Back to Journals » Journal of Pain Research » Volume 16
Prevalence, Patterns, and Associated Factors for Musculoskeletal Disorders Among the Healthcare Workers of Northern Saudi Arabia: A Multicenter Cross-Sectional Study
Authors Alruwaili SH ![]() , Thirunavukkarasu A, Alanazi RM, Alsharari AY, Alruwaili DK, Alenzi HA, Alruwaili AN, Alruwaili GQ
, Thirunavukkarasu A, Alanazi RM, Alsharari AY, Alruwaili DK, Alenzi HA, Alruwaili AN, Alruwaili GQ
Received 10 April 2023
Accepted for publication 27 October 2023
Published 7 November 2023 Volume 2023:16 Pages 3735—3746
DOI https://doi.org/10.2147/JPR.S415919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Sager Holyl Alruwaili,1 Ashokkumar Thirunavukkarasu,2 Raghdah Muharib Alanazi,3 Amani Yasr Alsharari,3 Danah Khalid Alruwaili,3 Hanaa Abdalkreem Alenzi,3 Aryam Nafea Alruwaili,3 Ghadah Qasem Alruwaili3
1Department of Surgery, Division of Orthopedic Surgery, College of Medicine, Jouf University, Sakaka, Al-Jouf, Saudi Arabia; 2Department of Family and Community Medicine, College of Medicine, Jouf University, Sakaka, Al-Jouf, Saudi Arabia; 3Medical Student, College of Medicine, Jouf University, Sakaka, Al-Jouf, Saudi Arabia
Correspondence: Sager Holyl Alruwaili, Department of Surgery, Division of Orthopedic Surgery, College of Medicine, Jouf University, Sakaka, Al-Jouf, Saudi Arabia, Tel +966- 591112218, Email [email protected]
Background: Musculoskeletal disorders (MSDs) have emerged as a pressing concern among healthcare workers (HCWs), gaining significant attention, particularly in the aftermath of the COVID-19 pandemic. This study evaluated the prevalence, pattern, and associated factors for MSDs among HCWs in northern Saudi Arabia.
Participants and Methods: Employing a cross-sectional study design, the standardized Nordic Musculoskeletal Questionnaire (NMQ) was used to collect data from participants. Systematic sampling method was employed to select 384 HCWs from diverse healthcare settings. Multivariate logistic regression analysis was conducted to identify factors associated with MSDs.
Results: Among the participants, 72.4% reported one or more NMQ-listed MSDs. The most commonly affected body regions were the neck, shoulder, and lower back. MSDs showed significant associations with physical activity (adjusted odds ratio [AOR]= 0.72, 95% confidence interval [CI] = 0.53– 0.93, p = 0.024), obesity status (AOR = 3.08, 95% CI = 1.56– 4.71, p = 0.003), and ergonomic training (AOR = 0.38, 95% CI = 0.23– 0.55, p < 0.001).
Conclusion: Implementing preplacement and periodic ergonomic training for HCWs is recommended. This proactive measure holds the potential to alleviate MSD-related discomfort, reduce sickness absenteeism, and enhance overall productivity. Future longitudinal studies across different regions of Saudi Arabia are essential to establish causal links between risk factors and MSDs.
Keywords: healthcare workers, neck pain, ergonomics, Saudi Arabia, musculoskeletal disorders
Introduction
Musculoskeletal disorders (MSDs) encompass disorders or injuries affecting the muscles, joints, cartilages, nerves, and tendons, encompassing over 150 conditions related to the locomotor system.1,2 According to the World Health Organization (WHO), MSDs constitute the primary cause of disability in most countries, affecting approximately 1.71 billion individuals.1 A systematic review of the Global Burden of Disease indicated that musculoskeletal conditions are the foremost contributor to worldwide disability, accounting for 16% of all years lived with disability.3 Although the prevalence of musculoskeletal conditions varies widely based on age, occupation, and diagnosis, approximately one-third of the global population grapple with painful musculoskeletal issues, primarily during their peak productive years.2,4 Data from the Bone and Joint Initiative in the USA show that one in two Americans experience some form of MSD, a prevalence equivalent to that of chronic respiratory and cardiovascular diseases combined.5
Similar to other non-communicable diseases, the risk factors for MSDs are often multifaceted. They can be broadly categorized as individual-related factors, including gender, age, sleep, physical activity, and work-related factors.6–8 An MSD is deemed work-related when the work environment significantly contributes to its development, exacerbation of existing conditions, or prolongation of previous ones.4 Research has indicated that commonly affected body parts due to MSDs include the lower back, neck, shoulder, forearm, and hand.9,10 MSDs exert various health and socio-economic impacts on communities.11,12 Given that MSDs and other non-communicable diseases share many risk factors, between one-third and half of MSD patients also suffer from other multimorbid conditions, heightening their risk of depression and other chronic illnesses.13–15 A study conducted in the Riyadh region of the Kingdom of Saudi Arabia (KSA) revealed that musculoskeletal symptoms were among the primary causes of certified sickness absenteeism.16 Furthermore, such absenteeism may lead to a loss of productivity, exerting a significant negative impact on the overall economy of society.17,18 A study conducted at Majmaah University in the KSA found that nearly half (55%) of the applied medical college faculty members suffered from one form of work-related MSD or another. In their investigation, the distribution pattern of conditions was as follows: neck (53.5%), lower back (43.3%), and hand (31.6%).19 These prevalence rates of MSDs were self-reported and assessed using a standardized and validated questionnaire. Another study conducted in Riyadh by Alsultan et al found that a very high proportion (82.9%) of participants reported experiencing musculoskeletal complaints.20 The study by Alsultan et al utilized a self-administered questionnaire administered to their study participants.
