Back to Journals » Infection and Drug Resistance » Volume 16
Prolonged Viral Shedding in Cancer Patients with Asymptomatic or Mild Omicron Infection: A Retrospective Study
Authors Yang Q, He Y, Zhou Y, Jia Q, Dai N, Ma S ![]() , Yang X, Zhang X, Sun J
, Yang X, Zhang X, Sun J
Received 18 July 2023
Accepted for publication 6 December 2023
Published 20 December 2023 Volume 2023:16 Pages 7735—7741
DOI https://doi.org/10.2147/IDR.S431126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Qiao Yang,1,* Ying He,2,* Yi Zhou,3 Qinzhu Jia,3 Nan Dai,4 Siyuan Ma,5 Xiu Yang,3 Xi Zhang,6 Jianguo Sun3
1Department of Ultrasound, The 941st Hospital of the PLA Joint Logistic Support Force, Xining, 810007, People’s Republic of China; 2Department of Psychiatry, Xinqiao Hospital, Army Medical University, Chongqing, 400037, People’s Republic of China; 3Department of Oncology, Xinqiao Hospital, Army Medical University, Chongqing, 400037, People’s Republic of China; 4Department of Oncology, Daping Hospital, Army Medical University, Chongqing, 400042, People’s Republic of China; 5Institute of Burn Research, State Key Laboratory of Trauma, Burns and Combined Injury, Army Medical University, Chongqing, 400038, People’s Republic of China; 6Department of Hematology, Xinqiao Hospital, Army Medical University, Chongqing, 400037, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianguo Sun; Xi Zhang, Xinqiao Hospital, Army Medical University, 83 Xinqiao Zhengjie Road, Shapingba District, Chongqing, 400037, People’s Republic of China, Tel +86-23-68774490, Fax +86-23-68774631, Email [email protected]; [email protected]
Background: This study aimed to investigate the risk factors for persistent viral shedding in cancer patients after Omicron infection.
Methods: Patients with asymptomatic or mild Omicron infection (≥ 18 years) who were treated in a makeshift hospital in Shanghai were enrolled from 9 Apr to 11 May, 2022. Deidentified information of all patients were collected retrospectively. Logistic regression model was used to identify risk factors associated with prolonged duration of viral shedding (defined as the time from the day of first positive SARS-CoV-2 RNA test to the first day of two consecutive negative SARS-CoV-2 RNA tests).
Results: A total of 1442 Omicron-infected patients were enrolled, including 129 cancer patients and 1313 non-cancer patients. The baseline clinical characteristics of cancer and non-cancer patients were balanced by propensity score matching (1:4). Compared with non-cancer patients, a higher odds ratio ([OR] 1.84, 95% CI 1.24– 2.76, P = 0.003) of lasting viral shedding for ≥ 7 days was found in cancer patients. Further subgroup analyses found that cancer patients were at higher risk for prolonged viral shedding in a subgroup of patients without hypertension (OR 1.89), diabetes (OR 1.80), or other chronic disease (OR 2.13), unvaccinated (OR 1.97), and asymptomatic (OR 2.36). In addition, 29 patients with active cancer and 19 patients with inactive cancer were identified. The median duration of viral shedding in the active cancer group was longer than that in the inactive cancer group (10 vs 6 days, P = 0.002). The risk of persistent viral shedding ≥ 7 days was also increased in the active cancer group (OR 5.33, 95% CI 1.49– 21.51, P = 0.013).
Conclusion: Cancer disease is an independent risk factor for prolonged viral shedding in Omicron infected patients, especially in patients with active cancer.
Keywords: omicron, cancer, persistent viral shedding, SARS-CoV-2
Introduction
Omicron was first found in Gauteng province, South Africa.1 Omicron has a high transmissibility2 and has spread rapidly around the world. In late February 2022, a wave of Omicron infections spread rapidly in Shanghai, China. As of June 2, 2022, more than 600,000 patients had been infected, approximately 90% of whom were asymptomatic.3 The Omicron variant has increased transmissibility and is more susceptible to immune evasion.2 Currently, the major Omicron variants include BA.1-BA.5, BQ, XBB, and EG.5.4 The changes of S protein characteristics of Omicron strain may be related to immune escape and resistance to antibody treatment.5
Prolonged shedding of SARS-CoV-2 RNA has been shown to be associated with sustained SARS-CoV-2 transmission and poor clinical outcomes,6,7 especially in immunocompromised patients.8 One study reported that shedding of infectious SARS-CoV-2 in patients with chronic lymphocytic leukemia could last as long as 70 days.9 Persistent viral shedding can impair host immunity and have a certain impact on subsequent anti-cancer therapy.10 The shedding of Omicron in cancer patients is unclear, although a recent study showed a reduction in the severity of COVID-19 phenotypes in cancer patients in 2022 compared with 2020.11
This study collected the clinical data of patients with Omicron infection admitted to makeshift hospitals during the pandemic in Shanghai. In this study, we first investigated the risk factors associated with prolonged viral shedding in Omicron-infected cancer patients, aiming to provide recommendations for such patients.
