Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 9
Prognostic analysis of CD5 expression in double-hit diffuse large B-cell lymphoma and effectiveness comparison in patients treated with dose-adjusted EPOCH plus rituximab/R-CHOP regimens
Authors Zhang F, Li L, Zhang L, Li X, Fu X, Wang X, Wu J, Sun Z, Kong F, Ren L, Zhang M
Received 19 May 2019
Accepted for publication 11 July 2019
Published 19 August 2019 Volume 2019:9 Pages 33—43
DOI https://doi.org/10.2147/BLCTT.S216292
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Dingli
Fangwen Zhang,1,2,* Ling Li,1,2,* Lei Zhang,1,2 Xin Li,1,2 Xiaorui Fu,1,2 Xinhua Wang,1,2 Jingjing Wu,1,2 Zhenchang Sun,1,2 Fei Kong,1,2 Liangliang Ren,1,2 Mingzhi Zhang1,2
1Department of Oncology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan 450052, People’s Republic of China; 2Department of Oncology, Lymphoma Diagnosis and Treatment Center of Henan Province, Zhengzhou, Henan 450052, People’s Republic of China
Correspondence: Ling Li; Mingzhi Zhang
Department of Oncology, Zhengzhou University First Affiliated Hospital, No. 1 Jianshe East Road , Zhengzhou, Henan 450052, People’s Republic of China
Email [email protected]
[email protected]
*These authors contributed equally to this work
Objectives: To compare the efficacy of rituximab, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide and doxorubicin (DA-EPOCH-R) with traditional rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP) regimens in CD5+ double-hit lymphoma (DHL) and to evaluate prognostic factors.
Methods: We retrospectively studied 139 patients with newly diagnosed DHL/THL diffuse large B-cell lymphoma (including 20 cases CD5+ and 119 cases CD5−), 87 cases were MYC/BCL2 DHL, 30 cases were MYC/BCL6 DHL, 22 cases were THL. MYC, BCL2 and BCL6 rearrangements were examined by fluorescence in-situ hybridization. CD5 is detected by immunohistochemistry (IHC).
Results: The objective response rate (ORR) difference between CD5+ and CD5− was significant (80.0% vs 63.8%, P=0.003). The median follow-up time was 18 months (range: 4–39 months). Progression-free survival (PFS) of CD5+ group was significantly worse than that of CD5- (28.1% vs 59.0%, P=0.028), while no significant difference was observed in overall survival (OS) (32.1% vs 59.9%, P=0.057). Compared with the two regimens, the 2-year survival rate of DA-EPOCH-R group was significantly superior than that of R-CHOP (63.6% vs 45.4%, P=0.034 for PFS; 67.4% vs 47.8%, P=0.038 for OS). Besides, CD5+ patients receiving DA-EPOCH-R had survival benefits compared with R-CHOP in PFS (85.7% vs 23.0%, P=0.029), but there was no statistical difference in OS (87.7% vs 34.4.0%, P=0.064). However, in DA-EPOCH-R protocol, there was no significant difference between CD5+ DHL (MYC/BCl2 and MYC/BCL6) and triple-hit lymphoma (P=0.776 for PFS; P=0.728 for OS). Multivariate analysis showed that CD5+ treatment regimen and disease stage were independent prognostic factors.
Conclusion: Our retrospective study shows that CD5+ has a poorer prognosis than CD5− patients. Based on its improved lifetime and good tolerance on CD5+ patients, which is expected to become the first-line treatment for high-risk DLBCL types based on more clinical research.
Keywords: CD5, DA-EPOCH-R, R-CHOP, diffuse large B-cell lymphoma, double-hit, treatment, prognosis
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin lymphoma, which represents approximately ~40% of all cases.1,2 The category of DLBCL represents a heterogeneous group of neoplasms, different subsets of DLBCL have a different underlying disease biology explaining differences in prognosis.3,4 In the rituximab time, R-CHOP regimen has greatly improved the survival rate of DLBCL patients, approximately 60% of patients with DLBCL are cured.5 However, there are still some high-risk DLBCL patients who show poor prognosis after receiving standard R-CHOP chemotherapy, with a less than 50% of 5-year survival rate.6 The 2016 WHO classification of the lymphoid hematopoietic system clearly defined the concurrent translocation of the MYC and BCL2/BCL6 genes as double-hit lymphoma (DHL).7 The result of DHL patients treated with R-CHOP regimen is poor, especially those with aggressive prognosis factors.8 Rituximab with DA-EPOCH (DA-EPOCH-R) has been shown to be effective in the treatment of DHL patients, and superior PFS has been reported in comparison with R-CHOP protocol.9–11
CD5-positive (CD5+) DLBCL accounts for approximately 5–10% of all DLBCL,1,4,5 patients with CD5+ have distinctive clinic features including higher international prognostic index (IPI), higher frequency of extranodal sites involvement, easy central nervous system (CNS) involvement and relapse when compared with patients with CD5-negative DLBCL.12–16 Patients with CD5-positive DHL-DLBCL are rare and have poorer OS when treated with CHOP or R-CHOP regimens.17–20 R-EPOCH is a dose-adjusted infusional regimen that has shown improved outcome (versus R-CHOP) in untreated patients with aggressive and high-risk DLBCL.10,21,22 However, the effect in patients with CD5+ DHL-DLBCL is rarely reported.
In this study, we compared the survival outcome in CD5+ with CD5-negative DHL-DLBCL patients as well as the prognostic significance of CD5 expression in DHL-DLBCL patients treated with DA-EPOCH-R and R-CHOP, the purpose is to evaluate whether DA-EPOCH-R regimen is better than R-CHOP in CD5+ DHL-DLBCL patients.
Materials and methods
Patients selection
We collected 718 cases of newly diagnosed DLBCL patients who underwent fluorescence in-situ hybridization (FISH) detection from June 2015 to August 2018 in the database of First Affiliated Hospital of Zhengzhou University. One hundred and thirty-nine patients were conformed the DHL/THL diagnostic criteria (including 20 cases CD5+ and 119 cases CD5−); among them, 87 cases were MYC/BCL2 DHL, 30 cases were MYC/BCL6 DHL and 22 cases were MYC/BCL2/BCL6 THL. Patients were identified by at least three lymphoma pathologists in our hospital. Patients with primary mediastinal DLBCL, primary cutaneous DLBCL, lymphomatoid granulomatosis, T-cell/histiocyte-rich large B-cell lymphoma, plasmablastic lymphoma, small mature B-cell lymphoma and primary CNS lymphoma were excluded. The baseline clinical characteristics included age, gender, Ann Arbor stage, IPI score, serum lactate dehydrogenase (LDH) level, serum B2M level, extranodal sites involvement, COO subtype and CNS positive at involvement. The genetic abnormality of MYC and BCL2/BCL6 was detected by FISH. The Hans classification was used to analyze the cell of origin subtype, positive detection of CD antigen by immunohistochemistry.
