Back to Journals » Journal of Pain Research » Volume 16
Prolotherapy at Multifidus Muscle versus Mechanical Needling and Sterile Water Injection in Lumbar Spinal Stenosis
Authors Chen CPC ![]() , Suputtitada A
, Suputtitada A ![]()
Received 3 May 2023
Accepted for publication 6 July 2023
Published 18 July 2023 Volume 2023:16 Pages 2477—2486
DOI https://doi.org/10.2147/JPR.S417444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Carl PC Chen,1 Areerat Suputtitada2,3
1Department of Physical Medicine & Rehabilitation, Chang Gung Memorial Hospital at Linkou and College of Medicine, Chang Gung University, Taoyuan City, Taiwan; 2Department of Rehabilitation Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Department of Rehabilitation Medicine, King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, Bangkok, Thailand
Correspondence: Areerat Suputtitada, Department of Rehabilitation Medicine, Faculty of Medicine, Chulalongkorn University, and Department of Rehabilitation Medicine, King Chulalongkorn Memorial Hospital, The Thai Red Cross Society, Rama 4 Road, Patumwan, Bangkok, 10330, Thailand, Email [email protected]; [email protected]
Objective: This observational study aimed to compare ultrasound-guided (USG) prolotherapy with 5% dextrose in water (D5W) in the multifidus muscle to USG mechanical needling and sterile water injections for the treatment of lumbar spinal stenosis (LSS).
Patients and Methods: The data was extracted from the medical records of ageing patients with LSS who received USG D5W in the multifidus muscle or USG mechanical needling and sterile water injections for the treatment of LSS by the first author. Low back pain or axial pain and leg pain or radicular pain were assessed by the visual analogue scale, and gait ability with walking distance were obtained at six different time points.
Results: Among the 211 older people who were diagnosed with LSS, 104 got USG mechanical needling and sterile water injections over the course of four weeks, while the other 107 got D5W at the multifidus muscles in a single session. Chronic low back pain, radiating pain, and the ability to walk all got much better at 1 and 3 months after the intervention, compared to VAS measures taken at the start. Patients who underwent mechanical needling with injections of sterile water performed consistently and significantly better than those who received prolotherapy in the multifidus muscles on all measures at 1, 3, and 6 months.
Conclusion: After receiving USG mechanical needling and sterile water, LSS patients reported significant improvements in low back pain, radicular pain, and ability to walk for at least 6 months. Prolotherapy with D5W in the multifidus muscle has a moderate effect for only three months.
Keywords: mechanical needling plus sterile water injection, prolotherapy with D5W, multifidus muscle, ultrasound-guided, USG, lumbar spinal stenosis, LSS
A Plain Language Summary
Lumbar spinal stenosis (LSS) affects a significant proportion of older adults and is characterised by back pain and neurogenic claudication. Age-related changes in the lumbar intervertebral discs, facet joints, and ligaments are the primary causes of spinal canal narrowing, compression, and/or ischemia of the spinal nerves, all of which contribute to back pain. The optimal treatment for LSS is still debatable It has been demonstrated that the removal of calcification and fibrosis through mechanical needling and sterile water injections is highly effective and has a longer-lasting effect on pain and walking ability than injections of corticosteroids or lidocaine. This study demonstrated higher effectiveness and a longer effect compared to prolotherapy of multifidus muscles. To remove calcification and fibrosis from the facet joints, medial branch, and multifidus muscles, a needle must be inserted precisely under ultrasound guidance. In addition, mechanical removal of calcification and fibrosis near the neurovascular bundle in these regions must be performed with extreme caution. Despite requiring multiple injections every three months, prolotherapy of the multifidus muscle carries fewer risks and is thus a more practical option. The disadvantage of D5W is that it causes pain during the procedure and has little effect on pain relief. Long-term exposure, often to D5W in prolotherapy is another area requiring investigation.
