Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Prognostic Nutritional Index (PNI) as a Predictor in Patients with Metabolic Syndrome and Heart Failure
Authors Zhang X ![]() , Zhang J, Liu F, Li W, Zhang T
, Zhang J, Liu F, Li W, Zhang T ![]() , Fang B, Zhang Z, Xie Q, Yang Y
, Fang B, Zhang Z, Xie Q, Yang Y ![]() , Li X
, Li X
Received 11 May 2023
Accepted for publication 12 July 2023
Published 18 August 2023 Volume 2023:16 Pages 2503—2514
DOI https://doi.org/10.2147/DMSO.S420924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Xuehe Zhang,1,* Jixin Zhang,1,* Fen Liu,2 Wenling Li,1 Tong Zhang,1 Binbin Fang,2 Zhiyang Zhang,1 Qian Xie,1 Yining Yang,3 Xiaomei Li1
1Department of Cardiology, First Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China; 2State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia, Clinical Medical Research Institute, the First Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China; 3Department of Cardiology, People’s Hospital of Xinjiang Uygur Autonomous Region, Urumqi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yining Yang, Department of Cardiology, People’s Hospital of Xinjiang Uygur Autonomous Region, 91 Tianchi Road, Urumqi, 830054, People’s Republic of China, Tel +86-991-4361690, Email [email protected] Xiaomei Li, Department of Cardiology, First Affiliated Hospital of Xinjiang Medical University, 137 Liyushan South Road, Urumqi, 830054, People’s Republic of China, Tel +86-991-4362611, Email [email protected]
Purpose: There is a lack of research on nutritional status and poor prognosis in patients with metabolic syndrome and heart failure. This study evaluated the relationship between nutritional status as defined by the PNI and adverse outcomes in patients with metabolic syndrome and heart failure.
Methods: A total of 1048 heart failure patients with metabolic syndrome admitted to the Heart Center of the First Affiliated Hospital of Xinjiang Medical University from January 2015 to December 2019 were consecutively. PNI was used to assess their nutritional status.
Results: A total of 51.0% of the patients were in the nonmalnutrition group (PNI≥ 45), 27.9% were in the mild malnutrition group (40≤PNI< 45), and 21.1% of patients were in the malnutrition group (PNI< 40). At 36 months of follow-up, after adjusting for other confounding factors, malnutrition (PNI< 40) was independently associated with all-cause death (HR: 1.787, 95% CI: 1.451– 2.201, P< 0.001) and cardiovascular death (HR: 1.837, 95% CI: 1.467– 2.301, P< 0.001). PNI showed additional prognostic predictive value when included in the established risk factor model, both for all-cause death (AUC: 0.620, 95% CI: 0.579– 0.661, P< 0.001) and cardiovascular death (AUC: 0.596, 95% CI: 0.555– 0.636, P< 0.001).
Conclusion: In patients with metabolic syndrome and heart failure, malnutrition assessed by PNI is an independent predictor for all-cause death and cardiovascular death, and PNI is negatively correlated with the occurrence of adverse outcomes.
Keywords: prognostic nutritional index, metabolic syndrome, heart failure, malnutrition, prognosis
Introduction
Heart failure (HF) is the fastest growing cardiovascular disease worldwide, resulting in severe disease burden. Heart failure represents the end stage of various heart diseases, among which ischemic heart disease caused by coronary artery disease is the most common cause of heart failure. Heart failure is a condition in which the heart fails to supply blood and oxygen in the amount required by the body. The decrease in cardiac output leads to the development of heart failure.1,2 The management of HF has improved dramatically over the past few decades, especially with the use of novel agents, and the prognosis of HF has improved.3 However, the risk of death and rehospitalization remains high, which represents a growing public health burden worldwide. Treatment of patients with chronic HF has also moved from a focus on improving hemodynamics to a more comprehensive assessment.4,5 In recent years, nutritional status has attracted attention as a modifiable risk factor for patients with heart failure.6–8 Malnutrition is usually caused by inadequate or unbalanced nutrient intake, resulting in insufficient caloric intake, protein intake, or intake of other nutrients required for tissue maintenance and repair. Malnutrition is prevalent in patients with heart failure and is independently associated with adverse outcomes.9 In addition, malnutrition may reflect a state of abnormal drug metabolism, which may lead to poor therapeutic effects.10,11 A state of systemic and/or pulmonary congestion characterized by poor nutritional status and significant weight loss. This condition itself creates an environment that is prone to aggravate cardiac energy metabolism, worsening existing heart failure.12 Studies have shown that nutritional status is an independent prognostic factor in patients with acute or chronic HF. Baseline nutritional status itself has a strong prognostic effect. Early nutritional intervention can improve the outcome of patients with chronic heart failure. Therefore, heart failure guidelines recommend the assessment of nutritional status in patients.13,14 It is important to assess malnutrition in patients with heart failure, monitor this aspect of patients, and identify accurate assessment tools to aid in risk stratification and treatment strategies.
Several multidimensional nutritional screening tools, including the Nutrition Risk Screening 2002 (NRS 2002) and the Mini Nutritional Assessment (MNA), have been developed to assess nutritional risk in patients with HF.15,16 However, these tools include multiple clinical measures and dietary factors extracted from questionnaires, are time-consuming to perform, have limited applicability in routine use, and may be confounded by patient-derived recall bias. In contrast, the prognostic nutritional index (PNI) has been proposed as a simple and convenient indicator. It can be easily calculated from serum albumin levels and lymphocyte counts, which are available in most clinical laboratories. The PNI is used to assess nutritional status in a variety of clinical situations, including cancer and postoperative pneumonia. Recent studies suggest that in acute and chronic HF patients, lower PNI is associated with an increased risk of death or major adverse cardiac events.17–21
Metabolic syndrome is a complex disease, and its diagnosis involves the evaluation of multiple risk factors, including central obesity, elevated triglycerides, reduced high-density lipoprotein cholesterol, hypertension, and hyperglycemia. When these factors are present together, they increase the risk of atherosclerotic cardiovascular disease.22–24 Obesity as an important component of the metabolic syndrome implies that overnutrition contributes to the syndrome. Interestingly, recent studies have shown that obese individuals who are malnourished have a higher burden of complications, inappropriate cardiac remodeling and worse cardiac outcomes.25 Malnutrition may represent a metabolically abnormal state, and nutritional assessment may be more important for heart failure patients with metabolic syndrome. To our knowledge, no study has evaluated the relationship between nutritional status and cardiovascular risk in patients with metabolic syndrome.
Methods
Study Population
In this study, patients with metabolic syndrome and heart failure admitted to the Heart Center of the First Affiliated Hospital of Xinjiang Medical University from January 2015 to December 2019 were continuously enrolled. Metabolic syndrome was defined as any three or more of the following: waist circumference >102 cm in men, >88 cm in women; blood pressure >130/85 mmHg or on medication; fasting plasma glucose (FPG) ≥110 mg/dL or on medication; triglyceride (TG) ≥150 mg/dL; HDL-C < 40 mg/dL for men and < 50 mg/dL for women.26 Patients with autoimmune diseases, chronic inflammatory diseases, acute infectious diseases, severe hepatic and renal insufficiency, malignancies, hematological diseases, or incomplete clinical data or who were lost to follow-up were excluded from the current study. The study was conducted in accordance with the principles of the Declaration of Helsinki. The study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (20141201-03-1701A). All patients provided informed consent.
