Back to Journals » International Medical Case Reports Journal » Volume 16
Progressive Cerebral Venous Thrombosis with Cranial Nerve Palsies in an Adolescent African Girl & Associated Diagnostic Pitfalls: A Rare Case Report
Authors Asfaw YA ![]() , Huang H
, Huang H ![]() , Taimur M, Anand A
, Taimur M, Anand A ![]() , Poudel S, Garg T, Asfaw BA, Abebe BM
, Poudel S, Garg T, Asfaw BA, Abebe BM ![]() , Akbariromani H, Lazovic G, Cueva W
, Akbariromani H, Lazovic G, Cueva W
Received 9 July 2022
Accepted for publication 31 December 2022
Published 12 January 2023 Volume 2023:16 Pages 45—51
DOI https://doi.org/10.2147/IMCRJ.S381748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Yonathan Aliye Asfaw,1,2 Helen Huang,2,3 Muhammad Taimur,2,4 Ayush Anand,2,5 Sujan Poudel,2 Tulika Garg,2,6 Bethlehem Aliye Asfaw,1,2 Befekadu Molalegn Abebe,1,2 Hanieh Akbariromani,2,7 Gavrilo Lazovic,8 Wilson Cueva9
1Internal Medicine Department, University of Gondar, College of Medicine and Health Sciences, Gondar, Ethiopia; 2Department of Research & Academic Affairs, Larkin Community Hospital, South Miami, FL, USA; 3Internal Medicine Department, University of Medicine and Health Sciences, Royal College of Surgeons in Ireland, Dublin, Ireland; 4Internal Medicine Department, Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan; 5Internal Medicine Department, B. P. Koirala Institute of Health Sciences, Dharan, Nepal; 6Internal Medicine Department, Government Medical College and Hospital, Chandigarh, India; 7Internal Medicine Department, Islamic Azad University, Tehran Medical Branch, Tehran, Iran; 8Department of Emergency Medicine, Larkin Community Hospital, South Miami, FL, USA; 9Department of Neurology, Larkin Community Hospital, South Miami, FL, USA
Correspondence: Yonathan Aliye Asfaw, Internal Medicine Department, University of Gondar, College of Medicine and Health Sciences, Gondar, Ethiopia, Email [email protected]
Abstract: Cerebral venous thrombosis (CVT) is a cerebrovascular disorder caused by complete or partial occlusion of the cerebral venous and sinus system. The etiology has been attributed to hypercoagulability and pro-thrombotic states, leading to raised intracranial pressures that often manifest as headaches and focal neurological deficits. However, the multifactorial nature of CVT can create a diagnostic conundrum for clinicians. We describe a unique case of a 16-year-old female who presented with convulsions, postictal confusion, and drowsiness followed by residual weakness of her extremities. She initially presented to the primary care center with headache, high-grade fever, and altered mental status and was empirically treated for pyogenic meningitis. The patient failed to improve with a week of antibiotics and was referred to the tertiary care center for urgent attention. On presentation, the patient developed VI and VII cranial nerve palsy. Subsequently, MRI images showed filling defects in the superior sagittal, right transverse, and sigmoid sinuses with right parietal gyral T1 hyperintensity and T2 hypo-intensity. She was diagnosed with septic CVT based on sinus venous thrombosis and venous infarction, probably secondary to meningococcal pneumonia. It can be challenging to distinguish between both conditions as their presentations overlap. Moreover, cranial nerve palsy is an infrequent manifestation of CVT, with unclear pathogenesis. We highlight the role of neuro-imaging in the early detection of CVT and bring to light the unfamiliar symptoms and a more varied clinical spectrum that may hinder the diagnosis in a limited-resource setting. Future research should be explicitly modeled to improve the diagnostic efficiency of CVT and improve outcomes in younger patient populations.
