Back to Journals » Infection and Drug Resistance » Volume 15
Prognostic Effects of Delayed Administration of Appropriate Antimicrobials in Bacteraemic Adults Initially Presenting with Various Body Temperatures
Authors Ho CY, Hung YP ![]() , Chen PL
, Chen PL ![]() , Hsieh CC, Chung-Hsun Lee, Lee CC
, Hsieh CC, Chung-Hsun Lee, Lee CC ![]() , Ko WC
, Ko WC ![]()
Received 5 January 2022
Accepted for publication 3 June 2022
Published 17 June 2022 Volume 2022:15 Pages 3149—3160
DOI https://doi.org/10.2147/IDR.S357183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Ching-Yu Ho,1,2,* Yuan-Pin Hung,3– 5,* Po-Lin Chen,3,5 Chih-Chia Hsieh,3,6 Chung-Hsun Lee,3,6 Ching-Chi Lee,3,7 Wen-Chien Ko3,5
1Department of Adult Critical Care Medicine, Tainan Sin-Lau Hospital, Tainan, 70142, Taiwan; 2Department of Nursing, National Tainan Junior College of Nursing, Tainan, 700007, Taiwan; 3Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, 70403, Taiwan; 4Department of Internal Medicine, Tainan Hospital, Ministry of Health and Welfare, Tainan, 70043, Taiwan; 5Department of Medicine, College of Medicine, National Cheng Kung University, Tainan, 70101, Taiwan; 6Department of Emergency Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, 70403, Taiwan; 7Clinical Medicine Research Centre, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, 70403, Taiwan
*These authors contributed equally to this work
Correspondence: Ching-Chi Lee, Clinical Medicine Research Centre, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, No. 138, Sheng Li Road, Tainan, 70403, Taiwan, Tel +886 6-2353535 ext. 6058, Fax +886 6-2380239, Email [email protected] Wen-Chien Ko, Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, No. 138, Sheng Li Road, Tainan, 70403, Taiwan, Tel +886 6-2353535 ext. 3596, Fax +886 6-2752038, Email [email protected]
Purpose: To investigate the different impact of delayed administration of appropriate antimicrobial therapy (AAT) on short-term mortality of bacteraemia patients initially presenting with various body temperatures (BTs).
Materials and Methods: A six-year, two-center cohort consisting of adults with community-onset bacteraemia in emergency departments (EDs) was retrospectively collected. Through the multivariable analyses, clinical impacts of delayed AAT, assessed by the time gap between the first dose of AAT and ED arrival, on 30-day mortality (primary outcomes) were respectively examined in the different groups of initial BTs (iBTs).
Results: Of the 3171 adults, despite the similarities of delayed AAT in six iBT categories, hourly AAT delay was associated with an average increase in 30-day mortality rates of 0.24% in the group of iBT < 36.0℃, 0.40% in the 36.0℃– 36.9℃ group, 0.48% in the 37.0℃– 37.9℃ group, 0.59% in the 38.0℃– 38.9℃ group, 0.58% in the 39.0℃– 39.9℃ group, and 0.71% in the ≥ 40.0℃ group, after respective adjusting independent predictors of mortality. Furthermore, for 589 patients who inappropriately received empirical antimicrobial treatment (ie, delayed AAT ≥ 24 hours), with a cutoff of 34.0℃, each 1℃ increase in iBTs was independently associated with an average increase in 30-day mortality rates of 42%.
Conclusion: For adults with community-onset bacteraemia, the iBT-related differences in the prognostic impacts of delayed administration of appropriate antimicrobials might be evident.
Keywords: body temperature, empirical, antibiotic, community-onset, bloodstream infection, mortality
Introduction
Bacteraemia is indicative of high morbidity and mortality and consequently incurs substantial healthcare costs.1 Rapid identification of patients with bloodstream infections or septic shock and prompt administration of appropriate antimicrobial therapy (AAT) are essential for improving short-term prognoses.2–4 However, bacteraemia may initially have atypical manifestations (such as afebrile presentation) in specific populations, such as the elderly5 and cirrhotic patients.6 Accordingly, delayed treatment efforts are always the serious concern for treating such patients.
Increases in body temperatures (BTs) that normally occur in response to sepsis syndrome or systemic bloodstream infections, exert numerous beneficial effects by fighting causative pathogens and enhancing chemotaxis, neutrophil migration, phagocytosis, antibody production, and T-cell proliferation.7 By contrast, decreases in BTs are associated with declines in humoral and cellular immunity.8,9 In the real world, afebrile bacteraemia was often observed in immunocompromised individuals,6 and the first-line physician frequently reported the episodes of hypothermia in critically ill patients.10 Although numerous studies have previously reported that initial hypothermia or afebrile status results in unfavourable outcomes in patients experiencing sepsis or bacteraemia,6,11 the evidence is limited regarding the comparisons of the prognostic effect of delayed AAT between bacteraemia patients with initial presentation of hypothermia, normothermia, and high febrile status. We hypothesised that the prognostic impact of delayed AAT differed in bacteraemia patients presenting with different iBTs. Therefore, we categorised adults with community-onset bacteraemia according to their iBTs and investigated the adverse effects of delayed AAT administration on their short-term survival in each iBT group.
