilities are important for people having cognitive impairments.1
Cognitive Rehabilitation Therapy (CRT) is a cognitive activity that helps people with cognitive decline to reestablish their previous cognitive skills or helps in learning new cognitive skills.2 Rehabilitation is of two types, Restorative and Compensatory rehabilitation. It is a non-pharmacological method of treatment as it uses problem-solving techniques to help people with cognitive decline sustain their daily life activities.2 In addition, the implementation of cognitive training may be employed to enhance cognitive abilities in individuals with no impairments.3 It can also be utilized to augment academic achievement in students or bolster cognitive reserve in older persons.
Digital technologies in healthcare, including AI in mental health, have indeed revolutionized the field by offering a wide range of applications.4 Machine learning has made significant advancements in the field of healthcare and specifically, reinforcement learning has made treatment interventions personalized.5 The applications of AI in mental health extend beyond diagnosis and drug recommendation.6 Virtual therapy sessions using AI chatbots or virtual reality platforms have shown promising results in providing accessible support thus, offering a safe environment for patients to express their thoughts and emotions, facilitating effective therapy without geographical barriers.7 One of the primary advantages of technology-based interventions is their enhanced accessibility.8 Unlike traditional methods, these technology-based interventions are often cost-effective and can be easily accessed by individuals from the comfort of their own homes.9,10
A wide range of CRT interventions for mild cognitive impairment (MCI) or neurocognitive disorders can be implemented through smartphone apps, web-based applications, or gaming consoles without acquiring expensive equipment9 as shown in Figure 1. Such interventions can be made adaptive by using a reinforcement learning agent that interacts with the trainee during each exercise/task. Based on the performance of the trainee, a tailored policy is pursued making training interventions personalized and adaptive. Such personalization of treatment will maximize the effectiveness of cognitive training programs.11
 |
Figure 1 AI-based adaptive cognitive rehabilitation therapy (CRT) interventions. |
Recent technological advancements have made it possible for therapists to conduct traditional interventions via social robots, eliminating the need for traditional paper-and-pencil methods.12 With a heterogeneity in it, social robots include humanoid robots like MATILDA, MERO, NAO, PEPPER, SILBOT, SOPHIE etc13,14 and zoomorphic robots like AIBO and PARO.15 Although using humanoid robots as a mediating tool has shown potential in engaging participants in memory training programs12 yet to gain a better understanding of the training components and robot responsiveness, additional studies are required.
Along with these merits of technology-based CRT, some challenges need to be addressed. The most significant challenge among all is the adoption of rehabilitation techniques and the factors influencing adoption include cost, trust in technology, and access.16 Others include less education, lack of awareness, improper training, and unavailability of user-friendly interface.17 However, it is essential to note that AI should never replace human expertise in healthcare. Instead, it should be seen as a valuable tool that complements the skills of healthcare professionals. The combination of human judgment and AI-driven insights can improve diagnoses, personalized treatment plans, and patient care overall.
This study aims at the most critical aspects of the Rehabilitation process that have benefited from the use of AI, including Personalized Rehabilitation Apps, Rehabilitation through Assistance, Rehabilitation for Neurological Disorders, Rehabilitation for Developmental Disorders, Virtual Reality Rehabilitation, and Rehabilitation of Neurodegenerative Diseases. The primary focus of this survey is to identify personalized and adaptive AI-based interventions for individuals with cognitive impairments. It includes interventions for neurodevelopmental disorders (ie Autism spectrum disorder (ASD), Attention deficit hyperactivity disorder (ADHD), learning disorder), neurocognitive disorders (i.e, stress, anxiety and depression, brain stroke, etc), and neurodegenerative disorders (i.e, dementia, Alzheimer’s disease (AD), Parkinson’s disease, etc).
I. RELATED SURVEYS AND SELECTION PROCESS This section consists of two parts, where the first subsection highlights some recent survey papers related to AI technology or the rehabilitation process. We review the main contributions of each article as well as limitations concerning the scope of our contribution. The second subsection presents the survey studies’ selection criteria, including the search strategy, inclusion criteria, and data synthesis.
Related Surveys
It is important to have effective treatments for all diseases including neurodegenerative diseases. Therefore, the review work in18 highlights the Machine Learning (ML) applications for early diagnosis, discovery of new therapies, and interpretation of medical images. They discussed how high-dimensional sources of data are utilized in various ML applications for neurodegenerative diseases. However, the article fails to cover diverse rehabilitation processes based on AI methods. Similarly, the review work in19 presents diverse types of personalized robot behavior patterns. Different schemes from the area of child–robot interaction and human-robot interaction are discussed. The authors compare them using their deficits, potential usability, and feasibility for autism-specific robot-assisted therapy. During therapeutic games, one limitation on the methods used by robot to learn interaction strategies is to give more autonomy to robot and it is linked with a robot’s decision-making. The article does not address the potential uses of AI and ML in various rehabilitation processes.
Considerable work done in20 where authors consider older patients with dementia and mild cognitive impairments and identified rehabilitation plans as well as cognitive stimulation and training. The authors provided a qualitative synthesis of the study characteristics and features of every software. The studies found on cognitive intervention software highlight that several technological plans are available for people with MCI and dementia. This study does not provide comprehensive information about the AI-based rehabilitation process but can be used to distinguish between programs if they have different characteristics, usage modes, and objectives. The review work of21 highlights developments and issues in human–robot interaction perspective assistive robotics and rehabilitation. The authors also identify various subdomains in rehabilitation and assistive robotic research.
A significant work reported in4 where authors have presented reinforcement learning based diverse healthcare applications including precision medicine, control systems, personalized rehabilitation, dynamic treatment regimes, diagnostic systems, healthcare management systems, medical imaging, and dialog systems. Although this survey article covers many intelligent healthcare applications, it presents a few RL-based applications in personalized rehabilitation. Recently wearable technology proved useful in rehabilitation, assessment, diagnosis, and monitoring.22 Therefore, the applications of review wearables by Parkinson’s disease patients as well as patients with neurocognitive disorder are discussed in.22 However, regarding the rehabilitation process, this study only considers existing wearable insoles and their use in rehabilitation.
We summarize about mentioned relevant studies, their limitations with respect to the scope of our work and our contributions in Table 1. The contribution of this article is to analyze the impact of AI-enabled solutions in various Rehabilitation processes including Personalized Rehabilitation Apps, Rehabilitation through Assistance, Rehabilitation for Neurological Disorders, Rehabilitation for Developmental Disorders, Virtual Reality Rehabilitation, and Rehabilitation of Neurodegenerative Diseases.
 |
Table 1 A Brief Comparison of Related Surveys in Terms of Contributions and Limitations |
Selection Process
The standard guidelines that have been adopted in this review work are that of the PRISMA statement23 as shown in Figure 2. For example, first, we employed a combination of keywords and research queries such as rehabilitation, artificial intelligence, adaptive cognitive rehabilitation, personalized rehabilitation, cognitive rehabilitation for MCI, computerized cognitive training with reinforcement learning, rehabilitation for neurocognitive and neurodegenerative disorder, etc as also indicated in Figure 2. In the next step, we utilized popular search database sources, including IEEEXplore, SpringerLink, ScienceDirect, Google Scholar, Nature, and ACM Digital Library. Our priority is on the studies published after review process in journals, book chapters, and conferences. We gave preference to top-ranked journal studies, and our review contains about 90% journal papers. It was challenging to include all different sorts of deficits because cognitive rehabilitation (CR) includes a wide range of mental illnesses. Rehabilitation for brain tumors, brain injuries, drug addiction, epilepsy, and stress/anxiety induced by other diseases, like, HIV or cancer, are not included in this study.
 |
Figure 2 Steps involved in the present survey. |
Following the PRISMA guidelines, we collected about 300 studies, but some of them were removed due to duplication and our criteria for inclusion as shown in Figure 3. However, some articles were removed that do not match the following eligibility criteria:
- Published from 2020 to 2023.
- Relevance of the AI-based method in any aspect of a rehabilitation process.
- Full-text availability.
- Academic empirical and theoretical studies.
- Peer-reviewed studies.
- English language.
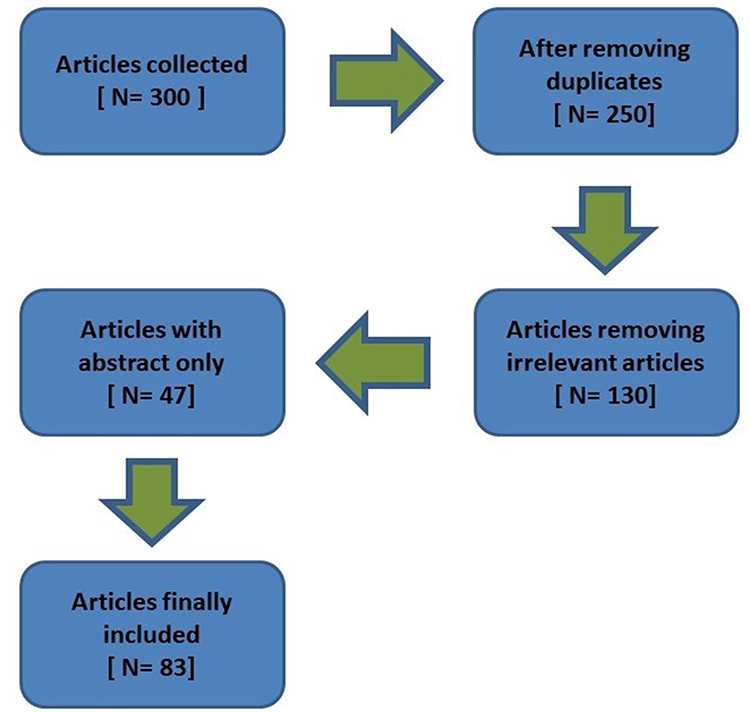 |
Figure 3 Articles selection process following PRISMA. |
Background
Preliminary to Rehabilitation
This subsection presents a brief introduction to rehabilitation, in particular to cognitive rehabilitation. The last part of this section outlines the reasoning behind the six chosen categories for this review work.
