Back to Journals » Patient Preference and Adherence » Volume 16
Psychological Status During the Second Pregnancy and Its Influencing Factors
Authors Cai Y, Shen Z, Zhou B, Zheng X, Li Y, Liu Y, Yang J, Xie N, Chen H
Received 13 May 2022
Accepted for publication 1 August 2022
Published 26 August 2022 Volume 2022:16 Pages 2355—2363
DOI https://doi.org/10.2147/PPA.S374628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Yimin Cai,1,* Zhoumin Shen,1,* Bifang Zhou,2 Xiali Zheng,3 Yulian Li,2 Yuming Liu,3 Jiayu Yang,3 Nian Xie,4 Hongjiao Chen4
1Department of Nursing, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, 410005, People’s Republic of China; 2Department of Interventional Vascular Surgery, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, Hunan, 410005, People’s Republic of China; 3Department of Pediatrics, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, Hunan, 410005, People’s Republic of China; 4Department of Nursing, Medical School, Medical College of Hunan Normal University, Changsha, Hunan, 410013, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bifang Zhou, Department of Interventional Vascular Surgery, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), No. 61 of Jiefang West Road, Furong District, Changsha, 410005, People’s Republic of China, Tel +86-13755027990, Fax +86-0731-82278012, Email [email protected]
Objective: To investigate the psychological status of women during their second pregnancy.
Methods: A total of 162 women who were pregnant for the second time were selected as the research subjects. The general demographic data and pregnancy-related conditions of the subjects were investigated by a questionnaire developed for this study. The anxiety and depression of the subjects were evaluated with a self-rating anxiety scale (SAS) and a self-rating depression scale (SDS).
Results: The subjects scored themselves on the SAS and on the SDS. There was a statistically significant difference when comparing the scores and total scores with the domestic norm. Statistical data analysis was conducted using SPSS 19.0 software. The results of a multi-factor logistics regression analysis showed that four factors, namely a low age, low education level, low monthly household income and foetal sex expectations, were the main influencing factors for the occurrence of anxiety among women during their second pregnancies (p < 0.05). Three factors, namely a low education level, low monthly household income and a poor relationship between the husband and wife, were the main influencing factors for the occurrence of depression among the subjects (p < 0.05).
Conclusion: During their second pregnancies, women have different degrees of anxiety and depression. Measures should be taken to intervene and guide women who develop these adverse emotions.
Keywords: second child, psychological condition, anxiety, depression, influencing factors
Introduction
Pregnancy is a special time in a woman’s life when a foetus develops and grows inside her body. The internal environment of the pregnant woman’s body changes significantly, and she also faces many external stimuli from her family and society. The combination of many internal and external factors makes pregnant women susceptible to severe and persistent psychological stress.1 Although women in their second pregnancies already have relevant pregnancy and parenting experience, the incidence of anxiety, depression and panic during pregnancy and delivery may be higher than that of women during their first pregnancies.2 Adverse emotions such as anxiety and depression during pregnancy directly affect both the mother and the foetus and likely lead to a variety of pregnancy complications and adverse delivery outcomes such as postpartum haemorrhage, prolonged labour, increased rates of caesarean delivery and neonatal monitoring, preterm delivery and low-birth-weight infants.3 An analysis was performed of risk factors for increased maternal depression in second pregnancies compared to first pregnancies, with the following results: generally speaking, the prognosis of postpartum depression is good, and most mothers can recover within one year, but the recovery period in severe cases is more than two years, resulting in damage to the physical and mental health of mothers.4 Since the implementation of the “two-child policy”, the number of pregnant women has increased. The negative emotions women experience during their first pregnancies are very likely to lead to more negative emotions during their second pregnancies. According to research reports by Zhou Guilan and others,5 the prevalence of postpartum depression symptoms under the two-child policy is as high as 43.92%. Factors such as neonatal gender satisfaction, weight gain during pregnancy, early contact and early sucking, and family monthly income affect the incidence of postpartum depression. These individual and family factors act on women during their second pregnancies, greatly increasing the risk of postpartum depression, so it is necessary to analyse the psychological status of pregnant women during their second pregnancies and other relevant influencing factors. The aim of this study is to understand the psychological status of women during their second pregnancies, to explore the factors influencing the psychological status of these pregnant women, and to provide theoretical support and guidance for clinical workers so they can help women improve their adverse emotions and health care during pregnancy.