Introduction
Lumbar spinal stenosis (LSS) is a health problem that affects a lot of older people and is getting worse. It causes back pain and neurogenic claudication. The condition can affect both sides of the body, is characterised by pain, weakness, or heaviness, and gets worse with walking or prolonged standing but gets better with bending forward. Age-related changes in the lumbar intervertebral discs, facet joints, and ligaments are the primary causes of spinal canal narrowing, compression, and/or ischemia of the spinal nerves, leading to back pain.1 Magnetic resonance imaging (MRI) may not be strongly related to the signs and symptoms of LSS.2 Facet joint enlargement and breakdown can cause pain signals to travel along the nerve endings of the innervated medial branch.3 Spinal nerve root compression or inflammation causes radicular pain in spinal stenosis, often due to a herniated disc.4 The onset of degenerative disc disease can lead to more serious underlying issues such as facet arthropathy, osteophytes, spondylosis, and degenerative spinal stenosis.5 The treatment guidelines for spinal stenosis are still a matter of debate. Although lumbar facet interventions have a long history of clinical effectiveness, their efficacy and the optimal diagnostic and treatment protocols are still the subject of debate. To improve diagnostic accuracy, standardised criteria for diagnosing lumbar facet pain, including the use of physical examination signs and diagnostic injections, are required. Consensus guidelines indicate that lumbar medial branch radiofrequency ablation (RFA) may be beneficial for carefully selected patients, with medial branch block (MBB) being more predictive than intraarticular facet joint injections. To clarify the optimal screening method prior to RFA and to establish the prognostic value of diagnostic blocks for facet interventions, additional research is required.5
A recent treatment involves the removal of calcification and fibrosis through mechanical needling and sterile water injections, which have been shown to be effective and have a longer-lasting effect on pain and walking ability in cases of facet joint syndrome and lumbar spinal stenosis than corticosteroids or lidocaine injections.6,7 The somewhat high difficulty and risk require the use of a needle inserted around the facet joints and the medial branch under ultrasound guidance.6,7 We would like to examine an alternative treatment that is simpler for injectors by injecting 5% dextrose in water (D5W) into the multifidus muscle. The risks associated with a multifidus muscle injection are lower, making it a more practical option. Through segmental hypersensitization, active trigger points can refer pain. When the central nervous system becomes sensitised to painful stimuli and amplifies pain signals, segmental sensitization occurs, resulting in pain that is disproportionate to the original injury or tissue damage. With segmental desensitisation, trigger point injections (TPIs) can relieve chronic back pain. TPIs utilising local anaesthetics are a safe and effective treatment option with a low risk of myotoxicity if using low amount. TPIs are one of several options for the treatment of pain caused by trigger points and segmental sensitization.8 The multifidus muscle and facet joint both receive nerve impulses from the medial branch of the lumbar spinal cord. The pain from facet joint syndrome can be alleviated by injecting 5% dextrose in water (D5W) into the multifidus muscle. Prolotherapy, a non-conventional method of treating musculoskeletal injuries and disorders, has seen a rise in popularity over the past century.9,10
Objective
The purpose of this observational study was to compare the efficacy of ultrasound-guided (USG) prolotherapy with 5% dextrose in water injection (D5W) in the multifidus muscle versus USG mechanical needling and sterile water injections for the treatment of lumbar spinal stenosis (LSS).
Methods and Materials
Ethical Approval
The Institutional Review Board of Chang Gung Medical Foundation approved this study (IRB number 202200443A3). Since this was an observational retrospective study, written informed consent was waived.
Methods
An observational retrospective study compared two different treatments for patients with LSS. The first treatment consisted of USG mechanical needling and sterile water injections developed by Suputtitada A6,7 into the lumbar facets, medial branches to the facet joints, and the multifidus muscles,11 while the second new treatment consisted of D5W injections into the multifidus muscles. Both treatments were targeted at the most common areas of spinal stenosis on both sides of the lower back, specifically the L4-5 and L5-S1 areas.
The data of LSS patients recruited for a study at the outpatient clinic of the Department of Rehabilitation Medicine at Chang Gung Memorial Hospital in Taoyuan City, Taiwan, achieved the following diagnostic and selection criteria: The symptoms used to diagnose LSS were leg or buttock pain when walking, relief when bending forward, motor or sensory disturbances while walking, symmetrical foot pulses, lower extremity weakness, decreased walking ability, and low back pain. Only patients with pinched spinal nerves at the L4-5 and L5-S1 levels on both sides and no abnormal mass detected by magnetic resonance imaging along the lumbosacral spine were recruited. Certain conditions, however, led to patient exclusion, including the presence of a red flag sign, discogenic pain from acute disc herniation as demonstrated by a positive straight leg raising test, low back pain due to infection, inflammation, or tumor, inadequate medical history records, concurrent use of NSAIDs, analgesics, rehabilitation, or other lumbar interventions, and prior operative spine procedures.
