Back to Journals » Psoriasis: Targets and Therapy » Volume 12
Psoriasis and Exercise: A Review
Authors Yeroushalmi S, Hakimi M, Chung M, Bartholomew E ![]() , Bhutani T
, Bhutani T ![]() , Liao W
, Liao W ![]()
Received 31 March 2022
Accepted for publication 11 June 2022
Published 2 July 2022 Volume 2022:12 Pages 189—197
DOI https://doi.org/10.2147/PTT.S349791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Uwe Wollina
Samuel Yeroushalmi, Marwa Hakimi, Mimi Chung, Erin Bartholomew, Tina Bhutani, Wilson Liao
Department of Dermatology, University of California, San Francisco, CA, USA
Correspondence: Wilson Liao, Email [email protected]
Abstract: Psoriasis is a prevalent inflammatory skin disorder that is associated with a number of comorbidities including cardiovascular disease and metabolic syndrome. Exercise can influence the outcomes of chronic inflammatory diseases, and the presence of these diseases can also influence physical activity in afflicted patients. We reviewed the available literature published on exercise in psoriasis patients and aimed to explore physical activity levels, barriers to exercise, physical fitness, exercise as a prevention strategy as well as a treatment modality. Overall, patients with moderate to severe psoriasis are more sedentary than the general population and experience barriers to exercise secondary to their skin disease. Moderate to vigorous exercise may be an independent preventative factor in reducing the incident risk of developing psoriasis and the utilization of exercise as a weight loss strategy may improve disease severity especially in overweight patients. Expert panels agree that exercise can be beneficial as an adjunct treatment in patients with psoriasis who are overweight; however, more randomized clinical trials are needed to establish these links.
Keywords: physical activity, weight loss, lifestyle
Introduction
Psoriasis is a chronic inflammatory disease that presents with a range of severities and varying levels of debilitation. In addition to the burdens patients face from skin disease, psoriasis is associated with a number of comorbidities. These include, but are not limited to, other disorders associated with systemic inflammation such as psoriatic arthritis, inflammatory bowel disease, cardiovascular disease, and metabolic syndrome.1
Similar to other systemic diseases, the risk of developing psoriasis is associated with body weight. High body mass index (BMI) and elevated body fat are both associated with an increased risk of developing psoriasis.2,3 Adipose tissue possesses endocrine functionalities and has been shown to produce pro-inflammatory adipokines such as leptin and resistin, as well as pro-inflammatory cytokines like TNF-alpha and IL-6.4,5 In cardiovascular disease, physical activity is a well-known lifestyle factor that can favorably modulate disease outcomes and even prevent disease onset.6 Patients with inflammatory or immune-mediated conditions like multiple sclerosis, type 1 diabetes, and rheumatoid arthritis tend to be less active than the general population, even though physical activity can improve disease course and improve quality of life.7 Physical activity has been shown to provide many mental health benefits such as improvement of mood which can be impactful for patients with psoriasis who are at a higher risk of having depression.8,9 Exercise has even been shown to improve diseases outcomes as well as comorbidities for patients who have psoriatic arthritis.10 These benefits of exercise can be attributed to many mechanisms, not only through adipose tissue reduction but also a possible decrease in oxidative stress which may drive lesion production that is seen in psoriasis.11,12 A previous review by Wilson et al examined nine studies that focused on physical activity in psoriasis patients and concluded that exercise could be a potentially effective treatment for comorbid conditions in psoriasis.13 This review was limited by the number of studies as well as lack of clinical trials, however.
In this review, we aim to review published literature on the relationship between exercise and psoriasis. We chose to focus on the relationship between physical activity and psoriasis itself as a primary aim rather than the impact of physical activity on its comorbidities (eg, metabolic syndrome, cardiovascular disease, etc.). We also aimed to include a wide array of study types describing any potential bidirectional relationship between psoriasis and physical activity. This includes studies that examine the epidemiology of exercise in psoriasis patients and the level of physical activity patients with psoriasis engage compared to non-psoriatic patients. Barriers to exercise in patients with psoriasis will also be reviewed as well as any possible differences in physical fitness from those who do not have psoriasis. Finally, exercise as a preventative measure against psoriasis as well as a treatment modality will be discussed.
Methods
We aimed to include all clinical trials as well as observational studies (case-control, cohort, and cross-sectional) published in English which included patients with psoriasis and evaluated exercise and physical activity. PubMed and Embase databases were searched on December 9th, 2021 using the criteria:
(“physical activity” OR exercise) AND psoriasis.
Title and abstract review were conducted independently by SY and MH. Studies which included mention of psoriasis, psoriatic arthritis, or inflammatory skin disease and exercise or physical activity were marked for full-text review. Studies which were deemed irrelevant on title and abstract screening were excluded. Conflicts were resolved by adjudication between the two authors. Publications which were successfully screened for full text review were independently screened again by SY and MH, with conflicts resolved by adjudication between the two authors. For the purposes of this review, only full text, peer reviewed articles were included in the final inclusion of studies. One thousand eighty-six articles in total were found from our literature search, and 28 studies were included for review (Figure 1).14 Due to study heterogeneity, a meta-analysis was not performed.