Neurological Populations (eg, neurodevelopmental disorders, neurodegenerative diseases, stroke, disorders of consciousness, rare genetic syndromes) may experience daily difficulties while dealing with environmental requests. Intellectual disabilities, extensive motor impairments, sensorial deficits, and communication delays (eg, lack of speech) may be included. Their clinical conditions rely on persons with acquired brain injuries on both families and/or caregivers’ assistance.24,25 This situation may be seriously deleterious for their quality of life and their social image, status, and desirability may be significantly hampered.26,27 To tackle this issue, assistive technology, new technologies, and artificial intelligence-based programs or interventions may be envisaged.28–30 Assistive technology-aided treatments include any piece, device, tool, or equipment capable of ensuring individuals suffering from neurological consequences with self-determination and independence towards their environment. Thus, a functional bridge between the behavioral repertoire and the environmental requests may be built.11 New technologies (ie, virtual and augmented, reality, mixed and extended reality, serious games) may provide immersive scenarios similar to real life, pursuing assessment, educational, and rehabilitative purposes.31,32 AI with Reinforcement Learning (RL) as branch of ML may represent an interactive way to support users with individualized solutions by learning and being reinforced by their performance.33,34 The above-detailed technology-based solutions may be implemented in daily and clinical settings for diagnostic and functional recovery objectives and may be considered complementary to standard cognitive rehabilitation. Both may contribute to an accurate and valid help to support the neurological population.35,36
Cognitive Rehabilitation (CR) usually refers to systematic and specific cognitive therapy aimed at enabling personal functional modifications through (a) restoring or enhancing already acquired patterns of behavior, or (b) teaching or improving new patterns of cognitive activity and compensatory processes for impaired neurological systems.37 Accordingly, CR commonly defines either restorative or compensatory strategies. Restorative schemes are developed on the principles of learning and exercise. The repetitive exercise of neural connectivity assisting cognitive function improves the learning process of novel skills which can restore the damage. Restorative strategies are based on neuronal plasticity. Hence, the intact or non-impaired neurons and neural circuits will replace lost functions. On the other hand, compensative approaches imply the replacement of the neural pathways previously needed to obtain a certain activity. By substituting functional mechanisms, modalities are acquired to get particular objectives. Both strategies may be combined in a rehabilitative program due to the fact that simulation of cognitive processes during compensatory training can improve and support neural connectivity.38,39
CR may be delivered via conventional approaches as well as through computerized solutions mediated by the use of Information and Communication Technologies (ICT).40 Computer-mediated interventions overcome some limitations of conventional strategies. For instance, human resources, time and cost can be handled by using computerized systems. Response time, stimuli delivery and task difficulty can change regularly and can be adjusted to the participant’s features and performance.41,42
We identified seven main categories. Four categories are named after treatment interventions while the rest after mental illness/disorder. There is a broad spectrum of further impairments that come under the umbrella of neurodegenerative diseases, neurodevelopmental disorders, and neurocognitive disorders. The first category labelled Personalized Rehabilitation Apps includes some illustrative examples of highly customized and tailored solutions in which adapted apps and software were used to support CR in neurological populations with different targeted behaviors and technological options implemented. The second category labelled Rehabilitation through Assistance emphasizes the importance of physical robots or technology-aided programs to support individuals with severe to profound neurological impairments involved in the management and the achievement of daily activities. The third category, labelled Rehabilitation for Neurological Disorders, provides the reader with an overview of cognitive-behavioral therapy focused on helping persons with neurological diseases like depression, anxiety and other mental illness in daily independent functioning.
The fourth category labelled Rehabilitation for Developmental Disorders, is centered on children and adolescents with neurodevelopmental delays. Different technology-based programs were detailed that highlight different ways of helping children to survive independently. The fifth category, labelled Virtual Reality-based Rehabilitation, refers to new technologies. Thus, virtual reality setups may involve users in immersive situations similar to real life enabling participants, clinicians, and researchers with high ecological validity, behavioral tracking, and experimental control. The sixth category, labelled Rehabilitation for Neurodegenerative Diseases, is specifically targeted at technological interventions in individuals with either cognitive or motor extensive impairments. The last category labelled Telerehabilitation for cardiovascular and other diseases is targeted to highlight the role of telerehabilitation for various diseases. It not only encompasses evaluation and monitoring, but also intervention, supervision, education, consultation, and coaching. The idea was to provide readers with a comprehensive although not exhaustive picture of AI and technological- aided treatments in neurological disorders.
Preliminary to Artificial Intelligence
Artificial Intelligence (AI) refers to the creation of a computer system (machine) capable of performing tasks that require human intelligence (smarter than humans) like reasoning, perception, problem-solving, language processing, etc. AI has changed our way of living and it has revolutionized technology through its ability to support, enhance, empower, and inspire humans practically. Artificial Intelligence is a computational approach that enables computers to learn from data and find approximations for difficult problems. AI has been extensively used in large-scale fields including robotics, airline flight control, and healthcare because of its flexibility and robustness. In Psychology, learning is an experience-based process that results in a change in behavior or understanding for better performance.43 The scientific study of algorithms and statistical models applied to computer systems performing particular tasks is known as Machine Learning (ML) and is acknowledged as a domain of AI. The field involves the autonomous construction of mathematical models by ML algorithms using sample data, or training data, to make predictions or judgments without being primarily programmed to do the task.44 ML encompasses a wide-ranging field that incorporates diverse paradigms, including supervised, unsupervised, online, batch, meta-learning, and reinforcement learning. Its applications span across various domains, such as medicine, computer vision, agriculture, email filtering, and speech recognition.11 Among all types of ML, reinforcement learning (RL) is an AI-based adaptive method used to train and improve systems by interacting with their environments.45 RL makes decisions and adapts its behavior based on the feedback signal and is often used to solve complex problems.46
Deep learning (DL) is the fastest-growing field of data science and is built on artificial neural networks to tackle unstructured data including image and video processing, text, voice, etc. The field has been in account since the 1980s but it reached its full potential during the last few years.47 Neural networks used by DL are trained end-to-end to make the challenges easier to solve, but sometimes, such techniques are not considered user-friendly due to their steep learning curves.48 Additionally, several domain-specific restrictions are hindering the widespread adoption of deep learning in various industries.
Impact of Ai in Rehabilitation Process
This is the main section of this study where we analyze the diverse applications of AI-powered techniques in Rehabilitation process as indicated in Figure 4. Moreover, we have summarized a few studies from each category in Table 2.
 |
Table 2 Summary of Different Studies to Highlight Their Objective, AI Technology and Methodology |
 |
Figure 4 Layout of the Section IV. |
Personalized Rehabilitation Apps
Adaptive rehabilitation is tailored according to the requirements and impairment level of an individual, most of the rehabilitation interventions come in the form of web applications smartphone applications, or a combination of both. This section contains studies with treatment intervention in the form web/smartphone app for different kinds of impairments.
The study in49 describes a custom Android application designed for dementia patients that uses games and activities to improve cognitive function. The application is designed to target four cognitive domains of dementia: concentration and attention, executive functioning, language improvement, and memory. Each participant practiced the game for a month, with and without reinforcement learning (RL), and the results showed that training with RL produced better outcomes. The study of50 aimed to rehabilitate Multiple Sclerosis (MS) patients with mild cognitive impairments using a personalized adaptive system. The system combined a computerized cognitive training program with an RL agent. The study had two phases, and the performance of trainees was measured with the Paced Auditory Serial Addition Test (PASAT) before and after the training. The results showed that trainees who trained with RL showed better results than those who trained without RL. MCI can lead to dementia, specifically Alzheimer’s disease, as cognitive decline progresses.
In,51 authors proposed an RL framework by using recorded conversations of normal and MCI individuals with expert interviewers and fed them in a supervised learning model that distinguishes between normal individuals and MCI patients. The agent was trained for disease-specific lexical probability distributions which engage the agent and individual in conversations for diagnosis accuracy with less number of dialogue turns. The clinical trials of the proposed framework prove its effectiveness and it outperformed prevailing supervised learning methodologies significantly.
The investigation of the study68 suggests that computer-assisted cognitive behavior therapy has the potential for wider-spread implementation as an efficient, acceptable, and effective treatment for depression in primary care. The authors have performed randomized clinical trials and they suggest this with a modest amount of clinician support. The method is more beneficial for patients with depression in primary care, who have a lack of internet access, and low levels of education, income, and reading proficiency. Smartphone-assisted interventions could be efficacious in treating a few forms of generalized anxiety disorder. Therefore, smartphone-based trials were done on college students in.69 The students with self-reported generalized anxiety disorder were randomized to receive guided self-help from a smartphone or no treatment. Post-treatment after a six-month follow-up outcome contains the state-trait anxiety inventory-trait, the Penn State worry questionnaire, and the depression anxiety stress scales-short form stress subscale.
The authors of52 have designed a mobile application for children with Autism Spectrum Disorder (ASD). Focusing on simple icons and letters with a maximum of three colors, the aim was to develop a mobile application that can fulfill the special needs of children with ASD not only in schools and therapeutic sites but also at home. Assistive technology applications, such as mobile apps, can enhance social and language skills in young children with ASD, benefiting both parents and children. In,53 an app is developed to specifically improve numeracy skills in children with ASD. Many apps are already available for teaching numeracy skills to children but this app is developed in a user-friendly way by keeping focus on icon size, display, graphics, soft touch, background sound, etc to grab the attention of children with ASD.
In,70 a cognitive rehabilitation program is being discussed to help children with ADHD through the use of games and Unity3D technology. UNITY3D is a game engine capable of creating web-based applications that can be integrated into both computers and mobile phones, comprising four functional modules, with the cognitive training module being the core component. The training module employs targeted games to help children overcome their illness, improve their ability to integrate into society, and contribute to their overall treatment. Cognitive incapacity, characterized by cognitive and physical impairment, requires rehabilitation interventions. The study of71 introduces Brain m-App, developed for home-based cognitive rehabilitation of incapacities. It focuses on improving executive functions, attention, and spatial memory. Brain m-App consists of a 10-day program that uses virtual reality along with 360-degree videos, making it well-suited for home-based rehabilitation. Based on a small clinical study, Brain m-App was found to have improved executive functions and memory performances.
The study in72 aimed to design and analyze the feasibility of an interactive physical-cognitive game-based training system for older adults. The first phase consists of exercise prototypes while the second phase involves different cognitive games. Participants rated their enjoyment level and provided positive feedback on the well-designed interactions and interfaces. Physical-cognitive game-based and interactive exercise program for older adults shows promise for fall risk reduction, but effectiveness needs further examination. The work of73 compares Serious Games (SG) with traditional methods (TM) for cognitive rehabilitation (CR) in healthcare. SG is considered a useful tool to connect healthcare specialists with patients and track their rehabilitation progress. The study includes a literature review, conceptual research, and a model to assess the impact of SG on CR. Specific SG applications like CogniFit, KiMentia, and Sea Hero Quest are mentioned, which focus on cognitive areas like attention, memory, coordination, and reasoning. SG is found to be superior to TM in enhancing training and generating high-quality data for analysis in a secure environment.
The objective of the study in74 is to implement the GREAT Cognitive Rehabilitation intervention for individuals having mild to moderate dementia. The strategy used to implement the intervention involved identifying and supporting leadership, conducting collaborative planning, training, and assisting practitioners. The outcome evaluation indicated that the intervention was received positively by the local steering group members, practitioners, and service users. People with dementia, their caregivers, and practitioners gave positive feedback about the intervention. The study75 aimed to evaluate the usability of a stepping exergame among older adults with the major neurocognitive disorder (MNCD) living in long-term care facilities. The study used a mixed-methods approach, where participants played the exergames and provided feedback using the think-aloud method, field notes, and interviews. The study included 22 participants with MNCD and found that the stepping exergame was user-friendly and suitable for older adults with MNCD.
The authors of76 aimed to assess the effectiveness of a cognitive training app named MeMo, designed to improve behavioral and cognitive performance in people with neurocognitive disorders. The study concluded that MeMo was effective in enhancing behavioral and cognitive performance in individuals with neurocognitive disorders if used regularly. The purpose of the study in77 is to evaluate the effectiveness of the self-administered mobile cognitive training intervention called “NeuroNation MED” in individuals with Mild Cognitive Impairment. The study will provide insights into the effectiveness of mobile training on cognitive endpoints, neuropsychiatric symptoms, usability, and participant engagement.
Rehabilitation Through Assistance
Patients with down syndrome, brain stroke, and severe dementia are unable to perform their activities of daily living (ADL) on their own. Hiring a professional caregiver to assist such individuals costs a lot. Hence, to make such individuals being able to perform their daily activities rehabilitation can be done by assistance, ie, robot assistance, AI-based dialogue therapists/simulators, etc.