Immunohistochemistry
Immunohistochemical studies were performed using formalin-fixed, paraffin-embedded (FFPE) tissue sections. The following panel of antibodies used was as follows: CD3, CD20, CD5, CD10, BCL-2, BCL-6, MUM1, FOXP-1, cyclin D1, SOX-11 and Ki-67. Cutoffs ≥50% tumor cells with a strong expression for CD5 were considered positive. The cutoffs for positivity were ≥30% for CD10, BCL-6 and MUM-1 to distinguish these tumors as germinal center or non-germinal center cell-like immunophenotype (Hans algorithm).23 According to Visco–Young algorithm, the positive cutoff for FOXP1 was ≥60%.24 The cutoffs for positive MYC or BCL-2 results were ≥40% and ≥50%, respectively, as reported previously.
Fluorescence in situ hybridization
FISH was performed using LSI dual-color break-apart probes for MYC and BCL6, and dual-color, dual fusion probe for BCL2/IGH. For biopsy specimens, 4-μm FFPE tissue sections were used. The signals from 200 nuclei were analyzed. All cutoffs were low (≤5%) and all cases positive for rearrangements had a positive signal in ≥25% of nuclei examined. Cases were designated as DHL if concurrent MYC and BCL2 or BCL6 were rearranged.
Treatment programs
All patients were treated with R-CHOP or DA-EPOCH-R regimen. The choice of therapy (DA-EPOCH-R versus R-CHOP) for these patients was up to the discretion of the oncology physician and patient’s will. The DA-EPOCH-R regimen was preferred for patients with high-risk clinical or pathologic features.
The R-CHOP regimen includes rituximab (375 mg/m2) on day 1, followed by CHOP, which consisted of cyclophosphamide 750 mg/m2 as an intravenous infusion on day 1, vincristine 1.4 mg/m2 (the maximum dose 2 mg) as an intravenous infusion on day 1, doxorubicin 50 mg/m2 as an intravenous infusion on day 1 and prednisone 100 mg/m2 orally on days 1–5. The DA-EPOCH-R regimen comprised rituximab (375 mg/m2) on day 1, followed by DA-EPOCH. Starting dose of DA-EPOCH composed of etoposide 50 mg/m2 as a continuous intravenous infusion on days 1–4, vincristine 0.4 mg/m2 as a continuous intravenous infusion on days 1–4, doxorubicin 10 mg/m2 as a continuous intravenous infusion on days 1–4, cyclophosphamide 750 mg/m2 intravenous on day 5 and prednisone 60 mg/m2 orally on days 1–5. The meaning of the DA-EPOCH-R regimen is that when grade 4 myelosuppression was not reached at the end of the previous cycle of treatment, 20% of the original dose was increased in the subsequent cycles until patient got grade 4 myelosuppression. The cycle of both regimens was 21 days. All patients underwent blood tests before chemotherapy to rule out chemotherapy contraindications. Chemotherapy-related adverse reactions were graded according to the WHO criteria for cancer treatment results,25 granulocyte colony-stimulating factor (G-CSF) was given when patients suffered form leukopenia or neutropenia and recombinant human thrombopoietin was applied for thrombocytopenia symptom. When necessary, the infusion of hemoglobin can be carried out. Symptomatic supportive care was given for non-hematological toxicities. Clinical information on patients meeting the inclusion criteria was obtained from the medical records from the First Affiliated Hospital of Zhengzhou University. Informed consent for the collection of medical information was obtained from all patients. This study was approved by the ethics committee of the First Affiliated Hospital of Zhengzhou University. This study was conducted in accordance with the Declaration of Helsinki.
Adverse reactions evaluation and follow-up
Efficacy was evaluated after completion of every two cycles of chemotherapy, and the final evaluation was conducted after completion of the last cycle chemotherapy 1 month later. 18F-FDG PET-CT scan was generally used to evaluate the standard uptake value of the lesion before treatment, and CT scan was used to evaluate the efficacy of every 2 cycles. Evaluation of adverse reactions was implemented during each cycle. The responses were assessed in the light of modified Cheson criteria.26,27 Complete response (CR) was defined as the disappearance of all lesions for at least 4 weeks, including clinical indicators, laboratory and radiological findings. Partial response (PR) was an indicator of all clinical and imaging baseline abnormalities with a reduction of at least 50% and without new lesions. Stable disease (SD) means less than 50% of tumor shrinkage or less than 25% of tumor growth, at least 4 weeks. Progressive disease (PD) was defined as a greater than 25% increase in the tumour lesions or the appearance of new lesions. According to the WHO adverse reaction evaluation criteria,25 toxicities were evaluated at each cycle from the first administration day to 1 month after completion of treatment. The principle of follow-up is visiting patients every 3 months within 1 year after the end of treatment, every semi-annual for the next 2 years and then annual follow-up until relapse.
Research end points and statistical analysis
The primary study end points were PFS and OS. OS was calculated from the date of diagnosis to the time of death or last follow-up. PFS was computed from the date of diagnosis to the time of last follow-up or an treatment failure, relapse, death. The second study end points were ORR. Statistical analyses were performed with SPSS version 22 and GraphPad Prism7. We used the chi-squared test and Fisher’s exact test to compare the categorical variables. Two-year PFS and OS rates were compared between groups using the log-rank test, their 95% CIs were estimated by using the Kaplan–Meier method. Prognostic factors were analyzed using COX proportional hazards regression model. All P-values reported were bilateral, and P<0.05 was considered to be statistically significant. Follow-up was completed in March 2019 for analysis.
