Back to Journals » Nature and Science of Sleep » Volume 17

Proteome Profiling Identifies CDH2 as a Potential Screening Marker for NAFLD and Liver Fibrosis in the Snoring Population
Authors Huang S, Deng X, Chen J, Huang J ![]() , Xie H, Wang B, Lian N
, Xie H, Wang B, Lian N
Received 29 April 2025
Accepted for publication 23 September 2025
Published 14 October 2025 Volume 2025:17 Pages 2669—2680
DOI https://doi.org/10.2147/NSS.S532717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marco Veneruso
Shiyuan Huang,1,2,* Xiaoyu Deng,1,2,* Jia Chen,1,2 Jiefeng Huang,1,2 Hansheng Xie,1,2 Biying Wang,1,2 Ningfang Lian1,2
1Department of Respiratory and Critical Care Medicine, Respiratory Disease Research Institute, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350005, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, National Regional Medical Center, Binhai Campus of The First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, 350005, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ningfang Lian, Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350005, People’s Republic of China, Tel +86-591-87981698, Email [email protected]
Purpose: Snoring individuals, particularly those with obstructive sleep apnea (OSA), exhibit a higher prevalence of nonalcoholic fatty liver disease (NAFLD) and liver fibrosis. The objectives of this study were to explore potential screening biomarkers for NAFLD and liver fibrosis in the snoring population.
Methods: The research was carried out as a cross-sectional study at the Sleep Center of the First Affiliated Hospital of Fujian Medical University. All patients underwent FibroScan and overnight polysomnography (PSG). The 96-metabolism related proteins were detected using liquid chromatography-high resolution mass spectrometry (Oink Proteomics).
Results: A total of 59 NAFLD were found among the 87 snoring patients. A total of 12 proteins with differential expression levels were identified between non-NAFLD group and NAFLD group via Oink Proteomics. The correlation analysis revealed a close correlation between Cadherin 2 (CDH2) and NAFLD, liver fibrosis (with correlation coefficients of 0.394 and 0.383, respectively, both P < 0.05). The risk of NAFLD and liver fibrosis was much higher in snorers with higher levels of CHD2 compared with snorers with lower levels of CHD2 (both P < 0.05). A combination of CHD2, age, BMI, glucose, AHI and waistline presented the acceptable AUC for the detection of NAFLD and liver fibrosis in snoring patients (0.92, 95% CI: 0.86– 0.98 and 0.81, 95% CI: 0.72– 0.91, respectively, both p < 0.001).
Conclusion: In snoring patients, higher level of CDH2 was identified as a risk factor for NAFLD and liver fibrosis; a combination of CDH2, age, BMI, glucose, AHI and waistline could act as a convenient and effective indicator for screening NAFLD and liver fibrosis. Future research should expand the sample size and conduct multicenter validation to further explore the value of CDH2.
Plain Language Summary: Snoring individuals have an elevated incidence of nonalcoholic fatty liver disease (NAFLD) and liver fibrosis. Oink Proteomics discovered that CDH2 expression was upregulated in individuals with snoring who also have NAFLD. Further analysis revealed that a combination of CDH2, age, Body mass index (BMI), glucose, Apnea hypopnea index (AHI) and waistline could act as a convenient and effective indicator for screening NAFLD and liver fibrosis in snoring patients.
Keywords: obstructive sleep apnea, nonalcoholic fatty liver disease, liver fibrosis, biomarkers, proteome profiling
Introduction
Nonalcoholic fatty liver disease (NAFLD), affecting about 30% of the global population, is a prevalent chronic liver condition that closely related metabolic disorders such as obesity, type 2 diabetes mellitus, and dyslipidaemia.1,2 Obstructive sleep apnea syndrome (OSA), which leads to intermittent hypoxia (IH) and hypercapnia caused by upper airway narrowing and collapse, is a high-risk factor for several metabolic diseases.3 Previous studies have found that NAFLD and liver fibrosis were common in OSA patients. OSA is linked to the development of NAFLD and contributes to the progression of NAFLD.4 In addition to individuals who are obese, NAFLD has a higher incidence even among non-obese snoring populations.5 NAFLD in snoring individuals is receiving increasing attention.
A subset of NAFLD patients with nonalcoholic steatohepatitis (NASH), particularly those with liver fibrosis, are at a high risk of progressing to severe liver complications, such as decompensated cirrhosis, liver cancer, and increased mortality.6 Because the NASH often presents asymptomatically or with mild symptoms in its early stages, a significant number of individuals remain undetected until the condition has advanced to more severe and potentially life-threatening levels, thereby imposing a substantial burden on public health.7 Thus, the timely identification of individuals at high risk for NASH is crucial for initiating timely interventions and effective management strategies. Previous studies have explored the use of simple serological parameters such as the triglyceride glucose index (TyG), platelet-related parameters, etc., to predict NAFLD in snoring populations, but the sensitivity and specificity are not ideal.8,9 It is very necessary to find convenient and efficient serological markers for the early diagnosis of NAFLD.
Olink Proteomics technology utilizes the Proximity Extension Assay (PEA), a high-throughput method that enables the detection of hundreds of proteins with high sensitivity and specificity.10 Previous studies have suggested that snoring populations developed liver metabolic abnormalities through mechanisms such as oxidative stress, leading to the occurrence of NAFLD. So, the metabolism related panel was chosen to search for biomarkers that may predict NAFLD.
This study aims to further investigate a potential screening biomarker for NAFLD and liver fibrosis in the snoring population.
Methods
Study Populations
A cross-sectional study was conducted at the Sleep Center of the First Affiliated Hospital of Fujian Medical University. We enrolled consecutive patients who visited our center with snoring and suspected sleep apnea hypopnea syndrome. The study carried out between December 16, 2023, to August 16, 2024.
The including criteria were as follows: (1) Snoring patients suspected of having sleep apnea hypopnea syndrome. Snoring was defined as self- or partner-reported loud and frequent snoring, ascertained during a face-to-face interview. (2) Age ranged from 18 to 80 years. (3) Underwent Fibroscan during hospitalization. (4) Underwent completed overnight polysomnography for sleep respiratory monitoring. (5) Had complete biochemical examination data. (6) Participants provided informed consent to take part in the study. Individuals with a history of liver cancer, viral hepatitis, alcoholic liver disease, or other chronic liver conditions were not included in the study.
The patients’ medical histories, including conditions such as hypertension and diabetes, were reviewed. Their anthropometric parameters, including height, weight, neck circumference, and waist circumference, were also measured. Fibroscan was performed. At night, the polysomnography respiratory monitoring system (Condi Australia) was used to obtain sleep-related parameters, including AHI (Apnea-Hypopnea Index), ODI (Oxygen Desaturation Index), lowest oxygen saturation, mean oxygen saturation and sleep staging. On the morning after the sleep respiration monitoring ends, we collected fasting blood samples to conduct routine blood tests, assess liver and kidney function, and determine the lipid profile, and Olink proteomics analysis. The TyG index was calculated as Ln[TG (mg/dL) × FBG (mg/dL)/2].