Measurements
The study assessed the severity of pain using the Visual Analogue Scale (VAS) and gait ability with a walking distance before calf pain. The symptoms and satisfaction details of all patients were analysed at six time points: pre-injection (T0), immediately after injection (T1), 1 week after injection (T2), 1 month after injection (T3), 3 months after injection (T4), and 6 months after injection (T5).
Statistical Analysis
The characteristics of the cohort were presented as mean, standard deviation, and frequency, and changes in clinical outcomes at the six time points were analysed using repeated measures ANOVA. If the assumption of broken sphericity was made, the Greenhouse-Geisser correction was used. Student’s t-tests or Mann–Whitney U-tests were used for continuous variables (depending on normality), and chi-square tests for categorical data were used where appropriate. The significant level was set at P < 0.05.
Results
A total of 223 LSS patients were assessed for eligibility. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) flowchart is shown in Figure 1. The researchers did not use 12 medical records because they either lacked necessary information (n = 3) or did not meet the inclusion criteria (n = 9) of the patients were excluded. 104 patients received USG mechanical needling and sterile water injection over the course of four weekly sessions, and 107 received D5W at multifidus muscles once. The mean age and gender were 69.78±9.25 years, range 60–89 years, 56.73% females, and 68.21±9.23 years, range 60–90 years, 54.89% females, respectively as shown in Table 1.
 |
Table 1 Baseline Characteristics of 211 Patients |
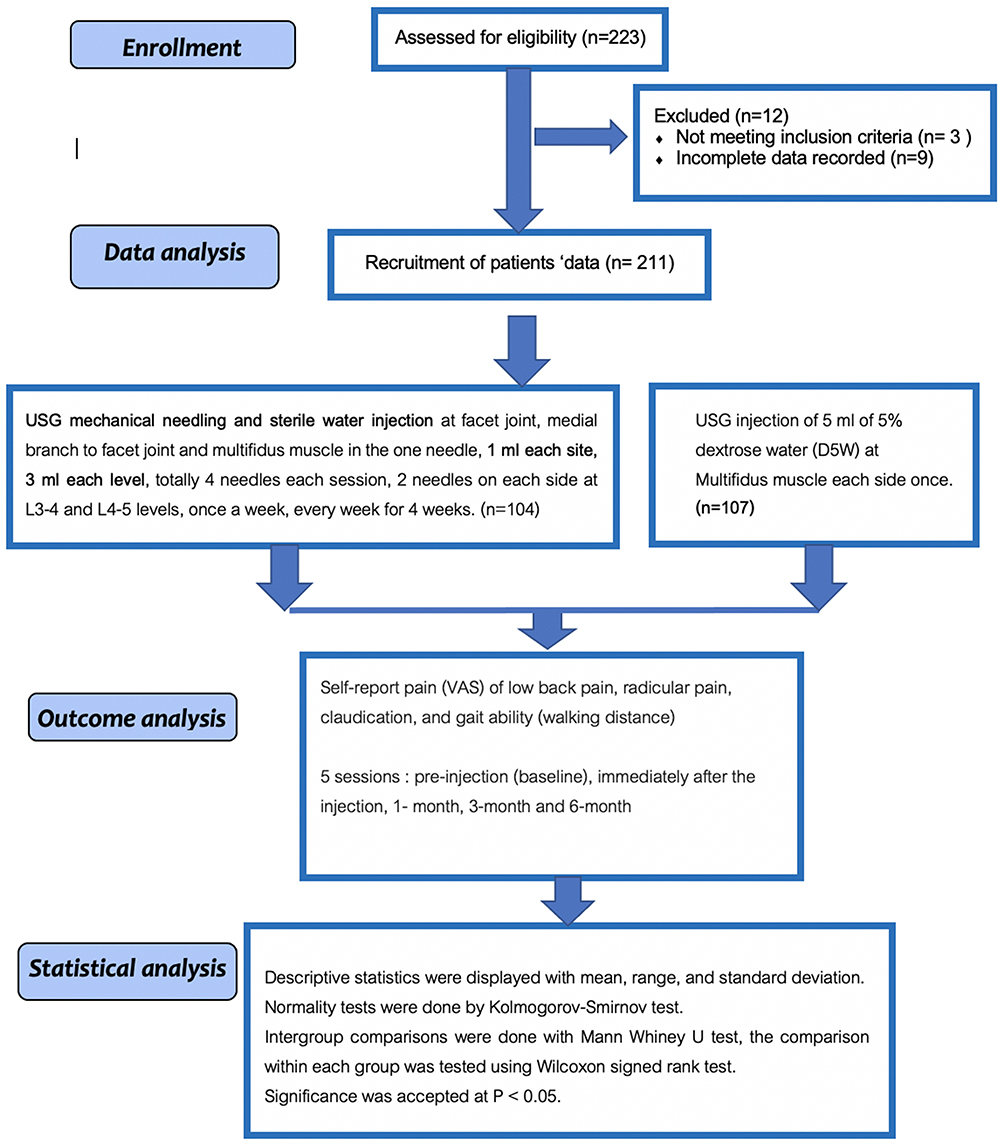 |