Methods
Clinical Data
A total of 162 women pregnant with their second child who visited the Obstetrics Outpatient Department or were hospitalised in the ward of a tertiary care hospital in Changsha from January to August 2018 were selected as the survey subjects. Inclusion criteria included the following: ① Women in their second pregnancy who were confirmed to be pregnant; ② informed consent and voluntary participation in the study; ③ no abnormal mental status, normal expression and comprehension, no communication barriers and the ability to fill in simple questionnaires on their own. Exclusion criteria included the following: ① severe infection during pregnancy, foetal malformation, twins or multiple pregnancies; ② women with acute and critical illnesses or serious pregnancy complications; ③ a history of psychosis or cognitive dysfunction.
Methods
A general data questionnaire, a self-rating anxiety scale (SAS) and a self-rating depression scale (SDS) were used for the survey. SPSS software was used for data analysis, and the citation specifications of SAS and SDS scales were added.6 The questionnaires were distributed and collected on site, with a recovery rate of 100.00%. The general data questionnaire included age, occupation, marital status, education level, place of residence, income, the couple’s relationship, family support (parents), foetal sex expectations, whether the pregnancy was planned, the number of pregnancies, pregnancy comorbidities, gestational weeks and the history of miscarriage. The SAS contained 20 items and included psychogenic-emotional symptoms (anxiety, fear, panic, palpitations and dizziness), somatic disorders (trembling of hands and feet, body aches, weakness, tingling of hands and feet, stomach pain or indigestion, frequent urination, sweating, facial flushing and sleep disorders), psychomotor disorders (akathisia and dyspnoea) and depressive psychological disorder (feelings of madness, unfortunate anticipations, fainting and nightmares). A four-point scale was used: no or very little time (≤1 day/week) was one point, a small amount of time (1–2 days/week) was two points, a considerable amount of time (3–4 days/week) was three points, and most or all of the time (5–7 days/week) was four points. (NOTE: Reverse-score items noted with *.) The scores of the 20 items were added up and multiplied by 1.25, with a full score of 100 points. The categories included severe anxiety: >69, moderate anxiety: 60–69 and mild anxiety: 50–59. The SDS consisted of 20 items, including psychogenic-emotional symptoms (depressed mood and crying), somatic disorders (constipation, loss of libido, weight loss, tachycardia, loss of appetite, sleep disturbances and day/night differences in mood), psychomotor disorders (agitation and psychomotor depression) and depressive disorders (dissatisfaction, feelings of emptiness, self-depreciation, irritability, feelings of hopelessness, confused thinking, recurrent thoughts and indecisiveness). The scale was scored on four levels: no or very little time (≤1 day/week) was one point, a small amount of time (1–2 days/week) was two points, a considerable amount of time (3–4 days/week) was three points and most or all of the time (5–7 days/week) was four points. (NOTE: Reverse-score items noted with *.) The scores of the 20 items were summed and multiplied by 1.25, with the result being the standard score, with a full score of 100 points. According to the scale, mild depression was 53–62 points, moderate depression was 63–72 points and severe depression was >72 points. The subjects’ SAS and SDS scores were compared with the SAS and SDS scores of the domestic norm (literature source required).
Statistical Methods
The data of this study were statistically analysed using SPSS 19.0 statistical software. The measurement data were expressed as (±s) with a t-test, the count data were expressed as percentages, a one-way ANOVA was performed for multiple comparisons (a chi-square test was not used; the t-test was used to compare the SAS and SDS scores of subjects in this study with the domestic norm) and a logistic regression analysis was used for a multi-factor analysis. Statistical significance was determined at p < 0.05.