Keywords: cerebral venous thrombosis, meningitis, cranial nerve palsy, systemic infection, neuro-imaging, case report
Introduction
Cerebral venous thrombosis (CVT) is a cerebrovascular disorder involving the intracranial veins and sinuses and contributes to nearly 0.5% of strokes.1–3 It is a rare disorder with an incidence of 3 to 5 people per million and about 7 cases per million in pediatric age group.1,2 Approximately four-fifths of patients have favorable neurological outcomes, and mortality is less than 10.1,2 Two distinct mechanisms can contribute to CVT.1,4 Firstly, CVT can develop due to cerebral vein occlusion leading to localized edema and venous infarction.1,4 Secondly, dural venous sinus occlusion can decrease cerebrospinal fluid absorption and intracranial hypertension.1,4 Though the causes are multifactorial, infection secondary to CVT can lead to septic thrombosis of the cavernous sinuses (CST) and has become an infrequent entity since the introduction of antibiotics. Despite this, the severe morbidity associated with CST necessitates early recognition and treatment to prevent lethal neurological complications. The developments in neuroimaging modalities in the past two decades have enabled clinicians to diagnose the case early, but CST can be complicated by many overlapping signs and symptoms of other diseases that require a high degree of clinical suspicion.1,2,4 This case report is unique in that an otherwise healthy young patient developed thrombosis in her dural venous sinus. It emphasizes to the clinician the point that infection anywhere in the body could create a hypercoagulable state with devastating consequences.
Case Report
A 16 years old girl presented with complaint of abnormal body movements for one week. The patient reported multiple generalized abnormal jerky movements of upper and lower extremities, up rolling of the eyes, and drooling of saliva, as witnessed by bystanders. She reported postictal confusion and drowsiness for half an hour with associated residual weakness of her left upper and lower extremities. Three weeks before her presentation, she mentioned having a productive cough with pleuritic chest pain, self-reported intermittent fever, night sweats, and decreased appetite. She also reported neck pain and a diffuse throbbing headache of a same duration. For this complaint, she was taken to another hospital where she was empirically treated for pyogenic meningitis with Ceftriaxone 2gm IV BID and Dexamethasone 8mg IV QID. However, she did not show improvement in her symptoms after a few days of treatment and was referred to our hospital for better care. Vancomycin was not given initially and the treatment she was given before referral to our hospital was empirical with no CSF analysis and CT scanning of the head. Upon presentation, she appeared lethargic with tachycardia (120 beats per minute), the temperature of 38.6°C, blood pressure of 110/70 mmHg, and respiratory rate of 22 breaths per minute. Lung examination was remarkable for left-sided bronchial breath sound. Cardiovascular and abdominal examination unremarkable. On CNS examination, she was conscious with intact orientation to time, person, and place. Cranial nerve (CN) examination revealed CN VI and CN VII palsy as she could not abduct her left eye and close her eyes bilaterally, more on the left. Muscle strength was 2/5 on the left upper and lower extremities and 3/5 on the right upper and lower extremities. Deep tendon reflex (DTR) was 3/4 on the right brachial and knee but normal on the left side. The tone was increased in all extremities. The Babinski sign was positive on the right side.
Extensive investigations showed normal WBC count, and normocytic normochromic anemia. Her Erythrocyte sedimentation rate was elevated, but ANA was non-reactive. She had mild albuminemia. RFT and LFT were within the normal range. PT, PTT and INR were also normal. HIV antibody test, VDRL, and rheumatoid factor were negative. Chest x-ray was remarkable for left lung opacity suggestive of pneumonia. Magnetic resonance imaging (MRI) showed filling defects on the superior sagittal sinus, right transverse, and sigmoid sinuses, indicating sinus venous thrombosis on the corresponding sinuses (Figure 1). There were right parietal gyral T1 hyperintensity and fluid attenuated inversion recovery (FLAIR) and T2 hyper-intensity with restriction on diffuse weighted imaging (DWI) indicating venous infarction (Figures 2 and 3). After imaging, lumbar puncture was done, which showed no WBC. Glucose and protein in the cerebrospinal fluid (CSF) were within a normal range. EEG was not done.