Figure 1 The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) flowchart. |
Within the group analysis of 104 patients who received mechanical needling with sterile water injection, they had significantly better VAS for low back pain (LBP) at T1, T3, T4, and T5 compared to T0 at P < 0.05, as shown in Figures 2A and Table 2. Within the group analysis of 107 patients who received D5W injection, the VAS of LBP was significantly better at T2 and T3 compared to T0 at P < 0.05, as shown in Figures 2A and Table 2. In addition, VAS for LBP at T1 was significantly better than T0 at P < 0.05, as shown in Figures 2A and Table 2. The VAS of LBP in the patients who received mechanical needling with sterile water was significantly better than that of those who received D5W at T1, T3, T4, T5, and T6 at P < 0.05, as shown in Figure 2B and Table 2.
 |
Table 2 Result of Treatments from 211 Medical Records |
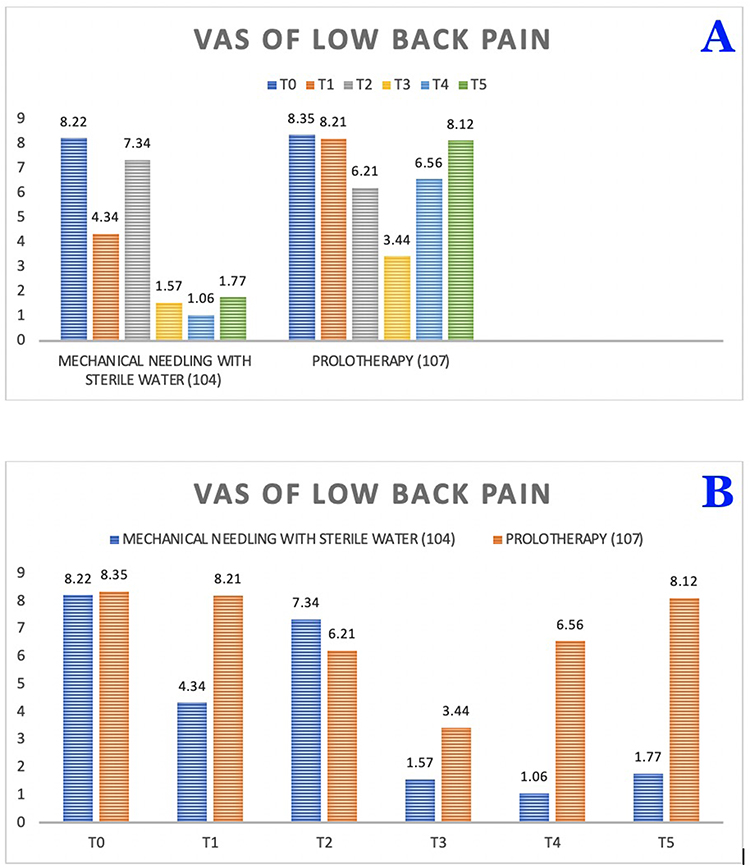 |
Figure 2 Visual analogue scales for low back pain. (A): Within group analysis. (B): Between group analysis. |
Within the group analysis of 104 patients who received mechanical needling with sterile water injection, they had significantly better VAS for leg pain at T1, T3, T4, and T5 compared to T0 at P < 0.05, as shown in Figures 3A and Table 2. Within the group analysis of 107 patients who received D5W injection, the VAS of leg pain was significantly better at T2 and T3 compared to T0 at P < 0.05, as shown in Figures 3A and Table 2. The VAS of leg pain in the patients who received mechanical needling with sterile water was significantly better than that of those who received D5W at T1, T3, T4, T5, and T6 at P < 0.05, as shown in Figure 3B and Table 2.
