Back to Journals » Patient Related Outcome Measures » Volume 13
Prostate Cancer Screening Practice and Associated Factors Among Men in Public Health Facilities of Hossana Town, Ethiopia
Authors Shanko A, Abute L ![]() , Tamirat T
, Tamirat T ![]()
Received 2 July 2022
Accepted for publication 12 November 2022
Published 22 November 2022 Volume 2022:13 Pages 229—238
DOI https://doi.org/10.2147/PROM.S380898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Howland
Ayano Shanko,1 Lonsako Abute,2 Temesgen Tamirat2
1Department of Internal Medicine, College of Medicine and Health Sciences, Wachemo University, Hossana, Ethiopia; 2Public Health Department, College of Medicine and Health Sciences, Wachemo University, Hossana, Ethiopia
Correspondence: Temesgen Tamirat, Email [email protected]
Background: Prostate cancer is a disease of the prostate gland. It is a recognized tumour in men and is common worldwide. It is the second most frequent cancer and the fifth leading cause of death in males worldwide. Worldwide, prostate cancer screening continues to be a highly contested topic with a variety of differences in recommendations for screening uptake. However, for men considered to be at risk, screening continues to be the most effective method for lowering death through early identification of prostate cancer.
Objective: To determine prostate cancer screening practice and associated factors among adult men in public health facilities of Hossana Town, Ethiopia.
Methods: Facility-based cross-sectional design was used. All adult men, whose age > 40 years attending public health facilities found in Hossana town were included in this study. From each public health facility, representative numbers of participants who fulfilled inclusion criteria were included in the study. A total of 422 sample sizes of adult men were used. A consecutive sampling technique was used to select study participants in each health facility. An interviewer-administered questionnaire was employed to collect data. Both descriptive and advanced analyses were performed using SPSS software version 26.0. In bivariable analysis, variables with a p-value < 0.25 were considered for multivariable analysis. Finally, odds ratio with 95% CI and p-value < 0.05 were used to declare factors as significantly associated with the outcome variable.
Results: About 7.2% (30) of the participants were screened for prostate cancer in this study. Ever heard about prostate cancer [AOR=26 (7.06– 96.90)], family history of prostate cancer [AOR=15.5(5.18– 46.77)] and awareness of anyone who has undergone prostate cancer screening [AOR= 6.8(1.95– 23.64)] were identified independent predictors for prostate screening practice.
Conclusion: In this study, prostate cancer screening practice is low. Ever heard about prostate cancer, family history of prostate cancer and awareness of anyone who has undergone prostate cancer screening were independent predictors of prostate cancer screening practice. Intervention measures aiming to increase awareness about prostate cancer and prostate cancer screening should be done.
Keywords: prostate cancer, screening practice, adult men, health facilities, Hossana
Introduction
Cancer is a leading cause of death and an important barrier to increasing life expectancy in every country of the world.1 Globally an estimated 19.3 million new cancer cases and almost 10 million cancer deaths occurred in the year 2020.2 Prostate cancer is the 2nd most commonly occurring cancer in men and there were more than 1.4 million new cases of prostate cancer and 375,304 deaths.3 The burden of prostate cancer is expected to increase by 1.7 million new cases and nearly half a million deaths by 2030 worldwide.4,5 The mortality due to prostate cancer is disproportionately affecting low- and middle-income countries with 165,000 deaths compared to 142,000 in high-income countries.6 It is the most common cause of mortality among men in Sub-Saharan Africa and the Caribbean.7 Prostate cancer contributes remarkably to the public health burden in Africa and is anticipated to continue increasing as a result of urbanization and growth in the population.8 A study result shows about the incidence of prostate cancer in Africa was 22–23.97 per 100,000 of the population10 and Kenyan men of varying ages and residences have reported prostate cancer screening rates between 1.3% and 2.6%.11
In Ethiopia, similar to other low-income countries, non-communicable diseases including cancer are emerging and prostate cancer has recently become more common and quietly growing across the country. It is the third most common cancer among men and those residing in rural areas were reported to have low levels of PC awareness and screening in comparison with those residing in the urban regions and the Age-Standardized Incidence Rate (ASR) of 40.6 per 100,000.12,13 According to Globocan, 2020, Prostate Cancer prevalence in Ethiopia was 3775 an incidence of 2720 with 1600 deaths and with age adjusted Death Rate is 6.02 per 100,000 population.17 Studies show in Ethiopia prostate cancer caused 1851 deaths and 33,056 disability-adjusted life years (DALYs)14,15 and a median survival rate of 28 months with an overall 2-, 3- and 5-year survival of 57%, 38.9% and 22%, respectively.16
Factors such as population growth, aging, physical inactivity, and increased prevalence of key risk factors, including those associated with social and economic transition, have been linked to the rise.18 There is a lot of importance of screening and early diagnosis that may help to be treated before spreading and may lower the chance of death from prostate cancer in men. But it has some possible harms of screening for prostate cancer including false-positive test results during screening, pain and infection during biopsy to diagnosis and urinary incontinence, erectile dysfunction and bowel problems due to surgery during treatment. Nevertheless, screening remains the key strategy for the reduction of mortality through early detection of prostate cancer among men considered at risk. In Ethiopia, mortality related to PC has been on the rise which is mainly attributed to late diagnosis.9 Prostate cancer is mostly asymptomatic in the early stages and it is diagnosed in the majority of the cases after progression to an advanced stage when the prognosis is poor. This evidence helped us to study the level of screening practice and associated factors in the study area. So, this study aimed to determine screening practice and associated factors among adult men in the Hossana public health facilities.
