")
Back to Journals » Cancer Management and Research » Volume 15
Primary Breast Burkitt Lymphoma. A Case Report of a 16-Year-Old Female with a Rapidly Growing Unilateral Breast Mass
Authors Mitala Y , Ssenkumba B , Nabulya R , Kitenda FN, Tumwesigye H, Birungi A, Dratu Chau R, Mushabe B, Baker N, Atwine R
Received 20 July 2023
Accepted for publication 21 September 2023
Published 26 September 2023 Volume 2023:15 Pages 1047—1052
DOI https://doi.org/10.2147/CMAR.S426780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Yekosani Mitala,1 Brian Ssenkumba,1 Rita Nabulya,1 Francis Nsumba Kitenda,1 Habert Tumwesigye,1 Abraham Birungi,1 Richard Dratu Chau,1 Branchard Mushabe,2 Nichole Baker,3 Raymond Atwine1
1Department of Pathology, Mbarara University of Science and Technology, Mbarara City, Uganda; 2Department of Pediatrics, Mbarara Regional Referral Hospital, Mbarara City, Uganda; 3Department of Public Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
Correspondence: Yekosani Mitala, Email [email protected]
Introduction: Primary breast Burkitt lymphoma is extremely rare. Commonly endemic Burkitt lymphoma presents with abdominal, jaw, periorbital, or genitourinary mass.
Case Presentation: We report a case of a 16-year-old girl with rapidly enlarging left breast swelling associated with evening fevers. This was later confirmed to be stage 1 primary breast Burkitt lymphoma involving the left breast. This represents the first described case of primary breast endemic Burkitt lymphoma in Uganda. She was started on chemotherapy and exhibited an impressive response to the drugs.
Conclusion: This case raises awareness of rare sites for endemic Burkitt lymphoma in Uganda. Accurately diagnosing this case was of great importance since it determined the treatment modality (mastectomy or not) which would have an everlasting impact on her life.
Keywords: primary breast Burkitt lymphoma, Uganda, a case report
Introduction
Burkitt lymphoma (BL) is a highly aggressive subtype of Non-Hodgkin Lymphoma (NHL) originally identified in Uganda as a sarcoma by Dr Dennis Burkitt.1 This rapidly growing tumor has shown significant responsiveness to chemotherapy and is considered curable. The distinct exhibits 3 distinct forms: sporadic, immunodeficiency associated, and endemic. Endemic Burkitt Lymphoma (eBL) is the most prevalent form, primarily observed in sub-Saharan Africa, where it accounts for up to 75% of childhood cancers in certain countries. eBL is strongly associated with plasmodium falciparum and Epstein Barr Virus (EBV) infection and geographical location.2 In Uganda, BL is frequently diagnosed in children and commonly presents with swelling in the abdomen, jaw, periorbital region, or genitourinary area.3,4 There is no clear local data about BL, although the available unpublished data reveals the disease is common in children below 10 years of age. However, primary Burkitt Lymphoma of the breast is an exceptionally rare occurrence. To the best of our knowledge, this might be the second documented case of primary breast BL in Uganda and the first case in a teenage female from Uganda.
Case Presentation
A 16-year-old female presented with a three-week history of a progressively enlarging and painful mass in her left breast, accompanied by low-grade fevers that responded to paracetamol. The patient tested negative for Human Immunodeficiency Virus (HIV) and exhibited normal vital signs and oxygen saturation levels. The left breast was grossly swollen with shiny skin, non-tender, and was of normal temperature. There were vaguely nodular soft masses with ill-defined margins and no ipsilateral lymph node swelling. Ultrasonography revealed multiple regular hypoechoic masses with no speculated edges commonly seen in breast carcinoma and no calcifications (see Figure 1). Consent was sought from her and the mother for a trucut biopsy to be done.
 |
Figure 1 (A) shows a diffusely swollen left breast with shiny skin (blue arrow). (B and C) are ultra-sonographic images of the breast showing multiple large hypoechoic masses (blue stars) (4.95cm by 4.96cm and 5.82 cm) respectively, regularly shaped with no calcifications. (D) shows a touch imprint with medium-sized cells, coarse chromatin, and occasional tingible body macrophages (see black arrow). |
Touch imprints of the cores were suggestive of BL (see Figure 1). H&E stained histology sections revealed a monomorphic population of moderately sized lymphoid cells with a high N:C ratio, frequent apoptotic bodies, frequent mitoses, and occasional tingible body macrophages giving it a starry sky appearance (see Figure 2). A diagnosis of Burkitt lymphoma was suggested and confirmed by immunohistochemistry. On IHC, the tumor was positive for CD45, and c-MYC. The proliferative index (ki67) was 100%. Tdt, BCL2, and CD3 were dead negative (see Figure 3). Diffuse large B cell lymphoma (DLBCL) was a differential. Other tests that could have been done like EBV staining, and cytogenetics to determine the presence of characteristic translocations were not available in our setting.