MSDs have emerged as a pressing concern among healthcare workers (HCWs). Despite being overlooked for an extended period, it has garnered significant attention, particularly in the context of the COVID-19 pandemic.21–23 The data in all of these studies were gathered through a self-administered method employing a validated questionnaire. HCWs frequently find themselves in prolonged standing positions, notably in operating rooms and during other procedures. Their roles often encompass various responsibilities, including daily clinical practice, teaching, research, and administration. This multitude of duties places HCWs in a more demanding and stressful environment, which may contribute to the increased prevalence of MSDs. A systematic review recently conducted by Jacquier-Bret and Gorce (2023) revealed that surgeons and dentists exhibited the highest incidence of musculoskeletal issues in the lower back and upper extremities. By contrast, nurses predominantly suffered from lower extremity MSDs. Their review identified repetitive awkward positions during working hours as a primary risk factor for MSDs.24 Alzeyadi’s study conducted in the KSA during the COVID-19 pandemic reported an escalation in work-related MSDs among HCWs. Factors such as nationality, alterations in working shifts, and assuming awkward positions were identified as predictors in their investigation.23 Given the vast sociocultural diversity, variances in the distribution of HCWs, and the contrasting climates across different regions of the KSA, it is imperative to refrain from generalizing findings from other studies to the entire HCWs population of the KSA. Consequently, ongoing assessment is crucial, as the epidemiological factors pertaining to MSDs among HCWs are subject to change. Furthermore, region-specific data on this intricate subject are imperative to drive necessary policy reforms. Therefore, continuous evaluation of the prevalence, patterns, and associated factors of MSDs will offer invaluable insights for policymakers to design effective health-related programs for HCWs, thereby optimizing their effectiveness. To the best of our knowledge and after an extensive literature review, it is evident that studies conducted in multiple healthcare settings in the KSA are limited, particularly in northern Saudi Arabia. Thus, this study was undertaken to gauge the prevalence and characteristics of MSDs among HCWs in northern Saudi Arabia, with the aim of identifying the factors associated with MSDs within this specific population.
Materials and Methods
Study Description
The present study is an analytical cross-sectional investigation conducted among randomly selected HCWs in the Al-Jouf province of the KSA, spanning from January 2022 to June 2022. Al-Jouf, located in northern Saudi Arabia, houses various healthcare settings including primary health centers (PHCs), general hospitals, and specialty hospitals. This study employed one tertiary care hospital, one general hospital, and all PHCs in the region as study settings. This study included all categories of HCWs from the selected healthcare facilities who were willing to participate, while excluding those solely engaged in academic activities, with musculoskeletal injuries in the past 12 months, or known to have autoimmune diseases.
Sampling Strategy
To ascertain the minimum number of HCWs required for this survey, the Raosoft online sample size calculator, which follows the principles of Cochran’s equation, was used. Given the prevalence of a wide range of MSDs among HCWs identified in the literature review, this study conservatively assumed an expected prevalence of 50%, with a 95% confidence interval (CI) and a 5% margin of error. Employing these parameters, 384 HCWs represented the minimum necessary for this survey. This study adopted a convenience sampling approach to recruit the required HCWs across categories and settings until the specified number of participants was reached.
Data Collection Process
The survey was initiated after obtaining ethical clearance from the Regional Ethics Committee, Qurayat Health Affairs, KSA (approval no.: 115). The data collectors, having secured prior approval from the respective healthcare settings’ authorities, visited the selected facilities to collect data from the HCWs. During the participants’ break time at their workplace, the data collectors extended invitations to the required number of participants from each type of healthcare facility and category of HCWs.
The data collection process began by providing a brief overview of the study to the HCWs. Subsequently, self-administered questionnaires were administered to selected participants, ensuring their informed consent in compliance with the Declaration of Helsinki.
The questionnaire comprised two sections.
Section A: This segment gathered sociodemographic, health, and work-related information from participants, including age, gender, nationality, smoking status, work setting, work experience, daily duration of computer and smartphone use, sustaining awkward positions at the workplace, weekly physical activity duration, and daily sleep duration. Additionally, participants’ height and weight were measured to calculate their body mass index (BMI). During the study briefing, participants were provided with visual aids to elucidate the concept of awkward positions and asked whether they had encountered these positions. Participants were also queried about any participation in formal ergonomics training programs within the last 3 years, with responses being “yes” or “no”.
Awkward workplace postures refer to body positions significantly deviating from the neutral position while performing tasks. Examples include twisting, bending, reaching, tugging, and lifting. Additionally, maintaining hands above the head, elbows higher than the shoulders, a bent wrist, and a neck or back bent more than 30 degrees without support are considered instances of awkward postures.25,26
Section B: This part focused on participants’ musculoskeletal issues and employed the standardized Nordic Musculoskeletal Questionnaire (NMQ). The NMQ is a validated tool utilized in various primary care and epidemiological studies globally, including in the KSA.27–29 Within the NMQ, participants were prompted to report any instances of acute pain, discomfort, or numbness in nine specific body regions over the past 12 months: neck, shoulders, elbows, wrists/hands, upper back, lower back, hips, knees, and ankles. Participants responding affirmatively were further queried about whether this trouble had hindered their regular work in the past 12 months. Finally, the NMQ inquired about participants’ experiences of such trouble within the past week.
Data Analysis
For qualitative variables, descriptive statistics were reported as frequency (n) and percentage, and for quantitative variables are described using the mean along with the standard deviation (SD). Initially, a univariate analysis was performed without controlling for other independent variables. Subsequently, a multivariate analysis employing binomial logistic regression was employed to identify the factors associated with MSDs. A CI was considered statistically significant if the p-value was less than 0.05 and did not encompass the null value of one. Data entry and analysis were conducted using Statistical Package for Social Sciences (SPSS) version 20.
Results
Of the 384 participating HCWs, the majority were males (54.2%), Saudi nationals (66.4%), married (73.7%), held a bachelor’s degree (50.5%), and worked in a general hospital (38.5%). The mean age ± SD of the participants was 35.28 ± 8.6 (Table 1).