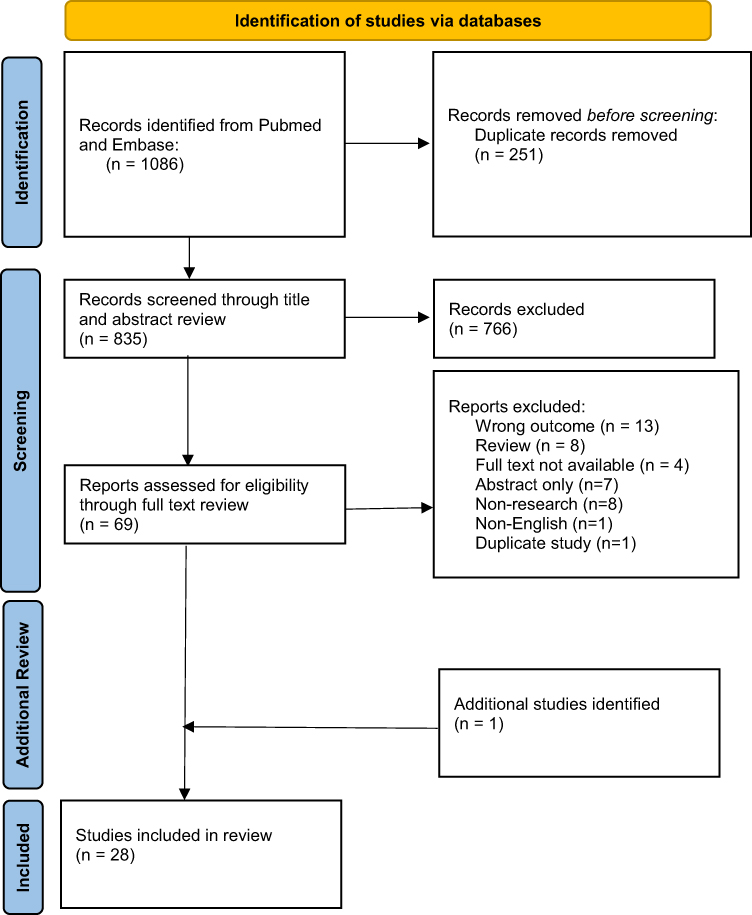 |
Figure 1 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram for selection of studies. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuy PM, et al. The PRISMA. Statement: an updated guideline for reporting systematic reviews. BMJ. 2020 Creative Commons.14 |
Physical Activity in Psoriasis Patients
The Centers for Disease Control and Prevention (CDC) recommends that Americans get 150 minutes of moderate-intensity aerobic exercise per week.15 However, only 53.3% of adults in the United States actually met these guidelines as of 2018. As psoriasis is a known risk factor for cardiovascular disease,16 it is important to identify the level and intensity of exercise for psoriasis patients. Overall, observational trials on the level of exercise in psoriasis patients show that psoriasis patients exercise less often and less intensely than those without psoriasis.
Several large observational cross-sectional and cohort studies have shown that patients with psoriasis participate in less physical activity than non-psoriatic patients. For instance, an online cross-sectional survey of 9940 psoriasis patients in Germany found that severe psoriasis was associated with impairment of physical activity and that only 21.2% were currently exercising with the intent of losing weight, even though 66.9% had a body mass index (BMI) greater than 25.17 Similarly, an analysis of 2011–2014 National Health and Nutrition Examination NHANES data of 9174 total patients and 232 patients with psoriasis showed that those with psoriasis were significantly less likely to engage in vigorous exercise compared to those who do not have psoriasis (16.1% vs 28%, p = 0.042).18 Another study examining NHANES data from 2003 to 2006 on a total of 6549 people aged 20–59 found that the amount of time spent on sports between patients with psoriasis and healthy patients was not significantly different; however, the metabolic equivalent tasks (METs) were 31% less in patients with psoriasis (95% CI:-0.57 to −0.05).19 A major limitation of these studies was that they did not report the prevalence of comorbid psoriatic arthritis, which may reduce physical activity in such patients.
Several smaller, controlled survey studies also showed that patients with psoriasis are generally less active than non-psoriatic patients. Torres et al administered 90 patients with severe plaque psoriasis and 160 matched healthy controls with the International Physical Activity Questionnaire (IPAQ) and found that there were significantly reduced activity levels of psoriatic patients compared to controls.20 Another survey study conducted by Deniz et al administered the Health-Promoting Lifestyle Profile II (HPLP-II) survey to 80 patients with psoriasis and 80 controls and concluded that psoriatic patients are less likely to take part in light-moderate physical activity such as sustained walking (p < 0.05).21 Nowowiejska et al recently published findings from a cross-sectional study of 56 hospitalized psoriasis patients and 36 matched controls and showed that patients with psoriasis exercised significantly less in terms of MET-min/week as compared to controls (p < 0.01).22 A major limitation of this study was the use of hospitalized patients which could have an associated with reduced exercise levels. The small sample sizes of these studies also limit the meaningfulness of the evidence presented but overall these results do mirror that of the larger cross-sectional studies described previously.