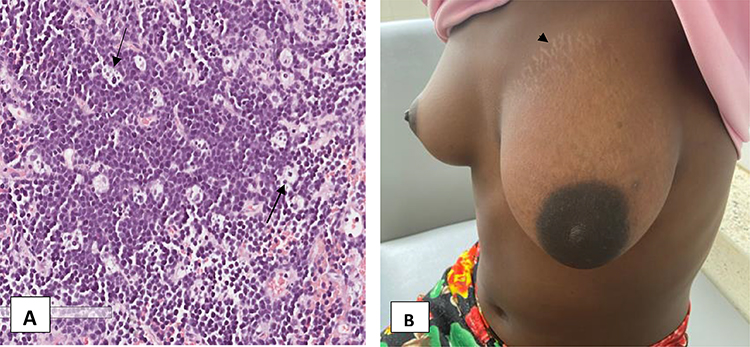 |
Figure 2 (A) (x20) shows an H&E stained section of the tumor with medium-sized cells, a high N: C ratio, and numerous tingible body macrophages (black arrows) giving it a characteristic starry sky. (B) shows a reduction in the size of the breast a week after her first cycle of chemotherapy with striae seen on the upper border of the breast (black arrowhead). |
 |
Figure 3 IHC stains showing positive CD45, Pax5, and c-MYC ((A–C) respectively) (x20). (D) shows 100% expression of Ki67. Panels E and F show negative Tdt and CD3 respectively. |
She was admitted to the pediatric oncology ward where a chest x-ray, abdominal ultrasound scan, CBC, bone marrow, and CSF examination were all unremarkable. A diagnosis of stage 1 primary breast BL was confirmed according to the International Pediatric Non-Hodgkin Lymphoma Staging system (IPNHLSS). Chemotherapy was initiated; methotrexate 1400mg, vincristine 2mg, doxorubicin 74.5mg, cyclophosphamide 1788mg, prednisolone 22mg, intrathecal methotrexate 15mg, intrathecal hydrocortisone 15mg, intrathecal cytarabine 70mg. The next day, she complained of vomiting. She was put on ondansetron, intravenous fluids, and allopurinol for tumor lysis syndrome prevention.
A week later, she was reviewed and was showing a good response to chemotherapy. The tumor had significantly shrunk, the skin was no longer shiny (see Figure 2B) and she was much happier. She was discharged home and was to be reviewed every month at the oncology clinic and also have her monthly cycle of chemotherapy to a total of 6 cycles. Due to the side effects of chemotherapy like hair loss, vomiting, and body weakness, the girl declined chemotherapy after the third cycle. However, with repeated engagements with the counselor and the nurse in charge of the Oncology clinic, she was convinced and is on course to completion timeline for these events is summarized in the timeline figure attached.
Consent
The mother consented and allowed us to use her daughters’ specimens for research and publication of this case report and other additional studies in which the daughters’ specimens might be potential participants. The consent also authorized us to publish images accompanying this case. This can be provided if needed.
Discussion
Primary breast lymphoma (PBL) is defined by the presence of lymphoma in the breast in the absence of a previously diagnosed lymphoma, and no concurrent metastatic disease. It is a rare occurrence because of the scarcity of lymphoid tissue in the breast. Breast in most cases is only secondarily involved by lymphoma, with the primary located elsewhere. PBL represents only about 0.5% of primary breast tumors among adults, most of which are diffuse large B-cell lymphoma (DLBCL), followed by follicular lymphoma, mucosal-associated lymphoid tumors, and BL.5–7 Primary breast BL (PBBL) is even a much rarer disease,8 representing only about 10.3% of all PBL and its occurrence in children as a breast mass is exceptionally rare.9 BL is the commonest childhood cancer at Uganda Cancer Institute (UCI) in Kampala, representing up to 28% of all pediatric cancers. Local data for Southwestern Uganda is not readily available despite having a regional satellite cancer treatment center managed by UCI. Commonly, BL cases in Uganda present with abdominal masses, jaw masses, or masses in the gonads according to a recent study conducted at UCI. No other sites were reported in this study.3 In Africa, there is only 4 reported case of PBBL, 1 from Guinea in an HIV infected 30 years old woman, and 3 from Ivory Coast.10,11 This case will represent the first case of PBBL from Uganda. Compared to other sites of extranodal NHL, it has been revealed that PBL tends to be more aggressive and has a much poor outcome6 although this is disputed by some authors.12
BL in our setting has been attributed to infections with the EBV virus, but research has revealed a strong association with malaria infections. Immunosuppressive conditions like HIV/AIDS also contribute a great deal to most NHL cases, however, for this case, no risk factor could be elicited except being a resident in a malaria-endemic region.