Materials and Methods
Study Area and Period
The study was conducted in public health facilities of Hossana town from May 2nd to 13th June 2022. There are four public health facilities in Hossana town. Public health facilities are a University hospital and three health centres. Hossana town is the capital town of the Hadiya zone. It is located 232 km away from the capital of Ethiopia, Addis Ababa. These public health facilities offer both curative and preventive health care services, including chronic care follow-up including cancer care for more than 2 million populations.
Study design: Facility-based cross-sectional study design was employed.
Population: All adult men, whose ages >40 years attending all the public health facilities of Hossana town were used as source populations. Those adult men who were randomly selected, fulfilled inclusion criteria and were available during the data collection period were used as a sample population. The individual men who provided data for the study were study units. But, those who were not willing to participate in the study were excluded.
Inclusion and Exclusion Criteria
Those adult men attending health facilities during the data collection period, and who were willing to participate in the study were included. Even if they fulfilled inclusion criteria, but due to their health condition, those patients who were critically ill and unable to communicate were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size was determined by using a single population proportion formula as follows:
The estimated proportion of screening for prostate cancer among adult men attending health facilities was assumed to be 50%, the margin of error was 5% and 95% CI, and the calculated sample size was 384. And, 10% non-response rate was added, and the final sample size was 422. All four public health facilities were purposively included in this study. The sample size was proportionally allocated to the four public health facilities of Hossana town based on the patient flow. About 219 participants from the hospital, 76 from Hosanna health centre, 67 from Melamba health centre and 60 from Bobicho Health centre. Then, in each health facility, a consecutive sampling technique was used until a proportionally allocated sample was obtained. All adult men who fulfilled the inclusion and visited health facilities during the data collection period participated.
Operational Definitions
Prostate cancer screening practice: If a man has ever undergone screening for prostate cancer during the study time.
Data Collection Measurements and Data Collection Methods
After a review of various kinds of literature, the English version questionnaire was developed. To ensure its consistency, this questionnaire was first translated into Amharic, and then back into English. It underwent pre-testing in another healthcare facility that was not a part of the study. The questionnaire mainly included awareness of prostate cancer, prostate cancer screening behaviour as well as socio-demographic factors such as age, educational status, marital status so on. An interviewer-administered questionnaire was used to collect the data. Four BSc nurses as data collectors and two senior public health professionals as supervisors were recruited for the study. To improve comprehension of the questionnaire and deal with difficulties, training was offered. It was also supposed to cover the participants’ information’s confidentiality and privacy.
Variables: Variables dependent: Screening practice level toward prostate cancer.
Independent variables: Socio-demographic factors such as age, education, home, income, marital status, awareness.
Data Quality Control
The data collectors and supervisors received a full day of training on the objective, methodology, and data collection method. The data collection tool was translated from English to the local tongue of Amharic. The pre-test was done on 5% of the actual sample size in another public health facility that was not included in the study. Based on the result of the pre-test necessary amendments were made.
Data Processing and Analysis
After checking for the data completeness, it was entered into Epi-Data version 3.1 software and then exported to SPSS version 26.0 software for further analysis. Descriptive statistics like percentages and proportions were calculated. Tables and texts were used to present the results. Binary logistic regression analysis was done. Both bi-variable and multivariable binary logistic regression analyses were done. The Hosmer–Lemeshow test was used to assess the model’s fitness. For the multivariable logistic regression analysis, variables having a p-value of less than 0.25 in the bivariate logistic regression were considered. Adjusted odds ratios (AOR) with a 95% confidence interval and a p-value of less than 0.05 were employed in the multivariable logistic regression to identify the factors significantly associated with prostate cancer screening practices.