Results
Patients clinical characteristics
One hundred and thirty-nine patients were diagnosed as DHL/THL-DLBCL by FISH test, 87 cases were MYC/BCL2 DHL, 30 cases were MYC/BCL6 DHL and 22 cases were MYC/BCL2/BCL6 THL. All patient’s characteristics are listed in Table 1 and the composition of DHL and THL in two treatment programs is shown in Table 2. Among them, 20 (14.4%) were with CD5+ and 119 (85.6%) were with CD5– lymphoma, and 63 (45.3%) were treated with the DA-EPOCH-R regimen and 76 (54.7%) with R-CHOP. The median age was 57 years (18–81 years), and 90 (64.7%) patients had a grade III/IV Ann Arbor stage. Seventy-six patients with 3–5 IPI score accounted for 63.9%. Seventy-four (62.2%) patients had an elevated serum lactate dehydrogenase level. Eighty-seven (73.1%) patients had two or more extranodal sites involvement. Most clinical features at diagnosis were similar between each groups, including age, gender, serum LDH, clinical stage, IPI score and frequency of involvement of bone marrow, CNS involvement and extranodal sites (Table 1, P>0.05). In our study, primary CNS lymphoma was excluded, because the treatment of primary central lymphoma and primary extranodal lymphoma invading the CNSis different. There were 26 patients CNS involved before treatment started, including 7 patients with CD5+, 19 patients with CD5-. CNS involvement was detected by assessing the patient’s symptoms, and then we carried out MRI scans of the head and had CSF analysis pretreatment. Central invasion was confirmed based on cerebrospinal fluid flow and cytology. Patients with CNSinvolvement before treatment were treated with DA-R-EPOCH or R-CHOP combined with CNS intrathecal injection (methotrexate 12 mg, cytarabine 50 mg, dexamethasone 5 mg, 21 days per cycle). One clinical difference was that CD5+ DHL/THL-DLBCL patients showed relatively higher CNS involvement rate than CD5-DLBCL patients (35.0% versus 16.0%, P=0.042). Of the 139 patients, 11 patients (9.2%) received transplantation. Eight of 20 CD5+DLBCL patients received autologous stem cell transplant (SCT), five patients as consolidation at first CR and the other three patients as salvage treatment after 2 lines disease relapse. Of these eight patients, six relapsed after SCT and two patients died. Three of 119 CD5-DLBCL patients received allogeneic transplantation after 3 lines of therapy prior to SCT, two patients achieved PR prior to SCT, one had SD, those three patients relapsed after transplant and died of disease. For the 11 transplanted patients, median time to SCT failure calculated from the time of the first SCT to relapse or death was 5.4 months (95% CI: 2.9–10.1).
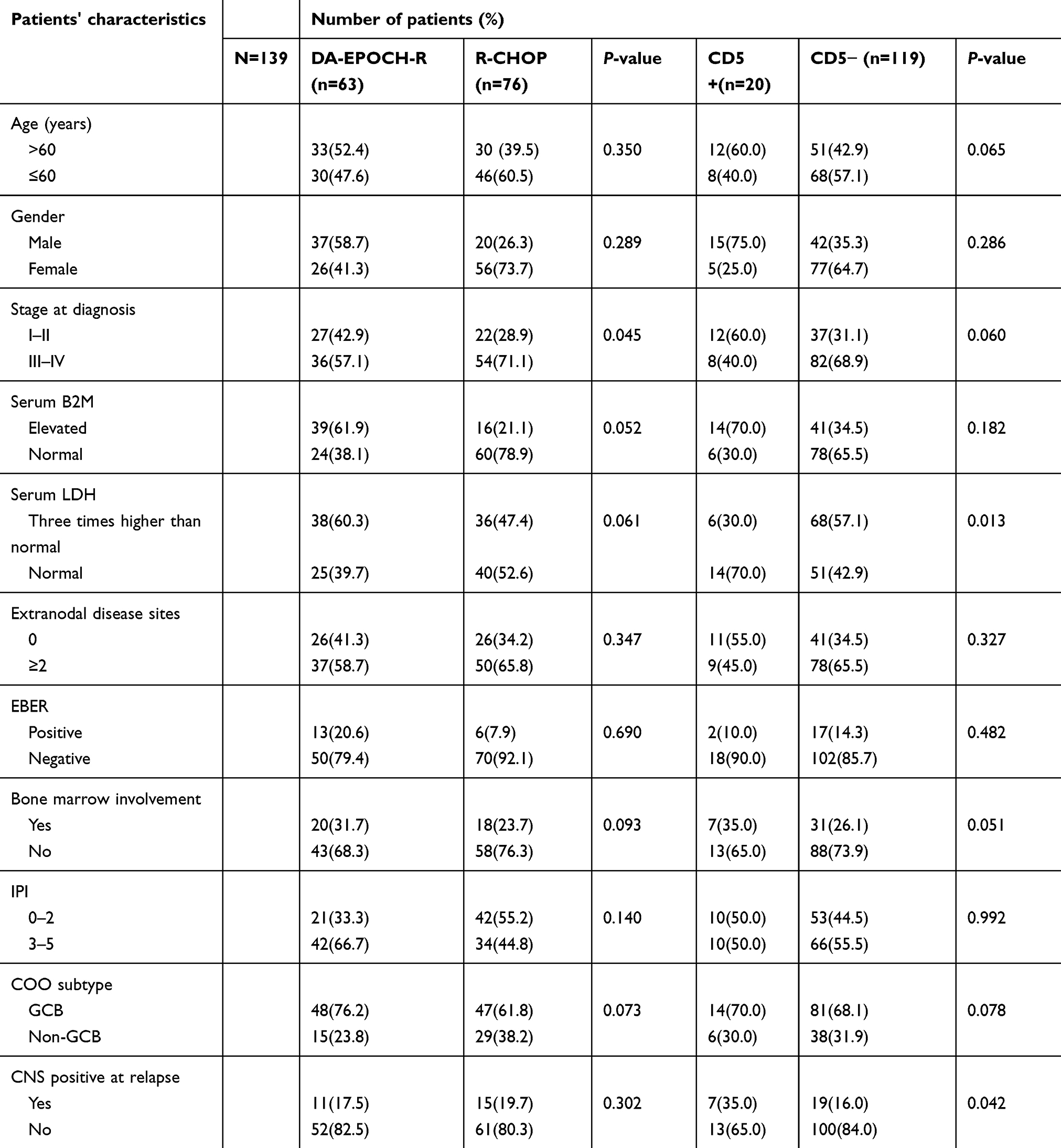 |
Table 1 Baseline clinical characteristics of patients |
 |
Table 2 The composition of DHL and THL in two regimens |
Short-term efficacy
The median chemotherapy cycle was 6 (range: 4–8); all 139 patients can be evaluated, including 90 cases CR (64.7%), 13 cases PR (9.4%), 16 cases SD (11.5%) and 20 cases PD (14.4%). The ORR was 74.1%. The chi-squared test was used to compare ORR between two chemotherapy groups, and the results showed that the ORR in DA-EPOCH-R group was significantly higher than in R-CHOP group (84.1% vs 65.8%, P<0.0001); similarly, the difference in ORR between CD5+ and CD5− was also significant (80.0% vs 63.8%, P=0.003). The results are shown in Table 3.