Clinically, PBL also tends to be in much younger people who are almost always females with a median age of 60–65 years, compared to secondary breast lymphoma that presents between 60 and 70 years.13 In our case, the patient was even much younger at 16 years probably because BL is more likely to affect younger people than other forms of NHL for which the above age may represent. Although PBL may present like breast carcinoma with B-symptoms, breast mass or masses, and swelling, it rarely causes nipple retraction, discharge, or peau d’orange. These are seen in high-grade lymphomas with diffuse parenchymal involvement. Our patient presented with fevers and painful diffuse left breast swelling which was non-tender. An ultrasound scan revealed multiple large hypoechoic masses with mixed echogenicity, regularly shaped, with indistinct margins, and no calcifications (see Figure 1B and C above). This is similar to ultrasound findings reported by Raj et al and Li et al.5,6 Our patient had neither axillary nor supraclavicular lymph node swellings, which is seen in up to about 40% of patients with breast lymphoma.
To diagnose PBL, a specimen with close anatomical proximity of breast parenchyma and lymphomatous infiltrate must be obtained, there should be no prior diagnosis of extramammary lymphoma, and there should be no evidence of concurrent widespread disease. Ipsilateral axillary lymphadenopathy may be present. The above criteria were suggested in 1972 by Wiseman and Liao.9 Accordingly, the criteria were fulfilled in this case report. There was no prior diagnosis of extramammary BL, and neither the tests nor the physical examination suggested the presence of a concurrently disseminated disease. To facilitate early diagnosis and commencement of treatment, we did a touch imprint, which suggested Burkitt lymphoma. This was necessary to avoid undue surgical interventions that had already been suggested to her mother at a peripheral health center.
Although the literature denotes that PBL is quite aggressive with a dismal prognosis, our case deviates from that notion. As expected in BL cases, our patient showed a tremendous response to chemotherapy with the tumor shrinking to almost half its size after the first cycle of chemotherapy. Other treatment options that have been suggested for PBL include mastectomy and radiotherapy although research has revealed that mastectomy has no benefit in managing PBL.14,15 The girl is still on chemotherapy and currently doing well. The mass has completely disappeared (see Figure 4), and she is back to school and living a normal life.
 |
Figure 4 Left breast is now almost equal in size to the right breast during the third cycle of chemotherapy. |
Limitations
It was impossible to determine the presence or absence of Epstein Barr Virus in our case because we lack the antibody (EBER) for its detection.
Conclusion
Primary breast Burkitt lymphoma is a rare occurrence but not exceptional. Early and accurate diagnosis is critical due to its impact on the treatment modality. Based on the rapid reduction in the size of the tumor seen in this case, chemotherapy is equally effective in treating primary breast Burkitt lymphoma as it is in the treatment of Burkitt lymphoma from other sites like the jaw with no need for mastectomy. This case should also alert clinicians of other non-infectious conditions that may mimic a breast abscess for which antibiotics and surgical management are not required as well as the fact that BL can occur at unusual sites other than the jaw, abdomen, and gonads which can easily be missed.
Patient Perspective
When the mother noticed that her daughters’ breast was enlarging, she initially thought she was pregnant but the daughter denied the allegation. The mother then sought advice from the elders in the community who told her it was an abscess and it needed to be burnt. Traditionally, this is done with red hot metal spokes pushed through the abscess and draining the pus. The mother declined the procedure and when she visited a local private clinic, the health worker advised her to have the daughter’s breast cut off, which she again declined. She then decided to come to Mbarara Regional Referral Hospital because she was told the hospital treats cancer patients.
After receiving the results and being educated about the prognosis, she was happy because her daughter was going to be normal once more. When the daughter started chemotherapy and the mass reduced, the mother was more than thankful. The girl was excited that she would be able to go back to school. Despite the renewed hope, the situation changed when she started losing her hair and experiencing nausea and vomiting. After completing three cycles, and the mass was no longer palpable, the girl declined chemotherapy and missed the subsequent appointment. With repeated counseling and patient education, she was convinced to continue care and she is on course to completing her remaining two cycles.