Ethical Consideration
Ethical approval committees of Wachemo University have approved this study according to the relevant guidelines and regulations of the university as indicated by approval number Ref. WCU/213/2022 and following the Declaration of Helsinki. Wachemo University provided a formal letter, which was forwarded to the public health facilities. After getting approval, informed consent was gained from each participant after it was made clear that there was no need to collect any other kind of data beyond verbal responses, such as blood or bodily fluids. They have been informed that we are free to end our participation at any moment and without penalty. Participants’ privacy was also protected at all times during the research process.
Result
Socio-Demographic Characteristics
Of a total of 422 participants, 417 respondents participated in this study with a response rate of 98.8%. The majority of the participants 47% (196) were in the age group above 60 years and greater than half of the rural residents. Of those participants who cannot read and write an account about 44.1% (184) (Table 1).
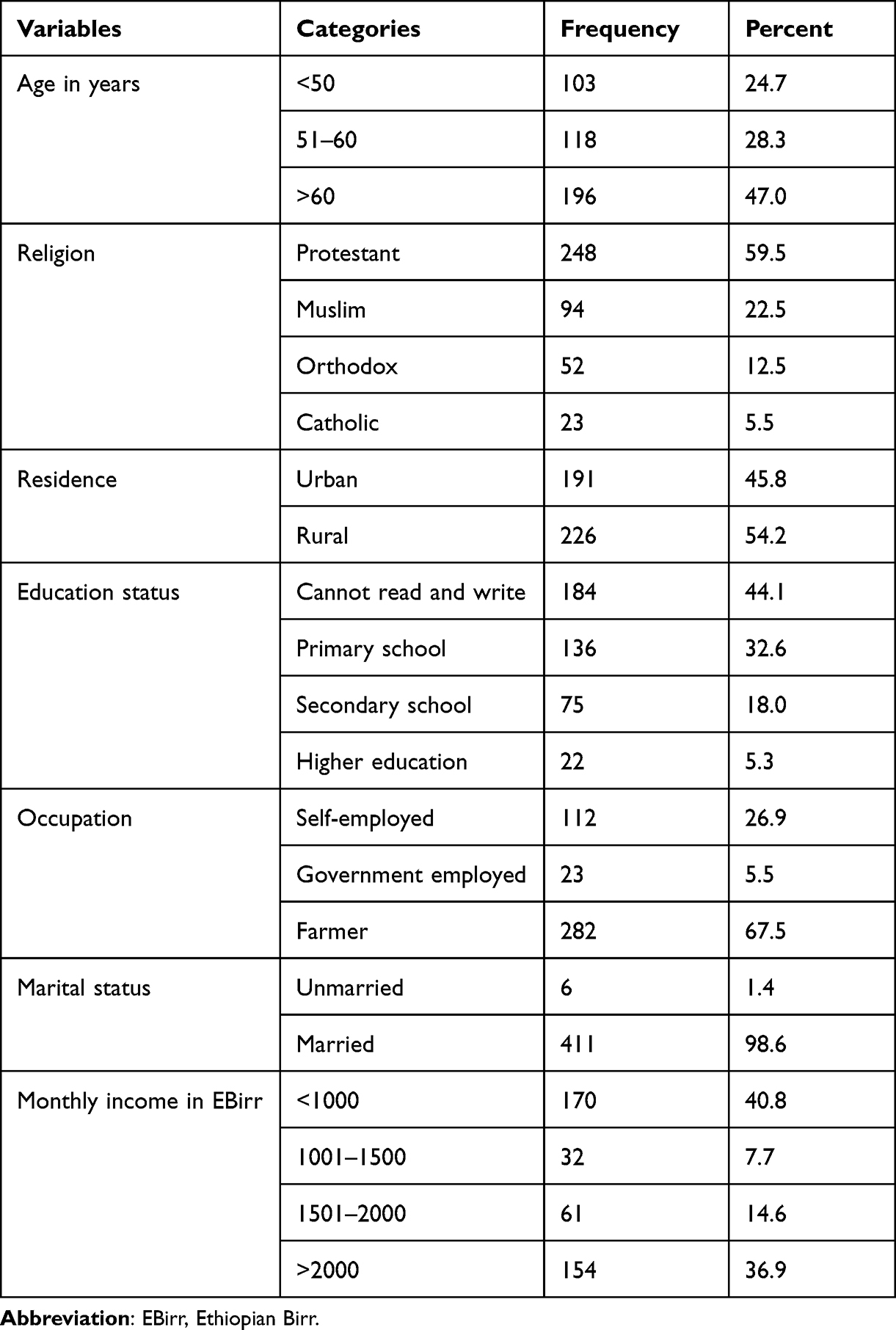 |
Table 1 Socio-Demographic Characteristic of the Study Participants in Hossana Town Public Health Facilities, Hosanna, South Ethiopia, 2022 |
Awareness of Prostate Cancer
Only 14.9% (62) of the respondents were ever heard about prostate cancer and frequently responded source of information for the individuals who ever heard about prostate cancer was health workers 56.4% (35) followed by mass media 37% (23). Of the total participants, only 11.3% (47) of them have a family history of prostate cancer; 8.9% (37) of them have awareness of the symptoms of prostate cancer and frequent/painful/difficulty in urination and erectile dysfunction were the frequently responded symptoms, respectively. More than twelve of the participants were ever heard about prostate cancer screening and Digital rectal examination 43.1% (22) and PSA screening 37.3%9 (19), respectively, were leading methods of prostate cancer screening (Table 2).