Methods
From April 9 to May 11, 2022, patients (≥ 18 years) with asymptomatic or mild Omicron infection who visited a makeshift hospital in Shanghai were enrolled. The deidentified information of all patients was retrospectively collected, including age, sex, hypertension history, diabetes mellitus history, history of other chronic diseases (such as chronic hepatitis B, chronic obstructive pulmonary disease, heart disease, chronic kidney disease, etc.), symptoms, vaccination status, and SARS-CoV-2 RNA test results. Vaccines included Sinovac vaccine (CoronaVac) and Sinopharm vaccine (BBIBP-CorV), and cycles and doses were not recorded at admission. Persistent viral shedding was defined as the time from the first positive SARS-CoV-2 RNA test to the first day of two consecutive negative SARS-CoV-2 RNA tests, which required an interval of more than 24 hours between two negative tests. SARS-CoV-2 RNA was detected with the use of a real-time fluorescent quantitative reverse transcription polymerase chain reaction kit (eDiagnosis, China). The Ct values of N and ORF genes ≥ 35 were considered as negative conversion, which was in line with the criteria of the 9th version of the Diagnosis and Treatment Plan of COVID-19 issued by the National Health Commission of China on Jun 27, 2022.12
The last follow-up time was on May 25, 2022. This study was approved by the Institutional Review Board of Xinqiao Hospital (2022-No.241-01). The informed consent requirement was waived by Xinqiao Hospital Institutional Review Board because only deidentified data were used.
Baseline clinical characteristics were compared between patients with and without cancer. Continuous variables were expressed as median and interquartile range (IQR), and comparison between groups was performed by the Mann–Whitney U-test. Categorical variables were expressed as frequencies and compared by Pearson’s Χ2 test.
Each cancer patient was matched to four non-cancer patients using propensity score matching (PSM) (MatchIt package, R, version 4.0.3) for further subgroup analysis. All clinical features were considered during PSM. The logistic regression model was used to identify risk factors associated with prolonged viral shedding (more than 7 days) in all patients after PSM, as well as in patients with cancer.
In addition, patients with solid cancer and a surgery history were selected for further analysis. Of these, patients who had undergone a surgery for more than five years but had not received more systemic therapy or radiotherapy were classified as having inactive cancer. Patients who had undergone surgery for less than 5 years, or who had undergone surgery for more than 5 years but still receiving systemic therapy and/or radiotherapy, were classified as active cancer. The median duration of persistent viral shedding of the two groups and the related odd ratio (OR) were calculated.
All statistical analyses were performed with the use of R software (version 4.0.3). Two-sided P value < 0.05 was considered statistically.
This study followed the principles outlined in the Declaration of Helsinki for all human investigations.
Results
A total of 1442 asymptomatic or mild patients with Omicron infection (≥ 18 years) were enrolled, including 129 cancer patients and 1313 non-cancer patients. Among all cancer patients, 17.2% of them were recorded with breast cancer, 16.1% were lung cancer, 11.5% were thyroid cancer, 10.3% were colorectal cancer, 6.9% were nasopharynx cancer, 5.7% were lymphatic and hematopoietic malignancy, 3.4% were bladder cancer, 3.4% were ovarian cancer, 2.3% were sarcoma, 23.2% were other cancers. Compared to non-cancer patients, cancer patients had higher proportions of age ≥ 60 years (55 vs 25%), female patients (57 vs 42%), hypertension history (22 vs 13%), and symptoms (29 vs 13%), but a lower proportion of vaccination (42 vs 57%) (Table 1).