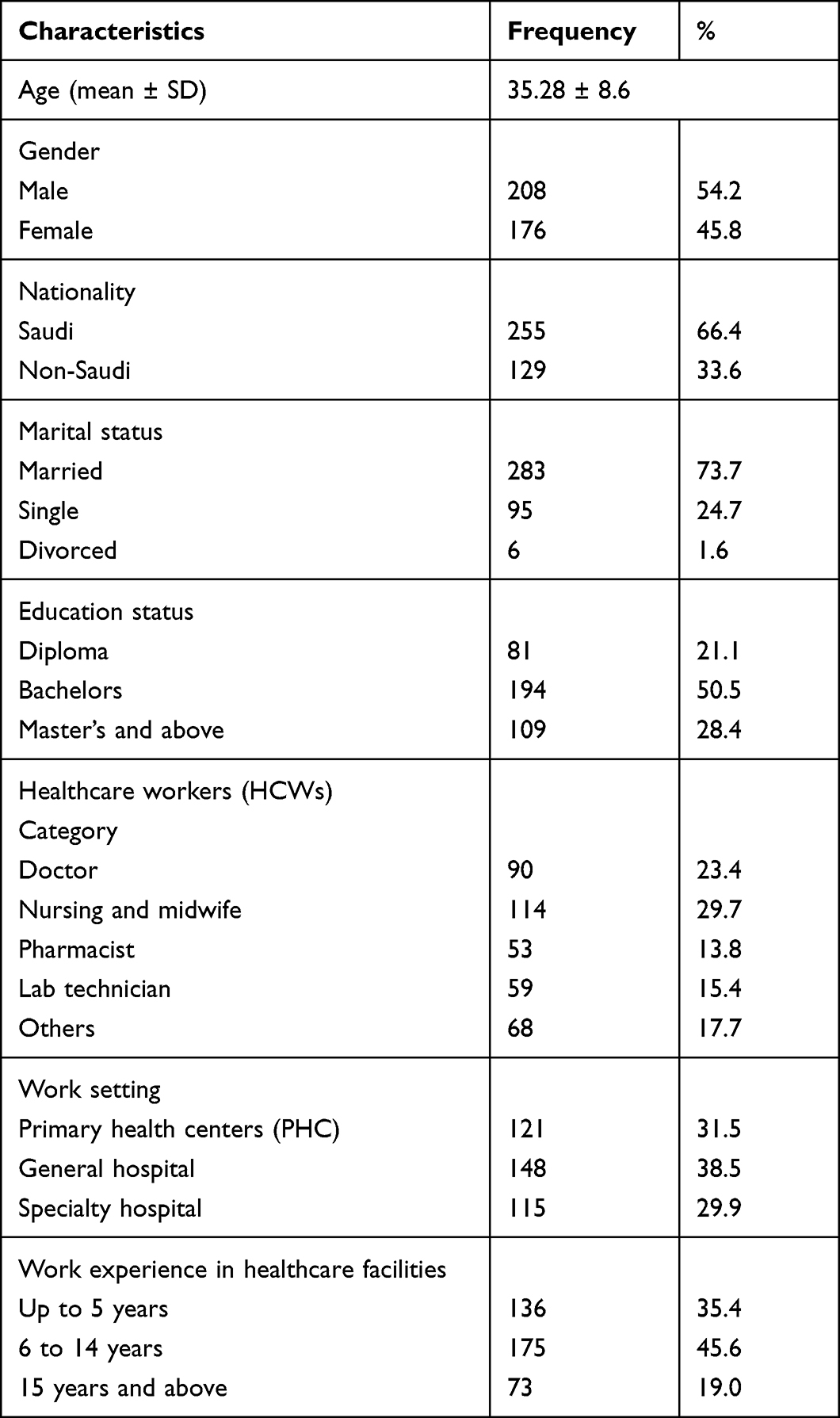 |
Table 1 Participants’ Sociodemographic Characteristics (n=384) |
In terms of health and ergonomics-related characteristics, most participants were non-smokers (73.4%), classified as overweight based on BMI (39.6%), with a mean ± SD of physical activity duration per week of 5.17 ± 3.3, and a mean ± SD duration of computer/laptop usage per day of 2.27 ± 1.11. Additionally, 64.3% reported having experienced repeated awkward positions during work, while less than one-fourth (24.7%) had received ergonomic-related training (Table 2).
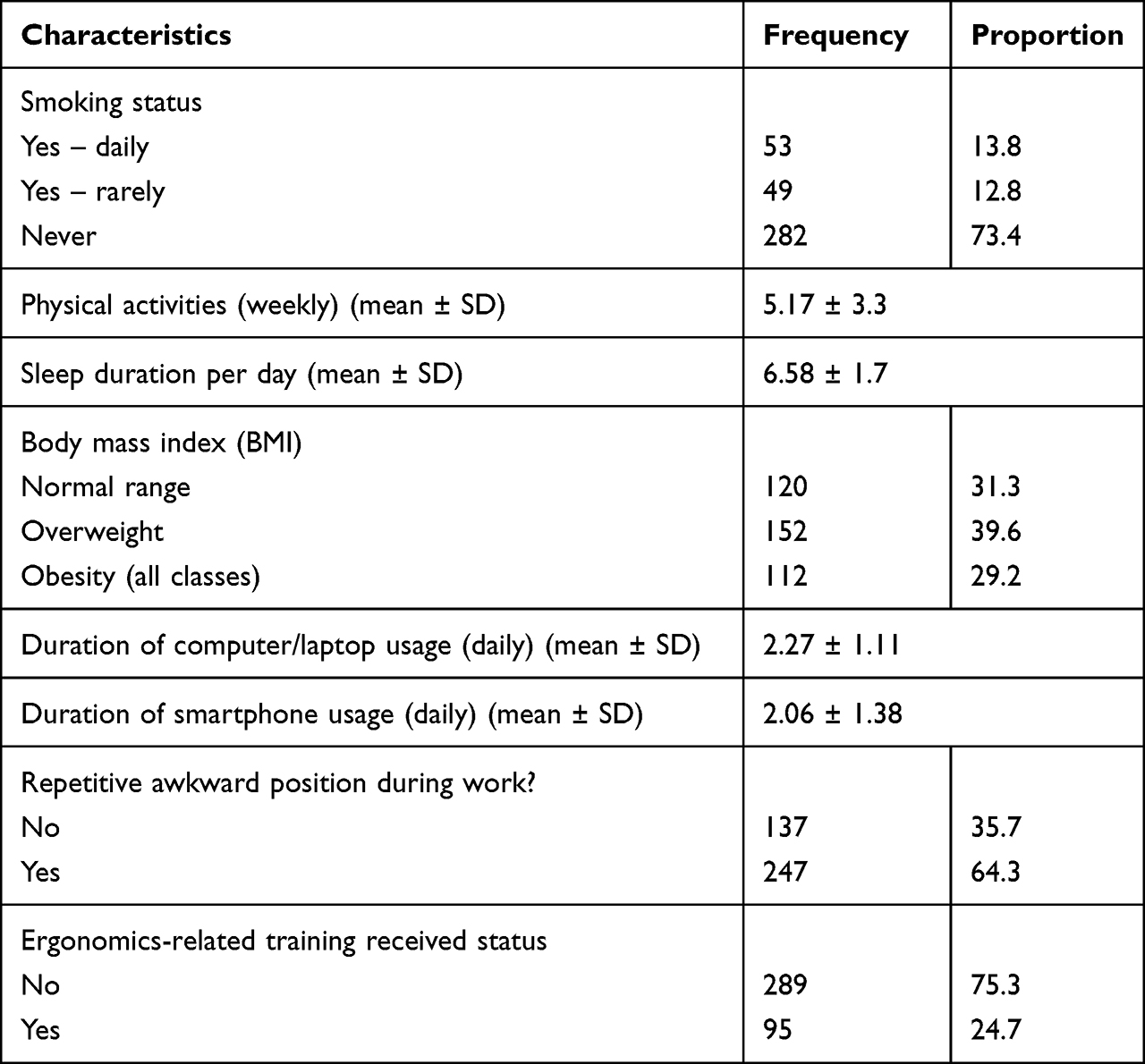 |
Table 2 Participants’ Health- and Ergonomics-Related Characteristics (n = 384) |
Approximately three-fourths (72.4%) of the HCWs reported trouble in one or more of the sites listed in the NMQ form over the past 12 months (Figure 1).