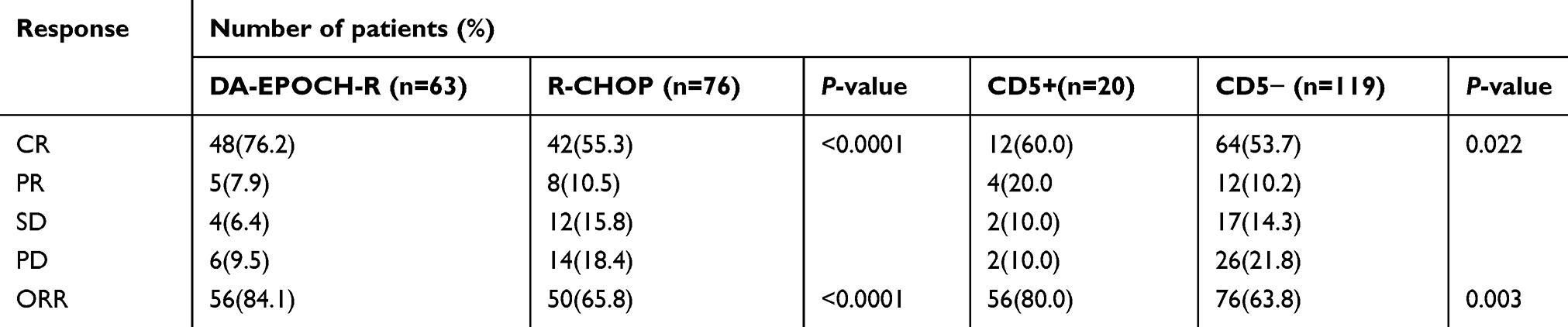 |
Table 3 Response rates of DA-EPOCH-R and R-CHOP regimen |
Long-term efficacy
The median follow-up time was 18 months (range: 4–39 months). PFS of CD5+ group was significantly worse than that of CD5− (28.1% vs 59.0%, P=0.028), while no significant difference was observed in OS (32.1% vs 59.9%, P=0.057) (Figure 1). At the end of the last follow-up time, 12 (19.0%) patients treated with DA-EPOCH-R regimen and 22 (29.0%) cases treated with R-CHOP died. Compared with the two regimens, the 2-year survival rate of DA-EPOCH-R group was significantly greater than that of R-CHOP (63.6% vs 45.4%, P=0.034 for PFS; 67.4% vs 47.8%, P=0.038 for OS) (Figure 2). Besides, CD5+ patients receiving DA-EPOCH-R had survival benefits compared with R-CHOP in PFS (85.7% vs 23.0%, P=0.029), but there was no statistical difference in OS (87.7% vs 34.4.0%, P=0.064) (Figure 3). However, in DA-EPOCH-R protocol, there was no significant difference between CD5+ DHL (MYC/BCl2 and MYC/BCL6) and triple-hit lymphoma (P=0.776 for PFS; P=0.728 for OS). Multivariate analysis showed that CD5+ treatment regimen and disease stage were independent prognostic factors.
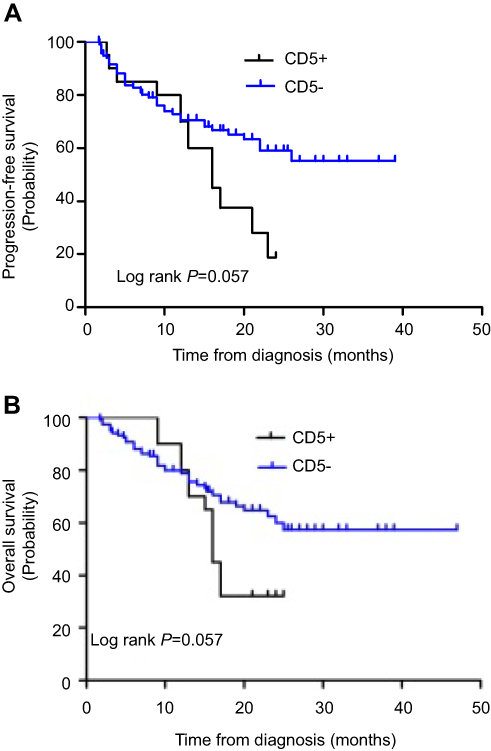 |
Figure 1 PFS (A) and OS (B) comparing in 20 cases CD5+ patients and 119 cases CD5- patients.Abbreviations: OS, overall survival; PFS, progression-free survival; DA-EPOCH-R, rituximab, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone. |
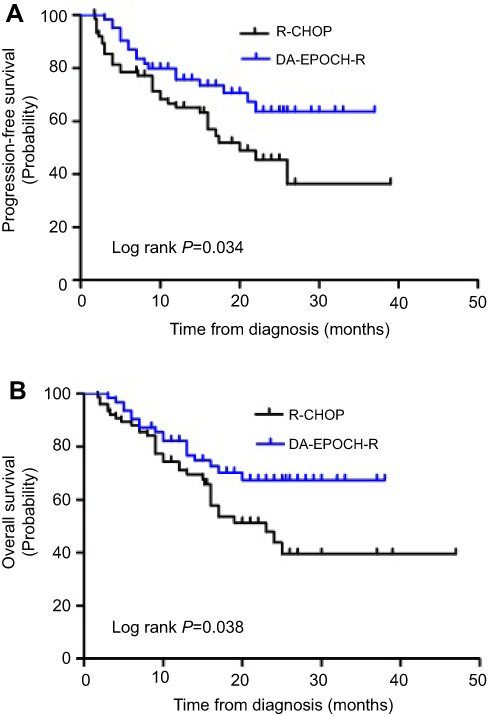 |
Figure 2 PFS (A) and OS (B) comparing DA-EPOCH-R and R-CHOP regimen in all patients.Abbreviations: OS, overall survival; PFS, progression-free survival; DA-EPOCH-R, rituximab, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone. |
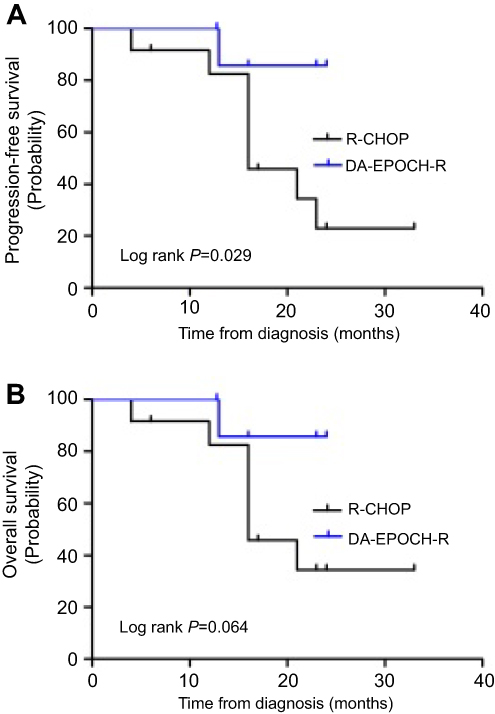 |
Figure 3 PFS (A) and OS (B) comparing in DA-EPOCH-R and R-CHOP regimen in 20 cases CD5+ patients.Abbreviations: OS, overall survival; PFS, progression-free survival; DA-EPOCH-R, rituximab, dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone. |
Univariate and multivariate analysis
Factors predictive of PFS and OS in univariate analysis were entered into multivariate analysis. Multivariate analysis showed that in DHL/THL-DLBCL patients with CD5+, the treatment regimen and disease stage were independent prognostic factors (Table 4). Patients treated with DA-EPOCH-R regimen had lower risk of death than traditional R-CHOP (PFS:HR 0.09; 95% CI: 0.03–2.74; P=0.017; OS:HR 0.82; 95% CI: 0.56–5.26; P=0.001). Besides, patients with CD5+ had higher risk of death than patients with CD5− (PFS: HR 1.32; 95% CI:0.09–13.35; P=0.011; OS: HR 1.40; 95% CI:0.00–10.89; P=0.009).