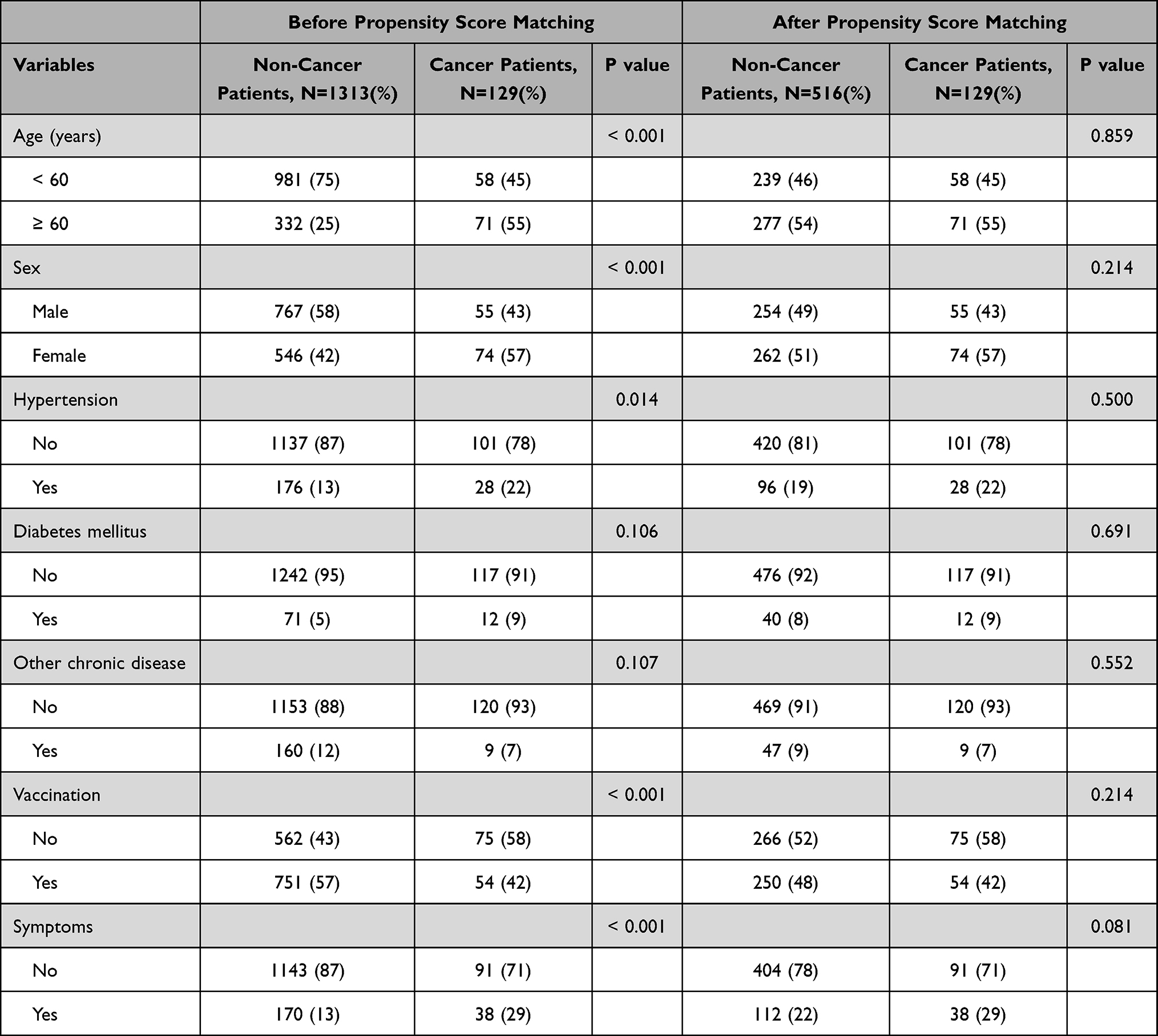 |
Table 1 Baseline Clinical Features Comparison in Omicron-Infected Patients with and without Cancer |
We performed the PSM to balance the baseline clinical features between cancer and non-cancer patients. Each cancer patient was matched with four non-cancer patients. As shown in Table 1, no difference of clinical features was found between matched groups. After PSM, the median duration of persistent viral shedding of cancer patients was 9 days (IQR 5–12 days), which was longer than that of non-cancer patients 5 days (IQR 3–7 days). An elevated OR (1.84, 95% CI 1.24–2.76, P = 0.003) of persistent viral shedding ≥ 7 days was found in cancer patients. Further subgroup analyses found that, in subgroups of age ≥ 60 years (OR 2.24, 95% CI 1.24–4.30, P = 0.011) and female (OR 2.12, 95% CI 1.25–3.66, P = 0.006), cancer patients had higher risks of persistent viral shedding ≥ 7 days. In addition, in subgroups of patients without hypertension (OR 1.89, 95% CI 1.22–2.96, P = 0.005), diabetes mellitus (OR 1.80, 95% CI 1.19–2.74, P = 0.005), or other chronic disease (OR 2.13, 95% CI 1.42–3.25, P < 0.001), unvaccinated (OR 1.97, 95% CI 1.17–3.40, P = 0.013), and asymptomatic (OR 2.36, 95% CI 1.48–3.83, P < 0.001), higher risks were also found in cancer patients. While in the counterpart subgroups, no significant difference was found (Figure 1).