 |
Figure 1 Prevalence of MSDs in the past 12 months (n = 384). |
The distribution of affected body regions (according to NMQ) over the past 12 months and 7 days is depicted in Figure 2. The most commonly affected body regions in the past 12 months were the neck (147 cases), followed by the shoulder (132 cases), lower back (117 cases), and wrist (99 cases).
 |
Figure 2 Distribution of body regions affected with MSDs in the past 1 year and 1 week. |
Initially, univariate logistic regression analysis was performed, and subsequently, multivariate logistic regression analysis was performed after adjusting for other covariables. Concerning sociodemographic characteristics, the univariate analysis revealed that the presence of MSDs was significantly associated with gender (Ref. Male; adjusted odds ratio [OR] = 4.11, 95% CI = 2.32–6.77, p < 0.001), nationality (Ref. non-Saudi nationals; OR = 0.63, 95% CI = 0.48–0.85, p < 0.001), and work setting (Ref. PHC; OR = 2.31, 95% CI = 1.25–4.13, p = 0.016; Table 3). The results of multivariate analysis suggested that the presence of MSDs was significantly associated with gender (Ref. Male; AOR = 2.72, 95% CI = 1.38–4.17, p = 0.001), nationality (Ref. Non-Saudi nationals; AOR = 0.45, 95% CI = 0.23–0.67, p = 0.001), work setting (Ref. PHC; AOR = 1.89, 95% CI = 1.32–2.35, p = 0.039), and work experience in healthcare facilities (Ref. Up to 5 years; AOR = 3.03, 95% CI = 1.99–4.32, p = 0.025; Table 3). Regarding health and ergonomics-related factors, both univariate and multivariate analyses yielded similar risk factors, albeit with different odds ratios and p-values. A significant association existed between MSDs and physical activity duration (AOR = 0.72, 95% CI = 0.53–0.93, p = 0.024), obesity status (Ref. normal range; AOR = 3.08, 95% CI = 1.56–4.71, p = 0.003), duration of daily computer/laptop usage (AOR = 1.54, 95% CI = 1.09–2.10, p = 0.031), duration of daily smartphone usage (AOR = 2.03, 95% CI = 1.14–3.18, p = 0.006), repeated awkward position at work (Ref. No; AOR = 3.67, 95% CI = 2.25–5.77, p < 0.001), and ergonomics training (Ref. No: AOR = 0.38, 95% CI = 0.23–0.55, p < 0.001; Table 4).