Data Collection
Electronic medical records are reviewed by researchers who are unaware of the purpose of the study for clinical data collection. Trained reviewers perform data verification. The patient’s age, sex, height, weight, systolic and diastolic blood pressure at admission, and history of smoking, drinking, and disease were recorded. Blood samples were collected 24 h after admission. The results of complete blood cell count, blood lipid, serum creatinine, FPG, serum albumin (ALB) and brain natriuretic peptide (BNP) were recorded. All transthoracic echocardiograms were performed within 24 hours after admission. PNI was calculated according to the ALB and lymphocyte (LYM) count: PNI= ALB (g/L)+ 5×LYM (109/L).27 According to the PNI, the patients were divided into three groups: malnutrition (PNI<40), mild malnutrition (40≤PNI<45), and nonmalnutrition (PNI≥45). Body mass index (BMI) was calculated as weight divided by the square of height (kg/m2).28 The estimated glomerular filtration rate (eGFR) was calculated as [(140-age) ×weight(kg)] ×0.85(if female)/ [72×serum creatinine(mg/dl)].29
Endpoints and Follow-Up
The primary endpoint was all-cause death, and the secondary endpoint was cardiovascular death. Cardiovascular death was defined as death from acute myocardial infarction, heart failure, arrhythmia, cardiac surgery, or other cardiovascular causes. Clinical follow-up included questionnaires and telephone contacts sent to patients or their families, treatment information of the patient in this institution, and death data obtained from other hospitals to which patients were admitted.
Statistical Analysis
Continuous variables were expressed as the means with standard deviations or as medians (interquartile ranges), depending on whether they were normally distributed. Categorical variables are expressed as cases (n) and percentages (%). Continuous variables were compared between groups using one-way analysis of variance or the Kruskal‒Wallis test. Categorical variables were compared between groups using the chi-square test. Multivariate linear regression was used to analyze the influencing factors of PNI. Unadjusted cumulative event rates were estimated with Kaplan-Meier curves and compared between groups with the Log rank test. Cox proportional hazards regression analysis was used to identify predictors of cardiovascular events. Model 