Multiple non-controlled survey studies also examined the prevalence and levels of exercise in psoriasis patients and similarly found reduced physical activity levels. For instance, a survey of 262 patients with psoriasis conducted by Leino et al found that 30.2% of patients had completely given up sports and 23.7% had reduced their sports activities.23 Another Polish multicenter survey-based study of 211 patients with psoriasis found that about 75% of patients exercised less than 30 minutes per day (most commonly 1–2 hours per week) which typically consisted of walking or cycling.24 The level of physical activity in psoriasis patients may also be dependent on disease severity. According to a cross-sectional survey study of 330 patients with mild to severe psoriasis in Kuwait, sporting activities were significantly decreased (p < 0.01) in patients with moderate to severe psoriasis compared to mild patients.25 Because of the cross-sectional design of these studies, causality cannot be directly inferred. A survey study by Lewis-Beck et al, however, examined 199 patients with moderate-severe psoriasis, of which 72% of reported impaired physical activity directly due to their psoriasis.26 Though these non-controlled studies can shed light on the impact of disease severity within the psoriasis population, a lack of a healthy comparator prevents limits more meaningful conclusions.
Most studies examined here found some level of reduced physical activity or exercise in patients with psoriasis, however, a small case control study of 65 psoriasis patients and 52 controls found no significant difference in exercise (p = 0.06) as determined by the Godin Leisure-Time Exercise Questionnaire.27
Exercise Barriers in Psoriasis Patients
As previously discussed, patients with psoriasis do not engage in as much physical activity compared to non-psoriatic patients. Low levels of exercise may potentially be a risk factor for psoriasis, as discussed later, but patients who have psoriasis also experience a number of barriers that may limit their physical activity.
One survey of 104 patients with severe psoriasis reported that 40% avoided sports because of their psoriasis alone.28 An analysis of 2003–2006 NHANES data that included 117 psoriasis patients did not find a correlation between body surface area (BSA) involvement and physical activity; however, they did find an inverse correlation with how badly patients rated their own psoriasis and the amount of moderate or vigorous physical activity they participated in.29 This suggests that patients’ own perception of disease severity influences their engagement in exercise.
A cross-sectional study of 378 psoriasis patients found that overall quality of life as measured by the Dermatology Life Quality Index (DLQI) disease was negatively correlated with level of exercise. Specifically, soreness or itch, influence of skin on clothing, the effect of skin on leisure activities and difficulty in managing disease were all associated with less exercise engagement.30 Another cross-sectional study of 404 patients with psoriasis also showed that over half engage in less than the recommended amount of exercise; reported barriers included skin sensitivity and reluctance to engage in leisurely activity.31 Patients with psoriasis have also been shown to also experience increased pruritus when they exercise, further increasing their discomfort.32 As with other questionnaire-based studies, recall bias can greatly influence the results and the heterogeneity of questionnaires in addition to lack of standardized physical evaluation makes comparison results between studies difficult.
Aside from quality of life and patient discomfort, psoriasis may also present physiologic barriers to exercise. One study of 16 men with psoriasis and ten controls showed that those with psoriasis were less efficient at dissipating heat and had reduced sweating over a two hour exercise test and thus had a higher risk for heat intolerance.33 More studies with larger patient groups are needed to determine if this finding is replicable.
Physical Fitness in Psoriasis Patients
Psoriasis may have an impact on the physical fitness of afflicted patients, although there is a dearth of literature examining this relationship. It is known that patients with moderate to severe psoriasis are more likely to be overweight, and thus it can be difficult to assume any causality on the impact of physical fitness as a result of the disease severity on its own.34
For instance, an experimental study in which 50 patients with psoriasis and 32 healthy controls were subjected to stress testing showed that those with psoriasis had a significantly lower heart rate recovery index that was correlated with disease duration (p < 0.001) and severity (p < 0.001). An important limitation of this study, however, was that the two groups may not have been matched with regard to physical fitness, thus inferring a relationship directly as a result of the disease state may not be appropriate.35 In another experimental study of psoriasis patients with BSA greater than 5% and healthy controls, patients were monitored with accelerometers for a one-week period as well as completed self-paced 20-minute treadmill bouts. The study found that patients with severe psoriasis participated in less day-to-day vigorous activity as well as chose slower speeds on the treadmill exercises possibly due to fear of increasing pruritus.32 This implies that a barrier to exercise such as discomfort during exercise may reduce physical fitness of these patients rather than the disease itself.