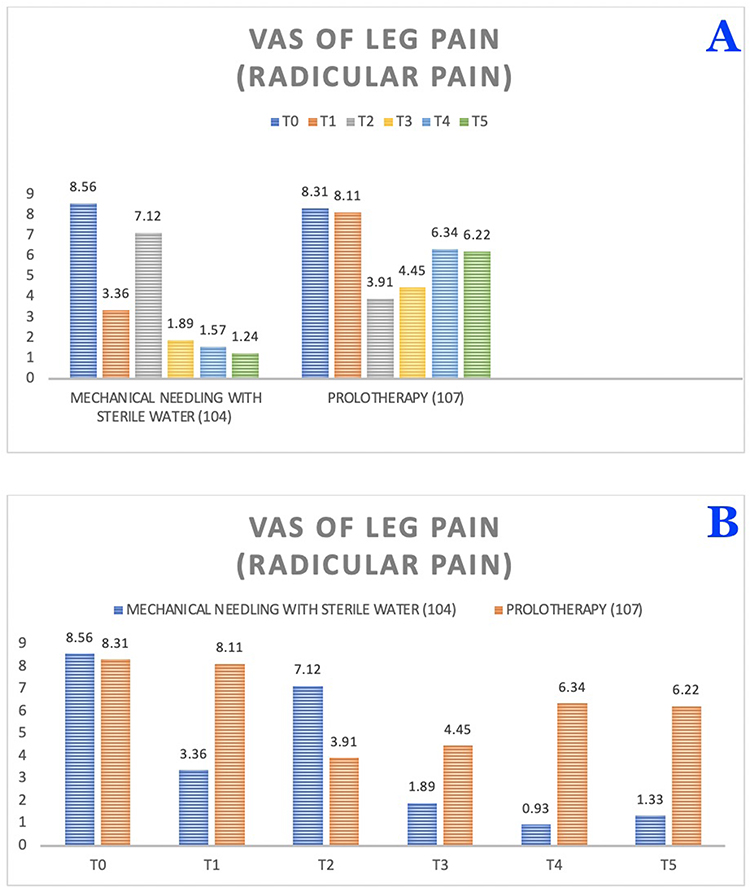 |
Figure 3 Visual analogue scales for leg pain. (A): Within group analysis. (B): Between group analysis. |
Within the group analysis of 104 patients who received mechanical needling with sterile water injection, they had significantly better walking distances at T3, T4, and T5 compared to T0 at P < 0.05, as shown in Figures 4A and Table 2. Within the group analysis of 107 patients who received D5W injection, the walking distances were significantly better at T2 and T3 compared to T0 at P < 0.05, as shown in Figures 4A and Table 2. The walking distances in the patients who received mechanical needling with sterile water were significantly better than those who received D5W at T1, T3, T4, T5, and T6 at P < 0.05, as shown in Figure 4B, and Table 2.
 |
Figure 4 Walking distances. (A): Within group analysis. (B): Between group analysis. |
There were considerably fewer incidences of dizziness after mechanical needling with sterile water injection for 1–2 hours and numbness of leg for 1–2 hours, decrease back stiffness after 1 week till 6 months, significantly at P < 0.05, as shown in Table 3. Pain and stiffness at the injection site are the most frequent adverse effects of prolotherapy. In addition to headaches, minor allergic reactions and leg pain were also reported, as shown in Table 3.