Results
The data collected from the survey were analysed with SPSS, and the reliability coefficient was 0.9. The validity was analysed to ensure construct validity; KMO > 0.6, showing that the collected data were valid and reliable. Language communication difficulties and unable to communicate normally. The ages of the 162 women in this survey ranged from 23 to 42 years, with an average age of 31.92 ± 2.97 years; this was close to the norm (p > 0.05). The SAS score of the subjects was 39.42 ± 7.18, and anxiety was present in 31 cases (19.14%), including 22 cases (13.58%) of mild anxiety, eight cases (4.94%) of moderate anxiety and one case (0.62%) of severe anxiety. The SDS score was 38.59 ± 9.61, and depression was present in 16 cases (9.88%), including mild depression in 11 cases (13.58%) and moderate depression in five cases (4.94%). Details are shown in Table 1.
 |
Table 1 SAS and SDS Scale Scores of Pregnant Women with Second Child |
The SAS and SDS scores of the women in their second pregnancies were higher than those of the domestic norm, and the difference was statistically significant (p < 0.001). For details, see Table 2.
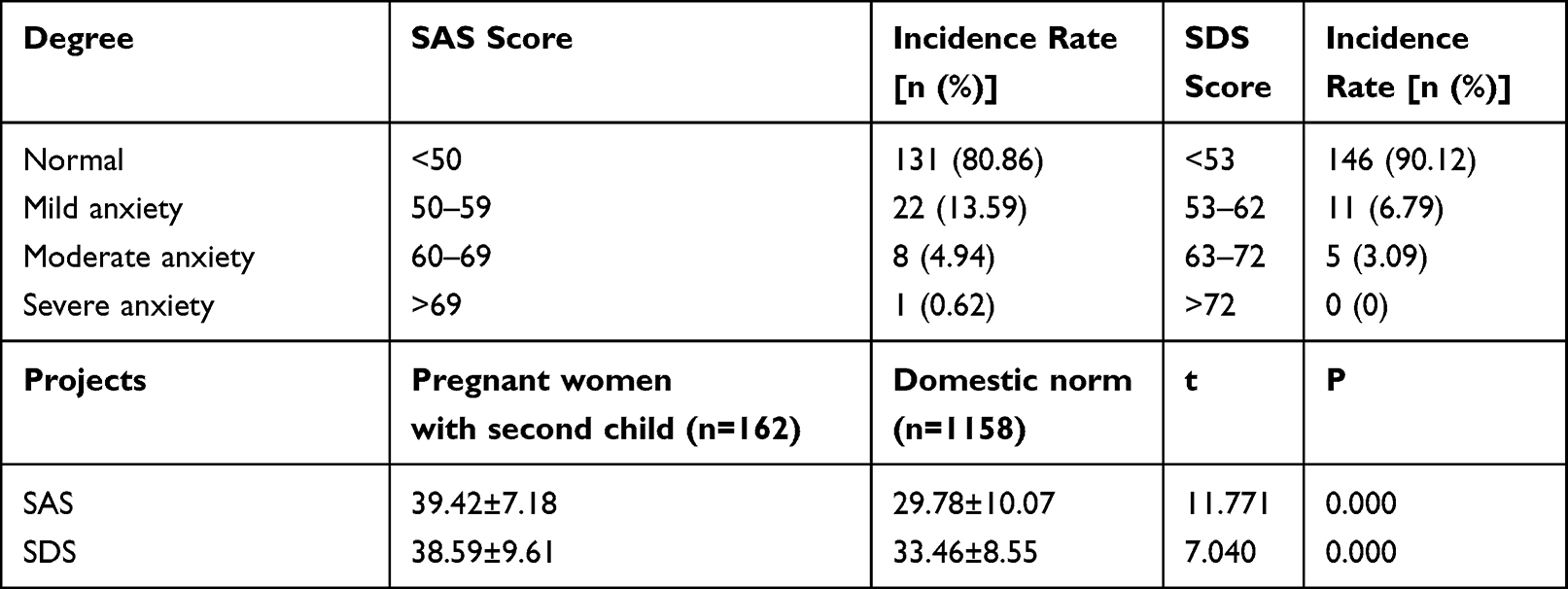 |
Table 2 Comparison of SAS and SDS Scale Scores of Pregnant Women with Second Birth with the Domestic Norm |
One-Way Analysis of Factors Influencing Anxiety
A one-way analysis of factors showed that seven factors (age, education level, monthly household income, the couple’s relationship, family support [parents], foetal gender expectations and whether the pregnancy was planned) were influential factors in the occurrence of anxiety among women in their second pregnancies (p < 0.05). For details, see Table 3.