 |
Figure 1 A forest plot to display the odd ratios for persistent viral shedding ≥ 7 days in cancer patients versus matched non-cancer patients in subgroup analysis. |
We also explored to identified risk factors of persistent viral shedding ≥ 7 days among cancer patients. Univariate analysis found that only age was a risk factor (≥ 60 years vs < 60 years, OR 4.59, 95% CI 2.16–10.15, P < 0.001). In addition, a trend of elevated OR was found in cancer patients with diabetes mellitus compared to those without (OR 3.13, 95% CI 0.78–20.94, P = 0.153) (Supplementary Table 1). Moreover, an analysis between active cancer group and inactive cancer group was performed. A total of 29 patients with active cancer and 19 patients with inactive cancer were identified. The median duration of persistent viral shedding in active cancer group was prolonged compared to inactive cancer group (10 vs 6 days, P = 0.002). The active cancer group also had an elevated risk of persistent viral shedding ≥ 7 days (OR 5.33, 95% CI 1.49–21.51, P = 0.013).
Discussion
In this study, we found that in the subgroups without underlying diseases (eg hypertension, diabetes mellitus, or other chronic diseases), cancer patients were at higher risk for prolonged viral shedding, which suggests that cancer may be an independent risk factor for prolonged SARS-CoV-2 positivity. Plausible reasons may be that the impaired immune system, immune tolerance, and escape in cancer patients, who have an inadequate immune response to SARS-CoV-2 infection, resulting in inefficient clearance of the SARS-CoV-2 virus.13 Virus persistence may increase the potential risk of transmission.14 Our further analysis suggested that prolonged viral shedding (median,10 days) was more pronounced in patients with active cancer. The median duration of persistent viral shedding was 6 days in both patients with inactive cancer and those without cancer. Patients with active cancer had a five-fold higher risk for persistent viral shedding ≥ 7 days than those with inactive cancer. These results support the theory that patients with active cancer represent a group with weakened immune systems that are induced by tumor growth and anticancer therapy.15
In addition, we found that patients with cancer had a higher risk of prolonged viral shedding than those without cancer in the unvaccinated subgroup, but not in the vaccinated subgroup. This suggests that vaccination of cancer patients could help to clear the virus and provide protection. Although the effectiveness of vaccination in cancer patients was relatively lower than in the control population, the overall effectiveness of vaccination in cancer patients was acceptable (approximately 65.5%).16 However, in China, the vaccination rate of the elderly is still very low, especially for the elderly with multiple underlying diseases such as cancer. Previous studies have shown that cancer patients were more susceptible to severe and critical COVID-19 and have higher mortality than patients without cancer.17,18 A few studies have suggested that the immune-related adverse events associated with COVID-19 vaccination are similar in cancer patients and in normal people.19 Vaccination is safe in cancer patients, even those are receiving treatment.20–22 Although the severity of COVID-19 phenotypes in cancer patients decreased from 2020 to 2022, patients with cancer remained at a higher risk of hospitalisation and mortality than those without cancer.11 Therefore, although the active anticancer treatment may reduce vaccine effectiveness,16 vaccination of cancer patients should be actively promoted to avoid high risk of severe disease and death due to COVID-19. However, some cancer patients are reluctant to be vaccinated against COVID-19, and some cancer patients are concerned about the possible long-term side effects of COVID-19 vaccination or its impact on cancer treatment. High vaccination coverage is highly correlated with a low COVID-19 fatality rate,3 and effective education should be intensified to increase the willingness of cancer patients to receive COVID-19 vaccination.
