Back to Journals » Clinical Optometry » Volume 18
Prevalence of Refractive Errors, Myopic Macular Degeneration, and Associated Risk Factors in a Maltese Population-Based Study
Authors Agius D ![]() , Mamo J, Calleja N, Cassar D, Marku X
, Mamo J, Calleja N, Cassar D, Marku X ![]() , Nappa MC, Zammit M
, Nappa MC, Zammit M ![]() , Pace ME, Carbonaro F
, Pace ME, Carbonaro F
Received 18 August 2025
Accepted for publication 21 January 2026
Published 7 February 2026 Volume 2026:18 561426
DOI https://doi.org/10.2147/OPTO.S561426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chris Lievens
David Agius,1,2 Julian Mamo,3 Neville Calleja,3 Daniel Cassar,2 Xeniya Marku,2 Maria Christina Nappa,4 Michaela Zammit,4 Maria Elena Pace,5 Francis Carbonaro1,2,6
1Department of Surgery, University of Malta, Msida, Malta; 2Department of Ophthalmology, Mater Dei Hospital, Msida, Malta; 3Department of Public Health, University of Malta, Msida, Malta; 4Department of Medicine, Mater Dei Hospital, Msida, Malta; 5Medical School, University of Malta, Msida, Malta; 6Department of Twin Research, King’s College, London, UK
Correspondence: David Agius, Ophthalmology Outpatients, Mater Dei Hospital, Triq id-Donaturi tad-Demm, Msida, MSD, 2090, Malta, Email [email protected]
Purpose: To estimate the prevalence of refractive error and myopic macular degeneration in a nationally representative sample of older adults from Malta, evaluate associations with established risk factors.
Patients and Methods: This population-based cross-sectional study included 1,794 participants aged 50– 80 years from Malta, recruited as part of The Malta Eye Study (response rate 44.8%). Demographic, medical, behavioral, and ocular data were collected using structured questionnaires. Standardized ophthalmic examinations were performed, including autorefraction and retinal imaging with optical coherence tomography. Refractive error was classified by spherical equivalent as myopia (< − 0.50 D) and hyperopia (> +0.50 D), while astigmatism was defined as ≤ − 0.75 D. Myopic macular degeneration was graded using the meta-analysis for pathologic myopia classification. Associations were assessed using multivariable logistic regression.
Results: Among right phakic, surgically untouched eyes, the prevalence of emmetropia, myopia, and hyperopia was 20.0% (95% CI 18.0– 22.1%), 25.1% (95% CI 23.0– 27.4%), and 54.8% (95% CI 52.3– 57.3%), respectively. Vector-derived average astigmatism prevalence in both eyes was 44.3% (95% CI 41.6– 46.9%), with against-the-rule astigmatism being the most common pattern. Effective refractive error coverage exceeded 90% for both distance and near vision. The prevalence of any myopic degeneration in either eye was 2.6% (95% CI 1.9– 3.4%). Myopia prevalence among individuals aged 50– 59 years was lower than that reported in other European populations, and use of long-acting anti-muscarinic agents was associated with myopic degeneration (OR 25.70, 95% CI 1.55– 426.04, p=0.023).
Conclusion: This study reports refractive error and myopic macular degeneration prevalence broadly comparable to other European settings. Lower myopia prevalence among individuals aged 50– 59 years may reflect complex gene–environment–behavior interactions. Further investigation of these interactions, as well as the potential impact of long-acting anti-muscarinic agents on myopic macular degeneration, is warranted, particularly in light of the wide confidence interval.
Plain Language Summary: This study explored how common vision problems are among adults aged 50 years and older living in Malta, and which factors may be linked to these problems. The focus was on short-sightedness, long-sightedness, uneven focus, and damage to the retina related to short-sightedness.
Why was this study done?
Uncorrected vision problems are a leading cause of reduced vision worldwide. In Malta, there are no recent national data on these conditions. Such information is important for planning eye care services and reducing avoidable vision loss.
What did the researchers do and find?
We examined a large, representative group of older adults in Malta. We measured vision, examined the eyes, and collected information about health and lifestyle. About one in four people had short-sightedness, while over half had long-sightedness. Many also had uneven focus. Most people who needed vision correction had their distance and near vision needs met. Damage related to short-sightedness affected a small proportion of the population. People aged 50 to 59 had lower rates of short-sightedness than those reported in other European countries. We also observed a possible link between the use of certain long-acting inhaled medicines for breathing conditions and short-sightedness-related eye damage, based on small numbers.
What do these results mean?
Vision problems are common among older adults in Malta, but access to vision correction is generally good. Differences between age groups and the possible medication link need further study.
Keywords: myopia, hyperopia, refractive error, astigmatism, anisometropia, myopic macular degeneration, prevalence, risk factors, ageing, population-based study, long-acting anti-muscarinic agents
Introduction
Refractive errors occur when light does not focus accurately on the retina, causing blurred vision. Myopia results from light focusing in front of the retina, hyperopia from light focusing behind it, and astigmatism from uneven focus across different meridians, while presbyopia develops with age due to reduced accommodative ability. Uncorrected refractive error (URE) is the leading global cause of moderate and severe visual impairment (MSVI) and a major contributor to blindness.1–4 In children, URE can cause amblyopia and strabismus, whereas in older adults it is typically driven by age-related lens changes, opacities, intraocular surgery, pseudophakia, aphakia and ocular pathology.5 Myopia also increases the risk of complications such as myopic macular degeneration (MMD), retinal detachment, cataract and glaucoma.6
Epidemiologic studies commonly define refractive error using spherical equivalent cut-offs of < −0.50D for myopia and > +0.50 D for hyperopia, with astigmatism thresholds of ≥ 0.50–1.00 D, as applied in this study.7–10 In Europe, myopia affects around 27–31% of adults, hyperopia 23–25%, and astigmatism 24–40%.10,11 Myopia prevalence is highest in younger adults, while hyperopia increases with age.11,12 Regionally, Southeast Asia (32.9%) and Europe (27.0%) report the highest myopia prevalence, and global projections estimate almost 50% prevalence by 2050, including 56% in Western Europe.9,10
Risk factors for refractive errors include age, sex, education, genetics, near work, and reduced outdoor activity.12–18 MMD is more common in females, urban populations, older individuals and those with high myopia.19,20 URE remains the most common cause of MSVI globally and the third leading cause of blindness in people aged 50+, despite the availability of effective correction.2 Effective refractive error coverage (eREC) is highest in high-income countries and lowest in low-income regions, with WHO aiming for a 40% global increase by 2030.21,22
In Malta, the only population-based study to date, conducted in 1989 in individuals aged 40+, reported a refractive error prevalence of 47.6%, corrected refractive error of 39.3%, and under-corrected refractive error of 8.3%, corresponding to an estimated eREC of 82.5%.23,24 No updated national data are available, highlighting the need for contemporary prevalence estimates to guide public health planning and eye care service provision.