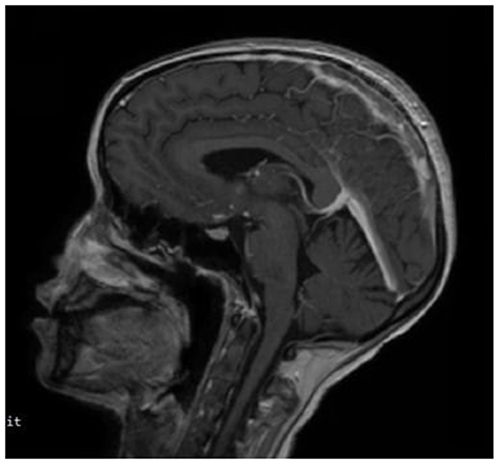 |
Figure 1 Magnetic resonance imaging T1 weighted image without contrast demonstrating filling defects in the superior sagittal sinus. |
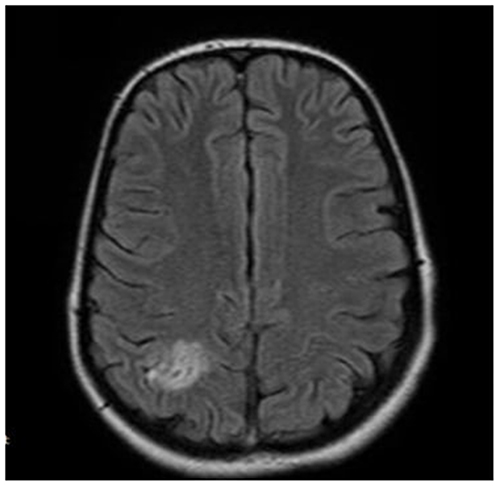 |
Figure 2 Magnetic resonance imaging FLAIR weighted image depicting subcortical hyperintensity in the right parietal lobe. |
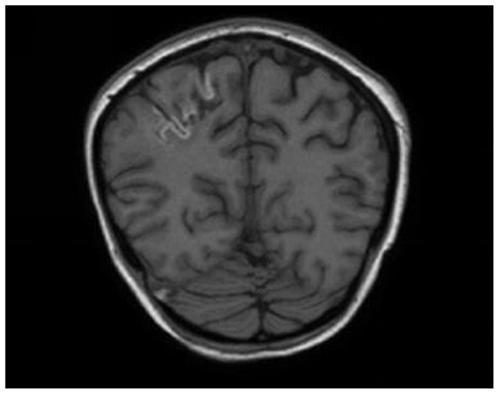 |
Figure 3 Magnetic resonance imaging T1 weighted image, without contrast, hyperintensity in the right parietal lobe; there is also hyperintense thrombus in the right transverse sinus. |
She was admitted with the working diagnosis of septic CVT and was started with a treatment dose of Unfractionated Heparin 12,500 IU BID. Warfarin 5 mg per os was later started for maintenance after an appropriate bridging period. The antiepileptic phenytoin was loaded with 10mg/kg and was maintained at 5mg/kg, which significantly controlled the abnormal body movements. Additionally, empirical course of antibiotics was commenced, including Ceftriaxone 2g IV BID, Vancomycin 1g IV BID, and Metronidazole 500mg IV TID. After 2 weeks of admission, her fever was controlled. There was a significant improvement in the extremity weaknesses noted at admission, and she was ambulatory during discharge. Power was 5/5 in all extremities at discharge. The patient is an otherwise healthy young individual with no comorbidity and no family history of a known disease. She was not taking any medication.