In,78 the authors developed an assistive system to help Alzheimer’s patients perform daily tasks such as drinking a beverage. The system extracts the position of the patient’s body joints, and the patient’s exact position during an activity. The RL agent analyzes all activities and generates an alert in case of an anomaly. The system’s real-time effectiveness was evaluated using precision and recall metrics, proving it to be the most suitable system for assisting Alzheimer’s patients in performing daily activities. In,54 the authors proposed a support system for the support of Alzheimer’s disease patients to help patients perform their tasks on their own. This assistive system consists of human activity recognition (HAR) systems, one with 2D skeleton data and a second with 3D skeleton data followed by CNN and transformers. The work concludes by comparing the proposed system’s performance to determine the most suitable assistive system among all.
In another study,55 an AI food assistance for AD patients is considered. Alzheimer’s patients are at high risk of dehydration, malnutrition, or overeating due to memory loss. This system assists the patient’s activities through video, monitors their timing of eating and drinking, and generates audio messages to stop them from overeating or to remind them to take their meal. The results proved the efficiency of application hence reducing the need for professional caregivers for patients. In,56 an assistive robot named LOLA2 has been developed, for the assistance of people with neurodevelopment disorders. The robot LOLA2 monitors real-time actions of a patient by monitoring the time and action of activity. The results obtained were acceptable enough to conclude that LOLA2 can perform as an assistant for neurodevelopmental disorders people.
The development of the M3Rob rehabilitation platform that integrates haptic robotics, neurofeedback, and augmented reality to aid in stroke rehabilitation is performed in.79 The M3Rob platform leverages electromyography (EMG) and electroencephalography (EEG) signals to identify the intent of hand and wrist movements, enabling personalized assistive therapies for neuromotor and cognitive rehabilitation. The research in80 develops an ontology-based cognitive assistance framework for ambient assisted living (AAL) systems, providing adaptive dialogue and assistance to individuals with cognitive impairments. The model uses the speech acts theory for translating cognitive assistance into adaptive assistive messages. The model’s usability and applicability are demonstrated via a real-life scenario, showcasing its effectiveness in providing graded guidance messages.
The authors in81 examine the outcomes of rehabilitation using gait robot-assisted training in stroke patients with hemiplegia. The experimental group received stroke rehabilitation using gait robot-assisted training while the control group received conventional rehabilitation. The gait robot-assisted rehabilitation with goal setting improved stroke self-efficacy, balance ability, gait ability, and health-related quality of life in patients.
Rehabilitation for Neurological Disorders
Neurological disorder includes a wide range of disorders like brain tumor, head injury, epilepsy, syndrome disorder, etc. This section refers to the studies related to the rehabilitation of serious mental illness, vascular disorders, and depression/anxiety.
The methodology developed in57 aims to improve CBT, especially for the treatment of depression by revealing the pattern of the brain under depression and by suggesting new ways to help people with depression through thinking and learning. It is a cross-sectional cohort study that reveals that understanding the association of RL with brain regions of people without depression can help improve CBT and also help clinicians treat people with depression. A study is presented in82 to investigate the differences in RL parameters between patients with anxiety or depression and control individuals. Authors have also performed a novel simulation meta-analysis in parallel with the conventional meta-analysis. A sequence of random-effects meta-analyses are performed after the extraction of individual-level parameters to examine whether any of the most commonly reported parameters showed differences between control individuals and patients.
A recent study83 considers the efficacy of Computerised Cognitive Training (CCT) on functional, psychosocial, mode, and cognitive outcomes and daily functioning in adults with depression. The authors investigated this in comparison with passive or active control. Moreover, the authors have examined the intervention design factors that may moderate CCT effects across each domain study. The quality and strength of the evidence for CCT in depression are also evaluated. The study84 aimed to enhance functional outcomes in people having serious mental illness. Modern ICTs, like mobile apps, provide solutions for patients experiencing serious mental illness to improve functional outcomes. The program provides psychiatric rehabilitation to help patients improve their social and cognitive disabilities.
The work of60 considers the cortical Striatal pathway for two common neurodevelopmental disorders. Differentiation between corticostriatal dysfunction in learning and attentional disorder has been studied through RL approaches by observing the cognitive processes involved. The whole study is observed in males only but the findings suggest the difference in patterns of learning disorder and attentional disorder for model-based RL and model-free RL. The efficacy of a computer-aided cognitive training program is investigated in85 on depressive symptoms, behavioral symptoms, and cognitive measures in patients having major vascular neurocognitive disorder. The subjects were divided into a control and a treatment group, and all of them received a neuropsychiatric inventory, the Aasberg depression rating scale, the Montgomery, and the mini-mental state examination.
A review study86 highlights ML approaches in post-stroke rehabilitation for functional recovery prediction and prognosis. Five electronic databases were investigated during the study. They extracted the validation approach, the algorithm used, the scheme for feature extraction and selection, outcome assessed, population characteristics, and health conditions. The research58 is a telerehabilitation program for neurocognitive disorder patients. The research is a controlled trial that compares the Core and HomeCore programs, one for hospital trials and the second for distance treatment. The program provides a wide range of cognitive exercises like exercises for episodic long-term memory, executive functioning, working memory, attention, and processing speed.
A review of the applications of LEAP motion for various psychological domains, in particular, implementation and basis for interventions in neurocognitive and neurodevelopmental disorders are given in.87 The survey work discussed studies on autism spectrum disorder and attention-deficit hyperactivity disorder as examples of neurodevelopmental disorders, and MCI, and dementia as examples of neurocognitive disorders. The study in88 discusses the importance of cognitive rehabilitation in individuals with type 2 diabetes. It evaluates the effectiveness of a program called Memory, Attention, and Problem-Solving Skills for Persons with Diabetes (MAPSS-DM) and aims to explore how it enhances cognitive functioning and diabetes management. The findings suggest that the intervention group showed improvement in memory and executive functioning with better diabetes self-management. The review work in89 found that cognitive rehabilitation programs using cognitive training, compensatory strategies, or a combination of both can improve cognitive function for breast cancer survivors with chemotherapy-related cognitive impairment. However, a clear recommendation could not be established due to methodological concerns and varied program parameters. The research done in90 focuses on improving cognitive rehabilitation for individuals with speech disorders through the use of machine learning. By combining the machine learning approach with data collected from the EEG and Kinect sensor, the model has achieved promising results for real-time scenarios and improved the overall quality of life.
The work in91 analyzes the relationship between delirium, physical exercise, and rehabilitation. There is a strong connection between delirium and physical functioning. Delirium affects cognitive and motor functions, so the motor component of delirium should also be considered when designing inter- ventions or strategies. In,92 a digital intervention was tested in adult patients with major depressive disorder and cognitive impairment. Improvement in sustained attention was observed with AKL-T03 compared to the control intervention. Further research is needed to understand the clinical consequences and impact of AKL-T03.
The study in93 aims to investigate the effectiveness of a new exergame-based motor-cognitive training called “Brain-IT” in enhancing cognitive functioning in older adults with the mild neurocognitive disorder (mNCD). The main measure of outcome is overall cognitive functioning, with additional measurements like brain structure and function, gait parameters, and daily activities.
Rehabilitation for Developmental Disorders
Developmental disorder refers to the incomplete development of a child’s behavior, mind, and language. A lot of disorders like autism spectrum disorder, and all kinds of learning disorder comes under developmental disorder. The successful treatment intervention is therapy (both cognitive and behavioral), the earlier it begins, the sooner the child will become independent. This section contains different AI-based treatment interventions for children with developmental disorders.
Neurodevelopmental disorder interventions are better treated with single-case experimental designs (SCEDs). In59 following SCED, two children one with autism spectrum disorder and the second with agenesis of Corpus Callosum have been studied using BEHAVE application for manding repertoire. BEHAVE application proves its effectiveness as a tool in collecting and analyzing data, and also in evaluating the frequency of independent minds performed by case studies. Intellectual development disability (IDD) affects cognitive functioning as well as causes learning and social impairment in children. In,62 the authors investigate the effects of CCT on intellectual and adaptive functioning in developmentally disordered children. The study investigates the effects of CCT in 4 cognitive domains ie learning, reasoning, working memory, and visual perception. The results imply that CCT raised the kids’ IQs by enhancing both their intellectual and adaptive functioning.
Dyslexia is another developmental disorder that limits the learning abilities of children63 proposes an adaptive framework (RALF) for helping children with dyslexia. RALF is designed to generate short- and long-term content for training students incorporating the Cellular Learning Automata (CLA) structure. Experimental application of RALF and its comparison with a control group indicated no significant overall achievement, but as a part, the reading abilities of dyslexic students improved by using this framework.
The authors in94 employed a randomized controlled model to perform a comparison of the training outcomes between remotely delivered neurofeedback, Computerized Cognitive Training (CCT), and combined neurofeedback/CCT training schemes. They randomly assigned 121 children with attention-deficit/hyperactivity disorder to the above three groups. The authors observed a significant improvement in the life skills, learning, working memory, inhibition, and the inattentive and hyperactive/impulsive symptoms of the 3 groups of children after three months of training. Moreover, the authors verified the training effects of neurofeedback, CCT, and combined neurofeedback/CCT training in children with attention- deficit/hyperactivity disorder. Children with autism spectrum disorder face learning difficulties along with memory issues. In,61 the authors have introduced an intelligent tutoring system namely RELETAS, to help children with ASD to fight learning disorders by using RL. RELETAS is based upon ANN and RL and is designed to enhance the working memory of the children along with Zone of Proximal Distribution (ZPD), although the evaluation is done only in a single concept and the RL agent achieved a reward by answering 1000 correct answers out of 10,000 questions. The study in95 was to evaluate how the cognitive enhancement training (COGENT) program impacted the reading and writing abilities of students with specific learning disabilities (SLD). The results showed that the COGENT program had a positive effect on reading speed, reading comprehension, and dictation skills among the treatment-group but no considerable difference in text copying. Feedback from teachers revealed that they observed improvements in the literacy skills of students as well as some social skills.
An evaluation on the effectiveness of telerehabilitation for learning disabilities in adolescents during the COVID-19 lockdown is done in.96 Twenty-four adolescents received cognitive treatment via a telehealth app for four weeks, leading to significant improvement in cognitive domains such as attention, memory, and information processing speed. Telerehabilitation can improve cognitive functioning in patients with learning disabilities and promote healthcare at home. This study97 tested the usability of telerehabilitation on reading and writing in children with Specific Learning Disabilities (SLD). Results indicate notable improvements in executive functions, text dictation, and reading fluency in the telerehabilitation group. Children participating in a combined training program showed improvements in word reading fluency and text dictation. These findings have important implications for clinical research and practice in the field of telerehabilitation for children with SLD.
Virtual Reality-Based Rehabilitation
This section focuses on showcasing a wide range of virtual reality (VR) therapies, intended to improve the cognitive performance of older persons. The therapeutic applications of VR are wider than anything as it provides personalized interventions, simulates real-life events, improves attention and concentration, provides exergaming at home, and much more. The human empowerment aging and disability VR protocol is explored in98 and found suitable in clinical and at-home telerehabilitation for patients in the chronic stage after stroke. The method is helpful in the continuity of care as it is effective at home in long-term maintenance and augmenting motor and cognitive abilities in the clinic. An immersive on-body feedback system using an iterative user-centered design process is developed in67 to conserve the advantages of the physically immersive setup of the ExerCube to be used at the home. The proposed system can evaluate the feasibility and training experience of the home-based exergame as well as its beginning-stage on-body feedback system.