The Malta Eye Study (TMES) is a population-based, cross-sectional study assessing the prevalence of visual impairment (VI) and common eye diseases in Maltese adults aged 50–80.25,26 The present analysis focuses primarily on the prevalence of refractive error, effective refractive error coverage, and associated risk factors in this population. Findings related to myopic macular degeneration are reported as a secondary outcome within the context of myopia-related complications.
Material and Methods
TMES methodology, including sample size derivation, is detailed elsewhere.25 The study adhered to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist,27(Supplementary Table 1).
Ethical Clearance and Permissions
Ethical approval was granted by the University of Malta Faculty Research Ethics Committee (FRECMDS_1819_94) before data collection in 2019. The study followed the Declaration of Helsinki28 and General Data Protection Regulation (GDPR)29 guidelines, with hospital and Data Protection Officer approvals. Informed consent was obtained, and data were pseudonymized.
Study Population
A random sample of 4006 individuals aged 50–80 years, stratified by age, sex, and locality, obtained from the Malta Electoral Register, was invited for an ophthalmic assessment between September 2021 and July 2024.
Ophthalmic Assessment
The individuals were examined at Mater Dei Hospital between September 2021 and May 2024 and at Gozo General Hospital between June 2024 and July 2024.
The assessment involved visual acuity tests and autorefraction, subjective refraction, anthropometric (weight, height) and clinical (blood pressure and capillary blood glucose) measurements, Goldmann tonometry, a slit lamp based anterior segment and dilated posterior segment indirect (90D) examination, fundus photography and swept-source optical coherence tomography (OCT) scanning of the macula and disc. Autorefraction was performed using the Visionix VX120 multimodal diagnostic platform (Visionix, Luneau Technology Group, Chartres, France).30 OCT was performed using the DRI OCT Triton (Topcon Corporation, Tokyo, Japan). Subjective refraction was performed only in participants with presenting visual acuity worse than 6/12 who demonstrated improvement with pinhole testing, primarily for clinical management rather than analytical purposes. Autorefraction data were therefore used for refractive error classification, as these were available for all participants. All ocular assessments were performed by the same ophthalmologist, the first author of this paper (DA).The questionnaire included themes related to sociodemographic status, medical and ocular history.
Definitions Used
Refractive status was defined based on spherical equivalent (SE = sphere + ½ cylinder, in diopters, D) and cylinder/axis data obtained from autorefraction. Emmetropia was classified as SE between −0.50 D and +0.50 D inclusive. Myopia was defined as SE < −0.50 D, further subdivided into low myopia (−3.00 D < SE < −0.50 D), moderate myopia (−6.00 D ≤ SE ≤ −3.00 D), and high myopia (SE < −6.00 D). Hyperopia was defined as SE > +0.50 D, with subcategories mild (+0.50 D < SE ≤ +2.00 D), moderate (+2.00 D < SE ≤ +5.00 D) and high hyperopia (SE > +5.00 D). Astigmatism was considered present when negative cylinder power was ≤ −0.75 D. Average eye astigmatism was further quantified using power-vector analysis,31 converting each eye’s cylinder (C) and axis (α) to J0 and J45 components where J0 = −(C/2)cos(2α) and J45 = −(C/2)sin(2α). These values were computed for both eyes, averaged per individual, then back transformed to conventional cylinder magnitude and axis to determine overall classification. Axis-specific astigmatism categories were defined using a ±20° allowance around the principal axes, with with-the-rule astigmatism defined as 160°–20°, against-the-rule astigmatism as 70°–110°, and oblique astigmatism as >20° to <160°, consistent with power-vector analysis approaches used in epidemiological studies. Anisometropia was defined as an interocular spherical equivalent difference ≥1.00 D, consistent with commonly used epidemiological definitions.
Distance and near eREC were calculated from presenting vision using met, undermet, and unmet need categories. For distance, “a” represented spectacle/contact lens wearers (or those with refractive surgery) with presenting visual acuity (VA) ≥ 6/12 (met need); “b” included spectacle/contact lens wearers (or refractive surgery) with presenting VA < 6/12 who improved to ≥ 6/12 on pinhole or refraction (undermet need); “c” comprised those with presenting VA < 6/12 without correction who improved to ≥ 6/12 on pinhole or refraction (unmet need). Distance eREC was calculated as a / (a + b + c). Near categories were defined analogously: “d” for near spectacle wearers (or multifocal implants) with presenting near VA ≥ N6 (met need); “e” for near spectacle wearers (or implants) with presenting near VA < N6 who improved to ≥ N6 with refraction (undermet need); and “f” for those with presenting near VA < N6 without correction who improved to ≥ N6 with refraction (unmet need). Near eREC was calculated as d / (d + e + f).21
MMD was graded from fundus images and 90D dilated fundoscopy using the meta-analysis for pathological myopia (META-PM) photographic classification: 0 = no myopic retinal changes; 1 = tessellated fundus; 2 = diffuse chorioretinal atrophy; 3 = patchy chorioretinal atrophy; 4 = macular atrophy; with additional plus-lesions (lacquer cracks, choroidal neovascularization/Fuch’s spot, posterior staphyloma) recorded separately.32
Exclusion Criteria
Although the TMES cohort included a broader population, the analysis on refractive error focused exclusively on phakic eyes without any history of ocular surgery. Only such surgically untouched eyes were included in the descriptive and refractive error analysis to ensure that refractive measurements represented the eye’s natural state. Excluding pseudophakic or surgically altered eyes prevented potential distortion of refractive error distributions and avoided bias in examining associations with relevant risk factors.