Ethical Approval and Consent to Participate
All participants provided written informed consent prior to the commencement of the study. The study complies with the Declaration of Helsinki, and the research protocol was approved by the Ethics Committee of the First Affiliated Hospital of Fujian Medical University (Approval Number: MRCTA, ECFAH of FMU|2024|690).
Definition of NAFLD and Liver Fibrosis
Hepatic steatosis and liver fibrosis were diagnosed using transient elastography (FibroScan, Echosens, France). The measurements were deemed reliable only under the following conditions: at least 10 valid liver stiffness measurements (LSM) were obtained; participants fasted for a minimum of 3 hours before the examination; and the interquartile range (IQR) to median ratio was less than 30%. Hepatic steatosis was diagnosed when controlled attenuation parameter (CAP) values exceeded 274 dB/m.11 NAFLD was diagnosed based on CAP results. Subjects with excessive alcohol consumption were excluded prior to assessment. Liver fibrosis was defined by LSM thresholds exceeding 7.4 kPa.12
Definition of Apnea, Hypopnea and OSA
The diagnosis of hypopnea, apnea, and OSA was based on the 2017 American Academy of Sleep Medicine (AASM) criteria, which are as follows: AHI of less than 5 events per hour indicates the absence of OSA; AHI between 5 and 14.9 events per hour signifies mild OSA; AHI between 15.0 and 29.9 events per hour indicates moderate OSA; and AHI greater than 30 events per hour denotes severe OSA.
Protein Biomarkers Analysis
Serum samples intended for protein analysis were stored at −80°C until the time of analysis. The analyses were conducted using the Olink Target 96 Metabolism Proteomics platform (Olink Proteomics, Sweden), which is capable of measuring 92 pre-specified metabolism-related proteins. This platform was predicated on the a priori identification of proteins that are hypothesized to play a significant role in the metabolic pathways of interest. This panel was selected to allow for a focused investigation of proteins with established biological relevance to our research question. This platform utilizes Proximity Extension Assay (PEA) technology, involving 92 unique oligonucleotide-labeled antibody-DNA probe pairs designed to bind specifically to target proteins within the samples. The quantification of multiplexed cytokine levels is achieved through real-time polymerase chain reaction (PCR) amplification of DNA from the antibody-DNA pairs, with the number of PCR cycles correlating to the protein concentration in the sample. The results are presented as Normalized Protein Expression (NPX) values, which reflect relative protein concentrations and are comparable to log2-transformed protein concentrations. Proteins with over 90% of their values falling below the lower limit of detection (LOD) were excluded from further analysis.