Methods
Study Design
This retrospective, two-centre cohort study was conducted during the 6-year period between January 2010 and December 2015 at the emergency departments (EDs) of two hospitals in Southern Taiwan. One hospital in the study is a university-affiliated medical centre with approximately 1400 beds, and another is a teaching hospital with 800 beds. This study was reported by the format recommended by STROBE (Strengthening the Reporting of Observational Studies in Epidemiology)12. Partial information on this cohort has been published.3,13,14
Patient Population and Data Collection
For adults attending the ED, data regarding bacterial growth on blood cultures sampled during the ED stay were screened in a computer database. Consistent with previous ED studies,13,15 to accurately collect the patients with “community-onset” bacteraemia, only the first bacteraemia episode was included for those with the multiple episodes of bacteraemia during the study period. Patients with contaminated blood cultures, incomplete clinical information, previously received steroids, antipyretics or antibiotics within 3 days before ED arrival, or transferred from other hospitals were excluded. In sum, only naïve adults experiencing community-onset bacteraemia were eligible in the present study. Clinical data were jointly collected by one board-certified ED physician and another clinician specializing in infectious diseases, both of whom received extensive training in the IRB course and were blind to the aim and hypotheses of the study. Any discrepancies that arose during data collection were resolved through periodic discussion between the authors.
Using a predetermined record form, demographic data (age, gender, and place of residence) were collected, along with data regarding any antipyretic and antibiotic prescribed prior to ED arrival, comorbidities, comorbidity severity, initial sepsis-related syndromes, bacteraemia severity (assessed by the Mortality in Emergency Department Sepsis [MEDS] score) within 24 hours after ED arrival, laboratory data, types and doses of antibiotics administered, imaging studies, surgical or radiological interventions, bacteraemia sources, causative microorganisms, and patient outcomes. To accurately capture data receiving antipyretics and antibiotics prior to ED arrival, the required information was retrieved from both chart records and telephone contacts, after the patient was discharged from our hospitals. The patients we could not reach by telephone or those with information discrepancies in the chart and telephone reports were excluded; and these excluded patients were regarded as those with incomplete clinical information. The primary study endpoint was crude mortality within 30 days after bacteraemia onset (ie, ED arrival).
Definitions
A patient’s iBT was defined as the temporal BT measurement obtained immediately at ED arrival (ie, the ED triage). Bacteraemia was defined as bacterial growth of blood cultures drawn from central or peripheral venipuncture, after exclusion of contaminant sampling. As previously described,3,13,14 community-onset bacteraemia indicates that the place of the acquisition of bacteraemia was the community and includes long-term healthcare-associated and community-acquired bacteraemia. The growth of potentially contaminated pathogens on blood cultures, such as coagulase-negative staphylococci, Clostridium perfringens, Micrococcus spp., Bacillus spp., Propionibacterium spp., and Gram-positive bacilli, was regarded as being contaminated, in accordance with previous criteria (shown in Supplemental Box 1) 16. Polymicrobial bacteraemia was defined as the isolation of more than one microbial species in a bacteraemia episode.
As previously described,3,13,14 antibiotic therapy was appropriate if the following two criteria were fully met: (i) antimicrobials were administered according to the route and dosage recommended in 2021 Sanford Guide17 and (ii) the antibiotics administered were in vitro active against all causative microorganisms of bacteraemia, according to the 2021 breakpoint issued by the Clinical and Laboratory Standards Institute (CLSI).18 The period of delayed AAT was defined as the time interval between bacteraemia onset (ie, ED arrival) and the first AAT administration.3 As the previous definition,13,15 delayed AAT ≥24 hours was regarded as the inappropriateness of empirical antimicrobial therapy (IEAT).
Comorbidities were defined as described previously,19 and the prognoses of comorbidities were assessed according to the delineated McCabe classification.20 The sources of bacteraemia were determined clinically on the basis of the presence of an active infection site coincident with bacteraemia or the isolation of a microorganism from other clinical specimens prior to or on the same date of bacteraemia onset. For complicated bacteraemia, the removal of infected hardware, drainage of infected fluid that had accumulated, or resolution of the obstruction of biliary or urinary tracts was regarded as appropriate control of the bacteraemia source.4 Bacteraemia severity was graded according to the MEDS score,21,22 which reflects measurements of nine crucial components available in EDs, and stratified patients according to their mortality risk, and a score of ≥13 points indicated the critical illness. Based on the Sepsis-3 definition,23 septic shock is a subset of sepsis with circulatory and cellular/metabolic dysfunction associated with a higher risk of mortality.