Statistical Analysis
Statistical analyses were done using SPSS Statistics v23 (IBM Corp).33 Demographic variables (age, sex, district) were compared with national census data34 for representativeness using chi-square and binomial tests while weights (Population proportion / Sample proportion) adjusted the sample to census data for ages 50–80. Spherical equivalent descriptives, including normality assessment with skewness, kurtosis and Kolmogorov–Smirnov testing, were produced for each eye. Interocular correlation was assessed using Spearman’s rho, agreement using intraclass correlation coefficients, and refractive status agreement using Cohen’s kappa. Wilcoxon signed-rank tests were used to compare paired measurements where appropriate. Descriptive statistics were used to provide prevalence estimates with 95% confidence intervals. Categorical predictors of refractive error types were tested with Chi-square or Fisher’s exact tests. Significant univariate predictors (p<0.05) were included in backward stepwise binary logistic regression models on the basis of the Wald test, with absence of ARMD as reference. The models’ final steps were presented. Missing data, being minimal, were handled by listwise deletion, assumed missing completely at random, with no imputation.
Comparison with European Datasets
For comparison with the E3 Consortium data,11 age-standardization was performed using the 2010 Standard European population.35 Cases with retinal detachment, cataract surgery, or refractive surgery were excluded to align with the original study criteria. Refractive error definitions matched those used by E3,11 employing the average SE between both eyes to classify cases: myopia as SE ≤ −0.75 diopters (D), high myopia as SE ≤ −6.00 D, and hyperopia as SE ≥ +1.00 D.
For comparison with Haarman et al,36 TMES applied its high myopia definition based on SE ≤ −6.00 D, as axial length data were unavailable. MMD was classified using the META-PM system, consistent with their approach. The TMES high myopia subgroup was age-standardized to match their age distribution, and analysis was limited to this group for direct comparison.
Results
A total of 1,794 individuals were assessed between September 2021 and July 2024, yielding a response rate of 44.8%. Sample representativity was evaluated against the national census,34 showing good alignment for age, sex, and district when considered separately. However, there was an underrepresentation of males (p<0.001) and females (p=0.009) aged 50–59 in Northern Harbor, and of females aged 50–59 in Gozo (p=0.004). To correct this, weighting based on national census34 data was applied. Missing data were minimal: 0.4% for most questionnaire items, 4.8% for autorefraction and 8.1% for education (post-assessment).
Within the assessed sample, 1733 individuals performed the autorefraction test in at least one eye (1707 right responses and 1619 left responses). Out of all the individuals interviewed, (n=1786), 92.6% (95% CI 91.3–93.8%) self-reported having the need for glasses (distance or near). Distance glasses were used among 34.0% (95% CI 31.8–36.3%) while near glasses were used among 58.6% (95% CI 56.2%, 60.9%) of the respondents. Varifocal lenses were used among12.4% (95% CI 10.9%, 14.1%) while bifocals were used by 8.4% (95% CI 7.2%, 9.8%). Descriptive statistics for the SEs of the right and left eye are available in Supplementary Table 2. Despite a 24.1% (95% CI 22.0–26.3%) rate of anisometropia (Supplementary Figure 1), the right and left SEs were strongly correlated (ρ = 0.856, p < 0.001) with good agreement (intraclass correlation coefficient (ICC) = 0.791). The refractive statuses of the right and left eyes were reliable (κ=0.636, p<0.001) and the right SE was used to categorize refractive status in TMES.
Right and left cylinder values showed moderate correlation (ρ = 0.518, p < 0.001), moderate agreement (ICC= 0.450) and no significant difference (Wilcoxon p = 0.538), indicating some variability between measurements. The reliability of astigmatism between each eye was poor (κ=0.360, p<0.001) and hence average astigmatism was calculated.
Prevalence of Refractive Errors and Myopic Macular Degeneration
The prevalence rates of emmetropia, myopia and hyperopia in right phakic surgically untouched eyes within the census-adjusted TMES population were 20.0% (95% CI 18.0–22.1%), 25.1% (95% CI 23.0–27.4%) and 54.8% (95% CI 52.3–57.3%) respectively. The prevalence of vector-derived average astigmatism among the phakic surgically untouched eyes was 44.3% (95% CI 41.6–46.9%), against the rule being the commonest kind. The prevalence of refractive error groups among the whole population and among the populations with ocular surgery are available as Supplementary Tables 3 and 4 respectively. The prevalence of any MMD in either eye was 2.6% (95% CI 1.9–3.4%). Further subgroup prevalence rates are provided in Table 1.