1 was adjusted for age and sex. Model 2 included the same variables as Model 1, in addition to smoking, drinking, previous stroke, previous myocardial infarction (MI). Model 3 was further adjusted for New York Heart Association (NYHA) class, low-density lipoprotein cholesterol (LDL-C), eGFR, left ventricular ejection fraction (LVEF), and BNP on the basis of Model 2. The association of PNI with adverse end-point events was analyzed using restricted cubic splines. Sensitivity, specificity and area under the curve (AUC) were used to compare the predictive efficacy of LYM, ALB and PNI for adverse outcomes. To assess whether adding PNI to the established risk factors had incremental predictive value for adverse outcomes, AUC, net reclassification improvement (NRI), and integrated discrimination improvement (IDI) were compared between models. All analyses were performed using SPSS version 20.0 (IBM Corp, Armonk, NY, USA) and R version 4.2.2 software (Vienna, Austria). A P value of <0.05 indicated statistical significance.
Results
Baseline Characteristics of Patients
A total of 5087 patients with heart failure were enrolled in this study, and 1170 patients with heart failure and metabolic syndrome were finally included.1048 patients in the study completed 36 months of follow-up, with a loss of follow-up rate of 10.4%. A total of 768 males (73.3%) and 280 females (26.7%) were included in the study (Figure 1). Patients were divided into three groups: nonmalnutrition (PNI≥45), mild malnutrition (40≤PNI<45) and malnutrition (PNI<40). The baseline characteristics are shown in Table 1. There were 221 (21.1%) patients in the malnutrition group (PNI<40), 292 (27.9%) patients in the mild malnutrition group (40≤PNI<45), and 535 (51.0%) patients in the nonmalnutrition group (PNI≥45). There were statistically significant differences in age, sex, BMI, waist circumference, NYHA calss, neutrophil count (NEUT), lymphocyte count (LYM), FPG, TG, total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), eGFR, ALB and BNP among the three groups. There were no statistically significant differences in other variables among the three groups.
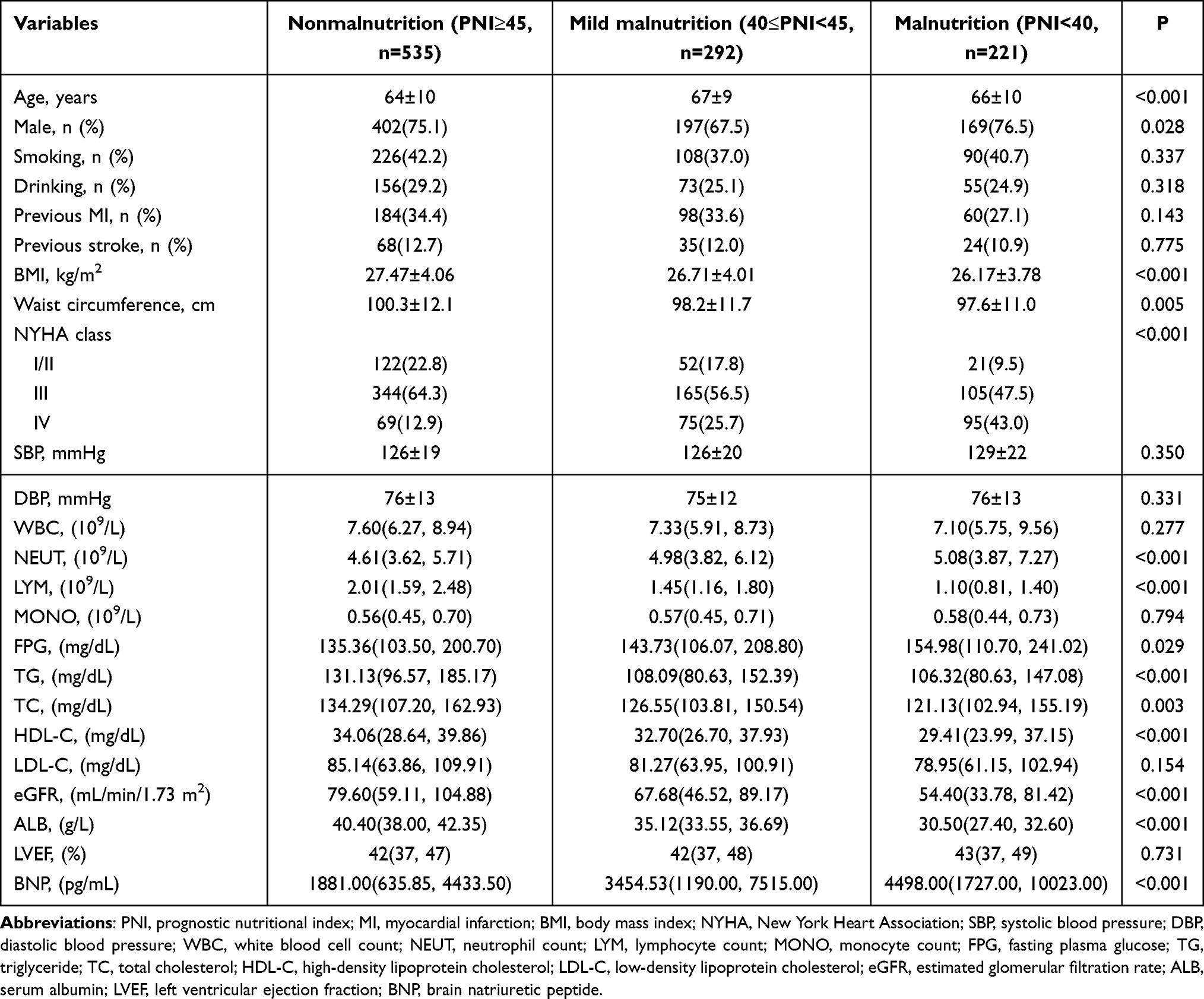 |
Table 1 Baseline Characteristics of Patients According to PNI |
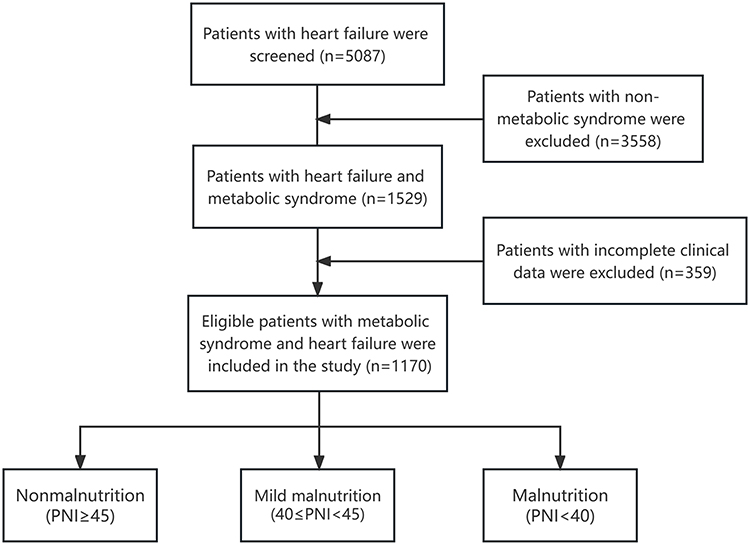 |
Figure 1 Flow chart of study participant screening. |