Microbiological Methods
Blood cultures were sampled by nurses or physicians in the ED, and two sets of blood cultures (one bottle of aerobic culture and one bottle of anaerobic culture) were obtained from different peripheral veins or arteries at intervals of at least 30 minutes. Approximately 5–10 mL (average 8 mL) of blood per bottle was collected from each patient. Blood culture bottles were transported immediately to the microbiology laboratory, where they were loaded into the BACTEC 9240 automated blood culture system (Becton Dickinson and Company, Franklin Lakes, NJ, USA) and incubated for 5 days. Bacteraemic isolates were identified by the matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS).
To ensure the accuracy of the AAT timing for each bacteraemia episode, bacteraemic isolates in the study cohort were prospectively stored. If antibiotics empirically administrated were not included in the initial susceptibility panel offered by the study hospital, susceptibilities to the administered antibiotics were retrospectively tested. The disk diffusion and agar dilution methods were respectively employed for aerobes and anaerobes, as recommended by the 2021 CLSI guidelines.18 The patients unidentified for the period of delayed AAT were excluded because of the lack of isolate storage, and the excluded patients were regarded as those with incomplete clinical information.
Statistical Analysis
The Statistical Package for the Social Sciences for Windows, version 23.0 (Chicago, IL, USA) was used for statistical analyses. Continuous and categorical variables were expressed as medians (interquartile ranges, IQRs) and numbers (percentages), respectively. The linear-by-linear association was assessed by Pearson’s correlation to identify iBT-related trends in the proportions of clinical variables or the mortality rates.
Two methods were adopted to investigate the prognostic effects of delayed AAT on patient presenting with varied iBTs. First, the variables identified through univariable analysis as having a P value of less than 0.2 were input into the multivariable logistic regression (stepwise and backward) model to determine the independent predictors of 30-day mortality. After adjustment for these independent predictors, prognostic effects of each hour of delayed AAT in the different iBT groups were determined by hierarchical logistic regression. Second, focusing on patients who received IEAT (ie, delayed AAT ≥ 24 hours), the prognostic effect of each increased degree of iBTs (using a cutoff of 34.0℃) was investigated after adjustment for independent predictors of 30-day mortality, recognised by the logistic regression (stepwise and backward) model analyzing on the variables having a P value of less than 0.2 in the univariable analysis. Finally, E values were tested to assess the potential effects of unmeasured confounders in each iBT group.24 P < 0.05 was considered indicative of statistical significance.
Results
Patient Populations
Of 6102 patients with bacterial growth in their blood cultures, 3342 (54.8%) had community-onset bacteraemia, 2117 (34.7%) had blood culture contamination (Supplemental Result and Supplemental Table 1), and 643 (10.5%) had been transferred from other hospitals. After the exclusion of 148 patients with incomplete clinical information (including 54 with uncertain pre-ED information [in terms of unavailable telephone contact and information discrepancy], 63 with a lack of AAT details, and 31 with uncertain mortality dates) and 23 patients who had received previously steroid, antipyretic, or antimicrobial therapy, 3171 adults with community-onset bacteraemia were included in our cohort. The information detailing patient demographics and bacteraemia characteristics in the overall cohort was exhibited in the Supplemental Table 2. Their median (IQR) ED and hospital stays were 16 (6–27) hours and 10 (6–18) days, respectively. Their median (IQR) iBT was 38.7℃ (38.2℃–39.4℃). The majority (2576 patients, 81.2%) of the patients were admitted to general wards through the ED, 323 (10.2%) were admitted to intensive care units, and 105 (3.3%) died during their ED stay. Only 167 (2.4%) patients were discharged from the ED and revisited the outpatient clinics. The 15- and 30-day crude mortality rates were 11.4% (360 patients) and 14.8% (469), respectively.