The use of digital technologies, like AI, advanced data analytics, VR, IoT, and game-based learning are discussed in.99 In the development of innovative rehabilitation techniques, in particular for mental health rehabilitation in people diagnosed with schizophrenia spectrum. Moreover, the authors proposed a VR serious game as an auxiliary solution for rehabilitation. It assists three forms of users including the medical team, the caregiver, and the patient. The work of100 focuses on developing and validating VR applications for the diagnosis and treatment of neurocognitive conditions including Alzheimer’s Disease. The goal here is to enhance the effectiveness of rehabilitation through the use of VR technology. The dynamics, features, architecture, and usability of the system are all customized to meet the requirements of the patient. The project investigates the existing and future applications of VR in the treatment of neurocognitive diseases. The potential use of therapeutic applications of VR is discussed in.101 These applications employed biofeedback designed along with massive virtual spaces to assist in breaking perpetual cycles of insomnia, anxiety, and depression. The VRs can take the shape of a fantastical cosmic scene, mountain tops, or a night sky. The authors also discuss the use of perceived massive spaces for therapy and the spatial foundation of the mind in virtual therapies66 discusses two cognitive interventions and their effects on people with mental and behavioral disorders. Caˆmara et al have tried Reh@City and Task Generator and the assessment results revealed that the Reh@City v2.0 program caused a significant reduction in depressive symptoms, whereas the TG program improved memory, processing speed, and social behavior of patients, hence leading them towards a quality life.
The use of telerehabilitation can be an innovative method to promote physical activity and implement home-based rehabilitation to provide rehabilitative therapy to individuals with physical, cognitive, or functional limitations. The102 evaluates the feasibility, enjoyment, and potential effect of telerehabilitation using a serious game’ MoveHero’ for people with ASD during the COVID-19 pandemic. All participants participated in telerehabilitation sessions with full adherence and there was a significant improvement in the performance of the non-ASD group at most moments. The findings support using gaming interventions and serious games to get people with ASD to be more active.
The authors of103 assessed the feasibility of non-immersive VR training for relearning functional living skills in patients with major neurocognitive disorders. The results showed significant improvement in all VR training variable scores for both EG with degenerative conditions and EG with non-degenerative conditions (NDC), with better outcomes in the EG-NDC group. The study confirmed the ecological validity of VR training for functional living skills. The work in104 aims to determine if combining RL-based virtual AI assistant with play therapy can improve physical activities like muscle reflexes, motor controls, and hand-eye coordination in wheelchair-bound children with Down syndrome. The AI assistant is designed to learn how a patient plays the game and provide challenges that are tailored to their specific abilities. The findings suggest that the agent trained with the PPO algorithm and Actor-Critic algorithm together outperforms other algorithms by being a powerful AI virtual assistant that can compete against a player with Down syndrome and help them enhance their skills as well as weaknesses.
In,105 a VR rehabilitation environment for the sake of stroke survivors has been discussed. VIRTUE application uses Unity3D along with VR Toolkit (VRTK) to enhance motivation in stroke survivor patients and help them re-learn their daily life activities. The successful deployment of VIRTUE in a hospital indicates that it is safe and acceptable for cognitive rehabilitation of stroke survivors under the supervision of occupational therapists. The study in106 evaluates the effectiveness of the VR platform namely Reh@city. Reh@City v2.0 was used in a randomized controlled trial on 36 chronic stroke patients. The results showed an improvement in over- all visuospatial ability, attention, executive functions, cognitive functioning, processing speed, verbal memory, and self-perceived cognitive deficits. The group that used Reh@City demonstrated superior performance in general cognitive functioning, visuospatial ability, and executive functions when compared to the control group.
The authors in107 evaluate the usability of non-immersive VR training on functional living skills in patients suffering from major neurocognitive disorders. The experimental group (EG) and control group (CG) were subjected to in vivo tests, and statistically significant differences were observed between them. The improvement in in vivo tests was found to be associated with the specific VRT utilized. A cognitive rehabilitation program based on self-efficacy theory was developed in108 using virtual reality technology and compared to conventional and computer-assisted cognitive rehabilitation. The study found significant differences in stroke self-efficacy, cognitive function, and health-related quality of life after implementing the virtual reality-based program. Significant group differences were observed among the groups specifically in self-efficacy and health-related quality of life.
In,109 the authors examined the impact of immersive VR on predementia individuals. Both control and experimental groups were evaluated for cognitive functioning and visual brain network connectivity. The study indicates that immersive VR cognitive training may enhance visuospatial functioning and alleviate psychiatric symptoms in predementia individuals.
Rehabilitation of Neurodegenerative Diseases
Neurodegenerative diseases refer to the gradual dysfunction of the brain with some of its parts damaged. The process is incurable however AI-based interventions have tended to delay the process successfully. Among all neurodegenerative diseases, the most common types are dementia, Alzheimer’s disease (AD), Parkinson’s disease, Huntington’s disease, etc. The study in110 is a meta-analysis to review the effectiveness of cognitive rehabilitation in non-demented Parkinson’s disease (PD) patients and findings revealed that commonly improved cognitive domains were attention, memory, and processing speed. However, further studies are necessary to determine more robust effects. The work in111 discusses the effectiveness of telephone-based reality orientation therapy (ROT) for dementia patients. The study found that implementing the ROT intervention resulted in significant improvements in patients’ understanding and sense of control over their surroundings. Furthermore, it was found to be effective for caregivers, as it helped to reduce their burden and stress levels. A systematic review22 analyzes the use of wearable devices in patients with Parkinson’s disease (PD) and neurocognitive disorders. The findings suggest that sensor-based wearable devices, particularly instrumented insoles, play a crucial role in monitoring, diagnosing, and tracking exercise for PD and neurocognitive patients. These wearables can help in improving early diagnosis, rehabilitation, and overall quality of life among PD patients.
The authors in112 analyzed that cognitive telerehabilitation improved cognition, neuropsychiatric symptoms, and memory strategies in patients with mild cognitive impairment. Results of the post-test showed that the treatment group had better scores in cognitive variables and experienced a reduction in affective symptomatology concluding that cognitive telerehabilitation is an effective intervention for mild cognitive impairment. The study of113 reviews cognitive rehabilitation for mild-to-moderate dementia and it found that cognitive rehabilitation improved self-efficacy, quality of life, and cognition in people with dementia and their care partners. However, there was insufficient evidence to determine whether it had any significant benefits for caregivers in reducing anxiety.
The work in64 is about creating and validating an AI model tailored to address cognitive impairment in dementia. The model utilized the RNN framework to forecast MMSE and MoCA scores following drug initiation. Notably, patients who received the drug recommended by the AI model exhibited enhanced cognitive performance. These findings underscore the potential for AI-informed personalized treatment to enhance cognitive outcomes in patients with dementia. In,65 the authors assess the efficacy of the cognitive rehabilitation program “GRADIOR” in individuals experiencing MCI and mild dementia. Results showed that the experimental group maintained cognitive functions with moderate to large effect sizes while the control group exhibited more decline even after a year. Using GRADIOR for longer periods may benefit people with mild cognitive impairment and mild dementia.
The research done in114 provides a comprehensive overview of how intelligent technologies can be used in clinical practice, specifically for Alzheimer’s disease. It discusses the potential benefits of these technologies and highlights areas in which their design can be improved. The study aims to provide a better understanding of the role of sensing technologies throughout the progression of the disease and identify research gaps. In,115 researchers aimed to investigate the effectiveness of a stepping exergame program in individuals with major neurocognitive disorders. The study evaluated outcomes such as gait speed, balance, reaction time, cognitive and neuropsychiatric measures, and daily life functioning. The exergaming program demonstrated significant reductions in depression when compared to the control group.
In,116 various factors are investigated that influence people with MCI and mild dementia following a CCT program. The GRADIOR program encompasses a wide array of exercises targeting orientation, memory, attention, perception, and executive functioning employing a user-friendly interface. The study aimed to identify cognitive, psychological, and physical health factors that adhere to the CCT program. The study in117 is about determining the effectiveness of an online CCT platform VIRTRAEL for clinical purposes. VIRTRAEL is designed to improve different cognitive skills in older adults with MCI. The post-test showed greater improvement in verbal learning, delayed recall, working memory, reasoning, and planning indicating that VIRTRAEL can be an effective tool in addressing cognitive symptoms associated with aging and neurodegenerative diseases.
The study in118 examined the effect of an Occupational Therapy program on the independence of older adults. The program was based on activities of daily living (ADL) cognitive stimulation. The results showed that the cognitive stimulation program helped participants to perform ADLs independently suggesting that it can help increase the independence of individuals with dementia. The article119 reviewed eight trials evaluating exergames for individuals with major neurocognitive disorders. The study found that exergames have physical and mental benefits, such as improving gait, mobility, balance, cognitive function, and quality of life. However, more controlled trials are necessary before exergames can be recommended for treatment guidelines. The objective of the study120 is to compare the efficacy of computerized training with web-based cognitive games and web-based crossword puzzles in patients with MCI. The study had a diverse sample, rigorous methodology, and a long study duration. Improvement in the ADAS-Cog score was observed in both groups, but the percentage of improvement was higher in the crossword group.
Telerehabilitation of Cardiovascular and Other Diseases
Telerehabilitation (TR) is the delivery of rehabilitation services through technology. Over the past few years, due to the advances in AI technologies and telemedical devices, telemedicine has gained a lot of attention. Long-distance communication can now be easily achieved through various means like videoconferencing, email, phone call and texting. This section contains telerehabilitation-based interventions for various diseases like cardiovascular, stroke survivors and cancer survivors.
The article121 emphasizes the necessity of performing clinical feasibility assessments of telehealth interventions, for cancer survivors in order to scrutinize effectiveness, safety, compliance, and user contentment of the intervention. The findings reveal the presence of obesity, depression and smoking in the patients which can be managed by conducting physical and telehealth exercises for each patient. In article122 researchers have highlighted the safety and impact of a home-based cardio-oncology rehabilitation (CORE) intervention utilizing a telerehabilitation among individuals who have survived hematological cancer. The approach encompassed three components: a sensor to measure heart rate, an internet platform, and remote supervision through telephone communication. The findings reveal that the participants experienced a noteworthy improvement in their cardiorespiratory fitness and maximum workload.
In123 Blioumpa et al conducted a telerehabilitation-based intervention for patients of type 2 diabetes. The intervention included exercise sessions through videoconferencing to enhance the functional capacity, regulation of blood sugar (HbA1c), quality of life and awareness of self-management in type 2 diabetes patients124 is a review article evaluating the effectiveness of wearable sensors in home-based cardiac rehab (HBCR) intervention for patients of cardiovascular diseases (CVD). The meta analysis reveals that wearable technology for the assistance of HBCR has the potential to replace center-based cardiac rehabilitation as it has improved the overall health profile of a patient with CVD. The review article125 evaluates the effects of telerehabilitation in chronic obstructive pulmonary disease (COPD) patients as compared to conventional interventions. The review suggests that telerehabilitation is safe and sound approach with noticeable diversity.
