")
Back to Journals » Stem Cells and Cloning: Advances and Applications » Volume 15
Prospect of Stem Cells as Promising Therapy for Brachial Plexus Injury: A Systematic Review
Authors Sumarwoto T , Suroto H, Mahyudin F , Utomo DN , Romaniyanto F , Prijosedjati A, Notobroto HB , Tinduh D, Prakoeswa CRS, Rantam FA , Rhatomy S
Received 21 February 2022
Accepted for publication 11 May 2022
Published 22 June 2022 Volume 2022:15 Pages 29—42
DOI https://doi.org/10.2147/SCCAA.S363415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bernard Binetruy
Tito Sumarwoto,1,2 Heri Suroto,3 Ferdiansyah Mahyudin,3 Dwikora Novembri Utomo,3 FNU Romaniyanto,2 Andhi Prijosedjati,2 Hari Basuki Notobroto,4 Damayanti Tinduh,5 Cita Rosita Sigit Prakoeswa,6 Fedik Abdul Rantam,7,8 Sholahuddin Rhatomy9,10
1Doctoral Program, Faculty of Medicine, Airlangga University, Surabaya, Indonesia; 2Department of Orthopaedics and Traumatology, Prof Soeharso Orthopaedic Hospital/Faculty of Medicine, Sebelas Maret University, Surakarta, Indonesia; 3Department of Orthopaedics and Traumatology, Dr. Soetomo General Hospital/Faculty of Medicine, Airlangga University, Surabaya, Indonesia; 4Faculty of Public Health, Airlangga University, Surabaya, Indonesia; 5Physical Medicine and Rehabilitation Department, Universitas Airlangga, Surabaya, Indonesia; 6Department of Dermatology and Venereology, Dr. Soetomo General Hospital/Faculty of Medicine, Airlangga University, Surabaya, Indonesia; 7Virology and Immunology Laboratory, Microbiology Department, Faculty of Veterinary Medicine, Airlangga University, Surabaya, Indonesia; 8Stem Cell Research and Development Center, Airlangga University, Surabaya, Indonesia; 9Department of Orthopaedics and Traumatology, Dr. Soeradji Tirtonegoro General Hospital, Klaten, Indonesia; 10Faculty of medicine, public health and nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
Correspondence: Sholahuddin Rhatomy, Department of Orthopaedics and Traumatology, Dr. Soeradji Tirtonegoro General Hospital, Klaten, Indonesia, Email [email protected]
Background: Brachial plexus injury is an advanced and devastating neurological injury, for which both nerve surgery and tendon transfers sometimes remain insufficient in restoring normal movement. Stem cell therapy may be applicable to rescue the injured motor neurons from degeneration which potentially improves muscle strength.
Study Design: Systematic Review; Level of evidence V.
Data Sources: A systematic literature search was conducted on PubMed (MEDLINE), EMBASE, the Cochrane Library, and Scopus using the terms (“stem cell”) AND (“brachial plexus”) as search keywords.
Methods: The process of study selection was summarized by PRISMA flow diagram. The study included in vivo and in vitro studies with English language, humans or animals with some brachial plexus injuries, interventions, some applications of stem cells to the groups of study, with functional, biomechanical, or safety outcomes.
Results: In total, there were 199 studies identified from the literature sources where 75 articles were qualified for forward evaluation following selecting the titles and abstracts. Ten studies were finally included in this systematic review after full-text assessment. Stem cells can produce neurotrophic factors in vitro and in vivo in rats, and their level was increased after injury. Electrophysiological measurement showed that the intervention group had distinctly higher CMAP amplitude and evidently shorter CMAP latency than the model group. Application of bone marrow stem cells (BMSCs) showed an elevation in the numbers of axons and density of myelinated fibers, the density of nerve fibers, the diameter of regenerating axons, and a decrease in axonal degeneration. A study in humans indicated an improvement of the movements in a patient with traumatic total BPI after injection of Ad-MSC. It is associated with increased muscle mass and sensory recovery and also suggested that mononuclear cell injection enhances muscle regeneration and reinnervation in the partly denervated muscle of brachial plexus injury. Various muscle groups had obtained strength together with restoration, the muscle strength attained after the previous transplantation were preserved. The results of this review support stem cell treatment in brachial plexus injury.
Conclusion: This review provides evidence of the positive effects of stem cell treatment in brachial plexus injury.
Keywords: stem cell, brachial plexus injury, promising therapy
Introduction
Brachial plexus injury (BPI) is an advanced peripheral nerve injury that results in paralysis of the upper extremities. This injury is often caused by high-energy trauma such as road traffic accidents and young adult groups often experience it. Massive motor neuron damage and impairment functions of the brachial plexus-innervated muscles are the results of severe injury due to the nerve roots avulsion of the brachial plexus.1–3
Various attempts have been performed to save the injured motor neurons from degeneration and to recover the peripheral innervation of muscles, including pharmaceutical administrations and microsurgical interventions during the past decade. However, there is still a limitation regarding the long-term motor neurons survival and the functional outcomes. Massive damage of motor neurons due to injury, presence of extracellular matrix inhibitory molecules such as the chondroitin sulfate proteoglycans (CSPGs), and myelin-associated inhibitors including myelin-associated glycoprotein (MAG), oligodendrocyte-myelin glycoprotein (OMgp), Nogo, Netrin−1, and Ephrin in the affected spinal cord and the lack of guidance molecules along the regenerating pathways are related with the poor outcomes in term of functional recovery.4–6
Denervation from injury leads to loss of contractile strength and muscle atrophy. Good restorative ability exists if innervation is restored quickly. In contrast, prolonged interruption of innervation causes irreversible atrophy, fattening of the muscle, and interstitial fibrosis. The muscle could be targeted for cell therapy since the denervated muscle’s regeneration depends on its nerve supply as well as its regenerative capability.7 Skeletal muscle has a remarkable capability to regenerate mainly due to its resident muscle stem cells (MuSCs). The characteristic of regeneration phase is shown by the activation of the stem cells population known as satellite cells in muscles which replace damaged myofibers.8,9
Recently, strategies for cell replacement have been implemented for treating motor neuron degeneration. Mesenchymal stem cells (MSCs) have become the main interest for neurological repair because of their neural fate and ability to differentiate into neural phenotypes − neural progenitor cells (NPCs). Nevertheless, the environment of injured adult spinal cord does not seem to aid the differentiation of grafted NPCs. Some studies showed evidence that in injured spinal cord, the grafted NPCs will differentiate primarily into glial phenotypes.10–13
Grafted NPCs can generate a large quantities of neuron-specific nuclear protein (NeuN)-positive neurons (revealed by all glial fibrillary acidic protein/GFAP positive cells) following transplantation into the ventral horn at 2 weeks after the avulsion. In addition, some of these graft-derived neurons secrete choline acetyltransferase (Ch-AT). These facts indicate that at 2 weeks after the avulsion, the ventral horn supports neuronal differentiation and a conducive environment to generate region-specific neurons.2
The transplantation of NPCs into the ventral horn as a treatment in brachial plexus injury could be a promising therapy, since NPCs have the capacity to differentiate into cell types appropriate to the structure into which they have been grafted. The neurotrophic factors serving to protect the injured neurons also could be secreted.2
As an emerging therapeutic modality, we need a systematic review from current preclinical studies to assign the safety and efficacy. This systematic review is also hoped to provide guidance for the next studies. The major aim of this review is to re-examine the finest obtainable substantiation studies concerning the utilization of stem cells for the management of brachial plexus injuries systematically. We hypothesized that stem cells application will promote brachial plexus regeneration.