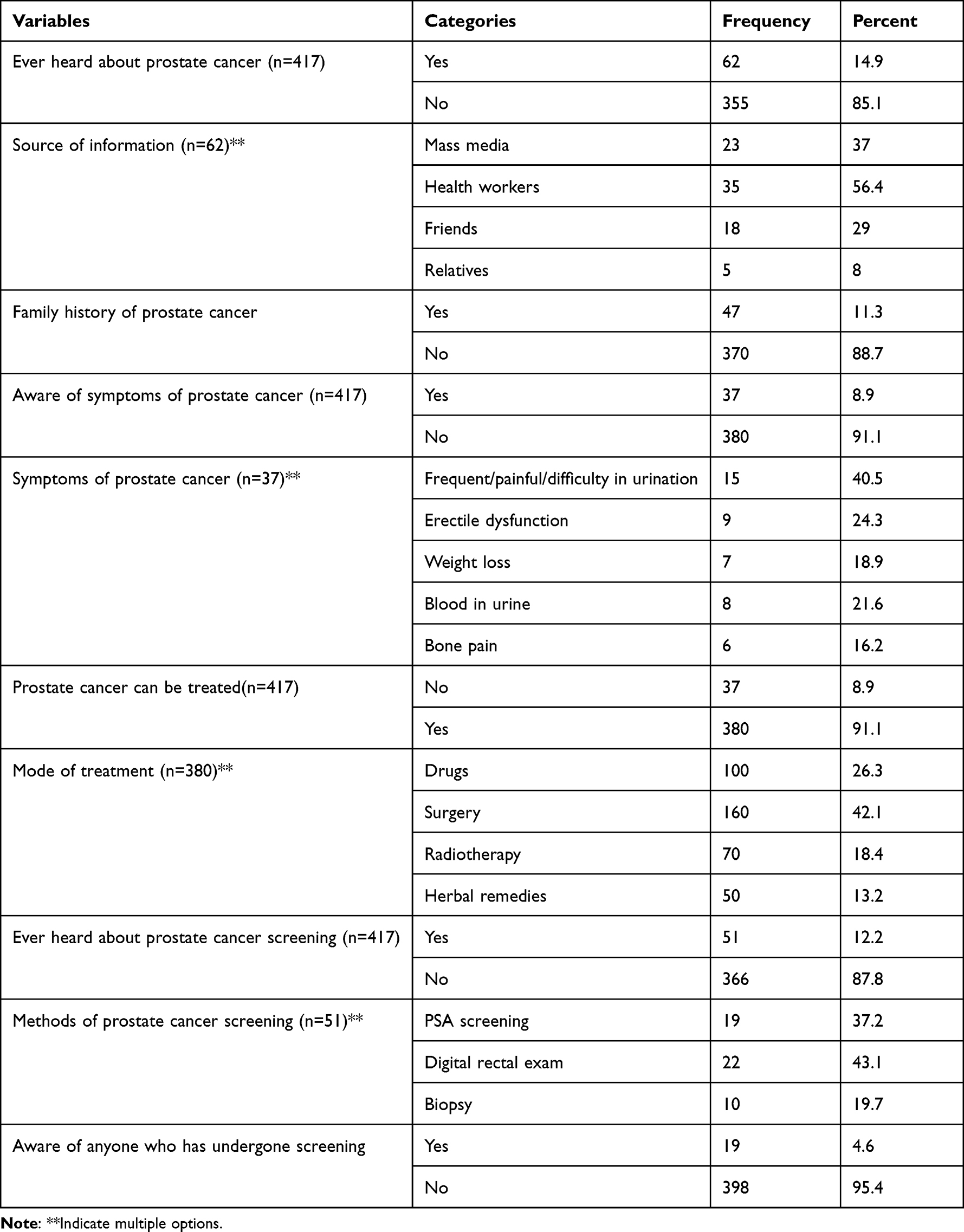 |
Table 2 Prostate Cancer Screening Awareness of the Study Participants in Hossana Town Public Health Facilities, Hossana, South Ethiopia, 2022 |
Prostate Cancer Screening Behaviours
Of the total 417 participants, 7.2% (30) of them have Prostate cancer screening behaviours. Of those who practised prostate cancer screening 53.3% (16) were Digital Rectal Examination and 16.7% (5) were PSA testing. Around two-thirds of the participants were screened two years ago, and for the majority, 90% (27) of them were screened by health professionals’ decision (Table 3).
