")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Quality of Life of People Living with HIV on Antiretroviral Therapy: A Cross-Sectional Study in Monastir, Tunisia
Authors Berrezouga L , Kooli I, Marrakchi W , Harzallah G, Chakroun M
Received 13 July 2023
Accepted for publication 12 October 2023
Published 10 November 2023 Volume 2023:15 Pages 671—682
DOI https://doi.org/10.2147/HIV.S430376
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Latifa Berrezouga,1– 3 Ikbel Kooli,4 Wafa Marrakchi,4 Ghaya Harzallah,4 Mohamed Chakroun4
1Department of Microbiology and Immunology, University of Monastir, Faculty of Dental Medicine, Monastir, Tunisia; 2Department of Endodontics, University of Monastir, Dental Clinic, Monastir, Tunisia; 3Faculty of Pharmacy, Laboratory of Medical and Molecular Parasitology and Mycology LR12ES09, University of Monastir, Monastir, Tunisia; 4Department of Infectious Diseases, University of Monastir, F. Bourguiba Teaching Hospital, Monastir, Tunisia
Correspondence: Latifa Berrezouga, Email [email protected]
Introduction: Despite the benefits of an efficient antiretroviral therapy (ART), HIV/AIDS epidemic still represents the most seriousaffection worldwide that negatively impacts people’s quality of life (QoL). As no studies exist on QoL in Tunisia, the aim of the present work was i: to assess, based on WHOQOL-HIV BREF tool, the perception of QoL of people living with HIV (PLHIV) receiving ART and ii: to investigate the relationship between socio-demographic features, disease-related variables and QoL domains’ mean scores.
Methods: This cross-sectional study was conducted at the department of infectious diseases of F. Bourguiba Teaching Hospital in Monastir, Tunisia. One hundred and five participants receiving ART were involved. QoL assessment was based on the WHOQOL-HIV Bref including six domains with 29 items with scores ranged from the lowest (4) to the highest (20). Results were reported as frequencies and means (±SD). The Student’s t-test for independent samples and the one-way ANOVA were performed to assess differences in QoL mean scores. Linear regression analysis was used to investigate predictors of QoL. The confidence interval was set at 95%.
Results: Clients’ mean age was 39.20± 10.18 years old with a male to female sex ratio of 3.12. Low mean scores were seen with the environment (12.34± 2.90), social relations (12.58± 3.94) and psychological domains (12.76± 3.31), and moderate mean scores were noted for the physical (14.11± 3.52), the spiritual (14.05± 3.78) and the level of independence (13.98± 3.57) domains. Regression analysis showed that health status and feeling healthy were related to all QoL domains and that profession, marital status and the presence of a confident person were related to environment and spiritual domains.
Conclusion: QoL of PLHIV on ART is affected. Concrete measures and strategies should be undertaken by healthcare stakeholders to improve QoL determinants.
Keywords: people living with HIV, WHO quality of life, Tunisia
Introduction
The HIV/AIDS epidemic still represents the most serious afection worldwide. In 2021, an estimated 38.4 million of people are living with HIV (PLHIV) with a higher frequency and severity in sub-Saharan Africa and Asia and an estimated 650.000 HIV-related deaths. Indeed, 28.7 million people are accessing antiretroviral treatment (ART).1 People from all over the world are experiencing hard times due to the COVID-19 pandemic and its social, economic and health impact, particularly in PLHIV with limited access to treatment and health care. HIV positive people with co-morbidities are at higher risk of being infected with SarsCov-2.2 According to WHO, an additional 500.000 AIDS related deaths could be recorded by the end of 2021 in sub-Saharan Africa, in case of a six-month disruption to medical supplies.3 The MENA region (Middle East and North Africa) is considered as a “real black hole” in terms of HIV/AIDS data4 and is still far from the 95-95-95 UNAIDS and WHO prevention program targets.1 The estimated reported number of PLHIV is 180.000 (150. 000–210. 000) and only 88.000 are accessing ART.1 HIV infection has increased by 22% over the last years.3 In fact, despite the low prevalence, less than 1%, HIV infection is on the rise, particularly for key populations like people who inject drugs, men who have sex with men and female sex workers.1,4–10 In Tunisia, the 2022 estimated number of PLHIV is 7.100 (5.200–10.000) with a prevalence rate <0.1 [<0.1–0.1] for adult aged 15 to 49 years old.11 This population is still marginalized with poor access to diagnosis, treatment and prevention because of discriminatory attitudes.12 This social behaviour has a negative impact on people’s quality of life (QoL) despite the significant improvement of their life expectancy thanks to the efficacy of antiretroviral therapy (ART) that significantly decreases co-morbidities and HIV-related deaths.13–19
According to WHO, QoL is defined as
indIviduals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.20
Although lacking in the MENA region, several studies using various tools or instruments have been reported to evaluate the impact of clinical determinants on QoL. These tools are based on a self-administered questionnaire investigating people’s physical, social relations, environmental, psychological or mental health and spiritual and religious beliefs as well.21–25 Results recorded as mean scores of QoL domains vary according to studies. They are, particularly, low or very low in some African and Middle East countries Unemployment and financial issues affect negatively people’s social relation, the level of independence and mental health, as well.26–28 Some studies reported a better perception of QoL in clients receiving ART29,30 and other findings confirmed the benefits of ART initiated at 1 month and 4 months31 and one year13 after clients’ enrolment, compared to ART naïve clients with symptoms and AIDS-related comorbidities.25 In fact, people receiving ART reported better physical function that positively affects their level of independence.
Therefore, as no studies exist on QoL in Tunisia, the aim of the present work was i: to assess, based on WHOQOL-HIV BREF tool, the perception of QoL of Tunisian HIV people on ART and ii: to investigate the relation between socio-demographic features, disease-related variables and QoL domains’ mean scores. The following hypotheses were considered: the null hypothesis (H0) assuming that QoL of PLHIV receiving ART is not affected and an alternative hypothesis (H1) assuming that QoL of PLHIV receiving ART is affected.
Methods
Clients’ Enrolment and Data Collection
This cross-sectional study, conducted following the STROBE checklist (strengthening the reporting of observational studies in epidemiology)32 was performed at the department of infectious diseases of F. Bourguiba teaching hospital in Monastir, Tunisia. The department is characterised by the existence of a day hospital dedicated for the diagnosis, treatment and follow-up of 150 PLHIV. Most of the clients are from different parts of Tunisia and some are from foreign African countries. The team is composed of specialized physicians, nurses, a pharmacist, a psychologist a social assistant and medical secretaries. Counselling services are provided in a counselling room. The medical team collaborate with all clinical and biological specialties related to PLHIV health (cardiology, endocrinology, radiology, dermatology, oral medicine, biology…).