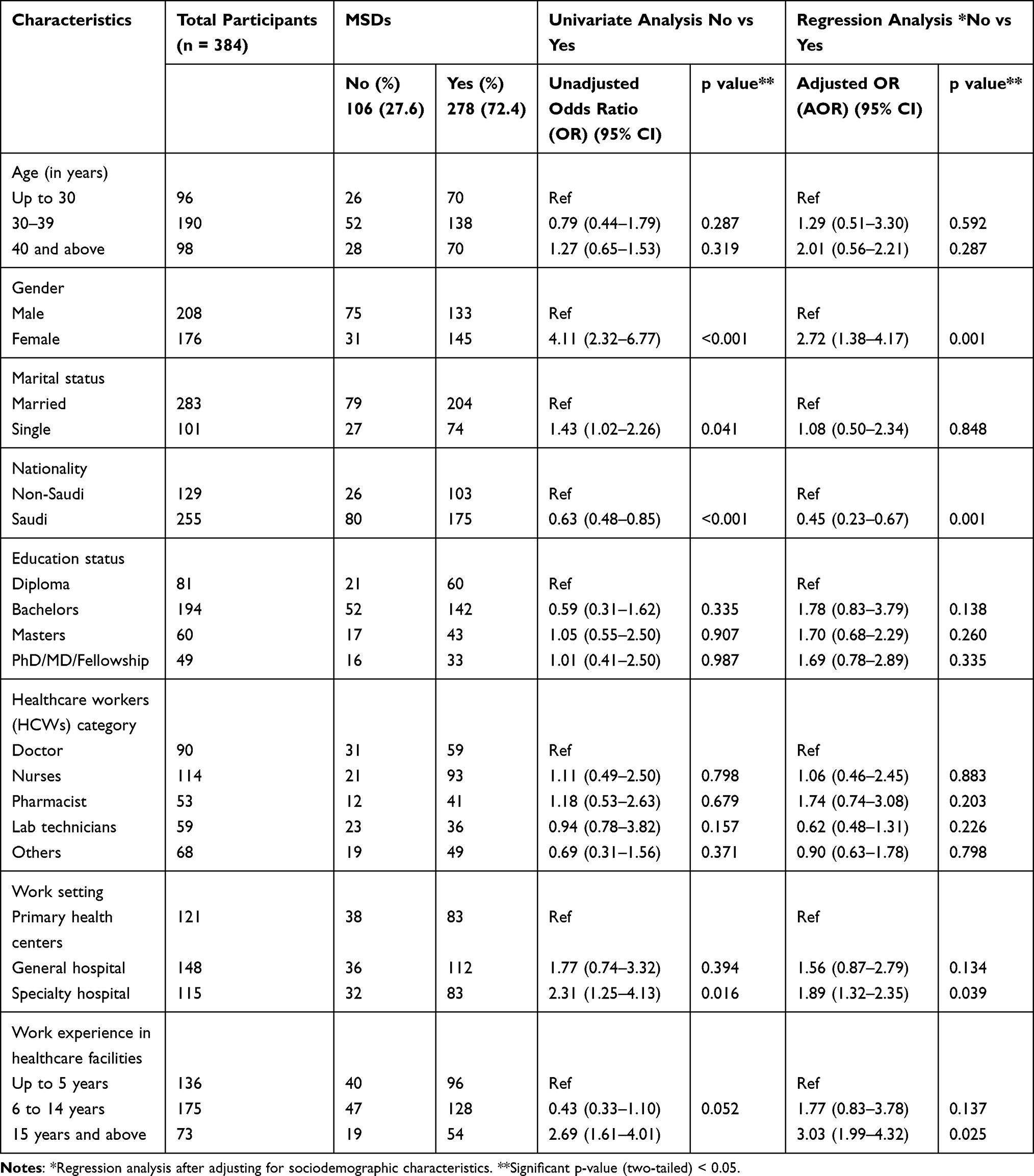 |
Table 3 Binomial Logistic Regression Analysis of Sociodemographic Factors Associated with the MSDs Among the Participants |
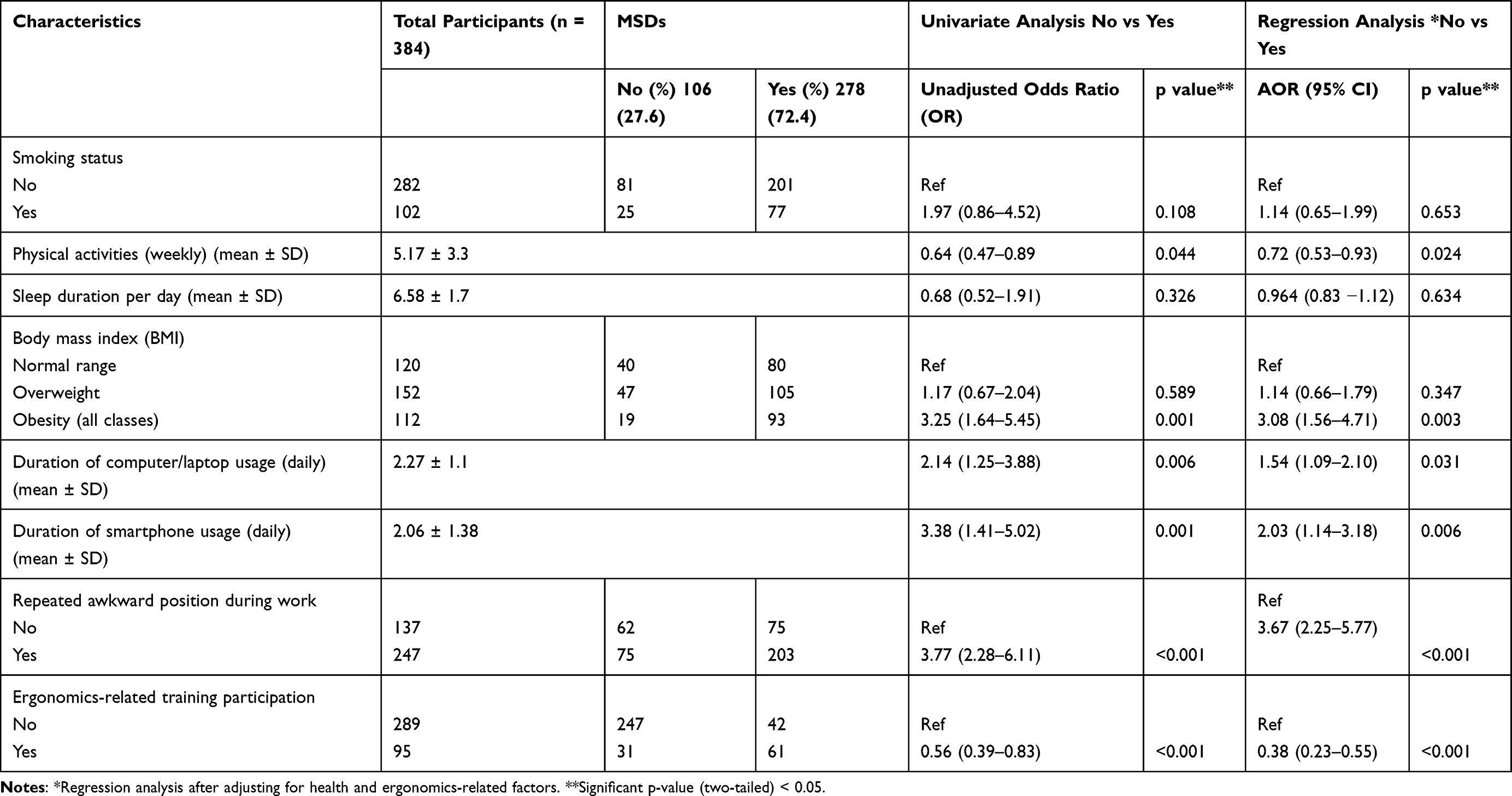 |
Table 4 Binomial Logistic Regression Analysis of Health- and Ergonomics-Related Factors Associated with the MSDs Among the Participants |
Discussion
Healthcare workforces play a pivotal role in a country’s healthcare system. Protecting HCWs from all health-related consequences, including MSDs, is emphasized by the WHO.30 This underscores the necessity of the present study, which aimed to evaluate the prevalence, pattern, and associated factors of MSDs among HCWs in northern KSA.
The current research findings indicated that approximately three-fourths (72.4%) of HCWs experienced one or more MSDs in the past 12 months. Similar results were reported by Alzeyadi et al from the KSA, where a high proportion of healthcare professionals suffered from MSDs.23 Interestingly, a study conducted in Malaysia during the COVID-19 pandemic by Krishnan et al indicated an even higher proportion (97.4%) of participants affected by MSDs in 13 different body parts over the same time period.31 The significant difference between the present study and Krishnan et al’s could be attributed to variations in healthcare settings, tools used, and inclusion/exclusion criteria. The present study was conducted toward the end of the pandemic, while Krishnan et al focused exclusively on nurses. A 2021 review by Shaikh et al indicated that the prevalence of MSDs among hospital staff ranged from 43% to 78%. This wide range may be attributed to varying factors such as the inclusion of a diverse range of HCWs and differing durations of self-reported MSDs. Nonetheless, this suggests that the prevalence of MSDs among the participants of the present study is notably high.32 These findings highlight the imperative need for focused attention on HCWs’ musculoskeletal health, given its negative impact on their quality of life and the efficient delivery of patient care. Furthermore, the healthcare industry bears a substantial financial burden due to MSDs affecting HCWs.