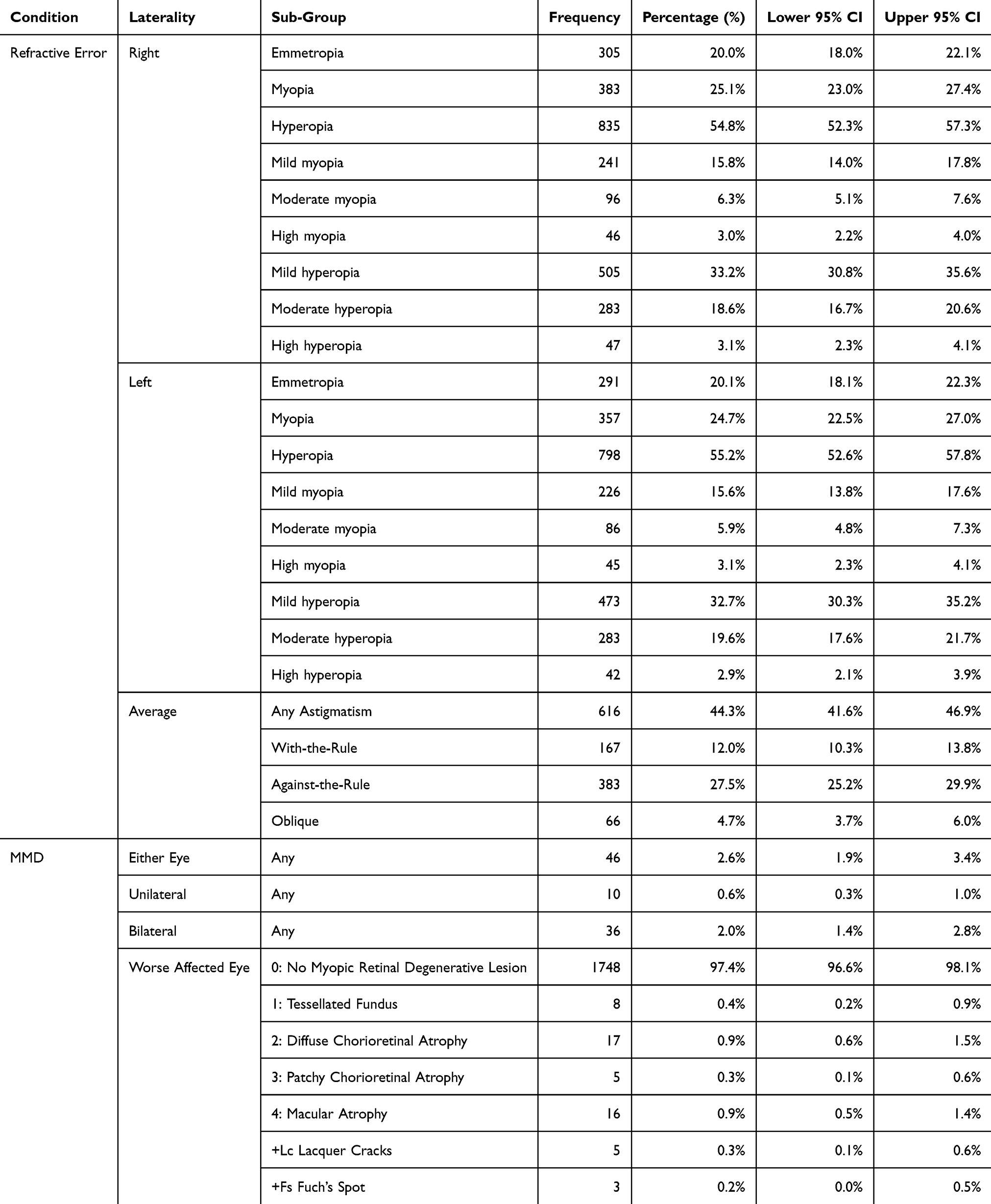 |
Table 1 Prevalence of Refractive Error Groups Among the Census-Adjusted TMES Population with Phakic, Surgically Untouched Eyes (n Right = 1523, n Left = 1446, n Both Eyes = 1392), by Laterality, and Prevalence of Myopic Macular Degeneration (MMD) According to the META-PM Study Classification Among the Census-Adjusted TMES Population (n = 1794) |
Refractive Errors and Myopic Degeneration by Age and Sex
The prevalence rates of myopia and its severity did not alter significantly with age or gender (Figure 1 and Supplementary Figure 2), while hyperopia (Figure 1), astigmatism (mainly against the rule - Figure 2) and anisometropia increased with age. Hyperopia was commoner in females (57.8%, 95% CI 54.2–61.4%) than in males (51.8%, 95% CI 48.2–55.4%) and this trend was mainly noted from the 60 years and older. Hyperopia’s increase by age was mainly seen with the rise in moderate hyperopia, and less-so with increasing high hyperopia (Supplementary Figure 3). Astigmatism was more common in males (47.9%, 95% CI 44.1–51.7%) than females (40.7%, 95% CI 37.0–44.4%) and this trend was mostly significant in the 50–59 years age group (Supplementary Figure 4). The corneal astigmatism in the average eyes changed significantly with increasing age (p=0.001) (Supplementary Figure 5). MMD increased significantly by age but not with gender (Supplementary Figure 6).
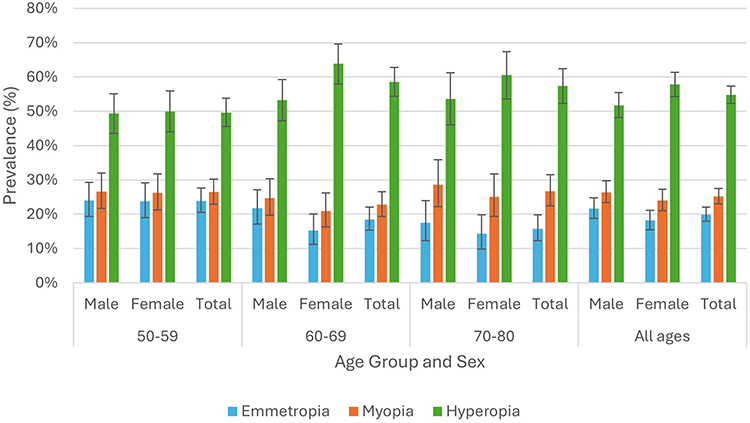 |
Figure 1 Prevalence rates of emmetropia, myopia, and hyperopia in the surgically untouched, phakic right eyes of individuals in the census-adjusted TMES population, stratified by age group and sex. |
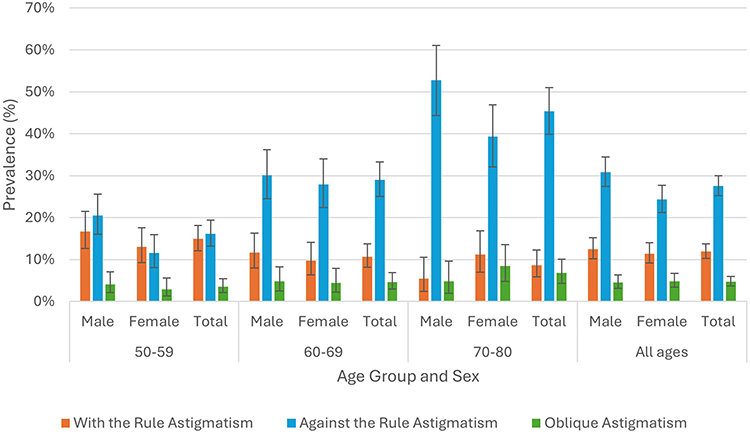 |
Figure 2 Prevalence rates of vector-analysed, averaged with-the-rule, against-the-rule, and oblique astigmatism in the surgically untouched, phakic eyes of individuals in the census-adjusted TMES population, stratified by age group and sex. |
Comparison with European Data
TMES participants showed significantly lower myopia rates in middle age compared to E3, with prevalence at 50–54 years of 14.1% (95% CI 10.7–18.2) in TMES versus 20.9% (95% CI 18.6–23.2) in E3, and at 55–59 years of 12.8% (95% CI 9.3–16.9) versus 16.6% (95% CI 14.2–18.9), respectively. Despite a downward trend in myopia in E3 beyond the age of 60, TMES showed significantly higher and increasing rates past the age of 70 (Figure 3). This pattern was also observed for low myopia and moderate myopia but not for high myopia (Supplementary Figures 7–9) TMES had significantly higher hyperopia rates than E3 in individuals aged 50–64 years, with hyperopia rates increasing in both studies within this age group and levelling out almost equally beyond the age of 65 (Figure 4). High hyperopia was significantly more prevalent in TMES than in E3 among the 50–54, 60–64, and 65–69 age groups (Supplementary Figure 10).