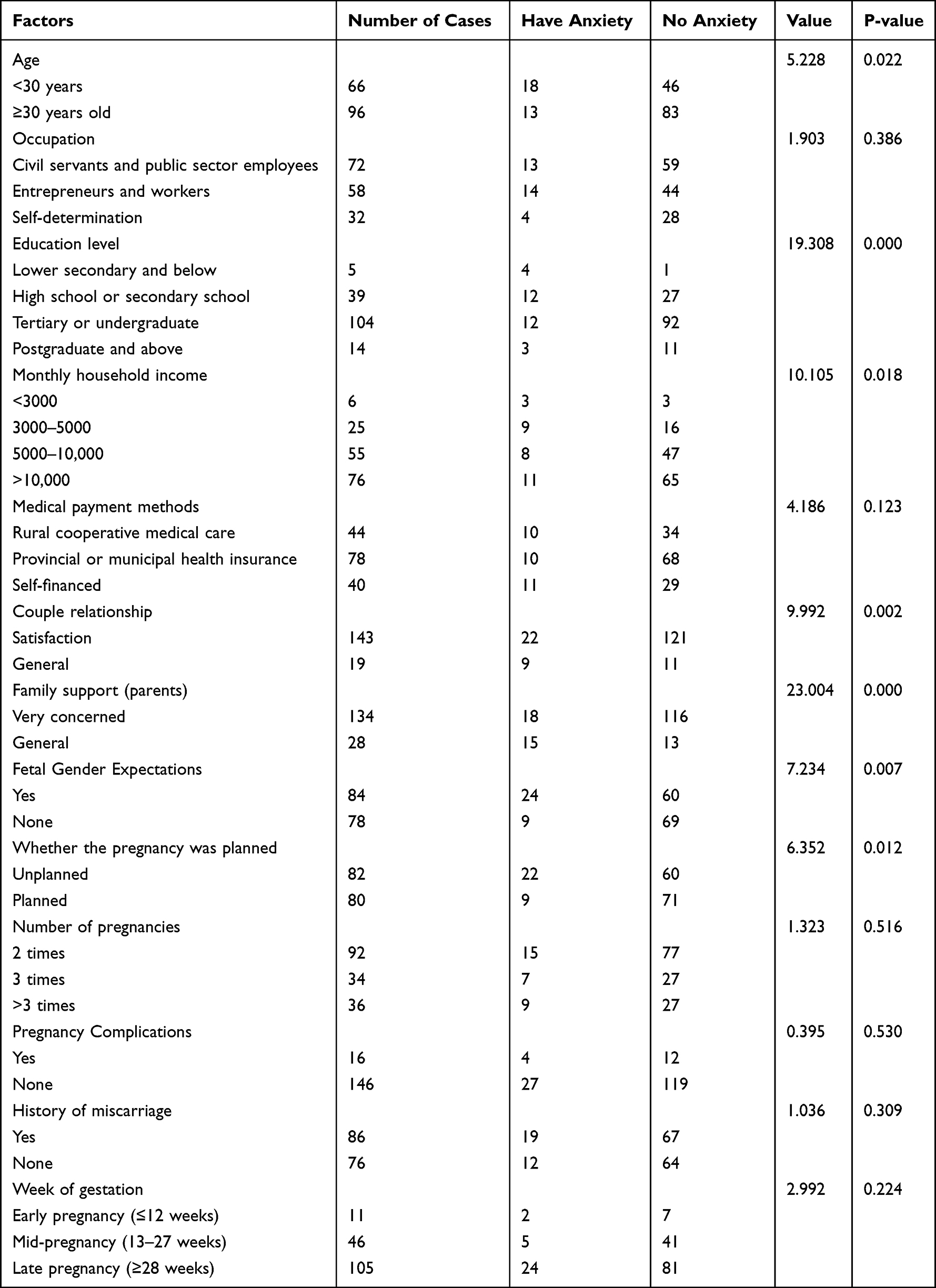 |
Table 3 One-Way Analysis of Factors Influencing Anxiety Among Pregnant Women with Second Birth [n (%)] |
Logistic Regression Analysis of Factors Influencing Anxiety
A multi-factor logistic regression analysis showed that four factors, namely low age, low education level, low monthly household income and having foetal gender expectations, were the main factors influencing anxiety among women during their second pregnancies (p < 0.05), as detailed in Table 4.