Risk factors for MSDs vary significantly across different occupational groups. The results of the present study align with those of some recent studies but deviate from others. Specifically, females had a higher risk (p = 0.001) of developing MSDs than their male counterparts. This corroborates with most studies, which consistently report a higher risk for females in developing MSDs, whether work-related or not.33,34 Additionally, Arcas et al reported that women experience longer durations of sickness absenteeism due to MSD problems.35 This significant finding may be attributed to gender-specific dynamics in the intersection between paid leave and family responsibilities. To mitigate sickness absenteeism and enhance healthcare delivery, the results of this study underscore the necessity for continued research and public health policies addressing sickness absenteeism from a gender perspective. Expatriates constitute a substantial proportion of the healthcare workforce in the KSA, especially in nursing. Addressing disparities and implementing necessary interventions is integral to healthcare development, ultimately alleviating the burden on the healthcare industry.32,36 This study revealed that MSDs were significantly more prevalent among expatriate HCWs than the Saudi nationals. This contradicts the findings of a study by Alzayani et al37 which may be attributed to differences in the inclusion of HCWs and healthcare facilities. The survey conducted in this study encompassed all HCW categories across various healthcare settings. The use of computers, mobile devices, and applications has surged in healthcare settings in recent years. Several researchers have touted the benefits of smartphone usage and telehealth services.38,39 However, the escalating use of smartphones in healthcare delivery is directly linked to a rise in MSDs, as HCWs extend their usage time for professional purposes in addition to personal use.40,41 The findings of the present study underscore that the durations of computer/laptop and smartphone usage are significant factors in the development of MSDs. Hence, healthcare professionals must be cognizant of the repercussions of excessive smartphone use, especially in awkward positions.
This study revealed that the neck, shoulder, lower back, and wrist were the most commonly affected body regions. By contrast, a study conducted by Ibrahim et al in Malaysia, employing NMQ, reported that the prevalence of MSDs was notably concentrated in the lower back (88.2%). This variance could be attributed to differences in study settings: our research encompassed all three levels of healthcare delivery, while the latter focused solely on a specialized center. Notably, work setting (p = 0.039) emerged as a significant predictor of MSDs among our participants.42 Research has underscored alarming risk factors associated with MSDs in Saudi Arabia, shedding light on the substantial challenges faced by healthcare professionals.43 Our study identified a significant association between MSDs and a lack of physical activity and increased BMI. A recent systematic review highlighted that maintaining high to moderate levels of physical activity plays a crucial role in safeguarding healthcare professionals from the risk of MSDs.44 Similar to our findings, Alnaami et al reported that HCWs with a higher BMI had elevated odds of developing low back pain, a significant musculoskeletal problem.45 Intriguingly, multiple studies have indicated that obesity and overweight rates tend to be higher among HCWs.46,47 Therefore, it is imperative for relevant authorities to implement measures aimed at reducing obesity and overweight prevalence among HCWs, thus alleviating the burden of MSDs. Physical exercise interventions hold promise in enhancing muscle activation and posture for affected individuals.45 Research strongly advocates for prophylactic measures to mitigate the adverse effects of lower back pain and other MSDs. Despite ergonomic factors such as repetitive awkward postures (p <0.001) and lack of training and knowledge on ergonomics in the workplace (p <0.001) being identified as critical predictors in our study and previous studies, over three-fourths (75.3%) of HCWs did not receive formal ergonomics training, and 35.3% reported experiencing repetitive awkward positions during duty hours.48,49 These findings carry substantial implications for policymakers, underscoring the urgent need for implementing pre-placement and periodic formal ergonomic training for HCWs.
Strengths and Limitations of the Study
Our study stands as the inaugural endeavor of its kind in the northern regions of the KSA. Furthermore, this study successfully recruited a substantial number of HCWs across different healthcare facilities, representing various categories. However, some limitations warrant consideration when interpreting our findings. First, this study employed a convenience sampling method to enlist HCWs solely from the northern region of the KSA, thus limiting the generalizability of our results to other areas of the KSA. Moreover, the cross-sectional design used in this study to assess the prevalence and associated factors of HCWs may not establish causal and temporal associations between exposure and outcome variables. Finally, it is important to acknowledge the potential for recall bias and the likelihood of participants providing self-reported and possibly exaggerated accounts.
Conclusion
The findings from our study underscore a remarkably high prevalence of MSDs among HCWs. The presence of MSDs exhibited significant associations with gender, nationality, work setting, obesity, repetitive awkward positions at work, and ergonomics training. The neck, followed by the shoulder, lower back, and wrist, emerged as the most commonly affected body regions. The results of this study strongly advocate the implementation of frequent screening programs among HCWs to identify risk factors for MSDs, develop prevention strategies, and ensure timely treatment. Additionally, it is imperative to conduct evaluations of postures and associated MSD risks across various healthcare delivery practices. Finally, relevant authorities should be called up on to seriously consider the implementation of pre-placement and periodic ergonomic training for HCWs, a measure that may help reduce sickness absenteeism and enhance productivity. Future longitudinal studies in other regions of Saudi Arabia are warranted to establish causal associations between risk factors and MSDs.
Acknowledgments
The authors wish to thank all the healthcare workers who participated in the survey. We extend our sincere thanks to Jeffry John, Flywings International College, Ernakulam for his immense help in formatting and preparing figures required for this study.
Funding
This work was funded by the Deanship of Graduate Studies and Scientific Research at Jouf University under grant No (DSR2023-01-02330).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Musculoskeletal Conditions. World Health Organization; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions.
2. Briggs AM, Woolf AD, Dreinhöfer K, et al. Reducing the global burden of musculoskeletal conditions. Bull World Health Organ. 2018;96(5):366–368. doi:10.2471/blt.17.204891
3. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/s0140-6736(18)32279-7
4. CDC. Work-related musculoskeletal disorders & ergonomics. Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/workplacehealthpromotion/health-strategies/musculoskeletal-disorders/index.html.