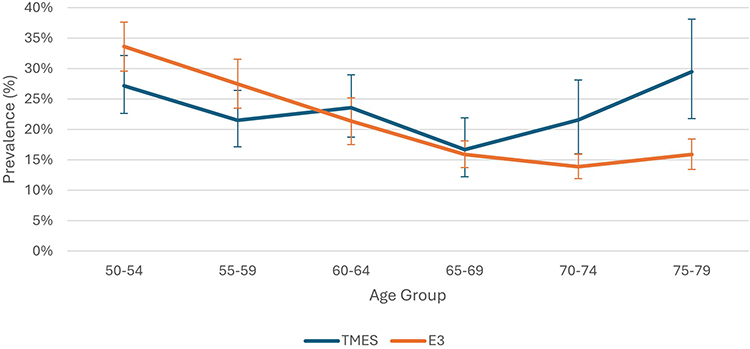 |
Figure 3 Line chart comparing the rates of myopia (with 95% CI bars), defined as an average spherical equivalent of ≤-0.75 D between both eyes, in phakic individuals without a history of retinal detachment or refractive surgery, between the E3 Consortium11 and the age-standardized TMES population, stratified by 5-year age groups. |
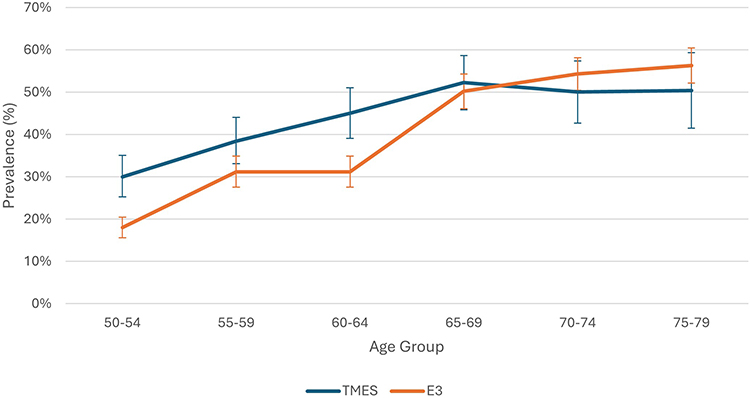 |
Figure 4 Line chart comparing the rates of hyperopia (with 95% CI bars), defined as an average spherical equivalent of ≥+1.00D between both eyes, in phakic individuals without a history of retinal detachment or refractive surgery, between the E3 Consortium11 and the age-standardized TMES population, stratified by 5-year age groups. |
Astigmatism rates were similar in TMES and E3 and increased with age in both studies (Supplementary Figure 11). 11 The proportions of MMD were similar between TMES and the Dutch study (Supplementary Table 5). 36
Predictors of Refractive Error and Myopic Macular Degeneration
Multivariate analysis (95% CI of ORs and p values in Supplementary Tables 6-9) showed that, compared to emmetropia, myopia was significantly associated with tertiary education (OR: 2.35), relative to primary education, as well as with the presence of anisometropia (OR: 3.22) and peripapillary atrophy (OR: 7.30). Myopia was significantly less prevalent among individuals who wore sunglasses (OR: 0.49). Compared to emmetropia, hyperopia’s prevalence was significantly lower with tertiary level education (OR:0.66), relative to primary education, and decreased significantly in those who wore sunglasses (OR:0.60) (Supplementary Table 6).
Astigmatism was significantly associated with the male gender (female vs male OR: 0.69) increasing age (OR per year: 1.04), with the presence of cortical lens opacities (OR:1.51), anisometropia (OR:2.08), mild bilateral (OR:1.89), mild unilateral VI (OR:1.47) and unilateral MSVI (OR:2.13) (Supplementary Table 7). On adjusting for age and educational level, corneal astigmatism was not found to be significantly associated with the female gender in TMES (OR:1.07, p=0.601). After adjusting for lens opacities, myopia, and hyperopia, each diopter increase in cylinder power was associated with significantly higher odds of anisometropia (OR per diopter: 1.73, 95% CI 1.47–2.02, p < 0.001). There was a weak negative correlation between interocular average spherical equivalent and interocular average positive cylinder (ρ = –0.089, p = 0.001). However, myopia was not significantly related to astigmatism after adjusting for anisometropia and other covariates.
Anisometropia was significantly associated with mild unilateral VI (OR:2.36), unilateral MSVI (OR:29.14), unilateral blindness (OR: 15.83) and myopia (OR:3.31). Additionally, compared to no astigmatism, anisometropia was associated with with-the-rule astigmatism (OR:1.66), against-the-rule astigmatism (OR: 2.07) and oblique astigmatism (OR: 2.99) (Supplementary Table 8).
Baseline characteristics and multivariable predictors of myopic macular degeneration within the TMES cohort are detailed in Supplementary Table 9. MMD was significantly associated with domestic work in relation to employed individuals (OR:4.52), self-reported use of long-acting anti-muscarinic agents (LAMA) (OR: 25.70), moderate myopia (OR:27.88), high myopia (OR:65.67), mild VIOU (OR:6.94), unilateral MSVI (OR:5.38), unilateral blindness (OR:12.43) and peripapillary atrophy (OR:20.60). Lower MMD rates were significantly associated with a history of hat wearing (OR:0.20).