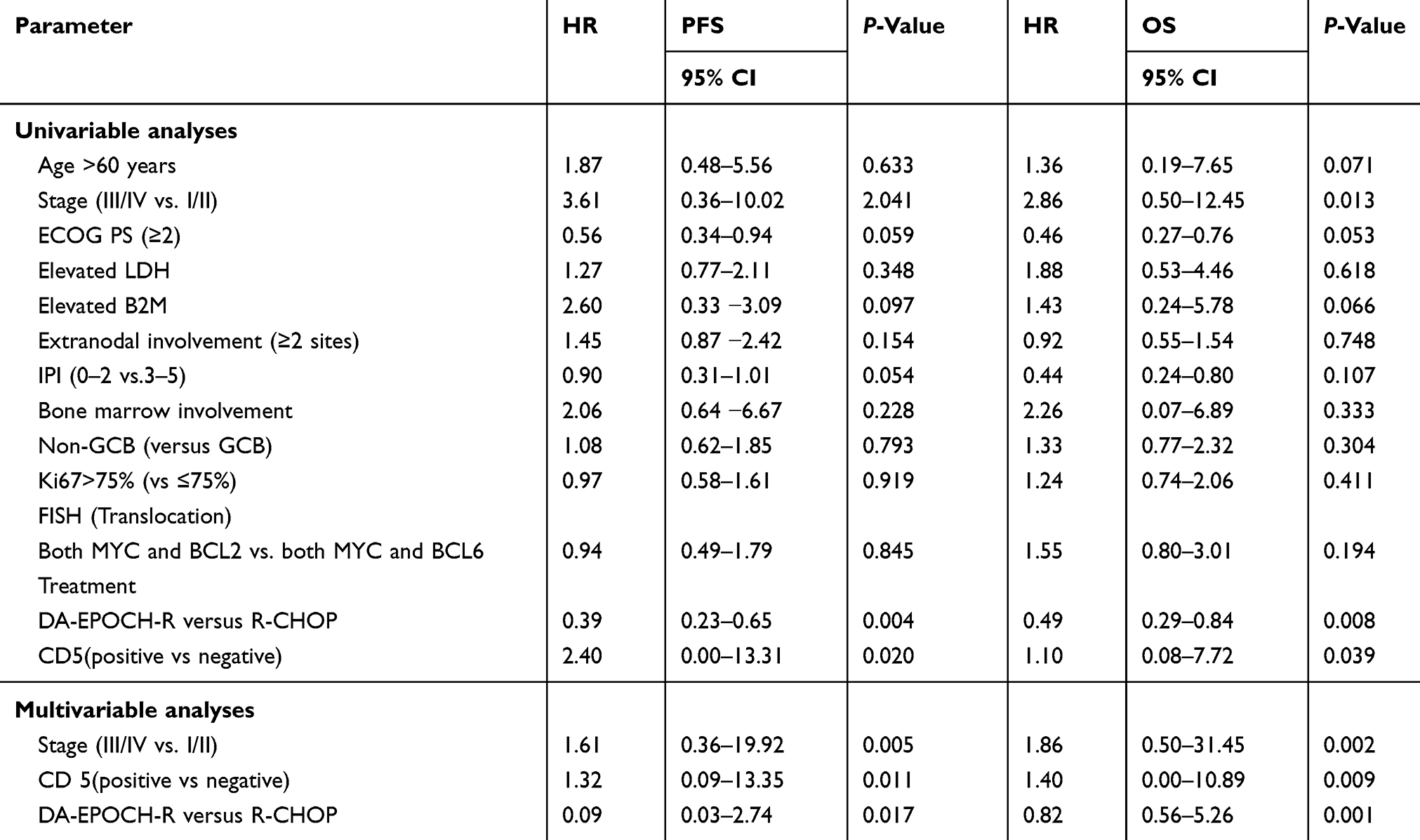 |
Table 4 Univariate and multivariate analysis for prognosis |
Adverse effects
ggssAdverse events (AEs) were evaluated in 139 patients, the most frequent AE was hematologic. The rate of grade 3/4 thrombocytopenia, anemia, leukopenia and neutropenia accounted for 36.7%, 38.1%, 25.8% and 28.1% of all patients, respectively. The non-hematological toxicity was mainly presented in 1/2 grade, including digestive tract toxicity, hepatic dysfunction, hypokalemia, cardiac toxicity, neurological toxicity and pulmonary infection. No chemotherapy-related deaths happened, and the grade 3/4 myelosuppression in DA-EPOCH-R was more frequent than in R-CHOP, but there was no statistical difference (P>0.05) (Table 5).