Two other studies did not find any meaningful difference in fitness of psoriasis patients compared to non-psoriatic patients. One study of patients with moderate psoriasis and healthy controls evaluated various physical parameters such as maximum aerobic capacity, body fat percentage, pulmonary function testing, and body fat measurement. This study found no significant difference in any of these parameter between diseased and healthy patients, suggesting that psoriasis does not play a major role in impacting fitness.36 In a survey of 66 psoriasis patients and 52 controls with other skin disorders (atopic dermatitis, vitiligo, etc.) psoriasis did not seem to impact exercise activities as no significant difference in composite exercise scores between the two groups.37
Exercise for Prevention of Psoriasis
It is well established that regular exercise reduces fat mass, which can subsequently reduce its contribution to systemic inflammation.38 This begs the question of whether psoriasis, as a chronic inflammatory skin disease, can be prevented by regular exercise. Indeed, a considerable amount of evidence exists supporting the notion that exercise may in fact reduce the incident risk of developing psoriasis. Observational studies examining the risk of developing psoriasis and exercise are summarized and are appraised for quality in Table 1.
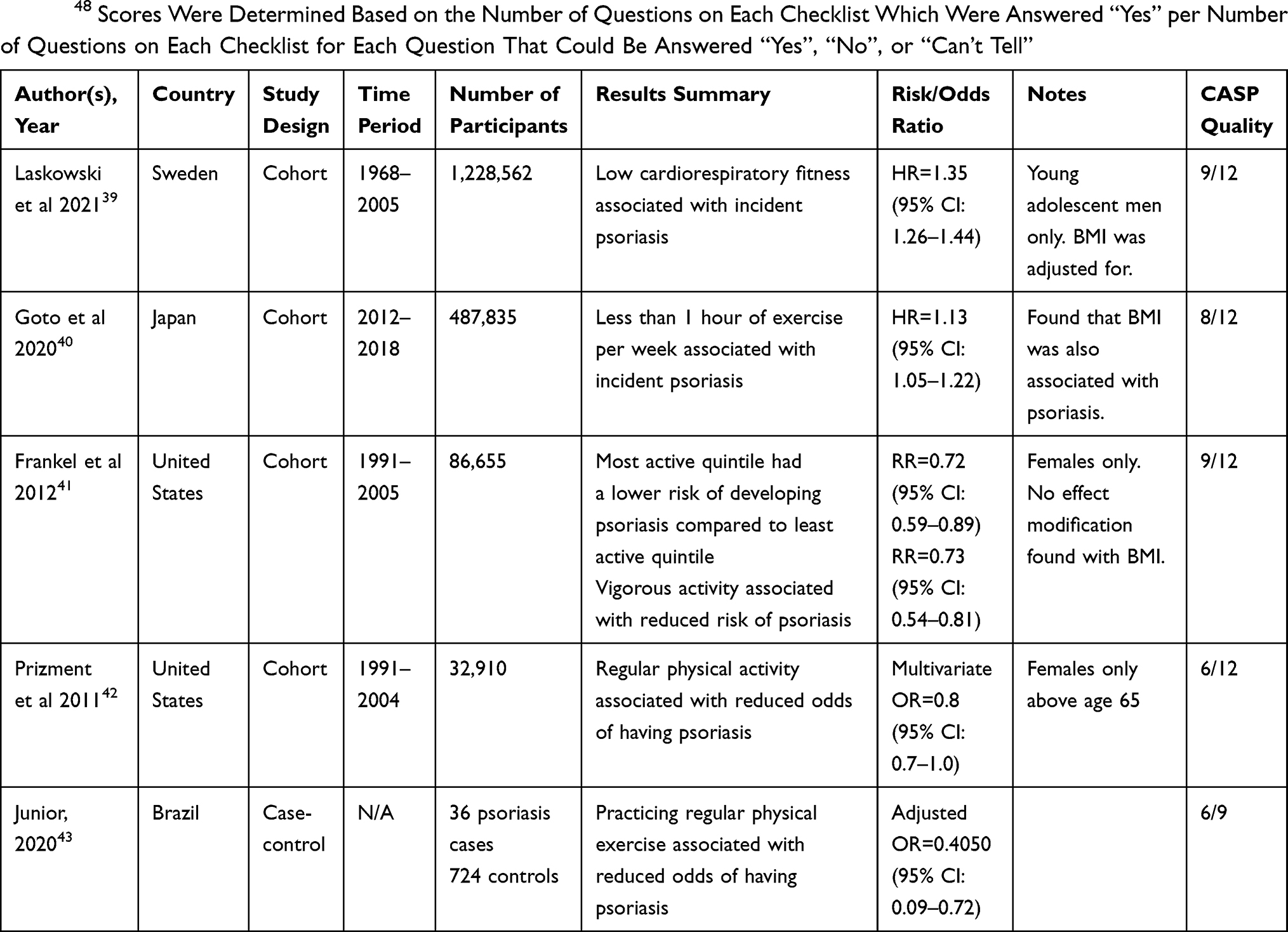 |
Table 1 Summary of Observational Studies Examining Risk or Odds of Developing Psoriasis with Respect to Levels of Physical Activity. Study Quality Was Assessed Using the Critical Appraisal Skills Programme (CASP) Checklists for Cohort and Cross-Sectional Studies.48 Scores Were Determined Based on the Number of Questions on Each Checklist Which Were Answered “Yes” per Number of Questions on Each Checklist for Each Question That Could Be Answered “Yes”, “No”, or “Can’t Tell” |
Several major cohort studies have found an inverse relationship between the level of physical activity and this incident risk. A cohort study by Laskowski et al of 1,228,562 Swedish men in compulsory military service between 1968 and 2005 which included 20,679 cases of psoriasis found that there was a statistically significant association between cardiorespiratory fitness assessed by bicycle ergonomic testing and the incidence of psoriasis (HR: 1.35, 95% CI:1.26–1.44). It should be noted that their analysis adjusted for BMI, however only young adolescent men were enrolled.39 A Japanese prospective survey study of 487,835 patients, of which 2793 (0.57%) developed moderate-severe psoriasis, also showed that not exercising for at least one hour per week was associated with developing moderate-severe psoriasis (HR: 1.13, 95% CI: 1.05–1.22).40 Another large prospective study by Frankel et al of 86,665 females found an inverse relationship between overall physical activity and the risk of developing psoriasis (RR = 0.72, 95% CI: 0.59–0.89) between the most active and least active quintile. Vigorous activity, which was defined as >6 metabolic equivalents, also was associated with a reduced risk of developing psoriasis (RR = 0.66, 95% CI 0.54–0.81) while walking showed no reduction of risk. The authors of this study also found that BMI was not an effective modifier in their analysis, suggesting exercise could play an independent role in reducing risk of psoriasis independently from weight.41 Though this study was highly powered, its all-female cohort does not represent the typical demographic of psoriasis patients.24 Finally, a prospective questionnaire administered to 32,910 women from above the age of 65 found that regular physical activity was associated with a lower risk of incident psoriasis (adjusted RR = 0.80, 95% CI: 0.70–1.0).42 Once again, the generalizability of this study is limited given the restriction on the study population examined. Overall, the consistency between these large observational studies suggests that more vigorous exercise is associated with a reduced risk of developing psoriasis, while lower intensity physical activity is not as protective.