Effective Refractive Error Coverage
The overall eREC for distance and near were 92.8% (95% CI 91.0–94.4%) and 93.7% (95% CI 91.2–95.6%) respectively. These indices did not vary by age group or gender (Supplementary Table 10).
Discussion
From a clinical and public health perspective, these findings provide contemporary, nationally representative refractive error prevalence estimates for Malta, addressing a long-standing evidence gap. The high effective refractive error coverage observed suggests generally good access to vision correction services; however, the substantial burden of hyperopia, astigmatism, and anisometropia in older adults highlights the ongoing need for targeted refractive services, regular eye examinations, and age-appropriate optical correction to reduce avoidable visual impairment.
Comparison with European Data
The differences in refractive error rates between TMES and the E3 Consortium could thus be influenced by methodology-related, genetic, environmental, and cohort-related factors.
TMES classifications were based on autorefractor measurements, whereas five of fifteen E3 studies used subjective refraction and the remainder employed various autorefractor models. Different definitions of refractive error hinder direct comparison. In E3, astigmatism was defined as ≥1 D, with no specification as to whether it was derived from cylinder powers or J0/J45 vectors.11
Myopia prevalence at ages 50–59 was significantly lower in TMES than in E3, possibly reflecting Malta’s mild winter climate, which encourages greater outdoor activity, a recognized protective factor in childhood and adolescence.37 Such early-life exposures may contribute to the lower mid-life prevalence observed. In the Southern European (Thessaloniki) E3 cohort,11 myopia rates increased in older age groups, potentially due to nuclear38 and non-nuclear sclerosis–related myopic shift.39 Historical differences in access to vision care may also have influenced refractive outcomes in older cohorts.
E3 hyperopia prevalence was lower than in earlier US, Australian, and Western European datasets.40 Higher TMES hyperopia rates, particularly at ages 50–64, may be attributable to early-life environmental factors, differences in cortical cataract prevalence or exclusion, or genetic predisposition. The observed plateau in hyperopia prevalence beyond age 65 in both cohorts may reflect a balance between age-related hyperopic and myopic lens changes, as well as cohort effects.
In TMES, astigmatism increase by age could not be attributed solely to lenticular changes, as corneal astigmatism also increased significantly with age.
Comparison of MMD rates with the Dutch study was limited by its inclusion of axial length (≥26 mm) in the high myopia definition, which was not available in TMES.36
Associations of Refractive Errors and Myopic Macular Degeneration
This study assessed associations of refractive error groups focusing on phakic eyes to avoid inaccuracies from self-reported pre-operative status. Consistent with prior research, increasing age correlated with astigmatism, reflecting age-related changes in corneal curvature and/or lens structure. Educational attainment was strongly associated with refractive error, with higher education linked to increased myopia and decreased hyperopia, supporting multifactorial lifestyle and environmental influences. Increased near-work like reading and computer use causes accommodative stress and axial elongation, while less outdoor time, common in higher education, is a known myopia risk.37
Sunglasses wear was associated with lower odds of myopia and hyperopia independently of cataract presence, likely reflecting easier access to non-prescription sunglasses among individuals without refractive errors. Cortical cataract remained significantly associated with astigmatism after adjusting for nuclear sclerosis, a relationship rarely quantified in the literature to date.
An association between long-acting anti-muscarinic agent (LAMA) use and MMD was observed; however, this finding was based on small numbers, with 2 of 9 individuals (22.2%) using these agents having myopic macular degeneration, compared with 2.5% among non-users. This resulted in a wide confidence interval, indicating substantial statistical uncertainty. Importantly, smoking history and self-reported respiratory disease were not significantly associated with myopic macular degeneration in univariate analyses. Nevertheless, residual confounding cannot be excluded, particularly as chronic obstructive pulmonary disease may be underreported or misclassified as asthma in questionnaire-based data. This association should be interpreted cautiously and regarded as exploratory rather than causal. Potential biological mechanisms may involve muscarinic receptor pathways: atropine is thought to slow myopia progression via M1 and M4 receptor blockade, while LAMA agents primarily block M3 receptors, which have also been implicated in myopia-related signaling.41–44 Further longitudinal and mechanistic studies are required to clarify the nature and direction of this association.
Protective factors for MMD included hat wearing, possibly reflecting more outdoor time and less myopization MMD was also associated with domestic work, indicating near-work-related risk. Finally, MMD was significantly associated with unilateral MSVI and blindness, emphasizing the need for early detection to preserve vision.
Strengths and Limitations
The strengths of this study include its large, representative, population-based and clinician-led design, with all examinations performed by the same validated specialist. This approach eliminated inter-observer variability and ensured intra-observer consistency, thereby enhancing the validity and robustness of the findings. Furthermore, the use of pupil-dilated indirect fundoscopy and swept-source OCT enabled comprehensive and high-quality MMD assessment.
Several limitations should also be acknowledged. The response rate and the application of sample weighting may have introduced selection bias, and non-responders may have had different, potentially higher, rates of ocular disease. Axial length measurements were unavailable using the Visionix VX120®, limiting direct comparison with studies incorporating biometric definitions of high myopia. Previous medical records were not accessible, and the refractive status of individuals prior to ocular surgery could not be determined; exclusion of these individuals may therefore have influenced prevalence estimates and reduced statistical power for associative analyses. The low prevalence of MMD further limited power for risk factor and severity subgroup analyses, as reflected by wide confidence intervals, including for associations with LAMA agent use. Information on respiratory disease and medication use relied on self-report, which may have led to misclassification, particularly between asthma and chronic obstructive pulmonary disease, and residual confounding cannot be excluded. Finally, the cross-sectional design precludes causal inference and limits assessment of temporal relationships.
Conclusion
This population-based study provides contemporary, nationally representative estimates of refractive error and myopic macular degeneration among adults aged 50–80 years in Malta. Overall refractive error patterns and MMD prevalence were broadly comparable to other European populations; however, myopia prevalence was notably lower among individuals aged 50–59 years. Effective refractive error coverage for both distance and near vision was high, indicating generally good access to refractive correction services.