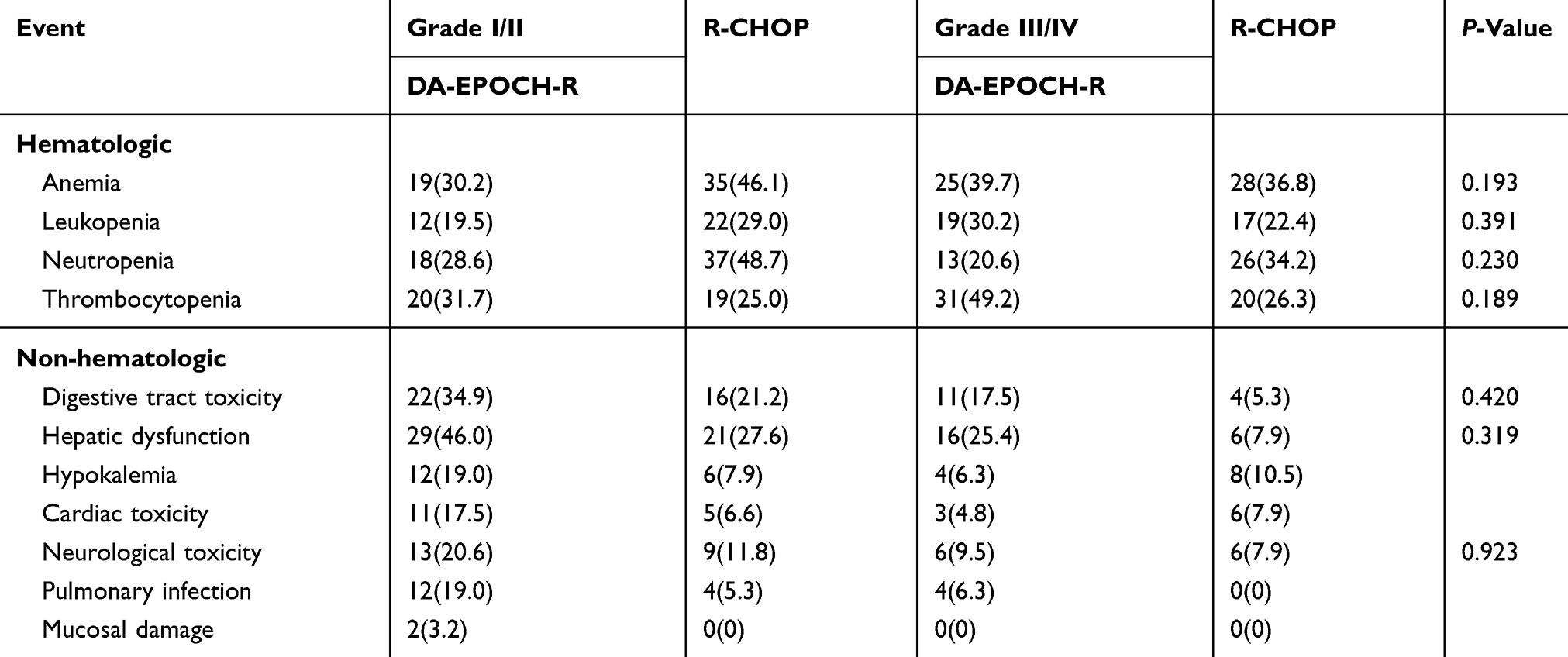 |
Table 5 Treatment-related adverse reaction between R-CHOP and DA-EPOCH-R regimen |
Discussion
CD5-positive DHL-DLBCL is a rare and malignant lymphoma subtype. There is no standard treatment regimes. The innovation of our study is that we compared the therapeutic effects of DA-EPOCH-R and R-CHOP in CD5+ DHL lymphoma. Our study reveals that CD5+ is a poor prognosis factor in patients with DHL-DLBCL, and DA-EPOCH-R can significantly improve the survival time of CD5+ DHL-DLBCL patients compared to the traditional R-CHOP treatment regimen.
CD5+ DLBCL is a rare and aggressive type disease, which accounts for 5–10% of all cases of DLBCL.13,17,19 CD5+ patients have particular characters, which include older age, elevated serum LDH level, advanced clinical stage, extranodal involvement and more frequent CNS relapse.28,29 Distinguishing CD5+ DLBCL from CD5-negative DLBCL is very important. At the molecular level, CD5+ DLBCL presents complex chromosomal aberrations and unmutated immunoglobulin heavy chain variable regions which may explain the aggressive course of CD5+ DLBCL.30,31 DHL is defined as both MYC and BCL2/BCL6 translocations or rearrangement. There are limited data about the frequency of MYC, BCL2 and BCL6 rearrangement or expression of MYC, BCL2 and BCL6 in CD5+ DLBCL cases, which are associated with poor prognosis in DLBCL patients.32,33 In our study, the ORR difference between CD5+ and CD5− was significant (80.0% vs 63.8%, P=0.003). PFS of CD5+ group was significantly worse than that of CD5− (28.1% vs 59.0%, P=0.028), while no significant difference was observed in OS (32.1% vs 59.9%, P=0.059). This may indicate that CD5-positive lymphoma has a poor prognosis.
Because of the insufficient evidence for the optimal treatment in CD5+ DLBCL in the era of rituximab, physicians choose treatments based on DLBCL therapy strategy.22,24,34 R-EPOCH had shown improved outcome (versus R-CHOP) in untreated patients with aggressive DLBCL, and 5-year time to progression and OS were 81% and 88%, respectively.10,21 Recently, a retrospective clinical study obtained only 12.3% of 130 cases CD 5+ DLBCL, and after the front-line R-EPOCH therapy, the median OS was significantly worse in CD5+ than CD5-negative patients (28.13 months vs not reached, pP=0.006), and they also concluded that CD5 expression and DHL were independent prognosis factors for OS in multivariate analysis; however, there were only two CD5+ DHL-DLBCL patients.35 Ennishi et al34 showed that CD5 expression was associated with poorer 2-year event-free survival (18% vs 73%) and OS (45% vs 91%, pP=0.01) when receiving rituximab plus CHOP therapy. Nitsu et al13 reported similar results, and the CR rate and PFS were lower in patients with CD5+ DLBCL than in CD5− DLBCL with the addition of rituximab chemotherapy. Taken together, no study focuses on the prognostic significance of CD5 expression in patients with DHL-DLBCL who received DA-EPOCH-R as front-line therapy. Our study analyzed the effects of R-CHOP and DA-EPOCH-R in the treatment of patients with DHL, and the 2-year survival rate of DA-EPOCH-R group was significantly greater than R-CHOP (63.6% vs 45.4%, P=0.034 for PFS; 67.4% vs 47.8%, P=0.038 for OS). PFS of CD5+ group was significantly worse than that of CD5− (28.1% vs 59.0%, P=0.028), while no significant difference was observed in OS (32.1% vs 59.9%, P=0.057). CD5+ patients receiving DA-EPOCH-R had survival benefits compared with R-CHOP in PFS (85.7% vs 23.0%, P=0.029), but there was no statistical difference in OS (87.7% vs 34.4.0%, P=0.064). To further explore the therapeutic effects of DA-EPOCH-R on CD5+ DHL and CD5+ THL, we separately analyzed the survival of patients with DHL and THL; however, there was no significant difference between CD5+ DHL (MYC/BCl2 and MYC/BCL6) and triple-hit lymphoma (P=0.776 for PFS; P=0.728 for OS). Considering the short observation period time and the lesser number of CD5+ DHL-DLBCL patients, some bias may exist in analysis, and further clinical studies are still needed to confirm these findings in the future.