Discussion
This case study presents a constellation of signs and symptoms that make CVT a complex condition to diagnose and treat. As a result, it is vital to identify the causes of local or systemic factors. The etiology of CVT is associated with multiple disorders that predispose patients to hypercoagulability and pro-thrombotic states, a risk factor that is also present in deep venous thrombosis (DVT).5–7 A summary of all possible etiologies is reported in Table 1. In the literature, the most common causes of septic CVT are bacterial infections spreading from a primary source (ie, lungs) to the cavernous sinuses, with a notable rise in viral cases due to the COVID-19 pandemic.9
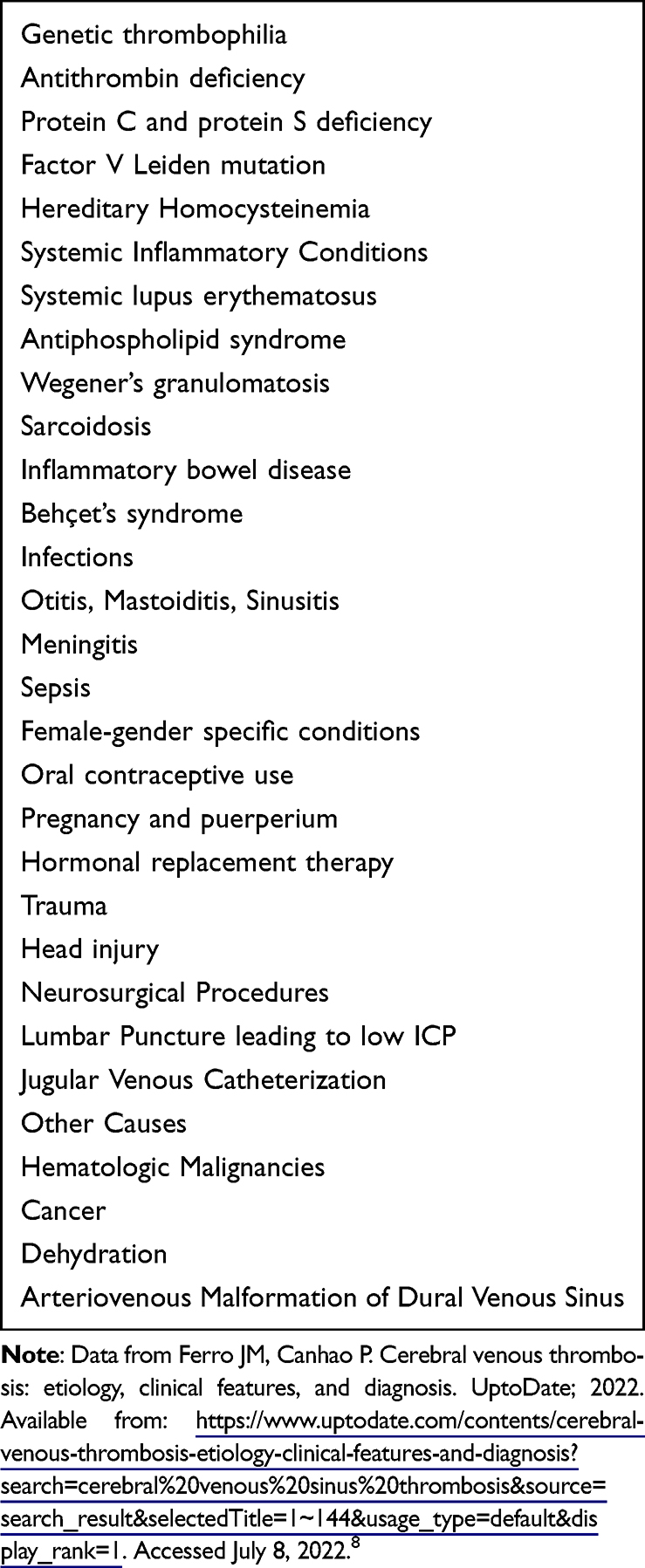 |
Table 1 Etiology and Risk-Factors Associated with Cerebral Venous Thrombosis |
Although the frequency of infectious causes complicated by CVT has declined in recent years to around 6% to 12% in adults, infections of the head and neck, and systemic infection may lead to thrombosis of the venous sinuses.5 Based on our patient’s history, symptoms of fever, chills, and pleuritic chest pain typically describe the clinical picture of pneumonia as the inciting event of septic cerebral venous thrombosis.10 It is difficult to discern the cause of pneumonia in this patient, as the absence of bacterial cultures from previous hospital visits could not conclude meningococcal pneumonia as the etiology. However, her previous medical history suggests pneumonia secondary to septic CVT was a late complication of pyogenic meningitis. These findings aligned with a retrospective study by Jacob et al, where 22 patients with CVT secondary to infectious etiologies were described, with 12 patients being treated with pyogenic meningitis.11 In this patient group, the most common sinuses involved were the transverse sinus followed by the sigmoid sinus. Though the mechanism of septic CVT is entirely unclear, direct bacterial invasion of the sinuses can cause intravascular coagulation due to a procoagulant and anti-fibrinolytic reaction as a possible mechanism. Additionally, a systemic infection could also stimulate a pro-inflammatory reaction that causes endothelial injury and thus creating a hypercoagulable state that predisposes patients to venous thrombosis.12 However, it can be challenging to recognize pneumococcal meningitis complicated by CVT, as symptoms of headache, focal neurological deficits, and seizures are clinical features present in both conditions.13
Based on disease progression, the most commonly reported presentations of CVT include headaches, visual deficits, papilledema, focal neurological deficits, and seizures accompanied by postictal confusion.5 In our case, these typical symptoms were accompanied by cranial nerve palsy, which has only been reported in around 12% of CVT cases with preferential involvement in CN II, IV, and VI.14,15 Facial palsy associated with CVT is relatively uncommon, and the understanding of its pathophysiology is very limited.16 Pressure palsy, either directly caused by a thrombotic clot laying near the nerve or indirectly induced by higher intracranial pressure, was assumed to be the origin of the cranial nerve disorders documented in the older literature.17 Kuehnen et al reported cranial nerve palsy as the only symptom of isolated transverse sinus thrombosis, likely