The lower mid-life myopia prevalence may reflect complex gene–environment interactions, including lifestyle and climatic factors, and warrants further investigation. An association between LAMA agent use and MMD was observed but given the small number of exposed cases and wide confidence intervals, this finding should be interpreted cautiously and regarded as exploratory. Further longitudinal and mechanistic studies are required to clarify causality and potential clinical implications.
Abbreviations
DNA, Deoxyribonucleic acid; E3, European Eye Epidemiology Consortium; eREC, Effective refractive error coverage; GDPR, General Data Protection Regulation; LAMA, Long-acting anti-muscarinic agents; META-PM, Metanalysis for Pathological Myopia; MMD, Myopic Macular Degeneration; MSVI, Moderate Severe Visual Impairment; OCT, Optical Coherence Tomography; OU, Oculus uterque (both eyes); SE, Spherical Equivalent; STROBE, The Strengthening of the Reporting of Observational Studies in Epidemiology Statement; TMES, The Malta Eye Study; URE, Uncorrected refractive error; VA, Visual Acuity; VI, Visual Impairment; VIOU, Bilateral visual impairment.
Acknowledgments
We thank the management at the Mater Dei and Gozo General Hospitals for their study support as well as all staff, volunteers, participants and assistants involved in data collection. Special thanks to Mrs. Marilyn Grech for her vital logistical support throughout this study.
Disclosure
Dr David Agius reports funding from the following funders:
- The Malta Community Chest Fund (MCCF), coordinated by the University of Malta’s Research, Innovation and Development Trust (RIDT), provided funding amounting to EUR 132,000. This covered equipment, publication and conference costs, and a stipend to Dr. David Agius under a University of Malta Scholarship agreement (30/01/2019, agreement 20190304).
- Tertiary Education Scholarship Scheme (TESS) funded Dr. Agius’s tuition.
- Prohealth Ltd® Malta provided stationery and postage.
- Class Optical® supplied participant gifts.
None of the funders were involved in the study’s design, data, or manuscript decisions. The other authors declare no conflicts of interest in this work.
References
1. Bourne RRA, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990-2010: a systematic analysis. Lancet Glob Health. 2013;1(6):e339–12. doi:10.1016/S2214-109X(13)70113-X
2. Bourne RRA, Steinmetz JD, Saylan M, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021;9(2):e144–e160. doi:10.1016/S2214-109X(20)30489-7
3. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
4. Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012;96(5):614–618. doi:10.1136/bjophthalmol-2011-300539
5. Hashemi A, Khabazkhoob M, Hashemi H. High prevalence of refractive errors in an elderly population; a public health issue. BMC Ophthalmol. 2023;23(1):1–11. doi:10.1186/S12886-023-02791-X/TABLES/4
6. Haarman AEG, Enthoven CA, Willem Tideman JL, Tedja MS, Verhoeven VJM, Klaver CCW. The complications of myopia: a review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61(4):49. doi:10.1167/IOVS.61.4.49
7. Flitcroft DI, He M, Jonas JB, et al. IMI - defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20–M30. doi:10.1167/IOVS.18-25957
8. Foster PJ, Jiang Y. Epidemiology of myopia. Eye. 2014;28(2):202. doi:10.1038/EYE.2013.280
9. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/J.OPHTHA.2016.01.006
10. Hashemi H, Fotouhi A, Yekta A, Pakzad R, Ostadimoghaddam H, Khabazkhoob M. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol. 2018;30(1):3–22. doi:10.1016/J.JOCO.2017.08.009
11. Williams KM, Verhoeven VJM, Cumberland P, et al. Prevalence of refractive error in Europe: the European Eye Epidemiology (E3) consortium. Eur J Epidemiol. 2015;30(4):305–315. doi:10.1007/S10654-015-0010-0/TABLES/3
12. Cumberland PM, Bao Y, Hysi PG, Foster PJ, Hammond CJ, Rahi JS. Frequency and distribution of refractive error in adult life: methodology and findings of the UK biobank study. PLoS One. 2015;10(10). doi:10.1371/JOURNAL.PONE.0139780
13. Tan CSH, Chan YH, Wong TY, et al. Prevalence and risk factors for refractive errors and ocular biometry parameters in an elderly Asian population: the Singapore Longitudinal Aging Study (SLAS). Eye. 2011;25(10):1294. doi:10.1038/EYE.2011.144
14. Gajjar S, Ostrin LA. A systematic review of near work and myopia: measurement, relationships, mechanisms and clinical corollaries. Acta Ophthalmol. 2022;100(4):376–387. doi:10.1111/AOS.15043;WEBSITE:WEBSITE:PERICLES;REQUESTEDJOURNAL:JOURNAL:17553768;WGROUP:STRING:PUBLICATION
15. Biswas S, El Kareh A, Qureshi M, et al. The influence of the environment and lifestyle on myopia. J Physiol Anthropol. 2024;43(1):1–22. doi:10.1186/S40101-024-00354-7
16. Martinez-Perez C, Sanchez-Tena MA, Sánchez-González JM, Villa-Collar C, Alvarez-Peregrina C. Influence of outdoor time on the spherical equivalent and axial length in childhood myopia: a meta-analysis. Acta Ophthalmol. 2025. doi:10.1111/AOS.17478;WGROUP:STRING:PUBLICATION
17. Mei Z, Zhang Y, Jiang W, et al. Efficacy of outdoor interventions for myopia in children and adolescents: a systematic review and meta-analysis of randomized controlled trials. Front Public Health. 2024;12:1452567. doi:10.3389/FPUBH.2024.1452567/BIBTEX
18. Yu CY, Dong L, Li YF, Wei WB. Vitamin D and myopia: a review. Int Ophthalmol. 2024;44(1):1–14. doi:10.1007/S10792-024-03009-9/METRICS
19. Zou M, Wang S, Chen A, et al. Prevalence of myopic macular degeneration worldwide: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(12):1748. doi:10.1136/bjophthalmol-2019-315298
20. Wong YL, Zhu X, Tham YC, et al. Prevalence and predictors of myopic macular degeneration among Asian adults: pooled analysis from the Asian Eye Epidemiology Consortium. Br J Ophthalmol. 2021;105(8):1140–1148. doi:10.1136/BJOPHTHALMOL-2020-316648
21. Bourne RRA, Cicinelli MV, Sedighi T, et al. Effective refractive error coverage in adults aged 50 years and older: estimates from population-based surveys in 61 countries. Lancet Glob Health. 2022;10(12):e1754–e1763. doi:10.1016/S2214-109X(22)00433-8
22. WHO. Web-Based Consultation on the Development of Feasible Global Targets for 2030 on Integrated People-Centred Eye Care; 2020.