Methods
Eligibility Criteria
The inclusion criteria:
- Design of study: in vivo study and in vitro study.
- Group of study: humans or animals with some brachial plexus injuries.
- Interventions: some applications of stem cells to the groups of study.
- Outcomes: either functional, biomechanical, or safety.
- Language: English
Studies in languages other than English, transcriptions, review study and unrelated articles were excluded in this study.
Literature Search and Study Selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was used as a guideline to perform a comprehensive search of the literature.14 The search was held in PubMed (MEDLINE), EMBASE, the Cochrane Library, and Scopus. August 2, 2020 was the deadline for all research data used in this study. The terms (“Stem Cell”) AND (“brachial plexus”) were used as search keywords. Two researchers (T.S. and S.R.) separately scanned the titles and abstracts for eligibility after removing duplicates and reviewing the articles. An additional search was done applying the reference lists of the earlier included studies. To apply the inclusion and exclusion criteria, all elected studies were read in full text by the two researchers. A discussion was performed to resolve any disagreement between the two researchers.
Assessment of Methodological Quality and Risk of Bias
Animal Research: Reporting of In vivo Experiments (ARRIVE) guideline was applied to evaluate methodological quality of the included studies.15 Hence, modified ARRIVE in combination with Consolidating Reporting of Trials (CONSORT) were used.16 Systematic Review Centre for Laboratory Animal Experimentation’s risk of bias tool (SYRCLE’s RoB tool) was used to assess internal validity.17 All the assessments were performed by two researchers (T.S. and S.R.) separately. Discussions with other authors were used to resolve any discrepancy.
Extraction and Synthesis of Data
Two researchers (T.S. and S.R.) separately took data from each included study. Some contradictions between the two researchers were addressed by discussion with other researchers. The subsequent data including design of study, type of studies, formation process for humans or animals or cells in the included studies, types of MSCs and their particular donors, the isolation process of the stem cells, interventions, proportion, length of follow-up, the major result for the studies and the outcomes, any significant difference from control or baseline, and other results were extracted.
Any available blinding effort would be notified. The establishment of the humans, animals, interventions and follow-up were also reported. For in vivo studies, any disadvantageous reactions, quantitative outcome measures similar to clinical outcomes and biomechanical tests as the major results were also reported.
Meta-analysis cannot be conducted because of the elevated heterogeneity of the data (i.e. the origin of MSCs, subject, outcome measures, and length of follow-up).
Results
Study Selection
PRISMA flow chart (Figure 1) shows the study selection procedure.14 There were 199 studies recognized from the literature sources, and 10 studies were finally incorporated for this systematic review.
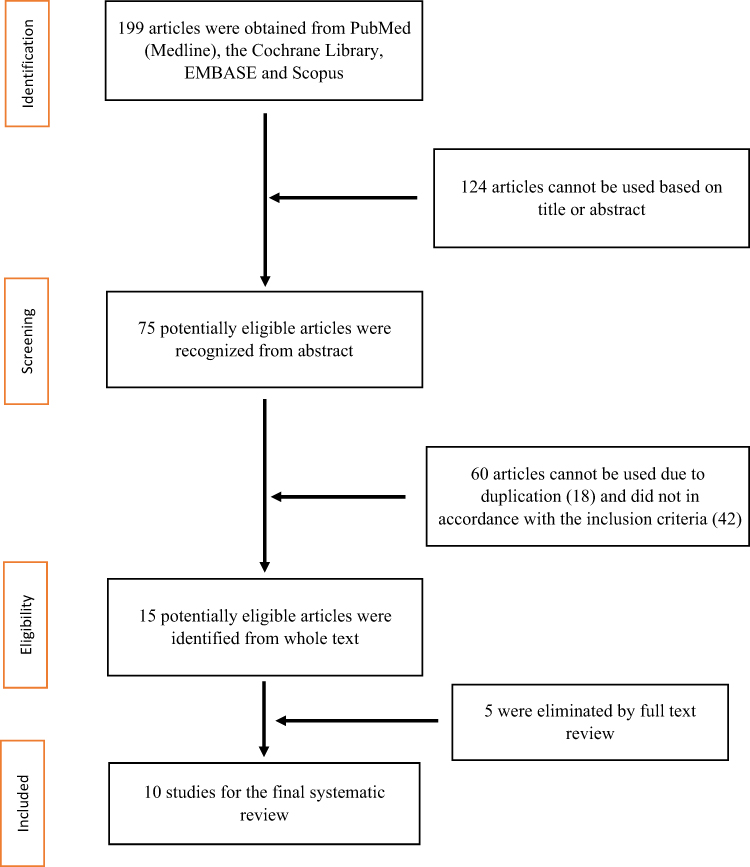 |
Figure 1 PRISMA flow chart of study process selection. Notes: Adapted from: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: https://doi.org/10.1136/bmj.n7114 Creative Commons Attribution (CC BY 4.0) license (https://creativecommons.org/licenses/by/4.0/legalcode). |
Study Characteristics
An outline of the study is summarized in Table 1 and certain explanations regarding the study are presented in Table 2 including the types of MSCs and their origins, isolation of the conditioned medium (CM) associated with its subcomponents, models of injury for in vivo study, and the interventions.