5. USBJI. The burden of musculoskeletal diseases in the United States. United States Bone and Joint Initiative; 2022. Available from: https://www.boneandjointburden.org/.
6. AlOmar RS, AlShamlan NA, Alawashiz S, Badawood Y, Ghwoidi BA, Abugad H. Musculoskeletal symptoms and their associated risk factors among Saudi office workers: a cross-sectional study. BMC Musculoskelet Disord. 2021;22(1):763. doi:10.1186/s12891-021-04652-4
7. Jain R, Meena ML, Dangayach GS, Bhardwaj AK. Association of risk factors with musculoskeletal disorders in manual-working farmers. Arch Environ Occup Health. 2018;73(1):19–28. doi:10.1080/19338244.2017.1289890
8. Tuček M, Vaněček V. Musculoskeletal disorders and working risk factors. Cent Eur J Public Health. 2020;28(Suppl):S06–s11. doi:10.21101/cejph.a6183
9. Wu D, Wong P, Guo C, Tam LS, Gu J. Pattern and trend of five major musculoskeletal disorders in China from 1990 to 2017: findings from the global burden of disease study 2017. BMC Med. 2021;19(1):34. doi:10.1186/s12916-021-01905-w
10. Zaheer S, Amir Q, Waseem HF, et al. Patterns of musculoskeletal disorders in health care providers and their association with ergonomic risks. Intern J Occupat Saf Ergon. 2022:1–9. doi:10.1080/10803548.2022.2154483
11. Woolf A. Musculoskeletal health, wealth and business, and wider societal impact. Eur J Public Health. 2022;32(5):831–833. doi:10.1093/eurpub/ckac087
12. Chen N, Fong DYT, Wong JYH. Health and economic outcomes associated with musculoskeletal disorders attributable to high body mass index in 192 countries and territories in 2019. JAMA Network Open. 2023;6(1):e2250674–e2250674. doi:10.1001/jamanetworkopen.2022.50674
13. Duffield SJ, Ellis BM, Goodson N, et al. The contribution of musculoskeletal disorders in multimorbidity: implications for practice and policy. Best Pract Res Clin Rheumatol. 2017;31(2):129–144. doi:10.1016/j.berh.2017.09.004
14. Øverås CK, Nilsen TIL, Nicholl BI, et al. Multimorbidity and co-occurring musculoskeletal pain do not modify the effect of the SELFBACK app on low back pain-related disability. BMC Med. 2022;20(1):53. doi:10.1186/s12916-022-02237-z
15. Lowe DB, Taylor MJ, Hill SJ. Associations between multimorbidity and additional burden for working-age adults with specific forms of musculoskeletal conditions: a cross-sectional study. BMC Musculoskelet Disord. 2017;18(1):135. doi:10.1186/s12891-017-1496-2
16. Khawaja RA, Sikander R, Khawaja AA, Jareno RJ, Halepota AT. Medically certified sickness absence among health care workers. J Pak Med Assoc. 2012;62(9):900–904.
17. Hultin H, Lindholm C, Malfert M, Möller J. Short-term sick leave and future risk of sickness absence and unemployment - The impact of health status. BMC Public Health. 2012;12(1):861. doi:10.1186/1471-2458-12-861
18. Strömberg C, Aboagye E, Hagberg J, Bergström G, Lohela-Karlsson M. Estimating the effect and economic impact of absenteeism, presenteeism, and work environment–related problems on reductions in productivity from a managerial perspective. Value Health. 2017;20(8):1058–1064. doi:10.1016/j.jval.2017.05.008
19. Sirajudeen MS, Alaidarous M, Waly M, Alqahtani M. Work-related musculoskeletal disorders among faculty members of college of applied medical sciences, Majmaah University, Saudi Arabia: a cross-sectional study. Int J Health Sci. 2018;12(4):18–25.
20. Alsultan A, Alahmed S, Alzahrani A, Alzahrani F, Masuadi E. Comparison of musculoskeletal pain prevalence between medical and surgical specialty residents in a major hospital in Riyadh, Saudi Arabia. J Musculosk Surg Res. 2018;2:161. doi:10.4103/jmsr.jmsr_36_18
21. Efe Is E, Sahillioglu A, Demirel S, Kuran B, Mustafa Ozdemir H. Effect of COVID-19 pandemic on physical activity habits, musculoskeletal pain, and mood of healthcare workers. Sisli Etfal Hastan Tip Bul. 2021;55(4):462–468. doi:10.14744/semb.2021.87523
22. Arca M, Dönmezdil S, Durmaz ED. The effect of the COVID-19 Pandemic on anxiety, depression, and musculoskeletal system complaints in healthcare workers. Work. 2021;69(1):47–54. doi:10.3233/wor-205014
23. Alzeyadi AA, Elsiddig AI, Khan MA, et al. Prevalence of musculoskeletal disorders among health care workers during covid-19 pandemic in the western region of Saudi Arabia. Med Sci. 2022;26:1. doi:10.54905/disssi/v26i121/ms104e2106
24. Jacquier-Bret J, Gorce P. Prevalence of body area work-related musculoskeletal disorders among healthcare professionals: a systematic review. Int J Environ Res Public Health. 2023;20:1. doi:10.3390/ijerph20010841
25. Kunda R, Frantz J, Karachi F. Prevalence and ergonomic risk factors of work-related musculoskeletal injuries amongst underground mine workers in Zambia. J Occup Health. 2013;55(3):211–217. doi:10.1539/joh.11-0175-fs
26. EU-OSHA. Work-related musculoskeletal disorders among hospital workers - OSHwiki | European Agency for Safety and Health at Work; 2023. Available from: https://oshwiki.osha.europa.eu/en/themes/work-related-musculoskeletal-disorders-among-hospital-workers.
27. Aljanakh M, Shaikh S, Siddiqui AA, Al-Mansour M, Hassan SS. Prevalence of musculoskeletal disorders among dentists in the Hail Region of Saudi Arabia. Ann Saudi Med. 2015;35(6):456–461. doi:10.5144/0256-4947.2015.456
28. López-Aragón L, López-Liria R, Callejón-Ferre Á-J, Gómez-Galán M. Applications of the standardized Nordic questionnaire: a review. Sustainability. 2017;9(9):1514. doi:10.3390/su9091514
29. Kahraman T, Genç A, Göz E. The Nordic musculoskeletal questionnaire: cross-cultural adaptation into Turkish assessing its psychometric properties. Disabil Rehabil. 2016;38(21):2153–2160. doi:10.3109/09638288.2015.1114034
30. World Health Organization. Health Workforce. World Health Organization; 2023. Available from: https://www.who.int/health-topics/health-workforce#tab=tab_1.