Smaller observational studies have similarly demonstrated the inverse relationship between exercise intensity and the presence of psoriasis. A Brazilian case control study which included 36 patients with psoriasis and 724 controls showed regular exercise by the World Health Organization (WHO) recommended standards was associated with a reduced adjusted OR (OR = 0.41, 95% CI: 0.09–0.72) of having psoriasis.43 This study did not account for confounding factors such as BMI, however. A cross-sectional study of 323 Italian second league soccer players and 357 matched controls found that only 1.6% of soccer players had psoriasis compared to 4.5% of controls (p < 0.05). Of the controls, there was a higher prevalence of psoriasis (15/296, 5.1%) in those who did not perform regular physical activity compared to those who did (1/61, 1.6%) (p < 0.05).44 These data may also support the notion that more intense physical exercise can reduce the risk of developing psoriasis; however, as previously discussed, the cross-sectional design does limit interpreting the direction of causality.
Exercise as Treatment/Management
There is very limited literature examining exercise as a potential treatment strategy for psoriasis patients. In our literature search, only one randomized controlled trial by Naldi et al examined the effect of exercise in patients who already had psoriasis. The trial, consisting of 303 overweight or obese psoriasis patients with a Psoriasis Area Severity Score (PASI) >10, randomized subjects to either a 20-week exercise program (aerobic exercise for at least 40 minutes, three times a week) and dietary intervention with a goal of 5% weight reduction, or simple informative counseling. The study found that patients who were randomized to the exercise program experienced a 48% reduction in PASI compared to a 25.5% reduction in PASI in the control group (p = 0.02).45 The design of this study does limit the generalization of its results, however. Almost one-third of psoriasis patients who participated in exercise also lost weight, and since they were also placed on a diet, these may be confounding factors that contributed to disease improvement, rather than exercise alone. It cannot be determined whether this benefit would apply to patients with lower BMI either, since only overweight or obese patients were enrolled. Patients were also allowed to continue other treatments during study duration, which may have contributed to PASI improvement too.
Discussion
As discussed above, there is a bidirectional relationship between physical activity and psoriasis. Psoriasis has an influence on how patients exercise, and exercise may also influence disease outcomes for patients with psoriasis. This is similar to the relationship between exercise and cardiovascular disease and metabolic syndrome. The effect of exercise in psoriasis may be in part due to decreases in adipose tissue, which can release inflammatory cytokines, but may also be possibly due to the direct effects of exercise itself.38 Adiposity has been shown to increase levels of several key cytokines involved in the pathogenesis of psoriasis such as TNF-alpha, and can induce Th17 cells that produce IL-17.34 This cytokine imbalance provides some explanation as to why obesity is a risk factor for psoriasis. Therefore, decreased exercise and obesity is likely to play a causative role in the induction of psoriasis. This is supported by the number of observational studies demonstrating the reduced risk of incident psoriasis in those with higher exercise levels.
