Back to Journals » Nursing: Research and Reviews » Volume 15
Protocol for a Pilot Randomized Controlled Trial of a Resilience Intervention Adapted for Older People Living with HIV: Resilience Intervention for Successful Aging Enhancement (RISE+)
Authors Fazeli PL ![]() , Vance DE
, Vance DE ![]() , Delgadillo JD
, Delgadillo JD ![]() , Haase SR, Chapman Lambert C, Bradley BL, Azuero A
, Haase SR, Chapman Lambert C, Bradley BL, Azuero A ![]() , Turan B, Kempf MC
, Turan B, Kempf MC
Received 6 May 2025
Accepted for publication 15 August 2025
Published 27 August 2025 Volume 2025:15 Pages 151—163
DOI https://doi.org/10.2147/NRR.S538597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ferry Efendi
Pariya L Fazeli,1 David E Vance,1 Jeremy D Delgadillo,2 Shakaye R Haase,2 Crystal Chapman Lambert,1 Brittany L Bradley,1 Andres Azuero,1 Bulent Turan,3 Mirjam Colette Kempf1
1School of Nursing, University of Alabama at Birmingham, Birmingham, AL, USA; 2Department of Psychology, University of Alabama at Birmingham, Birmingham, AL, USA; 3Department of Psychology, Koc University, Istanbul, Turkey
Correspondence: Pariya L Fazeli, UAB School of Nursing, NB 470C, 1720 2nd Avenue South, Birmingham, AL, 35294-1210, USA, Tel +1 205 996 0330, Email [email protected]
Purpose: Despite evidence that: 1) older people living with HIV (PLHIV) experience a high burden of stress that is associated with myriad poorer outcomes; 2) psychological resilience may buffer the negative effects of stress in older PLHIV; and 3) older PLHIV may possess lower levels of this protective factor than seronegative counterparts, little work has examined strategies to bolster resilience in older PLHIV. This article details the protocol for a pilot clinical trial examining the feasibility and efficacy of a theory-driven resilience intervention that has been adapted for older PLHIV.
Patients and Methods: This study plans to randomize 100 older PLHIV aged 45+ years with suboptimal HIV treatment management to either an intervention condition (ie, Resilience Intervention for Successful Aging Enhancement [RISE+]) or an attention-matched control condition. Both arms include weekly one-hour in-person group intervention sessions. The comprehensive assessment includes proximal mechanistic measures, (ie, real-time measurement of resilience resources and stress reactivity and recovery via experience sampling method [ESM] text message-prompted online surveys) and health (ie, psychological functioning and HIV outcomes) measures. Primary aims focus on intervention effects on: the use of resilience resources and whether such increases drive improved affective stress reactivity and recovery (Aim 1); and distal health outcomes at three months (Aim 2).
Conclusion: This study tests a novel resilience intervention among older PLHIV and has several strengths, including focusing on an at-risk and understudied population, rigorous examination of efficacy and mechanism, and utilizing an intervention with minimal facilitator involvement, which has implications for future scalability. Findings will identify intervention mechanisms and inform the development of potent and scalable interventions for building resilience in older PLHIV and other diverse populations of older adults.
Keywords: psychosocial intervention, positive psychology, stress reduction, HIV/AIDS, aging
Introduction
The percentage of people living with HIV (PLHIV) in the USA aged 50+ years is predicted to reach 73% by 2030.1 PLHIV experience unique burdens of managing a chronic illness as well as higher rates of trauma, socioeconomic adversity, stigma, and other life stressors than people without HIV, which are associated with poorer health behaviors and outcomes.2–5 Additionally, older PLHIV may experience combined effects of HIV and aging putting them at higher risk than younger PLHIV for poorer outcomes, including cardio-metabolic comorbidities, neurocognitive impairment, social isolation, affective disorders, stigma, and substance use.6–10 Stress may contribute to poorer health outcomes among older PLHIV indirectly via behavioral mechanisms such as reduced HIV medication adherence, and directly via inflammatory processes.11
Psychological resilience, or “the process of adapting well in the face of adversity”, encompasses several resources, including: dispositional (eg, optimism), self/ego (eg, self-efficacy), behavioral/cognitive (eg, adaptive coping skills), and interpersonal (eg, social support) factors.12 Resilience resources demonstrate clinically relevant associations with health outcomes among older PLHIV, including cognitive functioning, mental health, quality of life, and disease management.13–17 Yet PLHIV may experience lower resilience than seronegative counterparts.15 Interventions strengthening resilience resources may support better stress responses, thereby promoting better health among people aging with HIV. This topic is particularly salient in the Deep South, an epicenter of the US epidemic with a population that experiences a high burden of stress6 and the worst HIV outcomes.18
Evidence of efficacy has been mixed for existing psychosocial interventions in PLHIV. A systematic review19 on psychosocial interventions in PLHIV aged 18+ years identified 16 studies, which showed little to no effects on depression, anxiety, stress, and coping, and only one study targeted resilience resources, and very few studies focused on older PLHIV. In fact, another systematic review20 focused on older PLHIV found only nine psychosocial interventions for older PLHIV, and although small to moderate effects in improving psychosocial well-being were found, the majority of studies were designed to treat, rather than prevent, symptomatology. A systematic review and meta-analysis21 specifically examining the effect of psychosocial interventions to improve adherence in PLHIV aged 18+ years identified 43 studies and found a moderate positive effect (Hedges’ g=0.37) of psychosocial interventions on medication adherence in PLHIV. A recent pilot study among 13 older women with HIV tested an adapted version of the Relaxation Response Resiliency Program which provides psychoeducation on positive psychology, relaxation, and cognitive behavioral strategies.22 After the intervention of 8–10 weekly group sessions, those who completed the intervention (n=7) showed mean improvements in resilience and social support and reductions in depression, anxiety, and stigma, along with high satisfaction with the program. However, this study demonstrated challenges with retention. A critical limitation in the literature on psychosocial interventions among PLHIV is lack of data on mechanisms of change whereby psychosocial interventions may buffer the impact of stress on adherence behaviors and health outcomes. In summary, three critical limitations in the literature on psychosocial interventions among PLHIV include: paucity of studies targeting older PLHIV, use of broad psychosocial interventions focused on clinical samples (eg, PLHIV with depression) and not examining mechanisms whereby the intervention impacted outcomes. The current study aims to fill these gaps by: focusing on middle-aged and older PLHIV, targeting resilience resources, and employing a method to rigorously and ecologically assess efficacy and mechanisms (ie, experience sampling method [ESM] to examine stress responses in the moment via daily text messaging surveys).