 |
Table 1 Summary of the Included Studies Characteristics |
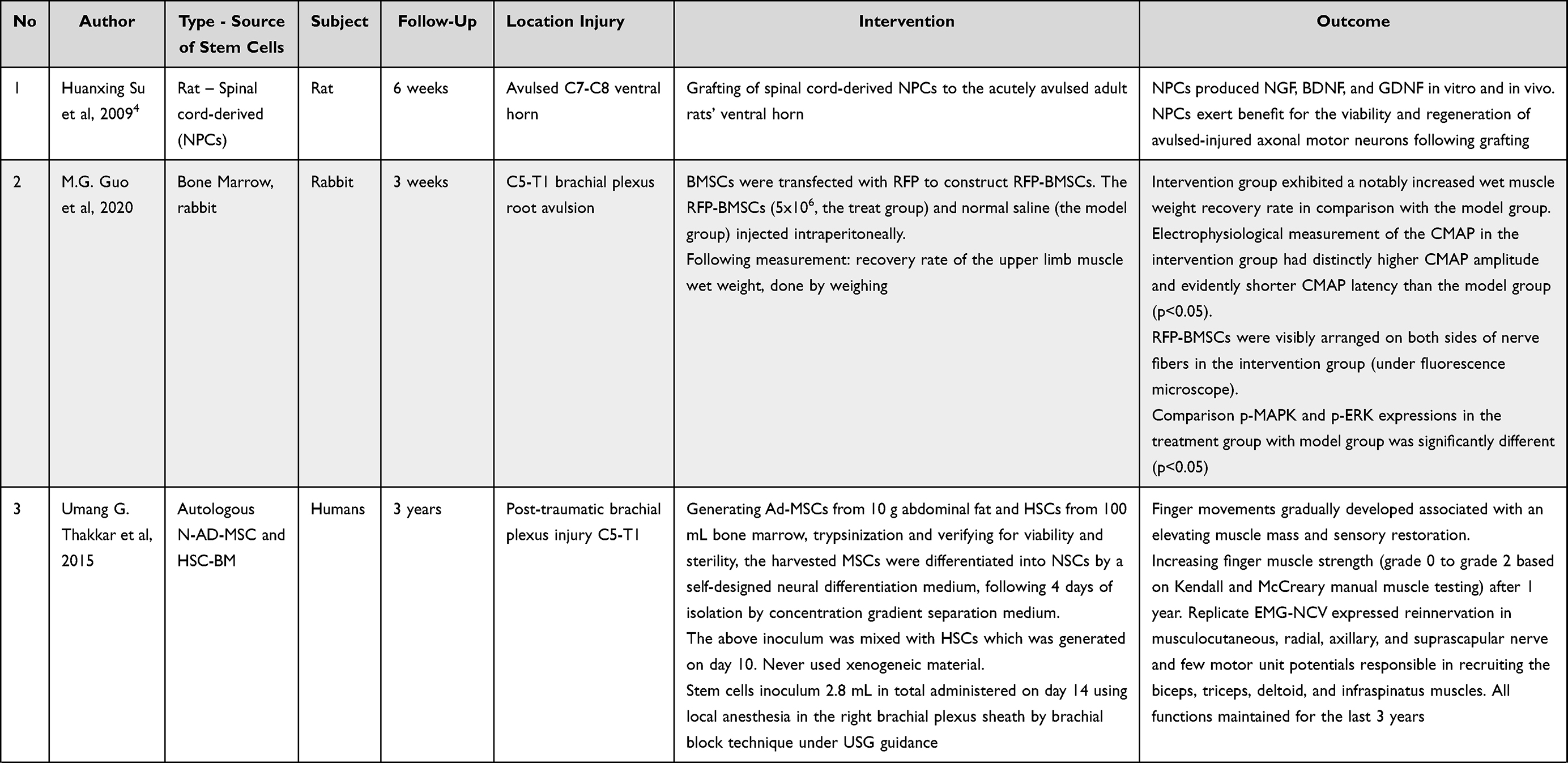 | 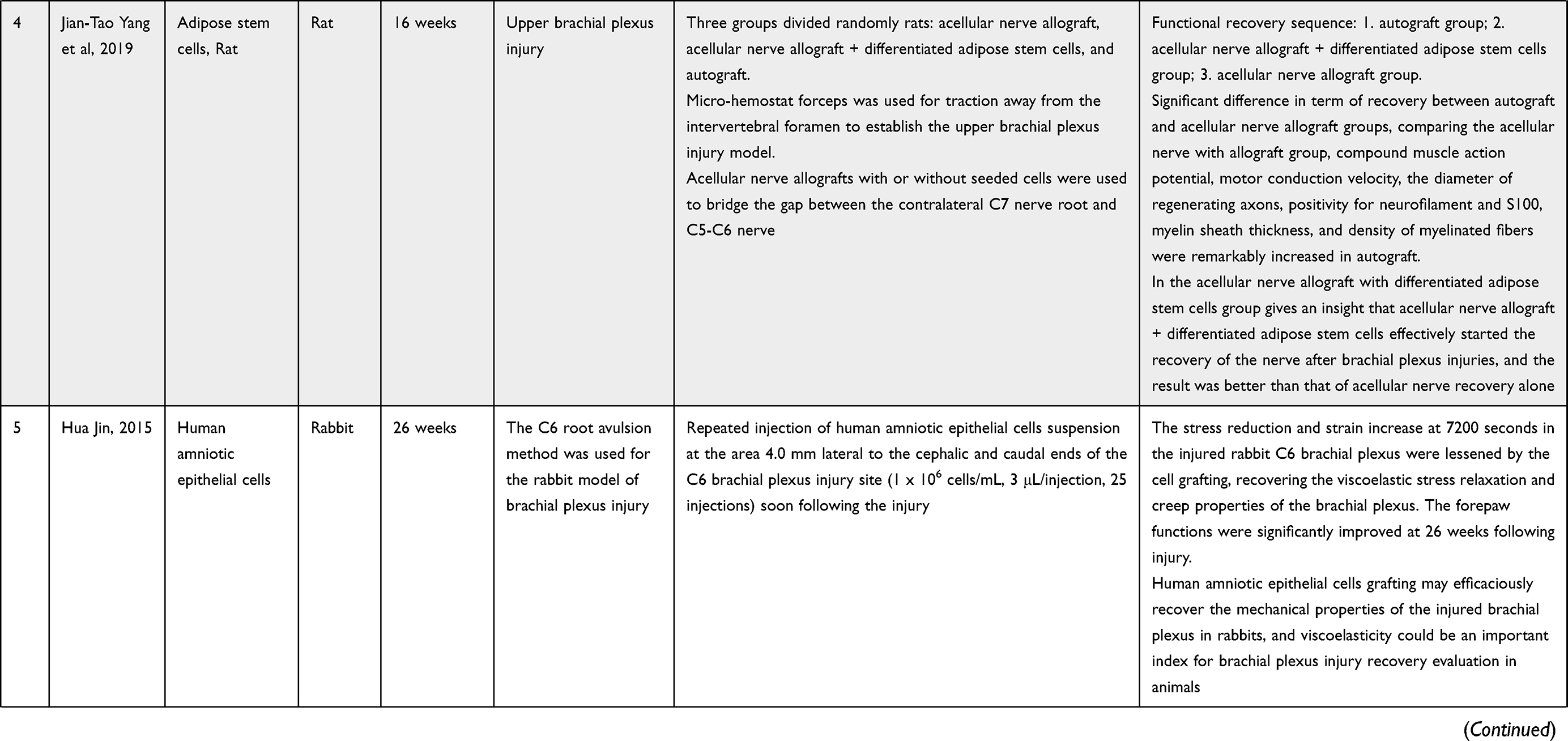 | 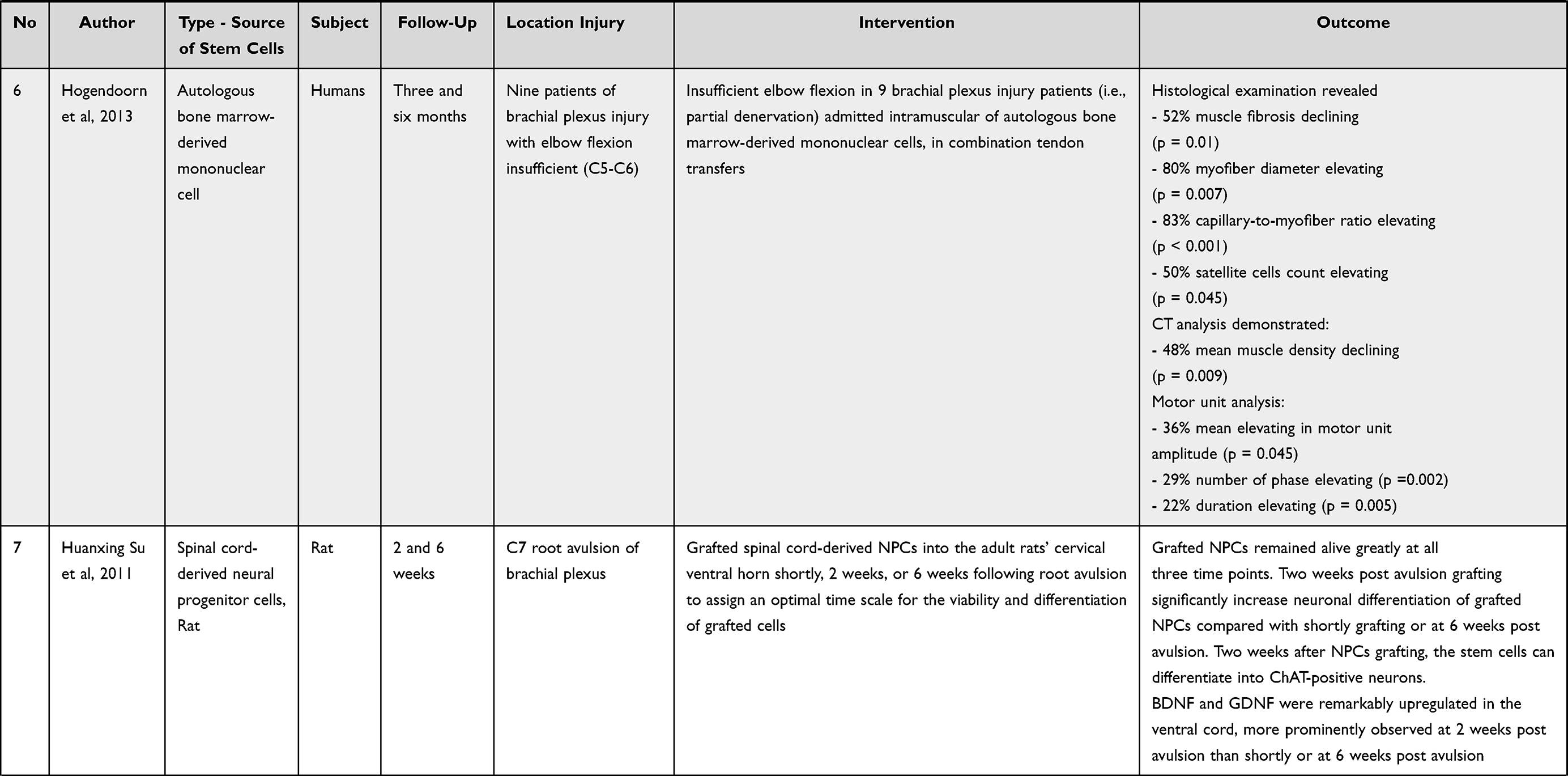 | 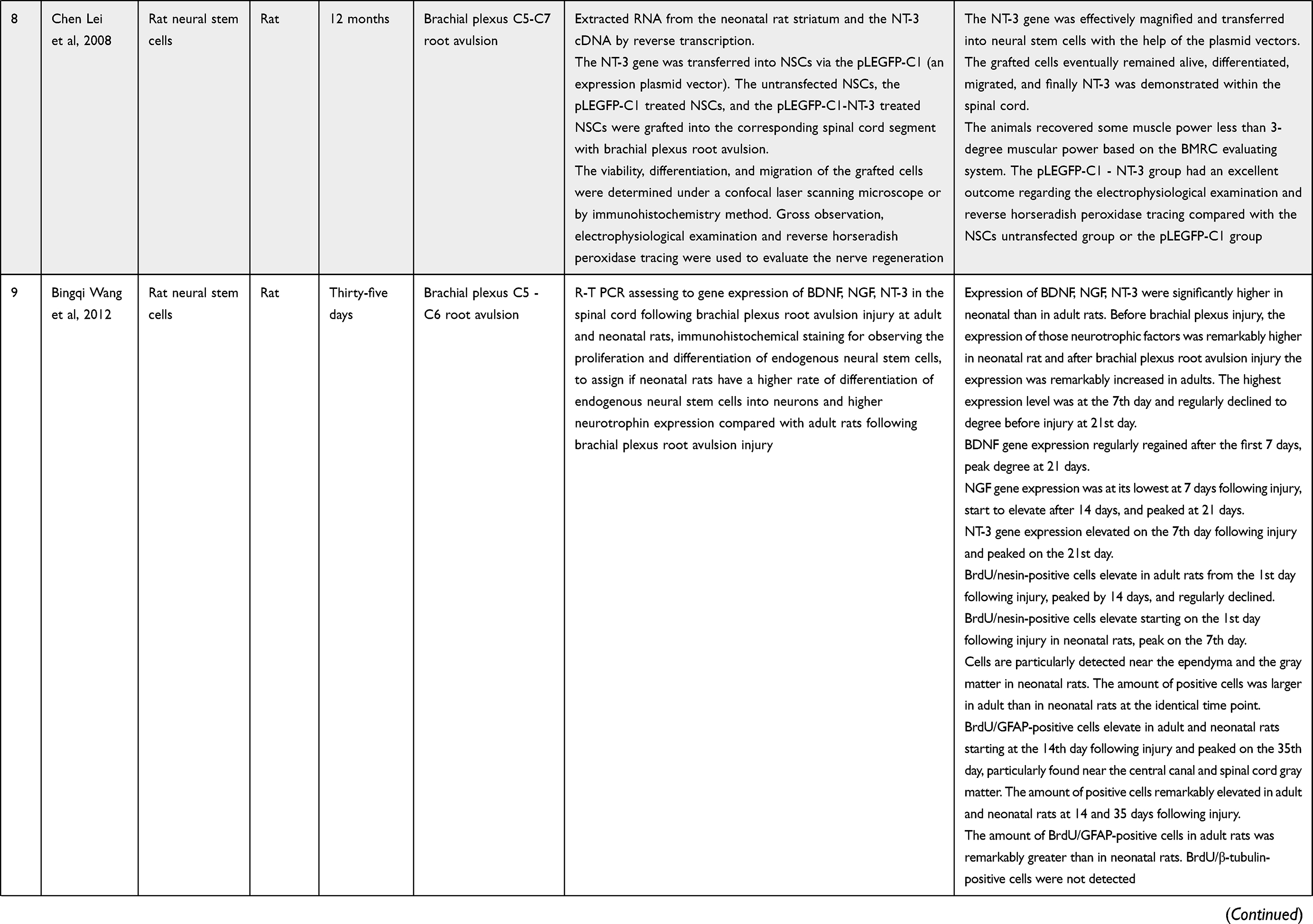 |
Table 2 Outcomes Measures Summaries |
Mostly of the studies were performed in China (7 studies/70%), the most common type of study was animal study which accounted for 7 studies (70%), and only 3 studies were conducted in humans. In the animal study literature, 5 studies used rats as models, and 2 studies used rabbits as models. The most common origins of stem cells were from bone marrow (4 studies), spinal cord-derived neural progenitor cells (2 studies), neural stem cells (2 studies), adipose (2 studies), and amnion (1 study).
All of the literature were in vivo studies, but Huanxing Su et al, 2009 performed in vitro and in vivo study in rat.2 Five studies used stem cells for the injury of the upper brachial plexus, 2 studies for the lower brachial plexus injury, and 3 studies for total brachial plexus injury.
Studies Outcomes
Studies outcomes are summarized in Table 2. This table includes length of follow-up, intervention, and major outcomes measures.
Growth Factor Production
Two studies by Su et al, 2009 and 20112,4 showed that neural progenitor cells (NPCs) can produce brain-derived neurotrophic factor (BDNF), nerve growth factor (NGF), and glial cell line-derived neurotrophic factor (GDNF). These cells can produce all the substances both in vitro and in vivo. Transplanted NPCs were able to differentiate into choline-acetyltransferase-positive neurons at 2 weeks after the initial injury. BDNF and GDNF were significantly more upregulated in the ventral cord at 2 weeks after injury than those with immediate transplantation or at 6 weeks post injury.