In addition to COVID-19 vaccination, AZD7442, a combination of two human monoclonal antibodies (tixagevimab/cilgavimab), had been proven to be effective against COVID-19 (in the pre-Omicron era).23 It has been granted emergency use authorization for moderately to severely immunocompromised patients who may not response to vaccination.24 However, the protective effect of AZD7442 on Omicron is uncertain, and real-world results are controversial. A few studies suggested that the neutralizing activity of AZD7442 against Omicron variants was significantly reduced, but it was effective.25–27 There is limited evidence for the anti-omicron effect of AZD7442 in patients with malignancies. Two studies showed that AZD7442 had low neutralizing activity against Omicron in patients with hematologic malignancies.24,28 Laracy’s study suggested that AZD7442 had positive protective effect on Omicron in patients with hematological malignancies, and the protective effect may be related to repeated administration or higher first dose.29 Evidence of solid tumors is lacking. Although the benefit may be lower, AZD7442 is currently the only available pre-exposure prophylaxis.
We also found that relatively older cancer patients were more likely to have prolonged viral shedding. The reason may be that elderly cancer patients have weaker immunity naturally. Most elderly patients may have multiple underlying diseases that lead to decreased immunity.30 Thus, these patients are less able to clear the SARS-CoV-2 virus. Diabetes is one of the major risk factors for poor outcomes in patients with SARS-CoV-2 infection.31 Although we found a trend toward prolonged viral shedding in cancer patients with diabetes, the number of cancer patients with diabetes are limited in our study. Further studies with large samples could be conducted to determine the association between diabetes and persistent viral shedding in cancer patients.
During the pandemic, without the protection of specific drugs and effective vaccines, cancer patients with persistent viral shedding will be locked in. In addition, medical resources are scarce. These may result in inadequate cancer treatment or delayed delivery of standard care.32,33 The impact of these factors on survival outcomes requires further investigation. In addition to anti-cancer treatment, the mental health of cancer patients during the pandemic is also of concern. A few studies reported that cancer patients had more mental disorders, such as anxiety, depression, and stress, than other patients during the pandemic.34–36 It’s more obvious in treatment-resistant, advanced, and painful cancer patients.36
Our study has some limitations. First, the sample size of cancer patients was limited. Thus, a univariate analysis of risk factors for persistent viral shedding ≥ 7 days in cancer patients may have limited significance. The limited sample size may also have affected the subgroup analysis after PSM. A further study with sufficient data is warranted. Second, the follow-up time was limited, and the long-term duration of positive nucleic acid testing in some patients could not be estimated. Third, the details of the anticancer treatment in this study were insufficient because the makeshift hospital is a temporal hospital used for Omicron treatment. How cancer treatment affects Omicron shedding remains unclear.
Conclusion
This study suggests that cancer disease is an independent risk factor for prolonged viral shedding in Omicron-infected patients, especially those with active cancer. This population is less able to clear the virus and may require longer SARS-CoV-2 RNA testing. In addition, vaccination should be aggressively promoted among cancer patients to better reduce the risk of severe disease and death. Moreover, education about the harms of COVID-19 in cancer patients should be strengthened to reduce the risk of infection and promote vaccination.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Xinqiao Hospital Institutional Review Board (2022-No.241-01). The Xinqiao Hospital Institutional Review Board waived the requirement for informed consent because only deidentified data were used.
Acknowledgments
We thank Prof. Rongxia Liao for English language editing. Qiao Yang and Ying He contributed equally to this work and should be considered as co-first authors.
Funding
There is no funding to report.
Disclosure
The authors declare no potential conflicts of interest.
References
1. Viana R, Moyo S, Amoako DG, et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in Southern Africa. Nature. 2022;603(7902):679–686. doi:10.1038/s41586-022-04411-y.
