Back to Journals » Journal of Pain Research » Volume 16
Protocol for Development and Validation of Multivariable Prediction Models for Chronic Postsurgical Pain Following Video-Assisted Thoracic Surgery
Authors Hu JH ![]() , Shi HJ, Han ZY, Liu H
, Shi HJ, Han ZY, Liu H ![]() , Ji FH
, Ji FH ![]() , Peng K
, Peng K ![]()
Received 10 April 2023
Accepted for publication 30 June 2023
Published 3 July 2023 Volume 2023:16 Pages 2251—2256
DOI https://doi.org/10.2147/JPR.S416450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Jing-Hui Hu,1,2,* Hai-Jing Shi,1,2,* Zhen-Yu Han,3,* Hong Liu,4 Fu-Hai Ji,1,2 Ke Peng1,2
1Departments of Anesthesiology, First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Institute of Anesthesiology, Soochow University, Suzhou, Jiangsu, People’s Republic of China; 3Department of Thoracic Surgery, First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 4Department of Anesthesiology and Pain Medicine, University of California Davis Health, Sacramento, CA, USA
*These authors contributed equally to this work
Correspondence: Ke Peng, Department of Anesthesiology, First Affiliated Hospital of Soochow University, 188 Shizi St, Suzhou, Jiangsu, 215006, People’s Republic of China, Tel +86-159-6215-5989, Email [email protected]
Purpose: Chronic postsurgical pain (CPSP) is a common complication after thoracic surgery and associated with long-term adverse outcomes. This study aims to develop two prediction models for CPSP after video-assisted thoracic surgery (VATS).
Methods and Analysis: This single-center prospective cohort study will include a total of 500 adult patients undergoing VATS lung resection (n = 350 for development and n = 150 for external validation). Patients will be enrolled continuously at The First Affiliated Hospital of Soochow University in Suzhou, China. The cohort for external validation will be recruited in another time period. The outcome is CPSP, which is defined as pain with the numerical rating scale score of 1 or higher 3 months after VATS. Univariate and multivariable logistic regression analyses will be performed to develop two CPSP prediction models based on patients’ data of postoperative day 1 and day 14, respectively. For internal validation, we will use the bootstrapping validation technique. For external validation, the discrimination capability of the models will be assessed using the area under the receiver operating characteristic curve, and the calibration will be evaluated using the calibration curve and Hosmer–Lemeshow goodness-of-fit statistic. The results will be presented in model formulas and nomograms.
Conclusion: Based on the development and validation of the prediction models, our results contribute to early prediction and treatment of CPSP after VATS.
Trial Registration: Chinese Clinical Trial Register (ChiCTR2200066122).
Keywords: chronic postsurgical pain, prediction, video-assisted thoracoscopic surgery
Introduction
Chronic postsurgical pain (CPSP) is defined as pain that develops at related surgical area and persists at least 3 months after surgical procedures, after ruling out other causes (eg, chronic infection, malignancy, and a pre-existing pain condition).1–4 Typically, CPSP is associated with adverse outcomes, such as poor recovery, psychological distress, sleep problems, and impaired physical function.5–8 Video-assisted thoracic surgery (VATS) has been increasingly performed in recent years and is associated with lower postoperative pain and improved quality of life when compared with thoracotomy;9 however, CPSP after VATS is still a significant clinical problem, with the incidence of 20−47%.10–12
Recent studies have reported the potential risk factors of CPSP, such as young age, female sex, intraoperative nerve injury, longer duration of surgery, preoperative pain, and severe acute postoperative pain.13–18 There has been a prediction model for CPSP after thoracic surgery (including both VATS and thoracotomy) with the retrospective design.19 A recent study developed the prediction models for CPSP using patients’ data on postoperative day (POD) 1 and POD 14, based on the underlying mechanisms that transition from acute to chronic pain initiates within 14 days after surgery.20,21 However, they did not include patients who underwent VATS procedures.
Therefore, we design this prospective cohort study to develop two models based on patients’ characteristics on POD 1 and POD 14 for early prediction of CPSP in patients undergoing VATS lung resection.