A study conducted by Wang et al, 2012 described that neural stem cells produced neurotrophic factors following root avulsion injury of brachial plexus. These three neurotrophic factors are BDNF, NGF, and NT-3, and their level was increased after injury.23
Electrophysiological Measurement
A study by Guo et al, indicated that the intervention group had distinctly higher CMAP amplitude and shorter CMAP latency than the model group.18 Lei et al conducted an anterior approach assessment of the latency and compound muscle action potential (CMAP) of left musculocutaneous nerve after neurotrophin-3 (NT-3) gene transfer into NSCs with the help of the pLEGFP-C1 (vector of expression plasmid) at the 12th month. The stimulator was attached to the nerve and acceptor to muscle belly of biceps. The results of this examination indicated that the result in the pLEGFP-C1-NT-3 group was excellent in comparison to the pLEGFP-C1 group or NSCs untransfected group.21 The other study stated an increase in action potential of compound muscle and motor conduction velocity.19
Histological Changes of Impaired Nerve Tissue Sections
BMSCs-treated BPI showed an increase in numbers of axons and myelinated fibers, the nerve fibers density, and the numbers of axonal regeneration, and a decrease in axonal degeneration;18 another study by Yang et al showed a remarkable increase in regenerating the axon’s diameter, myelin sheath’s thickness, and myelinated fibers’ density.19
Differentiation of Adult and Neonatal Endogenous Neural Stem Cells in Secreting Neurotrophic Factors
Wang et al 2012 described that the levels of BDNF, NGF, and NT-3 increased following root avulsion injury of brachial plexus. One day after injury the levels of BDNF, NGF, and NT-3 escalated rapidly in adult rats which then slowly reduced to normal levels within 21 days as shown by real-time PCR. In contrast, in neonatal rats, the levels of these neurotrophic factors diminished on the first day following injury. The levels then escalated slowly starting the 7th day and permanently at high levels for a certain time period.23
Human Study Outcome
A case report by Thakkar et al indicated that an improvement of finger movements was observed in a patient with traumatic total BPI after injection of Ad-MSC. Gradually finger movements of the patient developed and they were associated with an increase in muscle mass and improvement of sensory function. There was improvement in muscle power of the finger from grade 0 to grade 2 after 1 year based on Kendall and McCreary manual muscle testing. A replicate EMG-NCV examination indicated reinnervation in some nerves including musculocutaneous, radial, axillary, and suprascapular nerves. It also revealed several motor unit potentials were recruited in biceps, triceps, deltoid, and infraspinatus muscles, which has been preserved for the last 3 years.22
A study by Hogendoorn et al on nine patients revealed reduction of muscle fibrosis by 52% (p = 0.01), an 80% elevating of myofiber diameter, elevating satellite cell count by 50%, and elevating in capillary to myofiber ratio by 83%. CT analysis revealed a 48% reduction in mean muscle density (MMD). The analysis of motor unit demonstrated an average elevation of 36% in amplitude of motor unit. In this case, there was a 22% elevation in duration and 29% elevation in the number of phases. This study suggests that mononuclear cell injection enhances muscle regeneration and reinnervation in incomplete denervated muscles of the injured brachial plexus.7
Sharma et al reported a case with brachial plexus injury due to a road traffic accident (RTA). The follow up was done after four years from the first cell transplantation. The upper extremity range of motion had increased and there was a good function of the hand. The other restorations were maintained and there was no decline in muscle power over 4 years. Several muscle groups had obtained power and restorations in the muscle power attained following the previous transplantation were preserved.24
Discussion
The goal of nerve surgery in brachial plexus injuries is to restore innervation of the muscle, and in the elbow, it is flexion of the biceps muscle, even though there might be a deficit in arm function. In this case, secondary surgery is needed to improve arm function. This improvement is related to the transfer of the forearm flexor-pronator group (Steindler procedure) for the flexion of the elbow actively. Nevertheless, neurosurgery or tendon transfer cannot restore normal elbow flexion.7,25
Stem cells transplantation will become an efficacious treatment for many neurological disorders and injuries. Stem cells or progenitor cells treatment which had been shown by numerous animal studies can save some level of neurological function following the injury. A lot of positive outcomes following cells therapy seem to be related to salvage of the existing tissue rather than the repair or replacement of damaged tissue. The transplanted cells release growth factors, cytokines, and hormones to provide most of the benefits. These proteins have paracrine effect following the transplantation of the stem cells/progenitor cells. These include neuroprotection, trophic support, guidance for axonal outgrowth, and glial scar control.10,26
A narrow time window was provided for efficacious strategies of cell engrafting that have been previously demonstrated by some reports regarding the management of spinal cord injury. Severe acute inflammation is proven to occur immediately after spinal cord transection injury. Numerous cytokines for inflammation with the impacts of leading astrocyte or neurotoxicity are produced post-transection. The levels of Interleukin-1, Interleukin-6, and Tumor Necrosis Factor-α are very expressive in the beginning but then reduce sharply within 24 hours. During acute phase at the spinal cord injury, the microenvironment is unsavory for grafted cells neuronal differentiation due to acute inflammatory response. The glial scars development, the inhibitory molecules presentation, and the trophic factors lacking are the conditions that make therapeutic transplantation ineligible at the chronic phase of spinal cord injury. NPCs subacute transplantation at two weeks post-injury leads to a major viability and differentiation of engrafted cells and promotes useful restoration as well. Meanwhile, the grafted cells in transplantation models at 6–8 weeks post-injury (chronic) after spinal cord injury remain alive unsatisfactorily and show no impact on the useful restoration.2
The ideal origins of stem cells for clinical therapy must have these following characteristics, including the ability of the stem cells to be personalized, no immune rejection and tumorigenesis, simple to obtain and amplify, and efficacious in cellular or molecular replacement. The potent cell resources for grafting are mesenchymal stem cells (MSCs) and neural stem cells that may be extended in a long period of time.26,27
The ventral horn NPCs transplantation would be giving a good result for managing brachial plexus injury due to its differentiation capacity. NPCs are able to differentiate to the same cell type where they have been grafted. Following grafting into the ventral horn, human neural NPC-derived motor neurons can create axonal growth via the ventral root and peripheral nerve to establish neuromuscular junctions with their muscle targets, raising the possibility of cell replacement therapy for motor neurons loss.2,13
NPCs can secrete several neurotrophic factors both in vitro and in vivo for protecting injured neurons. These neurotrophic factors are brain-derived neurotrophic factor (BDNF), nerve growth factor (NGF), and glial cell line–derived neurotrophic factor (GDNF).2,4 These growth factors are potent factors for neuronal survival and axonal growth.2 One of the primary contributing factors to the poor functional recovery following peripheral nerve injury is the progressive decline in the capacity of motor neurons to regenerate their axons. This particularly happens over a long period in which the motor neurons remain axotomized before reinnervating the denervated muscle target.28 Therefore, the application of small doses of neurotrophic factors such as GDNF and BDNF can improve the poor functional recovery of peripheral nerve injury due to trauma by promoting the regeneration of axons in the chronically axotomized motor neurons. The presence of these neurotrophic factors encourages regeneration, increases the axonal myelination level, and augments the recovery of the sensory and motor function.29,30
The survival of injured motor neurons and their regeneration were significantly enhanced by transplanted NPCs in the avulsed ventral horn. These facts suggest that NPCs have beneficial effects on the avulsed motor neurons’ survival and axonal regeneration. This beneficial effect may be due to their innate ability to release some trophic factors in vivo.4 The stem cells transplantation by implantation of MSCs locally in the injured peripheral nerve has proven to promote the regeneration of nerve by axonal regrowth and formation of myelin. Mesenchymal stem cells apparently act as the neurotrophic generator which encourages functional recovery through neurogenesis, synaptogenesis, angiogenesis, and axonal remodeling.22
Stem cells promoted brachial plexus regeneration in preclinical studies. Ten in vivo studies have shown promising results in the majority of cases. These interventions were sustained by in vitro and in vivo studies, in which growth factor production was increased. Additionally, according to human studies, it was shown that there were improvements in motor and sensory recovery,7,22 and the muscle biopsy showed a decrease in the amount of muscle fibrosis and an elevation in the diameter of myofiber, satellite cells, and the ratio of capillary-to-myofiber.7 Side effects concerning the utilization of stem cells were not reported in these studies.