 |
Table 3 Symptoms After Injections |
Discussion
LSS patients reported significant improvements in LBP, leg pain or radicular pain, and walking ability after receiving USG mechanical needling and sterile water for at least 6 months. Prolotherapy with D5W in the multifidus muscle has only a mild effect and lasts only three months. The most common side effects of prolotherapy are pain and stiffness at the injection site. Minor allergic reactions and leg pain were also reported, in addition to headaches. The recommendation used the GRADE approach to evaluate the balance of desirable and undesirable outcomes for each treatment option and recommended multimodal rehabilitation consisting of manual therapy, supervised exercise, and cognitive-behavioral therapy as the preferred method for the management of LSS.12,13 Facet joint injections (FJI) and epidural steroid injection have been used to treat pain from spinal stenosis.5,13 However, there are still debates about their effectiveness and optimal techniques.12,13 Standardized diagnostic criteria are required to properly diagnose lumbar facet pain. While the majority of reviews support the efficacy of MBB with RFA,5 some studies disagree,5 and more research is required to determine the optimal cutoff for determining a positive diagnostic block and the appropriate volume of local anaesthetic to inject. Physical examination signs and imaging studies are insufficient to diagnose lumbar facet pain, and MBB are predictive, as recommended by consensus practice guidelines.
A recent treatment for facet joint syndrome and lumbar spinal stenosis appears to involve mechanical needling and sterile water injections to eliminate calcification and fibrosis. It has been determined that this innovative treatment is more effective and longer-lasting than injections of corticosteroids or lidocaine.6,7 Under ultrasound guidance, a needle must be inserted around the facet joints and the medial branch, which poses some difficulty and risk. Alternately, we discovered that injecting D5W into the multifidus muscle relieves pain associated with facet joint syndrome with fewer risks than needle insertion around the facet joints and medial branch. The perineural injection using D5W has been shown to be effective in treating carpal tunnel syndrome, obturator neuralgia, sacroiliac joint pain, and knee osteoarthritis.14–19 Steroid injections are not recommended due to potential neurotoxicity, and D5W can serve as a suitable alternative. The studies by Wu, Ke, et al14 and Beco and Mouchel15 demonstrate the effectiveness of perineural injection with D5W in treating carpal tunnel syndrome and obturator neuralgia, respectively. In the case of sacroiliac joint pain, Kim, Lee, et al16 found that intra-articular injections of D5W yielded better outcomes compared to steroid injections. The proposed mechanism for this improvement involves dextrose-mediated inhibition of the transient receptor potential cation channel subfamily V member 1 (TRPV1) receptors and neurogenic inflammation, as suggested by Morgan, Nencini et al17 Moreover, study by Chen, et al18 indicate that nerve blocks using D5W for genicular nerves can provide effective pain reduction lasting from 4 hours to several weeks in patients with knee osteoarthritis. The similarity of D5W’s osmolality to the human physiological condition suggests that using it as an injectant is not harmful to the nerves14,19 Chronic LBP patients may derive analgesic benefits from epidural injections of D5W. This may be the result of multiple mechanisms, including modulation of pain via the TRPV1 ion channel, replenishment of low energy stores in peripheral nerves, and hyperpolarization of nerves via activation of tandem-pore K+ channels. Nonetheless, additional research is required to confirm these mechanisms and the efficacy of D5W injections in reducing chronic pain. The potential for D5W injections to provide long-lasting relief from chronic LBP is promising and warrants additional study.9,10,12 Unfortunately, there is currently insufficient high-quality evidence to support the use of prolotherapy with dextrose as an adjunctive treatment for chronic LBP.9,10 Many studies on prolotherapy and chronic LBP yield conflicting results due to the lack of standardised patient selection criteria and the inclusion of confounding interventions.9 However, it is not yet known how exactly prolotherapy works to alleviate pain so rapidly. The most common adverse effect of prolotherapy is temporary pain and stiffness at the injection site, caused by acute inflammation. In addition to headache, leg pain, diarrhoea, nausea, and minor allergic reactions, other transient side effects may occur.5,9,10 Due to the presence of spurs and cartilaginous metaplasia, FJI and MBB can be challenging procedures in elderly patients, particularly for spinal stenosis, although the outcomes are still debatable. Mechanical needling can be used to scrape away calcification and fibrosis to improve the nociceptive effect, while sterile water injection can more extensively remove these nociceptors stimuli and cause more desensitisation, potentially enhancing the treatment’s efficacy.6,7 By modifying spinal dorsal horn activity and stimulating the central inhibitory pain pathway, this procedure can reduce both peripheral and central sensitization. When a needle is inserted into the body, various neurophysiological responses are triggered, stimulating A and C fibres and activating cortical brain regions.6,7,20 Using sterile water, the water jet procedure can also remove calcification and fibrosis from the facet joint, nerves, and muscles. It has been determined that the procedure is effective for up to six months, according to previous studies.6,7