PNI and Adverse Outcome in Patients with MS and HF
The associations between PNI and cardiovascular risk factors were analyzed using linear regression analysis. Multivariate linear regression analysis showed that the PNI level was related to NYHA class, TG, HDL-C and eGFR (P<0.05) (Table 2). During a follow-up period of 36 months, 641 (61.2%) all-cause deaths were recorded, including 543 (51.8%) cardiovascular deaths. The Kaplan-Meier curve showed that the survival probability of patients in the malnutrition group was significantly lower than that in the mild and nonmalnutrition groups (Log rank test, both P<0.05) (Figure 2). Cox proportional hazards analysis of all-cause death and cardiovascular death showed that in the unadjusted Cox model, the proportion of all-cause death (HR:1.728, 95% CI:1.427–2.093, P<0.001) and cardiovascular death (HR:1.753, 95% CI:1.426–2.155, P<0.001) increased with decreasing PNI level. After adjusting for age and sex, Model 1 reached a similar conclusion. On the basis of Model 1, Model 2 further adjusted for smoking, drinking, previous stroke and previous MI. Model 3 further adjusted for NYHA class, LDL-C, eGFR, LVEF and BNP. Multivariate Cox regression analysis showed that malnutrition (PNI<40) was independently associated with all-cause death (HR:1.787, 95% CI:1.451–2.201, P<0.001) and cardiovascular death (HR:1.837, 95% CI:1.467–2.301, P<0.001) (Table 3). Restricted cubic splines were used to further analyze the relationship between PNI and HR of all-cause death and cardiovascular death. The adjustment of variables was consistent with model 3 in cox regression analysis. In heart failure patients with metabolic syndrome, the risk of all-cause death and cardiovascular death decreased with increasing PNI (Figure 3).
 |
Table 2 Univariate and Multivariate Linear Regression Analysis for PNI |
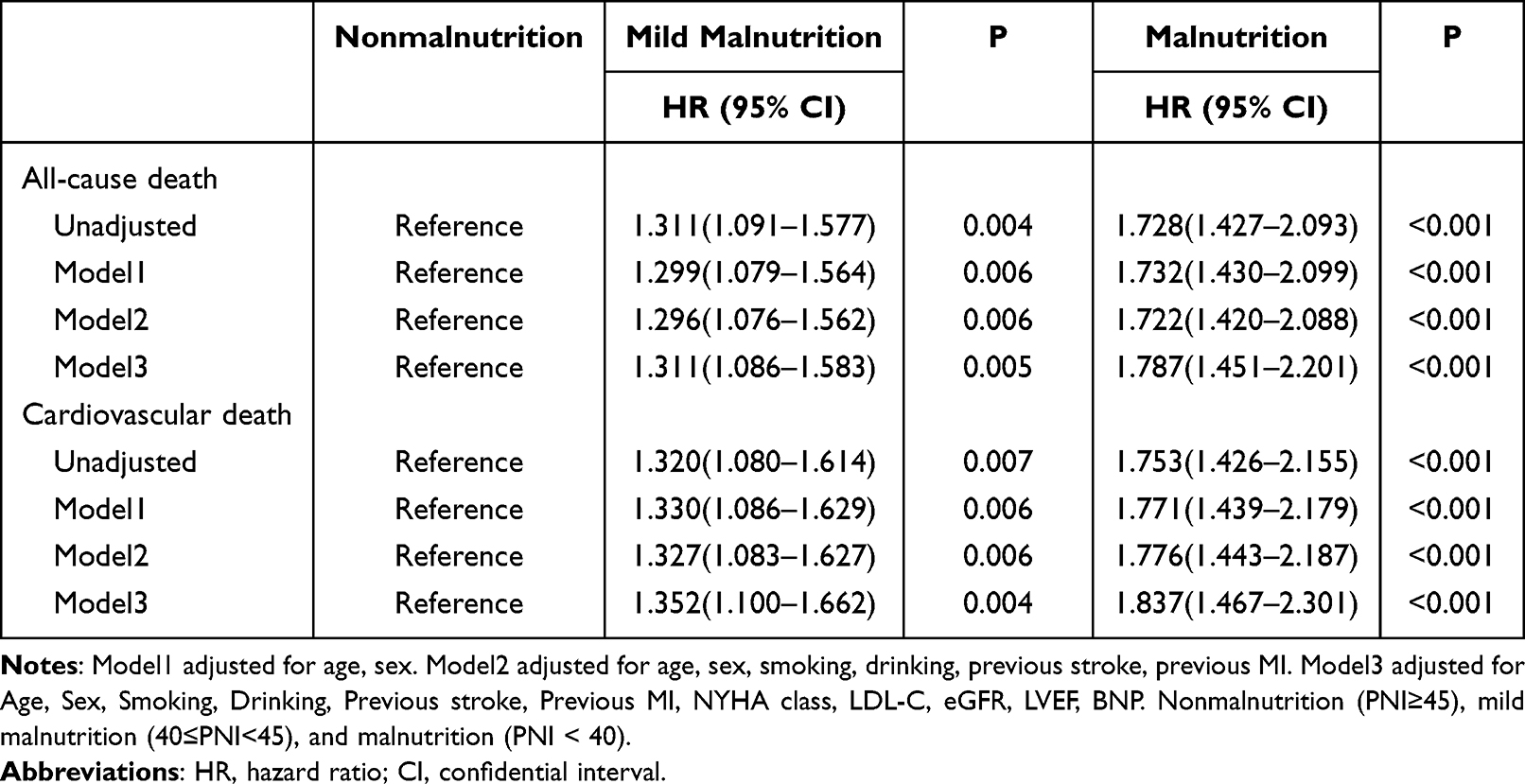 |
Table 3 Unadjusted and Adjusted Cox Regression Analyses for Adverse Outcomes |
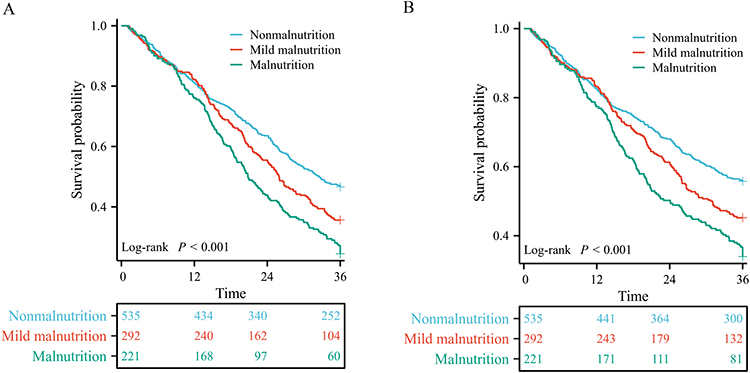 |
Figure 2 Kaplan‒Meier analyses of adverse outcomes categorized by PNI. (A) All-cause death. (B) Cardiovascular death. |
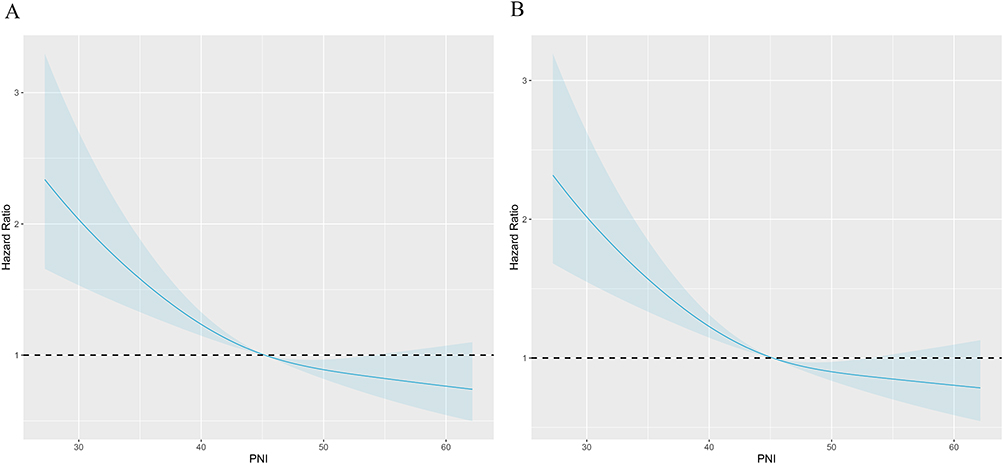 |
Figure 3 Restricted cubic splines visualize the association between PNI and adverse outcomes in patients with metabolic syndrome and heart failure. (A) All-cause death. (B) Cardiovascular death. |