 |
Table 4 Logistic Regression Analysis of Factors Influencing Anxiety Among Second Pregnancy Women (n=162) |
One-Way Analysis of Factors Influencing Depression
A one-way analysis of factors influencing depression revealed that six factors, namely age, education level, monthly household income, the couple’s relationship, whether the pregnancy was planned and a history of miscarriage, influenced the occurrence of depression among women during their second pregnancies (p < 0.05). For details, see Table 5.
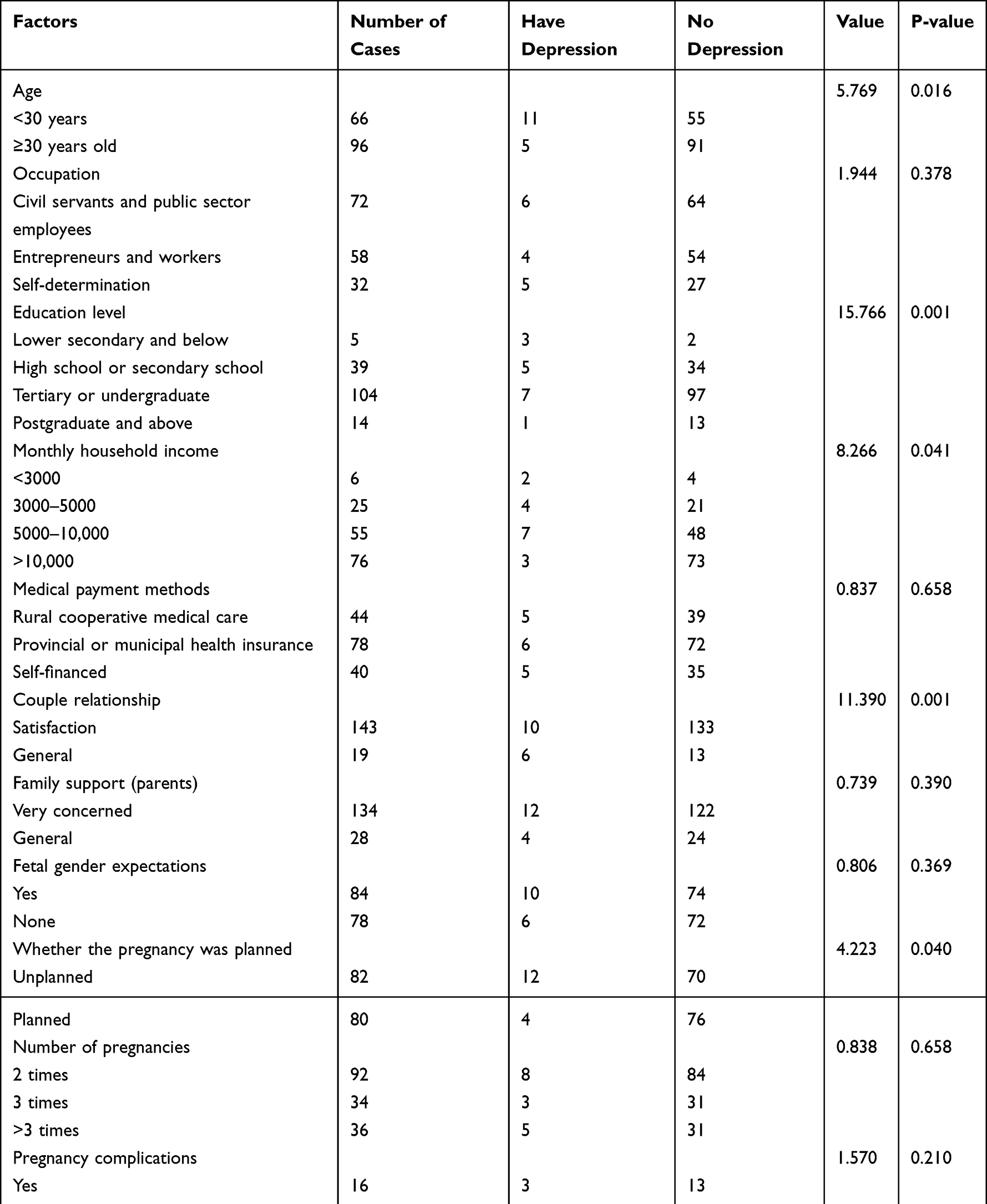 |
Table 5 One-Way Analysis of Factors Influencing Depression Among Second Pregnancy Women [n (%)] |
Logistic Regression Analysis of Factors Influencing Depression
A multi-factor logistic regression analysis showed that three factors, namely low education level, low monthly household income and the couple having a poor relationship, were the main factors influencing depression among women during their second pregnancies (p < 0.05), as detailed in Table 6.