due to transient oxygen impairment or glucose intake caused by venous drainage impairment.18 A false localizing sign is the most common symptom of sixth cranial nerve palsy. CN VI palsy is characterized by impaired abduction of the ipsilateral eye, leading to diplopia or double vision.19 Though its pathogenesis is unclear, abducens nerve palsy is thought to develop due to increased intracranial pressure and has previously been reported in Özgönül et al and Marzo et al.20,21 The involvement of cranial nerves in thrombosis of the petrosal sinuses is known from the older literature, along with other neurological events. Petrosal sinuses thrombosis is primarily defined by a CN V palsy for the superior sinus and CN 6 palsy for the inferior one.22 Klestadt et al linked CN VI lesions to inferior petrosal sinus thrombosis, suggesting that the lateral rectus palsy associated with otitic hydrocephalus could have stated the emergence of the syndrome in the petrosal sinus attributed to an increased intracranial pressure.23
Over the past decades, increased awareness of the diagnosis and improved neuroimaging have helped in effective management.24 Computed tomography scan of head is often the first investigation performed to exclude various acute or subacute cerebral disorders. However, an MRI offers a significant advantage for evaluating possible CVT- sensitivity to blood flow and the ability to visualize intraluminal thrombus promptly with T1 and T2 weighted images.25 T2 hyperintensity is suggestive of thrombus in subacute or chronic phase.25 However, diffusion-weighted imaging (DWI) and perfusion-weighted MRI can help improve the accuracy of CVT diagnosis with high signal intensity as restricted diffusion.26 One can use a contrast agent or not when doing the MR venography modality.27 Time-resolved contrast-enhanced MR venography has very superior accuracy which relies on luminal filling by contrast material rather than MR flow phenomena when utilizing the time-of-fight method.27
Nevertheless, there were certain limitations in our case. Even though meningitis was the suspected cause of CVT in our case, a blood sample for culture was not obtained emergently, which may have helped isolate the causative organism.28 A lumbar puncture for CSF analysis after brain imaging would have assisted in the diagnosis by demonstrating the characteristic CSF appearance of a bacterial infection or CVT, the latter of which has no specific CSF abnormalities.25 Given the significant overlap of clinical signs and symptoms of meningitis and CVT, further research explicitly modeled to improve the diagnostic efficiency of CVT in a suspected patient is needed to improve clinical outcomes and minimize the impact of long-term sequelae.
Conclusion
The constellation of clinical presentations present in CVT may prevent a timely diagnosis of the condition. CVT secondary to infection such as meningococcal pneumonia is an infrequent neurological complication that can create a diagnostic conundrum due to the overlapping symptoms of headaches and focal neurological deficits. Cranial nerve palsy is an underreported clinical feature in the literature and can be caused by increased intracranial pressure from the impediment of venous outflow. Neuroimaging plays an essential role for the accurate diagnosis of CVT, as prompt treatment is essential.