In predicting all-cause death, PNI had the same AUC as ALB but with a slight increase in sensitivity and specificity. In predicting cardiovascular death, LYM had a low AUC, sensitivity, and specificity, whereas PNI had a higher AUC and sensitivity than ALB (Table 4). On the basis of the established risk factor model, LYM, ALB, and PNI were added. The addition of ALB and PNI significantly improved the predictive value of all-cause death and cardiovascular death. Compared with ALB, the addition of PNI improved the prognostic predictive value of all-cause death (AUC=0.620, 95% CI:0.579–0.661) and cardiovascular death (AUC=0.596, 95% CI:0.555–0.636), but the optimization effect was not significant (Table 5). A subgroup analysis showed that after adjusting for age, sex, smoking, drinking, previous stroke, previous MI, NYHA class, LDL-C, eGFR, LVEF, and BNP, PNI can still independently predict all-cause death in patients with heart failure complicated by MS, and it is not impacted by age, sex or LVEF (Table 6).
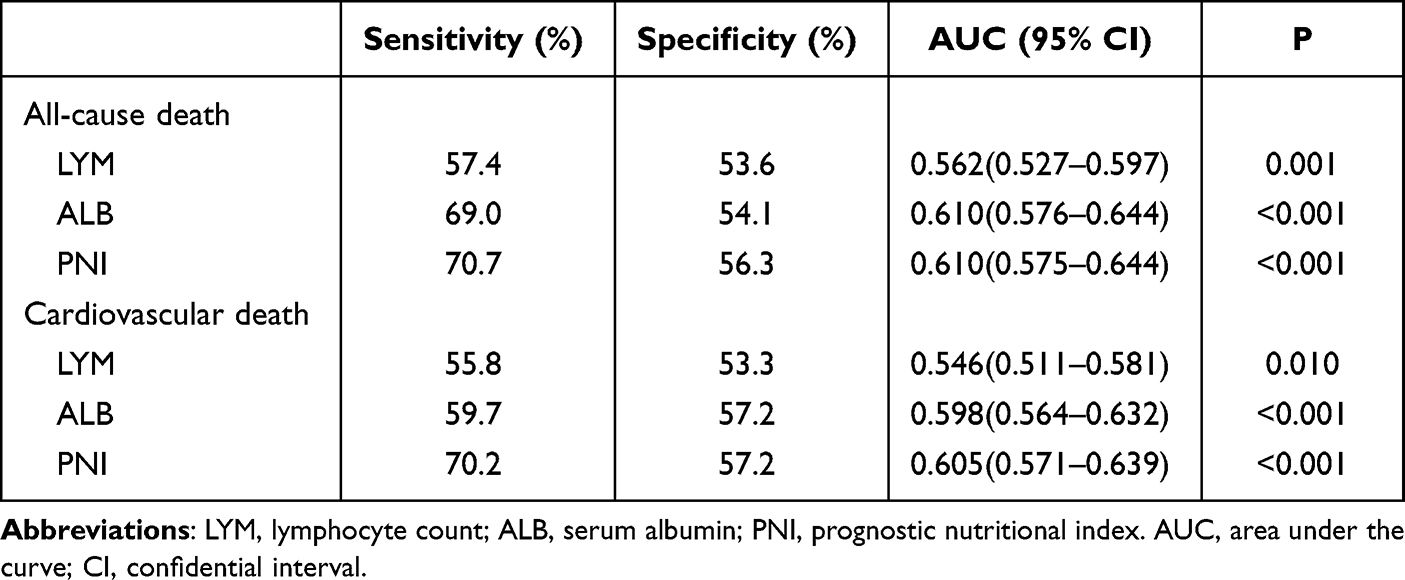 |
Table 4 Prognostic Predictive Value of Different Indicators |
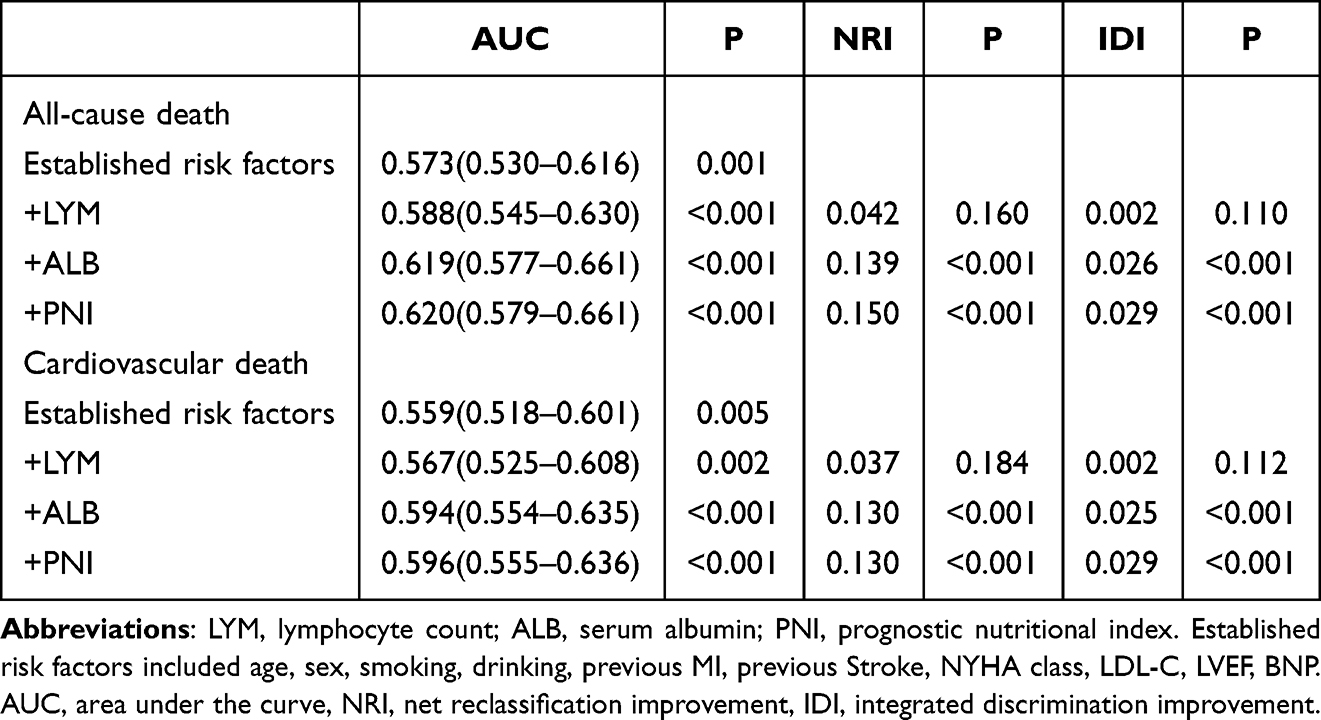 |
Table 5 Prognostic Predictive Value of Different Models |
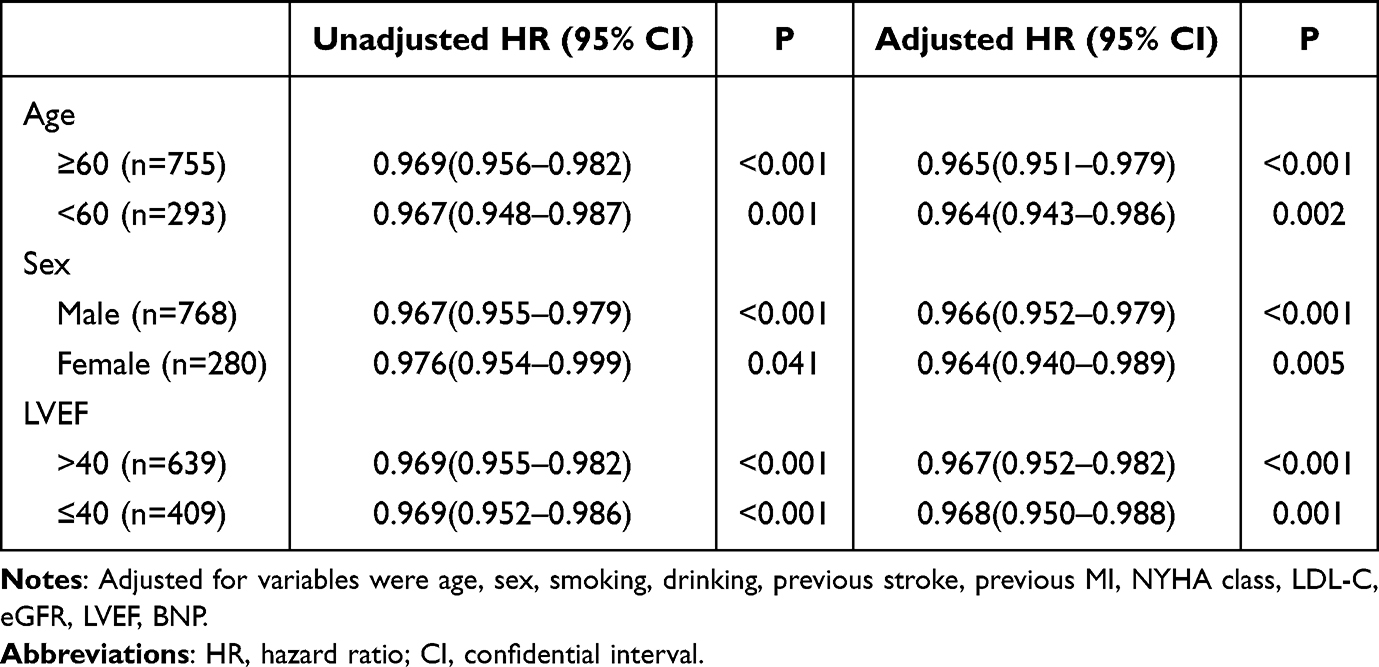 |
Table 6 Prognostic Value of PNI for All-Cause Death in Various Subgroups |
Discussion
Previous studies have shown that PNI is associated with the occurrence of poor prognosis in patients with heart failure. However, the role of malnutrition in patients with heart failure and metabolic syndrome remains unknown. In our study, for heart failure patients with metabolic syndrome, 21.1% of patients were malnourished according to the PNI nutrition score, and the results showed that PNI was inversely associated with increased all-cause and cardiovascular death. The risks of all-cause death and cardiovascular death in patients with malnutrition based on PNI were significantly higher than those with no nutritional risk and mild nutritional risk, even after adjusting for other risk factors. To the best of our knowledge, this study is the first to demonstrate that PNI is an independent predictor of poor outcome in patients with metabolic syndrome and HF. Most importantly, this study suggests that nutritional assessment based on laboratory markers can be used to risk stratify adverse outcomes in patients with metabolic syndrome and HF.