The broader literature demonstrates the malleability of resilience resources in interventions among diverse clinical populations,23 which show promise for adaptation to older PLHIV. Specifically, the Transforming Lives Through Resilience Education (TLTRE) is a comprehensive resilience resource building program that is theoretically grounded in the Transactional Model of Stress and Coping,24 the Protective Factor Model of Resilience,25 Resilience and Thriving Models,26 and the Broaden-and-Build Model27 and covers the four resilience resource domains (dispositional self/ego, interpersonal, behavioral/cognitive).28–30 TRLTE combines practical cognitive behavioral strategies with psychoeducation on the connection between resilience and health, providing a toolbox of resilience resources rather than a single coping strategy. The program consists of four modules with videos and activities to deepen understanding of material (Table 1) and is freely available at http://sites.edb.utexas.edu/resilienceeducation/modules/. It has been used in corporate, military, educational, and clinical settings for over 20 years.31,32 Most relevant to the present study was a study among African Americans with type-2 diabetes, which showed that combining the TLTRE curriculum with diabetes self-management education demonstrated medium to large effects at 6 months in improving diabetes knowledge, self-management behaviors, and diabetes biomarkers via improvements in perceived stress, empowerment, and positive meaning.30
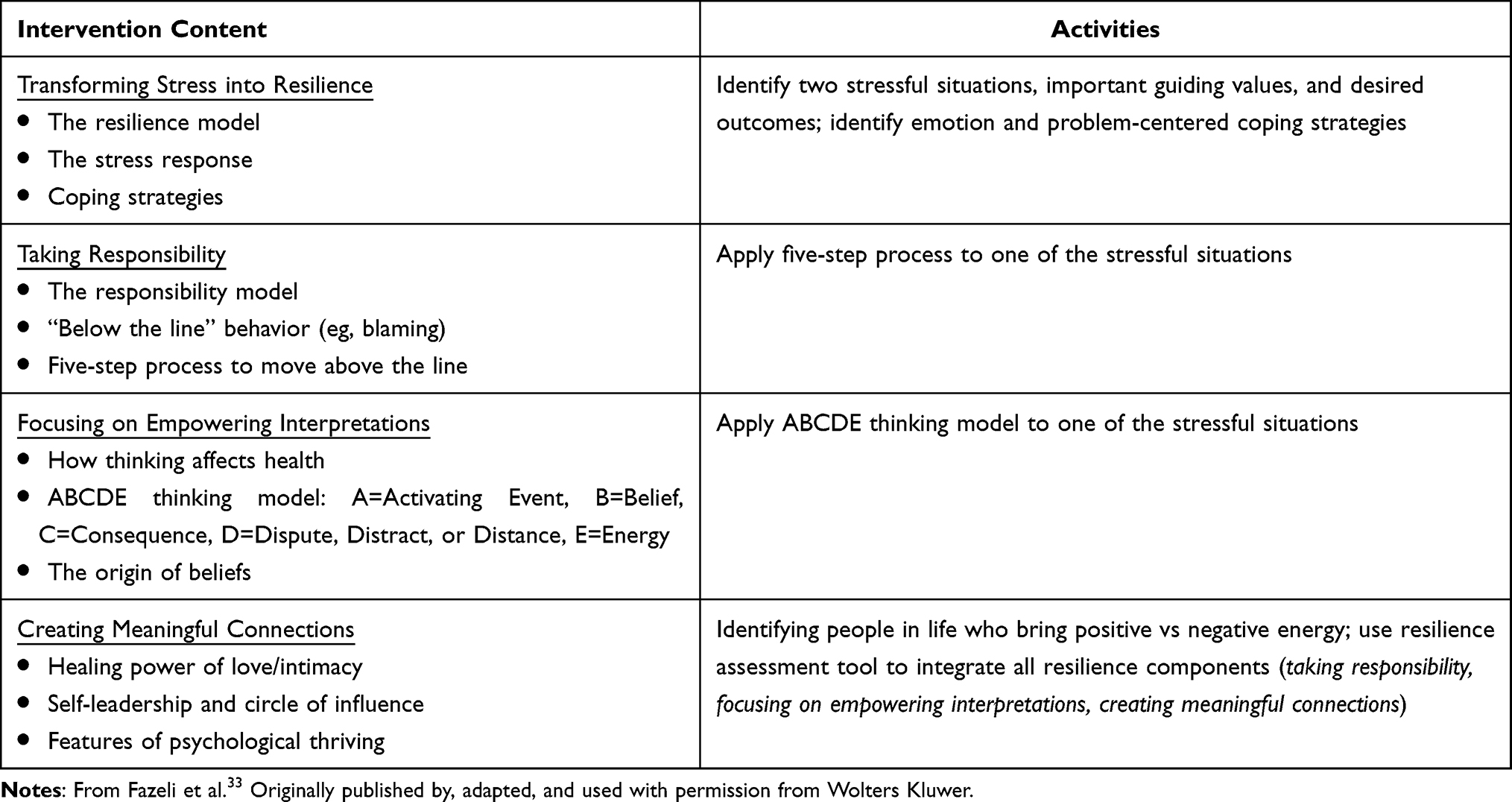 |
Table 1 Resilience Program |
Feasibility, acceptability, and adaptation of the TLTRE Program (dubbed RISE+: Resilience Intervention for Successful Aging Enhancement) was piloted among small groups of 4–5 (total N=14) PLHIV (mean age 52.6 [10.3] years, 57% African American, 57% male, 62% virally suppressed, 50% with depressive symptoms), where the core TLTRE intervention content (Table 1) was presented, which included videos, quizzes, and written activities.33 In this pilot study the intervention was delivered as a one-time 3.5-hour group session rather than four weekly one-hour sessions for feasibility purposes and because this study was not powered to assess changes in outcomes. Participants returned after ~1 week and completed qualitative and quantitative surveys. Results from quantitative and qualitative feedback were positive, and indicated feasibility and acceptability of the program. Results also suggested that uptake of the program may be improved by including content on HIV-specific stressors (eg, stigma, health concerns) and improving comprehensibility.33 These data, combined with the literature, were used to adapt the intervention videos (to be tested in this R21) by modifying several examples and scenarios/vignettes to be more accessible to PLHIV. Modifications include more diverse and realistic animations, HIV-specific vignettes and vignettes more relevant to lower socioeconomic groups, content on spiritual coping and posttraumatic growth, and education on the connection between stress and immune functioning in PLWH. Full details on the adaptation process for the intervention videos can be found elsewhere.33
This current ongoing R21 is testing the efficacy of this modified intervention in a pilot RCT, and will also use participant feedback to further refine the intervention. In this article, we describe the methods and protocol for this RISE+ R21 pilot RCT, as well as study progress, pitfalls, and modifications made to date. This study uses innovative methodology, ESM, to examine a novel intervention in a population with an increased risk of stress and poor health outcomes. The first aim of this study is to evaluate the effects of an adapted resilience intervention on use of resilience resources (ie, hardiness, optimism, self-efficacy, locus of control, reframing, proactive coping, social support) and stress reactivity (ie, magnitude of immediate change in affect during a stressor moment compared to non-stressor moment) and recovery (ie, extent to which affect returns to baseline following a stressor moment) in response to momentary stressors. Specifically, we hypothesize that changes in resilience resource use will mediate changes in stress reactivity and recovery, and these changes will be greater for the RISE+ group as compared to an attention-matched control group. The second aim of this study is to determine whether the effect of the intervention translates to improvements in health outcomes (ie, psychological functioning [quality of life, depressive symptomatology], and HIV outcomes [ART and visit adherence, treatment self-efficacy, viral suppression, and CD4 count]) at 3 months after the end of the intervention. The long-term goal of this study is to inform the development of effective and scalable interventions for building resilience among older PLHIV. If such interventions are effective in improving mental and physical health outcomes, they could aid in ending the HIV epidemic, reducing comorbidities and health disparities, and improving the health and well-being of people aging with HIV.