In a pandemic like COVID-19 researchers find out the need of telerehabilitation for the patients to perform their rehabilitation tasks. Article126 aims to do the same, by developing a telerehabilitation platform for the individuals having a problem of “range of motion” (ROM). The results reveal the positive impact of real-time tracking of exercises and overall approach on patients. In article127 researchers have developed a machine learning-based rehabilitation system to be practised at homes for stroke survivors. The study suggests that a home care system using a commercial smartwatch and ML model can improve ROM in stroke survivors. In,128 Garzo et al describes the telerehabilitation platform namely ArmAssist (AA) developed to help patients of stroke. With the help of healthcare professionals, the following approach includes arm and hand exercises for the individuals. The training involves some serious games suggested by professionals while the evaluation has been done by standard clinical tests. Another telerehabilitation platform MediaPipe is discussed in article.10 MediaPipe is a website used for rehabilitation of ROM and knee fracture monitoring of patients. The primary focus of MediaPipe is to provide patients necessary facilities in the comfort of their homes. The reliability and validity of the platform are measured by real cases.
Statistics and Impact
Statistics analysis are important and help to quickly identify major information of the underlying topic. Therefore, in this section, we perform an analysis of the studies that we have discussed in section IV.
Publication type is an important aspect of any research work. Among, type of publication, the journal publication are considered better than the other types of publication. In Figure 5, we presented the number of papers that have been published in conferences and journals. Similarly, we highlighted the distribution of the papers in Figure 6. Both charts show that most of the cited papers are the journal papers and the distribution for studies belonging to book chapters, conferences, and journals are 0%, 8.4% and 91.6%, respectively. Figure 6 presents that this study is mostly based on the recent journal publications in the diverse areas and it highlights the impact of AI methods in Rehabilitation process. As this work primarily focuses on the use of AI methods in the various rehabilitation process. Therefore, it is important to know the use of each AI tool separately. We present the number of applications of each AI method and corresponding distribution in Figures 7 and 8 respectively.
 |
Figure 5 Number of the papers according to their category. |
 |
Figure 6 Percentage distribution of journal, conference, and book chapters publications. |
 |
Figure 7 Number of AI-based techniques for different Rehabilitation Process. |
 |
Figure 8 Distribution of surveyed AI-based techniques. |
It is also important to statistically analyze all the rehabilitation processes that we considered in the section IV. Figure 9 shows number of papers belong to each category while Figure 10 shows the distribution of each category. It is evident from Figure 10 we considered almost all areas equally. Moreover, we can observe that ICT is contributing in many important and diverse processes of Rehabilitation.
 |
Figure 9 Number of articles surveyed for each category. |
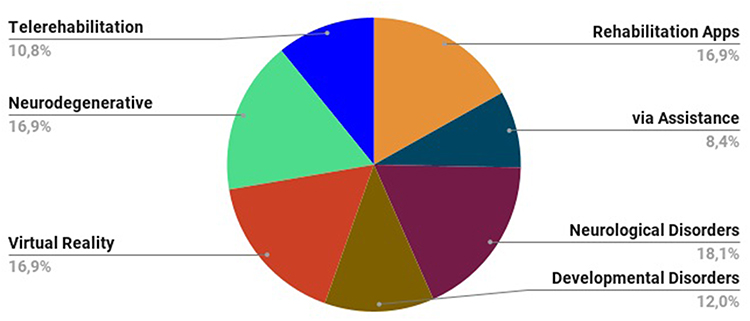 |
Figure 10 Distribution of surveyed articles for all categories. |
Furthermore, we can verify recent progress of AI and ML methods in various aspects of rehabilitation by analyzing the research work in most recent years. Therefore, we highlight the number of papers and their corresponding distribution for the years from 2020 to 2023 in Figures 11 and 12 respectively. We can quickly identify that the use of AI and ICT in rehabilitation processes has been continuously increasing over the past years. A thorough survey of the literature is very important for all research fields, and it helps the research community in identifying recent advances in the specific research direction. Similarly, there are many sub fields of a general research area like we discussed different rehabilitation process in section IV. So it is worthy to know the top cited works of each research area. To provide, such a quick and valuable information, we highlight in Table 3 the top five most cited studies against each rehabilitation process that we considered in Section IV. The column 1 indicates to the rehabilitation process and columns 2 to 6 refer to the reference of the top cited studies. For instance, the five most cited papers in the applications of AI in the category of’ Rehabilitation Apps’ in descending order are.51,53,69,75,76 Similarly, top-cited articles for Rehabilitation via Assistance, Rehabilitation for Neurological Disorders, Rehabilitation for Developmental Disorders, VR-based Rehabilitation, Rehabilitation of Neurodegenerative Diseases and Telerehabilitation of Cardiovascular & Other Diseases are22,54,57,106,129 and127 respectively.
 |
Table 3 Left To Right In Descending Order:First Five Most Cited Studies From Each Rehabilitation Type |
 |
Figure 11 Number of surveyed articles published from 2020 to 2023. |
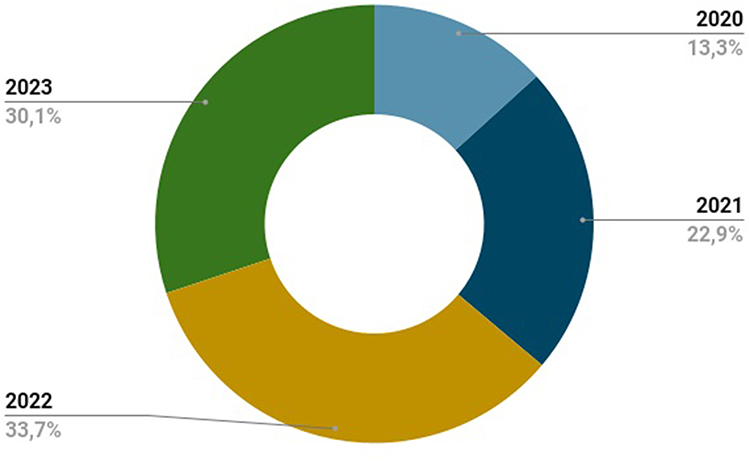 |
Figure 12 Distribution of surveyed articles for years 2020 to 2023. |
Discussion and Future Challenges
In this section, we summarize this study as well as discuss some challenges and future directions.
This review work discloses the state of the art on AI-powered methods providing cognitive stimulation, and rehabilitation for young and older adults. The study objective is to evaluate the characteristics of AI-based programs and the similarities and differences between the existing ML software, avoiding considering that all AI-enabled programs working for the rehabilitation process are identical. We divided AI-enabled techniques used for the rehabilitation process into seven different groups including Personalized rehabilitation Apps, Rehabilitation through Assistance, Rehabilitation for Neurological Disorders, Rehabilitation for Developmental Disorders, Rehabilitation for Neurodegenerative Diseases and Telerehabilitation of Cardiovascular & Other Diseases.
The study highlights that AI programs with standardized training sessions are not adaptable for treatments to the cognitive profile of patients. This is a considerable disadvantage as the training is identical for all, although the difficulty level of the exercise varies. It is also noted that a few programs can propose exercises of the most suitable cognitive difficulty level automatically. The software features can have both advantages and disadvantages as well. It also depends on the use and the characteristics of every individual, one AI program may be more appropriate than another. In our analysis, web-based software operating through an internet connection can enable the implementation of the intervention as it could be installed on any machine having an internet connection and will function remotely.
Moreover, the design and implementation of ML algorithms for neurodegenerative disease data remain hard. One apparent challenge is related to the data itself as ML models are as powerful depending on the data used for model training. A barrier to the application of ML for many diseases is the lack of large data sets, in particular, multidimensional patient data. Because such data sets normally contain data from hundreds of patients and may be noisy due to inconsistent measurement, participants drop-out. Metadata analyses can be useful as the overlap between results obtained from different datasets may be small. Therefore, metadata analyses can detect inconsistencies across datasets and enhance the statistical power of the data.18 Sometimes data are also biased towards specific demographic populations, which often limits the learning generalization and there may be a disparity in healthcare.130 Similarly, new ML methods like active learning techniques can be employed to mitigate the issue of small data sets. Active learning methods enable quality inferences from a few samples compared to ML strategies and eliminate the need to label large datasets, which can be expensive.18
The use of virtual reality for cognitive rehabilitation is increasing. Therefore, there is a need to conduct studies and research efforts focusing on the efficiency, effectiveness, validity, and reliability to validate existing VR schemes.131 Additionally, telerehabilitation and VR methods have no precise effect on a single realm, instead, plan to stimulate multiple domains simultaneously to obtain a higher degree of ecological validity.132 The design and modeling of specific VR approaches comparable with conventional techniques may provide challenging options for future research. Another issue with VR therapy is the limitation of clinical training that hampers its diffusion133 and this issue could be addressed by training some health professionals like neuropsychologists.
Some traditional examination tests concerning rehabilitation to monitor gait deflation are time-consuming and dependent on task performance, and multiple parameters such as incapability to complete due to fatigue, physical exertion by the participant, the complexity of the task assigned to the patient and walking area may affect the results.22 The AI-based wearable devices can assist in rehabilitation exercises as well as in analyzing the disease evolution. However, it should be noted that significant research is still required for wearable solutions on the reliability, precision, accuracy, and objective support of healthcare systems and patients for validation and adoption. Finally, we should agree that AI tools are already integrated into our healthcare setup and will continue to improve its applications in health-related aspects. Similarly for rehabilitation, AI is being employed for personalized treatment regimens, injury prevention, remote rehabilitation, patient monitoring, and the automation of many rehabilitation tasks. These technologies offer efficiency for practitioners, improve patient rehabilitation process, and enhance care access. However, legal implications like data protection and privacy are still a concern. Moreover, the potential negative impact of less human interaction with the use of AI is another concern that need to be considered. These challenges demand for more education, continued research, and additional legal considerations to adequately integrate the use of AI in order to provide benefits to practitioners and patients and to decrease the possible unintended negative consequences.
Conclusions
The need for rehabilitation globally is expected to increase according to WHO due to changes in the characteristics and health of the population. Keeping in view this importance, this study reviewed the recent impacts of AI technology on the rehabilitation process. We investigated AI’s role in the diverse aspects of the rehabilitation process, like personalized rehabilitation apps, rehabilitation through assistance, rehabilitation for neurological disorders, rehabilitation for developmental disorders, virtual reality rehabilitation, rehabilitation of neurodegenerative diseases and Telerehabilitation of Cardiovascular. Similarly, we highlighted the increasing use of AI for the rehabilitation process using statistical analysis. In the end, we briefly outlined some challenges regarding AI technology integration into rehabilitation processes. Future research perspectives should include both assessment and rehabilitation processes among neurological populations. Thus, AI-based technology and RL setups may be firstly implemented to differentiate between a normal/typical cognitive development and a risk of pathology. Secondly, technology- aided options may be considered in the recovery process of cognitive functions. Furthermore, one might differentiate cognitive processes (eg, attention, memory, and language). Finally, one can envisage the use of AI app and RL to investigate also emotional processes and differentiate between a typical emotional competence and/or personality disorders.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Henderson C TG, Evans-Lacko S. Mental illness stigma, help seeking, and public health programs. Am J Public Health. 2013;103(5):777–780.
2. Novakovic-Agopians T, Abrams G. Cognitive rehabilitation therapy. In: Aminoff MJ, Daroff RB, editors. Encyclopedia of the Neurological Sciences.