 |
Table 3 Prostate Cancer Screening Behaviours of the Study Participants in Hossana Town Public Health Facilities, Hossana, South Ethiopia, 2022 |
Factors Affecting Prostate Screening Practice
Variables that showed a significant association with prostate screening practice were adjusted for their confounders using the multivariate logistic regression ever heard about prostate cancer, family history of prostate cancer and awareness of anyone who has undergone prostate cancer screening that became independent predictors for prostate screening practice. Those participants who ever heard about prostate cancer were more likely [26(7.06–96.90)] to practice prostate cancer screening practice than those who did not ever hear about prostate cancer. Those who had a family history of prostate cancer were fifteen times [15.5(5.18–46.77)] more likely to practice prostate cancer screening than their counterparts. Participants with awareness of anyone who has undergone prostate cancer screening were six times [6.8(1.95–23.64)] more likely to have prostate cancer screening than those with awareness of anyone who has undergone prostate cancer screening (Table 4).
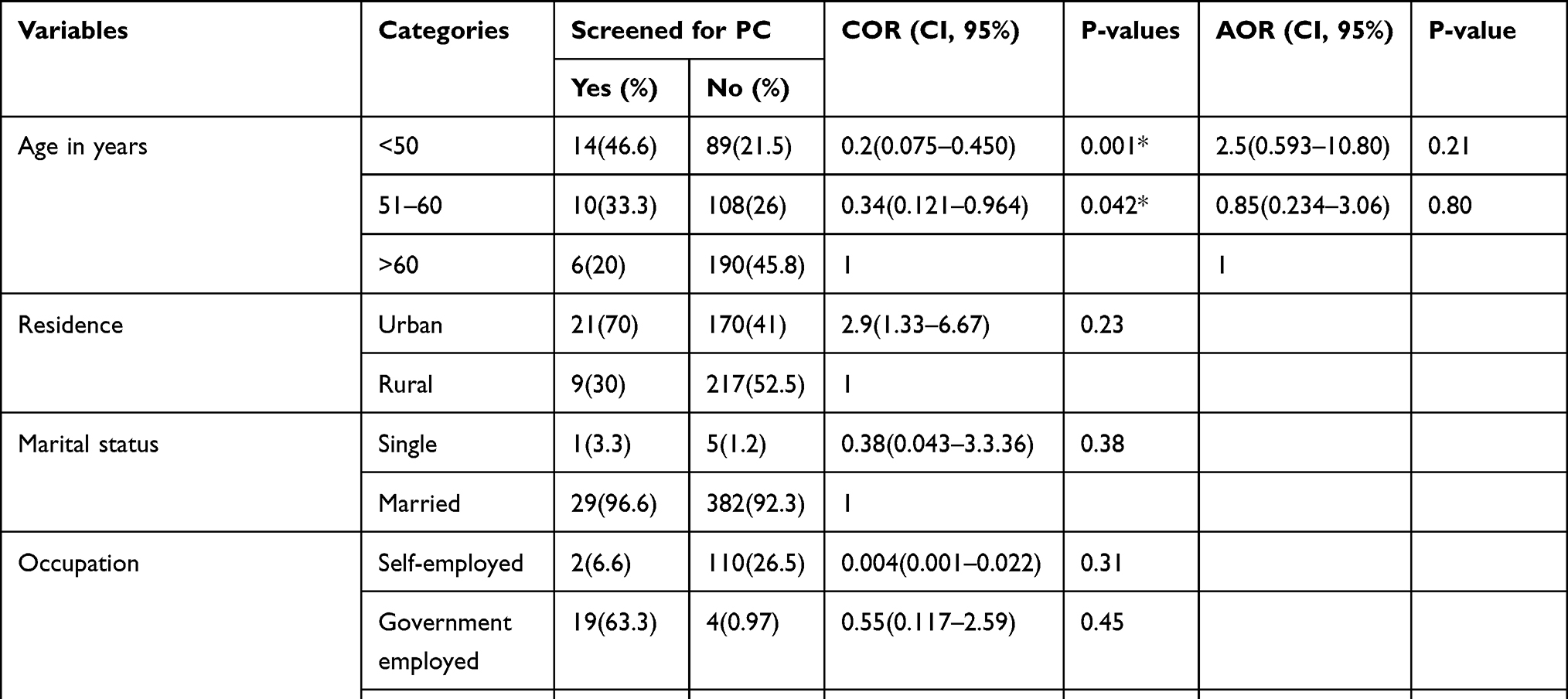 |
Table 4 Factors Affecting Prostate Screening Practice Among the Participants in Hossana Public Health Facilities, Hossana, South Ethiopia, 2022 |
Discussion
In the current study, 7.2% of the participants practised prostate cancer screening, which is much lower than a study done in Turkey among men 40 years old and beyond 23.8% of participants experienced prostate cancer screening,23 cross-section study done among Cameroun had shown that 8.1% reported that they had been screened for prostate cancer24 and Dar es salaam Tanzania (7.7%).20 But slightly it is higher than a study done in Kenya (5%).11 The different levels of screening practice reported might be due to the difference in the study population, setting, time and design. In addition to the accessibility of the health facility, the awareness level of the study participants and educational status difference might be taken as the reason for this different level of screening practice. This study reveals that 14.9% of the participants were ever heard about prostate cancer and only 8.9% of them were aware of the symptoms of prostate cancer. This finding is lower than studies conducted in Rwanda Kigali (60.8%) of them were aware of symptoms of prostate cancer, Kenya (40.6%) were ever heard about prostate cancer, Benin City, Nigeria (34%) have awareness of prostate cancer and study conducted in Addis Ababa Ethiopia (43.8%) aware of symptoms of prostate cancer.11,19,21,22 This low level of awareness about prostate cancer and symptoms of the disease in the study area might be due to study participants in a different setting might have a different level of exposure and this gives the clue that awareness creation was not that much conducted and this is also the reason for low utilization of the service.
This study reveals that participants who ever heard about prostate cancer were significantly associated with prostate cancer screening practice. Those participants who ever heard about prostate cancer were 26 times more likely to practice prostate cancer screening than their counterparts. The possible justification for this might be when the individuals were exposed to the information about their risk for some disease condition and if the belief that the risk may be serious for their health condition, the probability to practice the preventive behaviour might be increased. That is why those participants in this study with awareness were more likely to practice prostate cancer screening practice.