Clinical Presentations, Severity, and Outcomes Among Various iBT Groups
Clinical characteristics and outcomes were compared between patients with iBTs in each following category: <36.0℃ (239 patients, 7.5%), 36.0℃–36.9℃ (127, 4.0%), 37.0℃–37.9℃ (276, 8.7%), 38.0℃–38.9℃ (1187, 37.4%), 39.0℃–39.9℃ (943, 29.7%), and ≥40.0℃ (399, 12.6%; Table 1). The proportion of the IEAT patients (ie, delayed AAT ≥ 24 hours), the elderly, male patients, polymicrobial bacteraemia, streptococcus bacteraemia, comorbidities of cardiovascular diseases, neurological diseases, or liver cirrhosis, and bacteremic pneumonia decreased, as the iBT increased. In contrast, the proportion of Escherichia coli bacteraemia and bacteraemia due to urinary tract infections decreased, as the iBT increased. Notably, despite similarities in the period of delayed AAT between iBT groups, the patient proportion of the critical illness (MEDS score ≥ 13) and fatal comorbidities (McCabe classification) as well as 15- and 30-day crude mortality rates increased, as the iBT increased (Figure 1).
 |
Table 1 The iBT-Related Trends in the Clinical Characteristics of Adults with Community-Onset Bacteraemia* |
 |
Figure 1 The iBT-related trends in the patient proportion of the critical illness and fatal comorbidities (McCabe classifications) as well as 15- and 30-day crude mortality rates. Abbreviations: AAT, appropriate antimicrobial therapy; iBT, initial body temperature; MEDS, Mortality in Emergency Department Sepsis. |
Predictors of 30-Day Mortality in Overall Patients
Through the multivariable regression model (Table 2), nine independent predictors of mortality only were identified: inadequate source control during antimicrobial therapy, comorbid malignancies, polymicrobial bacteraemia, causative microorganisms of Staphylococcus aureus, Pseudomonas species, or Acinetobacter species, the critical illness (a MEDS score ≥ 13) in EDs, and bacteraemia caused by urinary tract infections or liver abscess. The median (IQR) of delayed AAT in fatal patients and survivors was 2.0 (1.1–12.0) and 2.0 (0.9–7.0) hours, respectively. Notably, each hour of AAT delay was associated with an average increase in the 30-day crude mortality rate of 0.3% (adjusted odds ratio [AOR], 1.003; 95% confidence interval, 1.002–1.004; P < 0.001) in the overall cohort, after adjusting these nine independent prognosis determinants.
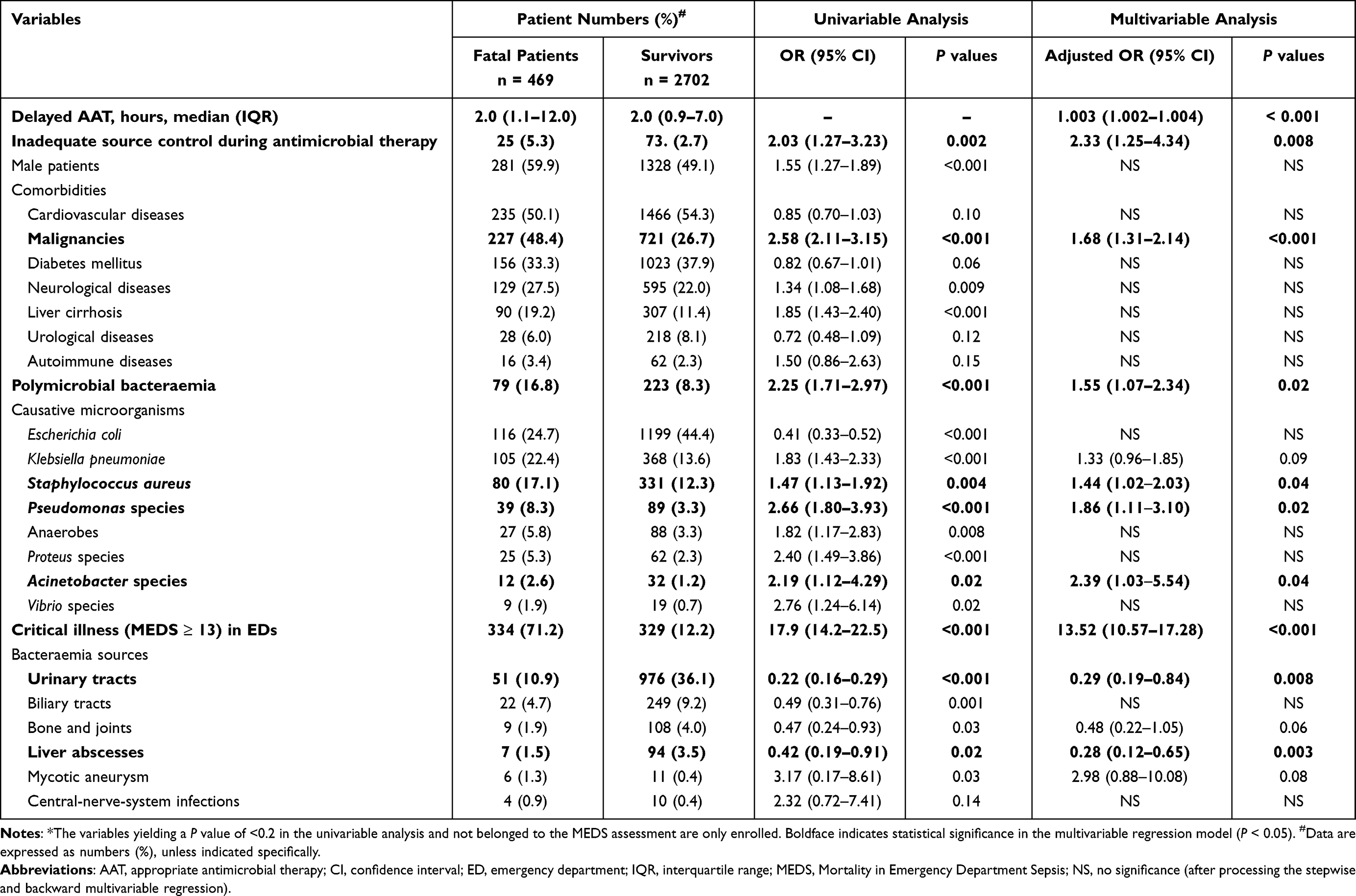 |
Table 2 Predictors of 30-Day Crude Mortality in Overall 3171 Patients with Community-Onset Bacteraemia* |
Prognostic Impacts of Delayed AAT in Varied iBT Groups