Materials and Methods
Overview of Study Design
This RCT plans to randomize 100 (20% attrition is accounted for in sample size) older (aged 50+ years, see Results section below for modifications based on age) PLHIV (Figure 1). The sample size was determined on the basis of feasibility, consistent with guidance for pilot studies not focused on statistical inference.34 Eligible participants complete a baseline assessment including a 10-day ESM protocol (Table 2), and then are randomized to the intervention group (n=50) or an attention control group (n=50). We stratify randomization based on race (white or non-white), sex (male or female), and high (≥26) or low resiliency (≤25) based on the Connor Davidson Resilience Scale (described below). Both groups return for four weekly one-hour group visits, followed by a one-month post intervention assessment and a second ESM protocol. A three-month follow-up (comparable to baseline) assesses health outcomes. Participants are compensated $50 for the two-hour baseline, $40 each for the one-month post-test and three-month follow-up, up to $100 for each of two ESM protocols (baseline and one month), and $75 for completing the four intervention or control sessions. If participants have not completed a routine blood draw at our university HIV outpatient clinic recently (within three months prior to baseline or within 30 days prior to three-month follow-up), they are compensated an additional $20 at the baseline and/or three-month follow-up to complete the blood draw at the research laboratory. These procedures are detailed further below.
 |
Table 2 Ten-Day Experience Sampling Method Survey at Baseline and One month Post-test |
 |
Figure 1 Study Design. |
Participants and Procedure
This study is funded by the National Institute on Aging, was approved by the Institutional Review Board at the University of Alabama at Birmingham (protocol # 300008740), and is being conducted in accordance with the Declaration of Helsinki. The ClinicalTrials.gov number is NCT05314088. We are recruiting via our university HIV outpatient clinic (>3,600 active patients, ~50% aged 50+ years) by running eligibility queries of EMR data yielding a list of patients meeting basic criteria that have consented to be contacted for future studies. Specifically, 99% of our university HIV outpatient clinic patients share EMR data with the CFAR Network of Integrated Clinical Systems (CNICS; R24AI067039). These initial criteria determined via EMR include: current university HIV clinic patient, age 50+ years, and no neurological or severe psychiatric (eg, schizophrenia, bipolar disorder, untreated major depression) disorders.
Participants must also have a recent history (within the past 12 months) of suboptimal HIV management based on either of the following data from clinic records: viral load – defined as having greater than or equal to 50% of viral load measurements being detectable (eg, an individual with two measurements of a viral load >50 copies/mL and one measurement <50 copies/mL within the past 12 months would be characterized as having suboptimal treatment management, while an individual with two measurements of a viral load <50 copies/mL and one measurement >50 copies/mL within the past 12 months would be characterized as having optimal treatment management); or HIV clinic attendance – defined as having greater than or equal to 50% of scheduled clinic visits missed/no showed without prior cancellation/reschedule (eg, an individual with two missed clinic visits and two clinic visits attended within the past 12 months would be characterized as having suboptimal treatment management, while an individual with two clinic visits attended and one missed clinic visit within the past 12 months would be characterized as having optimal treatment management).
After determining initial eligibility via EMR, we obtain verbal consent to conduct a phone screen which determines additional eligibility criteria: owning a smart phone with unlimited texting (phones are provided if a participant does not have one, however this has not been needed to date), living in a house or an apartment (not homeless), able to read and write in English, self-report absence of neurological or severe psychiatric disorders that may not have been captured from EMR (eg, schizophrenia, bipolar disorder, Alzheimer’s disease), self-report absence of other medical conditions that can potentially affect mental/thinking abilities, not being blind or deaf, not currently undergoing radiation or chemotherapy, and never experienced brain trauma with loss of consciousness > 30 minutes. After eligibility is determined, participants are scheduled for their baseline assessment where written informed consent is obtained before completing a baseline assessment which includes the following assessments. Although we did provide transportation (ie, Uber) in occasional situations, it was generally expected that participants have transportation to the study visits, which was explained at enrollment.
Measures
With the exception of the ESM protocol, all study assessments occur in person at our laboratory. Resilience resource measures, including ESM items (Table 2), were selected from the NIH Science of Behavior Change initiative and the NIH UCSF Stress Measurement Network.35–37 Our approach to measuring/analyzing stress reactivity was adapted from the MIDUS study’s Daily Inventory of Stressful Events. Clinical data will be extracted from our university HIV outpatient clinic. If participants have not completed a routine blood draw at our university HIV outpatient clinic recently (within three months prior to baseline or within 30 days prior to three-month follow-up), they will be asked to complete a blood draw at the research laboratory to assay viral load and CD4 count.
The baseline survey consists of the measures below delivered via a REDCAP survey at our laboratory, plus a 10-day ESM protocol. The one-month post-test includes all baseline measures except the Ten-Item Personality Inventory (TIPI), Alcohol, Smoking and Substance Involvement Screening Test – Lite (ASSIST-Lite), the Childhood Traumatic Events Scale (CTES), and the Recent Traumatic Events Scale (RTES), plus an exit survey and a 10-day ESM protocol. Finally, the three-month follow-up includes the same measures used in the one-month post-test except the exit survey.
Background Information
A socio-demographic questionnaire is used to collect basic information such as: age, race, sex, education level, annual household income, marital status, and occupation.
Substance Use
Alcohol, Smoking and Substance Involvement Screening Test – Lite (ASSIST-Lite)38 is a brief seven-item screening tool to identify risk of substance use concerns across seven domains (alcohol, cannabis, nicotine, stimulants, sedatives, opioids and psychoactive drugs) within the past three months. Example items are: “Did you smoke a cigarette containing tobacco?” and “Have you tried and failed to control, cut down or stop drinking?”. Responses on each question are: 1 = “yes” and 2 = “no”, and scores on each substance use domain can range from 0 to 3. Higher scores indicate greater risks.
Personality Traits
The Ten-Item Personality Inventory (TIPI)39 is a brief measure of personality traits based on the five-factor model (FFM) personality (openness, conscientiousness, agreeableness, extraversion, and neuroticism). Respondents are asked to what extent they agree or disagree with different statements about their own personality characteristics. Item includes “I see myself as extraverted, enthusiastic” and “Reserved, quiet.” Responses are measured on a Likert-type scale with responses ranging from 1 = “disagree strongly” to 7 = “agree strongly”.