In recent years, SCT has been shown to be an effective therapy compared with salvage chemotherapy for those chemo-sensitive DLBCL patients in the first relapse.36,37 CD5+ DLBCLs are a distinct subgroup of DLBCL with poor prognosis. However, there are few reports on the efficacy of salvage or consolidation transplantation in CD5-positive DLBCL patients. A recent retrospective study suggested that stem cell transplantation fails to salvage the majority of CD5-positive patients who received initial rituximab-containing chemotherapy.38 In our research, 11 patients underwent SCT, including eight autologous SCT in CD5+DLBCL patients and three allogeneic transplantations in CD5-DLBCL patients. Of these patients, six relapsed after SCT, two patients died and three patients died after transplant recurrence. For the 11 transplanted patients, median time to SCT failure calculated from time of the first SCT to relapse or death was 5.4 months. Our study suggests that hematopoietic stem cell transplantation has a limited therapeutic effect in patients with CD5+ or CD5− DLBCL, which is similar to other studies. However, due to the lesser number of patients with transplants in this study, we did not specifically compare the value of hematopoietic stem cell transplantation in CD5+ and CD5-DLBCL. It is necessary to further increase the sample size and conduct prospective clinical studies.
The administration of the DA-EPOCH-R regimen is a continuous intravenous infusion, and the adverse reactions are obvious. Our results showed that the grade 3/4 myelosuppression in DA-EPOCH-R was higher than in R-CHOP, but there was no statistical difference (P>0.05). These AEs can be dealt with well and returned to normal quickly after given symptomatic treatment, and there were no chemotherapy-related deaths.
Conclusion
Our retrospective research indicates that CD5 expression in DHL-DLBCL is associated with poorer prognosis. Compared with traditional R-CHOP chemotherapy, DA-EPOCH-R is an effective and well-tolerated regimen for CD5+DHL-DLBCL, and it is expected to be the first-line treatment for CD5+ DHL-DLBCL. Besides, evaluation of CD5 expression in DLBCL at the beginning of diagnosis contributes to make stratification. However, due to the potential limitations of single center, small sample, retrospective analysis, it still needs further prospective, multicenter and large-scale studies to conform those results.
Acknowledgment
We are indebted to the Lymphoma Diagnosis and Treatment Cancer Center of Henan Province for providing assistance. We also thank all the patients for allowing us to analyze their data. Fangwen Zhang and Ling Li are co-first authors for this study. This study was supported by the National Natural Science Foundation of China (grant number 81570204).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jain P, Fayad LE, Rosenwald A, et al. Recent advances in de novo CD5+ diffuse large B cell lymphoma. Am J Hematol. 2013;88(9):798–802. doi:10.1002/ajh.23467
2. Yamaguchi M, Seto M, Okamoto M, et al. De novo CD5+ diffuse large B-cell lymphoma: a clinicopathologic study of 109 patients. Blood. 2002;99(3):815–821. doi:10.1182/blood.V99.3.815
3. Lenz G, Wright GW, Tolga Emre NC, et al. Molecular subtypes of diffuse large B-cell lymphoma arise by distinct genetic pathways. Proc Natl Acad Sci. 2008;105(36):13520–13525. doi:10.1073/pnas.0804295105
4. Vose JM. Relapsed diffuse large B-cell lymphoma: clinical utility of cell of origin. J Clin Oncol. 2011;29(31):4065–4066. doi:10.1200/JCO.2011.37.5733
5. Martelli M, Ferreri AJ, Agostinelli C, et al. Diffuse large B-cell lymphoma. Crit Rev Oncol Hematol. 2013;87(2):146–171. doi:10.1016/j.critrevonc.2012.12.009
6. Smith A, Howell D, Crouch S, et al. Cohort profile: the Haematological Malignancy Research Network (HMRN): a UK population-based patient cohort. Int J Epidemiol. 2018;47(3):700. doi:10.1093/ije/dyx190
7. Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375–2390. doi:10.1182/blood-2016-01-643569
8. Gang AO, Strř C, Pedersen M, et al. R-CHOEP-14 improves overall survival in young high-risk patients with diffuse large B-cell lymphoma compared with R-CHOP-14. A population-based investigation from the Danish Lymphoma Group. Ann Oncol. 2012;23:147–153. doi:10.1093/annonc/mdr058
9. Wilson WH, Grossbard ML, Pittaluga S, et al. Dose-adjusted EPOCH chemotherapy for untreated large B-cell lymphomas: a pharmacodynamic approach with high efficacy. Blood. 2002;99:2685–2693. doi:10.1182/blood.v99.8.2685
10. Garcia-Suarez J, Banas H, Arribas I, et al. Dose-adjusted EPOCH plus rituximab is an effective regimen in patients with poor-prognostic untreated diffuse large B-cell lymphoma: results from a prospective observational study. Br J Haematol. 2007;136(2):276–285. doi:10.1111/j.1365-2141.2006.06438.x
11. Howlett C, Snedecor SJ, Landsburg DJ, et al. Front-line, dose-escalated immunochemotherapy is associated with a significant progression-free survival advantage in patients with double-hit lymphomas: a systematic review and meta-analysis. Br J Haematol. 2015;170:504–514. doi:10.1111/bjh.13463
12. Yamaguchi M, Nakamura N, Suzuki R, et al. De novo CD5+ diffuse large B-cell lymphoma: results of a detailed clinicopathological review in 120 patients. Haematologica. 2008;93(8):1195–1202. doi:10.3324/haematol.12810
13. Niitsu N, Okamoto M, Tamaru JI, et al. Clinocopathologic characteristics and treatment outcome of the addition of rituximab to chemotherapy for CD5-positive in comparison with CD5-negative diffuse large B-cell lymphoma. Ann Oncol. 2010;21:2069–2074. doi:10.1093/annonc/mdq057