In this study participants, those with a history of prostate cancer in the family were 15 times higher more likely to practice prostate cancer screening practice than those with no history of prostate cancer. This finding is in line with the study done in Rwanda Kigali where participants with a history of prostate cancer in their family were more likely practices prostate cancer screening practice than their counterpart. The possible reason might be when there is prior information and perception about the getting of risk to the individuals, families and people around, the probability of practising that behaviour will be high and the likelihood hood practising it will be enhanced.19
This study shows that participants who had awareness of anyone who has undergone prostate cancer screening were significantly associated with prostate cancer screening practice. Those participants who had awareness of anyone who has undergone prostate cancer screening were six times more likely to practice prostate cancer screening than those who did not have awareness of anyone who has undergone prostate cancer screening. This reveals that the exposure of the participants to the presence of screening service utilization and awareness of others getting that service enhances their utilization behaviour. In addition to that, the effect of awareness of the prostate cancer screening service on the utilization of that service is paramount.
Limitation of the Study
The nature of the cross-sectional study might have produced a chicken or egg dilemma. The study was prone to recall bias since the participants were asked about ever screening practice for prostate cancer and they might have failed to distinguish the type of screening methods.
Conclusion
In this study, screening practice for prostate cancer was low. Ever heard about prostate cancer, family history of prostate cancer and awareness of anyone who has undergone prostate cancer screening were independent predictors of prostate cancer screening practice. Further studies should be conducted to generate strong evidence to develop appropriate strategies to enhance awareness of prostate screening and utilization of screening programs.
Data Sharing Statement
The datasets of this study will be available upon reasonable request.
Ethics Approval and Consent to Participant
Ethical approval committees of Wachemo University have approved this study according to the relevant guidelines and regulations of the university as indicated by approval number Ref. WCU/213/2022 and by the Declaration of Helsinki. Wachemo University provided a formal letter, which was forwarded to the public health facilities. After getting approval, informed consent was gained from each participant after it was made clear that there was no need to collect any other kind of data beyond verbal responses, such as blood or bodily fluids. They have been informed that we are free to end our participation at any moment and without penalty. Participants’ privacy was also protected at all times during the research process.