Trauma History
The Childhood Traumatic Events Scale (CTES) and the Recent Traumatic Events Scale (RTES)40 assess different traumatic experiences and perceived severity. The CEST assesses traumatic events across different domains (eg, sexual trauma, physical abuse, major illness) before the age of 17 years. Participants are asked if they have ever experienced different traumatic events (eg, “Prior to the age of 17, did you experience a death of a very close friend or family member?”), how traumatic the event was (“If yes, how traumatic was this?”, “1 = not at all traumatic” to “7 = extremely traumatic”), and if they confided in others (“If yes, how much did you confide in others”, “1 = not at all to 7 = a great deal”). The RTES assesses these similar traumatic events within the past three years. Higher scores on the CTES and RTES indicate higher levels of traumatic experiences.
Stress
The Perceived Stress Scale (PSS)41 is a ten-item measure of the degree to which individuals appraise situations in their life as stressful. Items include: “In the last month, how often have you been upset because of something that happened unexpectedly?” and “In the last month, how often have you felt difficulties were piling up so high that you could not overcome them?”. Responses are measured on a Likert-type scale with responses ranging from 0 = “never” to 4 = “very often”.
Anxiety
Generalized Anxiety Disorder 7 item scale (GAD-7) is a self-report measure of anxiety based on the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for generalized anxiety.42 Responses on the scale range from 0 = “not at all” to 3 = “nearly every day”, and example items are: “Feeling nervous, anxious, or on edge” and “Worrying too much about different things”. Overall scores range from 0 to 27, with higher scores indicating greater levels of anxiety.
Depressive Symptoms
The Center for Epidemiologic Studies Depression Scale (CESD) is a self-report measure of depressive symptoms based on the DSM fifth edition (DSM-V) criteria.43 The CESD consists of 20 items, with scores ranging from 0 to 60, and higher scores suggest greater depressive symptoms. Responses range from 0 = “Rarely or none of the time (less than 1 day)” to 3 = “Most or all of the time (5–7 days)”. Example items are: “I felt depressed” and “I felt that I could not shake off the blues even with the help of my family or friends”.
Resilience
The Connor Davidson Resilience Scale 10 item (CDRS-10) is a measure of dispositional resilience and the ability to adapt when faced with adversity.44,45 The items consist of Likert-type questions with responses ranging from 0 = “not true at all” to 4 = “true nearly all the time”. Example items are: “Having to cope with stress can make me stronger” and “I believe I can achieve my goals, even if there are obstacles”. Scores on the CDRS-10 range from 0 to 40, and higher scores indicate higher levels of resilience.
Coping Skills
The Brief COPE46 is a 28-item measure used to assess different ways in which individuals cope with stressful situations. The Brief COPE examines coping responses along 14 domains (self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, acceptance, religion, and self-blame). Items include: “I’ve been turning to work or other activities to take my mind off things” and “I’ve been getting emotional support from others.” Responses are measured on a Likert-type scale with responses ranging from 1 = “I haven’t been doing this at all” to 4 = “I’ve been doing this a lot”. Higher scores indicate greater use of the specific coping strategy.
Locus of Control
Locus of control was measured using the Personality in Intellectual Aging Contexts (PIC) Inventory Control Scales Short Form.47,48 The PIC short form is a six-item measure that assesses an individual’s perceived control over their cognitive and intellectual functioning. Items include “I have little control over my mental state” and responses range from 1= “strongly agree” to 6 = “Strongly disagree”.
Social Support
The Duke Social Support Index (DSSI)49 is a 11-item self-report measure of social support. Items include “Other than members of your family how many persons in your local area do you feel you can depend on or feel very close to?” and “Can you talk about your deepest problems with at least some of your family and friends?”. Responses on each item vary and higher scores indicate greater levels of social support.
Insomnia
The Insomnia Severity Index (ISI)50,51 is a brief seven-item screen of insomnia, specifically sleep disturbance, sleep satisfaction, and disruption to daily life due to poor sleep. Scores range from 0 to 28, with higher scores indicating more symptoms of insomnia.
Post-Traumatic Stress Disorder (PTSD)
PTSD symptoms were assessed using the Primary Care PTSD Screen for DSM-5 (PC-PTSD-5),52 which is a five-item screening measure of probable PTSD. Participants were asked about exposure to traumatic events, with follow-up questions about trauma symptoms within the past month (eg “In the past month have you: tried hard not to think about the event(s) or went out of your way to avoid situations that reminded you of the event(s)?”).
HIV Stigma
The HIV Stigma Scale (HSS-32)53,54 is a 32-item measure of HIV related stigma and other psychosocial aspects of living with HIV. The scale examines four broad dimensions of stigma, specifically personalized stigma, negative self-image, disclosure concerns, and concern with public attitudes about PLHIV. Example items include: “I never feel ashamed of having HIV” and “People with HIV are treated like outcasts”. Responses on each item range from 1 = “strongly agree” to 4 = “strongly disagree”, and higher scores indicates greater levels of stigma.
Quality of Life/Well-Being
The Medical Outcome Study (MOS) RAND 36-Item Short-Form Health Survey (RAND 36SF) is a measure of health-related quality of life.55 The RAND 36SF assesses quality of life among eight domains: physical functioning, bodily pain, role limitations due to physical health problems, role limitations due to personal or emotional problems, emotional well-being, social functioning, energy/fatigue, and general health perceptions. Example items include: “In general, would you say your health is: (Poor to excellent)” and “Compared to one year ago, how would you rate your health in general now?” Responses on each item vary based on subdomains and higher scores indicate better quality of life.
HIV Treatment Management
The HIV Treatment Adherence Self-Efficacy Scale (HIV-ASES)56 is a 12-item measure of an individuals’ ability to engage in important treatment-related behaviors (eg, following recommended treatment plan, medication adherence) despite potential barriers. Items include: “Continue with your treatment even if doing so interferes with your daily activities?” and “Continue with your treatment even when you are feeling discouraged about your health?”. Responses are measured on a Likert-type scale with responses ranging from 0 = “cannot do at all” and 10 = “completely certain can do”. Higher scores indicate a greater confidence in adhering to one’s treatment plan.
HIV Medication Adherence
The Visual Analogue Scale (VAS)57 for medication adherence is a visual, one-item self-reported measure of medication adherence. Respondents are asked to mark a point along a line ranging from 0 to 100%, indicating their consistency with taking their medication within the past month. The Medication Adherence Questionnaire58,59 is a three-item measure of medication adherence within the past 30 days. Items include “In the last 30 days, how good a job did you do at taking your HIV medications in the way you were supposed to?”. Higher scores indicate greater medication adherence.