 |
Table 6 Logistic Regression Analysis of Factors Influencing Depression in Pregnant Women with Second Birth (n=162) |
Discussion
Analysis of the Psychological Profile of Women During Their Second Pregnancies
The results of this study showed that the SAS score of women pregnant with their second child was 39.42 ± 7.18, which was statistically significant (p < 0.001) when compared with the domestic norm. Among these pregnant women, 31 (19.14%) experienced anxiety, of which 22 (13.58%) were mild, eight (4.94%) were moderate and one (0.62%) was severe. The SDS score (38.59 ± 9.61) for the subjects was statistically significant (p < 0.001) when compared with the domestic norm. Among these pregnant women, 16 (9.88%) experienced depression, of which 11 cases (13.58%) were mild and five cases (4.94%) were moderate. In this study, the incidence of anxiety and depression among women pregnant with their second child was higher than that of the domestic norm, and the detection rate was at a high level.
With the implementation of China’s two-child policy in 2016, the number of women having a second pregnancy has rapidly increased. Because the implementation of the one-child policy for many years led to increased costs and changes in the concept of child rearing, women pregnant with their second child face more pressure, including financial, psychological, familial and social, leading to varying degrees of psychological problems, such as anxiety and depression, and the quality of their sleep can be affected as well. Poor psychological status during pregnancy can lead to adverse outcomes such as preterm births, dystocia, low-birth-weight babies, gestational diabetes and hypertension, prolonged labour, antenatal and postpartum haemorrhage and postpartum depression.7,8 Therefore, the study of mental health in pregnant women has very important clinical implications.
According to the results of a survey, the financial cost of raising a child in an average family can be as high as 50% of the total household expenditure,9 which may be acceptable for families with only one child, but the financial burden of a second child may be too great. Women pregnant with their second child may also suffer from heavy career pressure and family responsibilities. Another major concern may be their children’s education, especially finding an apartment that is located near key schools or having a choice of elite schools; this gives families an even greater burden. The above-mentioned social problems plague many families with two children, causing a serious mental burden for women pregnant with their second child.10
Analysis of the Factors Influencing the Psychological Status of Women During Their Second Pregnancies
The results of this study indicated that four factors, namely low age, low education level, having foetal sex expectations and low monthly household income, were the main factors leading to anxiety among women pregnant with a second child. Of these, three factors, namely low education level, having a poor relationship with a partner and low monthly family income, were the main factors for depression.