Clients already scheduled for a routine clinical and biological follow-up and ART pick-up were enrolled according to the following inclusion criteria: i: aged more than 18 years with confirmed HIV disease and not known psychiatric illness, understand the Arabic language and consent to answer voluntarily the questionnaire. Clients excluded from the study were: children aged between 7 and 11 years old (n = 5), non-consenting individuals (n = 8), clients treated for neurological disorders (n = 2), and those who do not understand the Arabic language (n = 30). Each client answered the questionnaire in a private room for 10 minutes, after a discussion with the physician about the objectives and outcomes of the survey.
Data collection was performed from 8.30 a. m to 2 p. m, 3 days per week over a period of 4 months, from December 2021 to March 2022. The overall number of individuals included was 105.
The present study is part of Latifa Berrezouga research project on PLHIV that was approved by the committee of ethics of the faculty of pharmacy, University of Monastir, Tunisia, under the reference CER-SVS/ISBM 013/2020 with respect to Helsinki declaration. Verbal and written consent was obtained from every consent client.
WHOHIVQOL-Bref Instrument
WHOQOL-HIV-Bref instrument21 [Annex 1] is a short version of the WHOQOL-HIV (120 items) developed by researchers from UNAIDS and WHO aiming at assessing QoL of PLHIV. This tool is a self-administered questionnaire including two parts. The first one concerns personal information related to age, sex, education level, marital status, health status, HIV onset, HIV-related symptoms and HIV transmission. The questionnaire was supplemented with questions about the living place, profession, consulting with a psychologist, and the person informed about the individual’s HIV status. ART duration and CD4 T lymphocytes’ counts were obtained from clients’ medical files.
The second part comprises 31 items or questions randomly allocated and scored on a Likert-scale from 1 (lowest) to 5 (highest). Of these, 29 questions investigate six domains: physical, psychological, level of independence, social relations, environmental and spiritual/religious/beliefs domains. Briefly, the physical domain examines 4 items: pain, HIV-related symptoms, energy and sleep. The psychological domain examines 5 items: life enjoy, ability to concentrate, bodily appearance, self-satisfaction and negative feelings. The level of independence examines 4 items: treatment dependence, daily activities and capacity to function and work. The social relationships domain examines 4 items: acceptance by others, personal relationship and social interaction, sexual activities and social support. The environment domain examines 8 items: daily life safety, environment healthiness, financial resources, information availability, leisure activities, health services access, living place and transport. The spiritual domain examines 4 items: life meaningful, blame, fear of the future and death worries. The last 2 questions are related to the overall QoL (Q1) and general health perception (Q2). Before computing, the scores of negatively phrased questions (Q3, 4, 5, 8, 9, 10 and Q31) were inverted. The scores’ domains were obtained by calculating the sum of scores of “n” questions of each domain, divided by the number of domain questions. The result was multiplied by 4. Therefore, QoL is assessed from the lowest score being 4 to the highest score being 20 (Table 1).
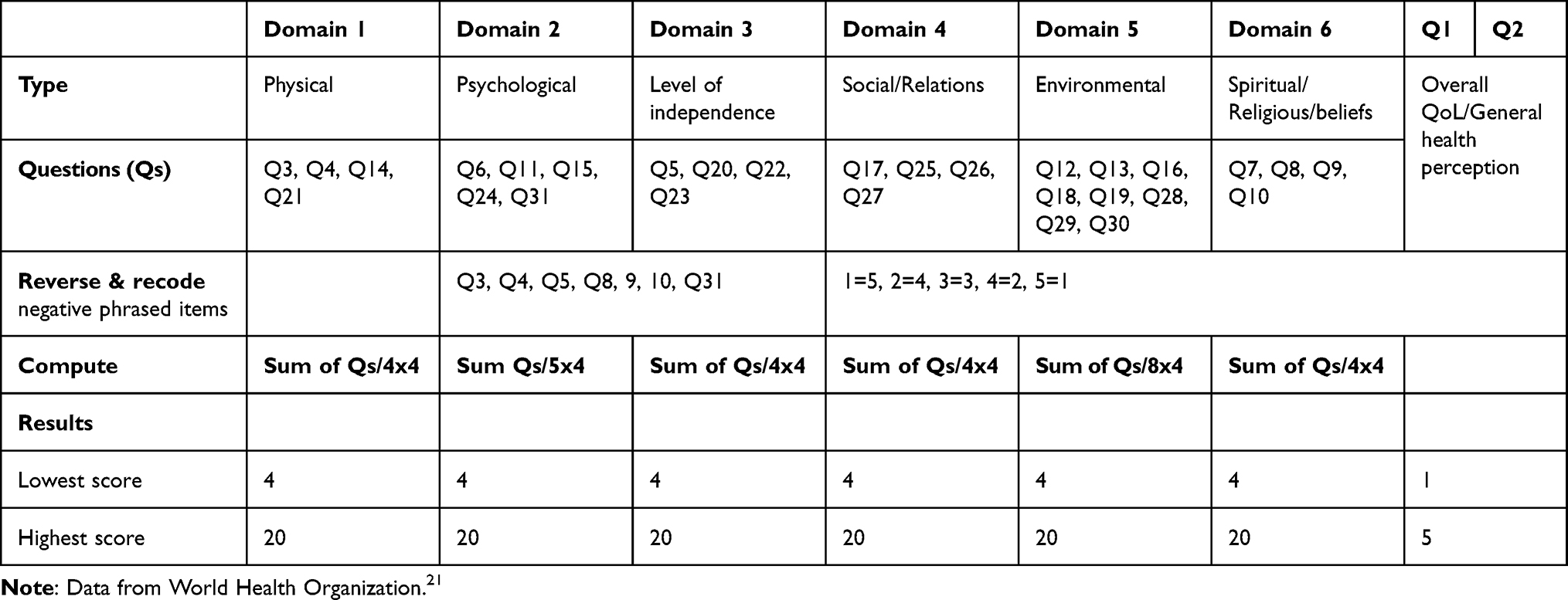 |
Table 1 WHO Quality of Life HIV-Bref Instrument |
In the present study, a valid and a reliable literary Arabic version of the questionnaire was used.33–35 Two authors, L.B & I.K conducted a pilot study including 32 clients to test the questionnaire and improve any ambiguities. In fact, illiterate individuals or individuals having a low level of education (primary school) have been assisted to answer the questionnaire.
Statistical Analysis
Data analysis was performed using SPSS vs 21.0 software (Statistical Package for Social Sciences) for windows. Results were reported as frequencies, and means (±standard deviation). Independent t-test for dichotomous variables and one-way ANOVA for ordinal and nominal variables were used to assess differences in means’ QoL in relation to independent variables. Linear regression analysis was performed in enter method to evaluate the association of independent variables (predictors) with all QoL domains (dependent). The confidence interval was set at 95% and therefore the results were considered significant when p < 0.05.