Consent
Written informed consent was obtained from the legal guardian of the patient to publish this report per the journal’s patient consent policy.
Acknowledgments
We want to thank Larkin Hospital Internal Medicine Research Group for creating a networkable organization for international medical students worldwide.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005;352(17):1791–1798. doi:10.1056/NEJMra042354
2. Bousser MG, Ferro JM. Cerebral venous thrombosis: an update. Lancet Neurol. 2007;6(2):162–170. doi:10.1016/S1474-4422(07)70029-7
3. Danwang C, Mazou TN, Tochie JN, Tankeu R, Bigna JJ. Global epidemiology and patterns of cerebral venous thrombosis: a systematic review and meta-analysis protocol. BMJ Open. 2018;8(4):e019939. doi:10.1136/BMJOPEN-2017-019939
4. Coutinho JM. Cerebral venous thrombosis. J Thromb Haemost. 2015;13(S1):S238–S244. doi:10.1111/JTH.12945
5. Ferro JM, Canhão P. Cerebral venous sinus thrombosis: update on diagnosis and management. Curr Cardiol Rep. 2014;16(9). doi:10.1007/S11886-014-0523-2
6. Idiculla PS, Gurala D, Palanisamy M, Vijayakumar R, Dhandapani S, Nagarajan E. Cerebral venous thrombosis: a comprehensive review. Eur Neurol. 2020;83(4):369–379. doi:10.1159/000509802
7. Ameri A, Bousser MG. Cerebral venous thrombosis. Neurol Clin. 1992;10(1):87–111. doi:10.1016/S0733-8619(18)30235-4
8. Ferro JM, Canhao P. Cerebral venous thrombosis: etiology, clinical features, and diagnosis. UptoDate; 2022. Available from: https://www.uptodate.com/contents/cerebral-venous-thrombosis-etiology-clinical-features-and-diagnosis?search=cerebral%20venous%20sinus%20thrombosis&source=search_result&selectedTitle=1~144&usage_type=default&display_rank=1.
9. Khatri IA, Wasay M. Septic cerebral venous sinus thrombosis. In: International Neurology. John Wiley & Sons, Ltd; 2016:239–242. doi:10.1002/9781118777329.CH62
10. Feldman C, Anderson R. Meningococcal pneumonia: a review. Pneumonia. 2019;11(1). doi:10.1186/S41479-019-0062-0
11. Jacob MS, Gunasekaran K, Miraclin AT, et al. Clinical profile and outcome of patients with cerebral venous thrombosis secondary to bacterial infections. Ann Indian Acad Neurol. 2020;23(4):477. doi:10.4103/AIAN.AIAN_341_20
12. Ding J, Song B, Xie X, et al. Inflammation in cerebral venous thrombosis. Front Immunol. 2022;13. doi:10.3389/FIMMU.2022.833490
13. Deliran SS, Brouwer MC, Coutinho JM, van de Beek D. Bacterial meningitis complicated by cerebral venous thrombosis. Eur Stroke J. 2020;5(4):394–401. doi:10.1177/2396987320971112
14. Kartal A. Facial palsy in cerebral venous thrombosis: an atypical case in a young girl. J Pediatr Neurosci. 2017;12(2):160–161. doi:10.4103/JPN.JPN_155_16
15. Lefkowitz D. Cortical Thrombophlebitis and Sinovenous Disease. Vol. 54. Elsevier Science Publishing Co Inc; 1989.
16. Bousser MG, Chiras J, Bories J, Castaigne P. Cerebral venous thrombosis--a review of 38 cases. Stroke. 1985;16(2):199–213. doi:10.1161/01.STR.16.2.199
17. Straub J, Magistris MR, Delavelle J, Landis T. Facial palsy in cerebral venous thrombosis. Stroke. 2000;31(7):1766–1769. doi:10.1161/01.STR.31.7.1766
18. Kuehnen J, Schwartz A, Neff W, Hennerici M. Cranial nerve syndrome in thrombosis of the transverse/sigmoid sinuses. Brain. 1998;121(Pt 2):381–388. doi:10.1093/BRAIN/121.2.381
19. Nguyen V, Reddy V, Varacallo M. Neuroanatomy, Cranial Nerve 6 (Abducens). StatPearls Publishing; 2021. https://www.ncbi.nlm.nih.gov/books/NBK430711/.