14. Armitage JO. How I treat patients with diffuse large B-cell lymphoma. Blood. 2007;110(1):29–36. doi:10.1182/blood-2007-01-041871
15. Sehn LH, Gascoyne RD. Diffuse large B-cell lymphoma: optimizing outcome in the context of clinical and biologic heterogeneity. Blood. 2015;125(1):22–32. doi:10.1182/blood-2014-07-591040
16. Alizadeh AA, Eisen MB, Davis RE, et al. Distinct type of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403(6769):503–511. doi:10.1038/35000501
17. Miyazaki K, Yamaguchi M, Suzuki R, et al. CD5-positive diffuse large B-cell lymphoma: a retrospective study in 337 patients treated by chemotherapy with or without rituximab. Ann Oncol. 2011;22(7):1601–1607. doi:10.1093/annonc/mdq627
18. Yamaguchi M, Ohno T, Oka K, et al. De novo CD5-positive diffuse large B-cell lymphoma: clinical characteristics and therapeutic outcome. Br J Haematol. 1999;105(4):1133–1139. doi:10.1046/j.1365-2141.1999.01513.x
19. Hyo R, Tomita N, Takeuchi K, et al. The therapeutic effect of rituximab on CD5-positive and CD5-negative diffuse large B-cell lymphoma. Hematol Oncol. 2010;28(1):27–32. doi:10.1002/hon.896
20. Westin J, McLaughlin P. De novo CD5+ diffuse large B-cell lymphoma: a distinct subset with adverse features, poor failure-free survival and outcome with conventional therapy. Leuk Lymphoma. 2010;51(1):161–163. doi:10.3109/10428190903324244
21. Wilson WH, Jung SH, Porcu P, et al. A Cancer and Leukemia Group B multi-center study of DA-EPOCH-rituximab in untreated diffuse large B-cell lymphoma with analysis of outcome by molecular subtype. Haematologica. 2012;97(5):758–765. doi:10.3324/haematol.2011.056531
22. Garcia-Suarez J, Flores E, Callejas M, et al. Two-weekly dose-adjusted (DA)-EPOCH-like chemotherapy with high-dose dexamethasone plus rituximab (DA-EDOCH14-R) in poor-prognostic untreated diffuse large B-cell lymphoma. Br J Haematol. 2013;160(4):510–514. doi:10.1111/bjh.12144
23. Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103(1):275–282. doi:10.1182/blood-2003-05-1545
24. Visco C, Li Y, Xu-Monette ZY, et al. Comprehensive gene expression profiling and immunohistochemical studies support application of immunophenotypic algorithm for molecular subtype classification in diffuse large B-cell lymphoma: a report from the International DLBCL Rituximab-CHOP Consortium Program Study. Leukemia. 2012;26(9):2103–2113. doi:10.1038/leu.2012.83
25. Miller AB, Hoogstraten B, Staquet M, et al. Reporting results of cancer treatment. Cancer. 1981;47(1):207–214. doi:10.1002/(ISSN)1097-0142
26. Cheson BD, Horning SJ, Coiffier B, et al. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI sponsored international working group. J Clin Oncol. 1999;17(4):1244. doi:10.1200/JCO.1999.17.4.1244
27. Cheson BD, Pfistner B, Juweid ME, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25(5):579–586. doi:10.1200/JCO.2006.09.2403
28. Matolcsy A, Chadburn A, Knowles DM. De novo CD5-positive and Richter’s syndrome-associated diffuse large B cell lymphomas are genotypically distinct. Am J Pathol. 1995;147(1):207–216.
29. Harada S, Suzuki R, Uehira K, et al. Molecular and immunological dissection of diffuse large B cell lymphoma: CD5+, and CD5- with CD10+ groups may constitute clinically relevant subtypes. Leukemia. 1999;13(9):1441–1447.
30. Horn H, Ziepert M, Becher C, et al. MYC status in concert with BCL2 and BCL6 expression predicts outcome in diffuse large B-cell lymphoma. Blood. 2013;121(12):2253–2263. doi:10.1182/blood-2012-06-435842
31. Aukema SM, Kreuz M, Kohler CW, et al. Biological characterization of adult MYC-translocation-positive mature B-cell lymphomas other than molecular Burkitt lymphoma. Haematologica. 2014;99(4):726–735. doi:10.3324/haematol.2013.091827
32. Li S, Weiss VL, Wang XJ, et al. High-grade B-cell lymphoma with MYC rearrangement and without BCL2 and BCL6 rearrangements is associated with high P53 expression and a poor prognosis. Am J Surg Pathol. 2016;40(2):253–261. doi:10.1097/PAS.0000000000000542
33. Green TM, Young KH, Visco C, et al. Immunohistochemical double-hit score is a strong predictor of outcome in patients with diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol. 2012;30(28):3460–3467. doi:10.1200/JCO.2011.41.4342
34. Ennishi D, Takeuchi K, Yokoyama M, et al. CD5 expression is potentially predictive of poor outcome among biomarkers in patients with diffuse large B-cell lymphoma receiving rituximab plus CHOP therapy. Annals of Oncology: Official Journal of the European Society for Medical Oncology/ESMO. 2008;19(11):1921–1926.
35. Thakral B, Edeiros LJ, Desai P, et al. Prognostic impact of CD5 expression in diffuse large B-cell lymphoma in patients treated with rituximab-EPOCH. Eur J Haematol. 2017;98(4):415–421. doi:10.1111/ejh.12847
36. Gisselbrecht C, Glass B, Mounier N, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(27):4184–4190. doi:10.1200/JCO.2010.28.1618
37. Stiff PJ, Unger JM, Cook JR, et al. Autologous transplantation as consolidation for aggressive Non-Hodgkin’s lymphoma. N Engl J Med. 2013;369(18):1681–1690. doi:10.1056/NEJMoa1301077
38. Alinari L, Gru A, Quinion C, et al. De novo CD5+ diffuse large B-cell lymphoma: adverse outcomes with and without stem cell transplantation in a large, multi-center, rituximab treated cohort. Am J Hematol. 2016;91(4):395–399. doi:10.1002/ajh.24299
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.