Malnutrition is a common complication in patients with HF and is associated with high mortality and readmission outcomes. Malnutrition can further aggravate heart failure, forming a vicious cycle. Malnutrition is the result of decreased appetite and cardiac cachexia.30 Patients with heart failure have reduced albumin production due to hepatic congestion and reduced nutrient absorption due to intestinal edema.31,32 Inadequate energy intake in patients with heart failure may lead to decreased skeletal muscle strength and to an inability to perform daily physical activities and exercise due to reduced cardiac output.33 In addition, HF patients have an increased cardiac resting metabolic rate and nutritional requirements, leading to an imbalance between energy intake and expenditure.34 Increased resting metabolic rate and gastrointestinal malabsorption are prevalent in patients with advanced disease. The pathophysiology may involve reduced intestinal perfusion and disturbance of intestinal microcirculation, leading to local edema, abnormal mucosal permeability of endotoxin, and subsequent inflammation.35 Malnutrition can also affect immune function. The lower immune system function in HF patients may be reflected by increased complications and infections, which may also explain the comorbidity and high mortality in HF patients. Frequent infections combined with decreased cardiac output increase the risk of heart failure exacerbation and reduce the survival rate of patients.36
As a chronic state, multiple forms of malnutrition may occur and may overlap in different ways, and the co occurrence of undernutrition with overweight and obesity can create a double burden of malnutrition. The most likely pathogenesis of metabolic syndrome is overnutrition, leading to the accumulation of excessive lipids in organs or tissues. This in turn disrupts metabolic processes.37 Metabolic syndrome (MS) is a collection of metabolic risk factors, including atherogenic dyslipidemia (elevated serum triglycerides and low high-density lipoprotein cholesterol), elevated blood pressure, dysglycemia (insulin resistance and elevated blood glucose), a proinflammatory state, and a prothrombotic state.38 These factors directly increase the risk of coronary heart disease, other forms of cardiovascular atherosclerotic disease, and type 2 diabetes mellitus. In recent years, chronic inflammation and other abnormalities, such as prothrombotic states, nonalcoholic fatty liver disease, and sleep apnea, have been incorporated into the syndrome, complicating its definition.39 Studies have shown an increased risk of cardiovascular disease in patients with MS regardless of the diagnostic criteria used.40–42
As a predictor of the prognosis of heart failure,43 it is necessary to evaluate nutritional status during the treatment of heart failure. Studies have shown that improving the nutritional status of patients with heart failure can also improve the prognosis, prevent the deterioration of the disease, and reduce the mortality of patients.44 At the same time, major guidelines have begun to consider the nutritional needs of obese patients and put forward specific nutritional support recommendations.45 For patients with heart failure and metabolic syndrome, the assessment of nutritional status may be more complicated. Traditionally, malnutrition can be assessed by body mass index, triceps skinfold thickness, and different biochemical indicators,46,47 however, these parameters are not always accurate and some are rather subjective. Using these anthropometric measures alone to assess malnutrition in patients with fluid retention and wasting HF may be misleading.48 This has prompted the development of more comprehensive, objective, and convenient nutritional status assessment tools such as the Controlling Nutritional Status (CONUT) score, Geriatric Nutritional Risk Index (GNRI) score, and Prognostic nutritional index (PNI) score. However, the CONUT score is calculated based on serum albumin, lymphocyte count, and cholesterol, which may be confounded by the widespread use of statins in patients with HF. The calculation of the GNRI requires a measure of body weight and may be confounded by the dramatic changes in volume overload resulting from HF treatment during hospitalization. Using the CONUT and GNRI to evaluate the nutritional status of patients with metabolic syndrome may cause a certain deviation. Therefore, PNI may be a more appropriate indicator that can be easily calculated from routine laboratory parameters, providing a practical tool for the assessment of nutritional risk in HF patients with metabolic syndrome.
The prognostic nutritional index was first proposed by Buzby et al in 1980. It is mainly calculated by measuring serum albumin and peripheral blood lymphocytes, which can comprehensively reflect the nutritional status and immune status of patients.49,50 A number of studies have evaluated the relationship between PNI and long-term outcomes in hospitalized patients with HF. Yoshihisa et al demonstrated that a low PNI was independently associated with poor outcomes in patients with severe decompensated acute heart failure. Cheng et al51 showed that PNI at admission was independently associated with long-term survival in patients hospitalized for acute heart failure. Kawata et al17 showed that changes in PNI on admission and at discharge during hospitalization were associated with 1-year mortality in patients with acute heart failure. These findings further support the use of PNI to guide risk stratification in HF. In this study, PNI was used as an independent predictor for all-cause death and cardiovascular death in patients with metabolic syndrome and heart failure, and PNI values were inversely correlated with the risk of mortality. In the subgroup analysis we found that the independent predictive effect of PNI was not affected by age, sex, or LVEF. Serum albumin, the most abundant protein in plasma, is synthesized in the liver, secreted into the vascular space and distributed throughout the body. It is traditionally used to assess nutritional status and visceral protein synthesis function.52,53 Hypoalbuminemia is a predictor of short-term prognosis in patients with acute heart failure.54,55 The decrease in serum albumin levels may be influenced by a state of malnutrition or indications of renal and hepatic dysfunction. Low albumin levels are associated with decreased immunity, and frequent infections combined with reduced cardiac output increase the risk of worsening heart failure and reduce survival at any level of cardiac function. However, albumin levels can be affected by hemodilution, kidney loss, and a shortened half-life due to severe disease. Meanwhile, other pathophysiological processes in addition to malnutrition can also lead to hypoalbuminemia in such patients. The single parameter of serum albumin may not be accurate in assessing nutritional status. Lymphocyte count may be another factor of nutritional status in HF patients. Lymphocytes can be used to assess immunonutritional status. A low lymphocyte count indicates a poor immune status. Weight loss associated with the development of cardiogenic cachexia is often associated with decreased physical function and worse prognosis. Decreased lymphocyte counts, caused by physical stress, malnutrition, and chronic inflammation, predict 1-year outcomes in patients with advanced HF.56,57 The activation of the neurosecretory and inflammatory systems leads to a decrease in lymphocyte counts. Elevated serum cortisol levels can also lead to a decrease in lymphocyte counts.58 Activation of the neurosecretory and inflammatory systems also leads to a decrease in lymphocyte counts. Advanced malnutrition can lead to the loss of some important nutrients and the suppression of cellular or humoral immune function. The number and function of B cells and T cells are significantly reduced, which may lead to a decrease in lymphocyte count. In fact, based on the established risk factor model, ALB and PNI can improve the prediction effect of the model. Compared with ALB, PNI has better sensitivity and AUC for predicting adverse outcomes. Although the increase is slight, given that PNI assesses both ALB and LYM, it could theoretically represent both malnutrition and chronic inflammation in HF. It has the potential to compensate for the lack of a single variable.
Study Limitations
This study has several limitations. First, as a cohort study targeting a single center, and no matter how the analysis is adjusted, unknown confounding factors may affect the results. Second, this study only assessed PNI at baseline and did not assess changes in PNI during follow-up. In addition, our results did not include other relevant end-point events. Therefore, due to these limitations, our results need to be validated in a larger, prospective, multicenter study. However, exploring nutritional indicators that affect the prognosis of patients with metabolic syndrome combined with heart failure is still valuable for screening those at risk for heart failure.
Conclusions
This study demonstrates that malnutrition as assessed by PNI is associated with all-cause mortality as well as cardiovascular mortality in patients with metabolic syndrome and heart failure. There was a significant negative correlation between the PNI and adverse outcomes of patients. These results support PNI as an indicator of nutritional status as well as prognosis in patients with metabolic syndrome and heart failure.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This study followed the Declaration of Helsinki. Approved by the Medical Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (20141201-03-1701A).
Acknowledgments
We thank all the investigators and subjects who participated in this project. Xuehe Zhang and Jixin Zhang are co-first authors for this study.