Statistical Analysis
The normality of continuous variables was assessed using the Kolmogorov–Smirnov test. For continuous variables that did not follow a normal distribution, differences were analyzed using the Mann–Whitney U-test. In contrast, Student’s t-test was employed for normally distributed continuous variables. Categorical variables were presented as percentages and analyzed using the Chi-squared test. Additionally, multivariate logistic regression analysis was conducted to identify independent factors associated with NAFLD and liver fibrosis in patients with snoring. The diagnostic accuracy of CHD2 and the combined prediction index for NAFLD and liver fibrosis in snoring patients were evaluated using receiver operating characteristic (ROC) curve analysis. A p value less than 0.05 was considered statistically significant. All analysis was conducted by R 4.3.2 (https://www.r-project.org/).
Results
Baseline Characteristics of Snoring Patients
The study prospectively screened 107 snoring patients who had undergone FibroScan examination. Exclusion criteria were applied, resulting in the exclusion of 20 patients who did not meet the inclusion criteria, 2 due to not meeting the age criteria, 9 due to incomplete data, 3 with viral hepatitis, 5 with alcoholic liver disease and 1 with liver cancer. A final cohort of 87 patients with complete data was included in the analysis. The flow chart of the study is summarized in Figure 1. The baseline characteristics of these subjects are presented in Table 1. In the entire queue, the median age was 49.00 (range 35.00–59.50) years, 81.6% were male. The prevalence rates for OSA were 97.70% (85/87), with 22.99% (20/87) moderate OSA and 68.97% (60/87) severe OSA respectively. Fifty-nine (67.82%) had NAFLD and 27 (31.03%) had liver fibrosis. Snoring patients with NAFLD had higher levels of necklace, waistline, BMI and liver fibrosis (all p < 0.05). The NAFLD group suffered from more severe OSA (all p < 0.05).
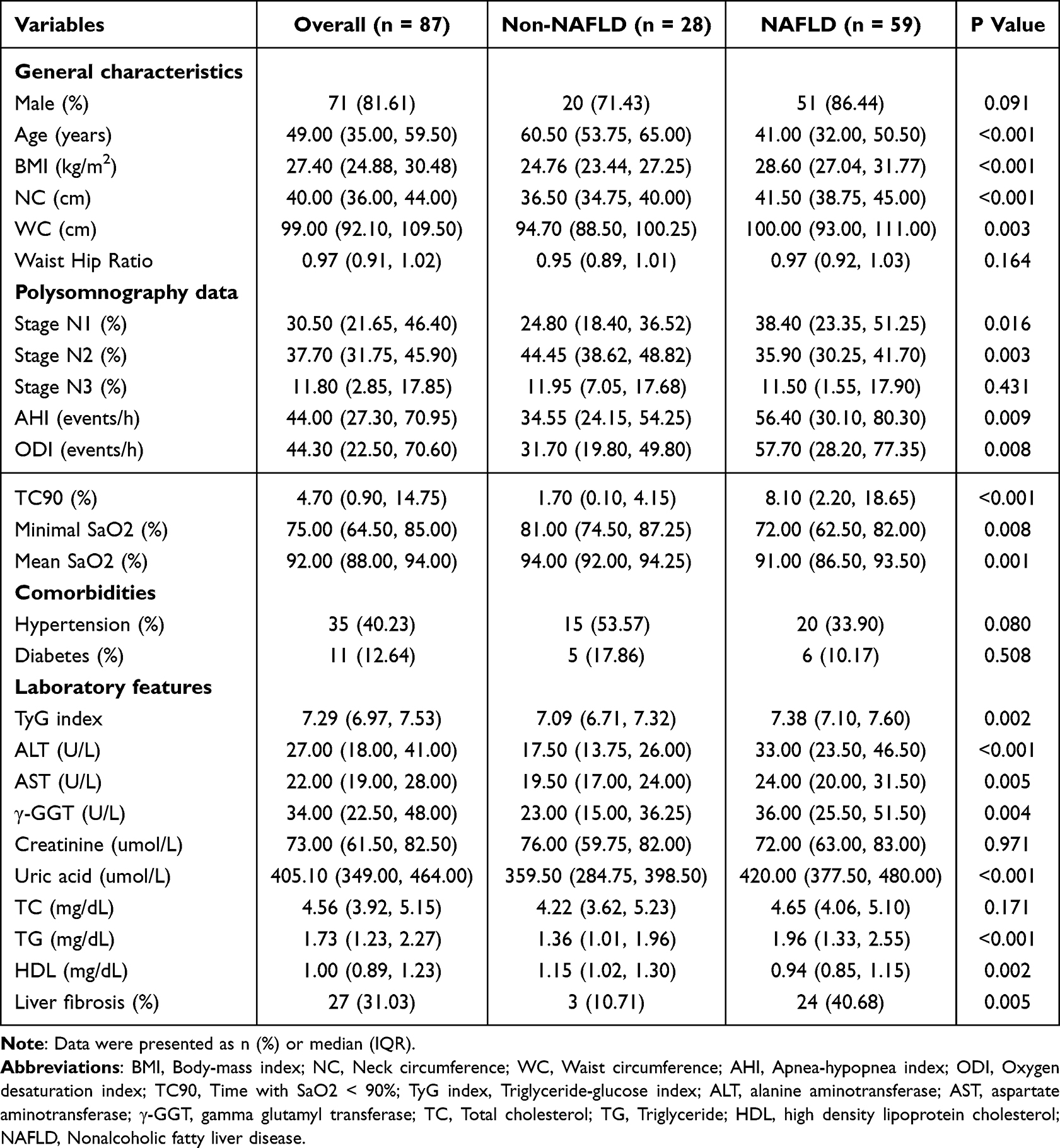 |
Table 1 Clinical and Polysomnographic Characteristics of the Study Population at Baseline |
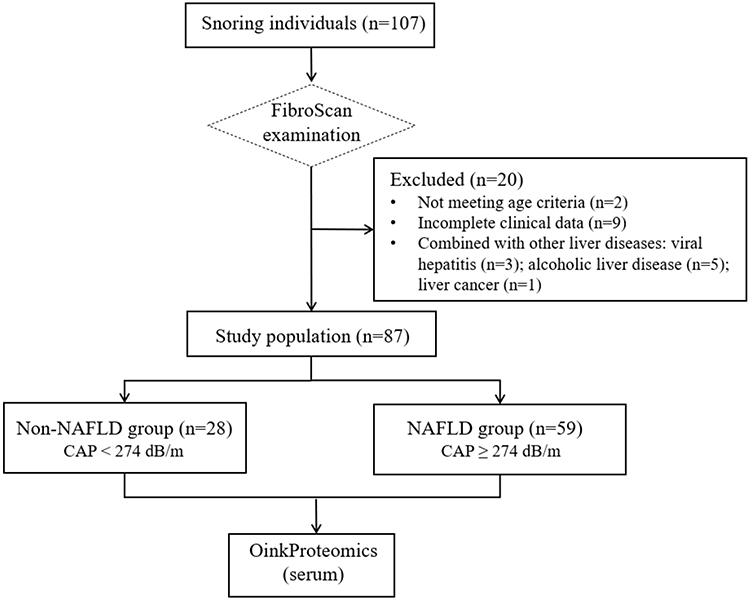 |
Figure 1 Flowchart of the study. |
Identification of CDH2 in the Snoring Patients with NAFLD and Liver Fibrosis