Data Sharing Statement
The data and materials of this case report are available from the corresponding author upon request after approval from the Pathology Department and Mbarara Regional Referral Hospital.
Ethical Clearance
Institutional approval was not necessary, although we sought site clearance from the head of the pathology department and the laboratory chief.
Acknowledgment
The patient and her family are acknowledged for allowing us to take pictures of their valuable body parts and to use their specimen for research purposes. We also acknowledge the pathology department of Mbarara University and the Oncology Clinic at Mbarara regional referral hospital for the caring for sick.
Funding
This project was not funded and is not intended for profit-making purposes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Walusansa V, Okuku F, Orem J. Burkitt lymphoma in Uganda, the legacy of D enis B urkitt and an update on the disease status. Br J Haematol. 2012;156(6):757–760.
2. Redmond LS, Ogwang MD, Kerchan P, et al. Endemic Burkitt lymphoma: a complication of asymptomatic malaria in sub-Saharan Africa based on published literature and primary data from Uganda, Tanzania, and Kenya. Malar J. 2020;19:1–14. doi:10.1186/s12936-020-03312-7
3. Mutyaba I, Wabinga HR, Orem J, Casper C, Phipps W. Presentation and outcomes of childhood cancer patients at Uganda Cancer Institute. Glob Pediatr Health. 2019;6:2333794X19849749. doi:10.1177/2333794X19849749
4. Kalungi S. Burkitt Lymphoma in Uganda. A Study of Some Biological and Epidemiological Aspects of Endemic Burkitt Lymphoma. The University of Bergen; 2011.
5. Li Y, Zhang Y, Wang W, Wei C, Zhao D, Zhang W. A comprehensive model for diagnosis of primary breast lymphoma differentiated from breast cancer and prognosis evaluation of surgical treatment. Front Oncol. 2022;2022:12.
6. Raj SD, Shurafa M, Shah Z, Raj KM, Fishman MD, Dialani VM. Primary and secondary breast lymphoma: clinical, pathologic, and multimodality imaging review. Radiographics. 2019;39(3):610–625. doi:10.1148/rg.2019180097
7. Duncan VE, Reddy VV, Jhala NC, Chhieng DC, Jhala DN. Non-Hodgkin’s lymphoma of the breast: a review of 18 primary and secondary cases. Ann Diagn Pathol. 2006;10(3):144–148. doi:10.1016/j.anndiagpath.2005.09.018
8. Asghari R, Abbasi A, Mojdeganlou H, Farrokhi Y, Mahmoodzadeh L. Primary Burkitt lymphoma of breast presented by bilateral breast enlargement. Immunopathol Persa. 2022. doi:10.34172/ipp.2022.29283
9. Restivo GA, Pillon M, Mussolin L, et al. Primary breast lymphoma of childhood: a case report and review of the literature. BMC Pediatr. 2021;21:1–6. doi:10.1186/s12887-021-03002-6
10. Traoré B, Fondrevelle M-E, Condé M, et al. Primary Breast Burkitt’s Lymphoma in an HIV-Infected Woman. Case Rep Med. 2015;2015:1–4. doi:10.1155/2015/792041
11. Kouassi Gustave K, Emeraude ND, Aissata T, et al. Localisations exceptionnelles du Lymphome endémique de Burkitt (à propos de 21 cas vus en Côte d’Ivoire) [Exceptional locations of endemic Burkitt lymphoma (about 21 cases seen in Ivory Coast)]. Cahiers D’études Et de Recherches Francophones. 2010;20(2):69–72.
12. Moura C, Leite MI, Parreira R, Medeiros A. Primary breast lymphoma. J Surg Case Rep. 2020;2020(1):rjz405. doi:10.1093/jscr/rjz405
13. Yoneyama K, Nakagawa M, Hara A. Primary lymphoma of the breast: a case report and review of the literature. Radiol Case Rep. 2021;16(1):55–61. doi:10.1016/j.radcr.2020.10.039
14. Mouna B, Saber B, Tijani EH, Amina T, Hassan E. Primary malignant non-Hodgkin’s lymphoma of the breast: a study of seven cases and literature review. World J Surg Oncol. 2012;10(1):1–6. doi:10.1186/1477-7819-10-1
15. Radkani P, Joshi D, Paramo JC, Mesko TW. Primary breast lymphoma: 30 years of experience with diagnosis and treatment at a single medical center. JAMA Surg. 2014;149(1):91–93. doi:10.1001/jamasurg.2013.2283
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.