However, psoriasis may also limit physical activity in patients due to physical discomfort and pruritus experienced while exercising. Psoriasis can also cause embarrassment and create self-conscious feelings associated with exercise, limiting patient’s motivation to engage in physical activity. Given that exercise may also psoriasis in patients’ disease severity in psoriasis patients, these obstacles can hamper patients’ ability to treat their disease with lifestyle modifications. In fact, in a two round Delphi study, which included a panel of dermatologists and rheumatologists to generate recommendations to manage moderate-severe psoriasis and psoriatic arthritis, 76% agreed that moderate-severe psoriasis patients who were obese should initiate lifestyle changes aimed at reducing 5–10% body weight, involving both diet and aerobic and muscle strengthening exercises. All panelists agreed patients should do aerobic exercises as often as possible and strengthening exercises every other day.46 Additionally, a joint-guideline review between the Journal of the Academy of Dermatology and the National Psoriasis Foundation published in 2019 recommended that dermatologists should counsel their patients on lifestyle changes that include regular exercise in order to reduce the risk of associated comorbidities such as metabolic syndrome.47
In conclusion, patients with moderate to severe psoriasis may be more sedentary than the general population and may experience a number of barriers with regard to participating in exercise. Exercise may be an effective preventative strategy against psoriasis and can potentially improve the disease in patients who are also overweight. Physicians should be aware of these findings in order to appropriately counsel their patients who are interested in focusing on lifestyle changes which can improve the outcomes of their skin health.
A major limitation of this review is the lack of randomized controlled trials which examine the effect of physical activity on psoriasis, which limits our ability to draw conclusions related to causality. Most studies evaluated in this review also did not include patients with mild disease. Additionally, many studies also examined patients who were overweight or obese, which may have been a confounding factor in evaluating physical activity’s impact on psoriasis separately from changes in weight which are influenced by other factors such as diet. More mechanistic studies are needed to determine the physiologic effects exercise has on patients who have psoriasis.
Funding
There is no funding to report.
Disclosure
Tina Bhutani is a principal investigator for trials sponsored by AbbVie, Castle, CorEvitas, Dermavant, Galderma, Mindera, and Pfizer. She has received research grant funding from Novartis and Regeneron. She has been an advisor for AbbVie, Arcutis, Boehringer-Ingelheim, Bristol Myers Squibb, Janssen, Leo, Lilly, Novartis, Pfizer, Sun, and UCB. Wilson Liao has received research grant funding from AbbVie, Amgen, Janssen, Leo, Novartis, Pfizer, Regeneron, and TRex Bio. The authors report no other conflicts of interest in this work.
References
1. de Oliveira M, de Rocha FSP, Duarte GV. Psoriasis: classical and emerging comorbidities. An Bras Dermatol. 2015;90(1):9–20. doi:10.1590/abd1806-4841.20153038
2. Setty AR, Curhan G, Choi HK. Obesity, waist circumference, weight change, and the risk of psoriasis in women: nurses’ health study II. Arch Intern Med. 2007;167(15):1670–1675. doi:10.1001/archinte.167.15.1670
3. Snekvik I, Smith CH, Nilsen TIL, et al. Obesity, waist circumference, weight change, and risk of incident psoriasis: prospective data from the HUNT study. J Invest Dermatol. 2017;137(12):2484–2490. doi:10.1016/j.jid.2017.07.822
4. Cao H. Adipocytokines in obesity and metabolic disease. J Endocrinol. 2014;220(2):T47–T59. doi:10.1530/JOE-13-0339
5. Versini M, Jeandel PY, Rosenthal E, Shoenfeld Y. Obesity in autoimmune diseases: not a passive bystander. Autoimmun Rev. 2014;13(9):981–1000. doi:10.1016/j.autrev.2014.07.001
6. Nystoriak MA, Bhatnagar A. Cardiovascular effects and benefits of exercise. Front Cardiovasc Med. 2018;5:135. doi:10.3389/fcvm.2018.00135
7. Sharif K, Watad A, Bragazzi NL, Lichtbroun M, Amital H, Shoenfeld Y. Physical activity and autoimmune diseases: get moving and manage the disease. Autoimmun Rev. 2018;17(1):53–72. doi:10.1016/j.autrev.2017.11.010
8. Knapen J, Vancampfort D, Moriën Y, Marchal Y. Exercise therapy improves both mental and physical health in patients with major depression. Disabil Rehabil. 2015;37(16):1490–1495. doi:10.3109/09638288.2014.972579
9. Sahi FM, Masood A, Danawar NA, Mekaiel A, Malik BH. Association between psoriasis and depression: a traditional review. Cureus. 2020;12(8):e9708. doi:10.7759/cureus.9708
10. Kessler J, Chouk M, Ruban T, Prati C, Wendling D, Verhoeven F. Psoriatic arthritis and physical activity: a systematic review. Clin Rheumatol. 2021;40(11):4379–4389. doi:10.1007/s10067-021-05739-y
11. Vanizor Kural B, Orem A, Cimşit G, Yandi YE, Calapoglu M. Evaluation of the atherogenic tendency of lipids and lipoprotein content and their relationships with oxidant-antioxidant system in patients with psoriasis. Clin Chim Acta. 2003;328(1–2):71–82. doi:10.1016/S0009-8981(02)00373-X
12. Hollander J, Fiebig R, Gore M, Ookawara T, Ohno H, Ji LL. Superoxide dismutase gene expression is activated by a single bout of exercise in rat skeletal muscle. Pflugers Arch. 2001;442(3):426–434. doi:10.1007/s004240100539
13. Wilson PB, Bohjanen KA, Ingraham SJ, Leon AS. Psoriasis and physical activity: a review. J Eur Acad Dermatol Venereol. 2012;26(11):1345–1353. doi:10.1111/j.1468-3083.2012.04494.x
14. Page MJ, McKenzie JE, Bossuy PM, et al. The PRISMA. Statement: an updated guideline for reporting systematic reviews. BMJ. 2020. Available from: https://www.bmj.com/content/372/bmj.n71.