The samples were tested using the Olink metabolism proteomics panel. Ninety-two proteins were quantified in all samples. We identified a total of 12 proteins with different expression levels between the non-NAFLD group and NAFLD group. These proteins include Cadherin-2 (CDH2), Amyloid-like protein 1 (APLP1), Aldehyde Dehydrogenase 1 Family Member A1 (ALDH1A1), Cathepsin O (CTSO), C-type lectin domain family 5 member A (CLEC5A), Ectonucleotide pyrophosphatase/phosphodiesterase family member 7 (ENPP7), Fructose-1,6-bisphosphatase 1 (FBP1), Meprin A subunit beta (MEP1B), Nodal modulator 1 (NOMO1), Reticulon-4 receptor (RTN4R), Scavenger receptor cysteine-rich domain-containing group B protein (SSC4D) and Thimet oligopeptidase (THOP1) (all p < 0.05) (Figure 2). Among these differentially expressed proteins, 10 proteins were up-regulated and 2 proteins were down-regulated. Table 2 showed the correlations between differentially expressed serum proteins and NAFLD, liver fibrosis in snoring patients. The correlation analysis revealed a close correlation between CDH2 and NAFLD, liver fibrosis (with correlation coefficients of 0.394 and 0.383, respectively, both P < 0.05).
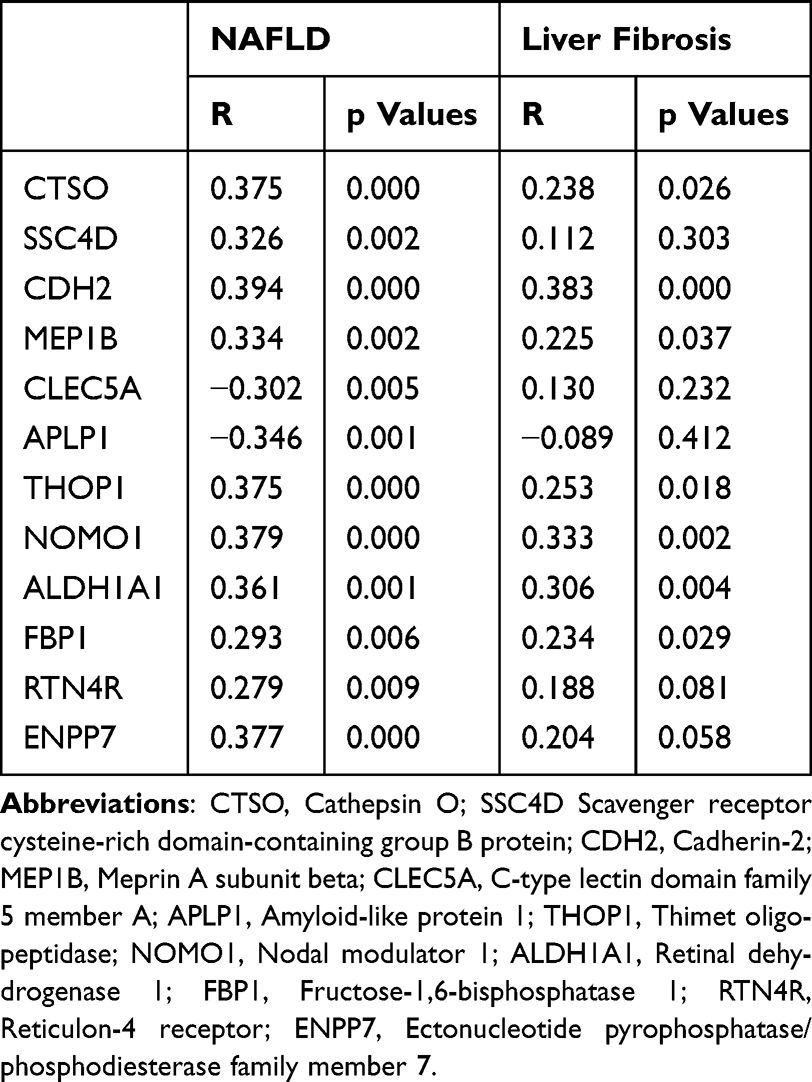 |
Table 2 Spearman’s Rank Correlation Coefficients Between NAFLD and Liver Fibrosis in Snoring Patients |
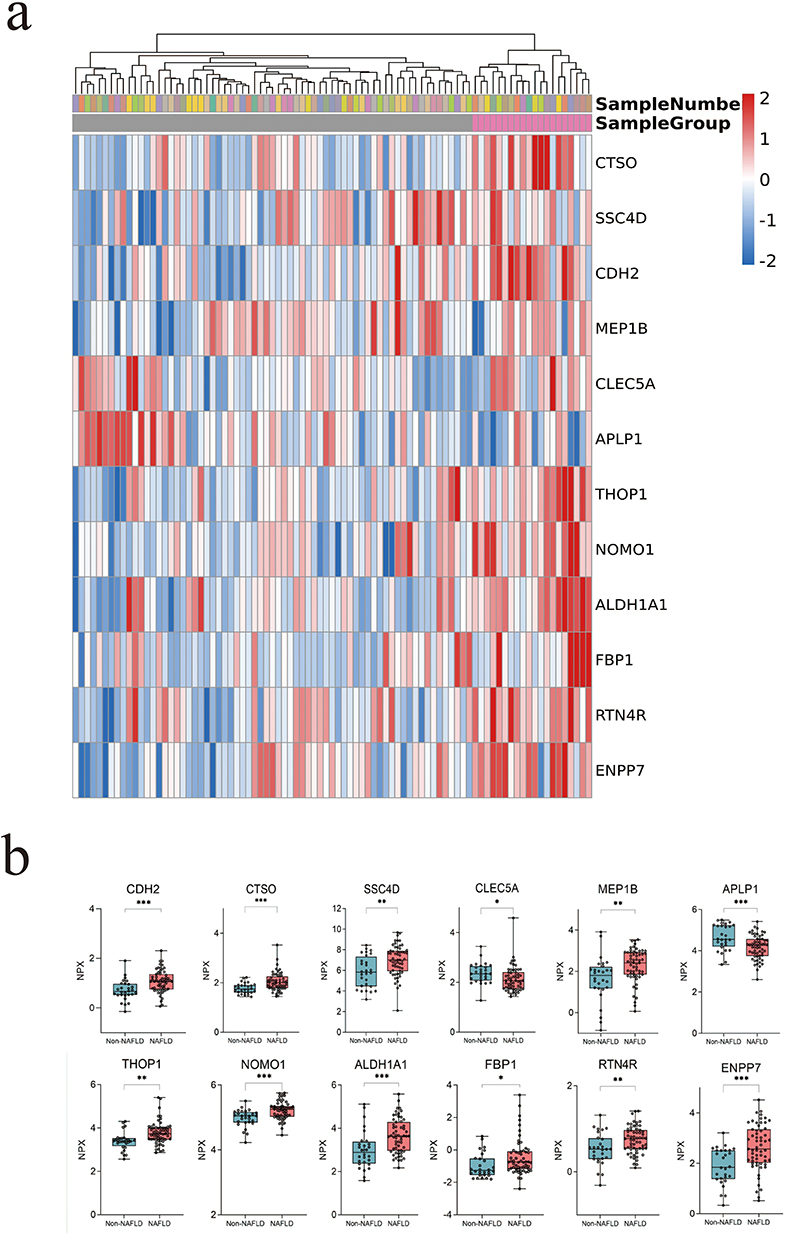 |
Figure 2 Differential expression serum proteins in snoring patients with and without NAFLD. (a) Heat map of differentially expressed proteins. (b) Relative expression levels of differentially expressed proteins. *p < 0.05, **p < 0.01, ***p < 0.001. |
The Association Between of CDH2 and NAFLD, Liver Fibrosis
As shown in Table 3, a positive association was observed between CDH2 levels and NAFLD. This significance remained more significant after adjustment for gender, Age, AHI (Model 2, OR = 6.58, 95% CI: 1.83–23.64; p = 0.004). After fully adjusted by gender, age, AHI, BMI, hs-CRP, HbA1C and triglyceride (Model 3), CHD2 levels were still positively associated with the risk of NAFLD (OR = 10.77, 95% CI: 1.75–74.63; p = 0.016). A positive association between CDH2 levers and liver fibrosis was also observed (Table 4) in snoring patients. After fully adjusting for gender, age, AHI, BMI, hs-CRP, HbA1C and triglyceride, CDH2 was still positively associated with the risk of liver fibrosis (OR = 12.58, 95% CI: 2.15–73.49; p = 0.019). Furthermore, patients were divided into high-level CDH2 group and low-level CDH2 group based on CDH2’s median value of 0.96. The risk of NAFLD and liver fibrosis was much higher in snoring patients with higher levels of CHD2 compared with snorers with lower levels of CHD2 (both P < 0.05).