Acknowledgments
The authors would like to thank Wachemo University for providing this study with ethical approval. The authors would like to express their heartfelt gratitude to the data managers, participants, and collectors for their willingness to take part in the study.
Disclosure
The authors declare that they do not have conflicts of interest in this work.
References
1. Bray F, Laversanne M, Weiderpass E, Soerjomataram I. The ever-increasing importance of cancer as a leading cause of premature death worldwide. Cancer. 2022;127(16):3029–3030.
2. Li GS, Huang HQ, Liang Y, et al. BCAT1: a risk factor in multiple cancers based on a pan‐cancer analysis. Cancer Med. 2022;11(5):1396–1412. doi:10.1002/cam4.4525
3. World Cancer Research Fund International. Prostate cancer statistics.Available from: https://www.wcrf.org/cancer-trends/prostate-cancer-statistics/. Accessed November 17, 2022.
4. Zhou CK, Check DP, Lortet-Tieulent J, et al. Prostate cancer incidence in 43 populations worldwide: an analysis of time trends overall and by age group. Int J Cancer. 2016;138:1388–1400. doi:10.1002/ijc.29894
5. Banerjee S, Kaviani A. Worldwide prostate cancer epidemiology: differences between regions, races, and awareness programs. Int J Clin Exp Med Sci. 2016;2:1–6.
6. Fitzmaurice C, Allen C, Barber RM, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3(4):524–548. doi:10.1001/jamaoncol.2016.56881
7. McCormack V, Newton R. Research Priorities for Social Inequalities in Cancer in Sub-Saharan Africa. Geneva, Switzerland: 150 cours Albert Thomas, 69372 Lyon Cedex 08, France© International Agency for Research on Cancer, 2019 Distributed by WHO Press, World Health Organization; 2019:319.
8. Taitt HE. Global trends and prostate cancer: a review of incidence, detection, and mortality as influenced by race, ethnicity, and geographic location. Am J Mens Health. 2018;12:1807–1823. doi:10.1177/1557988318798279
9. Baratedi WM, Tshiamo WB, Mogobe KD, McFarland DM. Barriers to prostate cancer screening by men in Sub-Saharan Africa: an integrated review. J Nurs Scholarsh. 2020;52(1):85–94. PMID: 31733043. doi:10.1111/jnu.12529
10. Cassell A, Yunusa B, Jalloh M, et al. A review of localized prostate cancer: an African perspective. World J Oncol. 2019;10(4–5):162–168. PMID: 31636789; PMCID: PMC6785274. doi:10.14740/wjon1221
11. Mbugua RG, Oluchina S, Karanja S. Prostate cancer awareness and screening among men in a rural community in Kenya: a cross-sectional study. Afr J Urol. 2021;27. doi:10.1186/s12301-020-00108-8
12. Solomon S, Mulugeta W. Diagnosis and risk factors of advantage cancers in Ethiopia. J Cancer Prev. 2019;24(3):163–172. doi:10.15430/JCP.2019.24.3.163
13. Federal Ministry of Health. Ethiopia: national cancer control plan 2016–2020 October 2015. Addis Ababa Ethiopia; 2020. Available from: https://www.iccp-portal.org/.
14. Naghavi M, Abajobir AA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
15. Hay SI, Abajobir AA, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1260–1344. doi:10.1016/S0140-6736(17)32130-X)
16. Beksisa J, Getinet T, Tanie S, Diribi J, Hassen HY, Woloschak GE. Survival and prognostic determinants of prostate cancer patients in Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia: a retrospective cohort study. PLoS One. 2020;15(3):e0229854. PMID: 32134996; PMCID: PMC7058322. doi:10.1371/journal.pone.0229854
17. International agency for research on cancer (GLOBACON 2020; ETHIOPIA). Available from: https://www.afro.who.int/countries/ethiopia. Accessed November 17, 2022.
18. Addis Ababa City Cancer Registry E. Addis Ababa city cancer registry cancer incidence report. African Cancer Registry Network; 2019. Available from: https://afcrn.org/membership/members/100-Addisababa.