15. CDC. Move more; sit less. Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/physicalactivity/basics/adults/index.htm.
16. Hu SCS, Lan CCE. Psoriasis and cardiovascular comorbidities: focusing on severe vascular events, cardiovascular risk factors and implications for treatment. Int J Mol Sci. 2017;18(10):2211. doi:10.3390/ijms18102211
17. Schwarz PEH, Pinter A, Melzer N, Barteczek P, Reinhardt M. ERAPSO: revealing the high burden of obesity in German psoriasis patients. Dermatol Ther (Heidelb). 2019;9(3):579–587. doi:10.1007/s13555-019-0314-1
18. Wilson PB. Prevalence of weight loss attempts and behaviors used by individuals with psoriasis in the United States population. J Dermatol Treat. 2017;28(6):515–519. doi:10.1080/09546634.2016.1277180
19. Do YK, Lakhani N, Malhotra R, Halstater B, Theng C, Østbye T. Association between psoriasis and leisure-time physical activity: findings from the national health and nutrition examination survey. J Dermatol. 2015;42(2):148–153. doi:10.1111/1346-8138.12721
20. Torres T, Alexandre JM, Mendonça D, Vasconcelos C, Silva BM, Selores M. Levels of physical activity in patients with severe psoriasis: a cross-sectional questionnaire study. Am J Clin Dermatol. 2014;15(2):129–135. doi:10.1007/s40257-014-0061-0
21. Deniz F, Altunay IK, Ozkur E, Cerman AA, Erdogan HK, Bulur I. Evaluation of healthy lifestyle behaviors in psoriasis patients. Sisli Etfal Hastan Tip Bul. 2021;55(2):197–202. doi:10.14744/SEMB.2020.01799
22. Nowowiejska J, Baran A, Grabowska P, Lewoc M, Kaminski TW, Flisiak I. Assessment of life quality, stress and physical activity among patients with psoriasis. Dermatol Ther (Heidelb). 2022;12(2):395–406. doi:10.1007/s13555-021-00662-1
23. Leino M, Mustonen A, Mattila K, Koulu L, Tuominen R. Perceived impact of psoriasis on leisure-time activities. Eur J Dermatol. 2014;24(2):224–228. doi:10.1684/ejd.2014.2282
24. Pankowski D, Janowski K, Owczarek W, Borzęcki A. Sociodemographic variables, health-related behaviors, and disease characteristics in patients with psoriasis. Fam Med Prim Care Rev. 2018;20(2):149–153. doi:10.5114/fmpcr.2018.76459
25. Al-Mazeedi K, El-Shazly M, Al-Ajmi HS. Impact of psoriasis on quality of life in Kuwait. Int J Dermatol. 2006;45(4):418–424. doi:10.1111/j.1365-4632.2006.02502.x
26. Lewis-Beck C, Abouzaid S, Xie L, Baser O, Kim E. Analysis of the relationship between psoriasis symptom severity and quality of life, work productivity, and activity impairment among patients with moderate-to-severe psoriasis using structural equation modeling. Patient Prefer Adherence. 2013;7:199–205. doi:10.2147/PPA.S39887
27. Ahdout J, Kotlerman J, Elashoff D, Kim J, Chiu MW. Modifiable lifestyle factors associated with metabolic syndrome in patients with psoriasis. Clin Exp Dermatol. 2012;37(5):477–483. doi:10.1111/j.1365-2230.2012.04360.x
28. Ramsay B, O’Reagan M. A survey of the social and psychological effects of psoriasis. Br J Dermatol. 1988;118(2):195–201. doi:10.1111/j.1365-2133.1988.tb01774.x
29. Wilson PB. Moderate-to-vigorous physical activity in individuals with psoriasis: associations with body surface area and subjective disease severity. G Ital Dermatol Venereol. 2013;148(5):485–492.