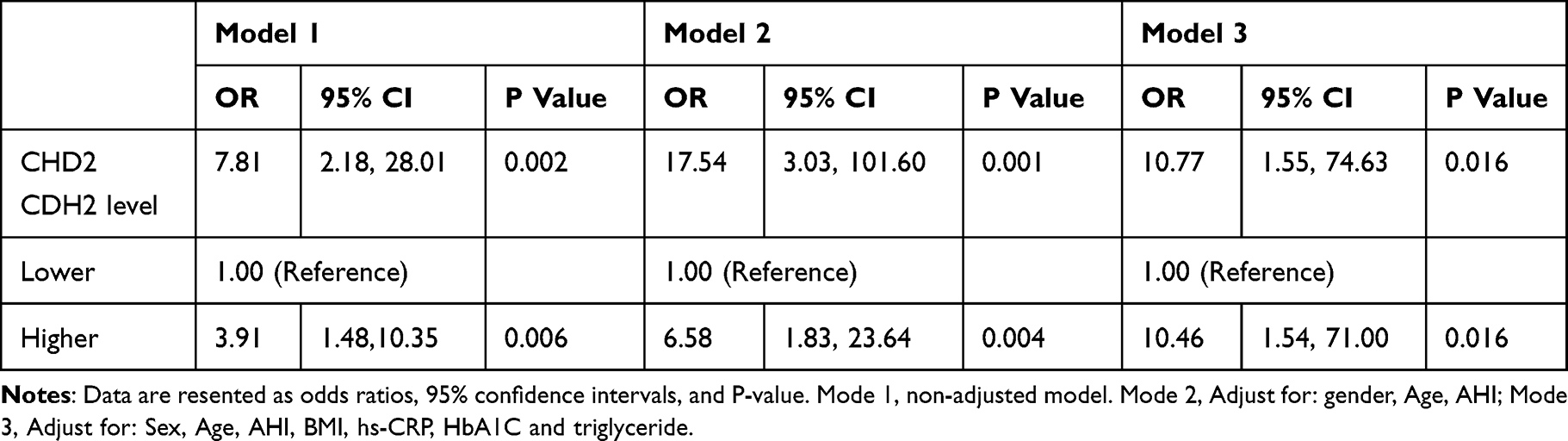 |
Table 3 The Relationship Between NAFLD and CDH2 in Snoring Patients |
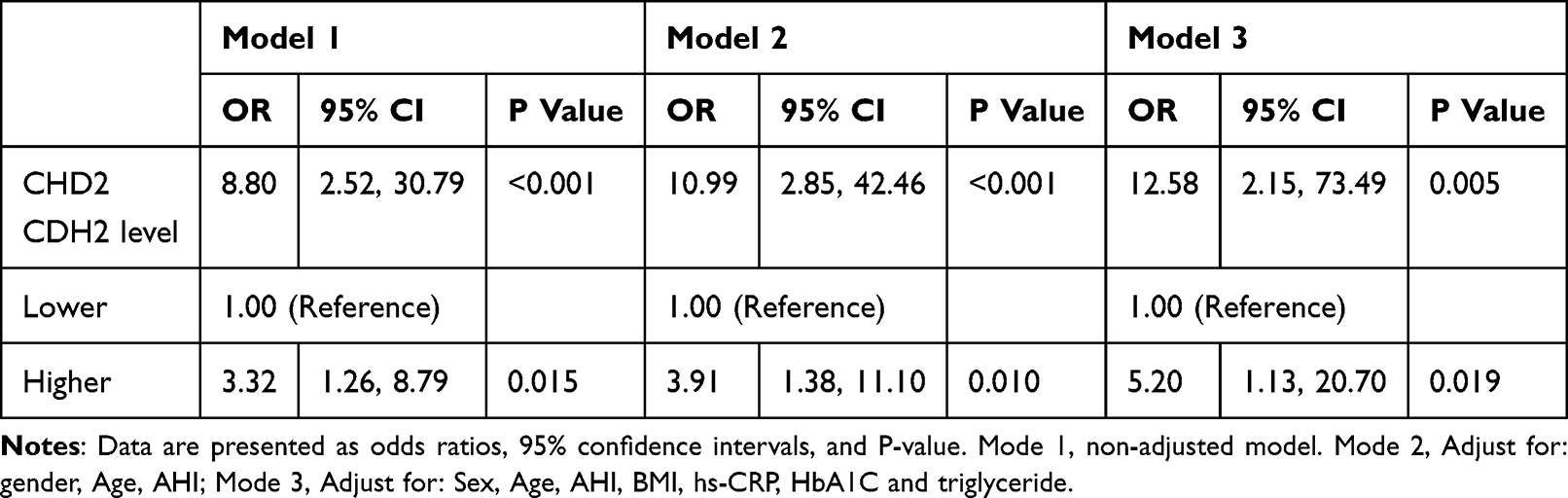 |
Table 4 The Relationship Between Liver Fibrosis and CDH2 in Snoring Patients |
The Value of CDH2 and Combined Index in Predicting NAFLD and Liver Fibrosis in Snoring Patients
Prediction models for NAFLD and liver fibrosis were conducted in snoring patients using CHD2, age, BMI, glucose, AHI and waistline. The predictive value of the combined index was evaluated using the ROC curve. Area Under the Curve (AUC) of the combined index for NAFLD and liver fibrosis were 0.92 (95% CI: 0.86–0.98) and 0.81 (95% CI: 0.72–0.91), respectively (Figures 3a and 4a). The calibration curve is used to evaluate the performance of the prediction model. As shown in Figures 3b and 4b, the scatter plot of actual occurrence rates and predicted occurrence rates exhibits good consistency. Predictive nomograms were constructed according to the results of the multivariate logistic regression analysis. We developed nomogram models for diagnosing NAFLD and liver fibrosis based on the combined index. In the nomogram prediction models, CDH2 had a great predictive value in NAFLD and liver fibrosis in Snoring Population (Figures 3c and 4c).
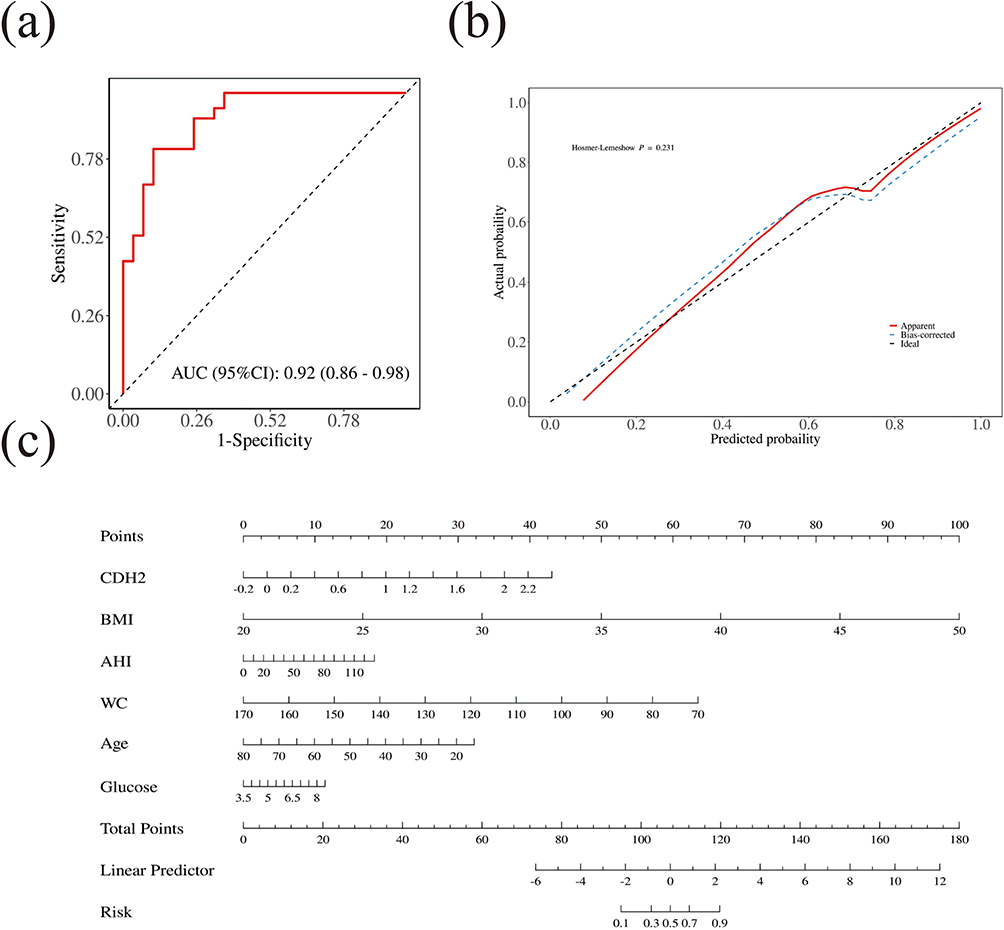 |
Figure 3 The efficiency and accuracy of the combined index for predicting the risk of NAFLD in snoring patients. (a) ROC curves for the model to predict the risk of NAFLD in snoring patients; The logit model has the following equation: NAFLD = -5.49+2.93*CDH2- 0.09*Age+ 0.59*BMI- 0.11*waistline+ 0.40*Glucose+ 0.02*AHI, achieving a diagnostic performance with an area under the curve of 0.92 with a sensitivity of 89% and specificity of 81%. (b) Calibration curves for the model predicting the risk of NAFLD in snoring patients; (c) Predicting the risk of NAFLD in snoring patients via the nomogram. |
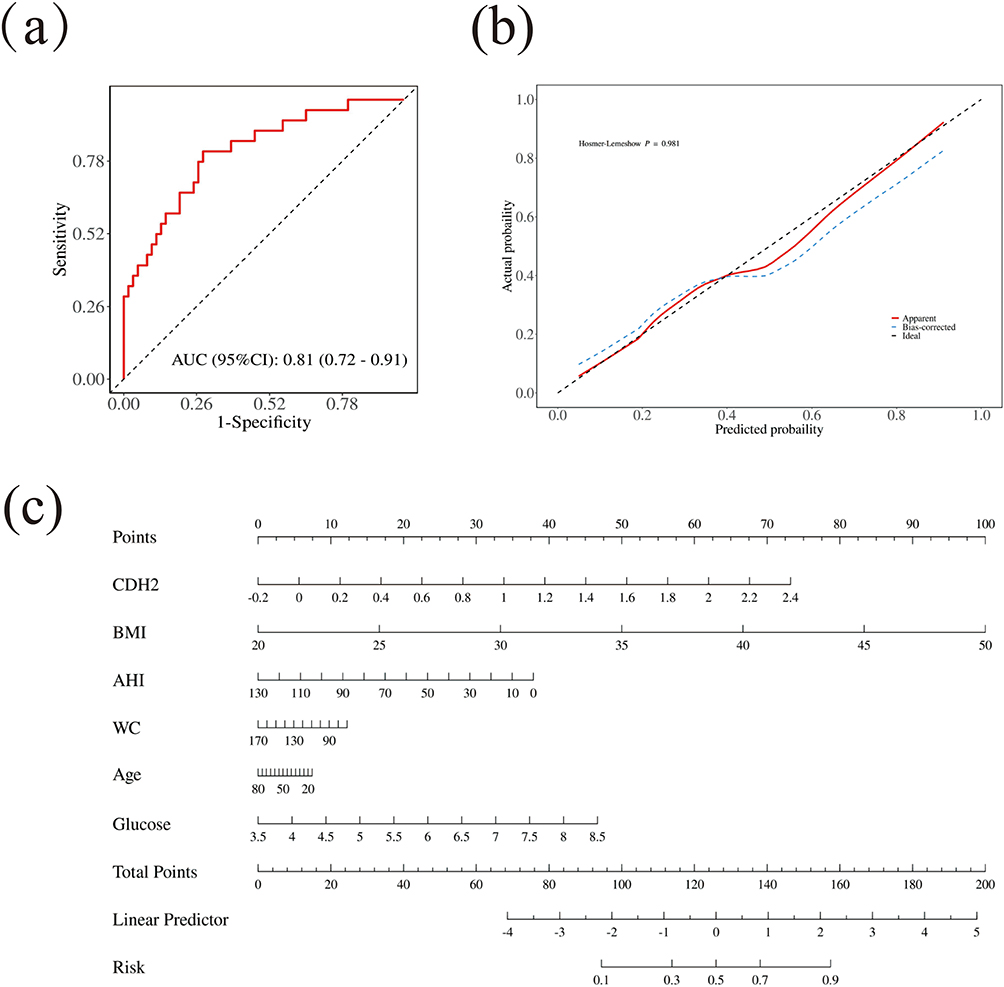 |
Figure 4 The efficiency and accuracy of the combined index for predicting the risk of liver fibrosis in snoring patients. (a) ROC curves for the model to predict the risk of liver fibrosis in snoring patients; The logit model has the following equation: liver fibrosis = -10.59+1.96*CDH2- 0.01*Age+ 0.23*BMI- 0.01*waistline+ 0.65*Glucose- 0.02*AHI, achieving a diagnostic performance with an area under the curve of 0.81 with a sensitivity of 72% and specificity of 81%. (b) Calibration curves for the model predicting the risk of liver fibrosis in snoring patients; (c) Predicting the risk of liver fibrosis in snoring patients via the nomogram. |
Discussion
In this study, CHD2 was upregulated in snorers with NAFLD. High expression levels of CHD2 are closely associated with increased risk of NAFLD and liver fibrosis. In addition, a combination of CHD2, age, BMI, glucose, AHI and waistline presented the acceptable AUC, high sensitivity and specificity for the detection of NAFLD in snoring patients.