Schwann cells as the orchestrators of the peripheral nerve restoration will proliferate and arrange the myelin sheath to encourage the renovation of axon starting from the proximal to the distal end. According to these studies, stem cells can enhance the conduction velocity of CMAP and thicken the myelin sheath.18,20 These features supported the hypothesis that electrical stimulation (ES) encourages the proliferation and myelination of Schwann cells.31,32 The feature of compound muscle action potential (CMAP) at EMG is an important index to assess neuromuscular recovery, serving as the earliest EMG measurement for the recovery of muscular function.31
Besides the regeneration of the nerve, it is also important to achieve muscle restoration and reinnervation of partially denervated muscle in brachial plexus injury. Stem cell therapy has the ability to potentially repair muscle strength.33 The application of autologous BM-derived mononuclear cells (MNCs) has been done in muscle-focused clinical studies of the heart and leg. Injection of autologous BM-derived MNC in a partially denervated biceps muscle is secure, with no adverse effects regarding vital signs, bone marrow aspiration sites, injection sites, or surgical wounds. Mild anemia was found but fully recovered. The interstitial fibrosis which usually occurs in the long term was diminished by 52% after MNCs injection. These results were in accordance with the pictures of CT scan analysis that illustrated a reduction of 48% in mean muscle density/MMD.7
This study has several limitations. First, the in vivo studies need more human subjects so that the effect of mesenchymal stem cells in the peripheral nerve regeneration after brachial plexus injury in humans can be assessed further; second, the in vivo study in humans did not mention the severity of the peripheral nerve injury to brachial plexus so we could not determine whether stem cells can promote and regenerate the peripheral nerve tissue in all classifications of peripheral nerve injury; third, this study has high heterogeneity of data such as the origin of MSCs, subjects, outcomes, and follow-up duration; fourth, only English language journals were included in this review which may lead to a potential bias; and lastly the side effects regarding the injection of the stem cells in brachial plexus injury were not reported in these studies.
Conclusion
Utilization of stem cells in brachial plexus injuries holds promise in enhancing the healing process, regeneration of the nerve and the denervated muscles, as demonstrated by the available preclinical (in vitro and in vivo) and clinical studies. However, more preclinical and clinical studies are required to further assure the advantages and to determine the most appropriate stem cells to be used in injury cases.
Abbreviations
Ad-MSCs, Adipose-derived Mesenchymal Stem Cells; BDNF, Brain-derived Neurotrophic Factor; BM, Bone Marrow; BMRC, British Medical Research Council; BMSCs, Bone Marrow Stem Cells; BPI, Brachial Plexus Injury; CD, Cluster of Differentiation; Ch-AT, Choline Acetyl Transferase; CM, Conditioned Medium; CMAP, Compound Muscle Action Potential; CT, Computed Tomography; EMG, Electromyography; ES, Electrical Stimulation; pERK, phosphorylated Extracellular signal Regulated Kinase; GDNF, Glial Cell-derived Neurotrophic Factor; GFAP, Glial Fibrillary Acidic Protein; HSCs, Hematopoietic Stem Cells; HSC-BM, Bone Marrow derived Hematopoietic Stem Cells; IL, Interleukin; pMAPK, phosphorylated Mitogen-Activated Protein Kinase; MMD, Mean Muscle Density; MNCs, Mononuclear Cells; MSCs, Mesenchymal Stem Cells; Neu N, Neuron-specific nuclear protein; N-AD-MSC, Neuronal differentiated-Adipose tissue-derived-Mesenchymal Stem Cells; NCV, Nerve Conduction Velocity; NPCs, Neural Progenitor Cells; NGF, Nerve Growth Factor; NT-3, Neurotrophin-3 gene; NSCs, Neural Stem Cells; PCR, Polymerase Chain Reaction; RFP, Red Fluorescent Protein; ROM, Range of Movement; RTA, Road Traffic Accident; TNF-α, Tumor Necrosis Factor-α; USG, Ultrasonography.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yoshikawa T, Naoto Hayashi S, Yamamoto YT, et al. Brachial plexus injury: clinical manifestations, conventional imaging findings, and the latest imaging techniques. RadioGraphics. 2006;26:133–144. doi:10.1148/rg.26si065511
2. Su H, Wu Y, Yuan Q, Guo J, Zhang W, Wu W. Optimal time point for neuronal generation of transplanted neural progenitor cells in injured spinal cord following root avulsion. Cell Transplant. 2011;20(852):167–176. doi:10.3727/096368910X522090
3. Tu Y-K, Tsai Y-J, Chang C-H, Su F-C, Hsiao C-K, Tan JS. Surgical treatment for total root avulsion type brachial plexus injuries by neurotization: a prospective comparison study between total and hemicontralateral C7 nerve root transfer. Microsurgery. 2013;34(2):91–101. doi:10.1002/micr.22148
4. Su H, Zhang W, Guo J, Guo A, Yuan Q, Wu W. Neural progenitor cells enhance the survival and axonal regeneration of injured motoneurons after transplantation into the avulsed ventral horn of adult rats. J Neurotrauma. 2009;80:
5. Mekaj A, Mekaj Y. The role of pharmacological agents in nerve regeneration after peripheral nerve repair. Peripher Nerve Regen Surg New Ther Approaches Incl Biomater Cell Based Ther Dev. 2017;2017:147–174.