30. Auker L, Cordingley L, Kane K, Griffiths C, Young H. Dermatology life quality index: a potential marker of exercise engagement in patients with psoriasis. Br J Dermatol. 2014;171(6):e146–e147. doi:10.1111/bjd.13488
31. Auker L, Cordingley L, Pye SR, Griffiths CEM, Young HS. What are the barriers to physical activity in patients with chronic plaque psoriasis?*. Br J Dermatol. 2020;183(6):1094–1102. doi:10.1111/bjd.18979
32. Enos C, Algrni K, Van Voorhees A, Wilson P. Physical activity engagement and responses to exercise in plaque psoriasis: a multifactorial investigation of influential factors. J Dermatol Treat. 2020;33:805–811. doi:10.1080/09546634.2020.1781756
33. Leibowitz E, Seidman DS, Laor A, Shapiro Y, Epstein Y. Are psoriatic patients at risk of heat intolerance? Br J Dermatol. 1991;124(5):439–442. doi:10.1111/j.1365-2133.1991.tb00622.x
34. Jensen P, Skov L. Psoriasis and obesity. Dermatology. 2016;232(6):633–639. doi:10.1159/000455840
35. Sarli B, Dogan Y, Baktir AO, et al. Heart rate recovery is impaired in patients with psoriasis. Med Princ Pract. 2013;22:567–570. doi:10.1159/000351884
36. Demirel R, Genc A, Ucok K, et al. Do patients with mild to moderate psoriasis really have a sedentary lifestyle? Int J Dermatol. 2013;52(9):1129–1134. doi:10.1111/ijd.12042
37. Ahdout J, Kim J, Chiu M. Modifiable metabolic syndrome-associated lifestyle factors in psoriasis patients. J Am Acad Dermatol. 2009;60(3):AB169. doi:10.1016/j.jaad.2008.11.737
38. Gleeson M, Bishop NC, Stensel DJ, Lindley MR, Mastana SS, Nimmo MA. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol. 2011;11(9):607–615. doi:10.1038/nri3041
39. Laskowski M, Schiöler L, Gustafsson H, Wennberg AM, Åberg M, Torén K. Cardiorespiratory fitness in late adolescence and long-term risk of psoriasis and psoriatic arthritis among Swedish men. PLoS One. 2021;16(1):e0243348. doi:10.1371/journal.pone.0243348
40. Goto H, Nakatani E, Yagi H, Moriki M, Sano Y, Miyachi Y. Late-onset development of psoriasis in Japan: a population-based cohort study. JAAD Int. 2021;2:51–61. doi:10.1016/j.jdin.2020.10.011
41. Frankel HC, Han J, Li T, Qureshi AA. The association between physical activity and the risk of incident psoriasis. Arch Dermatol. 2012;148(8):918–924. doi:10.1001/archdermatol.2012.943
42. Prizment AE, Alonso A, Folsom AR, et al. Association between psoriasis and incident cancer: the Iowa’s women’s health study. Cancer Causes Control. 2011;22(7):1003–1010. doi:10.1007/s10552-011-9773-0
43. Júnior DST. Environmental and individual factors associated with protection and predisposition to autoimmune diseases. Int J Health Sci. 2020;14(6):13–23.
44. Megna M, Lobasso A, Napolitano M, et al. Soccer helps in controlling the development of psoriasis in Italian second league players. J Eur Acad Dermatol Venereol. 2017;31(4):e212–e214. doi:10.1111/jdv.13971
45. Naldi L, Conti A, Cazzaniga S, et al. Diet and physical exercise in psoriasis: a randomized controlled trial. Br J Dermatol. 2014;170(3):634–642. doi:10.1111/bjd.12735
46. Zarco Montejo P, Almodóvar González R, De Higes-Martínez E, et al. Delphi-based recommendations for the management of cardiovascular comorbidities in patients with psoriatic arthritis and moderate-to-severe psoriasis. Rheumatol Int. 2020;40(6):969–981. doi:10.1007/s00296-020-04573-w
47. JAAD. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2022. Available from: https://www.jaad.org/article/S0190-9622(18)33001-9/fulltext.
48. Critical Appraisal Skills Programme. CASP qualitative checklist; 2018. Available from: https://casp-uk.net/casp-tools-checklists/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Benefit of Healthy Lifestyle in the Era of New Medications to Treat Obesity
Dalle Grave R
Diabetes, Metabolic Syndrome and Obesity 2024, 17:227-230
Published Date: 15 January 2024
Impact of Fasting on Physical Activity Motivation and Weight Reduction in Patients Administered Glucagon-Like Peptide-1 Agonists: A Qualitative Study
Almaqhawi A, Alabdulqader RA, Alkhteeb NA, Alomair FI, Alhassan SR, Alnajjar JS
Patient Preference and Adherence 2025, 19:19-28
Published Date: 1 January 2025