High-precision proteomics serve as a reliable approach for protein analysis, enabling the discovery of biomarkers. This study employed Olink Proteomics, a reliable and stable tool for scientific research, offering high-throughput protein quantification with exceptional sensitivity and specificity.10 PEA technology minimizes variability and ensures consistent results across different experiments, making it an ideal platform for scientific studies and cross-cohort comparisons.10 Olink Proteomics has been widely used in searching for diagnostic biomarkers for chronic diseases, such as heart failure, diabetes mellitus and metabolic syndrome.13–15 In this paper, we found 12 differentially expressed serum proteins associated with NAFLD and liver fibrosis in snorers. Among these differentially expressed proteins, CDH2 showed the highest correlation with both NAFLD and liver fibrosis, so we have incorporated CDH2 into our subsequent investigative endeavors.16
CDH2, commonly referred to as N-cadherin, is a key component of the classical cadherin family and has been extensively implicated in the development of various tissues and organs during developmental processes.17 Human Protein Atlas portal (HPA) knowledge resource shows that CDH2 is a membrane protein that is most abundant in the liver, kidney, and heart muscle. Giraudi et al discovered that CDH2 serves as a valuable tool for accurately diagnosing fatty liver, with the strongest association to the degree of steatosis being CDH2 plasma abundances.18 The epigenetic variant rs11083271 mapped in CDH2 has been linked to metabolic dysregulation observed in steatotic liver disease (MASLD). Ferrell et al reported that the presence of the N-cadherin prodomain on the cell membrane may act as a potential indicator of pathological myofibroblasts and fibrotic tissues in organs such as the liver, lungs, and heart.19 Similarly, Pascut et al identified CDH2 as a critical marker involved in the epithelial-mesenchymal transition (EMT), a process characterized by increased CDH2 expression under certain pathological conditions, including fibrosis.20 Meanwhile, EMT has been recognized as a key contributor to the progression of liver fibrosis caused by NAFLD and transforms hepatocytes into mesenchymal cells, leading to liver fibrosis, which further develops into cirrhosis and hepatocellular.17 Based on previous study, this highlights the potential role of CDH2 as an important biomarker for NAFLD and liver fibrosis. Previous studies revealed that CDH2 was associated with hepatic steatosis in obese children and patients with Prader-Willi syndrome.21,22 Ghionescu et al observed that miR-26a-5p inhibits the epithelial-to-mesenchymal transition (EMT) in the early stages of diabetic liver disease by downregulating CDH2 expression, suggesting its potential as a valuable therapeutic target in this condition.23 Due to the limitations of the study subjects and sample size, further exploration of the value of CDH2 in the diagnosis of NAFLD is needed. Our study found an increased expression of CDH2 in patients with NAFLD and liver fibrosis. Furthermore, higher levels of CDH2 were the risk factor of NAFLD and liver fibrosis in the snoring population. The results confirmed that CDH2 may be a potential predictive and diagnostic biomarker for NAFLD and liver fibrosis in snorers.