3. Rai S, Misra D, Misra A, Jain A, Bisla S. Impact of oral health factors on quality of life of geriatric population - a systematic review. J Indian Acad Oral Med Radiol. 2021;33:453. doi:10.4103/jiaomr.jiaomr_98_20
4. Coronato A, Naeem M, De Pietro G, Paragliola G. Rein- forcement learning for intelligent healthcare applications: a survey. Artif. Intell. Med. 2020;109:101964. doi:10.1016/j.artmed.2020.101964
5. Naeem M, Coronato A, Paragliola G. Adaptive treatment assisting system for patients using machine learning. In:
6. Shah SIH, Coronato A, Naeem M, De Pietro G. Learning and assessing optimal dynamic treatment regimes through cooperative imitation learning. IEEE Access. 2022;10:78 148–78 158. doi:10.1109/ACCESS.2022.3193494
7. Bond RR, Mulvenna MD, Potts C, O’Neill S, Ennis E, Torous J. Digital transformation of mental health services. Npj Mental Health Res. 2023;2:2731–4251.
8. Shah SIH, Naeem M, Paragliola G, Coronato A, Pech- Enizkiy M. An ai-empowered infrastructure for risk prevention during medical examination. Expert Syst Appl. 2023;225:120048. doi:10.1016/j.eswa.2023.120048
9. Ge S, Zhu Z, Wu B, McConnell ES. Technology-based cognitive training and rehabilitation interventions for individuals with mild cognitive impairment: a systematic review. BMC Geriatr. 2018;18(1):1–19. doi:10.1186/s12877-018-0893-1
10. Latreche A, Kelaiaia R, Chemori A, Kerboua A. Reliability and validity analysis of mediapipe-based measurement system for some human rehabilitation motions. Measurement. 2023;214:112826. doi:10.1016/j.measurement.2023.112826
11. Stasolla F, Di Gioia M. Combining reinforcement learning and virtual reality in mild neurocognitive impairment: a new usability assessment on patients and caregivers. Front Aging Neurosci. 2023;15. doi:10.3389/fnagi.2023.1189498
12. Figliano G, Manzi F, Tacci AL, Marchetti A, Massaro D. Ageing society and the challenge for social robotics: a systematic review of socially assistive robotics for mci patients. PLoS One. 2023;18(11):e0293324. doi:10.1371/journal.pone.0293324
13. Palestra G, Pino O. Detecting emotions during a memory training assisted by a social robot for individuals with mild cognitive impairment (mci). Multimedia Tools Appl. 2020;79(47–48):35 829–35 844. doi:10.1007/s11042-020-10092-4
14. Kim GH, Jeon S, Im K, et al. Structural brain changes after traditional and robot-assisted multi-domain cognitive training in community-dwelling healthy elderly. PLoS One. 2015;10(4):e0123251. doi:10.1371/journal.pone.0123251
15. Takayanagi K, Kirita T, Shibata T. Comparison of verbal and emotional responses of elderly people with mild/moderate dementia and those with severe dementia in responses to seal robot, paro. Front Aging Neurosci. 2014;6:257. doi:10.3389/fnagi.2014.00257
16. Mitchell J, Shirota C, Clanchy K. Factors that influence the adoption of rehabilitation technologies: a multi-disciplinary qualitative exploration. J Neuroeng Rehabil. 2023;20(1):1–7. doi:10.1186/s12984-023-01194-9
17. Kerr A, Grealy MA, Kuschmann A, Rutherford R, Rowe P. A co-creation centre for accessible rehabilitation technology. Front Rehabil Sci. 2022;2. doi:10.3389/fresc.2021.820929
18. Myszczynska MA, Ojamies PN, Lacoste AM, et al. Applications of machine learning to diagnosis and treatment of neurodegenerative diseases. Nat Rev Neurol. 2020;16(8):440–456. doi:10.1038/s41582-020-0377-8
19. Stolarz M, Mitrevski A, Wasil M, Plo¨ger PG. Personalized behaviour models: a survey focusing on autism therapy applications. arXiv preprint arXiv. 2205;2022:8975.
20. Irazoki E, Contreras-Somoza LM, Toribio-Guzma´n JM, Jenaro- R´ıo C, Van der Roest H, Franco-Mart´ın MA. Technologies for cognitive training and cognitive rehabilitation for people with mild cognitive impairment and dementia. a systematic review. Frontiers in Psychology. 2020;11:648. doi:10.3389/fpsyg.2020.00648
21. Mohebbi A. Human-robot interaction in rehabilitation and assistance: a review. Curr Rob Rep. 2020;1:131–144. doi:10.1007/s43154-020-00015-4
22. Channa A, Popescu N, Ciobanu V. Wearable solutions for patients with Parkinson’s disease and neurocognitive disorder: a sys- tematic review. Sensors. 2020;20(9):2713. doi:10.3390/s20092713
23. Moher D, Liberati A, Tetzlaff J, Altman DG. Research methods & reporting-preferred reporting items for systematic reviews and meta-analyses: the prisma statement-David Moher and colleagues introduce prisma, an update of the quorom guidelines for reporting systematic reviews and meta-analyses. BMJ. 2009;338(7716):332.
24. Rutkowska A. Telemedicine interventions as an attempt to improve the mental health of populations during the covid-19 pandemic—a narrative review. Int J Environ Res Public Health. 2022;19(22):14945. doi:10.3390/ijerph192214945
25. Gerłowska J, Furtak-Niczyporuk M, Rejdak K. Robotic assis- tance for people with dementia: a viable option for the future? Exp Rev Med Dev. 2020;17(6):507–518. doi:10.1080/17434440.2020.1770592
26. Fuentes A, Deotto A, Desrocher M, deVeber G, Westmacott R. Determinants of cognitive outcomes of perinatal and childhood stroke: a review. Child Neuropsychol. 2016;22(1):1–38. doi:10.1080/09297049.2014.969694
27. Perez DL, LaFrance WC. Nonepileptic seizures: an updated review. CNS Spect. 2016;21(3):239–246. doi:10.1017/S109285291600002X
28. Krasny-Pacini A. “Single-Case Experimental Designs for Child Neuro- Logical Rehabilitation and Developmental Disability Research,” Develop- Mental Medicine & Child. Neurology; 2023.
29. Yi Y, Hu Y, Cui M, Wang C, Wang J. Effect of virtual reality exercise on interventions for patients with Alzheimer’s disease: a systematic review. Frontiers in Psychiatry. 2022;13:1062162. doi:10.3389/fpsyt.2022.1062162
30. Yao Z, Wang H, Yan W, et al. Artificial intelligence-based diagnosis of Alzheimer’s disease with brain MRI images. Eur. J. Radiol. 2023;110934. doi:10.1016/j.ejrad.2023.110934
31. Shirwaikar RD, Sarwari I, Najam M, Shama H. “Has machine learning enhanced the diagnosis of autism spectrum disorder? Crit Rev Biomed Eng. 2023;51:1.
32. Yen JM, Lim JH. A clinical perspective on bespoke sensing mechanisms for remote monitoring and rehabilitation of neurological diseases: scoping review. Sensors. 2023;23(1):536. doi:10.3390/s23010536
33. Surianarayanan C, Lawrence JJ, Chelliah PR, Prakash E, Hewage C. Convergence of artificial intelligence and neuroscience towards the diagnosis of neurological disorders—a scoping review. Sensors. 2023;23(6):3062. doi:10.3390/s23063062
34. Bhattarai K, Rajaganapathy S, Das T, et al. Using artificial intelligence to learn optimal regimen plan for Alzheimer’s disease. J Am Med Inf Assoc. 2023;30(10):1645–1656. doi:10.1093/jamia/ocad135
35. Kashif M, Ahmad A, Bandpei MAM, et al. Systematic review of the application of virtual reality to improve balance, gait and motor function in patients with Parkinson’s disease. Medicine. 2022;101(31):e29212. doi:10.1097/MD.0000000000029212
36. Moreno-Ligero M, Lucena-Anton D, Salazar A, Failde I, Moral-Munoz JA. mhealth impact on gait and dynamic balance outcomes in neurorehabilitation: systematic review and meta-analysis. J Med Syst. 2023;47(1):75. doi:10.1007/s10916-023-01963-y
37. Maggio MG, Luca A, Calabro` RS, Drago F, Nicoletti A. Can mobile health apps with smartphones and tablets be the new frontier of cognitive rehabilitation in older individuals? A narrative review of a growing field. Neurol Sci. 2023;2023:1–9.
38. Piras F, Piras F, Orfei MD, Caltagirone C, Spalletta G. Self- awareness in mild cognitive impairment: quantitative evidence from systematic review and meta-analysis. Neurosci Biobehav Rev. 2016;61:90–107. doi:10.1016/j.neubiorev.2015.10.002
39. Chung CS, Pollock A, Campbell T, Durward BR, Hagen S. Cognitive rehabilitation for executive dysfunction in adults with stroke or other adult non-progressive acquired brain damage. Cochrane Database Syst Rev. 2013;(4). doi:10.1002/14651858.CD008391.pub2
40. Radanliev P, De Roure D, Novitzky P, Sluganovic I. Ac- cessibility and inclusiveness of new information and communication technologies for disabled users and content creators in the metaverse. Disabil Rehabil. 2023;2023:1–15.
41. Modi N, Singh J. A survey of research trends in assistive technologies using information modelling techniques. Disabil Rehabil. 2022;17(6):605–623. doi:10.1080/17483107.2020.1817992
42. Narad ME, Shultz EL, Kurowski BG, et al. Technology-assisted rehabilitation interventions following pediatric brain injury. J Neuros Sci. 2018;62(2):187. doi:10.23736/S0390-5616.17.04277-1
43. Rodriguez R. How learning works: seven research-based principles for smart teaching [review]/Susan A. Ambrose, Michael W. Bridges, Marsha C. Lovett, Michele DiPietro, and Marie K. Norman. J Appl Chris Lead. 2011;5(2):106–107.
44. Khanzode KCA, Sarode RD. Advantages and disadvantages of artificial intelligence and machine learning: a literature review. Internat J Lib Inform Sci. 2020;9(1):3.
45. Naeem M, Rizvi STH, Coronato A. A gentle introduction to reinforcement learning and its application in different fields. IEEE Access. 2020;8:209 320–209 344. doi:10.1109/ACCESS.2020.3038605
46. Andriella A, Torras C, Alenya` G. Cognitive system framework for brain-training exercise based on human-robot interaction. Cogni Comput. 2020;12:793–810. doi:10.1007/s12559-019-09696-2
47. Kotu V, Deshpande B. Chapter 10 - deep learning. In: Kotu V, Deshpande B, editors. Data Science. Morgan Kaufmann; 2019:307–342.
48. Kirtas M, Tsampazis K, Tosidis P, Passalis N, Tefas A. Chapter 21 - deep learning for robotics examples using opendr. In: Iosifidis A, Tefas A, editors. Deep Learning for Robot Perception and Cognition. Academic Press; 2022:579–596.
49. Rathnayaka MH, Watawala WK, Manamendra MG, Silva SR, Kasthurirathna D, Jayalath T. Cognitive rehabilitation based personalized solution for dementia patients using reinforcement learning. In:
50. Zini F, Le Piane F, Gaspari M. Adaptive cognitive training with reinforcement learning. ACM Trans. Interact. Intell. Syst. 2022;12:1–29. doi:10.1145/3476777
51. Tang F, Lin K, Uchendu I, Dodge H, Zhou J. Improving mild cognitive impairment prediction via reinforcement learning and dialogue simulation; 2018.