Results
Male individuals were predominant (74.3%) comparing to female (25.7%) with a sex ratio of 3.12. The mean age was 39.20±10.18 years old. Nearly 60% of the clients (58.09%) were aged in the 15–40 age group and slightly more than 40% (41.91%) were aged more than 40 years. As for education level, 37.1% and 34.3% of the clients had a secondary and a university level, respectively. Almost equal percentages were noted between single (41%) and married people (40%). Most of the clients live in an urban area (71.4%) and only 33.4% are owner of their house. Indeed, more than half (53.3%) of the population have no job. When asking clients about their health status and whether they see a psychologist, 55.2% qualified their health status as “neither poor not good” and 82.9% denied being followed by a psychologist. Moreover, only one member of a family (39%) or a friend (43.8%) was informed about client’s HIV status. Regarding symptoms, the majority (90.6%) of the clients reported no HIV-related symptoms and 60.9% of respondents did not consider themselves ill. The mean period of seropositivity was 10.24±7.77 years. Nearly 60% of the individuals were diagnosed as HIV positive in a period ranged between 1 and 10 years. CD4 T lymphocytes count was available for 88 clients with a mean of 618.72±291.56 cells/mm3. Slightly more than 60% (61%) had a CD4 count >500 cells/mm3 and only 4 clients (4.5%) had a CD4 count <200/mm3. The most frequent mode of HIV transmission was heterosexual with a man or a woman, 40% and 36.2%, respectively. People using intravenous drugs were recorded in only 11.4% (Table 2).
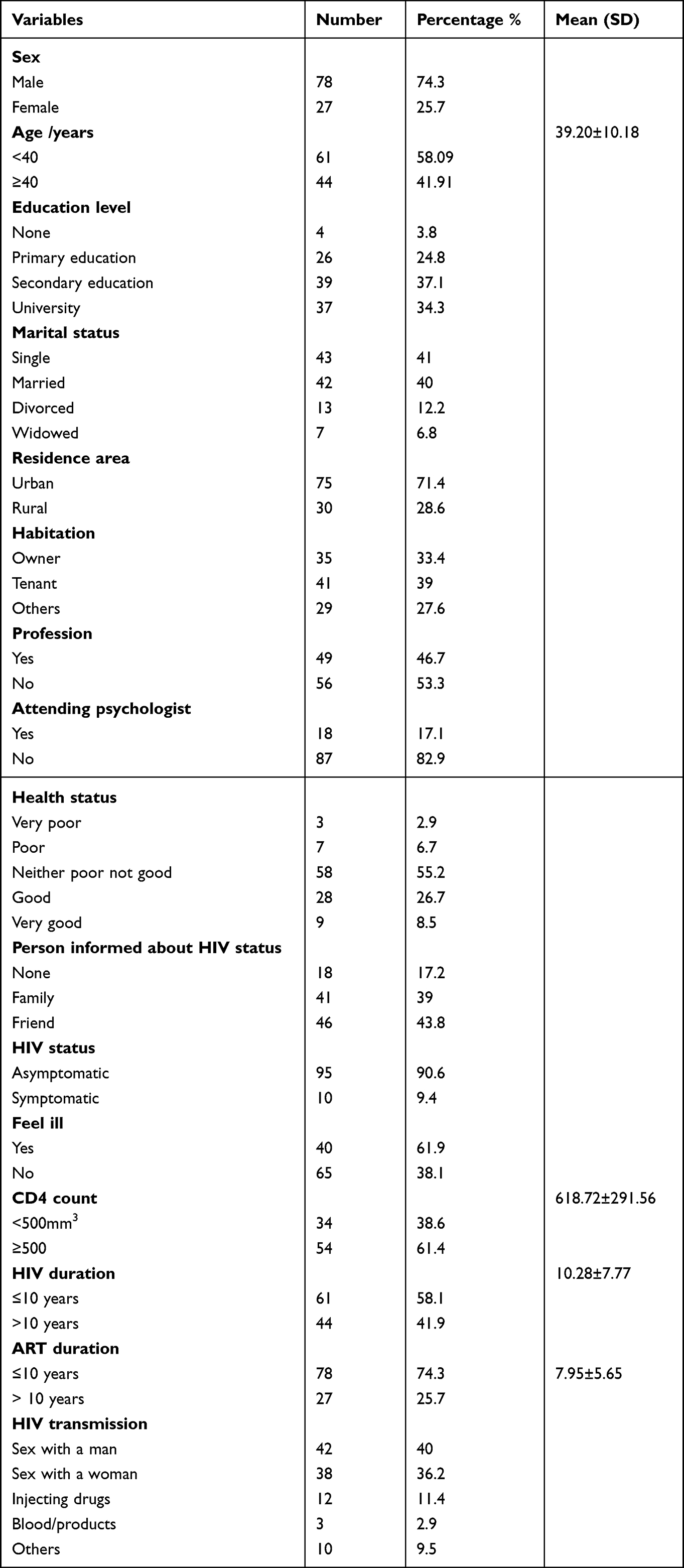 |
Table 2 People Living with HIV Personal Data and Clinical Determinants (n = 105) |
The results of QoL domains and the overall QoL as well are depicted in Table 3. The mean score for all domains was 13.30±3.50. The lowest means were seen with the environment (12.34±2.90), social relations (12.58±3.94) and psychological domains (12.76±3.31) and the highest mean scores were noted for the level of independence (13.98±3.57), the physical (14.11±3.52) and the spiritual domains (14.05±3.78). Mean scores for the overall QoL and general health perception were 3±.92 and 3.41±1.08, respectively.
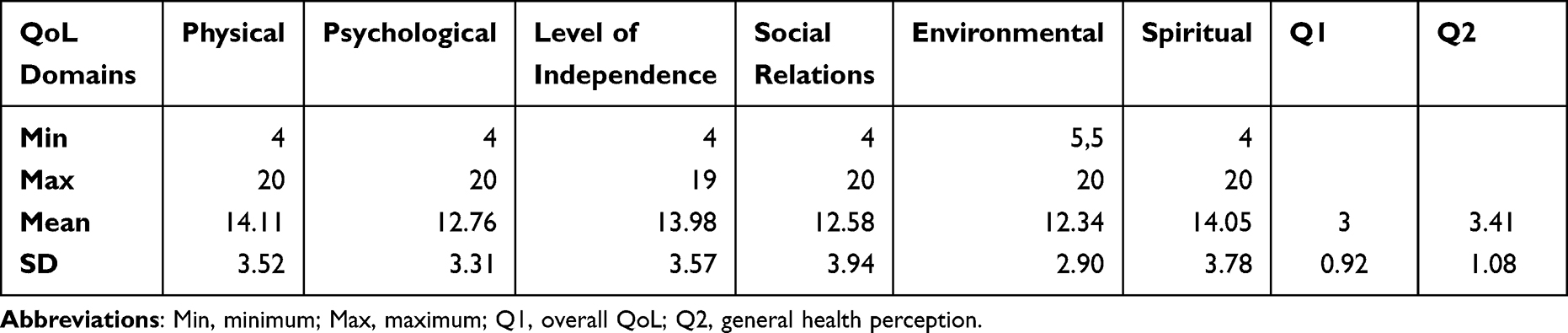 |
Table 3 Means and SD of Quality of Life Domains |
As for the association between the mean scores of QoL domains and the clients’ socio-demographic features and some disease-related variables, the Student’s t-test for independent samples showed a significant association between profession and QoL domains. Higher means in physical, psychological, level of independence, and environmental domains were seen in clients with a job compared to those with no job. Indeed, individuals who did not consider themselves ill presented significantly higher mean scores in all QoL domains (Table 4).