Women pregnant with a second child at a young age may be more likely to suffer from anxiety due to their immature emotional development and their lack of mental capacity, as well as the fear that pregnancy will affect their work or even force them to give up their job. Older women are more likely to have stable financial resources and a certain social status and are more experienced in life and better prepared for pregnancy, which may result in a lower incidence of anxiety during their second pregnancies.11,12
The lower prevalence of anxiety and depression among more educated women pregnant with their second child compared to less educated ones may be attributed to the fact that more educated women are more knowledgeable about pregnancy and childbirth and are better prepared for the birth of their second child.13,14 It is also possible that more educated pregnant women are more aware of self-care, have more access to relevant information and ways of accessing it, are able to attend health check-ups regularly during pregnancy, are aware of and familiar with delivery and its potential complications through a variety of means and proactively seek multiple sources of social support.15
Monthly household income was also an influential factor. As monthly income per capita increases, anxiety and depression scores for women pregnant with a second child gradually decrease.16 In the current economic and educational environment, the financial burden of raising children is greater, especially for urban residents, who need to think more about education, medical care and the particularly high financial costs. This is even more of a concern when a woman has two children. A higher monthly household income and good economic conditions can provide good material support for women during their second pregnancies and provide a greater sense of security in the face of future uncertainties.17
The relationship between the couple is another influencing factor for depression during second pregnancy. Women pregnant with a second child are relatively older, as is the father, so the physical stress and risks of having a second child are higher, as is the financial and emotional burden of raising two children. Having a good relationship, with good moral and material support from the husband, can effectively stabilise the mood of a woman pregnant with a second child and reduce the development of negative emotions such as depression. Some studies have shown that positive words and actions from close family members can improve the mindset of pregnant women in stressful situations and help them maintain good moods.18 Therefore, informing the husband of the risks of another pregnancy to help him understand the stress caused by a second pregnancy, encouraging him to pay more attention to his wife’s emotional changes and creating a good family atmosphere will help to keep the pregnant woman in a good frame of mind.
With the implementation of the two-child policy, pregnant women and their family members have begun to expect to have a second child, and, due to traditional Chinese beliefs, some families expect to have both a son and a daughter. However, the emotional and material costs of raising two boys are higher than the costs of having one boy and one girl, and expectations about the sex of the foetus can cause psychological stress and anxiety in women pregnant with a second child.19 Therefore, health education for women during their second pregnancies should encourage the woman’s family members to take the initiative to help the women adjust and welcome the arrival of a new baby with a positive and relaxed attitude.20
Our study found that low age, low education level, having foetal sex expectations and low monthly household income were the main factors causing anxiety among women during their second pregnancy, which is of great value in guiding clinical practice. There were also some limitations. Firstly, the number of participants was small. Secondly, we have not developed systematic measures that can guide pregnant women with second pregnancies to improve pregnancy care.
Conclusion
In summary, with the implementation of the two-child policy, it is necessary to pay more attention to the psychological conditions of mothers before childbirth. Contacting mothers and babies as soon as possible after childbirth can relieve the physical and mental stress of mothers and effectively prevent the occurrence of postpartum depression. Women pregnant with their second child have varying degrees of anxiety and depression, and low age, low education level, having foetal sex expectations and a low monthly household income were the main factors leading to anxiety among the participants in this study. We suggest that effective targeted interventions are needed in clinical practice to alleviate women’s anxiety and depression and promote healthy delivery and healthy foetal growth.
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Hunan Provincial People’s Hospital. Written informed consent was obtained from all participants.
Funding
This work was supported by programe Foundation of Hunan Provincial Health commission (B20180681).
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Liu HY. Analysis on the influencing factors of postpartum depression in rural women in Doumen District of Zhuhai city and the prevention countermeasures. Chin Matern Chil Heal Care. 2017;32(14):3100–3102.
2. Du H, Liu CY, He Y, Liu XT, Dong J, He D. Research of prevalence and risk factors of postpartum depression. Chin J Fam Plan. 2013;21(5):321–323.
3. Zhang HJ, Sun J, Li F. Effects of adverse emotions such as anxiety and depression on pregnancy outcome in pregnant women. Clin Med Res Pract. 2017;2(17):85–86. doi:10.1016/j.diabres.2017.07.008
4. Gu SS, Qian Y, Chen H, Fu R, Wang FQ, Cheng JY. Status and related factors of postpartum depression in patients with second child. Chin J Woman Child Health Res. 2017;28(10). doi:10.3969/j.issn.1673-5293.2017.10.005
5. Zhou GL, Tan HT, Chen XW, et al. Analysis of the current status of postpartum depression symptoms and related influencing factors after the two-child policy; 2021.
6. Wang XX, Huang PZ, Xin H. A clinical study on the prevalence of breast hyperplasia and uterine fibroids and their correlation by ultrasound. Chin Med Guide. 2017;15(8):2.
7. Du L, Fan YF, Cai LQ, Liu TY, Guo QW. A case-control study of risk factors for the development of gestational diabetes mellitus. Chin J Perinat Med. 2014;17(8):5334–5336.