Study Limitation and Implication
This was a retrospective examination of data from a single institution and an experienced injector, resulting in a potentially biased sample and restricted generalizability. However, the VAS measures outcomes comparable to Areerat Suputtitada6,7 for her innovation of mechanical needling and sterile water injection. Under ultrasound guidance, a needle must be inserted precisely to remove calcification and fibrosis from the facet joints, the medial branch, and the multifidus muscles. In addition, mechanical removal of calcification and fibrosis near the neurovascular bundle in these regions requires extreme caution.6,7
USG mechanical needling with sterile water injections can provide at least six months of pain relief. Reduced sensitization, resulting in analgesia, the elimination of calcification, and the reduction of fibrosis are all plausible mechanisms that promote joint and nerve regeneration via vasculature and joint gliding. Since no chemicals or pharmaceuticals are employed, the method is both cost-effective and extremely safe. Conversely, any pharmacological injection could be utilized in the future to aid in more joint regeneration. However, it requires exceptional skill and vigilance.6,7 Prolotherapy with D5W of the multifidus muscle carries fewer risks, making it the more practical option despite the fact that it requires multiple injections every three months and is less effective. Long-term exposure, typically to D5W used in prolotherapy, is another area that requires investigation. In addition, calcification and fibrosis continue to exist as a result of degenerative joint diseases. It will be challenging to inject regenerative agents in the future.
Conclusions
Patients with LSS who underwent USG mechanical needling with sterile water reported significant reductions in low back pain, radicular pain, and ability to walk that lasted for at least 6 months. Multifidus muscle prolotherapy with D5W has a moderate effect that lasts for only 3 months. Additionally, calcification and fibrosis are still present.
Ethical Approval
This study was performed in accordance with the principles of the Declaration of Helsinki, including patient data confidentiality. The Institutional Review Board of Chang Gung Medical Foundation approved this study (IRB number 202200443A3). Since this was an observational retrospective study, written informed consent was waived.
Acknowledgments
The authors are grateful to the data analysts and research management team at Chang Gung Memorial Hospital, Taoyuan City, Taiwan who were pivotal in curating and linking the data to inform the analysis presented.
Author Contributions
All authors, Areerat Suputtitada and Carl PC Chen, contributed to conception, methodology, data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Chang Gung Memorial Hospital at Linkou Research Project Grants of CMRPG5M0071 to Dr. Carl PC Chen.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Wong AYL, Karppinen J, Samartzis D. Low back pain in older adults: risk factors, management options and future directions. Scoliosis Spinal Disord. 2017;12:14. doi:10.1186/s13013-017-0121-3
2. Fushimi Y, Otani K, Tominaga R, Nakamura M, Sekiguchi M, Konno SI. The association between clinical symptoms of lumbar spinal stenosis and MRI axial imaging findings. Fukushima J Med Sci. 2021;67(3):150–160. doi:10.5387/fms.2021-22
3. Jaumard NV, Welch WC, Winkelstein BA. Spinal facet joint biomechanics and mechanotransduction in normal, injury and degenerative conditions. J Biomech Eng. 2011;133(7):071010. doi:10.1115/1.4004493
4. Chapman KB, Sayed D, Lamer T, et al. Best practices for dorsal root ganglion stimulation for chronic pain: guidelines from the American Society of Pain and Neuroscience. J Pain Res. 2023;16:839–879. doi:10.2147/JPR.S364370
5. Sayed D, Grider J, Strand N, et al. The American Society of Pain and Neuroscience (ASPN) evidence-based clinical guideline of interventional treatments for low back pain. J Pain Res. 2022;15:3729–3832. doi:10.2147/JPR.S386879
6. Suputtitada A, Chen CPC, Pongpirul K. Mechanical needling with sterile water versus lidocaine injection for lumbar spinal stenosis. Global Spine J. 2022;4:21925682221094533. doi:10.1177/21925682221094533
7. Suputtitada A, Chen CP, Pongpirul K. Mechanical needling with sterile water versus steroids injection for facet joint syndrome: a retrospective observational study. Pain Res Manag. 2022;2022:1–10. doi:10.1155/2022/9830766
8. Mense S, Gerwin RD. Central nervous system mechanisms of muscle pain: ascending pathways, central sensitization, and pain-modulating systems. In: Muscle Pain: Understanding the Mechanisms. Springer-Verlag; 2010:105–176.