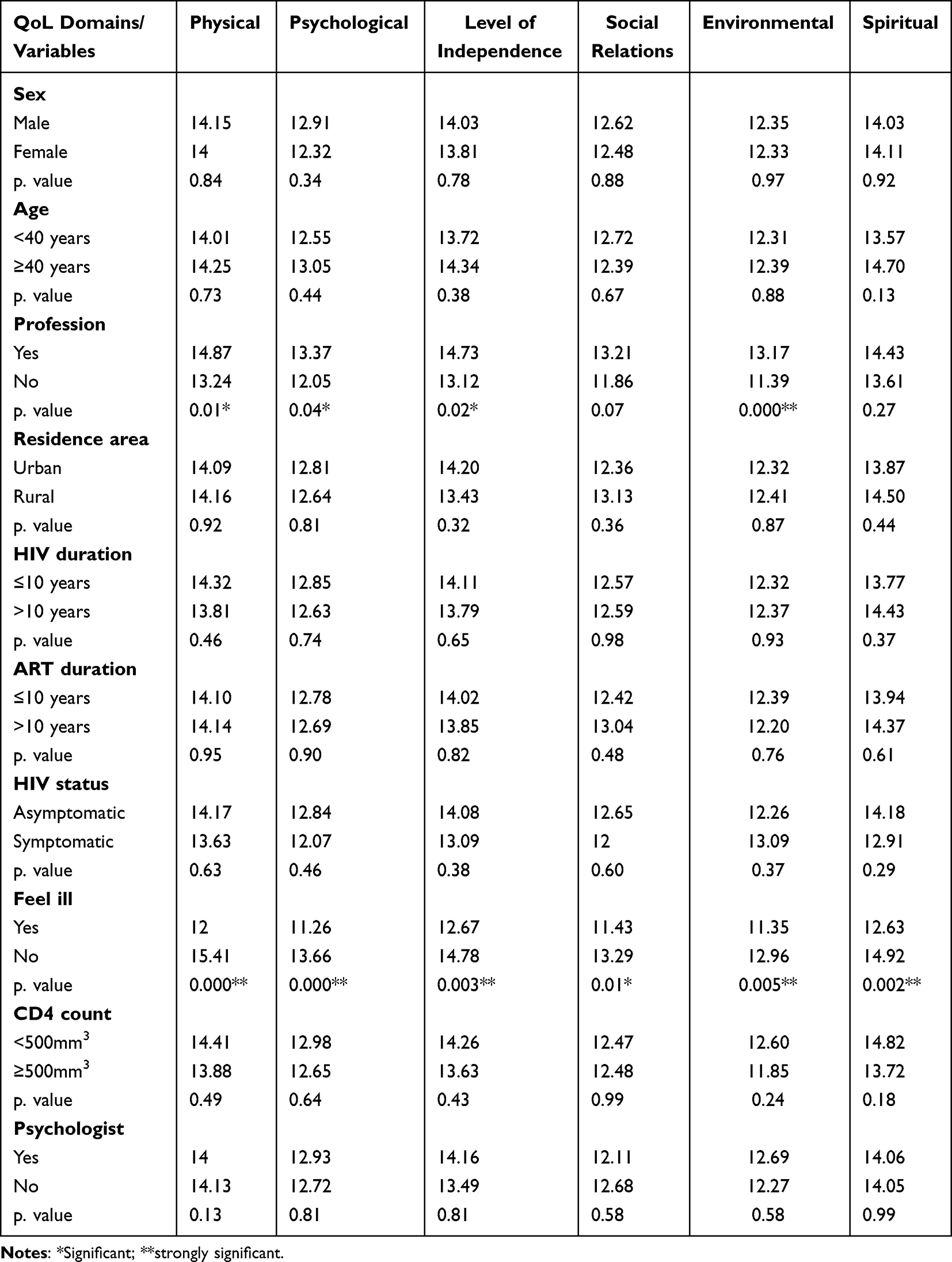 |
Table 4 Mean Differences in QoL Domains Using Independent t-Test in PLHIV (n = 105) |
The one-way ANOVA analysis showed a strong association between the education level and the physical domain, the level of independence and the environmental domains, a significant association between the marital status and all QoL domains except for the psychological domain and a strong association of the clients’ health status and all QoL domains (Table 5).