Methods
Study Design and Ethics
This single-center prospective cohort study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University, China (Approval No.2022–442) on November 8, 2022. The protocol was registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn, identifier: ChiCTR2200066122) on November 24, 2022. This trial will be conducted in accordance with the Declaration of Helsinki. All patients will provide written informed consent. We plan to conduct this study from December 2022 to September 2023. The protocol and study results will follow the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD) checklist (Supplemental File 1).22
Study Population
The inclusion criteria are 1) age ≥18 years, 2) American Society of Anesthesiologists (ASA) physical status classification I−III, and 3) elective VATS lung surgery under general anesthesia.
The exclusion criteria are 1) history of chronic pain, 2) previous thoracic surgery, 3) inability to communicate effectively or refusal for participation, 4) surgery cancelled or switched to thoracotomy, or 5) reoperation within 3 months after the primary surgery.
Study Plan
Table 1 shows the study timeline. One day prior to surgery, a researcher will identify eligible patients according to the inclusion and exclusion criteria. Patient baseline characteristics and perioperative data will be collected using the case report forms (Supplemental File 2) and electronic medical records. A trained investigator will be responsible for pain assessment on POD 1 via ward visit and on POD 14 and POD 90 via telephone.
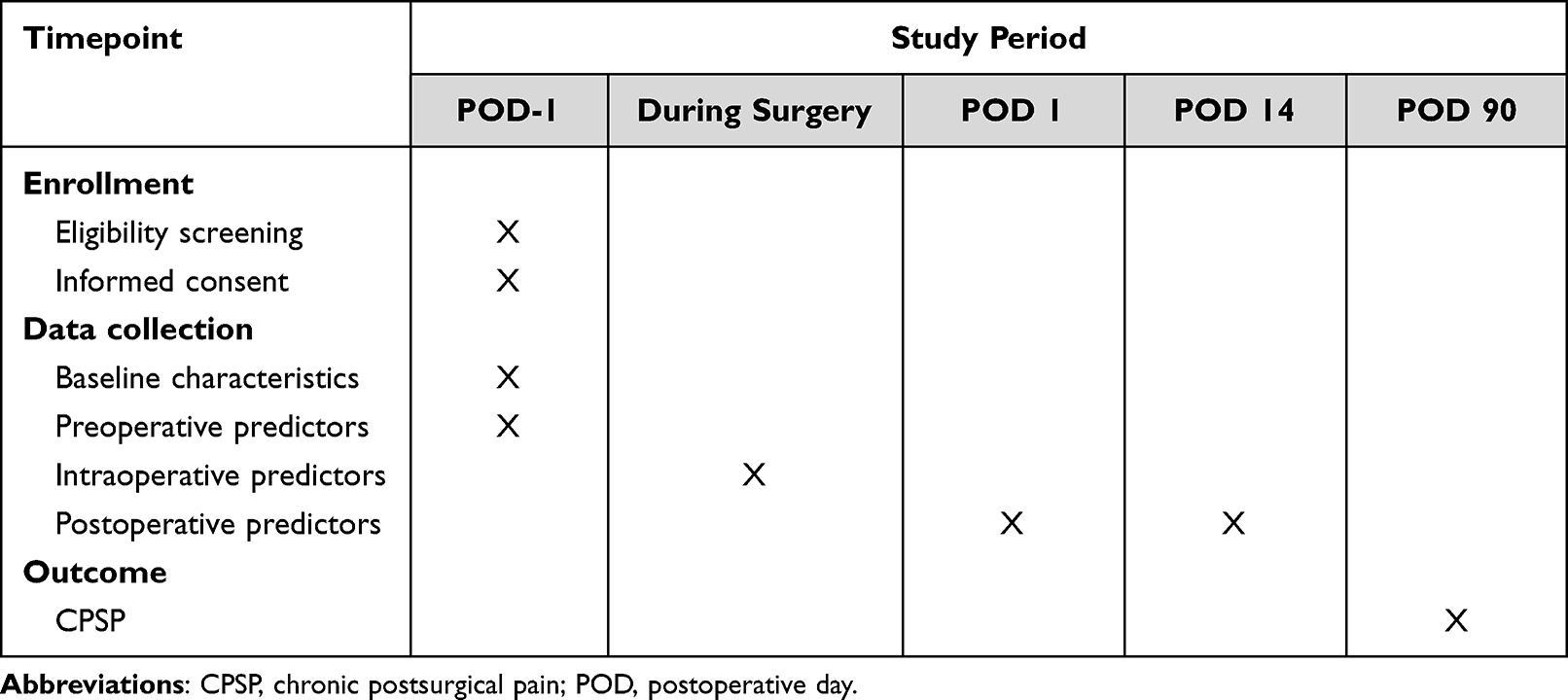 |
Table 1 Study Timeline |
On POD 1 and POD 14, pain intensity will be assessed using the Prince-Henry scale, and pain characteristics will be determined using the Douleur Neuropathique 4 (DN4) questionnaire. The Prince-Henry scale is an optimized pain scale for thoracic surgery (0 = no pain on coughing, 1 = pain on coughing or movement but not on deep breathing, 2 = pain on deep breathing but not at rest, 3 = slight pain at rest, and 4 = severe pain at rest).23–25 The DN4 questionnaire has a high specificity in identifying neuropathic pain (a total score of 0−10 and a score ≥4 points indicating neuropathic pain).19,21