23. Cachia J. A Programme for the Control of Primary Open-Angle Glaucoma. Faculty of Public Health; 1995.
24. Cachia J, Soler R, Blagojevic M, Agius Muscat H. Prevalence study of glaucoma in malta and gozo. Vol IV.; 1992. Available from: http://www.um.edu.mt/library/e-articles/mmj/mmj040120.pdf.
25. Agius D, Mamo J, Hammond C, Calleja N, Carbonaro F. The study design and methodology of the Malta Eye Study (TMES), an Ophthalmic Epidemiology Study. South East Eur J Public Health. 2024. doi:10.52710/seejph.498
26. Agius D, Cassar D, Mamo J, Carbonaro F. Visual impairment in malta - preliminary data from the malta eye study. In:Acta Ophthalmologica. Vol. 100. John Wiley & Sons, Ltd; 2022. doi:10.1111/J.1755-3768.2022.0491
27. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
28. The World Medical Association. Declaration of Helsinki – ethical principles for medical research involving human subjects. 1964. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
29. European Parliament and Council. General Data Protection Regulation (GDPR) compliance guidelines. 2016. Available from: https://gdpr.eu/.
30. Gordon-Shaag A, Piñero DP, Kahloun C, et al. Validation of refraction and anterior segment parameters by a new multi-diagnostic platform (VX120). J Optom. 2018;11(4):242–251. doi:10.1016/J.OPTOM.2017.12.003
31. Thibos LN, Wheeler W, Horner D. Power vectors: an application of fourier analysis to the description and statistical analysis of refractive error. Optometry Vision Sci. 1997;74(6).
32. Ohno-Matsui K, Kawasaki R, Jonas JB, et al. International photographic classification and grading system for myopic maculopathy. Am J Ophthalmol. 2015;159(5):877–883.e7. doi:10.1016/j.ajo.2015.01.022
33. IBM Corp. IBM SPSS statistics for windows, version 23.0. Preprint posted online 2015.
34. NSO. Census of population and housing 2021: final report: population, migration and other social characteristics volume 1. 2023. Available from: https://nso.gov.mt/events/census-of-population-and-housing-2021-final-report-population-migration-and-other-social-characteristics/.
35. Eurostat. Revision of the European standard population - report of eurostat’s task force - 2013 edition - products manuals and guidelines - eurostat; 2013. Available from: https://ec.europa.eu/eurostat/web/products-manuals-and-guidelines/-/ks-ra-13-028.
36. Haarman AEG, Tedja MS, Brussee C, et al. Prevalence of myopic macular features in dutch individuals of European ancestry with high myopia. JAMA Ophthalmol. 2022;140(2):115–123. doi:10.1001/JAMAOPHTHALMOL.2021.5346
37. Ying ZQ, Li DL, Zheng XY, Zhang XF, Pan CW. Risk factors for myopia among children and adolescents: an umbrella review of published meta-analyses and systematic reviews. Br J Ophthalmol. 2024;108(2):167–174. doi:10.1136/BJO-2022-322773
38. Lim R, Mitchell P, Cumming RG. Refractive associations with cataract: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci. 1999;40(12):3021–3026.
39. Lee KE, Klein BEK, Klein R, Wong TY. Changes in refraction over 10 years in an adult population: the Beaver Dam Eye Study. Invest Ophthalmol Vis Sci. 2002;43(8):2566–2571.
40. Kempen JH. The prevalence of refractive errors among adults in the United States,Western Europe, and Australia. Archives of Ophthalmology. 2004;122(4):495–505. doi:10.1001/ARCHOPHT.122.4.495
41. Mitchelson F. Muscarinic receptor agonists and antagonists: effects on ocular function. In: Handbook of Experimental Pharmacology. Vol. 208. Berlin, Heidelberg: Springer;2012:263–298. doi:10.1007/978-3-642-23274-9_12
42. Chierigo A, Desideri LF, Traverso CE, Vagge A. The role of atropine in preventing myopia progression: an update. Pharmaceutics. 2022;14(5):900. doi:10.3390/PHARMACEUTICS14050900
43. Alagha K, Palot A, Sofalvi T, et al. Long-acting muscarinic receptor antagonists for the treatment of chronic airway diseases. Ther Adv Chronic Dis. 2014;5(2):85. doi:10.1177/2040622313518227
44. Lin HJ, Wan L, Chen WC, Lin JM, Lin CJ, Tsai FJ. Muscarinic acetylcholine receptor 3 is dominant in myopia progression. Invest Ophthalmol Vis Sci. 2012;53(10):6519–6525. doi:10.1167/IOVS.11-9031
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: Six Month Results from the United States Food and Drug Administration Clinical Trial
Packer M
Clinical Ophthalmology 2022, 16:1541-1553
Published Date: 21 May 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
A Comprehensive Retrospective Analysis of EVO/EVO+ Implantable Collamer Lens: Evaluating Refractive Outcomes in the Largest Single Center Study of ICL Patients in the United States
Albo C, Nasser T, Szynkarski DT, Nguyen N, Mueller B, Libfraind L, Parkhurst G
Clinical Ophthalmology 2024, 18:69-78
Published Date: 9 January 2024
Prevalence of Refractive Errors Among School-Age Children and Adolescents in Saudi Arabia: A Systematic Review and Meta-Analysis
Al Khathami A, Baklola M, Alshehri AA, Alnasser LH, Alshehri RS, Salawi MA, Alwadai RH, Al Ghazwi M, Alanazi AAQ, Alshammari AM, Al-bawah N, Hafez M, Abu Melha A
Clinical Ophthalmology 2025, 19:2117-2132
Published Date: 5 July 2025