Exit Survey
Participants in both the RISE+ arm and control arm are administered a 15-item survey to provide feedback on their experiences during the study. The survey consists of both closed and open-ended questions, allowing a full range of responses. Sample items include: “On scale of 1 to 10, with 10 being the highest, overall, how would you rate this intervention?” and “What did you like or find helpful about this program? In other words, what should we leave as is?”
ESM Protocol
Prior to the first ESM assessment, we conduct a 15-minute training at baseline. We use a validated35–37,60,61 ESM protocol (Table 2) which includes twice a day text messages (morning and evening) for 10 days following both baseline and one month post intervention. Automated text messages based on morning and evening times selected by participants are sent to participants’ personal phones that contain a web link to complete the Redcap survey. If a participant does not report a stressor for item 1, they select “NA” for resilience resource items. The survey takes approximately three minutes. If a participant does not respond to a survey, a reminder message is sent one hour later. If a participant has not responded to any survey for 24 hours, we contact them to troubleshoot and encourage reporting.
Intervention
Participants in the intervention group come to the laboratory for four approximately one-hour weekly sessions in small groups of 3–4. The intervention includes psychoeducational videos and individual written activities on topics such as coping strategies, cognitive appraisals, the responsibility model, and social connections, all integrated into the overarching process of resilience. Details on the core curriculum and written activities are presented in Table 1. To ascertain engagement, short quizzes of material are given after each module to determine retention of the material. The intervention is facilitated by a trained research assistant but as in the pilot study, he/she is minimally involved (ie, only administering the videos and explaining the activities) to keep the private reflective nature of the program that participants preferred. This will allow for comparability with the attention-matched control and will yield implications for scalability. Upon completion of the fourth session, participants are given handouts with summaries of the program material and their responses to the written activities. We are gathering qualitative and quantitative feedback on the intervention at the one-month post-test (see Exit Survey above).
Similar to the RISE+ intervention group, participants in the control group come to the laboratory for four approximately one-hour weekly sessions in small groups of 3–4 (each participant is situated at their own desktop computer). Control participants complete an attention-matched internet stress reduction paradigm, which includes an internet navigation protocol62,63 and placebo computer games via SheppardSoftware.com (eg, “Locate Each State”, “Food Groups Game”, “World Landmarks Puzzle”). Facilitator involvement is the same as the intervention group (eg, the research assistant explains computer activities and games but otherwise does not interact with the participant) which will enhance fidelity. For both conditions, if a participant misses a session, they are given up to one week to make it up. We will examine whether session completion rates are similar across groups.
Results
Study Progress and Modifications
Although planned analyses (described below) will be conducted when the study concludes at the end of 2025, study modifications and current enrollment numbers are provided here. Enrollment began in January 2023. Thus far, the study has prescreened ~2,700 EMR cases, phone screened 108 people, and enrolled 91 (number screened eligible) participants, of whom 70 participants have completed baseline and 68 have been randomized (35 control, 33 RISE+). Fifty-one participants have completed one-month follow-up, 40 have completed three-month follow-up, and 14 have been lost to attrition (randomized but did not complete intervention or completed intervention but never completed any follow-up assessment).
Modifications to the study have been necessitated along the way which were all approved via IRB amendments. Firstly, as a means of increasing the pool by which the research team could recruit potential participants, we reduced our minimum age from 50+ to 45+ years. Secondly, to ensure that newly diagnosed PLWH would not be enrolled in this intervention, an item was added to our phone screener: “Are you a patient at the 1917 Clinic and have been diagnosed with HIV for at least 1 year”. This information is also confirmed with EMR data. Thirdly, a series of questions were added to the phone screener for anyone who had a history of depression in their EMR and had lower than 15 cutoff score for the PHQ-9 depression measure from the EMR: “Have you received any counseling or psychotherapy for any mental health conditions in the last 3 months?”, “Are you currently taking any medication for depression and has it been consistent for the 3 months?”, and “If YES, do you anticipate any upcoming changes with your medication?”. These questions were added as a means of excluding individuals who are currently or recently received counseling or psychotherapy and/or expected their prescription to change, as changes in medication and engagement in counseling or psychotherapy can impart unintended influences on the findings of the resilience intervention.
Planned Analyses
Baseline characteristics will be tabulated, and measures of effect size will be used to examine whether relevant chance imbalances between groups are present (ie, ≥ medium effect size). Characteristics, if any, with relevant imbalances will be used as adjusting covariates in subsequent between-group outcome comparisons.
Specific Aim 1 will examine the effects if the intervention on: a) resilience resource use; and b) stress reactivity. For each resource outcome, the intervention effect will be estimated as the mean between-group difference in change from baseline to post-intervention periods. Linear mixed models will be fitted to these outcomes, including random effects for subject and day (within-subject) to account for the multilevel structure of the data, fixed effects for group assignment, time period, and interaction between group assignment and period. These fixed effects are necessary to estimate outcome means by group and period combinations. Stress reactivity is operationalized as the difference in affect between a stressor instance and a proximally preceding non-stressor instance, and recovery is the difference in affect between a stressor instance and a proximally subsequent non-stressor instance. We will process the within-person data stream by ESM period to identify dyads of ESM instances with the patterns non-stressor → stressor (for reactivity) and stressor → non-stressor (for recovery). Separately for reactivity and recovery, using a dataset containing affect in the selected instances, we will fit a linear mixed model with fixed effects for group and period. A two-way interaction between group and period will be used to estimate between-group differences in change on reactivity/recovery from baseline to post-intervention. In post-hoc analyses, we will examine whether the use of resilience resources mediates intervention effects on reactivity and recovery using subject-specific between-period change (estimated via models with random effects) and applying path analytic methods64 to these (Intervention → Effect [change] on resource use [as mediator] → Effect [change] on reactivity or recovery).
Specific Aim 2 will examine intervention effects on psychological functioning and HIV outcomes. For each outcome, a linear mixed model with random effects for subject and time will be fitted with a group assignment indicator, time-point indicator (baseline, one month, three month), and group by time-point interaction as fixed effects. The intervention effect will be estimated by the interaction term. Exploratory mediation analyses will be conducted with ESM outcomes as proximal outcomes (from Aim 1) and health outcomes as distal outcomes using subject-specific slopes and applying path analytic methods to these. Effects on proximal outcomes will be used as mediators, assuming a causal chain of the form: Intervention → Effect [change] on proximal outcome [as mediator] → Effect [slope] on health outcomes.
Confidence intervals will be computed to assess uncertainty of all effect estimates. A False Discovery Rate approach (10% FDR)65 will be used to account for multiple inferences on the same data.
Feasibility will be assessed by examining screen-fail rates and reasons, retention and dropout rates and predictors (are there sociodemographic or psychological differences between those who are randomized and those who are not randomized [ie, eligible but do not show up for baseline] or those who complete the intervention and follow-ups and those who do not?). We also plan to examine whether feasibility outcomes differ by treatment group. We will also examine completion rates for the ESM surveys. Acceptability will be assessed via the quantitative and qualitative items from the Exit Survey.