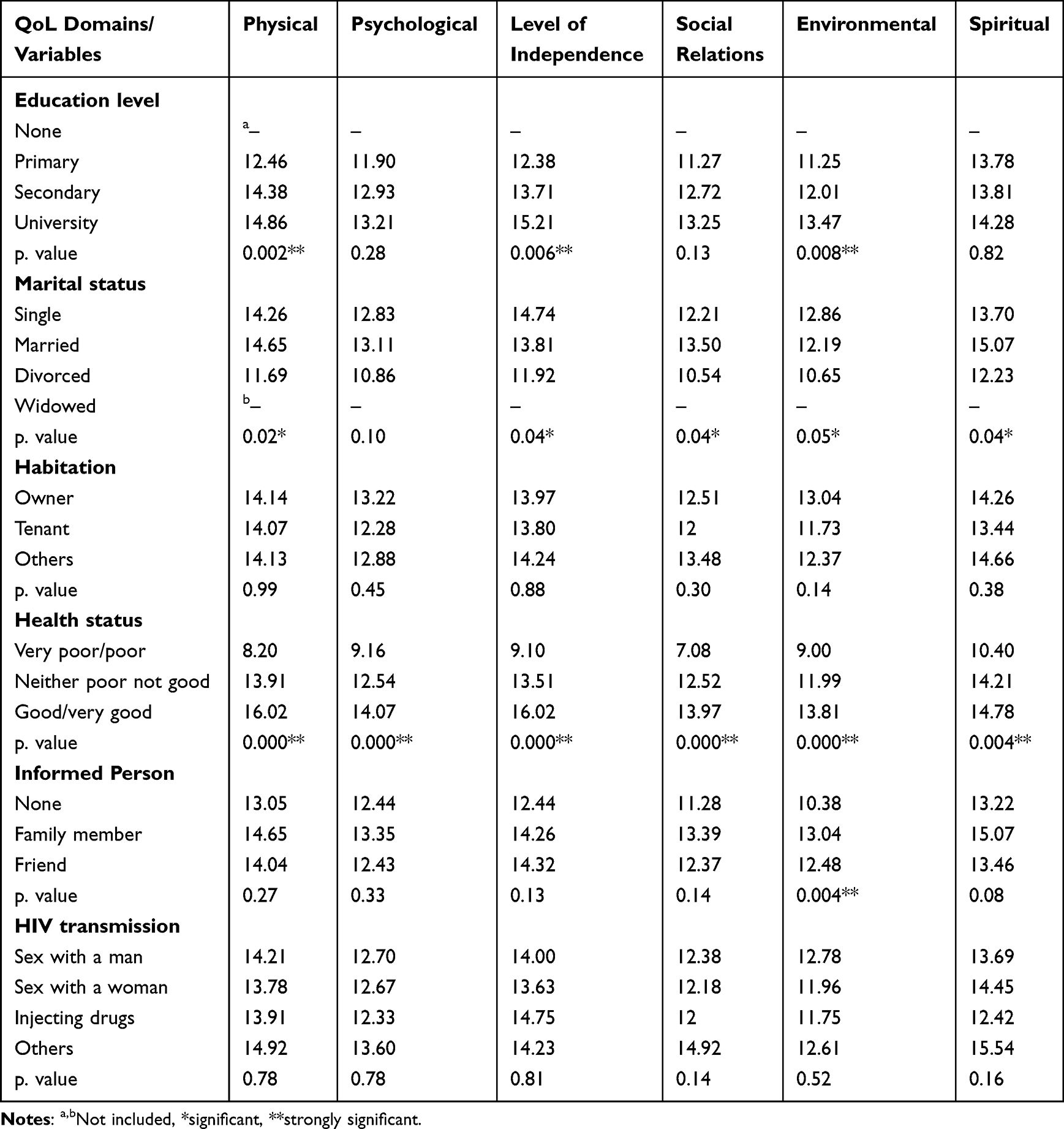 |
Table 5 Mean Differences in QoL Domains in PLHIV Using One-Way ANOVA (n = 105) |
Results of multiple linear regression analysis (Table 6) showed that all QoL models were statistically significant (p = 0.000). Health status and feeling healthy were found to be strong predictive independent variables associated with all QoL domains (p = 0.000). Indeed, profession, an informed person about the client’s HIV status as well as marital status were significant predictors associated with the environmental and the spiritual domains (p < 0.05) (Table 6).
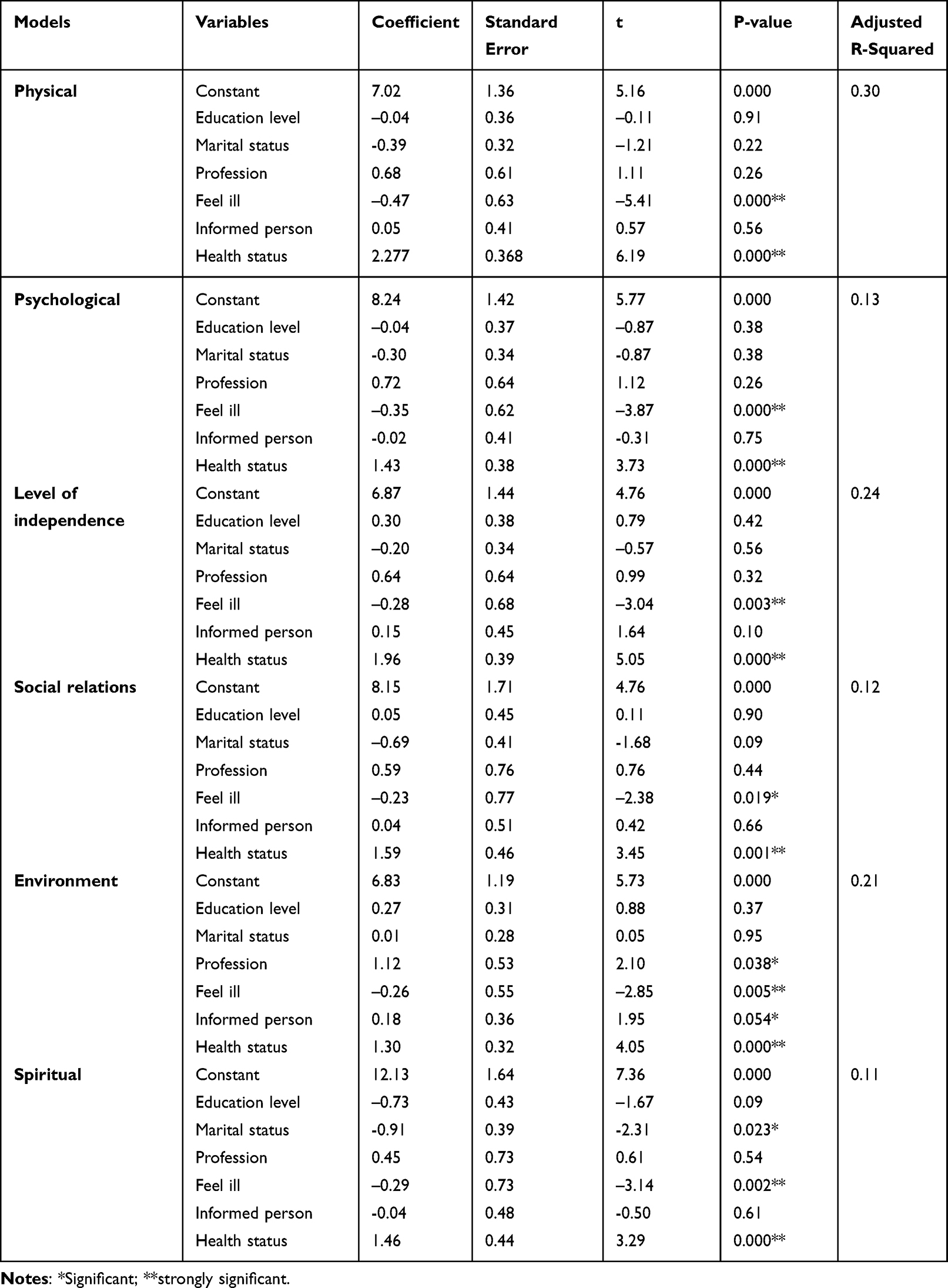 |
Table 6 Multiple Linear Regression Analysis |
Discussion
Our study included a higher number of PLHIV under ART compared to what was reported in the literature.26,34 To our best knowledge, this is the first study in the Maghreb and amongst the fewest in the MENA region. The scarcity of data in this region could be attributed to social, culture and religious stigma or stereotypes about HIV/AIDS disease, condition that breeds silence about this illness.19,26–28,36
As defined by the WHO, QoL refers to the well-being of the individual in the society.20
The present study aimed at assessing PLHIV perception of QoL determinants, in the region of Monastir. Tunisia. Although moderate, the overall mean scores of QoL domains were higher than that reported by Khademi et al. In Iran,10 but lower compared to the study of Osei-Yeboah et al in Ghana,25 Busi et al in Cameroon,29 Liping et al in China37 and Nobre et al in Finland.38 In fact, the lowest mean scores of QoL were recorded for the social relations, the environment and the psychological domains and the highest mean scores were noted for the physical, the level of independence and the spiritual domains. These findings were comparable to studies conducted in Ethiopia with clients receiving highly active antiretroviral therapy.14 It is very clear in the literature that people receiving ART have better physical function that may impact their level of independence. These findings were reported either for people already receiving ART14,22,25,29,30,34 or after ART initiation at 1–4 months31 or at one year.13
We may conclude that the absence of symptoms in the majority of individuals in the present study (90.6%), the high level of CD4 T lymphocytes (≥500/mm3, 61.4%) and the duration of ART (>10 years, 41.9%) could be attributable to the close clinical and biological monitoring of these clients and the very good adherence to ART thanks to efficient counselling services, thus preventing opportunistic infections and AIDS-related deaths31,39,40 even if no significant association was recorded with QoL domains.