6. Van Niekerk EA, Tuszynski MH, Lu P, Dulin JN. Molecular and cellular mechanisms of axonal regeneration after spinal cord injury. Mol Cell Proteom. 2016;15(2):394–408. doi:10.1074/mcp.R115.053751
7. Hogendoorn S, Duijnisveld BJ, Van Duinen SG, et al. Local injection of autologous bone marrow cells to regenerate muscle in patients with traumatic brachial plexus injury: a pilot study. Bone Joint Res. 2014;3(2):38–47. doi:10.1302/2046-3758.32.2000229
8. Musarò A. The Basis of Muscle Regeneration. Adv Biol. 2014;2014:1–16. doi:10.1155/2014/612471
9. Relaix F, Bencze M, Borok MJ, et al. Perspectives on skeletal muscle stem cells. Nat Commun. 2021;12(1):1–11. doi:10.1038/s41467-020-20760-6
10. Nutt SE, Chang E-A, Suhr ST, et al. Caudalized human iPSC-derived neural progenitor cells produce neurons and glia but fail to restore function in an early chronic spinal cord injury model. Exp Neurol. 2013;248:491–503. doi:10.1016/j.expneurol.2013.07.010
11. Ke Y, Chi L, Xu R, Luo C, Liu R, Liu R. Early response of endogenous adult neural progenitor cells to acute spinal cord injury in mice. Stem Cells. 2006;24(4):1–17. doi:10.1634/stemcells.2005-0249
12. Park KI, Ourednik J, Ourednik V, et al. Global gene and cell replacement strategies via stem cells. Gene Ther. 2002;9(10):613–624. doi:10.1038/sj.gt.3301721
13. Dulin JN, Adler AF, Kumamaru H, et al. Injured adult motor and sensory axons regenerate into appropriate organotypic domains of neural progenitor grafts. Nat Commun. 2018;9(1):1–13. doi:10.1038/s41467-017-02613-x
14. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
15. Kilkenny C, Browne W, Cuthill IC, Emerson M, Altman DG. Animal research: reporting in vivo experiments: the ARRIVE guidelines. Br J Pharmacol. 2010;160(7):1577–1579. doi:10.1111/j.1476-5381.2010.00872.x
16. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Br Med J. 2010;10:1–28.
17. Hooijmans CR, Rovers MM, De Vries RBM, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol. 2014;14(1):1–9. doi:10.1186/1471-2288-14-43
18. Guo M, Li D, Wu L, Li M, Yang B. Bone marrow mesenchymal stem cells repair brachial plexus injury in rabbits through ERK pathway. Eur Rev Med Pharmacol Sci. 2020;24:1515–1523. doi:10.26355/eurrev_202002_20210
19. Yang J, Fang J, Li L, Chen G, Qin B, Gu L. Contralateral C7 transfer combined with acellular nerve allografts seeded with differentiated adipose stem cells for repairing upper brachial plexus injury in rats. Neural Regen Res. 2019;14(11):1932–1940. doi:10.4103/1673-5374.259626
20. Jin H, Yang Q, Ji F, Zhang Y, Zhao Y, Luo M. Human amniotic epithelial cell transplantation for the repair of injured brachial plexus nerve: evaluation of nerve viscoelastic properties. Neural Regen Res. 2015;10(2):260–265. doi:10.4103/1673-5374.152380
21. Lei C, Lai-jin LU, Xiao-ting M, Dong C, Zhi-xin Z, Fan Y. Reimplantation combined with transplantation of transgenic neural stem cells for treatment of brachial plexus root avulsion. Chin J Traumatol. 2008;11(5):267–273. doi:10.1016/S1008-1275(08)60054-1
22. Thakkar UG, Aruna V, Vanikar HLT. Co-infusion of autologous adipose tissue derived neuronal differentiated mesenchymal stem cells and bone marrow derived hematopoietic stem cells, a viable therapy for post-traumatic brachial plexus injury: a case report. Biomed J. 2014;37(4):237–240. doi:10.4103/2319-4170.132893
23. Wang BQ, Chen L, Liu B, et al. Differentiation of endogenous neural stem cells in adult versus neonatal rats after brachial plexus root avulsion injury. Neural Regen Res. 2012;7(23):1786–1790. doi:10.3969/j.issn.1673-5374.2012.23.004
24. Sharma A, Sane H, Gokulchandran N, et al. Cellular therapy for chronic traumatic brachial plexus injury. Adv Biomed Res. 2018;7(1):51. doi:10.4103/2277-9175.228631
25. Fox IK, Miller AK, Curtin CM. Nerve and tendon transfer surgery in cervical spinal cord injury: individualized choices to optimize function. Top Spinal Cord Inj Rehabil. 2018;24(3):275–287. doi:10.1310/sci2403-275
26. Hsu YC, Chen SL, Wang DY, Chiu IM. Stem cell-based therapy in neural repair. Biomed J. 2013;36(3):98–105. doi:10.4103/2319-4170.113226
27. Ottoboni L, Merlini A, Martino G. Neural stem cell plasticity: advantages in therapy for the injured central nervous system. Front Cell Dev Biol. 2017;5:1–21. doi:10.3389/fcell.2017.00001
28. Boyd JG, Gordon T. Glial cell line-derived neurotrophic factor and brain-derived neurotrophic factor sustain the axonal regeneration of chronically axotomized motoneurons in vivo. Exp Neurol. 2003;183(2):610–619. doi:10.1016/S0014-4886(03)00183-3
29. Wang C, Lu CF, Peng J, Hu CD, Wang Y. Roles of neural stem cells in the repair of peripheral nerve injury. Neural Regen Res. 2017;12(12):2106–2112. doi:10.4103/1673-5374.221171
30. Houlton J, Abumaria N, Hinkley SFR, Clarkson AN. Therapeutic potential of neurotrophins for repair after brain injury: a helping hand from biomaterials. Front Genet. 2019;10:1–23. doi:10.3389/fgene.2019.00001
31. Zhang XU, Xin NA, Tong LEI, Tong X. Electrical stimulation enhances peripheral nerve regeneration after crush injury in rats. Mol Med Rep. 2013;7(2013):1523–1527. doi:10.3892/mmr.2013.1395
32. Choi EH, Blasiak A, Lee J, Yang IH. Modulation of neural activity for myelination in the central nervous system. Front Neurosci. 2019;13:1–6. doi:10.3389/fnins.2019.00952
33. Judson RN, Rossi FMV. Towards stem cell therapies for skeletal muscle repair. NPJ Regen Med. 2020;5(1):1–6. doi:10.1038/s41536-020-0094-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.