Discussion
This study is among the first to test an adapted, low burden, resilience intervention among older PLHIV in the Deep South, which is particularly germane, given that this region is the epicenter of the current HIV epidemic and yet is underrepresented in research on successful aging with HIV. Stress is deleterious to successful aging among PLHIV, and resilience resources demonstrate clinically meaningful associations with health outcomes among PLHIV, and are therefore a promising intervention target to buffer negative stress responses. Although existing psychosocial interventions have been tested in PLHIV, with mixed results, there is a paucity of studies among older PLHIV using preventative approaches targeting individual resilience resources which employ methods to rigorously assess efficacy and mechanisms. We have demonstrated preliminary feasibility and acceptability of an evidence-based resilience curriculum among older PLHIV,33 and have adapted this program for PLHIV, which we are testing for efficacy in the current study. This program is particularly appealing because it uses videos, requiring minimal facilitator involvement, which speaks to the future scalability of this program.
Prior resilience interventions in other populations, while promising, have not examined efficacy and mechanisms in real time. The most innovative aspect of this proposal is that we are examining mechanisms and efficacy of this intervention using an ecologically valid, real-time approach, which has not previously been done. We are using ESM to examine responses to stressors as they occur, allowing for a more nuanced assessment of intervention efficacy. ESM strengths include: increased ecological validity, minimizing memory distortions and biases, and allowing assessment of within-person processes (eg, day-to-day fluctuations in stress responses, change from pre- to post-intervention). Despite evidence of the utility of using ESM in clinical trials,66,67 including greater sensitivity to detect change,68 prior resilience interventions have primarily used traditional recall questionnaires. Using ESM is crucial to examining resilience as a mechanism to improve health outcomes.
This study will overcome gaps in and weaknesses of prior research by testing an adapted resilience intervention in a relevant, growing, and understudied population: older PLHIV in the Deep South. Our aims will allow us to examine whether this intervention increases use of resilience resources following times when stressors are reported, and in turn improves affective reactivity to stressors (Aim 1), and if this translates to health outcomes (Aim 2). Understanding, if, how, and for whom this intervention works will aid in development of potent and scalable resilience-based interventions. Results will provide feasibility and preliminary efficacy data for future studies that could further refine and test this intervention. For example, future studies with sophisticated designs may examine paring down the intervention to most potent ingredients (eg, Multiphase Optimization Strategy [MOST]) as well as hybrid effectiveness-implementation69 trials. The program may also be suitable to be combined with other content, such as disease management psychoeducation (eg, HIV) or relaxation techniques (eg, mindfulness meditation). Booster sessions could also be examined to enhance the durability of effects. Examining self-administration of this program via an online platform should be tested for efficacy, and if effective would expand the scalability of this program. Larger studies with long-term follow-up are needed to examine causal pathways of effects on long-term outcomes such as mood, quality of life, cognitive function, health behaviors, comorbidities, biomarkers.
Although this study aims to fill several gaps in the field, there are limitations worth noting. Our study excludes PLHIV with unstable housing, a population that may benefit from a resilience intervention. However, given this was a pilot study aimed to determine feasibility, acceptability, and preliminary efficacy, we focused on a generalizable sample of PLHIV who would be able to attend the multiple required study visits. Although we did provide transportation (ie, Uber) in occasional situations, it was generally expected that participants have transportation to the study visits, which was explained at enrollment. Another limitation is that we focused on PLHIV with evidence of suboptimal treatment management given that a goal of this study was determining whether the intervention had downstream impacts on HIV outcomes (ie, viral load, CD4 count, treatment and visit adherence). As a result, to identify this sample we had to reduce our age criteria, which limits generalizability to older PLHIV. Similarly, it limits generalizability to older PLHIV who may have well managed HIV, and yet may still benefit from a resilience intervention. Finally, while our data will allow us to examine common drivers of suboptimal treatment management such as substance use and social determinants of health as predictors of dropout, randomization, and treatment response, the intervention content itself does not address these topics, and therefore future adaptations of the program may need to be adapted to vulnerable subpopulations of PLHIV. Future studies of PLHIV with low socioeconomic status or who are not tech savvy may adopt ESM protocols that use SMS text messages not requiring a smart phone70 or phone call surveys, which although they limit the abundance and context of data to be collected, can nonetheless be an effective data collection tool.
Funding
This work was supported by the National Institutes of Health [R21 AG076377].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wing EJ. The aging population with HIV infection. Trans Am Clin Climatol Assoc. 2017;128:131–144.
2. Reif S, Safley D, McAllaster C, Wilson E, Whetten K. State of HIV in the US deep South. J Comm Health. 2017;42(5):844–853. doi:10.1007/s10900-017-0325-8
3. Brezing C, Ferrara M, Freudenreich O. The syndemic illness of HIV and trauma: implications for a trauma-informed model of care. Psychosomatics. 2015;56(2):107–118. doi:10.1016/j.psym.2014.10.006
4. Vance DE, Blake BJ, Brennan-Ing M, DeMarco RF, Fazeli PL, Relf MV. Revisiting successful aging with HIV through a revised biopsychosocial model: an update of the literature. J Assoc Nurses AIDS Care. 2019;30(1):5–14. doi:10.1097/jnc.0000000000000029
5. Bhatia R, Ryscavage P, Taiwo B. Accelerated aging and human immunodeficiency virus infection: emerging challenges of growing older in the era of successful antiretroviral therapy. J Neurovirol. 2012;18(4):247–255. doi:10.1007/s13365-011-0073-y
6. Reif S, Mugavero M, Raper J, et al. Highly stressed: stressful and traumatic experiences among individuals with HIV/AIDS in the deep south. AIDS Care. 2011;23(2):152–162. doi:10.1080/09540121.2010.498872
7. So-Armah KA, Chang J, Alcorn C, et al. HIV infection, antiretroviral therapy initiation and longitudinal changes in biomarkers of organ function. Curr HIV Res. 2014;12(1):50–59. doi:10.2174/1570162x1201140716101512
8. Greene M, Hessol NA, Perissinotto C, et al. Loneliness in older adults living with HIV. AIDS Behav. 2018;22(5):1475–1484. doi:10.1007/s10461-017-1985-1
9. Greene M, Covinsky KE, Valcour V, et al. Geriatric syndromes in older HIV-infected adults. J Acquir Immune Defic Syndr. 2015;69(2):161–167. doi:10.1097/QAI.0000000000000556
10. Deren S, Cortes T, Dickson VV, et al. Substance use among older people living with HIV: challenges for health care providers. Front Public Health. 2019;7:94. doi:10.3389/fpubh.2019.00094
11. Valdez AN, Rubin LH, Neigh GN. Untangling the gordian knot of HIV, stress, and cognitive impairment. Neurobiol Stress. 2016;4:44–54. doi:10.1016/j.ynstr.2016.02.005
12. Schetter CD, Dolbier C. Resilience in the context of chronic stress and health in adults. Soc Personal Psychol Compass. 2011;5(9):634–652. doi:10.1111/j.1751-9004.2011.00379.x
13. Haase SR, Billings R, Vance DE, Fazeli PL. The association between intrapersonal resilience resources and quality of life among older persons living with HIV: a systematic review. J Assoc Nurses AIDS Care. 2023;34(6):502–526. doi:10.1097/JNC.0000000000000432
14. Fazeli PL, Moore RC, Vance DE. Resilience attenuates the association between neurocognitive functioning and everyday functioning in individuals aging with HIV in the deep south. Int J Geriatr Psychiatry. 2019;34(1):72–78. doi:10.1002/gps.4988
15. Moore DJ, Fazeli PL, Moore RC, et al. Positive psychological factors are linked to successful cognitive aging among older persons living with HIV/AIDS. AIDS Behav. 2018;22(5):1551–1561. doi:10.1007/s10461-017-2001-5
16. McGowan JA, Brown J, Lampe FC, Lipman M, Smith C, Rodger A. Resilience and physical and mental well-being in adults with and without HIV. AIDS Behav. 2018;22(5):1688–1698. doi:10.1007/s10461-017-1980-6
17. Dale S, Cohen M, Weber K, Cruise R, Kelso G, Brody L. Abuse and resilience in relation to HAART medication adherence and HIV viral load among women with HIV in the United States. AIDS Patient Care STDS. 2014;28(3):136–143. doi:10.1089/apc.2013.0329
18. HIV.gov. Impact on racial and ethnic minorities. Available from: https://www.hiv.gov/hiv-basics/overview/data-and-trends/impact-on-racial-and-ethnic-minorities.