As a common clinical manifestation, snoring was a risk factor for various metabolic-related diseases. Studies have indicated that snoring is linked to both the development and severity of NAFLD, as sleep-disordered breathing causes chronic intermittent hypoxia, potentially leading to inflammation, lipid deposition, liver injury, and fibrogenesis through the activation of hypoxia-inducible factors (HIFs), nuclear factor kappa B (NF-κB), as well as the promotion of endoplasmic reticulum stress, systemic inflammation, and insulin resistance.24–26 Timely recognition of patients at elevated risk for NAFLD and hepatic fibrosis is essential to enable early intervention and the effective application of appropriate management strategies. For high cost, invasiveness and complications of liver biopsy,27 non-invasive monitoring techniques are widely used in the diagnosis of NAFLD and liver fibrosis.28 FibroScan was one of the widely used non-invasive procedures.29 Owing to limitations in equipment and staffing, a subset of community hospitals is precluded from conducting this diagnostic procedure. Many scholars have attempted to use a combination of serological markers and physiological parameters as predictive indicators.30–32 Multiple studies have reported that the combination of TyG with metabolic indicators such as waist circumference and BMI has good sensitivity and specificity for diagnosing NAFLD, but there are fewer reports on its predictive value for liver fibrosis. In the present study, the concomitant assessment of CDH2 alongside metabolic parameters and AHI demonstrated robust predictive capabilities for both NAFLD and liver fibrosis. Consequently, this composite index may be considered a novel biomarker for the screening of liver injury in snorers.
Our study identifies a promising biomarker combination, its translation to the clinic requires further development. The combined approach aims to exclude individuals at low risk, preventing unnecessary liver biopsies. Future research should expand the sample size and conduct multicenter validation to further explore risk assessment scores. The developed score may serve as a valuable tool for the identification of snoring patients who are at high risk for NAFLD and liver fibrosis.
This study has several limitations. Firstly, the modest sample size of the patient cohort could potentially limit the statistical power and the generalizability of our findings. An expanded cohort would enhance the robustness of the results. Secondly, the diagnosis of NAFLD and liver fibrosis relied on liver Fibroscan, a modality that may exhibit reduced sensitivity in detecting mild hepatic steatosis compared to liver biopsy. Future studies employing more sensitive diagnostic methods, such as histopathological assessment, could provide a more accurate characterization of liver disease severity. Future studies could explore the correlation of CDH2 and other panel biomarkers in response to interventions such as weight loss, continuous positive airway pressure (CPAP) therapy, or pharmacological treatments. This could help determine whether modulating these biomarkers translates to reduced risk or improved outcomes in NAFLD and liver fibrosis, potentially paving the way for targeted therapeutic strategies.
In summary, higher levels of CDH2 may serve as a strong indicator of increased risk for NAFLD and liver fibrosis among individuals who snore. Furthermore, a combination of CDH2, age, BMI, glucose, AHI and waistline could provide an effective approach for the early screening and risk assessment of NAFLD and liver fibrosis in this population.
Abbreviations
CDH2, Cadherin 2; NAFLD, Nonalcoholic fatty liver disease; OSA, Obstructive sleep apnea; Fibroscan, Transient elastography; PSG, polysomnography; IH, intermittent hypoxia; AHI, Apnea-hypopnea index; ODI, Oxygen desaturation index; NASH, nonalcoholic steatohepatitis; TyG, triglyceride glucose index; TG, triglyceride; FBG, fasting blood glucose; LSM, Liver stiffness measurements; CAP, Controlled attenuation parameter; PEA, Proximity Extension Assay; NPX, normalized protein expression; LOD, lower limit of detection; ROC, receiver operating characteristic; BMI, Body mass index; ALT, alanine aminotransferase; AST, aspartate aminotransferase; γ-GGT, gamma glutamyl transferase; TC, Total cholesterol; TG, Triglyceride; HDL, high density lipoproteincholesterol; hs-CRP, Plasma high sensitivity C-reactive protein; HBA1c, Haemoglobin A1c; HPA, Human Protein Atlas portal; MASLD, metabolic dysfunction associated with steatotic liver disease; EMT, epithelial-mesenchymal transition; hypoxia-inducible factors (HIFs); nuclear factor kappa B (NF-κB); continuous positive airway pressure (CPAP).
Data Sharing Statement
Data is available on request from the correspondence author.
Author Contributions
Shiyuan Huang: Writing – original draft, Visualization; Xiaoyu Deng: Writing – original draft, Data curation; Jia Chen: Conceptualization, Methodology, Project administration, Writing – review & editing; Jiefeng Huang: Formal analysis, Data curation, Software, Visualization, Writing – review & editing; Hansheng Xie: Investigation, Resources, Validation, Supervision; Writing – review & editing; Biying Wang: Supervision, Project administration, Data curation, Writing – review & editing; Ningfang Lian: Conceptualization, Methodology, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (No.82470082), Fujian Provincial Health Technology Project (No.2024CXA020), the Innovation of Science and Technology, Fujian Province (No. 2023Y9024).
Disclosure
The authors disclose no conflicts of interest.