52. Kurniawan Y, Christian W, Anwar N. Designing mobile applica- tions to support learning from home for children with autism spectrum disorder. In:
53. Ntalindwa T, Nduwingoma M, Karangwa E, Soron TR, Uwor- Wabayeho A, Uwineza A. Development of a mobile app to improve numeracy skills of children with autism spectrum disorder: participatory design and usability study. JMIR Pediat Par. 2021;4(3):e21471. doi:10.2196/21471
54. Snoun A, Bouchrika T, Jemai O. Deep-learning-based human activity recognition for Alzheimer’s patients’ daily life activities as- sistance. Neural Comput Appl. 2022;35:1–26. doi:10.1007/s00521-022-07048-0
55. Munteanu D, Bejan C, Munteanu N, et al. Deep-learning-based system for assisting people with alzheimerrsquo; s disease. Electronics. 2022;11(19):3229. doi:10.3390/electronics11193229
56. Nasri N, Lo´pez-Sastre RJ, Pacheco-da Costa S, et al. Assistive robot with an ai-based application for the reinforcement of activities of daily living: technical validation with users affected by neurodevelopmental disorders. Appl Sci. 2022;12(19):9566. doi:10.3390/app12199566
57. Brown VM, Zhu L, Solway A, et al. Reinforcement learning disruptions in individuals with depression and sensitivity to symptom change following cognitive behavioral therapy. JAMA Psychiatry. 2021;78(10):1113–1122. doi:10.1001/jamapsychiatry.2021.1844
58. Bernini S, Panzarasa S, Sinforiani E, et al. Homecore for telerehabilitation in mild or major neurocognitive disorders: a study protocol for a randomized controlled trial. Front Neurol. 2021;12. doi:10.3389/fneur.2021.752830
59. Merlo G, Chifari A, Chiazzese G, et al.The behave application as a tool to monitor inclusive interventions for subjects with neurode- velopmental disorders. Frontiers in Psychology. 2022;(13):943370. doi:10.3389/fpsyg.2022.943370
60. Nissan N, Hertz U, Shahar N, Gabay Y. Distinct reinforcement learning profiles distinguish between language and attentional neurode- velopmental disorders. Behav Br Funct. 2023;19:03. doi:10.1186/s12993-023-00207-w
61. Milani S, Fan Z, Gulati S, Nguyen TH, Fang F, Yadav A. In- telligent tutoring strategies for students with autism spectrum disorder: a reinforcement learning approach; 2020.
62. Wu J, Peng J, Li Z, et al. Multi-domain computerized cognitive training for children with intellectual developmental disorder: a randomized controlled trial. Frontiers in Psychology. 2023;13:1.
63. Minoofam SAH, Bastanfard A, Keyvanpour MR. Ralf: an adaptive reinforcement learning framework for teaching dyslexic students. Multimedia Tools Appl. 2022;81:1573–7721. doi:10.1007/s11042-021-11806-y
64. Liu Q, Vaci N, Koychev I, et al. Personalised treatment for cognitive impairment in dementia: development and validation of an artificial intelligence model. BMC Med. 2022;20(1):1–12. doi:10.1186/s12916-022-02250-2
65. Diaz Baquero AA, Franco-Mart´ın MA, Parra Vidales E, et al. The effec- tiveness of gradior: a neuropsychological rehabilitation program for people with mild cognitive impairment and mild dementia. results of a randomized controlled trial after 4 and 12 months of treatment. J Alzheimers Dis. 2022;86(2):711–727. doi:10.3233/JAD-215350
66. Caˆmara J, Ferreira R, Teixeira L, et al. Efficacy of adaptive cognitive training through desktop virtual reality and paper-and-pencil in the treatment of mental and behavioral disorders. Virtual Reality. 2023;27:291–306. doi:10.1007/s10055-021-00559-6
67. Scha¨ttin A, Pickles J, Flagmeier D, et al. De- velopment of a novel home-based exergame with on-body feedback: usability study. JMIR Seri Games. 2022;10(4):e38703. doi:10.2196/38703
68. Wright JH, Owen J, Eells TD, et al. Effect of computer-assisted cognitive behavior therapy vs usual care on depression among adults in primary care: a randomized clinical trial. JAMA Network Open. 2022;5(2):e2 146 716–e2 146 716. doi:10.1001/jamanetworkopen.2021.46716
69. Newman MG, Jacobson NC, Rackoff GN, Bell MJ, Taylor CB. A randomized controlled trial of a smartphone-based application for the treatment of anxiety. Psychother Res. 2021;31(4):443–454. doi:10.1080/10503307.2020.1790688
70. Chen L, Lin L, Weizhou J, Lin S, Lin W. The research of cognitive rehabilitation training system for ADHD children. In:
71. Pedroli E, Mancuso V, Stramba-Badiale C, et al. Brain m-app’s structure and usability: a new application for cognitive rehabilitation at home. Front Human Neurosci. 2022;16. doi:10.3389/fnhum.2022.898633
72. Kamnardsiri T, Phirom K, Boripuntakul S, Sungkarat S. An interactive physical-cognitive game-based training system using Kinect for older adults: development and usability study. JMIR Seri Games. 2021;9(4):e27848. doi:10.2196/27848
73. Gonc¸alves HIM, da Silva FO. Cognitive rehabilitation: a comparison model of a digital environment based on serious games and the traditional methods. Procedia Comput Sci. 2023;219:1333–1340. doi:10.1016/j.procs.2023.01.418
74. Clare L, Kudlicka A, Collins R, et al. Implementing a home-based personalised cognitive rehabilitation intervention for people with mild-to-moderate dementia: great into practice. BMC Geriatr. 2023;23(1):1–17. doi:10.1186/s12877-022-03705-0
75. Swinnen N, de Bruin ED, Dumoulin C, et al. The vital stepping exergame prototype for older adults with major neurocognitive disorder: a usability study. Front Aging Neurosci. 2021;13. doi:10.3389/fnagi.2021.701319
76. Robert P, Manera V, Derreumaux A, et al. Efficacy of a web app for cog- nitive training (memo) regarding cognitive and behavioral performance in people with neurocognitive disorders: randomized controlled trial. J Med Int Res. 2020;22(3):e17167. doi:10.2196/17167
77. Drin F, Oskar S, Luis P, et al. Effectiveness of a mobile application for independent cognitive training in patients with mild cognitive impairments: study protocol for the nenae study, a randomized controlled trial Research Square Preprint under review at BMC Trials. 2023;2023:1. doi:10.21203/rs.3.rs-3235206/v1
78. Ben Taleb W, Snoun A, Bouchrika T, Jemai O. Reinforcement learning for assistance of Alzheimer’s disease patients. In:
79. Cisnal A, Mart´ınez-Cagigal V, Alonso-Linaje G, et al. An overview of m3rob, a robotic platform for neuromotor and cognitive rehabilitation using augmented reality,” in de XL Congreso Anual de la Sociedad Espan˜ola de Ingenier´ıa Biome´dica. Valladolid. 2022;2022:1.
80. Ayimdji Tekemetieu A, Pigot H, Bottari C, Giroux S. From speech acts to assistance acts for cognitive assistance in ambient assisted living: how to nudge cognitively impaired people to act independently. J Amb Intellig Hum Com. 2023;14(9):11 767–11 793. doi:10.1007/s12652-022-03735-x
81. Ha Y, Park M. Effects of stroke rehabilitation using gait robot- assisted training and person-centered goal setting: a single blinded pilot study. In: Healthcare. MDPI; 2023:588.
82. Pike AC, Robinson OJ. Reinforcement learning in patients with mood and anxiety disorders vs control individuals: a systematic review and meta-analysis. JAMA psychiatry. 2022;79:313. doi:10.1001/jamapsychiatry.2022.0051
83. Lampit A, Launder NH, Minkov R, et al. Computerized cognitive training in people with depression: a protocol for a systematic review and meta-analysis. Syst Rev. 2022;11(1):1–6. doi:10.1186/s13643-021-01872-6
84. Rodriguez-Villa E, Camacho E, Torous J. Psychiatric rehabilita- tion through teaching smartphone skills to improve functional outcomes in serious mental illness. Inter Intervent. 2021;23:100366. doi:10.1016/j.invent.2021.100366
85. Vaia S, Iavarone A, Moschiano F, et al. Computer-aided cognitive training in patients with neurocognitive vascular impairment: effects on cognition, depression and behavior. J Gerontol Geri. 2022;70:99–104. doi:10.36150/2499-6564-N357
86. Campagnini S, Arienti C, Patrini M, Liuzzi P, Mannini A, Carrozza MC. Machine learning methods for functional recovery prediction and prognosis in post-stroke rehabilitation: a systematic review. J Neuroeng Rehabil. 2022;19(1):1–22. doi:10.1186/s12984-021-00978-1
87. Colombini G, Duradoni M, Carpi F, Vagnoli L, Guazzini A. Leap motion technology and psychology: a mini-review on hand movements sensing for neurodevelopmental and neurocognitive dis- orders. Int J Environ Res Public Health. 2021;18(8):4006. doi:10.3390/ijerph18084006
88. Cuevas H, Stuifbergen AK, Hilsabeck RC, Sales A, Wood S, Kim J. The role of cognitive rehabilitation in people with type 2 diabetes: a study protocol for a randomized controlled trial. PLoS One. 2023;18(5):e0285553. doi:10.1371/journal.pone.0285553
89. Alwi SMS, Narayanan V, Din NC, Taib NAM. Cognitive rehabilitation programs for survivors of breast cancer treated with chemotherapy: a systematic review. Rehabilit Oncol. 2021;39(4):155–167. doi:10.1097/01.REO.0000000000000268
90. Ghosh A, De Chatterjee S, Maji AK. Towards data- driven cognitive rehabilitation for speech disorder in hybrid sensor architecture. In
91. Gual N, Garc´ıa-Salmones M, Br´ıtez L, et al. The role of physical exercise and rehabilitation in delirium. Eur Geriatric Med. 2020;11:83–93. doi:10.1007/s41999-020-00290-6
92. Keefe RS, Can˜adas E, Farlow D, Etkin A. Digital intervention for cognitive deficits in major depression: a randomized controlled trial to assess efficacy and safety in adults. Am J Psychiatry. 2022;179(7):482–489. PMID: 35410496. doi:10.1176/appi.ajp.21020125
93. Manser P, Michels L, Schmidt A, Barinka F, de Bruin ED. Effectiveness of an individualized exergame-based motor- cognitive training concept targeted to improve cognitive functioning in older adults with mild neurocognitive disorder: study protocol for a randomized controlled trial. JMIR Res Protoc. 2023;12(1):e41173. doi:10.2196/41173
94. Luo X, Guo X, Zhao Q, et al. A randomized controlled study of remote computerized cognitive, neurofeedback, and combined training in the treatment of children with attention-deficit/hyperactivity disor- der. Eur Child Adolesc Psychiatry. 2023;32(8):1475–1486. doi:10.1007/s00787-022-01956-1
95. Atmaca F, Yıldız-Demirtas V. Does cognitive training affect reading and writing skills of students with specific learning disabil- ities? Learn Disability Q. 2023;46(2):106–119. doi:10.1177/07319487221085994
96. Maggio MG, Foti Cuzzola M, Calatozzo P, et al. Improving cognitive functions in adolescents with learning difficulties: a feasibility study on the potential use of telerehabilitation during covid-19 pandemic in Italy. Journal of Adolescence. 2021;89:194–202. doi:10.1016/j.adolescence.2021.05.005
97. Capodieci A, Graziani D, Scali V, Giaccherini S, Luccherino L, Pecini C. Telerehabilitation pathways in specific learning disorders: improving reading and writing. Br Sci. 2023;13(3):479. doi:10.3390/brainsci13030479