The hourly AAT delay was independently associated with an average increase in the 30-day mortality rate of 0.24% in the iBT group of <36.0℃ (239 patients; AOR, 1.0024; P = 0.04), 0.40% in 36.0℃–36.9℃ (127; AOR, 1.0040; P = 0.04), 0.48% in 37.0℃–37.9℃ (276; AOR, 1.0051; P = 0.001), 0.59% in 38.0℃–38.9℃ (1187; AOR, 1.0059; P < 0.001), 0.58% in 38.0℃–39.9℃ (943; AOR, 1.0058; P = 0.002), and 0.71% in ≥40.0℃ (399; AOR, 1.0071; P = 0.01), after respective adjustments of nine independent predictors. Notably, as the iBT increased, the prognostic effect of delayed AAT (ie, AORs) increased (γ = 0.970, P = 0.001; Figure 2).
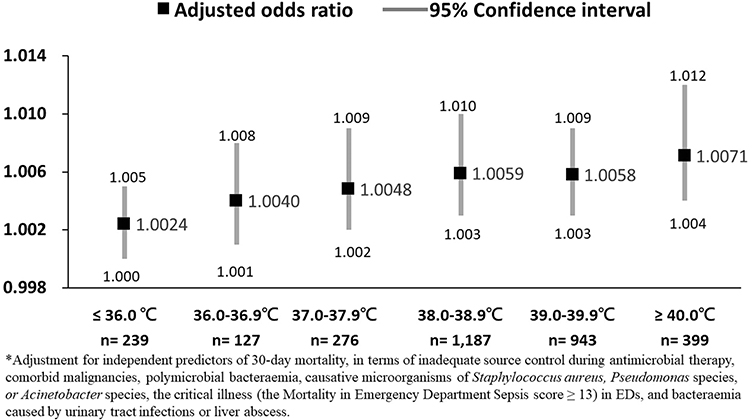 |
Figure 2 Prognostic effects of each hourly AAT delay in different iBT groups*. Abbreviations: AAT, appropriate antimicrobial therapy; iBT, initial body temperature. |
Prognostic Impacts of Elevated iBTs in Patients Who Received IEAT
For 589 patients who received IEAT (ie, delayed AAT ≥ 24 hours), the univariable analyses revealed that the clinical predictors of 30-day crude mortality included the critical illness (MEDS ≥ 13) in EDs, causative microorganisms of Escherichia coli or Klebsiella pneumoniae, bacteraemia caused by urinary tract infections, and comorbidities of malignancies, liver cirrhosis, or chronic obstructive pulmonary diseases (Table 3). Notably, the longer degree gap of iBTs from 34.0℃ in fatal patients than survivors was disclosed. Consequently, multivariable analyses revealed that each elevated 1℃ of iBTs was independently associated with an average increase in the 30-day mortality rate of 42% (AOR, 1.42; P < 0.001), using a cutoff of 34.0℃ and after adjustment for three independent predictors, namely the critical illness in EDs, Pseudomonas bacteraemia, and comorbid malignancies (Table 3).
 |
Table 3 Prognostic Effects of Elevated iBTs in Patients Who Received IEAT (ie, Delayed AAT ≥ 24 Hours)* |
Discussion
Fever is a normal response to systemic infections and has several beneficial effects, including the alleviation of sepsis and enhancement of host defence.7 Because fever is a common feature in response to sepsis or systematic infections, if a patient presents with an elevated BT, clinicians reasonably consider the possibility of infections. However, specific populations may present with afebrile at the episodes of bacteraemia or sepsis,5,25 such atypical presentations tend to cause delays in the accurate diagnosis and treatment efforts and consequently result in unfavourable prognoses.25 Extensive evidence supports the prognostic disadvantage of delayed AAT in patients with bloodstream infections.3,15,26 However, limited studies have investigated the effects of delayed AAT on the short-term survival of bacteraemic patients specifically experiencing afebrile status or hypothermia.6 Of note, the present cohort study is the first to disclose the different prognostic effects of delayed AAT on bacteraemia patients initially presenting with various BTs. In other words, patients presenting with higher iBTs exhibited more severe adverse effects of delayed administration of appropriate antimicrobials on their short-term mortality.