On POD 90, chronic pain will be assessed using the numerical rating scale (NRS), ranging from 0 to 10, with 0 = no pain and 10 = the most severe pain.
Potential Predictors of CPSP
The following 14 candidate predictive factors of CPSP are selected according to the published literature26–31 and clinical expertise.
There are 8 preoperative predictors including demographic data (age, sex, and body mass index), smoking history, comorbidities (age-adjusted Charlson Comorbidity Index),32 preoperative anxiety (total scores of the first four items of the Amsterdam Preoperative Anxiety and Information Scale),33 preoperative frailty (the FRAIL scale scores),34 preoperative pulmonary ventilation function (normal, small airway dysfunction, restrictive hypoventilation, obstructive hypoventilation, and mixed hypoventilation).
There are 3 intraoperative predictors including type of surgery (pneumonectomy, lobectomy, segmentectomy, wedge resection, biopsy and explorative surgery), duration of surgery, and analgesic regimen (nerve block, patient-controlled intravenous analgesia, and both or neither).
There are 3 postoperative predictors including the duration of chest tube drainage, and acute pain intensity (the Prince-Henry scale scores) and neuropathic pain characteristics (the DN4 scores) on POD 1 and POD 14.
Outcome
The outcome is CPSP, which is defined as NRS pain score of 1 or higher 3 months after VATS.19
Sample Size
Recent literature shows that the incidence of CPSP after VATS is about 40%.10 Based on the 10-events-per-covariate principle, we plan to enroll a total of 350 patients in the development cohort (ie, 14*10/0.4=350).35,36 For model external validation, we plan to enroll 150 consecutive patients from a different cohort in another time period.37 Thus, the planned sample size will be set to at least 500 patients.
Missing Data
We will use multiple imputations when a variable has ≤5% missing data. However, a variable with >5% missing data will be excluded.
Statistical Analysis
Normally distributed variables will be presented as mean ± standard deviation and analyzed using the Student's t-test, while non-normally distributed variables will be presented as medians (interquartile ranges) and analyzed using the Mann–Whitney U-test. Categorical and ordinal data will be summarized as n (%) and analyzed using the χ2 or Fisher’s exact test.