2. Cai J, Deng X, Yang J, et al. Modeling transmission of SARS-CoV-2 Omicron in China. Nat Med. 2022;35537471.doi:10.1038/s41591-022-01855-7
3. Zhang X, Zhang W, Chen S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet. 2022;399(10340):2011–2012. doi:10.1016/S0140-6736(22)00838-8
4. Zhou Y, Zhi H, Teng Y. The outbreak of SARS-CoV-2 Omicron lineages, immune escape, and vaccine effectivity. J Med Virol. 2023;95(1):e28138. doi:10.1002/jmv.28138
5. Parsons RJ, Acharya P. Evolution of the SARS-CoV-2 Omicron spike. Cell Rep. 2023;42(12):113444. doi:10.1016/j.celrep.2023.113444
6. Chang MG, Yuan X, Yuan X, et al. Time kinetics of viral clearance and resolution of symptoms in novel coronavirus infection. Am J Resp Crit Care. 2020;201(9):1150–1152. doi:10.1164/rccm.202003-0524LE
7. Yang Y, Hu X, Xiong L, et al. Clinical characteristics of hospitalized mild/moderate COVID-19 patients with a prolonged negative conversion time of SARS-CoV-2 nucleic acid detection. Bmc Infect Dis. 2021;21(1):141. doi:10.1186/s12879-021-05851-z
8. Xiao AT, Tong YX, Zhang S. Profile of RT-PCR for SARS-CoV-2: a preliminary study from 56 COVID-19 patients. Clin Infect Dis. 2020;71(16):2249–2251. doi:10.1093/cid/ciaa460.
9. Avanzato VA, Matson MJ, Seifert SN, et al. Case study: prolonged infectious SARS-CoV-2 shedding from an asymptomatic immunocompromised individual with cancer. Cell. 2020;183(7):1901–1912.e9. doi:10.1016/j.cell.2020.10.049
10. Gur I, Giladi A, Isenberg YN, Neuberger A, Stern A. COVID-19 in patients with hematologic malignancies: clinical manifestations, persistence, and immune response. Acta Haematol-Basel. 2022;145(3):297–309. doi:10.1159/000523872
11. Starkey T, Ionescu MC, Tilby M, et al. A population-scale temporal case-control evaluation of COVID-19 disease phenotype and related outcome rates in patients with cancer in England (UKCCP). Sci Rep-Uk. 2023;13(1):11327. doi:10.1038/s41598-023-36990-9
12. National Health Commission of the People’s Republic of China . 关于印发新型冠状病毒肺炎防控方案 (第九版) 的通知 [Notice on Issuing the Novel Coronavirus Pneumonia Prevention and Control Plan (Ninth Edition)]. Available from: http://www.nhc.gov.cn/jkj/s3577/202206/de224e7784fe4007b7189c1f1c9d5e85.shtml.
13. Yazdanpanah F, Hamblin MR, Rezaei N. The immune system and COVID-19: friend or foe? Life Sci. 2020;256:117900. doi:10.1016/j.lfs.2020.117900
14. Joukar F, Yaghubi KT, Khoshsorour M, et al. Persistence of SARS-CoV-2 RNA in the nasopharyngeal, blood, urine, and stool samples of patients with COVID-19: a hospital-based longitudinal study. Virol J. 2021;18(1):134. doi:10.1186/s12985-021-01599-9
15. Liu C, Zhao Y, Okwan-Duodu D, Basho R, Cui X. COVID-19 in cancer patients: risk, clinical features, and management. Cancer Biol Med. 2020;17(3):519–527. doi:10.20892/j.issn.2095-3941.2020.0289
16. Lee L, Starkey T, Ionescu MC, et al. Vaccine effectiveness against COVID-19 breakthrough infections in patients with cancer (UKCCEP): a population-based test-negative case-control study. Lancet Oncol. 2022;23(6):748–757. doi:10.1016/S1470-2045(22)00202-9
17. Zhou Y, Yang Q, Ye J, et al. Clinical features and death risk factors in COVID-19 patients with cancer: a retrospective study. Bmc Infect Dis. 2021;21(1):760. doi:10.1186/s12879-021-06495-9
18. Tian J, Yuan X, Xiao J, et al. Clinical characteristics and risk factors associated with COVID-19 disease severity in patients with cancer in Wuhan, China: a multicentre, retrospective, cohort study. Lancet Oncol. 2020;21(7):893–903. doi:10.1016/S1470-2045(20)30309-0
19. Waissengrin B, Agbarya A, Safadi E, Padova H, Wolf I. Short-term safety of the BNT162b2 mRNA COVID-19 vaccine in patients with cancer treated with immune checkpoint inhibitors. Lancet Oncol. 2021;22(5):581–583. doi:10.1016/S1470-2045(21)00155-8
20. Mandal A, Singh P, Samaddar A, et al. Vaccination of cancer patients against COVID-19: towards the end of a dilemma. Med Oncol. 2021;38(8):92. doi:10.1007/s12032-021-01540-8
21. Wang L, Xu Y, Zhang L, et al. COVID-19 vaccination for cancer patients: progress and preliminary recommendations. Zhongguo Fei Ai Za Zhi. 2021;24(6):377–383. doi:10.3779/j.issn.1009-3419.2021.101.18.