20. Özgönül C, Ceylan OM, Mutlu FM, Altınsoy Hİ, Aparcı M. Abducens palsy due to cerebral venous sinus thrombosis in a patient with heart failure. Turk J Ophthalmol. 2015;45(4):179–181. doi:10.4274/TJO.94468
21. Marzo SJ. Sigmoid sinus thrombosis with contralateral abducens palsy: first report of a case. Ear Nose Throat J. 2001;80(12):869–870. doi:10.1177/014556130108001210
22. Garcin R, Pestel M. Thrombo-Phlébites Cérébrales. Semantic Scholar. 1956;37. Available from: https://www.semanticscholar.org/paper/Thrombo-phl%C3%A9bites-c%C3%A9r%C3%A9brales.-Garcin-Pestel/b187012db8d99a8b012558730ef70d1b24cea70f. Accessed July 7, 2022.
23. Sadoghi M, Dabirmoghaddam P. Otitic hydrocephalus: case report and literature review. Am J Otolaryngol. 2007;28(3):187–190. doi:10.1016/J.AMJOTO.2006.07.007
24. Sidhom Y, Mansour M, Messelmani M, et al. Cerebral venous thrombosis: clinical features, risk factors, and long-term outcome in a Tunisian cohort. J Stroke Cerebrovasc Dis. 2014;23(6):1291–1295. doi:10.1016/J.JSTROKECEREBROVASDIS.2013.10.025
25. Saposnik G, Barinagarrementeria F, Brown RD, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American heart association/American stroke association. Stroke. 2011;42(4):605–635. doi:10.1161/STR.0B013E31820A8364
26. DiRenzo D, McMahan ZH, Desai NS, Manno R, Petri M. Cerebral venous thrombosis mimicking a discrete brain mass: a case report and literature review. Case Rep Rheumatol. 2018;2018:1–5. doi:10.1155/2018/5862912
27. Oliveira IM, Duarte JÁ, Dalaqua M, Jarry VM, Pereira FV, Reis F. Cerebral venous thrombosis: imaging patterns. Radiol Bras. 2022;55(1):54–61. doi:10.1590/0100-3984.2021.0019
28. Tunkel AR, Hasbun R, Bhimraj A, et al. 2017 infectious diseases society of America’s clinical practice guidelines for healthcare-associated ventriculitis and meningitis. Clin Infect Dis. 2017;64(6):e34. doi:10.1093/CID/CIW861
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diagnosis of Mycoplasma hominis Meningitis with Metagenomic Next-Generation Sequencing: A Case Report
Dong Y, He Y, Zhou X, Lv X, Huang J, Li Y, Qian X, Hu F, Zhu J
Infection and Drug Resistance 2022, 15:4479-4486
Published Date: 12 August 2022
The “White Cerebellum Sign”, a Striking Computed Tomography Scan Finding in a Critically Ill Infant: A Case Report
Shamavu GK, Mahmud FA, Maren MB, Arias Ortiz YE, Mseza B, Tsongo FK, Vahwere BM, Egesa WI
International Medical Case Reports Journal 2023, 16:693-697
Published Date: 13 October 2023
Diagnosis of Two Meningitis Cases Caused by Rickettsia Felis in China, with Metagenomic Next-Generation Sequencing: A Case Report
Wang J, Zhou H, Dong Z, Wang J, Wang R, Guan Y
Infection and Drug Resistance 2023, 16:7239-7245
Published Date: 14 November 2023
Otitis Media Progressing to Community-Acquired Meningitis in Diabetic Patients: A Case Report of K2-ST375 hypervirulent Klebsiella pneumoniae and Literature Review
Jin S, Xie H, Wang R
Infection and Drug Resistance 2024, 17:4707-4716
Published Date: 28 October 2024