8. Wu LL, Hong H, Rao DL, Chen JW. Investigation and research on factors affecting the effect of re-birth for couples with two separate children. J Clin Ration Drug Use. 2018;11(2):171–172.
9. Li PL. Analysis on influencing factors of di rect economic cost of child rearing in a family. J Fujian Admin College. 2016;5:103–112.
10. Hu HQ, Zhang J, Zhao W, Tian T, Huang AQ, Wang LL. The occurrence and determinants of anxiety and depression symptoms in women of six counties/districts in China during pregnancy. Chin J Prev Med. 2017;51(1):47–52.
11. Leshchenko IA, Moglitsenko TM, Myl’Nikova IV. [Influence of sociopsychological factors on the health status of pregnant women, puerperants and newborn infants]. Probl Sotsialnoi Gig Zdravookhranenniiai Istor Med. 2002;4:23–25. Russian.
12. Li X, Liu JP. Investigation on the prenatal psychological status of pregnancy women with hypertensive disorder and its influence factors. Nurs Inegr Tradition Chin Western Med. 2015. doi:10.11997/nitcwm.201501044
13. Gulson B, Korsch M, Matisons M, Douglas C, Gillam L, McLaughlin V. Windblown lead carbonate as the main source of lead in blood of children from a seaside community: an example of local birds as “canaries in the mine”. Toxicol Lett. 2009;117(1):148–154. doi:10.1289/ehp.11577
14. Martini J, Petzoldt J, Einsle F, Beesdo-Baum K, Höfler M, Wittchen HU. Risk factors and course patterns of anxiety and depressive disorders during pregnancy and after delivery: a prospective-longitudinal study. J Affect Disord. 2015;175:385–395. doi:10.1016/j.jad.2015.01.012
15. Zou XY. Analysis of the choice and reasons of delivery methods in 2186 cases in Maoming City, Guangdong Province. J Guangdong Med Coll. 2011;29(4):443–445.
16. Berle J, Mykletun A, Daltveit AK, Rasmussen S, Holsten F, Dahl AA. Neonatal outcomes in offspring of women with anxiety and depression during pregnancy. Archiv Women Mental Health. 2005;8(3):181–189. doi:10.1007/s00737-005-0090-z
17. Tang Y, Feng Q, Cai Y. Analysis of the willingness of primiparous women to give birth and related influencing factors under the two-child policy. Chn Matern Child Health Res. 2016;18:22–23.
18. Jiang W. The impact of psychological nursing interventions on the emotional state of primiparous women. World Health Inform Digest. 2014;31:500–501.
19. Xu C. Effect of psychological care interventions on the improvement of psychological anxiety status in elderly second-trimester pregnant women. Chn Health Care Nutr. 2016;26(25):220–221.
20. Fellenzer JL, Cibula DA. Intendedness of pregnancy and other predictive factors for symptoms of prenatal depression in a population-based study. Matern Child Health J. 2014;18(10):2426–2436. doi:10.1007/s10995-014-1481-4
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Subjective Sleep Disruption and Mood Disorders are Associated with the Risk of Chronic Pain in Patients with Obstructive Sleep Apnea
Liu L, Li X, Xue P, Wu M, Zeng S, Dai Y, Zhou J
Nature and Science of Sleep 2022, 14:2023-2032
Published Date: 7 November 2022
Vitamin B12, Folate, Homocysteine, Inflammatory Mediators (Interleukin-6, Tumor Necrosis Factor-α and C-Reactive Protein) Levels in Adolescents with Anxiety or Depressive Symptoms
Tan Y, Zhou L, Huang J, Chen X, Wu Y, Song X, Wang J, Hu H, Yang Q
Neuropsychiatric Disease and Treatment 2023, 19:785-800
Published Date: 7 April 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Longitudinal Problematic Social Media Use in Students and Its Association with Negative Mental Health Outcomes
Shannon H, Bush K, Shvetz C, Paquin V, Morency J, Hellemans KGC, Guimond S
Psychology Research and Behavior Management 2024, 17:1551-1560
Published Date: 8 April 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025