98. Darekar A. Virtual Reality for Motor and Cognitive Rehabilitation. Springer; 2023.
99. Lopes RP, Barroso B, Deusdado L, et al. Digital technologies for innovative mental health rehabilitation. Electronics. 2021;10(18):2260. doi:10.3390/electronics10182260
100. Merlo EM, Myles LAM, Pappalardo SM. The vespa project: virtual reality interventions for neurocognitive and develop- mental disorders. J Mind Med Sci. 2022;9(1):16–27. doi:10.22543/7674.91.P1627
101. Jerath R, Beveridge C. Harnessing the spatial foundation of mind in breaking vicious cycles in anxiety, insomnia, and depression: the future of virtual reality therapy applications. Frontiers in Psychiatry. 2021;12:645289. doi:10.3389/fpsyt.2021.645289
102. e Almeida AF, da Silva TD, de Moraes ÍA, et al. Virtual reality as a telerehabilitation strategy for people with autism spectrum disorder during the covid-19 quarantine scenario: physical activity, motor performance and enjoyment. Disabil Rehabil. 2023;1(1):1–11.
103. Panerai S, Catania V, Rundo F, et al. Functional living skills in patients with major neurocognitive disorder due to degenerative or non-degenerative conditions: effectiveness of a non-immersive virtual reality training. Sensors. 2023;23:4.
104. Mariselvam J, Rajendran S, Alotaibi Y. Reinforcement learning- based ai assistant and vr play therapy game for children with down syndrome bound to wheelchairs. AIMS Mathemat. 2023;8:16 989–17 011.
105. Chatterjee K, Buchanan A, Cottrell K, Hughes S, Day TW, John NW. Immersive virtual reality for the cognitive rehabilitation of stroke survivors. IEEE Transact NeuSyst Reha. 2022;30:719–728. doi:10.1109/TNSRE.2022.3158731
106. Faria AL, Pinho MS, Bermu´dez I Badia S. A comparison of two personalization and adaptive cognitive rehabilitation approaches: a randomized controlled trial with chronic stroke patients. J Neuroeng Rehabil. 2020;17:1–15. doi:10.1186/s12984-020-00691-5
107. Panerai S, Gelardi D, Catania V, et al. Functional living skills: a non-immersive virtual reality training for individuals with major neurocognitive disorders. Sensors. 2021;21(17):5751.
108. Park M, Ha Y. Effects of virtual reality-based cognitive rehabilitation in stroke patients: a randomized controlled trial. Healthcare. 2023;11(21). doi:10.3390/healthcare11212846
109. Kang JM, Kim N, Lee SY, et al. Effect of cognitive training in fully immersive virtual reality on visuospatial function and frontal-occipital functional connectivity in predementia: randomized controlled trial. J Med Internet Res. 2021;23(5):e24526.
110. Sanchez-Luengos I, Balboa-Bandeira Y, Lucas-Jime´nez O, Ojeda N, Pena J, Ibarretxe-Bilbao N. Effectiveness of cognitive rehabili- tation in Parkinson’s disease: a systematic review and meta-analysis. J Person Med. 2021;11(5):429. doi:10.3390/jpm11050429
111. Panerai S, Raggi A, Tasca D, et al. Telephone-based reality orienta- tion therapy for patients with dementia: a pilot study during the covid- 19 outbreak. Am J Occupat Therap. 2021;75:7502205130p1. doi:10.5014/ajot.2021.046672
112. Canyazo CM, Keller G, Helou B, et al. Effectiveness of cognitive rehabilitation on mild cognitive impairment using teleneuropsychology. Dem Neuropsychol. 2023;17(17):e20220079. doi:10.1590/1980-5764-dn-2022-0079
113. Kudlicka A, Martyr A, Bahar-Fuchs A, Sabates J, Woods B, Clare L. Cognitive rehabilitation for people with mild to moderate dementia. Cochrane Database Syst Rev. 2023;6(6). doi:10.1002/14651858.CD013388.pub2
114. Gillani N, Arslan T. Intelligent sensing technologies for the diagnosis, monitoring and therapy of Alzheimer’s disease: a systematic review. Sensors. 2021;21(12):4249. doi:10.3390/s21124249
115. Swinnen N, Vandenbulcke M, de Bruin ED, Akkerman R, Stubbs B, Vancampfort D. Exergaming for people with major neurocognitive disorder: a qualitative study. Disabil Rehabil. 2022;44(10):2044–2052. doi:10.1080/09638288.2020.1822934
116. Diaz Baquero AA, Perea Bartolome´ MV, Toribio-Guzma´n JM, et al. Determinants of adherence to a “gradior” computer-based cognitive training program in people with mild cognitive impairment (mci) and mild dementia. J Clin Med. 2022;11(6):1714. doi:10.3390/jcm11061714
117. Rute-Pe´rez S, Rodr´ıguez-Dom´ınguez C, Ve´lez-Coto M, Pe´rez- Garc´ıa M, Caracuel A. Effectiveness of computerized cognitive training by virtrael on memory and executive function in older people: a pilot study. Br Sci. 2023;13(4):684. doi:10.3390/brainsci13040684
118. Jiménez Palomares M, González López-Arza MV, Garrido Ardila EM, Rodríguez Domínguez T, Rodríguez Mansilla J. Effects of a cognitive rehabilitation programme on the Independence performing activities of daily living of persons with dementia—a pilot randomized controlled trial. Br Sci. 2021;11(3):319. doi:10.3390/brainsci11030319
119. Nathalie Swinnen MV, Vancampfort D, Vancampfort D. Exergames in people with major neurocognitive disorder: a systematic review. Disabil Rehabil. 2022;17(4):376–389. PMID: 32697614. doi:10.1080/17483107.2020.1785566
120. Devanand DP, Goldberg TE, Qian M, et al. Computerized games versus crosswords training in mild cognitive impairment. NEJM Evid. 2022;1(12):2200121. doi:10.1056/EVIDoa2200121
121. Batalik L, Filakova K, Radkovcova I, et al. Cardio-oncology rehabilitation and telehealth: rationale for future integration in supportive care of cancer survivors. Front Car Diovasc Med. 2022;9:858334. doi:10.3389/fcvm.2022.858334
122. Filakova K, Janikova A, Felsoci M, et al. Home-based cardio-oncology rehabilitation using a telerehabilitation platform in hematological cancer survivors: a feasibil- ity study. BMC Spor Sci Med Rehab. 2023;15(1):38. doi:10.1186/s13102-023-00650-2
123. Blioumpa C, Karanasiou E, Antoniou V, et al. Efficacy of supervised home-based, real time, videoconferencing telerehabilitation in patients with type 2 diabetes: a single-blind randomized controlled trial. Eur J Phys Rehabil Med. 2023;59(5):628. doi:10.23736/S1973-9087.23.07855-3
124. Antoniou V, Davos CH, Kapreli E, Batalik L, Panagiotakos DB, Pepera G. Effectiveness of home-based cardiac rehabilitation, us- ing wearable sensors, as a multicomponent, cutting-edge intervention: a systematic review and meta-analysis. J Clin Med. 2022;11(13):3772. doi:10.3390/jcm11133772
125. Hartman M, Mina´rikova´ J, Batalik L, et al. Effects of home-based training with internet telehealth guidance in COPD patients entering pulmonary rehabilitation: a systematic review. Int J Chronic Obstr. 2023;2305–2319. doi:10.2147/COPD.S425218
126. Latreche A, Kelaiaia R, Chemori A, Kerboua A. A new home- based upper-and lower-limb telerehabilitation platform with experimen- tal validation. Arab J Sci Eng. 2023;2023:1–16.
127. Chae SH, Kim Y, Lee K-S, Park H-S. Development and clinical evaluation of a web-based upper limb home rehabilitation system using a smartwatch and machine learning model for chronic stroke survivors: prospective comparative study. JMIR mHealth and uHealth. 2020;8(7):e17216. doi:10.2196/17216
128. Garzo A, Jung JH, Arcas-Ruiz-Ruano J, Perry JC, Keller T. Armassist: a telerehabilitation solution for upper-limb rehabilitation at home. IEEE Rob Autom Mag. 2022;30(1):62–71. doi:10.1109/MRA.2022.3225716
129. Kohli M, Kar AK, Bangalore A. Machine learning- based aba treatment recommendation and personalization for autism spectrum disorder: an exploratory study. Br Inform. 2022;9. doi:10.1186/s40708-022-00164-6
130. Popejoy AB, Fullerton SM. Genomics is failing on diversity. Nature. 2016;538(7624):161–164. doi:10.1038/538161a
131. Mishkind MC, Norr AM, Katz AC, Reger GM. Review of virtual reality treatment in psychiatry: evidence versus current diffusion and use. Current Psychiatry Reports. 2017;19:1–8. doi:10.1007/s11920-017-0836-0
132. Mantovani E, Zucchella C, Bottiroli S, et al. Telemedicine and virtual reality for cognitive rehabilitation: a roadmap for the covid-19 pandemic. Front Neurol. 2020;11:926. doi:10.3389/fneur.2020.00926
133. Wiederhold BK, Riva G. Virtual reality therapy: emerging topics and future challenges. Cyberpsychol, Behav Soc Network. 2019;22(1):3–6. doi:10.1089/cyber.2018.29136.bkw
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Promise and Provisos of Artificial Intelligence and Machine Learning in Healthcare
Bhardwaj A
Journal of Healthcare Leadership 2022, 14:113-118
Published Date: 20 July 2022
Undergraduate Medical Students’ and Interns’ Knowledge and Perception of Artificial Intelligence in Medicine

Jha N, Shankar PR, Al-Betar MA, Mukhia R, Hada K, Palaian S
Advances in Medical Education and Practice 2022, 13:927-937
Published Date: 23 August 2022
Machine Learning and AI in Cancer Prognosis, Prediction, and Treatment Selection: A Critical Approach
Zhang B, Shi H, Wang H
Journal of Multidisciplinary Healthcare 2023, 16:1779-1791
Published Date: 26 June 2023
Exploring the Role of Artificial Intelligence in Mental Healthcare: Current Trends and Future Directions – A Narrative Review for a Comprehensive Insight
Alhuwaydi AM
Risk Management and Healthcare Policy 2024, 17:1339-1348
Published Date: 21 May 2024
A Theoretical Framework for Shared Reasoning Fragility in Clinician-Chatbot Interactions Through the Example of Antibiotic Prescribing
Giacobbe DR, Grossi AA, Marelli C, Muccio M, Guastavino S, Murgia Y, Mora S, Signori A, Rosso N, Giacomini M, Campi C, Piana M, Bassetti M
Infection and Drug Resistance 2026, 19:601126
Published Date: 11 May 2026