Consistent with previous reported detailing the association of BTs and mortality in ED patients,27 we indicated that afebrile status or hypothermia in bacteraemia adults was corresponding to worse prognoses, compared with that of patients with febrile response at bacteraemia onset. We believe that the favourable prognoses of patients with higher iBTs are attributable to increased humoral and cellular immunity.7 However, like a double-edged sword, the enhanced immunity response, induced by higher BTs, might lead to the increased impacts of delayed AAT on short-term prognoses. From our suspect, our findings are consistent with comprehensive studies supporting the prognostic disadvantage of IEAT administration in patients experiencing septic shock,28 because the enhanced immunity activity in such critically ill individuals had been evident.29 Accordingly, further animal studies investigating the prognostic effect of delayed AAT on the specific populations with high iBTs are warranted.
Of the several scoring systems previously developed for predicting short-term mortality in patients with sepsis or bacteraemia, not all use iBTs as an indicator of severity assessment. For example, the iBT is regarded as the key parameter of the Simplified Acute Physiology Score (SAPS II),30 the Pitt bacteraemia score,3 and the Acute Physiology and Chronic Health Evaluation.31 Consistent with these scoring systems, a crucial association was observed between lower iBTs and poor prognoses in our cohort. Otherwise, the iBT is not used as an indicator of severity assessment in other scoring systems, such as the quick Sepsis-related Organ Failure Assessment (qSOFA),32 SOFA,30 and MEDS scores.21 We postulate that this discrepancy is primarily attributable to different study populations. Of these scoring systems, the Pitt bacteraemia score is reliable and useful for predicting the short-term outcome of patients experiencing various bacteraemia types, such as community-onset bacteraemia,3 S. aureus bacteraemia,33 and Enterobacteriaceae bacteraemia.34 However, the Pitt bacteraemia score was not adapted to avoid over-counting the BT variable in our analysis. We used the MEDS scores as the assessment of bacteraemia severity in the present study because the successful validation of MEDS scores on bacteraemia patients had been evidenced.21 In sum, our findings demonstrate that the iBT not only is linked to patient prognoses, but can also be used as a prognostic determinant in response to delayed AAT in patients with bacteraemia.
This study had several limitations inherent in its design. First, the performance of BT measurements with central thermometers, such as pulmonary artery catheter, urinary bladder, oesophageal, and rectal thermometers, in all ambulatory patients is infeasible in such overcrowding EDs. As previously suggested,6 the temporal area was selected as an adequate site for BT measurement for patients attending the ED, but this measurement really limits the external validation of our finding. Second, to avoid categorisation bias due to the defervescence effects of antipyretics and steroids, patients who had accepted these medications prior to their ED arrival were excluded from the study. To diminish record and recall bias, we design to achieve the information accuracy using two capturing methods. Because only 18 patients (categorized into the group of unavailable information prior to ED arrival) with information discrepancy were recognised. Therefore, these basis in our cohort can be considered negligible. Third, the E values for assessing the prognostic effect of delayed AAT were calculated to be 1.03%, 1.05%, 1.05%, 1.08%, 1.06%, and 1.03% in patients with iBTs of <36.0℃, 36.0℃–36.9℃, 37.0℃–37.9℃, 38.0℃–38.9℃, 39.0℃–39.9℃, and ≥40.0℃, respectively. Therefore, unmeasured confounders both interacting with delayed AAT and 30-day mortality are likely to be negligible. Fourth, because of the large patient cohort established in our study design, we did not conduct formal sample size calculations and all available patient information was captured to maximise the power. Finally, because of the nature of the retrospective study, recall and selection bias may have occurred during the review of chart records. To reduce recall collect clinical information, two IRB-trained researchers who were blind to the aims and hypotheses of the study reviewed the patients’ medical records to accurately collect clinical information. Additionally, by the multicentre design, only a small proportion (ie, 148 patients) of the entire cohort was excluded because of incomplete data collection, meaning that the exclusion process likely had minimal effects on the results of the current study. In the lack of the aforementioned concerns, we reasonably apply the study results to our daily practise in the ED.