However, our findings revealed significantly higher mean scores of almost all QoL domains in people with a high level of education (university), having a job, being married, do not consider themselves ill and reported a good/very good health status. These results are in line with several reports.13,14,22,25,29–31,34 In fact, poor QoL scores have been related to unemployed clients facing financial issues negatively affecting their social relationships, low level of independence resulting in less leisure opportunities affecting their mental health; in addition to poor health status perception, celibacy and a low level of education. Similarly, in Jordan, marital status (single), co-morbidities, unemployment influence negatively people’s QoL34 and in Lebanon, the lowest domain scores were for financial status, sexual functioning, and mental health.26 Indeed, ART naive clients, and clients with HIV/AIDS symptoms have significantly poorer QoL.25
As for regression analysis, marital status, health status, profession, feeling healthy, and having a confident either a friend or a member of the family was found to be strong predictors of QoL. Health status and feeling healthy were significantly related to all QoL domains. Nearly 60% of the population reported their health status as being “neither poor not good”. This in between perception (not very poor not very good), even if it indicates a fairly positive perception, may refer to the following spiritual and religious beliefs (fate) in the Tunisian individual in general, and PLHIV, in particular, with the following statements: “Thank God, I’m still alive” or “it’s God’s will”. Unlike Campos et al31 and Busi et al29 who reported higher percentages of clients qualifying their health status as “very good/good”, 66.4% and 71.8%, respectively.
Finally, the highest scores recorded for the spiritual domain corroborate the results of other authors.10,24,26,35 As PLHIV feel guilty and bear by themselves the burden of the disease, with no family, social and psychological supports; religion may help them reconstruct their relation with Allah/God; in order to cope with their condition and “accept” to live with their diagnosis. In Tunisia, HIV/AIDS is still considered as a “punishment” from Allah/God because of people’s sexual misconduct. Most of the studied clients were isolated and still live with the fear and the shame to be recognized as “dangerous and undesirable individuals” for the community.27 Unfortunately, only one member of a family (39%) or a friend (43.8%) was informed about their HIV status. This situation clearly denotes that cultural and religious stigmas could be the main barriers for people to access health care services and to be diagnosed and treated at an early stage. In fact, in some developing countries, a high mortality rate is still reported (51%), despite the progress of HIV research and considerable achievements in treatments.40 Several studies have been conducted to raise the issue of anxiety, depression and discriminatory behaviour related to stigma.15,41 These studies revealed that the efficacy of ART, good adherence and observance to treatment should be accompanied by rigorous social and psychological interventions.14,42,43 Because of the stigma-related to psychologists, 82.9% of the studied clients were being deprived of psychotherapy.
It is precisely in that direction that the following interventions and measures should be undertaken by policymakers, health-sector professionals and civil society:44–50
- Strengthen education on HIV/AIDS disease, by using modern information and communication technologies;12
- Identify key populations and ensure equitable access to prevention and social protection;
- Promote inclusive governance for health;12
- Raise peoples’ awareness on WHO QoL and well-being and their role to contribute in improving QoL determinants;
- Conduct rigorous research to better collect and analyse data related to QoL in PLHIV;
- Implement the international charter of human rights.51
Strengths and Limits of the Study
This first study conducted in Monastir-Tunisia, allows us to understand determinants of health-related QoL of PLHIV. Indeed, comparable results with literature reports prove the importance and the need to explore in-depth socio-psychological determinants and take rigorous actions to improve peoples’ QoL. In fact, bias due to the lack of clients’ reliable responses may be related to stigma, cultural and social barriers. Moreover, responses obtained by assisted clients who do not understand literary Arabic could be affected, but we think that their limited number (n = 15) has no significant impact on the overall QoL results. It is worth mentioning that literary Arabic version of WHOQOL-Bref, with no cultural adaptations, is applicable in almost all Arabic countries.33 Major limitations of this cross-sectional study are related to information bias and to the difficulty in establishing a causal inference.52 Finally, further investigations involving more participants in other regions of Tunisia should be conducted to better assess anxiety and depression related to stigma and discrimination.
Conclusion
The overall QoL determinants for PLHIV in the department of Infectious diseases of Monastir, Tunisia were moderate. Low scores of QoL were recorded for psychological, social and environmental domains, and moderate scores were recorded for physical, level of independence and religious/spiritual domains. The absence of symptoms and the relatively good physical health could be related to a close clinical and biological monitoring of the clients and effective counselling techniques. However, family and social stigma, disclosure and law criminalization, as well, are the main barriers leading to patients’ psychological, social and environmental discomfort that affect their daily life. Therefore, all efforts should be implemented by policy decision makers; along with health care professionals and the civil society to combat stigma and defend the right for PLHIV to live decently with dignity and enjoy the full range of guaranteed human rights.
Abbreviations
HIV/AIDS, Human immunodeficiency virus/Acquired immunodeficiency syndrome; PLHIV, people living with HIV; QoL, quality of life; WHO, World Health Organization; ART, antiretroviral therapy.
Data Sharing Statement
All data are displayed in the manuscript. They are available and could be sent upon request from the corresponding author.