Funding
This work was supported by the Xinjiang Uygur Autonomous Region University Scientific Research Program (No. XJEDU2020I013), the National Natural Science Foundation of China (No. 81960073), the Xinjiang Uygur Autonomous Region Postgraduate Scientific Research Innovation Project (No. XJ2022G158), and the State Key Lab of Pathogenesis, Prevention, and Treatment of High Incidence Diseases in Central Asia Fund (No. SKL-HIDCA-2020-2).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nat Rev Cardiol. 2016;13(6):368–378. doi:10.1038/nrcardio.2016.25
2. Tanai E, Frantz S. Pathophysiology of heart failure. Compr Physiol. 2015;6(1):187–214. doi:10.1002/cphy.c140055
3. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J Am Coll Cardiol. 2022;79(17):1757–1780. doi:10.1016/j.jacc.2021.12.011
4. Mai L, Wen W, Qiu M, et al. Association between prediabetes and adverse outcomes in heart failure. Diabetes Obes Metab. 2021;23(11):2476–2483. doi:10.1111/dom.14490
5. Li W, Huang A, Zhu H, et al. Gut microbiota-derived trimethylamine N-oxide is associated with poor prognosis in patients with heart failure. Med J Aust. 2020;213(8):374–379. doi:10.5694/mja2.50781
6. Anker SD, Negassa A, Coats AJ, et al. Prognostic importance of weight loss in chronic heart failure and the effect of treatment with angiotensin-converting-enzyme inhibitors: an observational study. Lancet. 2003;361(9363):1077–1083. doi:10.1016/S0140-6736(03)12892-9
7. Nochioka K, Sakata Y, Takahashi J, et al. Prognostic impact of nutritional status in asymptomatic patients with cardiac diseases: a report from the CHART-2 Study. Circ J. 2013;77(9):2318–2326. doi:10.1253/circj.CJ-13-0127
8. Castillo-Martínez L, Colín-Ramírez E, Orea-Tejeda A, et al. Cachexia assessed by bioimpedance vector analysis as a prognostic indicator in chronic stable heart failure patients. Nutrition. 2012;28(9):886–891. doi:10.1016/j.nut.2011.11.024
9. Sze S, Pellicori P, Zhang J, Clark AL. Malnutrition, congestion and mortality in ambulatory patients with heart failure. Heart. 2019;105(4):297–306. doi:10.1136/heartjnl-2018-313312
10. Krishnaswamy K. Drug metabolism and pharmacokinetics in malnourished children. Clin Pharmacokinet. 1989;17(Suppl 1):68–88. doi:10.2165/00003088-198900171-00006
11. Niederberger E, Parnham MJ. The Impact of Diet and Exercise on Drug Responses. Int J Mol Sci. 2021;22(14):7692. doi:10.3390/ijms22147692
12. Chan HY, Yu DS, Leung DY, Chan AW, Hui E. Quality of life and palliative care needs of elderly patients with advanced heart failure. J Geriatr Cardiol. 2016;13(5):420–424. doi:10.11909/j.issn.1671-5411.2016.05.016
13. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
14. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239. doi:10.1016/j.jacc.2013.05.019
15. Joaquín C, Alonso N, Lupón J, et al. Mini Nutritional Assessment Short Form is a morbi-mortality predictor in outpatients with heart failure and mid-range left ventricular ejection fraction. Clin Nutr. 2020;39(11):3395–3401. doi:10.1016/j.clnu.2020.02.031
16. Tevik K, Thürmer H, Husby MI, de Soysa AK, Helvik AS. Nutritional risk screening in hospitalized patients with heart failure. Clin Nutr. 2015;34(2):257–264. doi:10.1016/j.clnu.2014.03.014
17. Kawata T, Ikeda A, Masuda H, Komatsu S. Changes in prognostic nutritional index during hospitalization and outcomes in patients with acute heart failure. Heart Vessels. 2022;37(1):61–68. doi:10.1007/s00380-021-01888-x
18. Ju C, Zhou J, Lee S, et al. Derivation of an electronic frailty index for predicting short-term mortality in heart failure: a machine learning approach. ESC Heart Fail. 2021;8(4):2837–2845. doi:10.1002/ehf2.13358
19. Çinier G, Hayıroğlu Mİ, Pay L, et al. Prognostic nutritional index as the predictor of long-term mortality among HFrEF patients with ICD. Pacing Clin Electrophysiol. 2021;44(3):490–496. doi:10.1111/pace.14170
20. Sze S, Pellicori P, Zhang J, Weston J, Clark AL. The impact of malnutrition on short-term morbidity and mortality in ambulatory patients with heart failure. Am J Clin Nutr. 2021;113(3):695–705. doi:10.1093/ajcn/nqaa311
21. Candeloro M, Di Nisio M, Balducci M, et al. Prognostic nutritional index in elderly patients hospitalized for acute heart failure. ESC Heart Fail. 2020;7(5):2479–2484. doi:10.1002/ehf2.12812
22. Hu G, Qiao Q, Tuomilehto J, Balkau B, Borch-Johnsen K, Pyorala K. Prevalence of the metabolic syndrome and its relation to all-cause and cardiovascular mortality in nondiabetic European men and women. Arch Intern Med. 2004;164(10):1066–1076. doi:10.1001/archinte.164.10.1066
23. Gami AS, Witt BJ, Howard DE, et al. Metabolic syndrome and risk of incident cardiovascular events and death: a systematic review and meta-analysis of longitudinal studies. J Am Coll Cardiol. 2007;49(4):403–414. doi:10.1016/j.jacc.2006.09.032
24. Mottillo S, Filion KB, Genest J, et al. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol. 2010;56(14):1113–1132. doi:10.1016/j.jacc.2010.05.034
25. Chien SC, Chandramouli C, Lo CI, et al. Associations of obesity and malnutrition with cardiac remodeling and cardiovascular outcomes in Asian adults: a cohort study. PLoS Med. 2021;18(6):e1003661. doi:10.1371/journal.pmed.1003661
26. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
27. Buzby GP, Mullen JL, Matthews DC, Hobbs CL, Rosato EF. Prognostic nutritional index in gastrointestinal surgery. Am J Surg. 1980;139(1):160–167. doi:10.1016/0002-9610(80)90246-9
28. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i–xii, 1–253.
29. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
30. Jacobsson A, Pihl-Lindgren E, Fridlund B. Malnutrition in patients suffering from chronic heart failure; the nurse’s care. Eur J Heart Fail. 2001;3(4):449–456. doi:10.1016/S1388-9842(01)00139-8
31. Kalantar-Zadeh K, Anker SD, Horwich TB, Fonarow GC. Nutritional and anti-inflammatory interventions in chronic heart failure. Am J Cardiol. 2008;101(11A):89E–103E. doi:10.1016/j.amjcard.2008.03.007
32. Valentová M, von Haehling S, Doehner W, Murín J, Anker SD, Sandek A. Liver dysfunction and its nutritional implications in heart failure. Nutrition. 2013;29(2):370–378. doi:10.1016/j.nut.2012.06.002
33. Chung CJ, Schulze PC. Exercise as a nonpharmacologic intervention in patients with heart failure. Phys Sportsmed. 2011;39(4):37–43. doi:10.3810/psm.2011.11.1937
34. Poehlman ET, Scheffers J, Gottlieb SS, Fisher ML, Vaitekevicius P. Increased resting metabolic rate in patients with congestive heart failure. Ann Intern Med. 1994;121(11):860–862. doi:10.7326/0003-4819-121-11-199412010-00006
35. Sandek A, Swidsinski A, Schroedl W, et al. Intestinal blood flow in patients with chronic heart failure: a link with bacterial growth, gastrointestinal symptoms, and cachexia. J Am Coll Cardiol. 2014;64(11):1092–1102. doi:10.1016/j.jacc.2014.06.1179
36. Bourke CD, Berkley JA, Prendergast AJ. Immune dysfunction as a cause and consequence of malnutrition. Trends Immunol. 2016;37(6):386–398. doi:10.1016/j.it.2016.04.003
37. Grundy SM. Adipose tissue and metabolic syndrome: too much, too little or neither. Eur J Clin Invest. 2015;45(11):1209–1217. doi:10.1111/eci.12519
38. Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9(1):48. doi:10.1186/1741-7015-9-48
39. Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech. 2009;2(5–6):231–237. doi:10.1242/dmm.001180
40. Ford ES. The metabolic syndrome and mortality from cardiovascular disease and all-causes: findings from the National Health and Nutrition Examination Survey II Mortality Study. Atherosclerosis. 2004;173(2):309–314. doi:10.1016/j.atherosclerosis.2003.12.022
41. Huang Y, Chen Z, Wang X et al, et al. Comparison of the Three Most Commonly Used Metabolic Syndrome Definitions in the Chinese Population: A Prospective Study. Metabolites. 2022;13(1):. doi:10.3390/metabo13010012
42. Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes Care. 2005;28(7):1769–1778. doi:10.2337/diacare.28.7.1769
43. La Rovere MT, Maestri R, Olmetti F, et al. Additional predictive value of nutritional status in the prognostic assessment of heart failure patients. Nutr Metab Cardiovasc Dis. 2017;27(3):274–280. doi:10.1016/j.numecd.2016.09.009
44. Reber E, Gomes F, Vasiloglou MF, Schuetz P, Stanga Z. Nutritional risk screening and assessment. J Clin Med. 2019;8(7):1065. doi:10.3390/jcm8071065
45. Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019;38(1):48–79. doi:10.1016/j.clnu.2018.08.037
46. Bhattacharya A, Pal B, Mukherjee S, Roy SK. Assessment of nutritional status using anthropometric variables by multivariate analysis. BMC Public Health. 2019;19(1):1045. doi:10.1186/s12889-019-7372-2
47. Bharadwaj S, Ginoya S, Tandon P, et al. Malnutrition: laboratory markers vs nutritional assessment. Gastroenterol Rep. 2016;4(4):272–280.
48. Nicol SM, Carroll DL, Homeyer CM, Zamagni CM. The identification of malnutrition in heart failure patients. Eur J Cardiovasc Nurs. 2002;1(2):139–147. doi:10.1016/S1474-51510200005-1
49. Kwag SJ, Kim JG, Kang WK, Lee JK, Oh ST. The nutritional risk is a independent factor for postoperative morbidity in surgery for colorectal cancer. Ann Surg Treat Res. 2014;86(4):206–211. doi:10.4174/astr.2014.86.4.206
50. Schwegler I, von Holzen A, Gutzwiller J-P, Schlumpf R, Mühlebach S, Stanga Z. Nutritional risk is a clinical predictor of postoperative mortality and morbidity in surgery for colorectal cancer. Br J Surg. 2010;97(1):92–97. doi:10.1002/bjs.6805
51. Cheng YL, Sung SH, Cheng HM, et al. Prognostic nutritional index and the risk of mortality in patients with acute heart failure. J Am Heart Assoc. 2017;6(6). doi:10.1161/JAHA.116.004876
52. Yin M, Si L, Qin W, et al. Predictive value of serum albumin level for the prognosis of severe sepsis without exogenous human albumin administration: a prospective cohort study. J Intensive Care Med. 2018;33(12):687–694. doi:10.1177/0885066616685300
53. Huang W, Li C, Wang Z, et al. Decreased serum albumin level indicates poor prognosis of COVID-19 patients: hepatic injury analysis from 2623 hospitalized cases. Sci China Life Sci. 2020;63(11):1678–1687. doi:10.1007/s11427-020-1733-4
54. Bonilla-Palomas JL, Gámez-López AL, Moreno-Conde M, et al. Hypoalbuminemia in acute heart failure patients: causes and its impact on hospital and long-term mortality. J Card Fail. 2014;20(5):350–358. doi:10.1016/j.cardfail.2014.01.016
55. Arques S, Roux E, Sbragia P, Gelisse R, Pieri B, Ambrosi P. Usefulness of serum albumin concentration for in-hospital risk stratification in frail, elderly patients with acute heart failure. Insights from a prospective, monocenter study. Int J Cardiol. 2008;125(2):265–267. doi:10.1016/j.ijcard.2007.07.094
56. Bosma-Den Boer MM, Van Wetten ML, Pruimboom L. Chronic inflammatory diseases are stimulated by current lifestyle: how diet, stress levels and medication prevent our body from recovering. Nutrit Metabol. 2012;9:9. doi:10.1186/1743-7075-9-9
57. Tatsi C, Boden R, Sinaii N, et al. Decreased lymphocytes and increased risk for infection are common in endogenous pediatric Cushing syndrome. Pediatr Res. 2018;83(2):431–437. doi:10.1038/pr.2017.278
58. Acanfora D, Gheorghiade M, Trojano L, et al. Relative lymphocyte count: a prognostic indicator of mortality in elderly patients with congestive heart failure. Am Heart J. 2001;142(1):167–173. doi:10.1067/mhj.2001.115792
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Simplified Thrombo-Inflammatory Score as a Novel Predictor of All-Cause Mortality in Patients with Heart Failure: A Retrospective Cohort Study

Cheng MD, Zheng YY, Zhang XY, Ruzeguli T, Sureya Y, Didaer Y, Ailiman M, Zhang JY
Journal of Inflammation Research 2024, 17:1845-1855
Published Date: 20 March 2024
Correlation of Prognostic Nutritional Index and Systemic Immune-Inflammation Index with the Recurrence and Prognosis in Oral Squamous Cell Carcinoma with the Stage of III/IV
Ye M, Zhang L
International Journal of General Medicine 2024, 17:2289-2297
Published Date: 20 May 2024
The Effect of Systemic Immune-Inflammatory Index (SII) and Prognostic Nutritional Index (PNI) in Early Gastric Cancer
Jing Y, Ren M, Li X, Sun X, Xiao Y, Xue J, Liu Z
Journal of Inflammation Research 2024, 17:10273-10287
Published Date: 4 December 2024
The Prognostic Value of Combined Systemic Immune-Inflammatory Index (SII) and Prognostic Nutritional Index (PNI) in Solid Tumor
Zhang Y, Tang M, Gu QH, Zhou LN, Chen MB
Cancer Management and Research 2025, 17:1351-1359
Published Date: 8 July 2025
The Value of Combined Detection of Systemic Inflammation Response Index and Prognostic Nutritional Index in Predicting Short-Term Prognosis of Myasthenia Gravis
Chen T, Chen H, Wen Y, Huang Y, Lin Z, Liang Q, Huang W
Journal of Inflammation Research 2025, 18:13319-13333
Published Date: 26 September 2025