References
1. Younossi ZM, Golabi P, Paik JM, Henry A, Van Dongen C, Henry L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology. 2023;77(4):1335–1347. doi:10.1097/HEP.0000000000000004
2. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology [published correction appears in gastroenterology. Gastroenterology. 2012;142(7):1592–1609. doi:10.1053/j.gastro.2012.04.001
3. Zhang X, Wang S, Xu H, Yi H, Guan J, Yin S. Metabolomics and microbiome profiling as biomarkers in obstructive sleep apnoea: a comprehensive review. Eur Respir Rev. 2021;30(160):200220. doi:10.1183/16000617.0220-2020
4. Mesarwi OA, Loomba R, Malhotra A. Obstructive sleep apnea, hypoxia, and nonalcoholic fatty liver disease. Am J Respir Crit Care Med. 2019;199(7):830–841. doi:10.1164/rccm.201806-1109TR
5. Lian N, Wu J, Wang B, et al. Risk factors of nonalcoholic fatty liver disease and liver fibrosis in Non-Obese patients with obstructive sleep apnea. Nat Sci Sleep. 2022;14:2143–2149. doi:10.2147/NSS.S388203
6. Lekakis V, Papatheodoridis GV. Natural history of metabolic dysfunction-associated steatotic liver disease. Eur J Intern Med. 2024;122:3–10. doi:10.1016/j.ejim.2023.11.005
7. Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–1321. doi:10.1002/hep.20701
8. Cai Y, Chen J, Deng X, Wang B, Huang J, Lian N. Triglyceride-glucose index and combined indicators: effective indicators for screening NAFLD in snoring patients. BMC Pulm Med. 2024;24(1):359. doi:10.1186/s12890-024-03166-8
9. Chen M, Wang B, Huang J, Zhao J, Chen J, Chen G. The role of platelet-related parameters for the prediction of NAFLD in OSAHS patients. BMC Pulm Med. 2022;22(1):487. doi:10.1186/s12890-022-02291-6
10. Cui M, Cheng C, Zhang L. High-throughput proteomics: a methodological mini-review. Lab Invest. 2022;102(11):1170–1181. doi:10.1038/s41374-022-00830-7
11. Ciardullo S, Perseghin G. Statin use is associated with lower prevalence of advanced liver fibrosis in patients with type 2 diabetes. Metabolism. 2021;121:e154752.
12. Ciardullo S, Carbone M, Invernizzi P, et al. Impact of the new definition of metabolic dysfunction-associated fatty liver disease on detection of significant liver fibrosis in US adolescents. Hepatol Commun. 2022;6(8):2070–2078. doi:10.1002/hep4.1969
13. Ferreira JP, Verdonschot J, Wang P, et al. Proteomic and mechanistic analysis of spironolactone in patients at risk for HF. JACC Heart Fail. 2021;9(4):268–277. doi:10.1016/j.jchf.2020.11.010
14. Mir FA, Abdesselem HB, Cyprian F, et al. Inflammatory protein signatures in individuals with obesity and metabolic syndrome. Sci Rep. 2023;13(1):22185. doi:10.1038/s41598-023-49643-8
15. Yao P, Iona A, Pozarickij A, et al. Proteomic analyses in diverse populations improved risk prediction and identified new drug targets for type 2 diabetes. Diabetes Care. 2024;47(6):1012–1019. doi:10.2337/dc23-2145
16. Wu S, Liu M, Zhang M, et al. The gene expression of CALD1, CDH2, and POSTN in fibroblast are related to idiopathic pulmonary fibrosis. Front Immunol. 2024;15:1275064. doi:10.3389/fimmu.2024.1275064
17. László ZI, Lele Z. Flying under the radar: CDH2 (N-cadherin), an important hub molecule in neurodevelopmental and neurodegenerative diseases. Front Neurosci. 2022;16:972059. doi:10.3389/fnins.2022.972059
18. Giraudi PJ, Pascut D, Banfi C, et al. Serum proteome signatures associated with liver steatosis in adolescents with obesity. J Endocrinol Invest. 2025;48(1):213–225. doi:10.1007/s40618-024-02419-x
19. Ferrell PD, Oristian KM, Cockrell E, Pizzo SV. Pathologic proteolytic processing of N-cadherin as a marker of human fibrotic disease. Cells. 2022;11(1):156. doi:10.3390/cells11010156
20. Pascut D, Giraudi PJ, Banfi C, et al. Proteome profiling identifies circulating biomarkers associated with hepatic steatosis in subjects with Prader-Willi syndrome. Front Endocrinol. 2023;14:1254778. doi:10.3389/fendo.2023.1254778
21. Yu K, Li Q, Shi G, et al. Involvement of epithelial-mesenchymal transition in liver fibrosis. Saudi J Gastroenterol. 2018;24(1):5–11. doi:10.4103/sjg.SJG_297_17
22. Sookoian S, Pirola CJ. Genetics of nonalcoholic fatty liver disease: from pathogenesis to therapeutics. Semin Liver Dis. 2019;39(2):124–140. doi:10.1055/s-0039-1679920
23. Ghionescu AV, Sorop A, Linioudaki E, et al. A predicted epithelial-to-mesenchymal transition-associated mRNA/miRNA axis contributes to the progression of diabetic liver disease. Sci Rep. 2024;14(1):27678. doi:10.1038/s41598-024-77416-4
24. Umbro I, Fabiani V, Fabiani M, Angelico F, Del Ben M. Association between non-alcoholic fatty liver disease and obstructive sleep apnea. World J Gastroenterol. 2020;26(20):2669–2681. doi:10.3748/wjg.v26.i20.2669
25. Wang H, Gao Q, He S, et al. Self-reported snoring is associated with nonalcoholic fatty liver disease. Sci Rep. 2020;10(1):9267. doi:10.1038/s41598-020-66208-1
26. Wang Y, Shen R, Ge J. Association between self-reported snoring and metabolic-associated fatty liver disease: a cross-sectional analysis of the NHANES 2017-2018. Sleep Med. 2023;101:414–420. doi:10.1016/j.sleep.2022.11.029
27. Parola M, Pinzani M. Liver fibrosis in NAFLD/NASH: from pathophysiology towards diagnostic and therapeutic strategies. Mol Aspects Med. 2024;95:101231. doi:10.1016/j.mam.2023.101231
28. Tincopa MA, Loomba R. Non-invasive diagnosis and monitoring of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Lancet Gastroenterol Hepatol. 2023;8(7):660–670. doi:10.1016/S2468-1253(23)00066-3
29. Eddowes PJ, Sasso M, Allison M, et al. Accuracy of fibroscan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Gastroenterology. 2019;156(6):1717–1730. doi:10.1053/j.gastro.2019.01.042
30. Xue Y, Xu J, Li M, Gao Y. Potential screening indicators for early diagnosis of NAFLD/MAFLD and liver fibrosis: triglyceride glucose index-related parameters. Front Endocrinol. 2022;13:951689. doi:10.3389/fendo.2022.951689
31. Sheng G, Lu S, Xie Q, Peng N, Kuang M, Zou Y. The usefulness of obesity and lipid-related indices to predict the presence of Non-alcoholic fatty liver disease. Lipids Health Dis. 2021;20(1):134. doi:10.1186/s12944-021-01561-2
32. Michalak A, Guz M, Kozicka J, et al. Red blood cell distribution width derivatives in alcohol-related liver cirrhosis and metabolic-associated fatty liver disease. World J Gastroenterol. 2022;28(38):5636–5647. doi:10.3748/wjg.v28.i38.5636
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Insulin Resistance Across Cerebrovascular and Related Disorders: Mechanisms, Measurement, Genetics, and Clinical Implications
Chen K, Nong Y, Liu Y, Ye Z
Neuropsychiatric Disease and Treatment 2026, 22:575306
Published Date: 30 April 2026