22. Luo B, Li J, Hou X, et al. Indications for and contraindications of immune checkpoint inhibitors in cancer patients with COVID-19 vaccination. Future Oncol. 2021;17(26):3477–3484. doi:10.2217/fon-2021-0288.
23. Levin MJ, Ustianowski A, De Wit S, et al. Intramuscular AZD7442 (tixagevimab-cilgavimab) for prevention of Covid-19. New Engl J Med. 2022;386(23):2188–2200. doi:10.1056/NEJMoa2116620.
24. Stuver R, Shah GL, Korde NS, et al. Activity of AZD7442 (tixagevimab-cilgavimab) against Omicron SARS-CoV-2 in patients with hematologic malignancies. Cancer Cell. 2022;40(6):590–591. doi:10.1016/j.ccell.2022.05.007.
25. Chen B, Haste N, Binkin N, et al. Real world effectiveness of tixagevimab/cilgavimab (evusheld) in the Omicron era. PLoS One. 2023;18(4):e0275356. doi:10.1371/journal.pone.0275356.
26. Zhang J, Cong Y, Duan L, Zhang J. Combined antibodies evusheld against the sars-cov-2 omicron variants ba.1.1 and ba.5: immune escape mechanism from molecular simulation. J Chem Inf Model. 2023;63(16):5297–5308. doi:10.1021/acs.jcim.3c00813.
27. Zhao Q, Wang X, Zhang Z, et al. Serum neutralization of SARS-CoV-2 Omicron BA.2, BA.2.75, BA.2.76, BA.5, BF.7, BQ.1.1 and XBB.1.5 in individuals receiving Evusheld. J Med Virol. 2023;95(7):e28932. doi:10.1002/jmv.28932
28. Chang A, Koff JL, Lai L, et al. Low neutralizing activity of AZD7442 against current SARS-CoV-2 Omicron variants in patients with B-cell malignancies. Blood Adv. 2023;7(11):2459–2462. doi:10.1182/bloodadvances.2022009475
29. Laracy JC, Yan J, Steiger SN, et al. Predictors of SARS-CoV-2 Omicron breakthrough infection after receipt of AZD7442 (tixagevimab-cilgavimab) for pre-exposure prophylaxis among hematologic malignancy patients. Haematologica. 2023;108(11):3058–3067. doi:10.3324/haematol.2023.283015.
30. Nanda A, Vura N, Gravenstein S. COVID-19 in older adults. Aging Clin Exp Res. 2020;32(7):1199–1202. doi:10.1007/s40520-020-01581-5
31. Yonekawa A, Shimono N. Clinical significance of covid-19 and diabetes: in the pandemic situation of sars-cov-2 variants including Omicron (B.1.1.529). Biology-Basel. 2022;11(3). doi:10.3390/biology11030400
32. Melidis C, Vantsos M. [Comment] Ethical and practical considerations on cancer recommendations duringCOVID-19 pandemic. Mol Clin Oncol. 2020;13(3):5. doi:10.3892/mco.2020.2075
33. Boniface D, Tapia-Rico G. Oncology during the covid-19 pandemic: a lockdown perspective. Curr Oncol Rep. 2022;24(10):1219–1235. doi:10.1007/s11912-022-01301-4.PubMed:
34. Pigozzi E, Tregnago D, Costa L, et al. Psychological impact of Covid-19 pandemic on oncological patients: a survey in Northern Italy. PLoS One. 2021;16(3):e0248714. doi:10.1371/journal.pone.0248714
35. Miaskowski C, Paul SM, Snowberg K, et al. Stress and symptom burden in oncology patients during the covid-19 pandemic. J Pain Symptom Manag. 2020;60(5):e25–e34. doi:10.1016/j.jpainsymman.2020.08.037
36. Hesary FB, Salehiniya H. The impact of the covid-19 epidemic on diagnosis, treatment, concerns, problems, and mental health in patients with gastric cancer. J Gastrointest Cancer. 2022;53(3):797–804. doi:10.1007/s12029-021-00692-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.