Ethics Approval and Informed Consent to Participate
The present study is part of Latifa Berrezouga research project on PLHIV that was approved by the committee of ethics of the faculty of pharmacy, University of Monastir, Tunisia under the reference CER-SVS/ISBM 013/2020. Informed consent was obtained from every participant with respect to the Helsinki declaration.
Acknowledgments
The authors gratefully acknowledge all participants enrolled in the study, the nurses, the pharmacist, the psychologist, the social assistant and the medical secretaries for their precious support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The International Association for Dental, Oral, and Craniofacial Research (IADR, www.iadr.org) funds this study in the context of the Regional Development Program Award (18,290 USD) in 2021.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. The Joint United Nations Programme on HIV/AIDS. UNAIDS Data 2021. Available from: https://www.unaids.org/en/resources/fact-sheet.
2. The Joint United Nations Programme on HIV/AIDS. UNAIDS 2019: COVID-19 and HIV. Available from: http://www.unaids.org/en/covid19.
3. WHO/UNAIDS Data; 2020. Available from: http://www.unaids.org/en/resources/documents/2020/unaids-data-2020.
4. Abu-Raddad LJ, Akala FA, Semini I, Riedner G, Wilson D, Tawil O. Characterizing the HIV/AIDS epidemic in the Middle East and North Africa: time for strategic action. World Bank © World Bank; 2010. License: CC BY 3.0 IGO. Available from: https://openknowledge.worldbank.org/handle/10986/2457.
5. Shakiba E, Ramazani U, Mardani E, et al. Epidemiological features of HIV/AIDS in the Middle East and North Africa from 1990 to 2017. Int J STD AIDS. 2021;32(3):257–265. doi:10.1177/0956462420960632
6. Mumtaz GR, Chemaitelly H, Abu-Raddad LJ. The HIV epidemic in the Middle East and North Africa: key lessons. In: Laher I, editor. Handbook of Healthcare in the Arab World. Cham: Springer; 2021. doi:10.1007/978-3-030-36811-1_139
7. Mumtaz GR, Awad SF, Feizzadeh A, Weiss HA, Abu‐Raddad LJ. HIV incidence among people who inject drugs in the Middle East and North Africa: mathematical modelling analysis. J Intern AIDS Soc. 2018;21(3):e25102. doi:10.1002/jia2.25102
8. Najafi F, Shadmani FK, Ghalandari M, Darbandi M. Disability-adjusted life years and mortality rate attributed to unsafe sex and drug use for AIDS in the Middle East and North African countries. Arch Public Health. 2020;78(1):130. doi:10.1186/s13690-020-00511-1
9. Daw MA, Ahmed MO. Epidemiological characterization and geographic distribution of human immunodeficiency virus/acquired immunodeficiency syndrome infection in North African countries. World J Virol. 2021;10(2):69–85. doi:10.5501/wjv.v10.i2.69
10. Khademi N, Zanganeh A, Saeidi S, et al. Quality of life of HIV-infected individuals: insights from a study of patients in Kermanshah, Iran. BMC Infect Dis. 2021;21(1):203. doi:10.1186/s12879-021-05908-z
11. The Joint United Nations Programme on HIV/AIDS. UNAIDS Data. Country factsheets-Tunisia; 2022. Available from: https://www.unaids.org/en/regionscountries/countries/tunisia.
12. United Nations Development Programme NDP. HIV and Health Annual Report 2021–2022 HIV and Health in Times of Crisis. Available from: https://www.undp.org/sites/g/files/zskgke326/files/2023-03/UNDP-HIV-and-Health-Annual-Report-2021-2022.pdf.
13. Dutra BS, Lédo AP, Lins-Kusterer L, Luz E, Prieto IR, Brites C. Changes health-related quality of life in HIV-infected patients following initiation of antiretroviral therapy: a longitudinal study. Braz J Infect Dis. 2019;23(4):211–217. doi:10.1016/j.bjid.2019.06.005
14. Surur AS, Teni FS, Wale W, Ayalew Y, Tesfaye B. Health related quality of life of HIV/AIDS patients on highly active anti-retroviral therapy at a university referral hospital in Ethiopia. BMC Health Serv Res. 2017;17(1):737. doi:10.1186/s12913-017-2714-1
15. Ben Moussa A, Delabre RM, Villes V, et al. Determinants and effects or consequences of internal HIV-related stigma among people living with HIV in Morocco. BMC Public Health. 2021;21(1):163. doi:10.1186/s12889-021-10204-1
16. Rahmati‐Najarkolaei F, Niknami S, Aminshokravi F, et al. Experiences of stigma in healthcare settings among adults living with HIV in the Islamic Republic of Iran. J Int AIDS Soc. 2010;13(1):27. doi:10.1186/1758-2652-13-27
17. Igwe MN, Ndukuba AC, Olose EO, et al. Psychological distress and quality of life of people living with HIV/AIDS in a Nigerian teaching hospital. Ment Health Religion Culture. 2016;19(9):961–971. doi:10.1080/13674676.2017.1287166
18. Demirel OF, Mayda PY, Yıldız N, et al. Self-stigma, depression, and anxiety levels of people living with HIV in Turkey. Eur J of Psychiat. 2018;32(4):182–186. doi:10.1016/j.ejpsy.2018.03.002
19. Al Madhani A, Al Harthi L, Balkhair A, et al. Prevalence and correlates of depressive symptoms among people living with HIV attending tertiary care hospitals in Oman. Pan Afr Med J. 2020;37:90. doi:10.11604/pamj.2020.37.90.23294
20. World Health Organization. WHOQOL: Measuring quality of life. Available from: https://www.who.int/tools/whoqol.
21. World Health Organization. WHOQOL-HIV BREF. Department of mental health and substance dependence, CH-1211 Geneva 27, Switzerland; 2002. Available from: https://www.who.int/mental_health/media/en/613.pdf.