First, univariate logistic regression analysis will be performed to screen potential risk factors. The factors with P < 0.1 and the demographic data will be included in the multivariable modelling. Second, multivariable logistic regression will be performed to develop two CPSP prediction models based on the data of POD 1 and POD 14, respectively. Candidate predictors with P < 0.05 will be included in the final models. Next, the internal validation will be conducted using the bootstrap method, which is the preferred approach.37 External validation will be conducted in the validation cohort. The discrimination capability of the models will be assessed using the area under the receiver operating characteristic curve (AUROC), and its calibration will be evaluated using the calibration curve and Hosmer–Lemeshow goodness-of-fit statistic. Finally, the model formulas and nomograms will be presented to estimate the probability of developing CPSP based on the individual’s characteristics on POD1 and POD14.
All data will be analyzed using the R software (version 4.2.2, www.R-project.org/) and the SPSS software (version 26.0, IBM). A two-sided P < 0.05 indicates statistical significance.
Discussion
This prospective cohort study will establish two prediction models for CPSP after VATS in adults. Our models will be validated internally and externally to ensure reliable diagnostic performance. We will generate model formulas and nomograms for easy application of these models in clinical settings.
For patients undergoing thoracic surgery, there have been several prediction models for postoperative outcomes including postoperative air leakage, urinary retention, and cardiopulmonary complications.38–41 A recent retrospective study developed a prediction model for CPSP after thoracic surgery in elderly patients.19 In that study, the incidence of CPSP was 26.9%, and age ≥75 years and longer duration of hospital stay were associated with CPSP. Nevertheless, lack of detailed information and potential predictors of CPSP due to the retrospective design as well as mixing VATS procedures and thoracotomy limit the predicting ability of the model.
Glare et al summarized the risk factors for CPSP in five core aspects (ie, demographic, genetic, clinical, psychological, and surgery related).28 Gene mutations associated with pain are not detected in our institution. Thus, we choose the potential predictors for CPSP from demographics (age, sex, body mass index, and smoking), physical status (comorbidities, frailty, and pulmonary ventilation function), psychological status (anxiety), clinical management (type of surgery, duration of surgery, analgesic regimen, and duration of chest tube drainage), and postoperative pain (acute pain intensity and neuropathic pain characteristics).
We will assess acute pain intensity using the Prince-Henry scale and neuropathic pain characteristics using the DN4 questionnaire on POD 1 and POD 14, based on the association between acute pain, neuropathic pain and CPSP.21,27 The outcome of this study is the occurrence of CPSP 3 months after VATS. Based on the literature, it is determined using the NRS.19,21
As far as we know, our study is the first prospective cohort study to develop prediction models for CPSP in patients undergoing VATS lung resection. The limitations of our study include the single-center study design, a limited number of available predictors, and lack of postoperative long-term outcomes.
Conclusion
This study will reveal the independent predictors for CPSP after VATS lung resection. Through the development and validation of the prediction models, the results of this study will be helpful for clinical risk assessment, decision-making, and individualized treatment. In the future, sufficient data should be collected to validate the existing CPSP models to see the clinical effectiveness in a VATS surgery population.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the Jiangsu Medical Association Anaesthesia Research Project (SYH-32021-0036 (2021031) to KP), Suzhou Medical Health Science and Technology Innovation Project (SKY2022136 to KP), and National Natural Science Foundation of China (82072130 to FHJ).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Niraj G, Rowbotham DJ. Persistent postoperative pain: where are we now? Br J Anaesth. 2011;107(1):25–29. doi:10.1093/bja/aer116
2. Steyaert A, Lavand’homme P. Prevention and treatment of chronic postsurgical pain: a narrative review. Drugs. 2018;78(3):339–354. doi:10.1007/s40265-018-0866-x
3. Werner MU, Kongsgaard UEI. Defining persistent post-surgical pain: is an update required? Br J Anaesth. 2014;113(1):1–4. doi:10.1093/bja/aeu012
4. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
5. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
6. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287–2298. doi:10.2147/JPR.S144066
7. Kemp HI, Laycock H, Costello A, Brett SJ. Chronic pain in critical care survivors: a narrative review. Br J Anaesth. 2019;123(2):e372–e384. doi:10.1016/j.bja.2019.03.025
8. Niknejad B, Bolier R, Henderson CR Jr, et al. Association between psychological interventions and chronic pain outcomes in older adults: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(6):830–839. doi:10.1001/jamainternmed.2018.0756
9. Bendixen M, Jorgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016;17(6):836–844. doi:10.1016/S1470-2045(16)00173-X
10. Brown LM, Kratz A, Verba S, et al. Pain and opioid use after thoracic surgery: where we are and where we need to go. Ann Thorac Surg. 2020;109(6):1638–1645. doi:10.1016/j.athoracsur.2020.01.056
11. Wang H, Li S, Liang N, Liu W, Liu H, Liu H. Postoperative pain experiences in Chinese adult patients after thoracotomy and video-assisted thoracic surgery. J Clin Nurs. 2017;26(17–18):2744–2754. doi:10.1111/jocn.13789
12. Weinrib AZ, Azam MA, Birnie KA, Burns LC, Clarke H, Katz J. The psychology of chronic post-surgical pain: new frontiers in risk factor identification, prevention and management. Br J Pain. 2017;11(4):169–177. doi:10.1177/2049463717720636
13. Gjeilo KH, Stenseth R, Klepstad P. Risk factors and early pharmacological interventions to prevent chronic postsurgical pain following cardiac surgery. Am J Cardiovasc Drugs. 2014;14(5):335–342. doi:10.1007/s40256-014-0083-2
14. Jin J, Chen Q, Min S, Du X, Zhang D, Qin P. Prevalence and predictors of chronic postsurgical pain after colorectal surgery: a prospective study. Colorectal Dis. 2021;23(7):1878–1889. doi:10.1111/codi.15640
15. Lovich-Sapola J, Smith CE, Brandt CP. Postoperative pain control. Surg Clin North Am. 2015;95(2):301–318. doi:10.1016/j.suc.2014.10.002
16. Schnabel A. Acute neuropathic pain and the transition to chronic postsurgical pain. Pain Manag. 2018;8:317–319. doi:10.2217/pmt-2018-0026
17. Wylde V, Dennis J, Beswick AD, et al. Systematic review of management of chronic pain after surgery. Br J Surg. 2017;104(10):1293–1306. doi:10.1002/bjs.10601
18. Yoon S, Hong W-P, Joo H, et al. Long-term incidence of chronic postsurgical pain after thoracic surgery for lung cancer: a 10-year single-center retrospective study. Reg Anesth Pain Med. 2020;45(5):331–336. doi:10.1136/rapm-2020-101292
19. X-D W, Zeng -F-F, X-X Y, et al. Development and validation of a prediction model for chronic post-surgical pain after thoracic surgery in elderly patients: a retrospective cohort study. J Pain Res. 2022;15:3079–3091. doi:10.2147/JPR.S368295
20. Hankerd K, McDonough KE, Wang J, Tang SJ, Chung JM, La JH. Postinjury stimulation triggers a transition to nociplastic pain in mice. Pain. 2022;163(3):461–473. doi:10.1097/j.pain.0000000000002366
21. van Driel MEC, van Dijk JFM, Baart SJ, Meissner W, Huygen F, Rijsdijk M. Development and validation of a multivariable prediction model for early prediction of chronic postsurgical pain in adults: a prospective cohort study. Br J Anaesth. 2022;129(3):407–415. doi:10.1016/j.bja.2022.04.030
22. Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350:g7594. doi:10.1136/bmj.g7594
23. Yamashita S, Yokouchi T, Tanaka M. Effects of intraoperative high-dose vs low-dose remifentanil for postoperative epidural analgesia after gynecological abdominal surgery: a randomized clinical trial. J Clin Anesth. 2016;32:153–158. doi:10.1016/j.jclinane.2016.02.024
24. Qiu Y, Wu J, Huang Q, et al. Acute pain after serratus anterior plane or thoracic paravertebral blocks for video-assisted thoracoscopic surgery: a noninferiority randomised trial. Eur J Anaesthesiol. 2021;38(Suppl 2):S97–S105. doi:10.1097/EJA.0000000000001450
25. Xiao W, Zhou W, Chen X, Zhu J, Xue Q, Shi J. Analgesic effect of intercostal nerve block given preventively or at the end of operation in video-assisted thoracic surgery: a randomized clinical trial. Braz J Anesthesiol. 2022;72(5):574–578. doi:10.1016/j.bjane.2021.07.010
26. Chen YK, Boden KA, Schreiber KL. The role of regional anaesthesia and multimodal analgesia in the prevention of chronic postoperative pain: a narrative review. Anaesthesia. 2021;76(Suppl 1):8–17. doi:10.1111/anae.15256
27. Fregoso G, Wang A, Tseng K, Wang J. Transition from acute to chronic pain: evaluating risk for chronic postsurgical pain. Pain Physician. 2019;22(5):479–488.
28. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
29. Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101(1):77–86. doi:10.1093/bja/aen099
30. Pak DJ, Yong RJ, Kaye AD, Urman RD. Chronification of pain: mechanisms, current understanding, and clinical implications. Curr Pain Headache Rep. 2018;22(2):9. doi:10.1007/s11916-018-0666-8
31. Werner MU, Mjöbo HN, Nielsen PR, Rudin A, Warner DS. Prediction of postoperative pain: a systematic review of predictive experimental pain studies. Anesthesiology. 2010;112(6):1494–1502. doi:10.1097/ALN.0b013e3181dcd5a0
32. Liu J, Li J, He J, Zhang H, Liu M, Rong J. The age-adjusted Charlson Comorbidity Index predicts post-operative delirium in the elderly following thoracic and abdominal surgery: a prospective observational cohort study. Front Aging Neurosci. 2022;14:979119. doi:10.3389/fnagi.2022.979119
33. Moerman N, van Dam FS, Muller MJ, Oosting H. The Amsterdam Preoperative Anxiety and Information Scale (APAIS). Anesth Analg. 1996;82(3):445–451.
34. Kojima G. Quick and simple FRAIL scale predicts incident Activities of Daily Living (ADL) and Instrumental ADL (IADL) disabilities: a systematic review and meta-analysis. J Am Med Dir Assoc. 2018;19(12):1063–1068. doi:10.1016/j.jamda.2018.07.019
35. Wynants L, Bouwmeester W, Moons KGM, et al. A simulation study of sample size demonstrated the importance of the number of events per variable to develop prediction models in clustered data. J Clin Epidemiol. 2015;68(12):1406–1414. doi:10.1016/j.jclinepi.2015.02.002
36. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
37. Grant SW, Collins GS, Nashef SAM. Statistical Primer: developing and validating a risk prediction model. Eur J Cardiothorac Surg. 2018;54(2):203–208. doi:10.1093/ejcts/ezy180
38. Zheng W, Zhang X, Zheng X, Liang Y, Liu Y, Gao Y. Construction and validation of a risk prediction model for postoperative urinary retention in lung cancer patients. J Healthc Eng. 2022;2022:2227629. doi:10.1155/2022/2227629
39. Jin R, Zheng Y, Gao T, et al. A nomogram for preoperative prediction of prolonged air leak after pulmonary malignancy resection. Transl Lung Cancer Res. 2021;10(8):3616–3626. doi:10.21037/tlcr-21-186
40. Song Y, Liu J, Lei M, et al. An external-validated algorithm to predict postoperative pneumonia among elderly patients with lung cancer after video-assisted thoracoscopic surgery. Front Oncol. 2021;11:777564. doi:10.3389/fonc.2021.777564
41. Salati M, Migliorelli L, Moccia S, et al. A machine learning approach for postoperative outcome prediction: surgical data science application in a thoracic surgery setting. World J Surg. 2021;45(5):1585–1594. doi:10.1007/s00268-020-05948-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Does Preoperative Hookwire Localization Influence Postoperative Acute and Chronic Pain After Video-Assisted Thoracoscopic Surgery: A Prospective Cohort Study
Kong L, Gao L, Zhang H, Wang X, Zhang J
Journal of Pain Research 2023, 16:21-32
Published Date: 5 January 2023