Conclusion
For adults with community-onset bacteraemia, the iBT-related differences in the prognostic impact of delayed AAT might be evident. Accordingly, to achieve favourable outcomes, more attention should be paid to iBT for the optimal establishment of the antimicrobial stewardship programme. This would enable prompt AAT administration for bacteraemic patients with high iBT and achieve their favourable short-term prognoses.
Abbreviations
AAT, appropriate antimicrobial therapy; AOR, adjusted odds ratio; BT, body temperature; CLSI, Clinical and Laboratory Standards Institute; CI, confidence interval; ED; emergency department; iBT, initial body temperature; IEAT, inappropriate empirical antimicrobial therapy; IRB, institutional review board; IQR, interquartile range; MEDS = Mortality in Emergency Department Sepsis.
Data Sharing Statement
All data are fully available without restriction.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of National Cheng Kung University Hospital (B-ER-109-144), Sin-Lau Hospital (SLH 9919-108-006 and SLH 9919-108-009). The ethics committee waived the need for written informed consent provided by participants due to the retrospective nature of the study. Based on the Declaration of Helsinki, no additional informed consent was required, because all patient data were analyzed in anonymity.
Consent for Publication
All authors have provided consent for publication of the manuscript.
Acknowledgments
We would like to thank for providing experimental space and facilities by Diagnostic Microbiology and Antimicrobial Resistance Laboratory, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan. We also thank Ms Tzu-Jung Chuang for providing statistical consulting services.
Funding
This study was partially supported by research grants from the Ministry of Science and Technology (MOST 109-2314-B-006-097 and MOST 110-2314-B-006-068), the Ministry of Health and Welfare (MOHW109-TDU-B-211-114003), and National Cheng Kung University Hospital (NCKUH-11003036 and NCKUH-11104005), Taiwan.
Disclosure
The authors have no conflicts of interest in relation to this work to declare.
References
1. Laupland KB, Church DL. Population-based epidemiology and microbiology of community-onset bloodstream infections. Clin Microbiol Rev. 2014;27(4):647–664. doi:10.1128/CMR.00002-14
2. Kothari A, Morgan M, Haake DA. Emerging technologies for rapid identification of bloodstream pathogens. Clin Infect Dis. 2014;59(2):272–278. doi:10.1093/cid/ciu292
3. Lee CC, Lee CH, Yang CY, Hsieh CC, Tang HJ, Ko WC. Beneficial effects of early empirical administration of appropriate antimicrobials on survival and defervescence in adults with community-onset bacteremia. Crit Care. 2019;23(1):363. doi:10.1186/s13054-019-2632-1
4. Coopersmith CM, De Backer D, Deutschman CS, et al. Surviving sepsis campaign: research priorities for sepsis and septic shock. Intensive Care Med. 2018;44(9):1400–1426. doi:10.1007/s00134-018-5175-z
5. Berman P, Hogan DB, Fox RA. The atypical presentation of infection in old age. Age Ageing. 1987;16(4):201–207. doi:10.1093/ageing/16.4.201
6. Chen HY, Hsu YC. Afebrile bacteremia in adult emergency department patients with liver cirrhosis: clinical characteristics and outcomes. Sci Rep. 2020;10(1):1–8. doi:10.1038/s41598-019-56847-4
7. Roberts NJ
8. Ishikawa K, Tanaka H, Shiozaki T, et al. Characteristics of infection and leukocyte count in severely head-injured patients treated with mild hypothermia. J Trauma. 2000;49(5):912–922. doi:10.1097/00005373-200011000-00020
9. Hashiguchi N, Shiozaki T, Ogura H, et al. Mild hypothermia reduces expression of heat shock protein 60 in leukocytes from severely head-injured patients. J Trauma. 2003;55(6):1054–1060. doi:10.1097/01.TA.0000033252.43742.8B
10. Thomas-Rüddel DO, Hoffmann P, Schwarzkopf D, et al. Fever and hypothermia represent two populations of sepsis patients and are associated with outside temperature. Critical Care. 2021;25(1):1–10. doi:10.1186/s13054-021-03776-2
11. Tiruvoipati R, Ong K, Gangopadhyay H, Arora S, Carney I, Botha J. Hypothermia predicts mortality in critically ill elderly patients with sepsis. BMC Geriatr. 2010;10:70. doi:10.1186/1471-2318-10-70
12. Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
13. Hsieh CC, Chen PL, Lee CH, Yang CY, Lee CC, Ko WC. Definitive cefazolin therapy for stabilized adults with community-onset Escherichia coli, Klebsiella species, and proteus mirabilis bacteremia: MIC matters. J Clin Med. 2020;9(1):157. doi:10.3390/jcm9010157
14. Lee CC, Yang CY, Hsieh CC, et al. Timing of follow-up blood cultures for community-onset bacteremia. Sci Rep. 2019;9(1):14500. doi:10.1038/s41598-019-51032-z
15. Chen HC, Lin WL, Lin CC, et al. Outcome of inadequate empirical antibiotic therapy in emergency department patients with community-onset bloodstream infections. J Antimicrob Chemother. 2013;68(4):947–953. doi:10.1093/jac/dks475
16. Lee CC, Lin WJ, Shih HI, et al. Clinical significance of potential contaminants in blood cultures among patients in a medical center. J Microbiol Immunol Infect. 2007;40(5):438–444.