19. van der Heijden I, Abrahams N, Sinclair D. Psychosocial group interventions to improve psychological well-being in adults living with HIV. Cochrane Database Syst Rev. 2017;3(3):CD010806. doi:10.1002/14651858.CD010806.pub2
20. Bhochhibhoya A, Harrison S, Yonce S, Friedman DB, Ghimire PS, Li X. A systematic review of psychosocial interventions for older adults living with HIV. AIDS Care. 2021;33(8):971–982. doi:10.1080/09540121.2020.1856319
21. Spaan P, van Luenen S, Garnefski N, Kraaij V. Psychosocial interventions enhance HIV medication adherence: a systematic review and meta-analysis. J Health Psychol. 2020;25(10–11):1326–1340. doi:10.1177/1359105318755545
22. Psaros C, Stanton AM, Goodman GR, et al. Adapting, testing, and refining a resilience intervention for older women with HIV: an open pilot study. J Women Aging. 2023;35(4):395–415. doi:10.1080/08952841.2022.2094163
23. Joyce S, Shand F, Tighe J, Laurent SJ, Bryant RA, Harvey SB. Road to resilience: a systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open. 2018;8(6):e017858. doi:10.1136/bmjopen-2017-017858
24. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. Springer publishing company; 1984.
25. O’Leary VE. Strength in the face of adversity: individual and social thriving. J Social Issues. 1998;54(2):425–446. doi:10.1111/j.1540-4560.1998.tb01228.x
26. Carver CS. Resilience and thriving: issues, models, and linkages. J Social Issues. 1998;54(2):245–266. doi:10.1111/j.1540-4560.1998.tb01217.x
27. Fredrickson BL. What good are positive emotions? Rev Gen Psychol. 1998;2(3):300–319. doi:10.1037/1089-2680.2.3.300
28. Steinhardt M, Dolbier C. Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. J Am Coll Health. 2008;56(4):445–453. doi:10.3200/JACH.56.44.445-454
29. Steinhardt MA, Brown SA, Dubois SK, Harrison L, Lehrer HM, Jaggars SS. A resilience intervention in African-American adults with type 2 diabetes. Am J Health Behav. 2015;39(4):507–518. doi:10.5993/AJHB.39.4.7
30. Steinhardt MA, Mamerow MM, Brown SA, Jolly CA. A resilience intervention in African American adults with type 2 diabetes: a pilot study of efficacy. Diabetes Educ. 2009;35(2):274–284. doi:10.1177/0145721708329698
31. Dolbier CL, Jaggars SS, Steinhardt MA. Stress-related growth: pre-intervention correlates and change following a resilience intervention. Stress Health. 2010;26(2):135–147. doi:10.1002/smi.1275
32. Lehrer HM, Dubois SK, Brown SA, Steinhardt MA. Resilience-based diabetes self-management education: perspectives from African American participants, community leaders, and healthcare providers. Diabetes Educ. 2017;43(4):367–377. doi:10.1177/0145721717714894
33. Fazeli PL, Hopkins CN, Wells A, et al. Examining the acceptability of a resilience building intervention among adults aging with HIV. J Assoc Nurses AIDS Care. 2022;33(2):155–167. doi:10.1097/JNC.0000000000000229
34. National Center for Complementary and Integrative Health. Pilot studies: common uses and misuses. Available from: https://www.nccih.nih.gov/grants/pilot-studies-common-uses-and-misuses.
35. Almeida DM, Marcusson-Clavertz D, Conroy DE, et al. Everyday stress components and physical activity: examining reactivity, recovery and pileup. J Behav Med. 2020;43(1):108–120. doi:10.1007/s10865-019-00062-z
36. Almeida DM, Wethington E, Kessler RC. The daily inventory of stressful events: an interview-based approach for measuring daily stressors. Assessment. 2002;9(1):41–55. doi:10.1177/1073191102091006
37. Smyth JM, Sliwinski MJ, Zawadzki MJ, et al. Everyday stress response targets in the science of behavior change. Behav Res Ther. 2018;101:20–29. doi:10.1016/j.brat.2017.09.009
38. Ali R, Meena S, Eastwood B, Richards I, Marsden J. Ultra-rapid screening for substance-use disorders: the alcohol, smoking and substance involvement screening test (ASSIST-Lite). Drug Alcohol Depend. 2013;132(1):352–361. doi:10.1016/j.drugalcdep.2013.03.001
39. Gosling SD, Rentfrow PJ, Swann WB. A very brief measure of the big-five personality domains. J Res Personality. 2003;37(6):504–528. doi:10.1016/S0092-6566(03)00046-1
40. Pennebaker JW, Susman JR. Disclosure of traumas and psychosomatic processes. Social Sci Med. 1988;26(3):327–332. doi:10.1016/0277-9536(88)90397-8
41. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Social Behav. 1983;24(4):385–396. doi:10.2307/2136404
42. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
43. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Measurement. 1977;1(3):385–401. doi:10.1177/014662167700100306
44. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the connor-davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Traumatic Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
45. Connor KM, Davidson JR. Development of a new resilience scale: the connor-davidson resilience scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
46. Carver CS. You want to measure coping but your protocol’s too long: consider the brief COPE. Int J Behav Med. 1997;4(1):92–100. doi:10.1207/s15327558ijbm0401_6
47. Lachman ME. Locus of control in aging research: a case for multidimensional and domain-specific assessment. Psychol Aging. 1986;1(1):34–40. doi:10.1037/0882-7974.1.1.34
48. Lachman ME, Baltes P, Nesselroade JR, Willis SL. Examination of personality-ability relationships in the elderly: the role of the contextual (interface) assessment mode. J Res Personality. 1982;16(4):485–501. doi:10.1016/0092-6566(82)90007-1
49. Koenig HG, Westlund RE, George LK, Hughes DC, Blazer DG, Hybels C. Abbreviating the duke social support index for use in chronically Ill elderly individuals. Psychosomatics. 1993;34(1):61–69. doi:10.1016/S0033-3182(93)71928-3
50. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
51. Morin CM. Insomnia: Psychological Assessment and Management. Guilford Press; 1993:238.
52. Prins A, Bovin MJ, Smolenski DJ, et al. The primary care PTSD screen for DSM-5 (PC-PTSD-5): development and evaluation within a veteran primary care sample. J Gen Intern Med. 2016;31(10):1206–1211. doi:10.1007/s11606-016-3703-5
53. Bunn JY, Solomon SE, Miller C, Forehand R. Measurement of stigma in people with HIV: a reexamination of the HIV stigma scale. AIDS Educ Prev. 2007;19(3):198–208. doi:10.1521/aeap.2007.19.3.198
54. Berger BE, Ferrans CE, Lashley FR. Measuring stigma in people with HIV: psychometric assessment of the HIV stigma scale. Res Nurs Health. 2001;24(6):518–529. doi:10.1002/nur.10011
55. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): i. conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
56. Johnson MO, Neilands TB, Dilworth SE, Morin SF, Remien RH, Chesney MA. The role of self-efficacy in HIV treatment adherence: validation of the HIV treatment adherence self-efficacy scale (HIV-ASES). J Behav Med. 2007;30(5):359–370. doi:10.1007/s10865-007-9118-3
57. Giordano TP, Guzman D, Clark R, Charlebois ED, Bangsberg DR. Measuring adherence to antiretroviral therapy in a diverse population using a visual analogue scale. HIV Clinical Trials. 2004;5(2):74–79. doi:10.1310/JFXH-G3X2-EYM6-D6UG
58. Wilson IB, Fowler FJ, Cosenza CA, et al. Cognitive and field testing of a new set of medication adherence self-report items for HIV care. AIDS Behav. 2014;18(12):2349–2358. doi:10.1007/s10461-013-0610-1
59. Wilson IB, Lee Y, Michaud J, Fowler FJ, Rogers WH. Validation of a new three-item self-report measure for medication adherence. AIDS Behav. 2016;20(11):2700–2708. doi:10.1007/s10461-016-1406-x
60. Mroczek DK, Stawski RS, Turiano NA, et al. Emotional reactivity and mortality: longitudinal findings from the VA normative aging study. J Gerontol B Psychol Sci Soc Sci. 2015;70(3):398–406. doi:10.1093/geronb/gbt107
61. Short NA, Boffa JW, Clancy K, Schmidt NB. Effects of emotion regulation strategy use in response to stressors on PTSD symptoms: an ecological momentary assessment study. J Affect Disord. 2018;230;77–83. doi:10.1016/j.jad.2017.12.063
62. Vance D, Fazeli P, Shacka J, et al. Testing a computerized cognitive training protocol in adults aging with HIV-associated neurocognitive disorders: randomized controlled trial rationale and protocol. JMIR Res Protoc. 2017;6(4):e68. doi:10.2196/resprot.6625
63. Vance DE, Fazeli PL, Azuero A, et al. A 2-year longitudinal randomized control trial of speed of processing cognitive training in aging adults with HIV-associated neurocognitive disorder: results of the think fast study. AIDS Behav. 2024;28(10):3300–3314. doi:10.1007/s10461-024-04409-9
64. MacKinnon DP. Introduction to Statistical Mediation Analysis. Lawrence Erlbaum Associates; 2008.
65. Glickman ME, Rao SR, Schultz MR. False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. J Clin Epidemiol. 2014;67(8):850–857. doi:10.1016/j.jclinepi.2014.03.012
66. Verhagen SJ, Hasmi L, Drukker M, van Os J, Delespaul PA. Use of the experience sampling method in the context of clinical trials. Evid Based Ment Health. 2016;19(3):86–89. doi:10.1136/ebmental-2016-102418
67. Geschwind N, Peeters F, Drukker M, van Os J, Wichers M. Mindfulness training increases momentary positive emotions and reward experience in adults vulnerable to depression: a randomized controlled trial. J Consult Clin Psychol. 2011;79(5):618–628. doi:10.1037/a0024595
68. Moore RC, Depp CA, Wetherell JL, Lenze EJ. Ecological momentary assessment versus standard assessment instruments for measuring mindfulness, depressed mood, and anxiety among older adults. J Psychiatr Res. 2016;75:116–123. doi:10.1016/j.jpsychires.2016.01.011
69. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–226. doi:10.1097/MLR.0b013e3182408812
70. Fazeli PL, Hopkins C, Vance DE, et al. Cognitive prescriptions for reducing dementia risk factors among black/African Americans: feasibility, acceptability, and preliminary efficacy. Ethn Health. 2024;29(1):1–24. doi:10.1080/13557858.2023.2231669
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Unsafe Infant Feeding Practice and Associated Factors Among HIV Positive Mothers Attending PMTCT in Ethiopia: A Cross-Sectional Study
Zewdu D, Bekele DM, Bantigen KA, Wake AD
HIV/AIDS - Research and Palliative Care 2023, 15:325-337
Published Date: 14 June 2023
Medical Interns’ Knowledge, Attitude, and Practice Toward People Living with HIV: Multicenter Experience from Saudi Arabia
Malli IA, Hamdan D, Aljahdali A, Almutairi A, Jar R, Alzahrani R, Khan MA
HIV/AIDS - Research and Palliative Care 2023, 15:571-582
Published Date: 18 September 2023
Quality of Life of People Living with HIV on Antiretroviral Therapy: A Cross-Sectional Study in Monastir, Tunisia
Berrezouga L, Kooli I, Marrakchi W, Harzallah G, Chakroun M
HIV/AIDS - Research and Palliative Care 2023, 15:671-682
Published Date: 10 November 2023
A Systematic Literature Review of Mathematical Models for Coinfections: Tuberculosis, Malaria, and HIV/AIDS
Inayaturohmat F, Anggriani N, Supriatna AK, Biswas MHA
Journal of Multidisciplinary Healthcare 2024, 17:1091-1109
Published Date: 13 March 2024
Utilization of Social Media for the Prevention and Control of HIV/AIDS: A Scoping Review
Ibrahim K, Kahle EM, Christiani Y, Suryani S
Journal of Multidisciplinary Healthcare 2024, 17:2443-2458
Published Date: 21 May 2024