19. Benurugo G, Munyambaraga E, Chironda G, Bisanukuri E. Awareness on prostate cancer and screening practices among men attending outpatient at a referral hospital in Kigali, Rwanda: a quantitative study. Int J Afr Nurs Sci. 2020;13:100241. doi:10.1016/j.ijans.2020.100241
20. Bugoye FC, Leyna GH, Moen K, Mmbaga EJ. Knowledge, perceived risk and utilization of prostate cancer screening services among men in Dar es Salaam, Tanzania. Prostate Cancer. 2019;2019:2463048. PMID: 31871794; PMCID: PMC6913246. doi:10.1155/2019/2463048
21. Agbugui JO, Obarisiagbon EO, Nwajei CO, Osaigbovo EO, Okolo JC, Akinyele AO. Awareness and knowledge of prostate cancer among men in Benin City, Nigeria. J Med Biomed Res. 2013;12(2):42–47.
22. Gebru T, Mekonen H, Getahun NG, et al. Awareness of prostate cancer and its associated factors among Ethiopian men. Front Oncol. 2022. doi:10.21203/rs.3.rs-670064/v1
23. Bilgili N, Kitis Y. Prostate cancer screening and health beliefs: a Turkish study of male adults. Erciyes Med J. 2019;41(2):164–170.
24. Ernest K, Saleh R, Fran C, Rodrigue P, Matthew D. Oghenekome prostate cancer screening knowledge, attitudes, and beliefs among men in Bamenda, Cameroon. Int J Public Health Epidemiol. 2017;6(4):339–349.
25. Bostwick DG, Cooner WH, Denis L, Jones GW, Scardino PT, Murphy GP. The association of benign prostatic hyperplasia and cancer of the prostate. Cancer. 1992;70(1 Suppl):291–301. PMID: 1376199.
26. Moschovas MC, Timóteo F, Lins L, de Castro Neves O, Seetharam Bhat KR, Patel VR. Robotic surgery techniques to approach benign prostatic hyperplasia disease: a comprehensive literature review and the state of art. Asian J Urol. 2021;8(1):81–88. PMID: 33569274; PMCID: PMC7859458. doi:10.1016/j.ajur.2020.10.002
27. Mofolo N, Betshu O, Kenna O, et al. Knowledge of prostate cancer among males attending a urology clinic, a South African study. Springerplus. 2015;4:67. PMID: 25713760; PMCID: PMC4329121. doi:10.1186/s40064-015-0824-y
28. Darré T, Djiwa T, Kpatcha TM, et al. Prostate cancer screening: a survey of medical students’ knowledge in Lome, Togo, and associated determinants in a resource-limited African context. SAGE Open Med. 2021;9:20503121211032812. PMID: 34349998; PMCID: PMC8287366. doi:10.1177/20503121211032812
29. Dakum K, Ramyil VM, Agbo S, Ogwuche E, Makama BS, Kidmas AT. Digital rectal examination for prostate cancer: attitude and experience of final year medical students. Niger J Clin Pract. 2007;10(1):5–9. PMID: 17668707.
30. Conlisk EA, Lengerich EJ, Demark-Wahnefried W, Schildkraut JM, Aldrich TE. Prostate cancer: demographic and behavioral correlates of stage at diagnosis among blacks and whites in North Carolina. Urology. 1999;53(6):1194–1199. PMID: 10367851. doi:10.1016/s0090-4295(99)00005-9
31. Asare BY, Ackumey MM. Awareness and knowledge about prostate cancer among male teachers in the Sunyani municipality, Ghana. Afr Health Sci. 2021;21(2):655–662. PMID: 34795720; PMCID: PMC8568221. doi:10.4314/ahs.v21i2.22
32. Adeloye D, David RA, Aderemi AV, et al. An estimate of the incidence of prostate cancer in Africa: a systematic review and meta-analysis. PLoS One. 2016;11(4):e0153496. PMID: 27073921; PMCID: PMC4830589. doi:10.1371/journal.pone.0153496
33. Wilkinson S, List M, Sinner M, Dai L, Chodak G. Educating African-American men about prostate cancer: impact on awareness and knowledge. Urology. 2003;61(2):308–313. PMID: 12597936. doi:10.1016/s0090-4295(02)02144-1
34. Kabore FA, Kambou T, Zango B, Ouédraogo A. Knowledge and awareness of prostate cancer among the general public in Burkina Faso. J Cancer Educ. 2014;29(1):69–73. PMID: 24057691. doi:10.1007/s13187-013-0545-2
35. Clarke-Tasker VA, Wade R. What we thought we knew: African American males’ perceptions of prostate cancer and screening methods. ABNF J. 2002;13(3):56–60. PMID: 12108141.
36. Nakandi H, Kirabo M, Semugabo C, et al. Knowledge, attitudes and practices of Ugandan men regarding prostate cancer. Afr J Urol. 2013;19(4):165–170. PMID: 25221428; PMCID: PMC4162513. doi:10.1016/j.afju.2013.08.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.