17. Gilbert DN, Chambers HF, Saag MS, Pavia AT. Antimicrobial drug dosage/side effects. Sperryville, VA: Antimicrobial Therapy, Inc; 2021.
18. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; approved standard. 31th informational supplement. CLSI document M100-S31. Wayne, PA: CLSI; 2021.
19. Islam MM, Valderas JM, Yen L, Dawda P, Jowsey T, McRae IS. Multimorbidity and comorbidity of chronic diseases among the senior Australians: prevalence and patterns. PLoS One. 2014;9(1):e83783. doi:10.1371/journal.pone.0083783
20. McCabe WR. Gram-negative bacteremia. Adv Intern Med. 1974;19:135–158.
21. Hsieh CC, Yang CY, Lee CH, Chi CH, Lee CC. Validation of MEDS score in predicting short-term mortality of adults with community-onset bacteremia. Am J Emerg Med. 2020;38(2):282–287. doi:10.1016/j.ajem.2019.05.002
22. Zhang G, Zhang K, Zheng X, Cui W, Hong Y, Zhang Z. Performance of the MEDS score in predicting mortality among emergency department patients with a suspected infection: a meta-analysis. Emerg Med J. 2020;37(4):232–239. doi:10.1136/emermed-2019-208901
23. Napolitano LM. Sepsis 2018: definitions and guideline changes. Surg Infect. 2018;19(2):117–125. doi:10.1089/sur.2017.278
24. VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–274. doi:10.7326/M16-2607
25. Hyernard C, Breining A, Duc S, et al. Atypical presentation of bacteremia in older patients is a risk factor for death. Am J Med. 2019;132(11):1344–1352. doi:10.1016/j.amjmed.2019.04.049
26. Hernández-Bou S, Trenchs V, Alarcón M, Luaces C. Afebrile very young infants with urinary tract infection and the risk for bacteremia. Pediatr Infect Dis J. 2014;33(3):244–247. doi:10.1097/INF.0000000000000033
27. Schuttevaer R, Brink A, Alsma J, et al. The association of body temperature with antibiotic therapy and mortality in patients attending the emergency department with suspected infection. Eur J Emerg Med. 2021;28(6):440. doi:10.1097/MEJ.0000000000000817
28. Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749–1755. doi:10.1097/CCM.0000000000000330
29. Lolis E, Bucala R. Therapeutic approaches to innate immunity: severe sepsis and septic shock. Nat Rev Drug Discov. 2003;2(8):635–645. doi:10.1038/nrd1153
30. Granholm A, Møller MH, Krag M, Perner A, Hjortrup PB. Predictive performance of the simplified acute physiology score (SAPS) II and the initial sequential organ failure assessment (SOFA) score in acutely ill intensive care patients: post-hoc analyses of the SUP-ICU inception cohort study. PLoS One. 2016;11(12):e0168948. doi:10.1371/journal.pone.0168948
31. Sadaka F, EthmaneAbouElMaali C, Cytron MA, Fowler K, Javaux VM, O’Brien J. Predicting mortality of patients with sepsis: a comparison of APACHE II and APACHE III scoring systems. J Clin Med Res. 2017;9(11):907. doi:10.14740/jocmr3083w
32. Song J-U, Sin CK, Park HK, Shim SR, Lee J. Performance of the quick Sequential (sepsis-related) organ failure assessment score as a prognostic tool in infected patients outside the intensive care unit: a systematic review and meta-analysis. Critical Care. 2018;22(1):1–13. doi:10.1186/s13054-018-1952-x
33. Hsu MS, Huang YT, Hsu HS, Liao CH. Sequential time to positivity of blood cultures can be a predictor of prognosis of patients with persistent Staphylococcus aureus bacteraemia. Clin Microbiol Infect. 2014;20(9):892–898. doi:10.1111/1469-0691.12608
34. Ben-Chetrit E, Eldaim MA, Bar-Meir M, Dodin M, Katz DE. Associated factors and clinical outcomes of bloodstream infection due to extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae during febrile neutropenia. Int J Antimicrob Agents. 2019;53(4):423–428. doi:10.1016/j.ijantimicag.2018.12.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.