9. Giordano L, Murrell WD, Maffulli N. Prolotherapy for chronic low back pain: a review of literature. Br Med Bull. 2021;138(1):96–111. doi:10.1093/bmb/ldab004
10. Maniquis-Smigel L, Reeves KD, Rosen HJ, et al. Analgesic effect and potential cumulative benefit from caudal epidural D5W in consecutive participants with chronic low-back and buttock/leg pain. J Altern Complement Med. 2018;24(12):1189–1196. doi:10.1089/acm.2018.0085
11. Chen CPC, Chen JL, Ho CS, Suputtitada A. Ultrasound-guided medial branch blocks, facet joint, and multifidus muscle injections: how it is done under one needle insertion point! Anesthesiology. 2020;132:582–583. doi:10.1097/ALN.0000000000003043
12. Bussières A, Cancelliere C, Ammendolia C, et al. Non-surgical interventions for lumbar spinal stenosis leading to neurogenic claudication: a clinical practice guideline. J Pain. 2021;22(9):1015–1039. doi:10.1016/j.jpain.2021.03.147
13. Katz JN, Zimmerman ZE, Mass H, Makhni MC. Diagnosis and management of lumbar spinal stenosis: a review. JAMA. 2022;327(17):1688–1699. doi:10.1001/jama.2022.5921
14. Wu YT, Ke MJ, Ho TY, Li TY, Shen YP, Chen LC. Randomized double-blinded clinical trial of 5% dextrose versus triamcinolone injection for carpal tunnel syndrome patients. Ann Neurol. 2018;84(4):601–610. doi:10.1002/ana.25332
15. Beco J, Mouchel J. Perineural dextrose injections in the treatment of lower urinary tract symptoms and dyspareunia induced by obturator neuralgia. Med Hypotheses. 2020;144:109991. doi:10.1016/j.mehy.2020.109991
16. Kim WM, Lee HG, Jeong CW, Kim CM, Yoon MH. A randomized controlled trial of intra-articular prolotherapy versus steroid injection for sacroiliac joint pain. J Altern Complement Med. 2010;16(12):1285–1290. doi:10.1089/acm.2010.0031
17. Morgan M, Nencini S, Thai J, Ivanusic JJ. TRPV1 activation alters the function of Aδ and C fiber sensory neurons that innervate bone. Bone. 2019;123:168–175. doi:10.1016/j.bone.2019.03.040
18. Chen CPC, Chen JL, Hsu CC, Pei YC, Chang WH, Lu HC. Injecting autologous platelet rich plasma solely into the knee joint is not adequate in treating geriatric patients with moderate to severe knee osteoarthritis. Exp Gerontol. 2019;119:1–6. doi:10.1016/j.exger.2019.01.018
19. Li TY, Chen SR, Shen YP, et al. Long-term outcome after perineural injection with 5% dextrose for carpal tunnel syndrome: a retrospective follow-up study. Rheumatology. 2021;60(2):881–887. doi:10.1093/rheumatology/keaa361
20. Suputtitada A, Nopsopon T, Rittiphairoj T, Pongpirul K. Intra-articular facet joint injection of normal saline for chronic low back pain: a systematic review and meta-analysis. Medicina. 2023;59(6):1038. doi:10.3390/medicina59061038
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.