31. Krishnan KS, Raju G, Shawkataly O. Prevalence of work-related musculoskeletal disorders: psychological and physical risk factors. Int J Environ Res Public Health. 2021;18(17):9361. doi:10.3390/ijerph18179361
32. Shaikh S, Siddiqui AA, Alshammary F, Amin J, Agwan MAS. Musculoskeletal Disorders Among Healthcare Workers: prevalence and Risk Factors in the Arab World. In: Laher I, editor. Handbook of Healthcare in the Arab World. Springer International Publishing; 2020:1–39.
33. Holzgreve F, Fraeulin L, Haenel J, et al. Office work and stretch training (OST) study: effects on the prevalence of musculoskeletal diseases and gender differences: a non-randomised control study. BMJ Open. 2021;11(5):e044453. doi:10.1136/bmjopen-2020-044453
34. Higgins DM, Fenton BT, Driscoll MA, et al. Gender differences in demographic and clinical correlates among veterans with musculoskeletal disorders. Womens Health Issues. 2017;27(4):463–470. doi:10.1016/j.whi.2017.01.008
35. Arcas MM, Delclos GL, Torá-Rocamora I, Martínez JM, Benavides FG. Gender differences in the duration of non-work-related sickness absence episodes due to musculoskeletal disorders. J Epidemiol Community Health. 2016;70(11):1065–1073. doi:10.1136/jech-2014-204331
36. Alluhidan M, Tashkandi N, Alblowi F, et al. Challenges and policy opportunities in nursing in Saudi Arabia. Hum Resour Health. 2020;18(1):98. doi:10.1186/s12960-020-00535-2
37. Alzayani MK, Salama KF, Zafar M. Work-related musculoskeletal disorders among dental staff in Armed Force Hospital in Dhahran, Saudi Arabia. Afr Health Sci. 2022;22(2):602–611. doi:10.4314/ahs.v22i2.69
38. Nair AA, Afroz S, Ahmed BU, et al. Smartphone usage among doctors in the clinical setting in two culturally distinct countries: cross-sectional comparative study. JMIR Mhealth Uhealth. 2021;9(5):e22599. doi:10.2196/22599
39. King ALS, Pádua MK, Gonçalves LL, Santana de Souza Martins A, Nardi AE. Smartphone use by health professionals: a review. Digit Health. 2020;6:2055207620966860. doi:10.1177/2055207620966860
40. Eitivipart AC, Viriyarojanakul S, Redhead L. Musculoskeletal disorder and pain associated with smartphone use: a systematic review of biomechanical evidence. Hong Kong Physioth J. 2018;38(02):77–90. doi:10.1142/S1013702518300010
41. Alwatban O, Alshammari S, Alrabiah B, Alsadhan K, Alwhibi M. The association between smartphone usage and musculoskeletal pain among medical residents in Riyadh, Saudi Arabia during covid-19 pandemic. Med Sci. 2021;25:2383–2391.
42. Ibrahim NI, Mohanadas D. Prevalence of musculoskeletal disorders among staffs in specialized healthcare centre. Work. 2012;41:2452–2460. doi:10.3233/wor-2012-0480-2452
43. Abolfotouh M, Alomair F, Alangari D, Bushnak I, Aldebasi B, Almansoof A. Epidemiology of work-related lower back pain among rehabilitation professionals in Saudi Arabia. East Mediterr Health J. 2021;27(4):390–398. doi:10.26719/emhj.21.019
44. Parreira P, Maher CG, Steffens D, Hancock MJ, Ferreira ML. Risk factors for low back pain and sciatica: an umbrella review. Spine J. 2018;18(9):1715–1721. doi:10.1016/j.spinee.2018.05.018
45. Alnaami I, Awadalla NJ, Alkhairy M, et al. Prevalence and factors associated with low back pain among health care workers in southwestern Saudi Arabia. BMC Musculoskelet Disord. 2019;20(1):56. doi:10.1186/s12891-019-2431-5
46. Younis J, Jiang H, Fan Y, et al. Prevalence of overweight, obesity, and associated factors among healthcare workers in the Gaza Strip, Palestine: a cross-sectional study. Front Public Health. 2023;11:1129797. doi:10.3389/fpubh.2023.1129797
47. Kunyahamu MS, Daud A, Jusoh N. Obesity among health-care workers: which occupations are at higher risk of being obese? Int J Environ Res Public Health. 2021;18(8):4381. doi:10.3390/ijerph18084381
48. Fan LJ, Liu S, Jin T, et al. Ergonomic risk factors and work-related musculoskeletal disorders in clinical physiotherapy. Front Public Health. 2022;10:1083609. doi:10.3389/fpubh.2022.1083609
49. Aghilinejad M, Ehsani AA, Talebi A, Koohpayehzadeh J, Dehghan N. Ergonomic risk factors and musculoskeletal symptoms in surgeons with three types of surgery: open, laparoscopic, and microsurgery. Med J Islam Repub Iran. 2016;30:467.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Determinants of Knowledge of Musculoskeletal Disorders Among Healthcare Providers and Students in Saudi Arabia: A Cross-Sectional Study
Alrwaily M, Alanazi F
Journal of Multidisciplinary Healthcare 2022, 15:1789-1797
Published Date: 25 August 2022
Neck Pain, Mental Status, and Associated Factors Among Hospital Secretaries: A Cross-Sectional Study From Turkey
Medeni V, Gingir C, Medeni İ, Uğraş Dikmen A, İlhan MN
Journal of Pain Research 2024, 17:1223-1233
Published Date: 20 March 2024
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Serbaya SH, Khan AA, Surbaya SH, Alzahrani SM
Advances in Medical Education and Practice 2024, 15:269-280
Published Date: 5 April 2024
Healthcare Workers’ Knowledge, Awareness, and Practices Regarding Antimicrobial Use, Resistance, and Stewardship in Saudi Arabia
Abdallah MS, Al Meanazel OT, Alruwaili MM, AlRasheed HA
Infection and Drug Resistance 2025, 18:6035-6050
Published Date: 19 November 2025