22. Suryana K, Suharsono H, Joenputri N. Factors associated with quality of life among people living with HIV/AIDS on highly active anti-retroviral therapy: a cross-sectional study. Int J Pharm Pharm Sci. 2020;36–40. doi:10.22159/ijpps.2020v12i9.38628
23. Ghiasvand H, Waye KM, Noroozi M, Harouni GG, Armoon B, Bayani A. Clinical determinants associated with quality of life for people who live with HIV/AIDS: a Meta-analysis. BMC Health Serv Res. 2019;19(1):768. doi:10.1186/s12913-019-4659-z
24. Passos SMK, de M SLD. An evaluation of quality of life and its determinants among people living with HIV/AIDS from Southern Brazil. Cad Saúde Pública. 2015;31(4):800–814. doi:10.1590/0102-311X00000514
25. Osei-Yeboah J, Owiredu WKBA, Norgbe GK, et al. Quality of life of people living with HIV/AIDS in the Ho Municipality, Ghana: a cross-sectional study. AIDS Res Treat. 2017;2017:1–7. doi:10.1155/2017/6806951
26. Abboud S, Noureddine S, Huijer HAS, DeJong J, Mokhbat J. Quality of life in people living with HIV/AIDS in Lebanon. AIDS Care. 2010;22(6):687–696. doi:10.1080/09540120903334658
27. Karamouzian M, Akbari M, Haghdoost AA, Setayesh H, Zolala F. “I Am Dead to Them”: HIV-related stigma experienced by people living with HIV in Kerman. Iran J Ass Nurses AIDS Care. 2015;26(1):46–56. doi:10.1016/j.jana.2014.04.005
28. Maleki MR, Derakhshani N, Azami-aghdash S, Naderi M, Nikoomanesh M. Quality of life of people with HIV/AIDS in Iran: a systematic review and meta-analysis. Iran J Public Health. 2020;49(8):1399–1410. doi:10.18502/ijph.v49i8.3861
29. Busi AN, Nsoh M, Otieno MO, Ndeso SA, Halle-Ekane GE. Evaluation of quality of life and associated factors among HIV patients on antiretroviral therapy in North West region of Cameroon. Afr H Sci. 2021;21(1):8–17. doi:10.4314/ahs.v21i1.3S
30. Onyekonwu CL, Onyeka TC, Brenda NC, et al. Chronic HIV infection and health related quality of life in resource poor settings - an assessment from South East Nigeria. Afr H Sci. 2020;20(1):102–113. doi:10.4314/ahs.v20i1.15
31. Campos LN, César CC, Guimarães MDC. Quality of life among HIV-infected patients in Brazil after initiation of treatment. Clinics. 2009;64(9):867–875. doi:10.1590/S1807-59322009000900007
32. Strengthening the reporting of observational studies in epidemiology. STROBE Checklist for cross-sectional studies. Available from: https://www.strobe.statement.org/.
33. Eljedi A, Mikolajczyk RT, Kraemer A, Laaser U. Health related quality of life in diabetic patients and controls without diabetes in refugee camps in the Gaza strip: a cross-sectional study. BMC Public Health. 2006;6(1):268. doi:10.1186/1471-2458-6-268
34. Algaralleh A, Altwalbeh D, Al-Tarawneh F. Health-related quality of life among persons living with HIV/AIDS in Jordan: an exploratory study. HIV. 2020;64:897–907. doi:10.2147/HIV.S277941
35. Al Sayah F, Ishaque S, Lau D, Johnson JA. Health related quality of life measures in Arabic speaking populations: a systematic review on cross-cultural adaptation and measurement properties. Qual Life Res. 2012;22(1):213–229. doi:10.1007/s11136-012-0129-3
36. Omer T, Lovering S, Al Shomrani M. The lived experience of living with HIV/AIDS in the western region of Saudi Arabia. Div Equal Health Care. 2014;11:215–223.
37. Liping M, Peng X, Haijiang L, Lahong J, Fan L. Quality of life of people living with HIV/AIDS: a cross-sectional study in Zhejiang province, China. PLoS One. 2015;10(8):e0135705. doi:10.1371/journal.pone.0135705
38. Nobre N, Pereira M, Roine RP, Sintonen H, Sutinen J. Factors associated with the quality of life of people living with HIV in Finland. AIDS Care. 2017;29(8):1074–1078. doi:10.1080/09540121.2017.1281879
39. Sari PI, Martawinarti RN, Lataima NS, Berhimpong VM. The quality of life of patients with HIV/AIDS undergoing antiretroviral therapy. A systematic review. J Ners. 2019;14(3):50–54. doi:10.20473/jn.v14i3.16978
40. Hamarsheh O. HIV/AIDS in Palestine: a growing concern. Int J of Infect Dis. 2020;90:18–20. doi:10.1016/j.ijid.2019.10.019
41. Hipolito RL, Oliveira de DC, Costa da TL, Marques SC, Pereira ER, Gomes AMT. Quality of life of people living with HIV/AIDS: temporal, socio-demographic and perceived health relationship. Rev Latino-Am Enfermagem. 2017;20(25):e2874.
42. Mohamed Boushab B, Fall-Malick F-Z, Ould Cheikh Melaïnine ML, Basco LK. Forms of stigma and discrimination in the daily lives of HIV-positive individuals in Mauritania. Open AIDS J. 2017;11(1):12–17. doi:10.2174/1874613601711010012
43. Desai KT, Patel PB, Verma A, Bansal R. Environment and psychosocial factors are more important than clinical factors in determining quality of life of HIV-positive patients on antiretroviral therapy. Trop Doct. 2020;50(3):180–186. doi:10.1177/0049475520908180
44. Lindayani L, Chen Y-C, Der Wang J, Ko N-Y. Complex problems, care demands, and quality of life among people living with HIV in the Antiretroviral Era in Indonesia. J Assoc Nurses AIDS Care. 2018;29(2):300–309. doi:10.1016/j.jana.2017.10.002
45. Mak WWS, Mo PK, Ma GY, Lam MY. Meta-analysis and systematic review of studies on the effectiveness of HIV stigma reduction programs. Soc Sci Med. 2017;188:30–40. doi:10.1016/j.socscimed.2017.06.045
46. Joulaei H, Shooshtarian S, Dianatinasab M. Is UNAIDS 90-90-90 Target a dream or a reality for Middle East and North Africa Region on endingThe AIDS epidemic? A Review study. AIDS Rev. 2019;20(2):772. doi:10.24875/AIDSRev.M18000020
47. Vu GT, Tran BX, Hoang CL, et al. Global research on quality of life of patients with HIV/AIDS: is it socio-culturally addressed? IJERPH. 2020;17(6):2127. doi:10.3390/ijerph17062127
48. Stangl AL, Lilleston P, Mathema H, et al. Development of parallel measures to assess HIV stigma and discrimination among people living with HIV, community members and health workers in the HPTN 071 (PopART) trial in Zambia and South Africa. J Int AIDS Soc. 2019;22(12):e25421.
49. Mengistu N, Hareru HE, Shumye S, et al. Health related quality of life and its association with social support among people living with HIV/AIDS receiving antiretroviral therapy in Ethiopia: a systematic review and meta-analysis. Health Qual Life Outcomes. 2022;20(1):77. doi:10.1186/s12955-022-01985-z
50. Bannazadeh Baghi H, Soroush MH. HIV/AIDS in the Middle East and North Africa: a positive future. Sex Transm Infect. 2018;94(5):339. doi:10.1136/sextrans-2018-053695
51. The Joint United Nations Programme on HIV/AIDS. UNAIDS: Human rights. Available from: https://www.unaids.org/en/topic/rights.
52. Wang X, Cheng Z. Cross-sectional studies. Strengths, weaknesses, and recommendations (Supplement). Chest. 2020;158(1):S65–71. doi:10.1016/j.chest.2020.03.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.